Introduction
Hepatocellular carcinoma (HCC) is one of the most
common neoplasms and is considered the third leading cause of
cancer-related mortality worldwide (1). Spontaneous rupture with intratumoral
hemorrhage is one of the life-threatening complications of HCC.
Although the incidence of HCC rupture is ~3–15%, it is associated
with high mortality rates that range between 32 and 75% (2–5). The
disease prognosis remains poor in the absence of appropriate
treatment in the acute phase (6).
Therefore, appropriate treatment selection for patients with HCC
rupture is imperative.
The main treatment for HCC rupture includes
emergency or staged hepatectomy and transcatheter arterial
chemoembolization (TACE) (7).
Several studies have reported a promising outcome following
emergency liver resection (8–10).
However, patients with advanced HCC tend to have poor hepatic
function as a result of chronic hepatitis or liver cirrhosis.
Severe cirrhosis or poor patient status, as determined by vital
signs and blood examination, often reduce the tolerance of patients
to surgery. Conventional TACE has been a widely accepted
therapeutic option for unresectable HCC and has shown optimal
efficacy (11). TACE is a treatment
modality resulting from ischemic necrosis due to arterial
embolization. This condition requires the use of cytotoxic drugs
and results in a cytotoxic effect (12). In addition to the prevention of tumor
progression, TACE is useful in controlling hemorrhage in patients
with HCC rupture (13). However,
severe complications, including hepatic failure, biliary tract
injury, hepatic encephalopathy and renal failure, have been
reported in previous studies (14–16).
Therefore, assessment of the efficacy and safety of TACE treatment
in patients with a ruptured tumor is particularly important. To the
best of our knowledge, no definite recommendation has been issued
regarding the optimal therapeutic approach in cases of HCC rupture,
and the comparative survival benefits of surgery and TACE remain
unclear.
In the present retrospective study, the adverse
reactions of TACE and the independent predictors of post-treatment
survival outcomes in patients with spontaneously ruptured HCC were
investigated. The results were compared with the survival outcomes
of TACE and surgery in patients at a single center in China.
Materials and methods
Patients
The present retrospective study included patients
who underwent TACE or surgery for spontaneous HCC rupture between
April 2015 and October 2017 at the Department of Hepatic Carcinoma
of Fudan University Affiliated Zhongshan Hospital (Shanghai,
China). A total of 70 cases with HCC were enrolled. No patient had
a recent history of HCC treatment, such as surgery or TACE, within
1 month prior to the diagnosis of HCC rupture. HCC was diagnosed
based on the diagnostic criteria issued by the American Association
for the Study of Liver Diseases (17). HCC was staged according to the
Barcelona Clinic Liver Cancer (BCLC) staging system (18). Spontaneous HCC rupture was diagnosed
as disruption of the peritumoral liver capsule with surrounding
fluid in the perihepatic region. Detection was performed by dynamic
computed tomography (CT) and the diagnosis included the presence of
bloody fluid following abdominal puncture.
Database information, such as age, sex and
hypertension history, were reviewed. The presence of shock at
diagnosis was reviewed and the results of laboratory examinations,
including anemia level, baseline liver functions, viral hepatitis
findings and α-fetoprotein (AFP), were evaluated. Details of HCC
tumor status, such as tumor number, tumor size, the presence of
vascular thrombosis and the presence of extra-hepatic invasion,
were obtained by contrast-enhanced CT or magnetic resonance imaging
(MRI) scans. The present study was approved by the Clinical
Research Ethics Committee of Fudan University Affiliated Zhongshan
Hospital.
Treatment procedure
Following stabilization of the hemodynamic status by
volume replacement and transfusion, the patients underwent a full
clinical assessment to evaluate their suitability for surgical
treatment. Contraindications for surgical therapy were determined
as follows: Presence of poorly controlled predominant ascites
and/or hepatic encephalopathy, a prolonged prothrombin time >4
sec and poor performance status. In hemodynamically unstable
patients with an apparent continuous hemorrhage, TACE was
considered if reserve liver function was relatively good regardless
of the correction for coagulopathy.
TACE or open surgery was immediately performed
following diagnosis. These methods were performed concomitantly
with supportive treatment. TACE was performed by femoral artery
puncture using the Seldinger method (19). A total of 39 patients were enrolled.
Prior to TACE, thorough angiography was performed to identify all
feeding arteries of the tumor. Digital subtraction angiography was
performed to observe tumor staining and to confirm the arterial
feeders of the tumor. Following the introduction of a catheter
using the Seldinger technique through the femoral artery, a mixture
of 5–20 ml lipiodol, epirubicin suspension and gelatin sponge
fragments or granules was injected into the tumor-feeding arteries
based on the tumor size and the degree of hemorrhage. According to
the liver function status, 100–150 mg oxaliplatin or 5-fluorouracil
was slowly perfused into the feeding artery under the guidance of
digital subtraction angiography by a catheter. For patients with a
Child-Pugh score (20,21) of 5 and a white blood cell count
≥3×109/l, 150 mg oxaliplatin was given, while patients
with a Child-Pugh score ≥6 or a white blood cell count
<3×109/l, 100 mg oxaliplatin was given. All patients
received 1 g 5-fluorouracil. Angiography was performed to determine
the extent of embolization. A total of 31 patients with ruptured
HCC underwent hepatic resection. Hepatic portal interdiction was
used in 18 patients and 13 patients received blood transfusion
during the procedure.
Follow-up of patients with ruptured
HCC following treatment
The median follow-up period was 20 months. During
follow-up, the laboratory tests were obtained on the 7th day
following the operation. Contrast-enhanced liver CT or MRI scans
were performed at 1 month following the operation and subsequently
once every 3 months. The main endpoint of the study was the control
rate of rupture and hemorrhage of HCC. The overall survival (OS)
and the safety of the procedure were used as secondary
endpoints.
Statistical analysis
Categorical variables are expressed as frequencies
and percentages and were analyzed with the chi-square test.
Continuous variables are expressed as medians and ranges and were
analyzed with the independent sample t-test. Factors that were
found to be significant in univariate analysis were subjected to
multivariate analysis. Cox regression hazard model was used to
identify independent prognostic factors associated with OS.
Propensity score matching (PSM) analysis was used to avoid bias
between the TACE and surgery groups. The OS rates were analyzed
using the Kaplan-Meier method, and the differences were analyzed
with the log-rank test. Statistical analyses were performed using
SPSS 21 (IBM Corp.). P<0.05 was considered to indicate a
statistically significant difference.
Results
Baseline characteristics of
patients
A total of 70 patients were enrolled in the present
study between April 2015 and October 2017. A total of 39 patients
were treated with TACE following spontaneous HCC rupture and 31
were treated with open surgery. The median age was 54 years (range,
31–86 years) and the sample size comprised 55 men and 15 women. A
total of 52 (74.3%) patients exhibited hepatitis B virus (HBV)
infection. Hepatitis C virus (HCV) infection was not detected in
any patient in the present study. The AFP levels in 37 (52.9%)
patients were >400 ng/ml. The Child-Pugh classification
indicated that 40 (57.1%) patients were included in class A, 22
(31.4%) in class B and eight (11.4%) in class C. BCLC staging at
diagnosis indicated that one (1.4%) patient was classified as stage
A, 46 (65.7%) patients were classified as stage B, and 23 (32.9%)
as stage C. Of the 70 patients, 17 (24.3%) exhibited vascular
thrombosis. A total of 40 (57.1%) patients presented with a single
tumor, whereas 30 (42.9%) patients had multiple tumors. The maximum
tumor size in 17 (24.3%) and 24 (34.3%) patients was <5 and
>10 cm, respectively (Table I).
Eight (20.5%) patients exhibited distant metastasis, whereas three
patients presented with metastases in more than one location. Among
these, seven metastases were present in the lung, three in the bone
and three in distant lymph nodes. These eight patients with distant
metastasis were treated with TACE. In the surgery group, no
patients exhibited distant metastasis (Table I).
 | Table I.Clinical characteristics of patients
with spontaneously ruptured hepatocellular carcinoma. |
Table I.
Clinical characteristics of patients
with spontaneously ruptured hepatocellular carcinoma.
| Variable | TACE cases, n
(%) | Surgery cases, n
(%) | P-value | Total cases, n
(%) |
|---|
| Age >60 years | 13 (33.3) | 7 (22.6) | 0.323 | 20 (28.6) |
| Hypertension
history | 16 (41.0) | 12 (38.7) | 0.844 | 28 (40.0) |
| Child-Pugh |
|
| <0.001 |
|
| A | 11 (28.2) | 29 (93.5) |
| 40 (57.1) |
| B | 21 (53.8) | 1 (3.2) |
| 22 (31.4) |
| C | 7 (18) | 1 (3.2) |
| 8 (11.4) |
| AFP >400 ng/l | 27 (69.2) | 10 (32.3) | 0.002 | 37 (52.9) |
| ALT >3 N | 7 (17.9) | 0 (0.0) | 0.015 | 7 (9.9) |
| AST >3 N | 17 (43.6) | 6 (19.4) | 0.032 | 23 (32.9) |
| TBIL >1.5 N | 11 (28.2) | 3 (9.7) | 0.104 | 14 (20.0) |
| ALB ≤35 g/l | 17 (43.6) | 7 (22.6) | 0.066 | 24 (34.3) |
| PT >16 sec | 4 (10.2) | 1 (3.2) | 0.505 | 5 (7.1) |
| Hb, g/l |
|
| <0.001 |
|
|
>90 | 13 (33.3) | 25 (80.6) |
| 36 (51.4) |
|
90-60 | 23 (59.0) | 6 (19.4) |
| 29 (41.4) |
|
<60 | 3 (7.7) | 0 (0.0) |
| 3 (4.3) |
| Scr >1.5 N | 2 (5.1) | 0 (0.0) | 0.499 | 2 (2.9) |
| Positive HBsAg
status | 35 (89.7) | 17 (54.8) | 0.002 | 52 (74.3) |
| Maximum tumor size,
cm |
|
| 0.655 |
|
| ≥5 | 9 (23.1) | 8 (25.8) |
| 17 (24.3) |
| >5
and ≤10 | 18 (46.2) | 11 (35.5) |
| 29 (41.4) |
|
>10 | 12 (30.7) | 12 (38.7) |
| 24 (34.3) |
| Tumor number |
|
| 0.037 |
|
|
Single | 18 (46.2) | 22 (70.9) |
| 40 (57.1) |
|
Multiple | 21 (53.8) | 9 (29.0) |
| 30 (42.9) |
| Capsule
formation |
|
| 0.208 |
|
|
Yes | 18 (46.2) | 19 (61.3) |
| 37 (52.9) |
| No | 21 (53.8) | 12 (38.7) |
| 33 (47.1) |
| Vascular
thrombus |
|
| 0.391 |
|
|
Yes | 11 (28.2) | 6 (19.4) |
| 17 (24.3) |
| No | 28 (71.8) | 25 (80.6) |
| 53 (75.7) |
| Extrahepatic
invasion |
|
|
|
|
| Yes | 8 (20.5) | 0 (0.0) |
| 8 (11.4) |
| No | 31 (79.5) | 31 (100) | 0.007 | 62 (88.6) |
| Shock | 5 (12.8) | 0 | 0.062 | 5 (7.1) |
| BCLC stage |
|
| 0.049 |
|
| A | 0 (0.0) | 1 (3.2) |
| 1 (1.4) |
| B | 22 (56.4) | 24 (77.4) |
| 46 (65.7) |
| C | 17 (43.6) | 6 (19.4) |
| 23 (32.9) |
| Hospital admission
>10 days | 9 (23.1) | 19 (61.3) | <0.001 | 28 (40.0) |
Safety of TACE and surgical
treatment
To evaluate the safety of TACE and resection for
patients with HCC exhibiting spontaneous tumor rupture, the
post-treatment adverse reactions were investigated. Upper abdominal
pain (69.0%), fever (47.1%), neutrophilia (38.6%) and nausea (20%)
were the most common adverse reactions. The majority of the
toxicity events (54.3% of all reported events) was Grade 2 or less.
Grade 3/4 events occurred in 20 patients (14.3%), which included
gastrointestinal hemorrhage, cardiac failure, pulmonary embolism,
shock and recurrent tumor rupture. All of these patients recovered
and were discharged following symptomatic and supportive treatment,
with the exception of two cases of severe hemorrhagic shock and
hepatic failure prior to TACE treatment. These patients did not
survive the hospitalization period. The median duration of hospital
admission of patients in the TACE and surgery groups were 7 and 13
days, respectively (P<0.01; Table
II).
| Table II.Complications following TACE or
surgical treatment. |
Table II.
Complications following TACE or
surgical treatment.
|
| I–II degree
(%) | ≥III degree
(%) | Total (%) | Total after PSM (%)
(12 pairs) |
|---|
|
|
|
|
|
|
|---|
| Complication | TACE | Surgery | TACE | Surgery | TACE | Surgery | P-value | TACE | Surgery | P-value |
|---|
| Abdominal pain | 15 (38.5) | 16 (51.6) | 6 (15.4) | 12 (38.7) | 21 (53.8) | 28 (90.3) | <0.001 | 8 (66.7) | 9 (75.0) | 0.653 |
| Nausea and
vomiting | 10 (25.6) | 2 (6.5) | 2 (6.5) | 0 | 12 (30.8) | 2 (6.5) | 0.012 | 4 (33.3) | 1 (8.3) | 0.132 |
| Fever | 14 (35.9) | 18 (58.1) | 1 (2.6) | 0 | 15 (38.5) | 18 (58.1) | 0.103 | 5 (41.7) | 6 (50.0) | 0.682 |
| Neutrophilia | 15 (38.5) | 12 (38.7) | 0 | 0 | 15 (38.5) | 12 (38.7) | 0.983 | 4 (33.3) | 3 (25.0) | 0.653 |
| Renal failure | 1 (2.6) | 1 (3.2) | 0 | 0 | 1 (2.6) | 1 (3.2) | 0.869 | 0 | 0 | NS |
| Cholecystitis | 1 (2.6) | 0 | 0 | 0 | 1 (2.6) | 0 | 0.369 | 1 (8.3) | 0 | 0.307 |
| Recurrent tumor
rupture | NS | NS | 2 (5.1) | 1 (3.2) | 2 (5.1) | 1(3.2) | 0.696 | 0 | 0 | NS |
| Shock | NS | NS | 1 (2.6) | 1 (3.2) | 1 (2.6) | 1 (3.2) | 0.869 | 0 | 0 | NS |
| Respiratory
failure | 0 | 0 | 1 (2.6) | 0 | 1 (2.6) | 0 | 0.369 | 0 | 0 | NS |
| Pulmonary
embolism | NS | NS | 1 (2.6) | 0 | 1 (2.6) | 0 | 0.369 | 0 | 0 | NS |
| Cardiac
failure | 0 | 0 | 0 | 1 (3.2) | 0 | 1 (3.2) | 0.259 | 0 | 0 | NS |
| Gastrointestinal
hemorrhage | 0 | 0 | 0 | 1 (3.2) | 0 | 1 (3.2) | 0.259 | 0 | 1 (8.3) | 0.307 |
| Hydrothorax | 0 | 2 (6.5) | 0 | 0 | 0 | 2 (6.5) | 0.108 | 0 | 1 (8.3) | 0.307 |
In the TACE group, 21 patients reported various
degrees of upper abdominal pain. This symptom was considered to be
associated with tumor rupture following embolism. Nausea and
vomiting occurred in 12 patients following TACE treatment. However,
the majority of the patients were generally relieved of symptoms
within 24–48 h. Fever with a body temperature between 37.5 and
39.5°C occurred in 15 patients. This symptom gradually decreased
within 3–7 days, possibly due to tumor necrosis and absorption. The
majority of the patients exhibited transient liver damage following
TACE and recovered to normal or baseline levels within 5–8 days
following liver protection therapy. A total of two patients
exhibited renal failure, of which only one was newly diagnosed
following TACE treatment. Furthermore, one patient developed mild
pulmonary embolism and another developed acute cholecystitis of The
National Cancer Institute Common Terminology Criteria for Adverse
Events (22) level 2. The cause of
this was considered to be ectopic embolism. Following TACE, the
patient with cholecystitis recovered within 8 days of antibiotic
treatment, intravascular fluid replacement and fasting. A total of
six patients presented with shock in the TACE group. However, five
of these were in shock prior to the procedure. A total of two
patients (5.3%) exhibited re-rupture of HCC within 1 month
following TACE and underwent retreatment. No hepatic
encephalopathy, gastrointestinal bleeding, liver abscess or other
serious complications occurred.
In the surgery group, a high number of patients
presented with abdominal pain and a number of patients exhibited
nausea and vomiting following treatment (P<0.05). There were no
significant differences in the incidence of any other complications
between these two treatment groups. Two patients exhibited massive
hydrothorax, both recovering following thoracic puncturing and
piping. One patient experienced gastrointestinal hemorrhage and
recovered following 7 days of conservative treatment. One patient
presented with grade 3 cardiac failure and shock following
resection. This patient finally recovered following symptomatic and
supportive treatment.
Univariate and multivariate analysis
for predictors of TACE treatment
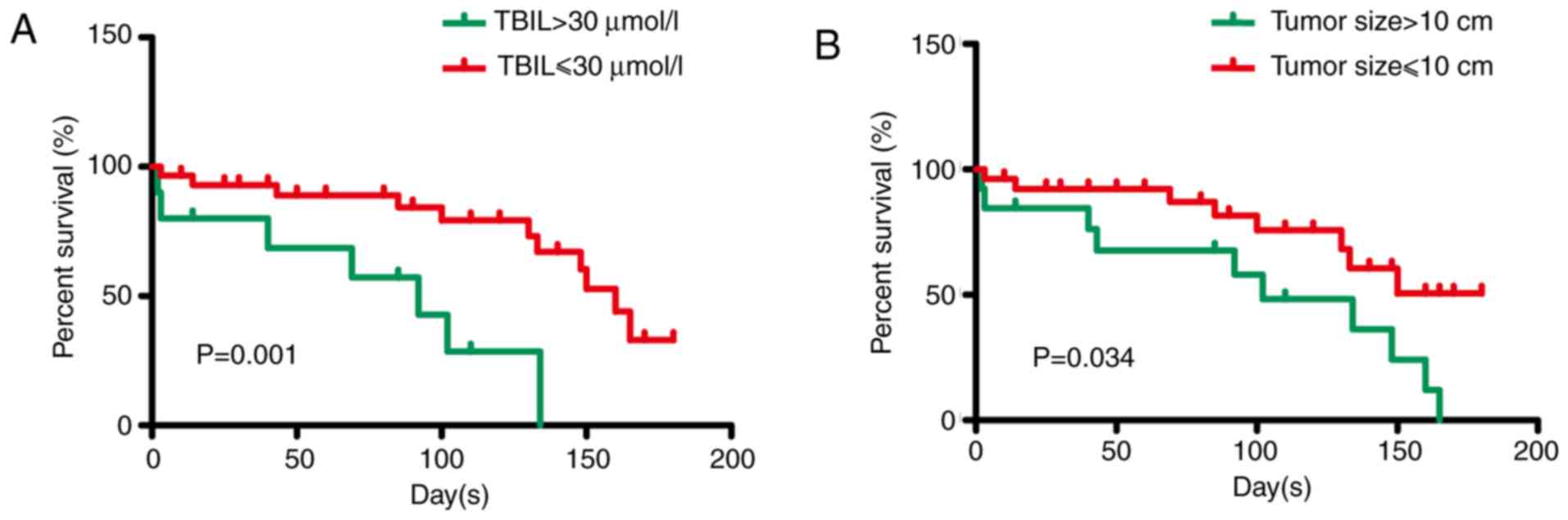
Prior to multivariate analysis, univariate analysis
was conducted in all 39 patients treated with TACE. Univariate
analysis resulted in the identification of the following thresholds
regarding specific parameters: Maximum tumor size >10 cm
(P=0.044), Child-Pugh score >7 (P=0.094), serum total bilirubin
levels >1.5 times higher than normal levels (P=0.001) and serum
aspartate transferase levels >3 times higher than normal levels
(P=0.086) (Table III). These
thresholds were used as determinants of poor 30-day survival
(Table III). Additional analysis
using multivariate Cox regression analysis led to the
identification of the following thresholds: Maximum tumor size
>10 cm (HR, 2.739; P=0.034) and serum total bilirubin levels
>30 µmol/l (HR=0.165, P=0.001). These were used as significant
determinants of inverse OS (Table
IV; Fig. 1A and B).
| Table III.Univariate analysis of factors
associated with overall survival. |
Table III.
Univariate analysis of factors
associated with overall survival.
| Factor | Cases | P-value |
|---|
| Hypertension
history | 16 | 0.923 |
| Child-Pugh score
>7 | 14 | 0.094 |
| AFP >400
ng/l | 27 | 0.698 |
| ALT >3 N | 7 | 0.255 |
| AST >3 N | 17 | 0.086 |
| TBIL >1.5 N | 11 | 0.001 |
| Maximum tumor size
>10 cm | 12 | 0.044 |
| Vascular
thrombus | 11 | 0.950 |
| Extrahepatic
invasion | 8 | 0.622 |
| BCLC stage C | 17 | 0.187 |
| Table IV.Multivariate analysis of factors
associated with overall survival. |
Table IV.
Multivariate analysis of factors
associated with overall survival.
| Factor | HR | 95% CI | P-value |
|---|
| TBIL >30
µmol/l | 0.165 | 0.055–0.497 | 0.001 |
| Maximum tumor size
>10 cm | 2.739 | 1.079–6.955 | 0.034 |
| AST >3 N | 0.615 | 0.387–2.176 | 0.170 |
| Child-Pugh score
>7 | 1.665 | 0.634–5.878 | 0.197 |
Comparison of clinical parameters and
survival analysis by treatment types
To determine the efficacy and prognosis of TACE for
spontaneously ruptured HCC, the OS rates of the patients with
ruptured HCC who received TACE and/or surgical treatment was
examined. Initially, the clinical parameters of the two therapies
were analyzed. No significant difference was noted with regard to
the parameters of age distribution and sex ratio between the TACE
and surgery groups. The history of hypertension and the
characteristics of the tumors, such as maximum tumor size, capsule
formation and vascular thrombus, were also similar between the two
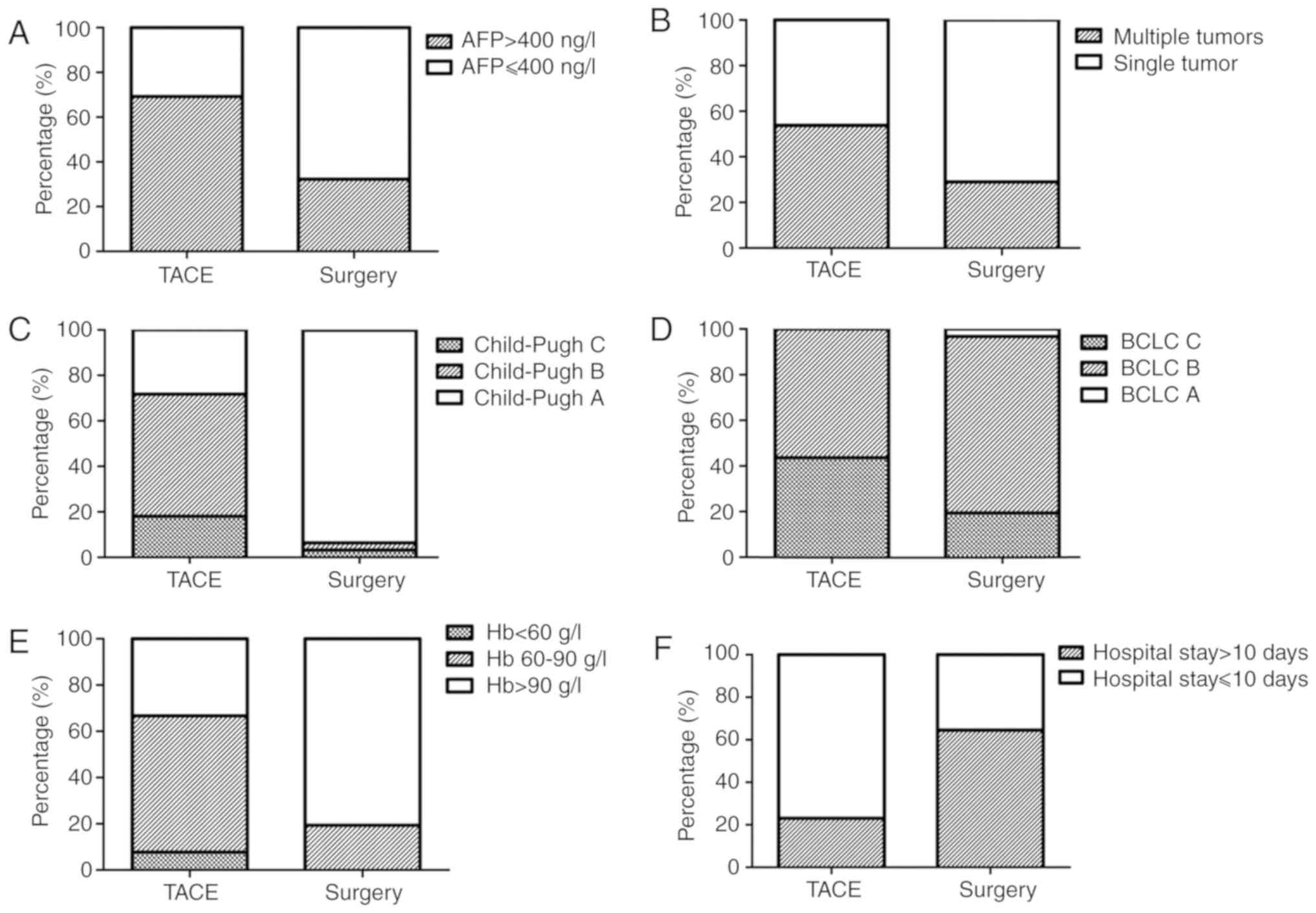
groups (Table I). The total serum
bilirubin levels in the TACE group were significantly higher than
those in the surgery group (P<0.01). Patients in the TACE group
exhibited higher Child-Pugh scores and BCLC stages compared with
those in patients in the surgery group (P<0.01; Fig. 2).
In the TACE group, rupture and hemorrhage of HCC
were effectively controlled in 37 (94.9%) patients. All of these
patients were discharged, although four underwent second-stage
resection. These four patients were excluded when comparing the OS
rates between the two treatments. Two (5.1%) patients did not
survive during the duration of hospital admission due to severe
hemorrhagic shock and consequent hepatic and renal failure. In the
surgery group, all patients were effectively treated and
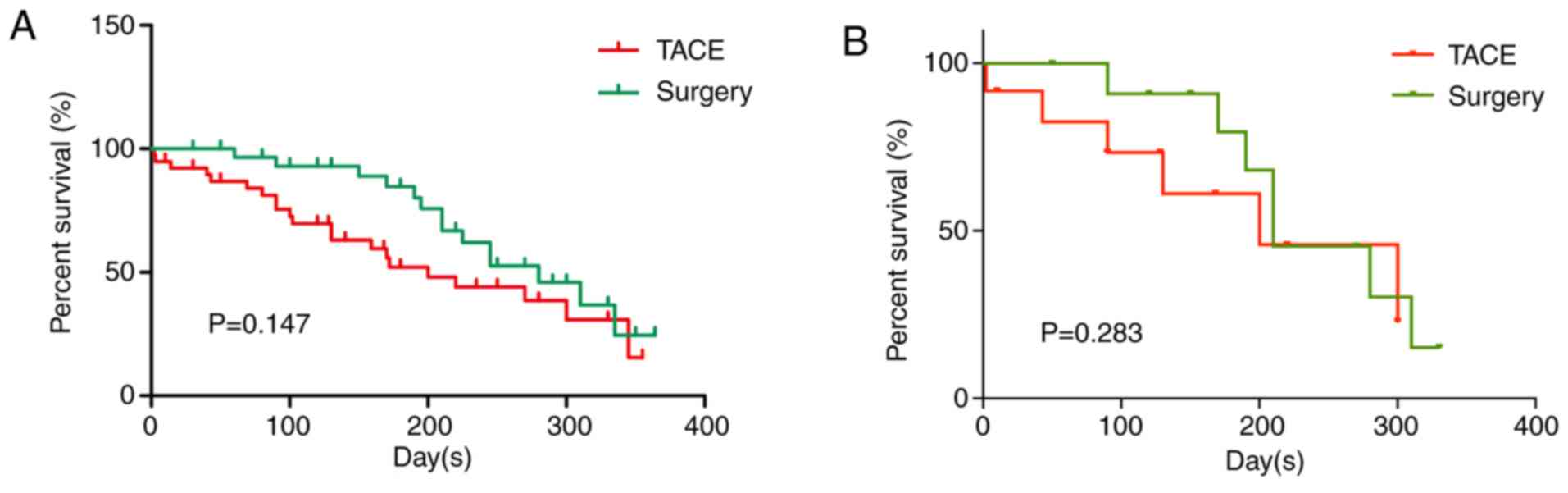
discharged. The median survival time periods were 7.4 and 8 months
for the TACE and surgery groups, respectively (P>0.05). The
cumulative survival rates at 1, 6 and 12 months were 92.3, 53.8 and
46.2%, and 100, 87.1 and 54.8%, for the TACE and surgery groups,
respectively (Fig. 3). In the TACE
group, 17 patients succumbed to hepatic failure, one to brain
metastasis and three to massive digestive hemorrhage. The causes of
death in the surgery group were similar (12 due to hepatic failure
and two due to massive digestive hemorrhage). The cumulative
survival rates of the surgery group patients at 1 and 6 months were
significantly higher than those noted in the TACE group
(P<0.01). This may be associated with the poor liver function
and severe liver cirrhosis noted in the TACE group. However, the
mortality rate at the 12-month period did not differ significantly
between the two groups (P>0.05; Fig.
3A). Survival analysis in 12 pairs of patients from the TACE
and surgery groups was matched with PSM. The mortality rate at the
12-month period did not differ significantly between the two groups
following PSM (P>0.05; Fig. 3B).
Additionally, the duration of hospital admission in the TACE group
was considerably shorter (P<0.01; Fig. 2F). These results demonstrated that
TACE and surgery treatment resulted in similar OS rates at the
12-month period, although TACE treatment revealed lower OS rates at
the 1- and 6-month periods. This indicated that TACE significantly
reduces the duration of hospital admission.
Discussion
Spontaneous rupture of HCC is one of the most common
emergencies in the advanced stage of this disease (23). Various hypotheses have been
formulated to explain the exact mechanism that leads to HCC rupture
(24–26). Central necrosis in the growing tumor,
portal hypertension, neoplastic invasion causing a local increase
of venous pressure within the tumor and a previous vascular injury
are associated with the incidence of hemorrhage within the tumor
(25). The optimal treatment
approach for HCC rupture has not been yet identified (27). Surgery is considered one of the best
options for the treatment of HCC with acute spontaneous rupture
(28). However, several studies have
reported that only a limited number of patients with ruptured HCC
can be managed with surgical hepatic resection (29–31).
Additionally, surgery is technically difficult to perform in cases
of a severely cirrhotic liver (5),
and patients with poor liver function and severely ruptured HCC
cannot tolerate hepatic resection (32). It has been reported that TACE is
effective in achieving immediate hemostasis for ruptured HCC
(33). However, the safety and
survival benefits of TACE compared with those of surgical resection
remain unclear.
The present study demonstrated that the levels of
liver enzymes were significantly higher in the first 3 days
following TACE compared with those noted at baseline. These
differences were reduced within 7 days and the levels of liver
enzymes returned to normal and/or baseline levels. These results
indicated that TACE treatment did not cause severe damage to normal
liver tissues. Serious injury to the bile duct is an additional
risk of TACE that can lead to cholesteatoma, as reported in
previous studies (14). In the
present study, only one patient (2.6%) presented with this
complication and recovered in a few days. Furthermore, no other
severe complications, such as hepatic encephalopathy, liver abscess
or gastrointestinal bleeding, were noted, which had been reported
by previous studies (34). In the
present study, the procedure was well tolerated by all study
subjects. The general post-procedure complications were minor and
self-limiting.
Kirikoshi et al (35) reported that poor liver function only
influenced the parameter of short-term mortality rate (21 days),
whereas long-term survival (140 days) was not noted in any cases of
ruptured HCC. In their study, the size of the tumor (diameter >7
cm) was the only independent factor influencing long-term survival
among patients who underwent successful TACE. However, in the
present study, the endpoint of a tumor diameter >5 or 7 cm had
no significant effect on the survival rate, as determined by
multivariate analysis. By contrast, the endpoints of maximum tumor
diameter >10 cm and serum total bilirubin levels >30 µmol/l
were determined to be independent predictors of survival rate by
multivariate analysis. This discrepancy may be associated with the
different review time and the different medical history of the
subjects. Additional investigations are required to address this
discrepancy.
Currently, there is debate regarding the optimal
treatment for spontaneous rupture of HCC (23). The 30-day mortality rate of the TACE
group was reported to be lower than that of the surgery group in a
previous study (36). The present
study revealed that the cumulative survival rate in the open
surgical group at 1 month was significantly higher than that of the
TACE group, which is in accordance with previous studies. However,
the cumulative survival rates at 12 months were similar between the
two treatment groups. The clinical characteristics between the TACE
and surgery groups were also analyzed and the data indicated that
patients in the TACE group exhibited higher Child-Pugh scores and
BCLC stages compared with those in patients of the surgical group.
Furthermore, comparison of the duration of hospital admission
revealed that TACE was associated with a significant reduction in
the duration of hospital admission compared with that in the
surgical group. These results indicated that the long-term survival
rate of patients treated with TACE was similar to that of patients
treated with open surgery and hospital admission was shorter.
In conclusion, the present study demonstrated that
the majority of the patients exhibited transient liver damage
following TACE and liver function recovered to normal or baseline
levels within a few days of treatment. TACE treatment did not cause
serious complications. The maximum tumor size and baseline
bilirubin levels were identified as major factors associated with
disease prognosis. TACE exhibited acceptable tolerability in
patients with spontaneously ruptured HCC, and long-term mortality
rates were similar to those in the open surgery treatment group.
Furthermore, TACE treatment significantly reduced the duration of
hospital admission. Therefore, TACE is considered an option for
unresectable HCC rupture due to its efficacy and safety. The
present study may provide useful information for clinicians and may
aid the determination of the most appropriate treatment option for
spontaneous tumor rupture.
Acknowledgements
Not applicable.
Funding
The present study was supported by the Young
Scientists Fund of the National Natural Science Foundation of China
(grant nos. 81702310 and 81502007).
Availability of data and materials
All data generated and/or analyzed during the
present study are included in this published article.
Authors' contributions
JZ designed the study and wrote the manuscript. CL
revised the manuscript, collected and analyzed the data. YC and RC
analyzed and interpreted the data. TX and XX statistical analyzed
the data. LZ and ZR designed the study. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Clinical Research
Ethics Committee of Fudan University Affiliated Zhongshan
Hospital.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Raoul JL and Gilabert M: Hepatocellular
carcinoma: Slow progress in a booming epidemic. J Oncol Pract.
13:365–366. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Wang ZM, Lu XS and Qiu F: Hepatectomy for
spontaneous rupture of hepatocellular carcinoma without portal
triad clamping. Oncol Lett. 14:3997–4004. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Zhu Q, Li J, Yan JJ, Huang L, Wu MC and
Yan YQ: Predictors and clinical outcomes for spontaneous rupture of
hepatocellular carcinoma. World J Gastroenterol. 18:7302–7307.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zhao GG, Xu W, Tian YH and Li DX: Survival
analysis of patients with spontaneous rupture of hepatocellular
carcinoma. Zhonghua Gan Zang Bing Za Zhi. 20:838–842. 2012.(In
Chinese). PubMed/NCBI
|
|
5
|
Zhang XF, Wei T, Liu XM and Lv Y:
Spontaneous tumor rupture and surgical prognosis of patients with
hepatocellular carcinoma. Scand J Gastroenterol. 47:968–974. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Han SR, Kim JM, Choi GS, Park JB, Kwon CH,
Kim SJ and Joh JW: Protrusion of hepatocellular carcinoma is a
predictor of early recurrence in hepatectomy patients after
spontaneous rupture. Ann Surg Treat Res. 91:17–22. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zhu Q, Qiao GL, Xu C, Guo DL, Tang J, Duan
R and Li Y: Partial hepatectomy for spontaneous tumor rupture in
patients with hepatocellular carcinoma: A retrospective cohort
study. Cancer Manag Res. 9:525–537. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ren A, Luo S, Ji L, Yi X, Liang J, Wang J
and Wan S: Peritoneal metastasis after emergency hepatectomy and
delayed hepatectomy for spontaneous rupture of hepatocellular
carcinoma. Asian J Surg. 42:464–469. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wu JJ, Zhu P, Zhang ZG, Zhang BX, Shu C,
Mba'nbo-Koumpa AA, Zhang ZW, Huang ZY, Zhang WG, Lau WY and Chen
XP: Spontaneous rupture of hepatocellular carcinoma: Optimal timing
of partial hepatectomy. Eur J Surg Oncol. 45:1887–1894. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Zhong F, Cheng XS, He K, Sun SB, Zhou J
and Chen HM: Treatment outcomes of spontaneous rupture of
hepatocellular carcinoma with hemorrhagic shock: A multicenter
study. Springerplus. 5:11012016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hiraoka A, Kumada T, Kudo M, Hirooka M,
Koizumi Y, Hiasa Y, Tajiri K, Toyoda H, Tada T, Ochi H, et al:
Hepatic function during repeated TACE procedures and prognosis
after introducing sorafenib in patients with unresectable
hepatocellular carcinoma: Multicenter analysis. Dig Dis.
35:602–610. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Li C, Wen TF, Yan LN, Lu WS, Li B, Wang
WT, Xu MQ and Yang JY: Liver resection versus liver resection plus
TACE for patients with hepatocellular carcinoma beyond Milan
criteria. J Surg Res. 209:8–16. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Maoz D, Sharon E, Chen Y and Grief F:
Spontaneous hepatic rupture: 13-year experience of a single center.
Eur J Gastroenterol Hepatol. 22:997–1000. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Tu J, Jia Z, Ying X, Zhang D, Li S, Tian F
and Jiang G: The incidence and outcome of major complication
following conventional TAE/TACE for hepatocellular carcinoma.
Medicine (Baltimore). 95:e56062016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Zou JH, Zhang L, Ren ZG and Ye SL:
Efficacy and safety of cTACE versus DEB-TACE in patients with
hepatocellular carcinoma: A meta-analysis. J Dig Dis. 17:510–517.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hu H, Han XK, Long XR, Fan J, Yan ZP, Wang
JH and Liu R: Prognostic nomogram for post-surgical treatment with
adjuvant TACE in hepatitis B virus-related hepatocellular
carcinoma. Oncotarget. 7:58302–58314. 2016.PubMed/NCBI
|
|
17
|
Marrero JA, Kulik LM, Sirlin CB, Zhu AX,
Finn RS, Abecassis MM, Roberts LR and Heimbach JK: Diagnosis,
staging, and management of hepatocellular carcinoma: 2018 practice
guidance by the American Association for the study of liver
diseases. Hepatology. 68:723–750. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Gómez-Rodríguez R, Romero-Gutièrrez M,
Artaza-Varasa T, González-Frutos C, Ciampi-Dopazo JJ,
de-la-Cruz-Pèrez G and Sánchez-Ruano JJ: The value of the Barcelona
clinic liver cancer and alpha-fetoprotein in the prognosis of
hepatocellular carcinoma. Rev Esp Enferm Dig. 104:298–304. 2012.(In
English, Spanish). View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Driscoll SH, Grollman JH, Ellestedt MH, Po
JB, Sample WF and Bos CJ: Single-wall arterial puncture with a
disposable needle. Radiology. 113:4701974. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Child CG and Turcotte JG: Surgery and
portal hypertension. Major Probl Clin Surg. 1:1–85. 1964.PubMed/NCBI
|
|
21
|
Pugh RN, Murray-Lyon IM, Dawson JL,
Pietroni MC and Williams R: Transection of the oesophagus for
bleeding oesophageal varices. Br J Surg. 60:646–649. 1973.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kim AY, Unger K, Wang H and Pishvaian MJ:
Incorporating Yttrium-90 trans-arterial radioembolization (TARE) in
the treatment of metastatic pancreatic adenocarcioma: A single
center experience. BMC Cancer. 16:4922016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Rathor M, Lal A and Dhiman RK: Spontaneous
rupture of hepatocellular carcinoma. J Clin Exp Hepatol. 4:188–189.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
You MX, Yu XX, Wu K, Lin YS, Zhu GQ and
Shi CS: Analysis of risk factors for spontaneous rupture of
hepatocellular carcinoma. Zhonghua Zhong Liu Za Zhi. 35:217–220.
2013.(In Chinese). PubMed/NCBI
|
|
25
|
Zhu LX, Geng XP and Fan ST: Spontaneous
rupture of hepatocellular carcinoma and vascular injury. Arch Surg.
136:682–687. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Zhu LX, Wang GS and Fan ST: Spontaneous
rupture of hepatocellular carcinoma. Br J Surg. 83:602–607. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Wang B, Lu Y, Zhang XF, Yú L, Pan CE and
Wu Z: Management of spontaneous rupture of hepatocellular
carcinoma. ANZ J Surg. 78:501–503. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Lai EC and Lau WY: Spontaneous rupture of
hepatocellular carcinoma: A systematic review. Arch Surg.
141:191–198. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Li J, Huang L, Liu CF, Cao J, Yan JJ, Xu
F, Wu MC and Yan YQ: Risk factors and surgical outcomes for
spontaneous rupture of BCLC stages A and B hepatocellular
carcinoma: A case-control study. World J Gastroenterol.
20:9121–9127. 2014.PubMed/NCBI
|
|
30
|
Lee HS, Choi GH, Kang DR, Han KH, Ahn SH,
Kim DY, Park JY, Kim SU and Choi JS: Impact of spontaneous
hepatocellular carcinoma rupture on recurrence pattern and
long-term surgical outcomes after partial hepatectomy. World J
Surg. 38:2070–2078. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Zhou SJ, Zhang EL, Liang BY, Zhang ZY,
Chen XP and Huang ZY: Distilled water lavage during surgery
improves long-term outcomes of patients with ruptured
hepatocellular carcinoma. J Gastrointest Surg. 19:1262–1270. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Aoki T, Kokudo N, Matsuyama Y, Izumi N,
Ichida T, Kudo M, Ku Y, Sakamoto M, Nakashima O, Matsui O, et al:
Prognostic impact of spontaneous tumor rupture in patients with
hepatocellular carcinoma: An analysis of 1160 cases from a
nationwide survey. Ann Surg. 259:532–542. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Raoul JL, Forner A, Bolondi L, Cheung TT,
Kloeckner R and de Baere T: Updated use of TACE for hepatocellular
carcinoma treatment: How and when to use it based on clinical
evidence. Cancer Treat Rev. 72:28–36. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Hsin IF, Hsu CY, Huang HC, Huang YH, Lin
HC, Lee RC, Chiang JH, Lee FY, Huo TI and Lee SD: Liver failure
after transarterial chemoembolization for patients with
hepatocellular carcinoma and ascites: Incidence, risk factors, and
prognostic prediction. J Clin Gastroenterol. 45:556–562. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Kirikoshi H, Saito S, Yoneda M, Fujita K,
Mawatari H, Uchiyama T, Higurashi T, Imajo K, Sakaguchi T, Atsukawa
K, et al: Outcomes and factors influencing survival in cirrhotic
cases with spontaneous rupture of hepatocellular carcinoma: A
multicenter study. BMC Gastroenterol. 9:292009. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Jin YJ, Lee JW, Park SW, Lee JI, Lee DH,
Kim YS, Cho SG, Jeon YS, Lee KY and Ahn SI: Survival outcome of
patients with spontaneously ruptured hepatocellular carcinoma
treated surgically or by transarterial embolization. World J
Gastroenterol. 19:4537–4544. 2013. View Article : Google Scholar : PubMed/NCBI
|