Introduction
Regorafenib and trifluridine/tiperacil combination
(TAS102) has shown survival benefit among patients with metastatic
or recurrent colorectal cancer in cases where salvage treatment of
fluoropyrimidine, irinotecan, oxaliplatin, anti-vascular
endothelial growth factors (VEGFs), and anti-epidermal growth
factor receptor therapy is required following failure of standard
therapy. However, a clear and objective evidence of response of
these drugs is rarely observed (1–4).
Herein, we report the case of a patient with rectal
cancer refractory to multiple surgical interventions and standard
chemotherapy, for whom administration of regorafenib treatment
resulted in immediate improvement of respiratory failure caused by
carcinomatous pulmonary lymphangitis in response to regorafenib
treatment. Written informed consent for publication was obtained
from the next of kin.
Case report
A 65-year-old Japanese man underwent curative
surgery for advanced rectal cancer with lymph node metastases at
Ina Central Hospital without consecutive adjuvant treatment in
April 2011. The tumor was diagnosed as Stage IIIB (T3N1bM0;
AJCC-TNM 8th edition) by the pathological department of Ina Central
Hospital. In October 2013, bilateral pulmonary metastases were
detected by computed tomography without clinical symptom during
routine follow-up and resected at Aizawa Hospital (Matsumoto city,
Nagano, Japan). No definite histological differences were noted
when compared with the specimen obtained during initial surgery.
KRAS exon 2 codon 12D mutation was detected in the primary lesion
and pulmonary metastases by Scorpion ARMS method
(TheraScreen®: K-RAS Mutation kit). In March 2015,
magnetic resonance imaging (MRI) revealed four brain metastases
during the investigation of persistent headache, which were treated
with stereotactic body radiotherapy (SBRT). Consecutively, followed
by general chemotherapy with capecitabine 1,000 mg/m2
(twice daily for 2 weeks), 7.5 mg/kg bevacizumab and 130
mg/m2 oxaliplatine on day 1 repeated every 3 weeks until
February 2016 when other brain metastases, multiple pulmonary
metastases with pleural deposits, and multiple bone metastases were
detected by MRI, computed tomography (CT) and positron emission
tomography scans. After pleurodesis and SBRT for symptom
palliation, general combination chemotherapy with 40
mg/m2 S-1 (a combination of tegafur, gimeracil and
oteracil) twice daily for 2 weeks, and irinotecan 150
mg/m2 on day 1 repeated every 3 weeks was initiated in
April 2016. After 3 weeks, the treatment was discontinued because
of grade 3 general fatigue and poor appetite.
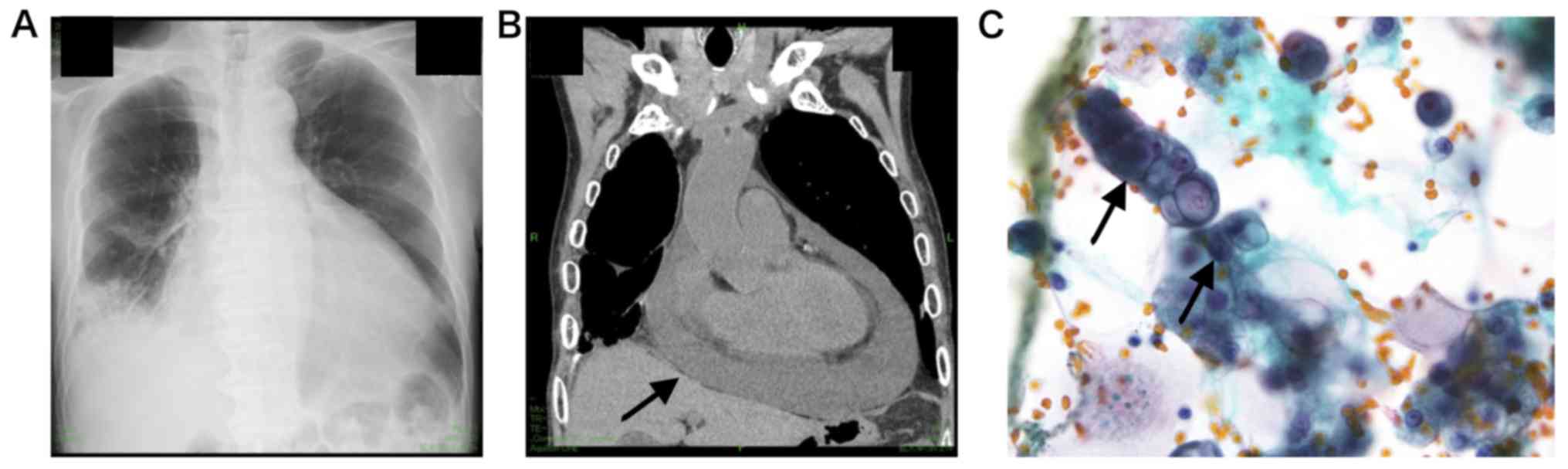
On June 23, 2016, the patient was admitted to Ina
Central Hospital with dyspnea. Assessment involving chest X-ray and
CT, revealed cardiac tamponade (Fig. 1A
and B). Pericardiocentesis detected 600 ml of pericardial
effusion, in which adenocarcinoma cells were detected. (Fig. 1C). The patient was discharged 4 days
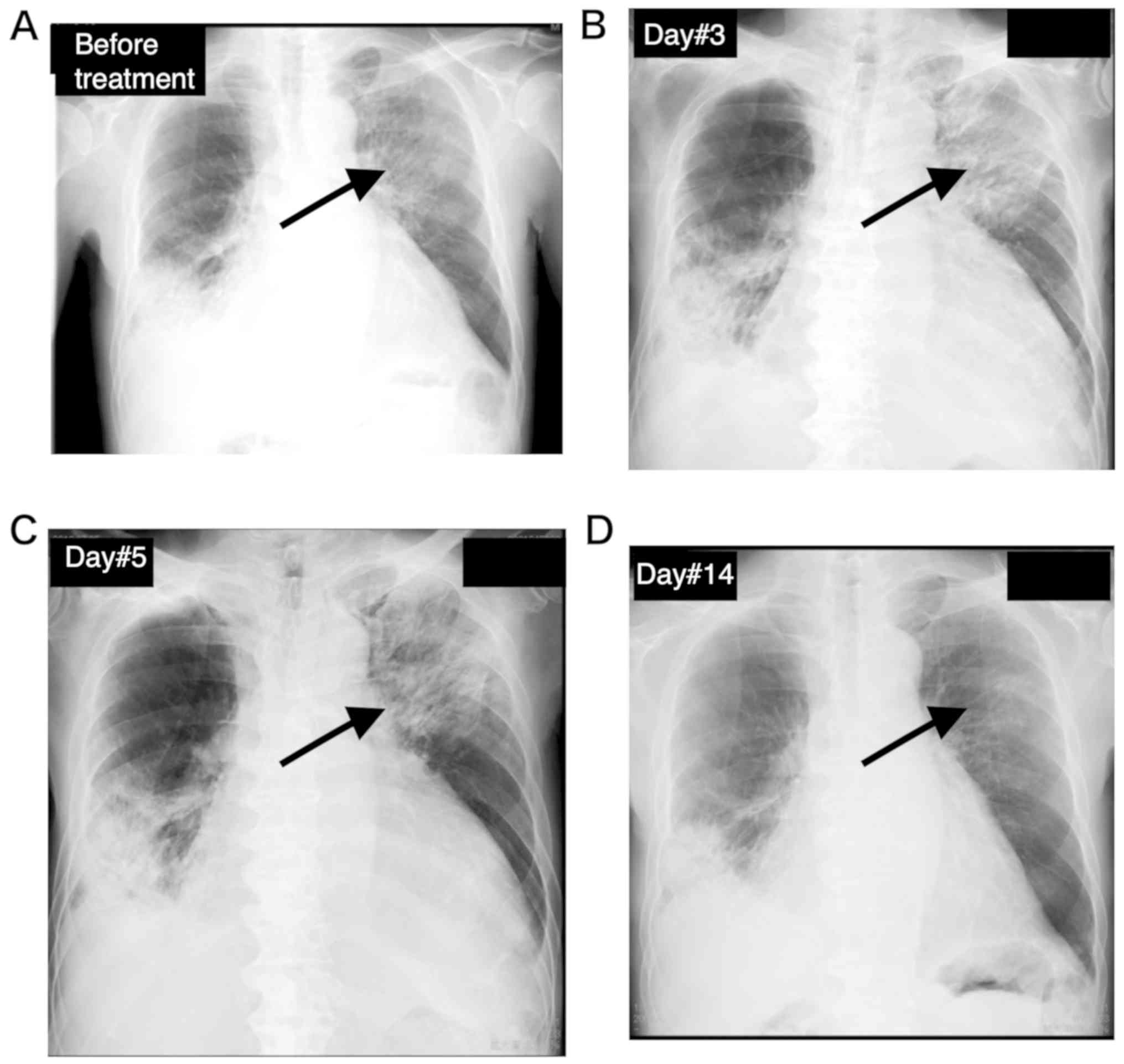
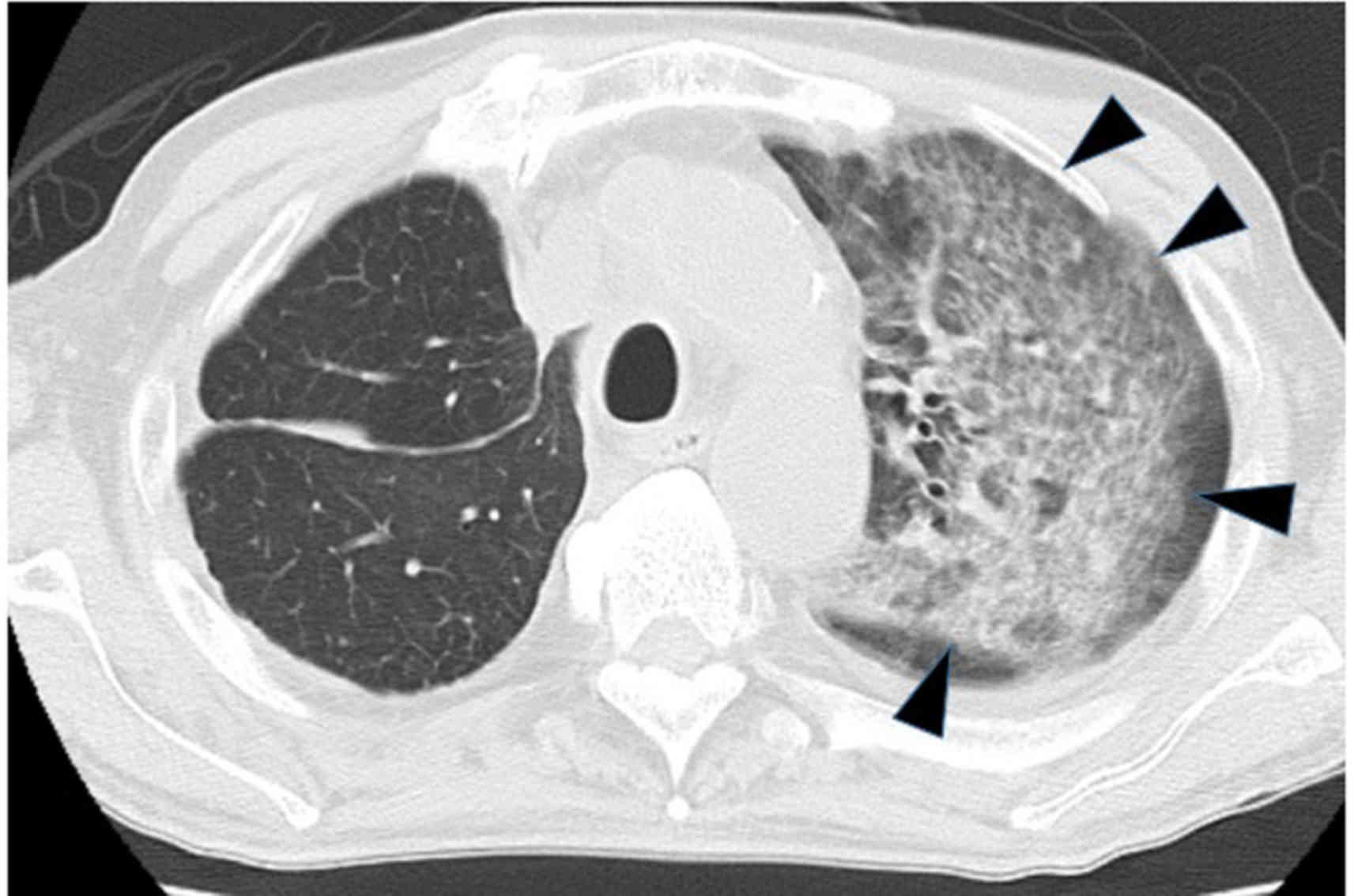
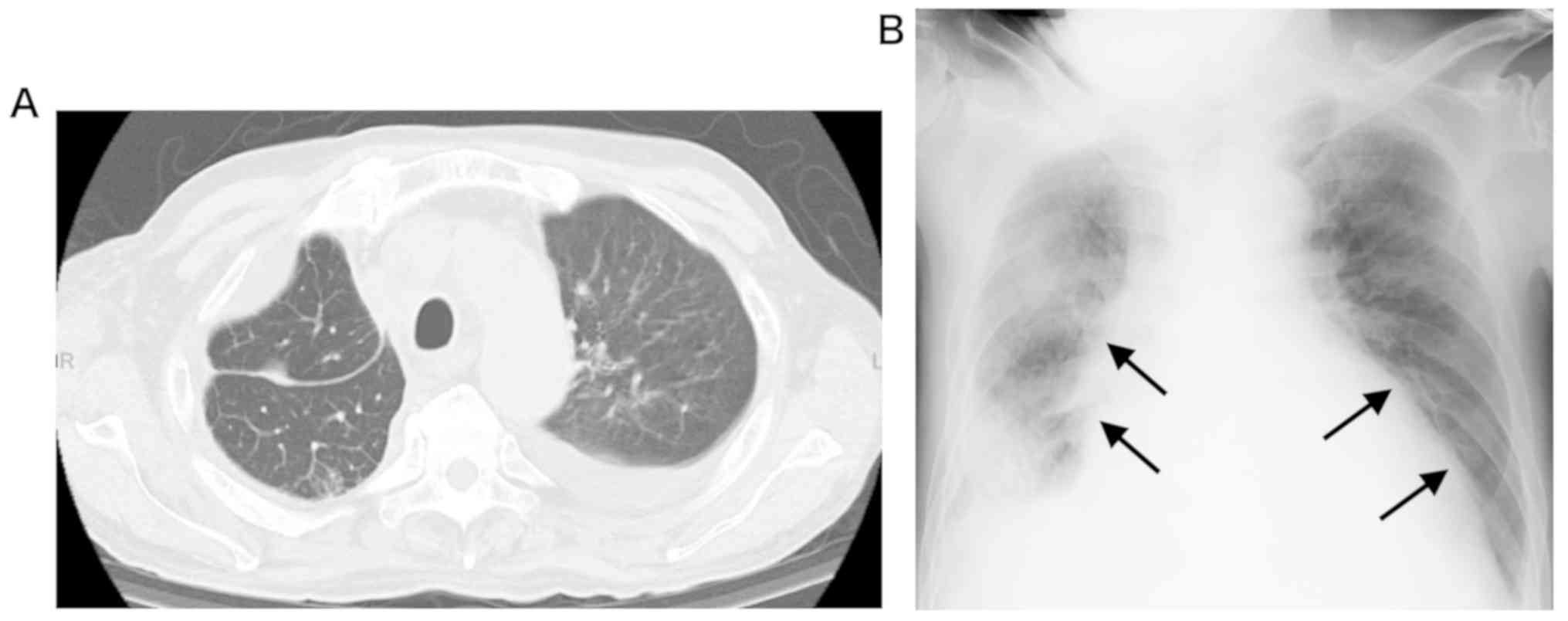
after pericardiocentesis; however, he was readmitted 2 days after
discharge because of dyspnea. Unlike the previous admission, chest
X-ray (Fig. 2A) and CT (Fig. 3) revealed an interstitial pattern in
the upper lobe of the left lung without evident increase in
pericardial effusion.
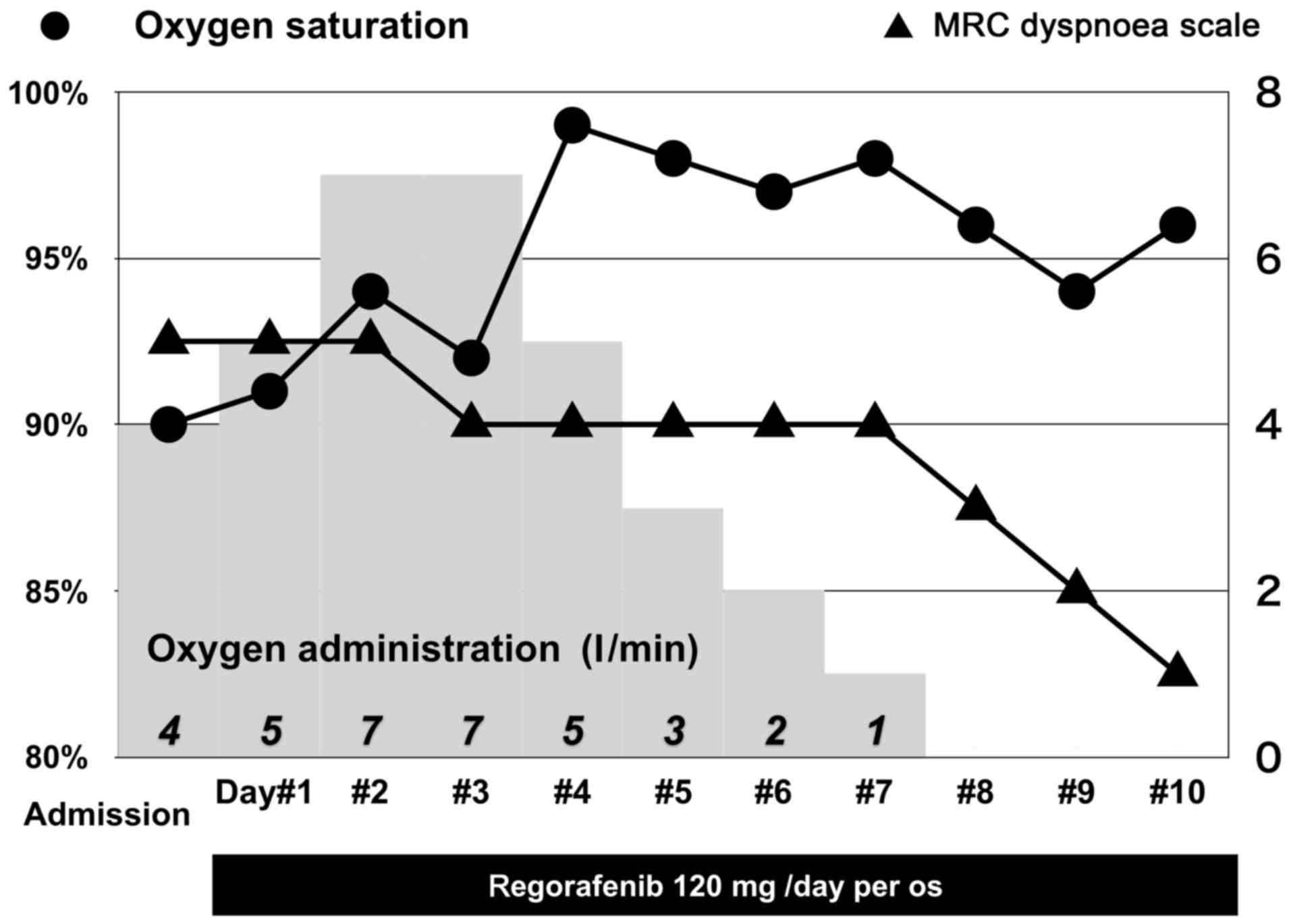
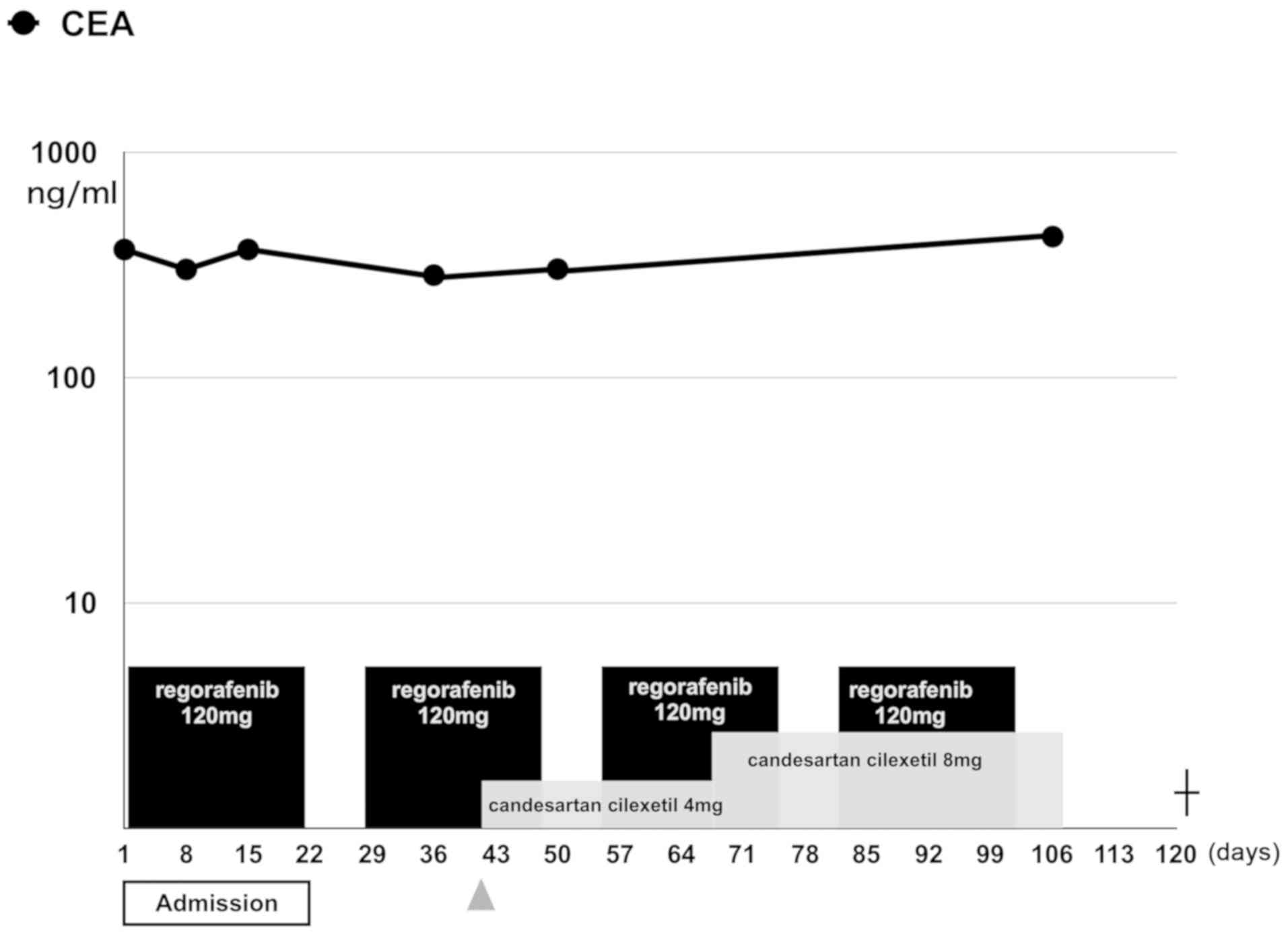
On the day after the readmission (day 1), once-daily
oral administration of 120 mg regorafenib was given for 21
consecutive days. Dyspnea was assessed by the Medical Research
Council (MRC) Dyspnea Scale (5),
following hospitalization and oxygen saturation improved quickly
and steadily following initiation of regorafenib. Oxygen
administration was decreased gradually from day 4 until day 8
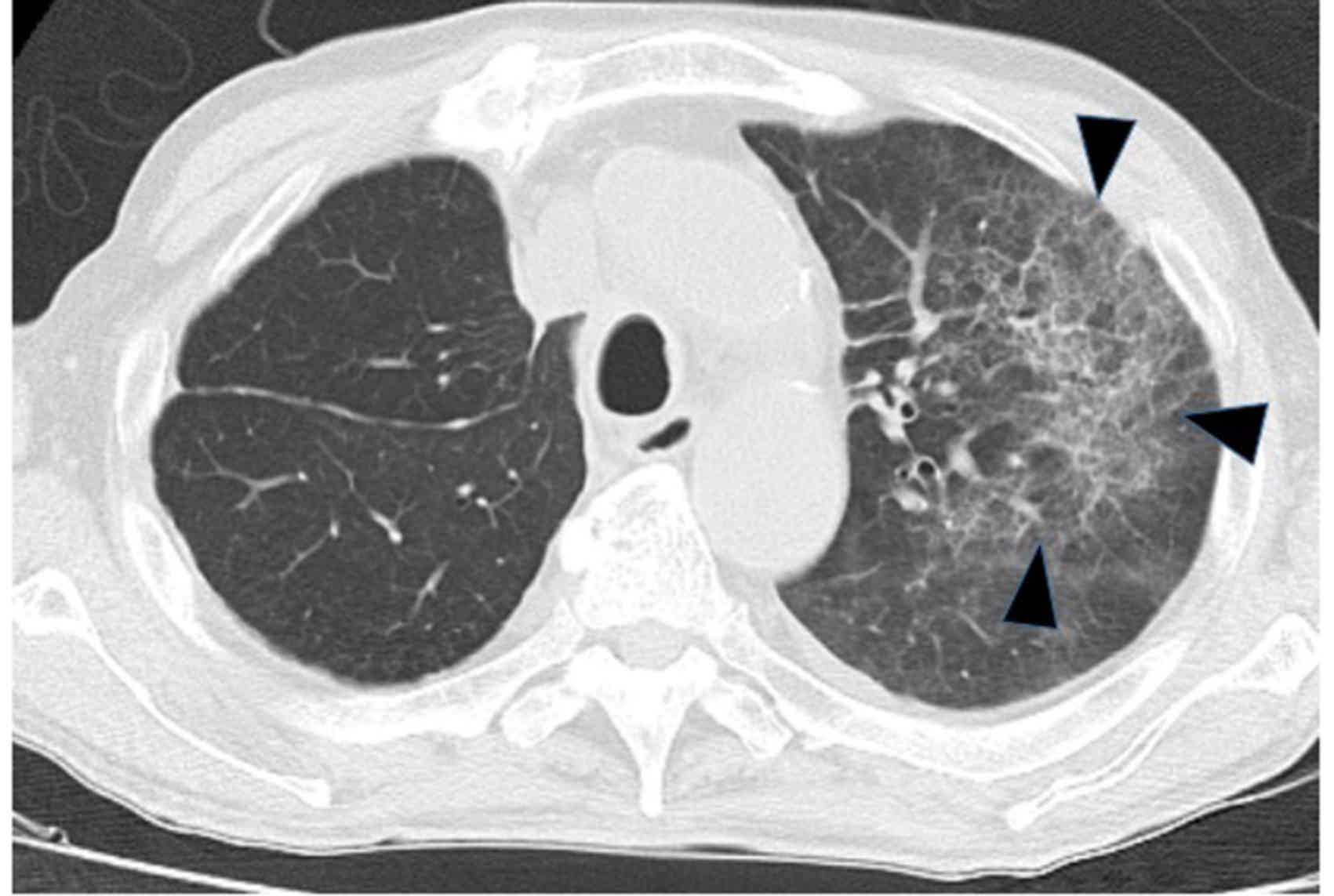
(Fig. 4). Chest X-ray revealed
visible improvement of the interstitial pattern after treatment
(Fig. 2B-D). Furthermore, CT on day
7 revealed clear improvement in the interstitial pattern (Fig. 5).
Regorafenib was orally administered for 21 days
without dose adjustment. Hematological and non-hematological
adverse effects did not occur until his discharge on day 22.
Regorafenib treatment as aforementioned was reinitiated at an
outpatient clinic after a 7-day resting period (Fig. 6). The patient experienced grade 2
hypertension and required the administration of candesartan
cilexetile, which was maintained by dose escalation during the
second course of treatment (▲ in Fig.
6), and administration of regorafenib was withdrawn after they
developed proteinuria (>1 g/dl) with hypoalbuminemia (2.5 mg/dl)
and grade 4 renal function depletion (6) on day 18 of the fourth course of
regorafenib treatment (103 days after initiation of treatment). The
patient was readmitted with general fatigue and hypotension, which
temporarily improved by pericardiocentesis, 6 days after
discontinuation of regorafenib. Chest X-ray and CT did not indicate
relapse of the interstitial pattern in the upper lobe of the left
lung (Fig. 7). However, the patient
died of cardiac tamponade on day 12 of admission, 121 days after
initiation of regorafenib treatment.
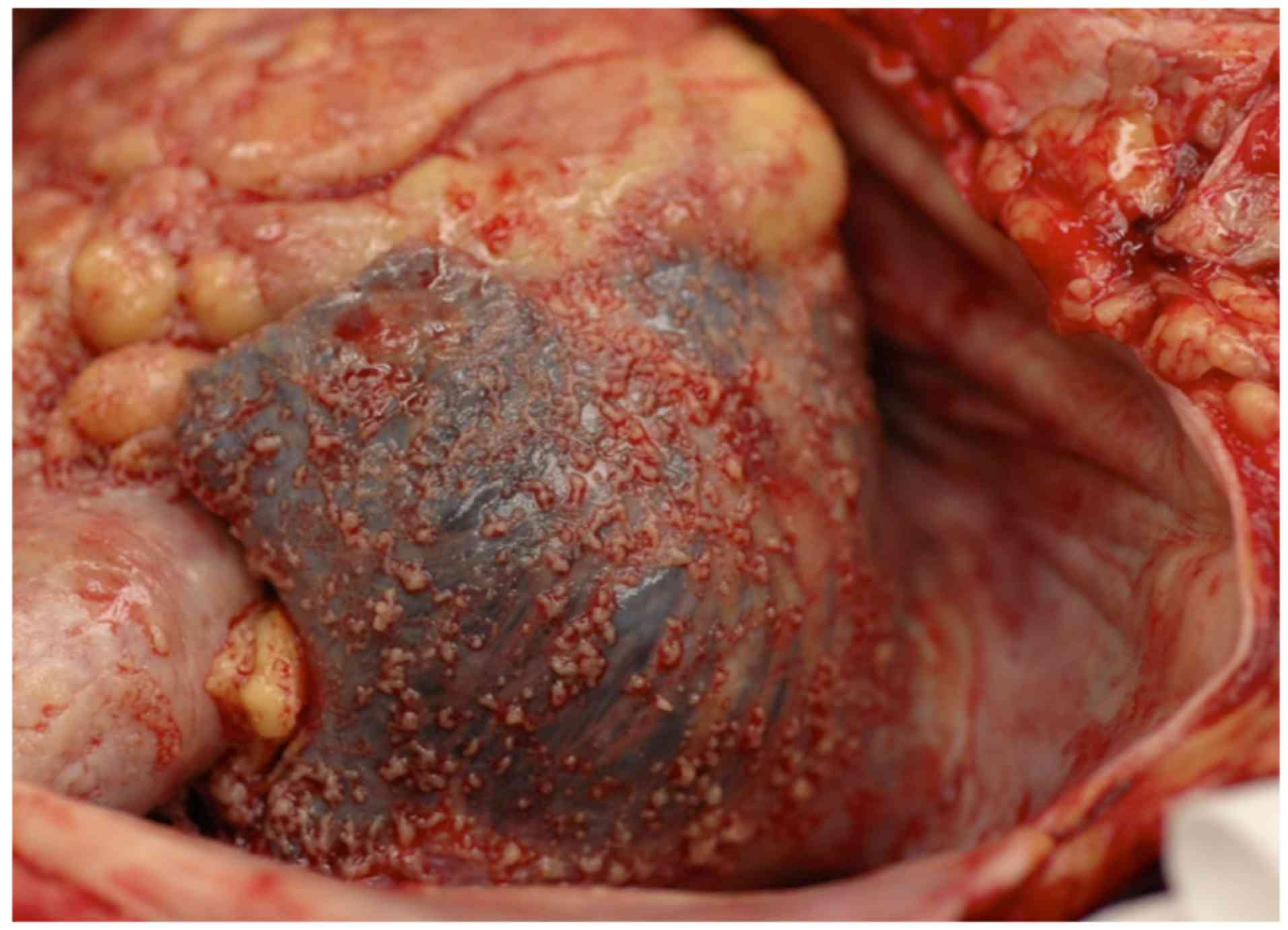
Autopsy revealed cardiac tamponade caused by bloody
pericardial effusion derived from disseminated nodules (1,130 ml;
Fig. 8), which was determined to be
the direct cause of death. In addition, bilateral carcinomatous
pleuritis with direct invasion of the attached lung was observed.
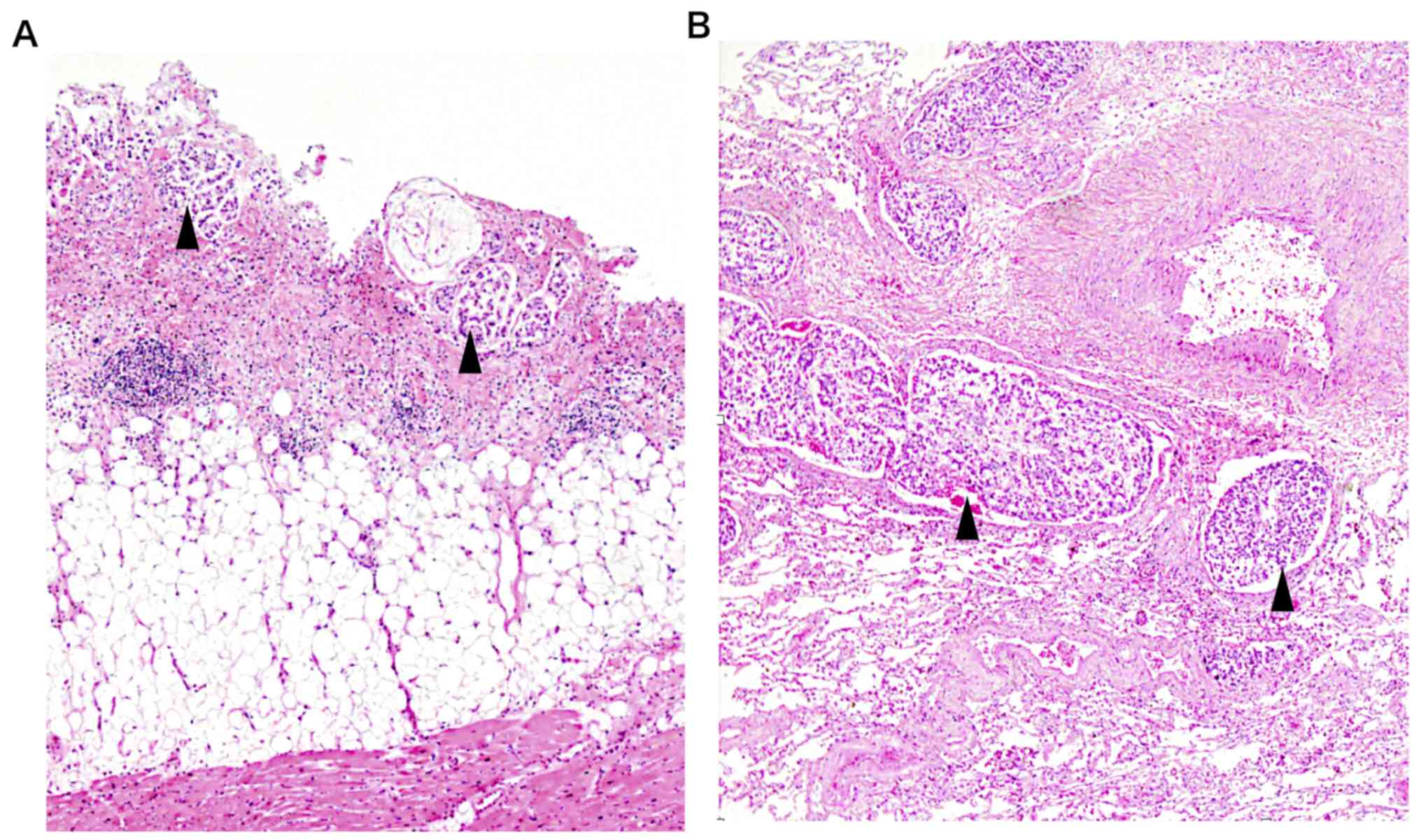
Microscopic examination (magnifications, ×100 or ×200) were
performed on 3 µm-thick sections of paraffin embedded specimen,
fixed in 10% formalin at room temperature for 24 h, and stained
with 0.1% hematoxylin for 4 min and 1% eosin for 2 min. Diffuse
lymphangitic carcinomatosis of the left lung without macroscopic
nodules and moderately differentiated adenocarcinoma were observed
throughout both lungs and the pericardium, with evidence of
lymphatic invasion without tumor necrosis (Fig. 9). The histological findings thus
indicate that chemotherapy has minimal effect.
Discussion
Regorafenib markedly extend the progression-free
survival time (PFS) and overall survival time (OS) in patients with
pretreated metastatic colorectal carcinoma (mCRC) in the
international phase III CORRECT study (NCT 01103323) (1–4). Dose
modification, due to toxicity associated with treatment, was
required in 49% of cases in the CONSIGN Phase IIIb study (7). Additionally, recent data on the real
clinical practice of using regorafenib for treatment have been
collated, which revealed that treatment was initiated at a
25%-decreased dose (120 mg/day) in 59- and 50% -decreased dose (80
mg/day) in 13% of cases, in order to avoid adverse effects due to
toxicity (such as hand-foot syndrome or general fatigue) (8). Bekaii-Saab et al (9) reported that the dose-escalation
strategy starting from half of the regulated starting dose (160 mg
once daily) provides a safe and effective alternative with improved
of quality of life of the patients during treatment in phase II
study.
Previous studies have reported observation of a
radiological response as defined by the response evaluation
criteria in solid tumors criteria (version 1.1) (10) in 1–4.4% of patients (1,2,11). Minimal to no tumor growth (≤9%
increase in the sum of target-lesion diameters) in the 8th week of
treatment was considered a predictive marker of improvement in the
OS as defined by the RadioCORRECT post-hoc radiological analysis
(12); however, this series did not
include cases of partial response or complete response, and the
disease control rate was 53.4% (12). In some studies, decreased density of
liver metastases and cavitating pulmonary metastases, which are
characteristic radiological changes induced by antiangiogenic
agents, are reported as predictive markers of improved prognosis
(13,14). The RadioCORRECT study reported that
these radiological findings do not affect the OS or PFS.
Furthermore, Lim et al (15)
reported that the magnitude of change in the tumor density does not
affect the clinical outcome.
Other agents, such as TAS102, have also proven to
exert long-lasting effects on the OS of patients with mCRC where
salvage treatment has not resulted in improvement of overall
response rate (3,4).
Lymphangitic carcinomatosis is essentially the
infiltration of the lung lymphatics with malignant cancer cells;
symptoms manifest as an increase in lung tissue permeability
(16–18). Previous studies involving
radiological imaging have shown that early reduction of tumor
perfusion and vascularity can be achieved by administration of
regorafenib in a xenograft model (19,20).
Furthermore, lymphatic spread of tumor cells is accelerated by
lymphangiogenesis promoted by VEGF-C and VEGF-D, which bind to the
VEGF receptor-3 on lymphatic endothelial cells (21,22).
This receptor is a target of regorafenib, which acts as a
multitarget tyrosine kinase inhibitor (19).
In the present case, regorafenib induced quick and
prominent reduction in lung permeability resulting in early
improvement of respiratory distress. This could be attributed to
the effect of regorafenib on tissue permeability, as established in
previous xenograft model studies (19,20).
Histological examination of the left lung reveled
viable tumor cells in the dilated lymphatic vessels. In contrast,
clinical imaging did not show lymphangitic carcinomatosis until the
death of the patient owing to pericardial dissemination. No evident
change in the increased levels of carcinoembryonic antigen (above
the normal range) during treatment suggested that regorafenib had
markedly improved lymphangitis and maintained the peritumoral
osmotic pressure, with a moderate effect on lymphatic invasion and
minimal direct effect on cancer cells. These results might be
attributed to the effects of regorafenib on the VEGF receptor-1,
−2, and −3.
In conclusion, the present study reports a case in
which regorafenib markedly reduced peritumoral edema via its
multityrosine kinase inhibitor activity toward VEGF receptors. The
administration of regorafenib rapidly alleviated the symptoms of
lymphangitic carcinomatosis, despite its inadequate potency.
The treatment regimen for regorafenib administration
requires further improvement to increase safety and efficacy
(9,23). In addition, combination treatment of
regorafenib with other cytotoxic agent warrants further
investigation (24); however, this
represents a promising approach for the treatment of osmotic
abnormalities in the peritumoral environment.
Acknowledgements
Not applicable.
Funding
No funding received.
Availability of data and materials
The data used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
NT collected and analyzed clinical data and
literature, and drafted, designed, wrote and revised the
manuscript. KK collected clinical data during treatment, designed
figures and drafted the manuscript. SY collected clinical data of
previous treatment in another hospital and drafted the manuscript.
MF reviewed the pathological findings and revised the manuscript.
All authors have approved the manuscript and agreed with its
submission.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient's sister for publication of this article and the
accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Grothey A, Van Cutsem E, Sobrero A, Siena
S, Falcone A, Ychou M, Humblet Y, Bouché O, Mineur L, Barone C, et
al: Regorafenib monotherapy for previously treated metastatic
colorectal cancer (CORRECT): An international, multicentre,
randomised, placebo-controlled, phase 3 trial. Lancet. 381:303–312.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Li J, Qin S, Xu R, Yau TC, Ma B, Pan H, Xu
J, Bai Y, Chi Y, Wang L, et al: Regorafenib plus best supportive
care versus placebo plus best supportive care in Asian patients
with previously treated metastatic colorectal cancer (CONCUR): A
randomised, double-blind, placebo-controlled, phase 3 trial. Lancet
Oncol. 16:619–629. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Mayer RJ, Van Cutsem E, Falcone A, Yoshino
T, Garcia-Carbonero R, Mizunuma N, Yamazaki K, Shimada Y, Tabernero
J, Komatsu Y, et al: Randomized trial of TAS-102 for refractory
metastatic colorectal cancer. N Engl J Med. 372:1909–1919. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Xu J, Kim TW, Shen L, Sriuranpong V, Pan
H, Xu R, Guo W, Han SW, Liu T, Park YS, et al: Results of a
randomized, double-blind, placebo-controlled, Phase III trial of
trifluridine/tipiracil (TAS-102) monotherapy in Asian patients with
previously treated metastatic colorectal cancer: The TERRA study. J
Clin Oncol. 36:350–358. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
National Collaborating Centre for Chronic
Conditions, . Chronic obstructive pulmonary disease: National
clinical guideline for management of chronic obstructive pulmonary
disease in adults in primary and secondary care. Thorax. 59 (Suppl
1):S1–S232. 2004.
|
|
6
|
Andrassy KM: Comments on KDIGO 2012
clinical practice guideline for the evaluation and management of
chronic kidney disease. Kidney Int. 84:622–623. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Van Cutsem E, Martinelli E, Cascinu S,
Sobrero A, Banzi M, Seitz JF, Barone C, Ychou M, Peeters M, Brenner
B, et al: Regorafenib for patients with metastatic colorectal
cancer who progressed after standard therapy: Results of the large,
single-arm, open-label phase IIIb CONSIGN study. Oncologist.
24:185–192. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ramaswamy A, Ostwal V, Pande N, Sharma A,
Patil S, Thippeswamy R, Ghadyalpatil N, Roy R, Peshwe H, Poladia B,
et al: Practice patterns and outcomes with the use of regorafenib
in metastatic colorectal cancer: Results from the Regorafenib in
metastatic colorectal cancer-an Indian Exploratory analysis study.
South Asian J Cancer. 8:22–26. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bekaii-Saab TS, Ou FS, Ahn DH, Boland PM,
Ciombor KK, Heying EN, Dockter TJ, Jacobs NL, Pasche BC, Cleary JM,
et al: Regorafenib dose-optimisation in patients with refractory
metastatic colorectal cancer (ReDOS): A randomised, multicentre,
open-label, phase 2 study. Lancet Oncol. 20:1070–1082. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New reponse evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Euro J Cancer. 45:228–247.
2009. View Article : Google Scholar
|
|
11
|
Yoshino T, Komatsu Y, Yamada Y, Yamazaki
K, Tsuji A, Ura T, Grothey A, Van Cutsem E, Wagner A, Cihon F, et
al: Randomized phase III trial of regorafenib in metastatic
colorectal cancer: Analysis of the CORRECT Japanese and
non-Japanese subpopulations. Invest New Drugs. 33:740–750. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ricotta R, Verrioli A, Ghezzi S, Porcu L,
Grothey A, Falcone A, Van Cutsem E, Argilés G, Adenis A, Ychou M,
et al: Radiological imaging markers predicting clinical outcome in
patients with metastatic colorectal carcinoma treated with
regorafenib: Post hoc analysis of the CORRECT phase III trial
(RadioCORRECT study). ESMO Open. 1:e0001112017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Nishino M, Cryer SK, Okajima Y, Sholl LM,
Hatabu H, Rabin MS, Jackman DM and Johnson BE: Tumoral cavitation
in patients with non-small-cell lung cancer treated with
antiangiogenic therapy using bevacizumab. Cancer Imaging.
12:225–235. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Boonsirikamchai P, Asran MA, Maru DM,
Vauthey JN, Kaur H, Kopetz S and Loyer EM: CT findings of response
and recurrence, independent of change in tumor size, in colorectal
liver metastasis treated with bevacizumab. AJR Am J Roentgenol.
197:W1060–W1066. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lim Y, Han SW, Yoon JH, Lee JM, Lee JM,
Paeng JC, Won JK, Kang GH, Jeong SY, Park KJ, et al: Clinical
implication of anti-angiogenic effect of regorafenib in metastatic
colorectal cancer. PLoS One. 10:e01450042015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Chandler GN and Telling M: Lymphangitis
carcinomatosa. Br Med J. 2:639–641. 1952. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Thomas A and Lenox R: Pulmonary
lymphangitic carcinomatosis as a primary manifestation of colon
cancer in a young adult. CMAJ. 179:338–340. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Bruce DM, Heys SD and Eremin O:
Lymphangitis carcinomatosa: A literature review. J R Coll Surg
Edinb. 41:7–13. 1996.PubMed/NCBI
|
|
19
|
Cyran CC, Kazmierczak PM, Hirner H, Moser
M, Ingrisch M, Havla L, Michels A, Eschbach R, Schwarz B, Reiser
MF, et al: Regorafenib effects on human colon carcinoma xenografts
monitored by dynamic contrast-enhanced computed tomography with
immunohistochemical validation. PLoS One. 8:e760092013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Wilhelm SM, Dumas J, Adnane L, Lynch M,
Carter CA, Schütz G, Thierauch KH and Zopf D: Regorafenib (BAY
73-4506): A new oral multikinase inhibitor of angiogenic, stromal
and oncogenic receptor tyrosine kinases with potent preclinical
antitumor activity. Int J Cancer. 129:245–255. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
He Y, Rajantie I, Pajusola K, Jeltsch M,
Holopainen T, Yla-Herttuala S, Harding T, Jooss K, Takahashi T and
Alitalo K: Vascular endothelial cell growth factor receptor
3-mediated activation of lymphatic endothelium is crucial for tumor
cell entry and spread via lymphatic vessels. Cancer Res.
65:4739–4746. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Shimizu K, Kubo H, Yamaguchi K, Kawashima
K, Ueda Y, Matsuo K, Awane M, Shimahara Y, Takabayashi A, Yamaoka Y
and Satoh S: Suppression of VEGFR-3 signaling inhibits lymph node
metastasis in gastric cancer. Cancer Sci. 95:328–333. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Bekaii-Saab T, Kim R, Kim TW, O'Connor JM,
Strickler JH, Malka D, Sartore-Bianchi A, Bi F, Yamaguchi K,
Yoshino T and Prager GW: Third- or later-line therapy for
metastatic colorectal cancer: Reviewing best practice. Clin
Colorectal Cancer. 18:e117–e129. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Schultheis B, Folprecht G, Kuhlmann J,
Ehrenberg R, Hacker UT, Köhne CH, Kornacker M, Boix O, Lettieri J,
Krauss J, et al: Regorafenib in combination with FOLFOX or FOLFIRI
as first- or second-line treatment of colorectal cancer: Results of
a multicenter, phase Ib study. Ann Oncol. 24:1560–1567. 2013.
View Article : Google Scholar : PubMed/NCBI
|