Introduction
Acute myeloid leukemia (AML), a highly heterogeneous
disease, is characterized by uncontrolled proliferative blasts
(1). At present, the treatment of
AML is challenging due to patient characteristics and intrinsic
biological factors (2). FMS-like
tyrosine kinase 3 (FLT3) gene mutations are present in ~30%
of patients with de novo AML; internal tandem duplication
(ITD) mutations in the juxtamembrane domain of FLT3
account for two-thirds of FLT3 mutations (3). Patients with an FLT3-ITD
mutation have a poor prognosis, with a shorter remission duration
and higher relapse rates compared with patients with
FLT3-unmutated AML (3). The
FLT3-ITD mutation usually coexists with other gene mutations
or fusion genes; it has been reported that the prognosis of
patients with FLT3-ITD and nucleophosmin (NPM1)
double mutations was better compared with that in those with a
FLT-ITD mono-mutation (4).
Previously, research has indicated that the occurrence of
FLT3-tyrosine kinase domain (TKD) and NPM1
double mutations were a highly favorable prognostic factor
(5). However, the prognostic
function of FLT3-ITD combined with other gene mutations or
fusion genes is not clear.
Small molecule inhibitors that target FLT3,
including sorafenib and midostaurin, have been revealed to be
effective in the treatment of patients with FLT3-ITD-mutated
AML; the multitargeted kinase inhibitor midostaurin combined with
standard chemotherapy prolonged the overall survival (OS) and
event-free survival times in patients with FLT3-mutated AML
who were in remission after consolidation therapy and entered a
maintenance phase compared with patients who received placebo plus
chemotherapy (2). In addition, a
novel irreversible FLT3 inhibitor, FF-10101, also
demonstrated excellent efficacy against FLT3-mutated AML
cells (6). However, the long-term
efficacy of these novel FLT3 inhibitors, and whether they
may be used as substitutes for hematopoietic stem cell
transplantation (HSCT) for patients with FLT3-ITD mutations
is currently unclear.
In the present study, a retrospective analysis was
performed to examine the complete remission (CR), relapse and
survival of newly diagnosed patients with FLT3-ITD-mutated
AML with or without other gene mutations or fusion genes, and the
effect of sorafenib was evaluated in patients with FLT3-ITD
mutated AML.
Patients and methods
Patient population
Adult patients with AML (n=103; age range 18–87
years; mean age, 50 years; 62 men and 41 women) diagnosed between
January 2013 and June 2018 at Huai'an No. 1 People's Hospital,
Nanjing Medical University (Nanjing, China), including 23 patients
harboring an FLT3-ITD mutation, who were treated with
different treatment regimens, were retrospectively included in the
present study. A total of 45 patients were revealed to be alive at
the time of data collection. Patients with acute promyelocytic
leukemia were excluded. The study was ethically approved by the
Institutional Review Committee of Huai'an No. 1 People's Hospital,
and written informed consent was obtained from all patients. The
diagnosis of AML was established according to the criteria of the
WHO classification (7), including
clinical presentations and morphological, immunophenotype and
recurrent cytogenetic abnormalities. All patients were analyzed
based on their response to induction therapy, CR, relapse, OS and
recurrence-free survival (RFS) rates.
Detection of FLT3-ITD and other
associated genes
Multiple markers for the diagnosis of AML were
identified, along with gene mutations, including AML1-ETO,
CBFB/MYH11, MLL/AF6, MLL/AF9, MLL/ENL, dupMLL, DEK/CAN, EVI1,
HOX11, BCR/ABL, FLT3-ITD, NPM1, CEBPA, C-kit and DNMT3A.
Fusion genes were detected using multiple nested RT-PCR. Total RNA
was extracted using Omega whole-blood RNA extraction kit (cat. no.
R6616-02; Omega Bio-Tek, Inc., Norcross, GA, USA). Nested RT-PCR
detection method and reaction system were used as previously
reported (8,9). AML-associated mutated genes were
detected using high-throughput sequencing technology. Total DNA was
extracted using whole blood DNA extraction kit (cat. no. D3392-02;
Omega Bio-Tek, Inc.), and genetic mutations were detected by
Kindstar Global Medical Laboratory Center (http://www.kindstar.com.cn/kindstar/cn/platform.html)
using Sanger sequencing, as previously described (9,10). Bone
marrow samples were used for this, and each patient signed a bone
marrow puncture written informed consent form.
Treatment regimens
All 103 patients received a ‘3+7’ chemotherapy
regimen (60 mg/m2/day daunorubicin or 10
mg/m2/day idarubicin for 3 days, and 100
mg/m2/day cytarabine for 7 days with a 24-h intravenous
pump maintenance). Out of the 23 patients harboring FLT3-ITD
mutations, 7 were treated with sorafenib combined with a ‘3+7’
chemotherapy regimen for induction therapy. If the interim bone
marrow (BM) examination, which was performed between days 14 and 21
of induction therapy, revealed residual leukemic blasts, a second
course of induction chemotherapy comprising cytarabine (100
mg/m2/day) plus 2 mg/m2/day homoharringtonine
was administered for 5 days. Patients who achieved CR usually
received four to six courses of consolidation chemotherapy or
allo-HSCT. Consolidation chemotherapy regimens included high-dose
cytarabine (3 g/m2 twice a day on days 1 to 3) or
intermediate-dose cytarabine (1 g/m2 for 4 days) plus
daunorubicin (45 mg/m2/day for 3 days) or mitoxantrone
(4 mg/m2/day for 3 days). The patients who achieved CR
whose induction regimen contained sorafenib with chemotherapy
received a continuous maintenance of sorafenib during the
chemotherapy interval. Allo-HSCT was performed in patients who
achieved CR at the discretion of the attending physician, usually
following two courses of consolidation chemotherapy; however,
decisions were often made on the basis of the patients'
willingness, disease status, risk classification, human leukocyte
antigen (HLA) matching and financial status.
Evaluation
CR was defined according to the standard criteria of
<5% blasts in BM. Hematologic recovery was measured in terms of
the absolute neutrophil (>1×109/l) and platelet
(>100×109/l) counts in the peripheral blood. Clinical
recurrence following CR was defined as the presence of ≥5% blasts
in BM or re-appearance of leukemic blasts in the peripheral blood,
or the presence of extramedullary disease. OS and RFS were
calculated from the date of diagnosis. An event was defined as
induction therapy failure, relapse following CR or mortality from
any cause. Relapse was evaluated in patients who achieved CR using
a cumulative incidence function with respect to competing
risks.
Statistical analysis
Statistical analysis was performed using SPSS 24.0
(IBM Corp., Armonk, NY, USA) and data were presented as the means ±
standard deviation/standard error of the mean. Pearson
χ2 survival distributions were estimated using the
Kaplan-Meier method and the differences were compared using the
log-rank (Mantel-Cox) test. Categorical variables were compared
using Pearson χ2 or Fisher Exact test. P<0.05 was
considered to indicate a statistically significant difference.
Results
Patient characteristics
A total of 103 patients with AML were investigated
during this period, 23 (22.3%) of which had an FLT3-ITD
mutation. The median age of the entire cohort was 50 years old (age
range, 18–87 years); 31 (30.1%) patients were aged ≥60 years.
Patient characteristics and FLT3-ITD mutation statuses are
summarized in Table I. Eleven out of
23 (47.83%) patients had both NPM1 and FLT3-ITD
mutation. High leukocyte counts usually occurred in patients with
FLT3-ITD mutations. In addition to NPM1, other gene
mutations combined with the FLT3-ITD mutation were observed
as follows: CEBPA (2/23, 8.69%), AML1-ETO (1/23,
4.35%), EVI1 (1/23, 4.35%), HOX11 (5/23, 21.74%) and
dupMLL (2/23, 8.96%) mutations.
 | Table I.Patient characteristics. |
Table I.
Patient characteristics.
|
Characteristics | Total (n=103) | FLT3-ITH(+)
(n=23) | FLT3-ITH(−)
(n=80) | P-value |
|---|
| Age (years), median
(range) | 50 (18–87) | 51 (18–87) | 49.5 (18–76) | 0.138 |
| <60 years, no.
(%) | 82 (79.61) | 15 (65.22) | 57 (71.25) |
|
| ≥60 years, no.
(%) | 31 (20.39) | 8 (34.78) | 23 (28.75) | 0.578 |
| Male, no. (%) | 62 (60.19) | 12 (52.17) | 50 (62.50) |
|
| Female, no.
(%) | 41 (39.81) | 11 (47.83) | 30 (37.50) | 0.372 |
| WBC
(×109/l), median (range) | 15.29
(0.63–257.0) | 40.44
(1.55–257.0) | 9.71
(0.63–211.0) |
<0.001a |
| HB (g/l), median
(range) | 74 (40–134) | 65 (46–127) | 79.5 (40–134) | 0.842 |
| PLT
(×109/l), median (range) | 44.0 (1–461) | 48 (4–219) | 41.5 (1–461) | 0.290 |
| Cytogenetics, no.
(%) |
|
|
|
|
| Abnormal
karyotype | 44 (42.72) | 5 (21.74) | 39 (48.75) |
|
| Normal
karyotype | 59 (57.28) | 18 (78.26) | 41 (51.25) | 0.021a |
| Other abnormal
genes no. (%) |
|
|
|
|
| NPM1 | 18 (17.48) | 11 (47.83) | 7 (13.75) | 0.0001a |
| CEBPA | 18 (17.48) | 2 (8.69) | 16 (20.00) | 0.208 |
|
AML1/ETO | 17 (16.50) | 1 (4.35) | 16 (20.00) | 0.074 |
| EVI1 | 9 (8.74) | 1 (4.35) | 8 (10.00) | 0.397 |
| HOX11 | 9 (8.74) | 5 (21.74) | 4 (5.00) | 0.012a |
|
C-kit/D816V | 7 (6.79) | 0 (0) | 7 (8.75) | 0.141 |
| Dup MLL | 3 (2.91) | 2 (8.96) | 1 (1.25) | 0.061 |
|
CBFB/MYH11 | 2 (1.94) | 0 (0) | 2 (2.50) | 0.281 |
|
BCR/ABL | 2 (1.94) | 0 (0) | 2 (2.50) | 0.443 |
|
DEK/CAN | 2 (1.94) | 0 (0) | 2 (2.50) | 0.443 |
|
MLL/AF6 | 2 (1.94) | 0 (0) | 1 (1.25) | 0.590 |
|
MLL/AF9 | 2 (1.94) | 0 (0) | 2 (2.50) | 0.443 |
|
MLL/AF10 | 1 (0.97) | 0 (0) | 1 (1.25) | 0.590 |
|
MLL/ELL | 2 (1.94) | 0 (0) | 2 (2.50) | 0.443 |
|
NuP98/HOxC11 | 1 (0.97) | 0 (0) | 1 (1.25) | 0.338 |
Treatment response
All 103 patients received a standard ‘3+7’ regimen
of induction chemotherapy. There were no significant differences in
the CR rate between the FLT3-ITD-positive and
FLT3-ITD-negative groups (65.22 vs. 62.5%; P=0.812; Table II). The overall response rate (ORR)
was 78.26% for the FLT3-ITD-positive group and 86.25% for
the FLT3-ITD-negative group (P=0.351). The relapse rate was
significantly higher in the FLT3-ITD-positive group compared
with the FLT3-ITD-negative group (34.78 vs. 15.0%;
P=0.034). One patient harboring an FLT3-ITD mutation
received allo-HSCT, and still had CR status 6 months later. In the
FLT3-ITD-negative group, 10 patients received autologous
stem cell transplantation, 3 received allo-HSCT and 4 received
micro-transplantation (11). Out of
the 23 patients harboring FLT3-ITD mutations, 7 were treated
with sorafenib combined with chemotherapy for induction therapy and
16 with mono-chemotherapy. The ORR was significantly higher in the
sorafenib plus chemotherapy group compared with in the
mono-chemotherapy group (P=0.039; Table III), but no significant differences
in the CR and relapse rates were observed between these two
groups.
| Table II.Treatment response between the
FLT3-ITD positive group and FLT3-ITD negative group. |
Table II.
Treatment response between the
FLT3-ITD positive group and FLT3-ITD negative group.
| Treatment | Total (n=103) | FLT3-ITH(+)
(n=23) | FLT3-ITH(−)
(n=80) | P-value |
|---|
| Therapy
regimens |
|
|
|
|
|
Mono-chemotherapy, no.
(%) | 96 (93.2) | 16 (69.57) | 80 (100.0) |
|
|
Sorafenib + chemotherapy, no.
(%) | 7 (6.8) | 7 (30.43) | 0 (0) |
|
| Treatment
response |
|
|
|
|
| NR, no.
(%) | 16 (15.53) | 5 (21.74) | 11 (13.75) | 0.351 |
| PR, no.
(%) | 22 (21.34) | 3 (13.04) | 19 (23.75) | 0.269 |
| CR, no.
(%) | 65 (63.12) | 15 (65.22) | 50 (62.5) | 0.812 |
| ORR,
no. (%) | 87 (84.46) | 18 (78.26) | 69 (86.25) | 0.351 |
|
Relapse, no. (%) | 20 (19.42) | 8 (34.78) | 12 (15.00) | 0.034a |
| Post-remission
treatment |
|
|
|
|
|
Autologous transplantation
(%) | 10 (9.71) | 0 (0) | 10 (12.5) |
|
|
Allogeneic transplantation
(%) | 4 (3.88) | 1 (4.35) | 3 (3.75) |
|
| Micro
transplantation (%) | 4 (3.88) | 0 (0) | 4 (5.00) |
|
| Table III.Treatment of patients with FMS-like
tyrosine kinase 3-internal tandem duplication mutation
mutations. |
Table III.
Treatment of patients with FMS-like
tyrosine kinase 3-internal tandem duplication mutation
mutations.
| Treatment response
(%) | Total (n=23) | Mono-chemotherapy
(n=16) | Sorafenib plus
chemotherapy (n=7) | P-value |
|---|
| NR, no. | 5 (21.74) | 5 (31.25) | 0 (0) | 0.039a |
| PR, no. | 3 (13.04) | 2 (12.50) | 1 (14.28) | 0.906 |
| CR, no. | 15 (65.22) | 9 (56.25) | 6 (85.71) | 0.172 |
| OR, no. | 18 (78.26) | 11 (68.75) | 7 (100.00) | 0.039a |
| Relapse, no. | 8 (34.78) | 4 (25.00) | 4 (57.14) | 0.136 |
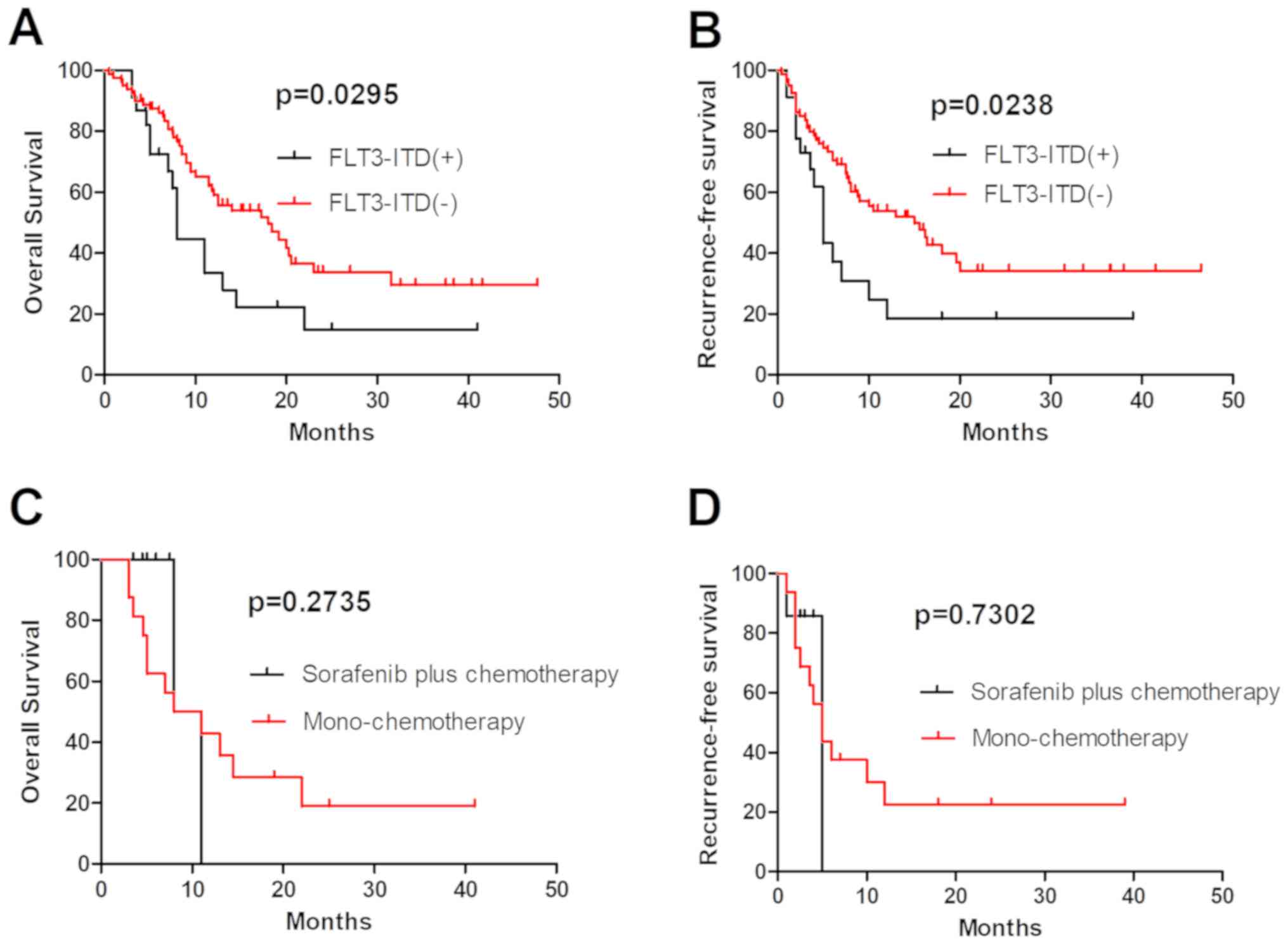
Sorafenib plus chemotherapy did not
improve the OS and RFS of patients with FLT3-ITD-mutations who did
not receive allo-HSCT
Patients with FLT3-ITD-mutated AML were
associated with a poor prognosis due to a high relapse rate
(12). In the present study, 103
patients with AML who completed at least one cycle of induction
therapy were analyzed, and the OS and RFS rates in 23 patients
harboring an FLT3-ITD mutation were revealed to be
significantly lower compared with those in patients with
FLT3-ITD-unmutated AML (P=0.0295 and P=0.0238, respectively;
Fig. 1A and B). A number of
FLT3 inhibitors have been revealed to specifically inhibit
the proliferation of leukemia cells in preclinical models. However,
first-generation FLT3 inhibitors in patients with
relapsed/refractory FLT3-mutated AML revealed transient
reductions in the number of blasts in the blood and bone marrow,
but rarely CR (13,14). In the present study, 7 patients with
an FLT3-ITD mutation received sorafenib plus chemotherapy,
and their ORR was revealed to be higher compared with those of
patients with FLT3-ITD-unmutated AML, but no significant
differences in the OS and RFS were observed between the
mono-chemotherapy and sorafenib plus chemotherapy groups (P=0.2735
and P=0.7302, respectively; Fig. 1C and
D). These results indicate that sorafenib was not able to
improve the long-term follow-up results of patients harboring an
FLT3-ITD mutation, and should receive allo-HSCT as soon as
possible.
Outcome of patients harboring an
FLT3-ITD mutation combined with other gene mutations or fusion
genes
The prognosis and outcome in patients harboring an
FLT3-ITD mutation combined with other mutations or fusion
genes are unclear. In the present study, two groups of patients
harboring an FLT3-ITD mutation combined with favorable-risk
genes (FRGs; defined as the presence alone of the AML1-ETO,
CBFB/MYH11 fusion gene or NPM1 mutation, and
CEBPA double mutation) or adverse-risk genes (DRGs; defined
as multiple gene mutations, specific genes associated with a poor
prognosis for AML, and complex chromosomal karyotype abnormalities,
for example FLT3-ITD, C-kit and DNMT3A mutations)
were analyzed. A total of 75 patients with genetic abnormalities
received standard regimens of chemotherapy. The survival of all
patients with an FLT3-ITD mutation combined with FRGs were
compared with those of patients with an FLT3-ITD mutation
combined with DRGs; no significant differences in OS and RFS were
observed between these two groups (P=0.3422 and P=0.6599; Fig. 2E and F). Among the 75 patients who
received standard treatment, 35 had a single FRG, 7 had a single
FLT3-ITD mutation, 11 had an FLT3-ITD mutation and
FRGs, 17 had a single DRG, and 5 had a combination of
FLT3-ITD mutation and DRGs (Table IV). Compared with patients with a
single FLT3-ITD mutation, the OS and RFS were significantly
longer in patients with an FLT3-ITD mutation together with
FRGs (P=0.0361 and P=0.0426, respectively; Fig. 2A and B). No significant differences
in OS and RFS were observed between patients with a single
FLT3-ITD mutation and those with DRGs (P=0.8549 and
P=0.7879, respectively; Fig. 2C and
D).
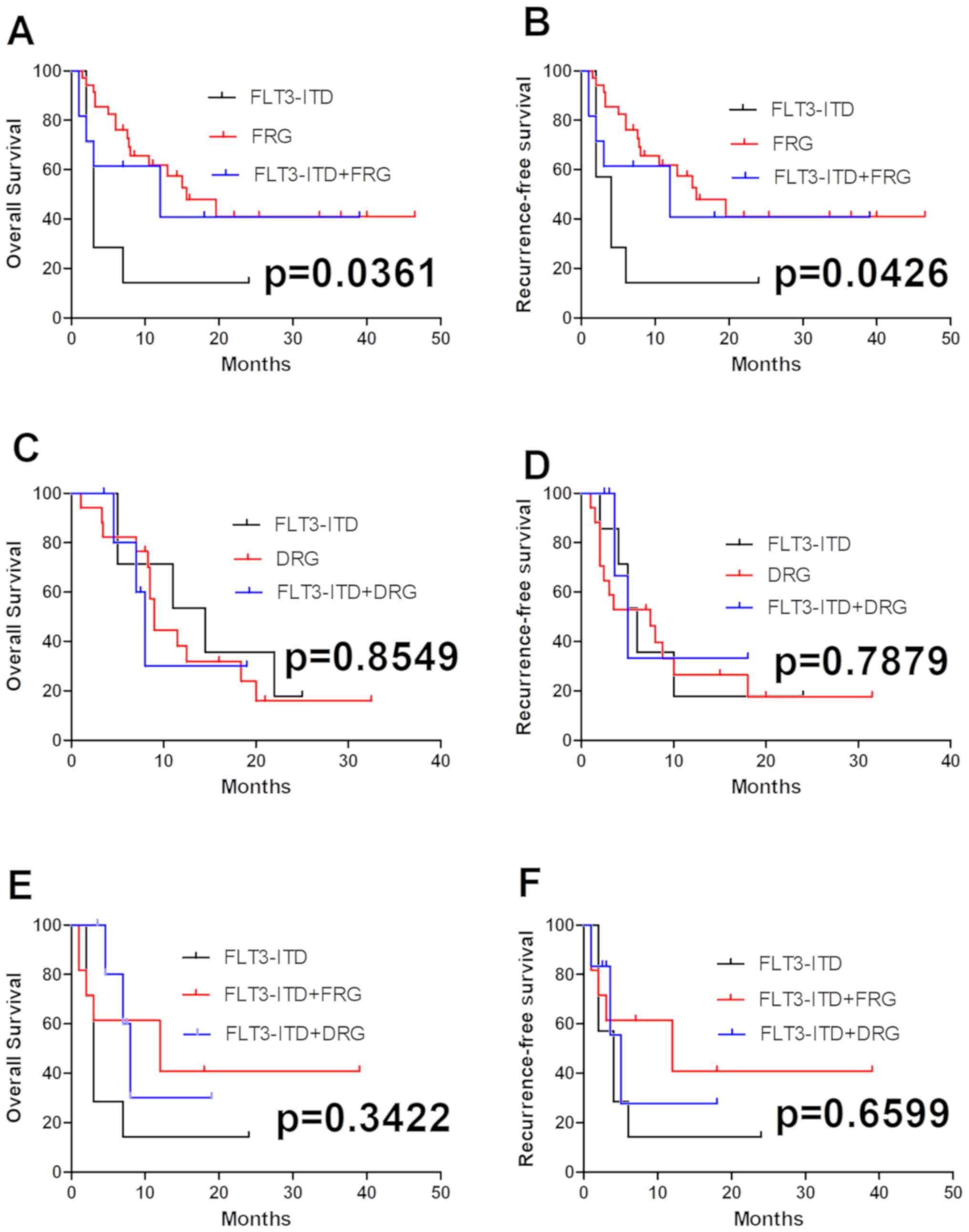 | Figure 2.Comparison of OS and RFS between FRGs
and DRGs in patients with FLT3-ITD-mutated AML. OS in (A)
FRGs alone, (C) DRGs alone or (E) compared with each other, with an
FLT3-ITD mutation. OS was significantly longer in patients
with an FLT3-ITD mutation combined with FRGs (P=0.0361).
There were no significant differences in OS between the patients
with a single FLT3-ITD mutation and the patients with DRGs
(P=0.8549). RFS in (B) FRGs or (D) DRGs combined with an
FLT3-ITD mutation, or (F) the two compared with each other.
RFS were significantly longer in patients with an FLT3-ITD
mutation combined with FRGs (P=0.0426), but no significant
differences in RFS were observed between the patients with a single
FLT3-ITD mutation and those with DRGs (P=0.7879). OS,
overall survival; RFS, recurrence free survival; FRGs,
favorable-risk genes; DRGs, adverse-risk genes; AML, acute myeloid
leukemia; FLT3-ITD, FMS-like tyrosine kinase 3-internal
tandem duplication mutation. |
| Table IV.FLT3-ITD mutation together with other
genetic abnormalities in 75 patients with acute myeloid
leukemia. |
Table IV.
FLT3-ITD mutation together with other
genetic abnormalities in 75 patients with acute myeloid
leukemia.
| FLT3-ITH
status | Total (n=75)
(%) | Favourable-risk
genes (n=46) (%) | Adverse-risk genes
(n=22) (%) | Neither (n=7) | P-value |
|---|
| FLT3-ITD
(+) | 23 (30.67) | 11 (23.91) | 5 (22.73) | 7 (100.0%) |
|
| FLT3-ITD
(-a) | 52 (69.33) | 35 (76.09) | 17 (77.27) | 0 | 0.914 |
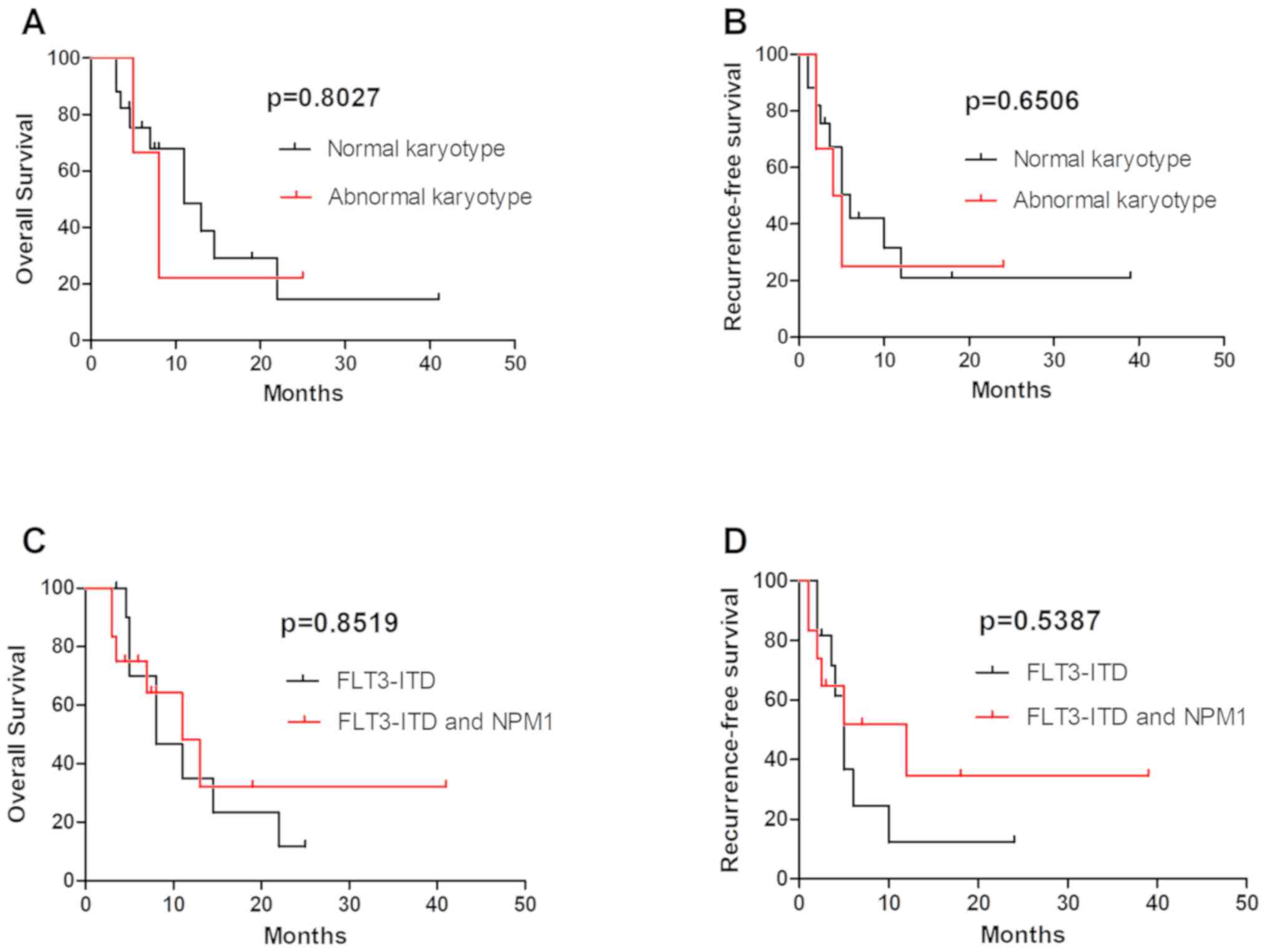
FLT3-ITD mutations in normal karyotype
(NK) and abnormal karyotype (AK)
The FLT3-ITD mutation was common in patients
with NK. A number of patients with AK also had FLT3-ITD
mutations. Out of the 23 patients with an FLT3-ITD mutation
were analyzed, 6 were AK and 17 NK; no significant differences in
OS and RFS were observed between these two groups (Fig. 3A and B). Further analysis revealed
that the 3-year OS and RFS were longer in patients with
FLT3-ITD combined with NPM1 mutations compared with
in patients with a single FLT3-ITD mutation, but there were
no statistically significant differences (Fig. 3C and D). This result may be
associated with the relatively small number of cases; further large
sample studies are therefore required to confirm it.
Discussion
AML is a heterogeneous disorder of hematopoietic
progenitor cells, characterized by blocked differentiation and
uncontrolled proliferation (15).
Sequencing of AML genomes has revealed that AML is genetically
diverse and clonally heterogeneous with multiple mutations, with a
majority of patients having >2 gene mutations and being clonally
represented (16,17). The most frequently mutated genes in
AML are NPM1 (25–35%), CEBPA (6–10%), RUNX1
(5–15%), FLT3-ITD (~20%), DNMT3A (18–22%),
ASXL1 (5–17%), KIT (<5%) and TET2 (7–25%)
(1). AML1-ETO, mutated
NPM1 without FLT3-ITD, biallelic mutated CEBPA
and CBFB-MYH11 were associated with a favorable prognosis
(1), and EVI1, MLL-AF6,
DEK-CAN and FLT3-ITD with adverse prognosis.
FLT3-ITD is a distinct clinical entity associated with a
poor prognosis (11,18,19). In
accordance with the results of the present study, AML with
FLT3-ITD tends to affect older patients with higher
peripheral white blood cell counts, NK (20), shorter remission duration and higher
relapse rates compared with patients with FLT3-unmutated
AML.
The FLT3-ITD mutation has been revealed to
usually coexist with other molecular genetics and cytogenetic
alterations; however, the prognostic function of FLT3-ITD
combined with other gene mutations or fusion genes is not clear. In
the present retrospective study, 103 patients with AML were
analyzed, and it was revealed that the OS and RFS rates in 23
patients harboring FLT3-ITD mutations were lower compared
with those in patients without FLT3-ITD mutations, but no
significant differences in the CR and OR rates were observed
between these two groups. NPM1 and FLT3-ITD are two
of the most common genetic abnormalities in AML. Patients with
NPM1 mutations have a favorable prognosis, older patients
with NPM1-positive and FLT3-ITD-negative genotype
have a relatively favorable prognosis, and patients with an
FLT3-ITD mutation have a poor prognosis (21). The prognostic effect of the
NPM1 mutation in de novo AML may also be influenced
by the relative abundance of the mutated allele (22). FLT3-ITD mutation rates were
twice as frequent in NPM1 mutant AML, when compared with AML
with wild-type NPM1 (22).
The FLT3-ITD co-mutation has been revealed to diminish the
favorable effect of the NPM1 mutation (23). Consistent with previous studies, the
prognosis of patients with the FLT3-ITD and NPM1
co-mutation in the present study was improved following high
intensity chemotherapy, when compared with the patients with a
single FLT3-ITD mutation. However, no statistically
significant differences were observed between these two groups,
which may be due to the small patient number. FLT3-ITD also
co-existed with other genetic abnormalities, including FRGs
including CEBPA and AML1-ETO, and DRGs including
N-RAS, NMT3A, EVI1, DupMLL and HOX11 (24,25). In
the present study, 76 patients with AML with genetic abnormalities
were analyzed and the survival of patients with an FLT3-ITD
mutation combined with good prognosis genes were compared with
those with an FLT3-ITD mutation combined with poor prognosis
genes. The results revealed no significant differences in OS and
RFS between these two groups, which may be due to the small sample
size. Among the 76 patients who received standard treatment, the OS
and RFS of patients with an FLT3-ITD mutation combined with
FRGs were longer compared with those of patients with a single
FLT3-ITD mutation. No significant differences in OS and RFS
were observed between the patients with a single FLT3-ITD
mutation and those with DRGs.
NK AML accounts for 50% of all AML and represents
the third and largest broad cytogenetic category in AML (26). FLT3-ITD has been recognized as
a marker of poor prognosis in patients with NK AML, but
FLT3-ITD mutations are also commonly observed in patients
with AK AML (27,28), and the prognostic function of the
FLT3-ITD mutation in these patients was unclear. A total of
23 FLT3-ITD mutated patients receiving treatment were
analyzed; 6 patients were AK and 17 NK, and no significant
differences in the OS and RFS were observed between these two
groups.
At present, tyrosine kinase inhibitors have been
demonstrated to be effective in the treatment of FLT3-mutant
AML. The multitargeted kinase inhibitor midostaurin, in combination
with chemotherapy, has emerged as a novel standard treatment of
patients with FLT3-ITD and TKD-positive AML. It was
approved by the FDA for the treatment of AML in 2017 (2,29). In
order to further improve the prognosis of patients with
FLT3-mutated AML, selective and potent second-generation
FLT3 inhibitors (including gilteritinib, crenolanib,
FF-10101 and quizartinib) are being investigated in clinical
trials. FF-10101 and quizartinib have each exhibited an excellent
efficacy against AML cells and in patients with FLT3
mutations (6,29–32).
High-dose daunorubicin or cladribine chemotherapy have also
improved clinical outcomes following acquired drug resistance in
FLT3-ITD-mutated AML (3,27).
However, first-generation FLT3 inhibitors in patients with
an FLT3 mutation have resulted in transient reductions in
the number of blasts but rarely CR improvement (13,14). In
the present study, 7 patients with an FLT3-ITD mutation
received sorafenib plus chemotherapy and exhibited a slightly
higher ORR, when compared with patients who were
FLT3-ITD-negative; however, no statistically significant
difference in OS and RFS was observed between the mono-chemotherapy
and sorafenib plus chemotherapy groups. This may be due to the
small number of patients that were treated with sorafenib, and
future studies should expand the number of cases in order to
confirm the conclusions of the present study.
In summary, the FLT3-ITD mutation has been
identified as a marker of poor prognosis in AML, and the clinical
outcomes of patients with FLT3-ITD-mutated AML combined with
favorable cytogenetics was improved, when compared with those of
patients with FLT3-ITD mono-mutated AML. OS and RFS have
been prolonged due to the application of FLT3 inhibitors and
adjustments in chemotherapy regimens. However, FLT3
inhibitors may lack a durable and deep response, which is mainly
due to acquired drug resistance (3).
Allo-HSCT should be performed as early as possible following CR in
patients with FLT3-ITD-mutated AML, and maintenance therapy
with FLT3 inhibitors may be recommended following
allo-HSCT.
In conclusion, the present data demonstrated that
favorable-risk cytogenetics may improve the clinical outcomes of
patients with FLT3-ITD-mutated AML, but not those of
patients with adverse-risk cytogenetic abnormalities. Sorafenib
combined with chemotherapy may increase OR rates but could not
improve OS and RFS.
Acknowledgements
Not applicable.
Funding
The present study was supported by the ‘333
Projects’ Foundation of Jiangsu Province (grant no. BRA2017243),
the ‘533 Projects’ Foundation of Huai'an City (grant no.
HAA201739), the Science and Technology Fund of Huai'an City (grant
no. HAB201810) and the Science and Technology Fund of Jiangsu
Commission of Health (grant no. H2018085).
Availability of data and materials
Not applicable.
Authors' contributions
ST, CW and LY conceptualized the original idea,
designed the experiments and analyzed the data. ST wrote the paper.
YC, YD, LS, YS, LL, BD and ZH collected the patient information,
treated patients with the regimens and analyzed the data with
statistical software. CW and LY revised the manuscript. All authors
read and approved the final manuscript.
Ethics approval and consent to
participate
The protocol was reviewed and ethically approved by
the Institutional Review Committee of Huai'an No. 1 People's
Hospital (Huai'an, China).
Patients consent for publication
A written informed consent form was obtained from
each patient.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
AML
|
acute myeloid leukemia
|
|
CR
|
complete remission
|
|
OS
|
overall survival
|
|
RFS
|
recurrence free survival
|
|
NPM1
|
nucleophosmin 1
|
|
FLT3-ITD
|
FMS-like tyrosine kinase 3-internal
tandem duplication
|
|
FLT3-TKD
|
FMS-like tyrosine kinase 3-tyrosine
kinase domain
|
References
|
1
|
Döhner H, Weisdorf DJ and Bloomfield CD:
Acute myeloid leukemia. N Engl J Med. 373:1136–1152. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Stone RM, Mandrekar SJ, Sanford BL,
Laumann K, Geyer S, Bloomfield CD, Thiede C, Prior TW, Döhner K,
Marcucci G, et al: Midostaurin plus chemotherapy for acute myeloid
leukemia with a FLT3 mutation. N Engl J Med. 377:454–464. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Choi EJ, Lee JH, Lee JH, Park HS, Ko SH,
Hur EH, Moon J, Goo BK, Kim Y, Seol M, et al: Comparison of
anthracyclines used for induction chemotherapy in patients with
FLT3-ITD-mutated acute myeloid leukemia. Leuk Res. 68:51–56. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Liu Y, He P, Liu F, Shi L, Zhu H, Zhao J,
Wang Y, Cheng X and Zhang M: Prognostic significance of NPM1
mutations in acute myeloid leukemia: A meta-analysis. Mol Clin
Oncol. 2:275–281. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Boddu P, Kantarjian H, Borthakur G, Kadia
T, Daver N, Pierce S, Andreeff M, Ravandi F, Cortes J and Kornblau
SM: Co-occurrence of FLT3-TKD and NPM1 mutations defines a highly
favorable prognostic AML group. Blood Adv. 1:1546–1550. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Yamaura T, Nakatani T, Uda K, Ogura H,
Shin W, Kurokawa N, Saito K, Fujikawa N, Date T, Takasaki M, et al:
A novel irreversible FLT3 inhibitor, FF-10101, shows excellent
efficacy against AML cells with FLT3 mutations. Blood. 131:426–438.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Vardiman JW, Thiele J, Arber DA, Brunning
RD, Borowitz MJ, Porwit A, Harris NL, Le Beau MM,
Hellström-Lindberg E, Tefferi A and Bloomfield CD: The 2008
revision of the World Health Organization (WHO) classification of
myeloid neoplasms and acute leukemia: Rationale and important
changes. Blood. 114:937–951. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Pallisgaard N, Hokland P, Riishøj DC,
Pedersen B and Jørgensen P: Multiplex reverse
transcription-polymerase chain reaction for simultaneous screening
of 29 translocations and chromosomal aberrations in acute leukemia.
Blood. 92:574–588. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Yang YL, Lin SR, Chen JS, Hsiao CC, Lin
KH, Sheen JM, Cheng CN, Wu KH, Lin SW, Yu SL, et al: Multiplex
reverse transcription-polymerase chain reaction as diagnostic
molecular screening of 4 common fusion chimeric genes in Taiwanese
children with acute lymphoblastic leukemia. J Pediatr Hematol
Oncol. 32:e323–e330. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Gou H, Zhou J, Ye Y, Hu X, Shang M, Zhang
J, Zhao Z, Peng W, Zhou Y, Zhou Y, et al: The prevalence and
clinical profiles of FLT3-ITD, FLT3-TKD, NPM1, C-KIT, DNMT3A, and
CEBPA mutations in a cohort of patients with de novo acute myeloid
leukemia from southwest China. Tumour Biol. 37:7357–7370. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Zhu Y, Zhao H, Zhang X, Wu Y, Xie Y, Li Y,
Lian Y, Huang J, Li J, Chen Y and Qian S: Decitabine prior to
low-dose cytarabine-based chemotherapy combined with HLA-mismatched
stem cell micro-transplantation improved outcomes in elderly
patients with newly diagnosed acute myeloid leukaemia. Biol Blood
Marrow Transplant. 23:830–835. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kottaridis PD, Gale RE, Frew ME, Harrison
G, Langabeer SE, Belton AA, Walker H, Wheatley K, Bowen DT, Burnett
AK, et al: The presence of a FLT3 internal tandem duplication in
patients with acute myeloid leukemia (AML) adds important
prognostic information to cytogenetic risk group and response to
the first cycle of chemotherapy: Analysis of 854 patients from the
United Kingdom Medical Research Council AML 10 and 12 trials.
Blood. 98:1752–1759. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Stone RM, DeAngelo DJ, Klimek V, Galinsky
I, Estey E, Nimer SD, Grandin W, Lebwohl D, Wang Y, Cohen P, et al:
Patients with acute myeloid leukemia and an activating mutation in
FLT3 respond to a small-molecule FLT3 tyrosine kinase inhibitor,
PKC412. Blood. 105:54–60. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Smith BD, Levis M, Beran M, Giles F,
Kantarjian H, Berg K, Murphy KM, Dauses T, Allebach J and Small D:
Single-agent CEP-701, a novel FLT3 inhibitor, shows biologic and
clinical activity in patients with relapsed or refractory acute
myeloid leukemia. Blood. 103:3669–3676. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kindler T, Lipka DB and Fischer T: FLT3 as
a therapeutic target in AML: Still challenging after all these
years. Blood. 116:5089–5102. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ding L, Ley TJ, Larson DE, Miller CA,
Koboldt DC, Welch JS, Ritchey JK, Young MA, Lamprecht T, McLellan
MD, et al: Clonal evolution in relapsed acute myeloid leukaemia
revealed by whole-genome sequencing. Nature. 481:506–510. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Shlush LI, Mitchell A, Heisler L, Abelson
S, Ng SWK, Trotman- Grant A, Medeiros JJF, Rao-Bhatia A,
Jaciw-Zurakowsky I, Marke R, et al: Tracing the origins of relapse
in acute myeloid leukaemia to stem cells. Nature. 547:104–108.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Fröhling S, Schlenk RF, Breitruck J,
Benner A, Kreitmeier S, Tobis K, Döhner H and Döhner K; AML Study
Group Ulm, : Acute myeloid leukemia: Prognostic significance of
activating FLT3 mutations in younger adults (16 to 60 years) with
acute myeloid leukemia and normal cytogenetics: A study of the AML
Study Group Ulm. Blood. 100:4372–4380. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Thiede C, Steudel C, Mohr B, Schaich M,
Schäkel U, Platzbecker U, Wermke M, Bornhäuser M, Ritter M,
Neubauer A, et al: Analysis of FLT3-activating mutations in 979
patients with acute myelogenous leukemia: Association with FAB
subtypes and identification of subgroups with poor prognosis.
Blood. 99:4326–4335. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Leick MB and Levis MJ: The future of
targeting FLT3 activation in AML. Curr Hematol Malig Rep.
12:153–167. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ostronoff F, Othus M, Lazenby M, Estey E,
Appelbaum FR, Evans A, Godwin J, Gilkes A, Kopecky KJ, Burnett A,
et al: Prognostic significance of NPM1 mutations in the absence of
FLT3-internal tandem duplication in older patients with acute
myeloid leukemia: A SWOG and UK national cancer research
institute/medical research council report. J Clin Oncol.
33:1157–1164. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Patel SS, Kuo FC, Gibson CJ, Steensma DP,
Soiffer RJ, Alyea EP 3rd, Chen YA, Fathi AT, Graubert TA, Brunner
AM, et al: High NPM1-mutant allele burden at diagnosis predicts
unfavorable outcomes in de novo AML. Blood. 131:2816–2825. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Döhner H, Estey E, Grimwade D, Amadori S,
Appelbaum FR, Büchner T, Dombret H, Ebert BL, Fenaux P, Larson RA,
et al: Diagnosis and management of AML in adults: 2017 ELN
recommendations from an international expert panel. Blood.
129:424–447. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Loghavi S, Zuo Z, Ravandi F, Kantarjian
HM, Bueso-Ramos C, Zhang L, Singh RR, Patel KP, Medeiros LJ, Stingo
F, et al: Clinical features of de novo acute myeloid leukemia with
concurrent DNMT3A, FLT3 and NPM1 mutations. J Hematol Oncol.
7:742014. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Bur illo-Sanz S, Morales-Camacho RM,
Caballero-Velázquez T, Vargas MT, García-Lozano JR, Falantes JF,
Prats-Martín C, Bernal R and Pérez-Simón JA: NUP98-HOXA9 bearing
therapy-related myeloid neoplasm involves myeloid-committed cell
and induces HOXA5, EVI1, FLT3, and MEIS1 expression. Int J Lab
Hematol. 38:64–71. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Cagnetta A, Adamia S, Acharya C, Patrone
F, Miglino M, Nencioni A, Gobbi M and Cea M: Role of genotype-based
approach in the clinical management of adult acute myeloid leukemia
with normal cytogenetics. Leuk Res. 38:649–659. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Mori M and Spraque J: The successful
remission induction by sorafenib and long-term complete remission
in a FLT3-ITD-positive patient with a refractory acute erythroid
leukemia and abnormal cytogenetics. Leuk Res. 36:e1–e3. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Libura M, Giebel S, Piatkowska-Jakubas B,
Pawelczyk M, Florek I, Matiakowska K, Jazwiec B, Borg K, Solarska
I, Zawada M, et al: Cladribine added to daunorubicin-cytarabine
induction prolongs survival of FLT3-ITD+ normal
karyotype AML patients. Blood. 127:360–262. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Stein EM: FLT3 inhibitors for relapsed or
refractory acute myeloid leukaemia. Lancet Oncol. 19:845–850. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Cortes JE, Tallman MS, Schiller GJ, Trone
D, Gammon G, Goldberg SL, Perl AE, Marie JP, Martinelli G,
Kantarjian HM and Levis MJ: Phase 2b study of two dosing regimens
of quizartinib monotherapy in FLT3-ITD mutated, relapsed or
refractory AML. Blood. 132:598–607. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Quizartinib bests chemo for FLT3-mutant
AML. Cancer Discov. 8:OF22018. View Article : Google Scholar
|
|
32
|
Cortes J, Perl AE, Döhner H, Kantarjian H,
Martinelli G, Kovacsovics T, Rousselot P, Steffen B, Dombret H,
Estey E, et al: Quizartinib, an FLT3 inhibitor, as monotherapy in
patients with relapsed or refractory acute myeloid leukaemia: an
open-label, multicentre, single-arm, phase 2 trial. Lancet Oncol.
19:889–903. 2018. View Article : Google Scholar : PubMed/NCBI
|