Introduction
Acute lymphoblastic leukemia (ALL) is the most
common malignancy in children (1).
In the worldwide pediatric population, ALL accounts for 81% of
childhood leukemias; leukemia overall accounts for one third of
cancers diagnosed in children between ages of 0 to 14 years
(1). With the development of
contemporary treatment regimens and advances in epigenomic and
genomic profiling, the overall survival (OS) in pediatric patients
with ALL is >80%, and our understanding of the biology of ALL
relapse has remarkably improved and facilitated more precise risk
determination during the past 10 years (2,3).
However, 20–35% of patients with ALL experience relapse, and
treating relapsed ALL patients is challenging (4–6). ALL
commonly arises from a series of genetic alterations, which may
occur due to inherited susceptibility, exogenous or endogenous
exposure to various mutagens or, rarely, by chance (7,8). Over
the past three decades, several traditional cytogenetic studies of
genetic aberrations including chromosomal translocations and
alterations in chromosome numbers have provided information on the
pathogenesis of ALL (7). To identify
potential molecular targets of ALL, it is crucial to study leukemic
cell and host genetics, as well as to identify new prognostic
markers to optimize individualized therapy, especially for
high-risk groups and relapsed patients (6).
Tumor suppressor protein p53 (TP53) is a gene
encoding a protein that acts as a cellular stress sensor, which is
activated by stress conditions such as DNA damage and oncogene
activation; TP53 induces cell cycle arrest, senescence, apoptosis
or changes in metabolism (9).
Wild-type TP53 has been demonstrated to suppress tumor development
and TP53-mediated protein synthesis, and has been further examined
in mouse models, for example, TP53 knockout mice and mice with
loss-of-function mutations in TP53 develop spontaneous tumors with
100% incidence by 9 months of age (10). TP53 is the most commonly mutated gene
in cancers; mutations have been identified in various types of
cancer and serve as independent markers of poor prognosis in breast
carcinoma, Waldenstrom's macroglobulinemia, non-Hodgkin lymphoma,
medulloblastoma and several other types of cancer (9,11–14). In
addition, median progression-free survival and overall survival
(OS) of TP53-mutated adult patients with chronic lymphocytic
leukemia were significantly decreased, indicating that TP53
mutations may be an adverse prognosis factor independent of the
presence of the 17p deletion (15).
However, TP53 expression and the impact on prognosis is poorly
defined in childhood ALL. Therefore, the aim of the present study
was to investigate TP53 expression and analyze its clinical
significance in patients with childhood ALL.
Materials and methods
Patients
In this retrospective study, a total of 146 patients
with childhood ALL were enrolled, including 60 girls and 86 boys
with a median age of 6 years (range, 1–14 years). All patients were
newly diagnosed with ALL and were consecutively treated in the
Children's Hospital of Zhejiang University School of Medicine
(Hangzhou, China) between January 2007 and September 2010.
Morphological, cytogenetic, immunologic and molecular
characterization criteria were routinely used to diagnose ALL. The
immunophenotypes of the patient included B-lineage ALL (B-ALL;
n=114) and T-lineage ALL (T-ALL; n=32). High risk patients (6 cases
of B-ALL and 6 cases of T-ALL) underwent hematopoietic
stem/progenitor cell transplantation (HSCT). A total of 23 patients
with idiopathic thrombocytopenic purpura (ITP) were recruited for
the control group, including 9 girls and 14 boys with a median age
of 5 years (range, 2–12 years), after written informed consents
were obtained from their parents or guardians. A total of 146 bone
marrow (BM) samples were collected at the time of diagnosis and 23
BM samples from de novo ITP patients at the time of
diagnosis. As peripheral blood (PB) taken at the time of diagnosis
for patients produced similar results as those taken using BM
samples, this was decided to be the main focus of the study. All
treatment protocols were in accordance with the Declaration of
Helsinki and approved by the Institutional Review Board of Ethics
of Children's Hospital of Zhejiang University School of Medicine.
Written informed consent was obtained from the parents or guardians
of all patients.
All patients received a modified National Protocol
of Childhood ALL in China 1997 (NPCAC97) (16). Patients were classified into a
low-risk group if they exhibited all of the following features: i)
Age, 1–10 years; ii) initial white blood cell (WBC) count
<5×1010 cells/l; iii) good prednisone response
(<1,000 blasts/µl); iv) not T cell or mature B cell types; v) no
translocation (t)(9;22), t(1;19) or mixed lineage leukemia (MLL)
rearrangements; vi) bone marrow morphology was M1 on day 15 or day
33; vii) no central nervous system or testicular leukemia at
diagnosis; and viii) minimal residual disease (MRD)
<1×10−4 on day 33. Patients aged >10 years, with
initial WBC between 5×1010 and 1×1011
cells/l, extramedullary involvement at diagnosis, T-ALL or
hypodiploidy (<45 chromosomes) were considered intermediate
risk. Patients aged <1 year old, or with initial WBC counts
≥100×109/l, or with t(9;22), t(4;11) or BCR/ABL1,
MLL/AF4 (the fusion of the MLL gene on chromosome 11 and the AF4
gene on chromosome 4) fusion genes, or poor response to prednisone
or not achieving complete remission (CR) on day 42 were considered
high risk. The median follow-up time was 96 months (range, 1–139
months).
RNA extraction and reverse
transcription-quantitative PCR (RT-qPCR)
Mononucleated cells from 146 cryopreserved BM stored
in liquid nitrogen and 23 BM samples from non-hematological
malignancy disease, i.e. ITP, were isolated by Ficoll gradient
centrifugation, at 350 × g for 20 min at 4°C. Total RNA was
extracted using the High Pure RNA Isolation kit (Roche Diagnostics
GmbH) according to the manufacturer's instructions, and RNA was
reverse-transcribed into cDNA using the ReverTra Ace qPCR RT kit
(Toyobo Life Science) according to the manufacturer's protocol. The
thermocycling conditions were as follows: 65°C for 5 min, followed
by 37°C for 15 min and 98°C for 5 min.
qPCR was performed to determine the TP53 mRNA levels
on a StepOnePlus™ Real-time PCR system (Applied Biosystems; Thermo
Fisher Scientific, Inc.) using GAPDH as an internal reference gene.
All samples were run in triplicates to reduce the chance of errors.
The primer sequences for TP53 amplification were designed using the
Primer 5 software (version 5.0; Premier Biosoft International) and
the sequences are as follows: TP53 forward,
5′-GCGTGTTTGTGCCTGTCCTG-3′ and reverse, 5′-GTGCTCGCTTAGTGCTCCCT-3′
and GAPDH forward, 5′-GAAGGTGAAGGTCGGAGTC-3′ and reverse,
5′-GAAGATGGTGATGGGATTTC-3′. GAPDH was used as the internal control.
Each mixture was composed of 2 µg cDNA, 1 µl TP53 or GAPDH primers
(10 µmol/l), 12.5 µl SYBR®-Green PCR Master mix (Toyobo
Life Science) and deionized water to a total volume of 25 µl. The
thermocycling conditions were as follows: 95°C for 5 min, followed
by 30 cycles of 94°C for 30 sec, 62°C for 30 sec and 72°C for 70
sec, 72°C for 10 min and 4°C for 20 min. The comparative cycle
quantification (Cq) value of the patient samples was used to
determine the relative expression levels of TP53 to GAPDH. The
cycle number difference (ΔCq=TP53-GAPDH) was counted for
each of the triplicates, calculated using the mean value and
expressed as 2−ΔΔCq (17).
Survival analysis
Relapse-free survival (RFS) was defined as the time
between the first CR and relapse, death, second tumor or last
contact with patients. Overall survival (OS) was defined as the
time between the diagnosis and death or last contact with patients.
The end of the follow-up period was September 2018. RFS and OS were
analyzed using the Kaplan-Meier method and log-rank test, while Cox
regression model was used for univariate and multivariate
analyses.
Statistical analysis
The median TP53 value was selected to divide
patients into low- and high-TP53 expression groups. Comparisons of
continuous variables between two groups were performed using the
nonparametric Mann-Whitney U test. Pearson's χ2 or
Fisher's exact test were used to compare the differences between
categorical variables. All analyses were performed using GraphPad
Prism v.5.01 (GraphPad Software, Inc.) and SPSS 25.0 (IBM Corp.).
P<0.05 was considered to indicate a statistically significant
difference.
Results
Association between TP53 expression
and patient clinicopathological characteristics
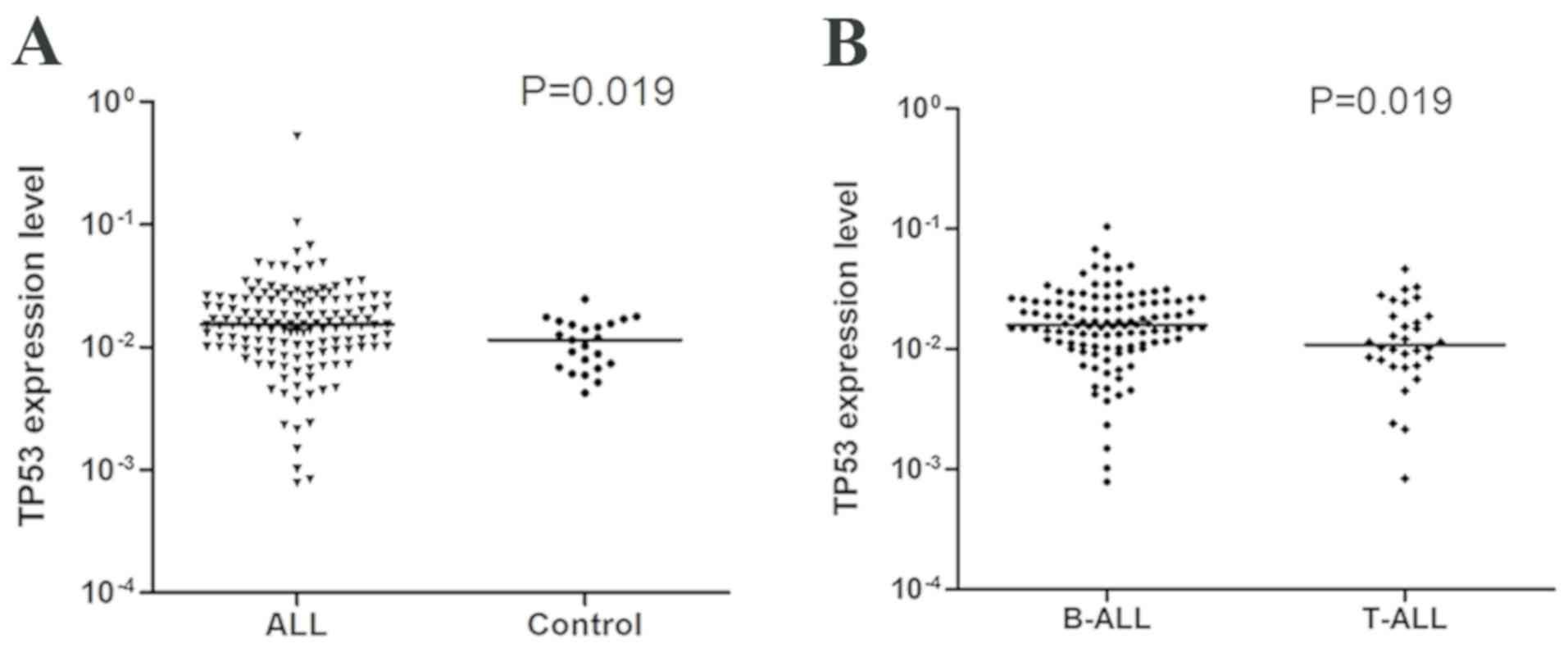
The level of TP53 mRNA was increased in patients
with ALL compared with ITP controls (P=0.019; Fig. 1A). For statistical analyses, patients
were divided into high- and low-TP53 expression groups according to
the median value. Associations between TP53 expression and clinical
and molecular features, including age, sex, WBC, PB blasts and
platelet count (PLT) at diagnosis, extramedullary involvement,
immunophenotype, risk stratification, breakpoint cluster region/ABL
proto-oncogene 1 (BCR/ABL1) and MLL/AF4-FMR2 family member 1
(MLL/AF4) fusion genes and MRD levels on days 15 and 33, were
compared between the two groups. Overall, patients in the high-TP53
expression group exhibited lower PB blast percentages (median, 10
vs. 25%; P=0.025) and a higher PLT count (median, 70×109
vs. 52×109 cells/l; P=0.043). However, no significant
association was observed between TP53 expression level and sex,
age, WBC count, BM blasts, extramedullary involvement, risk groups,
presence of BCR/ABL1 or MLL/AF4 fusion genes and MRD on day 15 or
33 (Table I).
 | Table I.Clinicopathological characteristics of
patients with high and low expression levels of TP53
expression. |
Table I.
Clinicopathological characteristics of
patients with high and low expression levels of TP53
expression.
| Characteristic | Low TP53 (n=73) | High TP53 (n=73) | P-value |
|---|
| Age, years |
|
| 0.696 |
|
Median | 6 | 6 |
|
|
Range | 1–14 | 1–14 |
|
| Sex, male, n (%) | 42 (58) | 44 (60) | 0.737 |
| WBC count,
×109 cells/l |
|
| 0.181 |
|
Median | 23.6 | 20.2 |
|
|
Range | 0.14–385.60 | 0.80–888.40 |
|
| PB blasts, % |
|
| 0.025a |
|
Median | 25 | 10 |
|
|
Range | 0–85 | 0–75 |
|
| BM blasts, % |
|
| 0.219 |
|
Median | 90 | 89 |
|
|
Range | 56–97 | 23–98 |
|
| PLT count,
×109 cells/l |
|
| 0.043a |
|
Median | 52 | 70 |
|
|
Range | 10–359 | 4–375 |
|
| Extramedullary
involvement, n (%) |
|
| 0.317 |
| Yes | 3 (4) | 1 (1) |
|
| Immunophenotype, n
(%) |
|
| 0.054 |
|
B-ALL | 52 (71) | 62 (85) |
|
|
T-ALL | 21 (29) | 11 (15) |
|
| Risk, n (%) |
|
| 0.264 |
|
Low | 27 (37) | 18 (25) |
|
|
Intermediate | 17 (23) | 19 (26) |
|
|
High | 29 (40) | 36 (49) |
|
| BCR/ABL1, n
(%) |
|
| 0.754 |
|
Present | 6 (8) | 5 (7) |
|
|
Absent | 67 (92) | 68 (93) |
|
| MLL/AF4, n (%) |
|
| 1.000 |
|
Present | 1 (1) | 1 (1) |
|
|
Absent | 72 (99) | 72 (99) |
|
| Day 15 MRD, n
(%) |
|
| 0.501 |
|
≥0.01% | 28 (38) | 32 (44) |
|
|
<0.01% | 45 (62) | 41 (56) |
|
| Day 33 MRD, n
(%) |
|
| 0.081 |
|
≥0.01% | 51 (70) | 60 (82) |
|
|
<0.01% | 22 (30) | 13 (18) |
|
TP53 is a risk factor in childhood
ALL
Patients in the high-TP53 expression group exhibited
poorer CR rates compared with those in the low-expression group (85
vs. 96%; P=0.025); however, no association was observed in the
prednisone response between the two groups (87 vs. 79%; P=0.387).
In addition, relapse rates between the low- and high-TP53
expression groups (19 vs. 26%; P=0.259) were not significantly
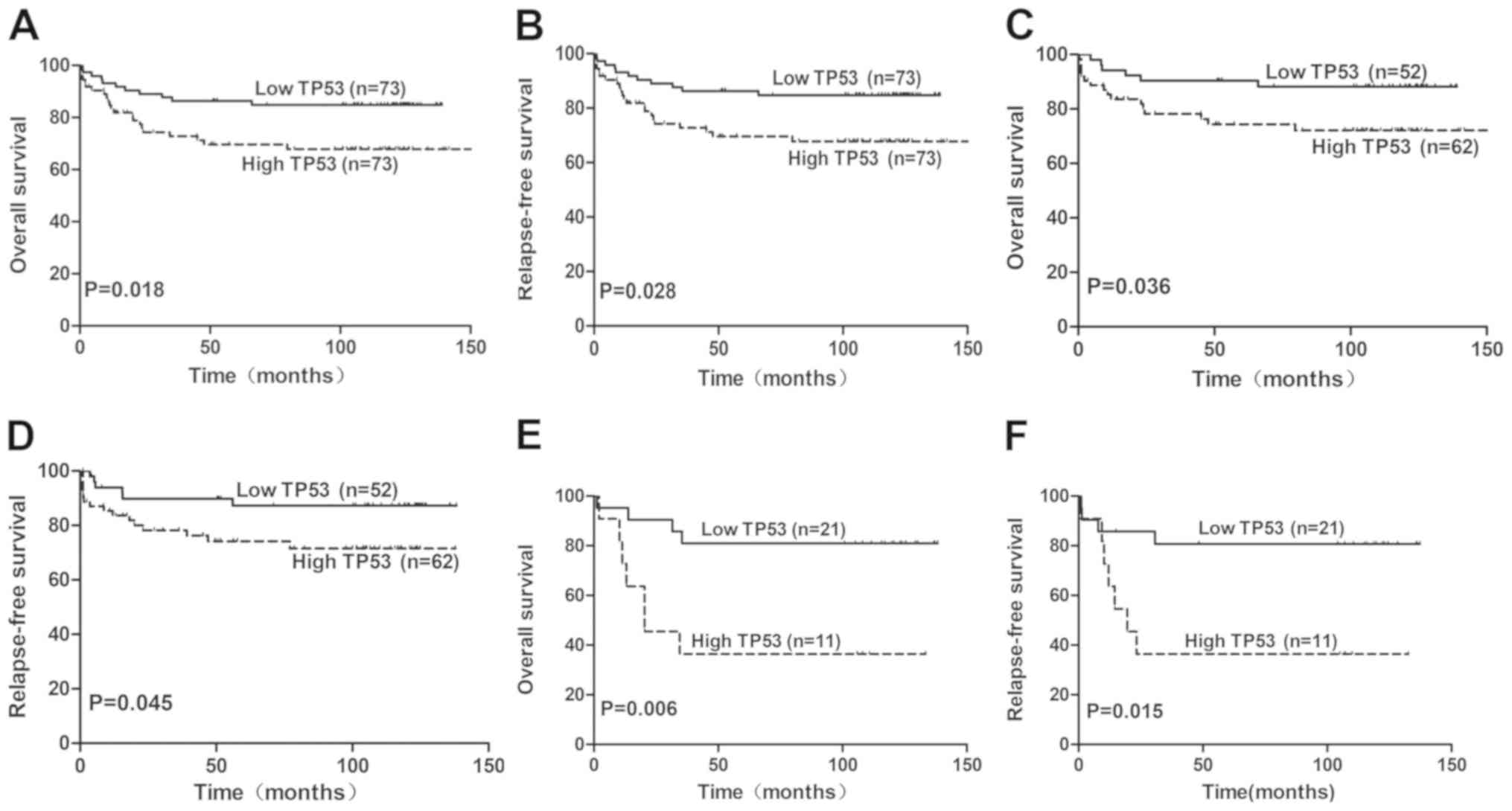
different (Table II). Compared with
the low-TP53 expression group, the OS rate of the high-TP53
expression group was significantly lower, with the 5-year OS rate
of 73 vs. 88% [95% confidence interval (CI), 65–82 vs. 78–97%;
P=0.018; Fig. 2A]. In addition, a
significant difference was identified between the 5-year RFS rates
of the low- and high-TP53 expression groups (median, 86 vs. 71%;
95% CI, 77–95 vs. 61–80%; P=0.028; Fig.
2B).
| Table II.Patient outcomes according to TP53
expression levels. |
Table II.
Patient outcomes according to TP53
expression levels.
| Outcome | Low TP53 | High TP53 | P-value |
|---|
| Induction
regimen-sensitive, n (%) | 62 (85) | 58 (79) | 0.387 |
| CR, n (%) | 70 (96) | 62 (85) | 0.025a |
| Relapse, n (%) | 13 (19) | 16 (26) | 0.259 |
| 5-year RFS, % (95%
CI) | 86 (77–95) | 71 (61–80) | 0.028a |
| 5-year OS, % (95%
CI) | 88 (78–97) | 73 (65–82) | 0.018a |
Multivariate analyses using the Cox proportional
hazards model revealed that in patients with childhood ALL, TP53
was an independent prognostic factor for OS and RFS. For OS, the
hazard of death from any cause for patients in the high-TP53
expression group was >3-fold higher compared with patients in
the low-TP53 expression group [hazard ratio (HR)=6.865; 95% CI,
2.665–17.685; P<0.001; Table
III). High TP53 expression was a poor independent prognostic
factor for RFS with a HR of 5.832 (95% CI, 2.340–14.533;
P<0.001; Table III). However,
sex, age, WBC count, BM blasts, PB blasts, MRD on day 15 or 33,
risk group and BCR/ABL1 fusion gene had no predictive value in the
prognosis of OS and RFS.
| Table III.Multivariate analyses for RFS and OS
in patients with childhood ALL. |
Table III.
Multivariate analyses for RFS and OS
in patients with childhood ALL.
|
| OS | RFS |
|---|
|
|
|
|
|---|
| Factor | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| TP53 expression
(high vs. low) | 6.865 | 2.665–17.685 |
<0.001a | 5.832 | 2.340–14.533 |
<0.001a |
| Sex (male vs.
female) | 2.184 | 0.949–5.029 | 0.066 | 2.228 | 0.973–5.863 | 0.083 |
| Age (≥10 vs. <10
years) | 1.425 | 0.625–3.248 | 0.400 | 1.537 | 0.675–3.500 | 0.306 |
| WBC count
(≥50×109 vs. <50×109 cells/l) | 1.835 | 0.527–6.395 | 0.340 | 1.494 | 0.435–5.128 | 0.524 |
| BM blasts (≥ median
vs. < median) | 0.770 | 0.336–1.7610 | 0.535 | 0.760 | 0.335–1.725 | 0.511 |
| PB blasts (≥ median
vs. < median) | 1.295 | 0.412–4.066 | 0.658 | 1.452 | 0.464–4.539 | 0.522 |
| Risk (high vs. low
+ intermediate) | 2.000 | 0.741–5.396 | 0.171 | 1.675 | 0.640–4.381 | 0.293 |
| CR (no vs.
yes) | 1.061 | 0.240–4.684 | 0.937 | 0.985 | 0.217–4.480 | 0.984 |
| BCR-ABL1 (present
vs. absent) | 0.774 | 0.172–3.494 | 0.739 | 0.613 | 0.137–2.750 | 0.523 |
| Day 15 MRD (≥0.01
vs. <0.01%) | 0.840 | 0.325–2.171 | 0.718 | 0.945 | 0.355–2.510 | 0.909 |
| Day 33 MRD (≥0.01
vs. <0.01%) | 1.224 | 0.490–3.060 | 0.665 | 1.255 | 0.517–3.045 | 0.615 |
Outcomes and prognostic significance
of TP53 expression in patients with B-ALL and T-ALL
Median TP53 gene expression was higher in B-ALL
compared with that in T-ALL (P=0.019; Fig. 1B). TP53 expression levels were
further investigated in 114 patients with B-ALL. Among the clinical
and molecular features, only BM blasts were significantly different
between the high- and low-TP53 expression groups (median, 89 vs.
92%; P=0.040; Table IV). The
association between TP53 expression levels and outcomes in patients
with B-ALL was subsequently analyzed. The patients in the low-TP53
expression group exhibited a higher 5-year OS rate (89 vs. 75%; 95%
CI, 79–98 vs. 66–85%; P=0.036; Table
IV; Fig. 2C) and a higher 5-year
RFS rate (87 vs. 68%; 95% CI, 78–97% vs. 59–76%; P=0.045; Table IV; Fig.
2D) compared with the high-TP53 expression group. In addition,
the high-TP53 expression group exhibited a lower CR rate compared
with the low-TP53 expression group (84 vs. 98%; P=0.011). No
significant differences were observed between the two groups in
induction regimen (P=0.622) or relapse rates (P=0.779). For
patients with B-ALL, results from multivariate analysis with Cox
proportional hazards model revealed that the upregulation of TP53
was an independent prognostic factor for poor OS (HR=6.436; 95% CI,
2.167–19.115; P=0.001; Table V). CR
was also an independent prognostic factor for OS (HR=0.175; 95% CI,
0.048–0.641; P=0.008; Table V). In
addition, high TP53 expression (HR=6.026; 95% CI, 2.050–17.717;
P=0.001) and CR (HR=0.2577; 95% CI, 0.073–0.900; P=0.034; Table V) were independent prognostic factors
for RFS.
| Table IV.TP53 expression in patients with
childhood B-ALL. |
Table IV.
TP53 expression in patients with
childhood B-ALL.
| Characteristic | Low TP53
(n=52) | High TP53
(n=62) | P-value |
|---|
| BM blasts, %,
median (range) | 89 (72–97) | 92 (23–98) | 0.040a |
| Induction
regimen-sensitive, n (%) | 43 (83) | 49 (79) | 0.622 |
| CR, n (%) | 51 (98) | 52 (84) | 0.011a |
| Relapse | 9
(18) | 12 (23) | 0.779 |
| 5-year RFS, % (95%
CI) | 87 (78–97) | 68 (59–76) | 0.045a |
| 5-year OS, % (95%
CI) | 89 (79–98) | 75 (66–85) | 0.036a |
| Table V.Multivariate analysis of RFS and OS
in patients with childhood B-ALL. |
Table V.
Multivariate analysis of RFS and OS
in patients with childhood B-ALL.
|
| OS | RFS |
|---|
|
|
|
|
|---|
| Factor | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| TP53 expression
(high vs. low) | 6.436 | 2.167–19.115 | 0.001a | 6.026 | 2.050–17.717 | 0.001a |
| Sex (male vs.
female) | 0.973 | 0.392–2.420 | 0.954 | 0.849 | 0.342–2.109 | 0.725 |
| Age (≥10 vs. <10
years) | 2.474 | 0.722–9.626 | 0.467 | 2.591 | 0.693–9.545 | 0.374 |
| WBC count
(≥50×109 vs. <50×109 cells/l) | 2.799 | 0.783–10.010 | 0.113 | 2.115 | 0.640–6.991 | 0.220 |
| BM blasts (≥ median
vs. < median) | 1.529 | 0.558–4.189 | 0.409 | 1.464 | 0.541–3.967 | 0.453 |
| PB blasts (≥ median
vs. < median) | 1.582 | 0.447–5.603 | 0.477 | 1.977 | 0.610–6.410 | 0.256 |
| Risk (high vs. low
+ intermediate) | 2.725 | 0.969–7.663 | 0.057 | 3.113 | 1.106–8.762 | 0.032a |
| CR (no vs.
yes) | 0.175 | 0.048–0.641 | 0.008a | 0.257 | 0.073–0.900 | 0.034a |
| BCR-ABL1 (present
vs. absent) | 0.661 | 0.161–2.713 | 0.565 | 0.609 | 0.148–2.506 | 0.492 |
| Day 15 MRD (≥0.01
vs. <0.01%) | 0.726 | 0.276–1.912 | 0.517 | 0.738 | 0.283–1.924 | 0.535 |
| Day 33 MRD (≥0.01
vs. <0.01%) | 1.441 | 0.506–4.105 | 0.494 | 1.519 | 0.532–4.334 | 0.435 |
Analysis of the association between TP53 expression
and patient outcomes was also performed in 32 patients with T-ALL.
Among all the clinical features, no statistical differences were
observed between the high- and low-TP53 expression groups. However,
in survival analyses, significant differences were observed between
the low- and high-TP53 groups in OS and RFS (P<0.05; Fig. 2E and F).
Discussion
Progress in ALL treatment development has led to a
cure rate of >80% in children; however, a certain number of
patients experience relapse (18).
TP53 is a crucial tumor suppressor gene responsible for major
defense against tumor growth as it promotes autophagy, apoptosis
signaling, transcription, immune or inflammatory responses
(10,18,19). In
addition, TP53 is an extensively studied gene in a variety of types
of cancer, including hematopoietic malignancies, especially in
acute myeloid leukemia (20–24). A previous study demonstrated that
TP53 upregulation predicts poor outcome in human laryngeal squamous
cell carcinoma (25). The present
study aimed to identify the association between the levels of TP53
expression and childhood ALL. To the best of our knowledge, this is
the first study to focus on TP53 mRNA levels in patients with
childhood ALL.
In the present study, TP53 expression was determined
in 146 patients with childhood ALL to test whether TP53 mRNA levels
had impact on treatment outcomes. The results demonstrated that the
expression of TP53 in patients with childhood ALL was significantly
higher compared with that in the control group. When the
association between TP53 expression levels and clinicopathological
characteristics was analyzed, the results revealed that the high
TP53 expression is associated with low percentage of PB blasts and
high PLT count. This suggests that high TP53 expression may be a
prognostic marker for patients with ALL. Elliott et al
(26) have reported that in
childhood ALL, circulating peripheral blood blasts rapidly decline
in response to the induction of chemotherapy; in addition,
prednisone has been identified as an important prognostic factor.
Another study demonstrated that the strong association between
platelet counts following induction treatment and MRD risk group
distribution enabled PLT count to be considered a strong prognostic
factor for the improvement of therapeutic risk stratification in
trials (27). In addition, from the
present study, in patients with childhood B-ALL, high TP53
expression was related to lower BM blasts and poor OS.
The results of the present study have revealed
significant associations between the levels of TP53 expression and
clinical outcomes; this may help independently predict the
prognosis of patients with newly-diagnosed ALL. Patients with low
TP53 expression levels were more likely to achieve CR following the
induction therapy; the results from the present study revealed a
promising 5-year OS of 88% and 5-year RFS of 86%. In addition, the
results of the present study demonstrated that in 132 patients with
B-ALL, BM blasts in the high-TP53 expression group were lower
compared with those in the low-TP53 expression group. The high-TP53
expression group also exhibited worse OS and RFS rates compared
with the low-TP53 expression group.
In the multivariate analyses, including 11 clinical
prognostic factors, high expression of TP53 was an independent
predictor for poor OS and RFS in the entire cohort. This indicated
that high TP53 expression levels may be considered an adverse
prognostic factor for OS and RFS of patients with childhood
ALL.
The reasons for increased TP53 expression levels in
patients with childhood ALL compared with those in the control
group, and for higher TP53 expression in B-ALL compared with that
in T-ALL remain uncertain. A feasible explanation would be that
TP53 directly activates a core transcriptional program with diverse
biological functions, which is associated with high-occupancy TP53
enhancers, high levels of paused RNA polymerases and accessible
chromatin (28). As TP53 is
upregulated in leukemia cells, the likelihood of a gene mutation
and loss of antitumor function increases. In addition, high TP53
expression may be an indicator of TP53 loss-of-function due to the
impairment of the auto-regulatory feedback loop, which consequently
induces TP53-induced protein degradation (29) and directly influences survival in
patients with childhood ALL. Additionally, upregulated TP53
expression in B-cell leukemia may be responsible for B cell lineage
leukemia activation, and may facilitate TP53 transcription levels
to exceed the normal value.
The results of the present study must be interpreted
with caution. As this study used a retrospective cohort, a
relatively small sample size was used, and all data originated from
a single center, which may have biased the analysis. In addition,
as all the available samples were transcribed into cDNA in our
previous studies, not enough BM tissue was present for
immunohistochemical analysis. A multi-center prospective study is
needed in the future to verify the results.
In summary, high TP53 expression may be associated
with poor prognosis and inferior CR in childhood ALL. TP53
upregulation may be a prognostic and predictive biomarker in
patients with childhood ALL.
Acknowledgements
Not applicable.
Funding
This study was supported in part by grants from the
National Natural Science Foundation of China (grant nos. 81470304
and 81770202) and Key Grants of Zhejiang Provincial Science and
Technology Department (grant no. 2019C03032).
Availability of data and materials
The data that support the findings of this study are
available from (Children's Hospital of Zhejiang University School
of Medicine, Zhejiang, China) but restrictions apply to the
availability of these data, which were used under license for the
current study, and so are not publicly available. Data are however
available from the authors upon reasonable request and with
permission of (Children's Hospital of Zhejiang University School of
Medicine).
Authors' contributions
WW and PZ performed the experiments, data collection
and analysis, as well as drafting the manuscript. JR, YZ and DB
assisted in completing the statistical analysis. YT designed the
study, validated the data and revised the manuscript. All authors
read and approved the final manuscript.
Ethics approval and consent to
participate
All treatment protocols were in accordance with the
Declaration of Helsinki and approved by the Institutional Review
Board of Ethics of Children's Hospital of Zhejiang University
School of Medicine. Written informed consent was obtained from the
parents or guardians of all patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Woo JS, Alberti MO and Tirado CA:
Childhood B-acute lymphoblastic leukemia: A genetic update. Exp
Hematol Oncol. 3:162014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Tasian SK, Loh ML and Hunger SP: Childhood
acute lymphoblastic leukemia: Integrating genomics into therapy.
Cancer. 121:3577–3590. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Harvey RC, Mullighan CG, Wang X, Dobbin
KK, Davidson GS, Bedrick EJ, Chen IM, Atlas SR, Kang H, Ar K, et
al: Identification of novel cluster groups in pediatric high-risk
B-precursor acute lymphoblastic leukemia with gene expression
profiling: Correlation with genome-wide DNA copy number
alterations, clinical characteristics and outcome. Blood.
116:4874–4884. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Vrooman LM and Silverman LB: Treatment of
childhood acute lymphoblastic leukemia: Prognostic factors and
clinical advances. Curr Hematol Malig Rep. 11:385–394. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Jaime-Perez JC, Pinzon-Uresti MA,
Jimenez-Castillo RA, Colunga-Pedraza JE, Gonzalez-Llano O and
Gomez-Almaguer D: Relapse of childhood acute lymphoblastic leukemia
and outcomes at a reference center in Latin America: Organomegaly
at diagnosis is a significant clinical predictor. Hematology.
23:1–9. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Bhojwani D and Pui CH: Relapsed childhood
acute lymphoblastic leukaemia. Lancet Oncol. 14:e205–e217. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Bhojwani D, Yang JJ and Pui CH: Biology of
childhood acute lymphoblastic leukemia. Pediatr Clin North Am.
62:47–60. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Inaba H, Greaves M and Mullighan CG: Acute
lymphoblastic leukaemia. Lancet. 381:1943–1955. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bykov VJN, Eriksson SE, Bianchi J and
Wiman KG: Targeting mutant p53 for efficient cancer therapy. Nat
Rev Cancer. 18:89–102. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Aubrey BJ, Strasser A and Kelly GL:
Tumor-suppressor functions of the TP53 pathway. Cold Spring Harb
Perspect Med. 6(pii): a0260622016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Zhukova N, Ramaswamy V, Remke M, Pfaff E,
Shih DJ, Martin DC, Castelo-Branco P, Baskin B, Ray PN, Bouffet E,
et al: Subgroup-specific prognostic implications of TP53 mutation
in medulloblastoma. J Clin Oncol. 31:2927–2935. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Xu P, Liu X, Ouyang J and Chen B: TP53
mutation predicts the poor prognosis of non-Hodgkin lymphomas:
Evidence from a meta-analysis. PLoS One. 12:e01748092017.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Poulain S, Roumier C, Bertrand E,
Renneville A, Caillault-Venet A, Doye E, Geffroy S, Sebda S,
Nibourel O, Nudel M, et al: TP53 mutation and its prognostic
significance in Waldenstrom's Macroglobulinemia. Clin Cancer Res.
23:6325–6335. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Petitjean A, Achatz MI, Borresen-Dale AL,
Hainaut P and Olivier M: TP53 mutations in human cancers:
Functional selection and impact on cancer prognosis and outcomes.
Oncogene. 26:2157–2165. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Zenz T, Eichhorst B, Busch R, Denzel T,
Häbe S, Winkler D, Bühler A, Edelmann J, Bergmann M, Hopfinger G,
et al: TP53 mutation and survival in chronic lymphocytic leukemia.
J Clin Oncol. 28:4473–4479. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
ang Y, Xu X, Song H, Yang S, Shi S and Wei
J: Long-term outcome of childhood acute lymphoblastic leukemia
treated in China. Pediatr Blood Cancer. 51:380–386. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Stengel A, Schnittger S, Weissmann S,
Kuznia S, Kern W, Kohlmann A, Haferlach T and Haferlach C: TP53
mutations occur in 15.7% of ALL and are associated with
MYC-rearrangement, low hypodiploidy and a poor prognosis. Blood.
124:251–258. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Rabinovich GA, Gabrilovich D and Sotomayor
EM: Immunosuppressive strategies that are mediated by tumor cells.
Annu Rev Immunol. 25:267–296. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Welch JS, Petti AA, Miller CA, Fronick CC,
O'Laughlin M, Fulton RS, Wilson RK, Baty JD, Duncavage EJ, Tandon
B, et al: TP53 and Decitabine in acute myeloid leukemia and
myelodysplastic syndromes. N Engl J Med. 375:2023–2036. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Stengel A, Kern W, Haferlach T,
Meggendorfer M, Fasan A and Haferlach C: The impact of TP53
mutations and TP53 deletions on survival varies between AML, ALL,
MDS and CLL: An analysis of 3307 cases. Leukemia. 31:705–711. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Prokocimer M, Molchadsky A and Rotter V:
Dysfunctional diversity of p53 proteins in adult acute myeloid
leukemia: Projections on diagnostic workup and therapy. Blood.
130:699–712. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Montalban-Bravo G, Takahashi K and
Garcia-Manero G: Decitabine in TP53-mutated AML. N Engl J Med.
376:796–797. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Bolouri H, Farrar JE, Triche T Jr, Ries
RE, Lim EL, Alonzo TA, Ma Y, Moore R, Mungall AJ, Marra MA, et al:
The molecular landscape of pediatric acute myeloid leukemia reveals
recurrent structural alterations and age-specific mutational
interactions. Nat Med. 24:103–112. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Qiu X, You Y, Huang J, Wang X, Zhu H and
Wang Z: LAMP3 and TP53 overexpression predicts poor outcome in
laryngeal squamous cell carcinoma. Int J Clin Exp Pathol.
8:5519–5527. 2015.PubMed/NCBI
|
|
26
|
Elliott MA, Litzow MR, Letendre LL, Wolf
RC, Hanson CA, Tefferi A and Tallman MS: Early peripheral blood
blast clearance during induction chemotherapy for acute myeloid
leukemia predicts superior relapse-free survival. Blood.
110:4172–4174. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Zeidler L, Zimmermann M, Möricke A,
Meissner B, Bartels D, Tschan C, Schrauder A, Cario G, Goudeva L,
Jäger S, et al: Low platelet counts after induction therapy for
childhood acute lymphoblastic leukemia are strongly associated with
poor early response to treatment as measured by minimal residual
disease and are prognostic for treatment outcome. Haematologica.
97:402–409. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Andrysik Z, Galbraith MD, Guarnieri AL,
Zaccara S, Sullivan KD, Pandey A, MacBeth M, Inga A and Espinosa
JM: Identification of a core TP53 transcriptional program with
highly distributed tumor suppressive activity. Genome Res.
27:1645–1657. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Muller-Thomas C, Rudelius M, Rondak IC,
Haferlach T, Schanz J, Huberle C, Schmidt B, Blaser R, Kremer M,
Peschel C, et al: Response to azacitidine is independent of p53
expression in higher-risk myelodysplastic syndromes and secondary
acute myeloid leukemia. Haematologica. 99:e179–e181. 2014.
View Article : Google Scholar : PubMed/NCBI
|