Introduction
Intrahepatic bile duct cancer (IHBDC) is a type of
cancer usually considered to be a primary liver malignancy
(1). The most common histological
type of IHBDC is intrahepatic cholangiocarcinoma (ICC), with a
5-year overall survival (OS) rate of 15–45% worldwide (2–5).
Considering these poor patient outcomes, an accurate staging system
is required to stratify patients by risk of mortality.
Recently, the 8th edition of American Joint
Committee on Cancer (AJCC) staging system for ICC has been released
and applied in clinical practice (6). The main changes focus on the definition
of T category. Of these, the T1 category was further divided into
T1a (≤5 cm) and T1b (>5 cm) by tumor size. This is the first
time the impact of tumor size in the AJCC staging system has been
accounted for.
Yamashita et al (7) identified that patients with ICC and a
tumor size ≥4.4 cm were more likely to relapse compared with
patients with ICC and a tumor size <4.4 cm. Furthermore,
Spolverato et al (8) reported
that the larger the tumor size, the higher the incidence of
microscopic vascular invasion. In addition, larger tumors were
associated with poor biological behaviors (e.g. worse tumor grade)
(8). These findings suggest that
large tumor sizes have a negative impact on the survival of
patients with ICC. However, the rationality of the cut-off value of
5 cm has not yet been validated in the latest AJCC staging
system.
In the present study, the Surveillance Epidemiology
and End Results (SEER) database, a population-based database, was
used to assess the relationship between the tumor size and
prognosis. Specifically, the optimal cut-off value for tumor size
in the stratification of T1 ICC tumors was investigated.
Materials and methods
Patients
Patient data were downloaded from the SEER database
(https:seer.cancer.gov) (between Jan 2004 and Dec
2013, during first diagnosis and entered into the database) using
the SEER*Stat software (version 8.2.0; National Cancer Institute).
ICC was retrieved from the site recode C22.1, according to the
International Classification of Diseases for Oncology (3rd edition)
(9). The inclusion criteria were as
follows: i) Age, ≥18 years; ii) diagnosed as ICC with positive
histology confirmed by histopathological and immunohistochemical
analysis; iii) stage I tumor according to the 8th AJCC TNM staging
system (10); iv) definite tumor
size stated in mm; v) first primary tumor; and vi) available
follow-up information. Demographic and pathological characteristics
included age, ethnicity, sex, marital status [classified as married
or other, (divorced, separated, single (never married), widowed and
unknown marital status)], tumor size, grade and surgical treatment.
The total follow-up time ranged between 0 and 118 months.
Statistical analysis
The differences between patients with stage IA and
IB tumors were evaluated using an independent t-test or
χ2 test. Univariate and multivariate analyses were
performed using the Cox regression model and the data is presented
as hazard ratio (HR) and 95% confidence interval (CI). Patients
with unknown grade information were excluded in the univariate and
multivariate analyses. Survival curves were then plotted using the
Kaplan-Meier method and the log-rank test. X-tile software (version
3.6.1; Yale University) was used to examine the optimal tumor size
(11). All analyses were performed
using PASW statistics v18 (SPSS, Inc). P<0.05 was considered to
indicate a statistically significant difference.
Results
A total of 407 patients with ICC, including 199
cases with stage IA and 208 cases with stage IB tumors, were
finally selected for further analysis using inclusion criteria.
Demographic and pathological characteristics are presented in
Table I. The median age of the
entire cohort was 66 years (range, 18–99 years), and the majority
of patients were Caucasian (73.0%). The mean tumor size was 58.1 mm
(range, 5–167). Additionally, the proportion of patients with well-
and moderately differentiated tumors (grade I+II) was higher
compared with those with poorly differentiated and undifferentiated
tumors (grade III+IV) (47.4 vs. 20.9%). Except for patients with
unknown grade information, the incidence of grade III+IV was
significantly higher in stage IB than in stage IA (34.5 vs. 26.6%).
There were no significant differences between stage IA and IB with
respect to patient age, ethnicity, sex and grade (P>0.05).
However, significantly more patients with stage IA received
surgical treatment compared with patients with stage IB (64.3 vs.
49.0%; P<0.001). Patients who were married also accounted for a
higher proportion of patients with stage IA compared with stage IB
(P<0.027).
 | Table I.Demographic and pathological
characteristics of patients with intrahepatic
cholangiocarcinoma. |
Table I.
Demographic and pathological
characteristics of patients with intrahepatic
cholangiocarcinoma.
| Variables | Overall (n=407) | Stage IA (n=199) | Stage IB (n=208) | P-value |
|---|
| Age,
yearsa | 66 (18–99) | 66 (35–97) | 67 (18–99) | >0.05 |
| Ethnicity |
|
|
| >0.05 |
|
Caucasian | 297 | 146 | 151 |
|
| African
American | 40 | 16 | 24 |
|
|
Other | 70 | 37 | 33 |
|
| Sex |
|
|
| >0.05 |
| Male | 183 | 95 | 88 |
|
|
Female | 224 | 104 | 120 |
|
| Marital status |
|
|
| 0.027 |
|
Married | 231 | 124 | 107 |
|
|
Otherb | 176 | 75 | 101 |
|
| Tumor
size, mmc | 58.1 (5.0–167.0) | 33.2 (5.0–50.0) | 82.0
(51.0–167.0) | <0.001 |
| Grade |
|
|
| >0.05 |
| I+II | 193 | 102 | 91 |
|
|
III+IV | 85 | 37 | 48 |
|
|
Unknown | 129 | 60 | 69 |
|
| Surgery |
|
|
| <0.001 |
| Yes | 230 | 128 | 102 |
|
| No | 177 | 71 | 106 |
|
Univariate and multivariate Cox regression model
analyses of OS time were performed for patients with ICC (Tables II and III). In univariate analysis, prognostic
factors identified in patients with stage IA ICC included age,
grade (I+II vs. III+IV) and surgery (yes vs. no). Prognostic
factors identified in patients with stage IB ICC included age,
grade (I+II vs. III+IV), surgery (yes vs. no) and tumor size (5–7
vs. ≥7 cm). In multivariate analysis, independent prognostic
factors identified in patients with stage IA ICC were age and
surgery (yes vs. no). Alternatively, independent prognostic factors
for patients with stage IB ICC included age, surgery (yes vs. no)
and tumor size (5–7 vs. ≥7 cm).
| Table II.Univariate Cox regression model
analysis of overall survival in patients with intrahepatic
cholangiocarcinoma. |
Table II.
Univariate Cox regression model
analysis of overall survival in patients with intrahepatic
cholangiocarcinoma.
|
| Stage IA | Stage IB |
|---|
|
|
|
|
|---|
| Variables | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age, years | 1.036
(1.016–1.055) | <0.001 | 1.039
(1.023–1.056) | <0.001 |
| Ethnicity |
|
|
|
|
|
Caucasian | Reference |
| Reference |
|
| African
American | 1.032
(0.516–2.062) |
0.929 | 1.044
(0.593–1.838) |
0.882 |
|
Other | 0.744
(0.457–1.211) |
0.234 | 1.131
(0.671–1.905) |
0.644 |
| Sex |
|
|
|
|
| Male | Reference |
| Reference |
|
|
Female | 1.023
(0.699–1.499) |
0.905 | 0.764
(0.530–1.101) |
0.148 |
| Grade |
|
|
|
|
| I+II | Reference |
| Reference |
|
|
III+IV | 1.680
(1.031–2.735) |
0.037 | 1.849
(1.158–2.952) |
0.010 |
| Marital status |
|
|
|
|
|
Married | Reference |
| Reference |
|
|
Other | 1.086
(0.731–1.613) |
0.682 | 1.092
(0.761–1.567) |
0.634 |
| Surgery |
|
|
|
|
| Yes | Reference |
| Reference |
|
| No | 4.178
(2.820–6.188) | <0.001 | 4.071
(2.732–6.066) | <0.001 |
| Tumor size, mm |
|
|
|
|
|
51–69 |
|
| Reference |
|
|
≥70 | – | – | 1.882
(1.242–2.851) |
0.003 |
| Table III.Multivariate Cox regression model
analysis of overall survival in patients with intrahepatic
cholangiocarcinoma. |
Table III.
Multivariate Cox regression model
analysis of overall survival in patients with intrahepatic
cholangiocarcinoma.
|
| Stage IA | Stage IB |
|---|
|
|
|
|
|---|
| Variables | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age, years | 1.027
(1.008–1.046) |
0.005 | 1.034
(1.017–1.052) | <0.001 |
| Ethnicity |
|
|
|
|
|
Caucasian | Reference |
| Reference |
|
| African
American | 1.165
(0.580–2.340) |
0.668 | 1.045
(0.583–1.870) |
0.883 |
|
Other | 0.699
(0.426–1.145) |
0.155 | 0.946
(0.553–1.617) |
0.839 |
| Sex |
|
|
|
|
|
Male | Reference |
| Reference |
|
|
Female | 0.909
(0.597–1.386) |
0.658 | 0.877
(0.593–1.295) |
0.509 |
| Grade |
|
|
|
|
|
I+II | Reference |
| Reference |
|
|
III+IV | 1.315
(0.797–2.170) |
0.284 | 1.643
(1.000–2.697) |
0.050 |
| Surgery |
|
|
|
|
|
Yes | Reference |
| Reference |
|
| No | 3.713
(2.431–5.670) | <0.001 | 2.765
(1.795–4.259) | <0.001 |
| Tumor size, mm |
|
|
|
|
|
51–69 |
|
| Reference |
|
|
≥70 | – | – | 1.757
(1.134–2.724) |
0.012 |
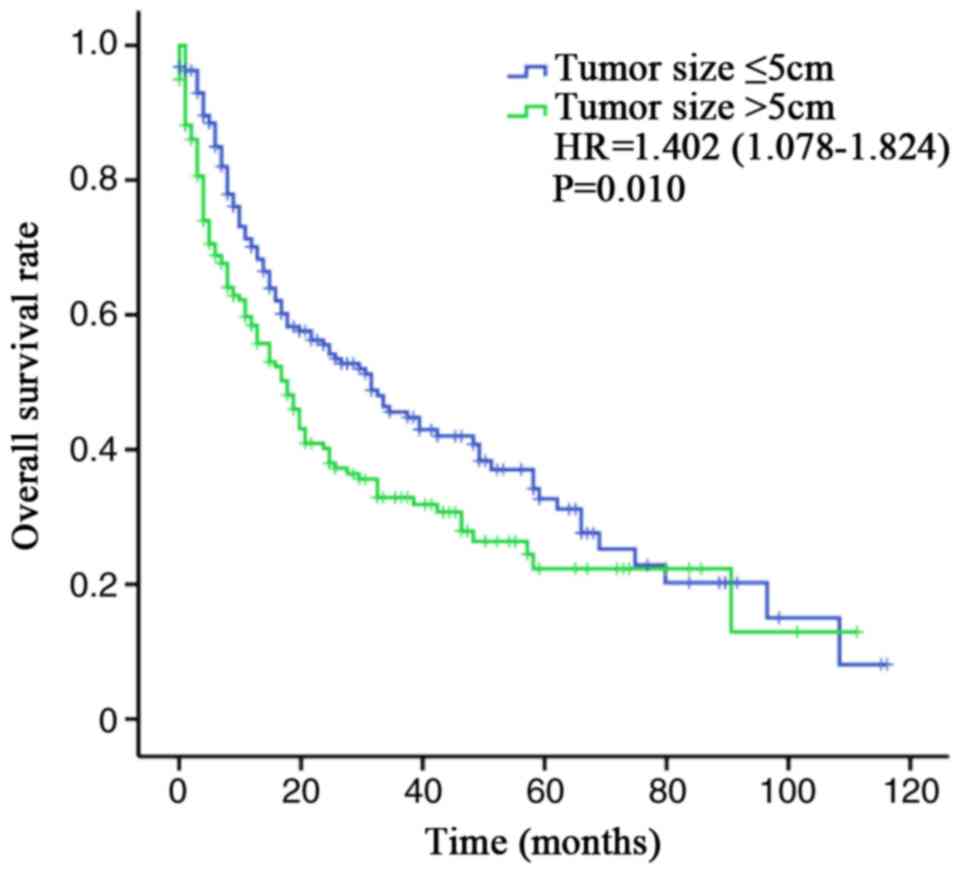
According to the current AJCC TNM staging system,
patients with stage IA had a significantly longer survival time
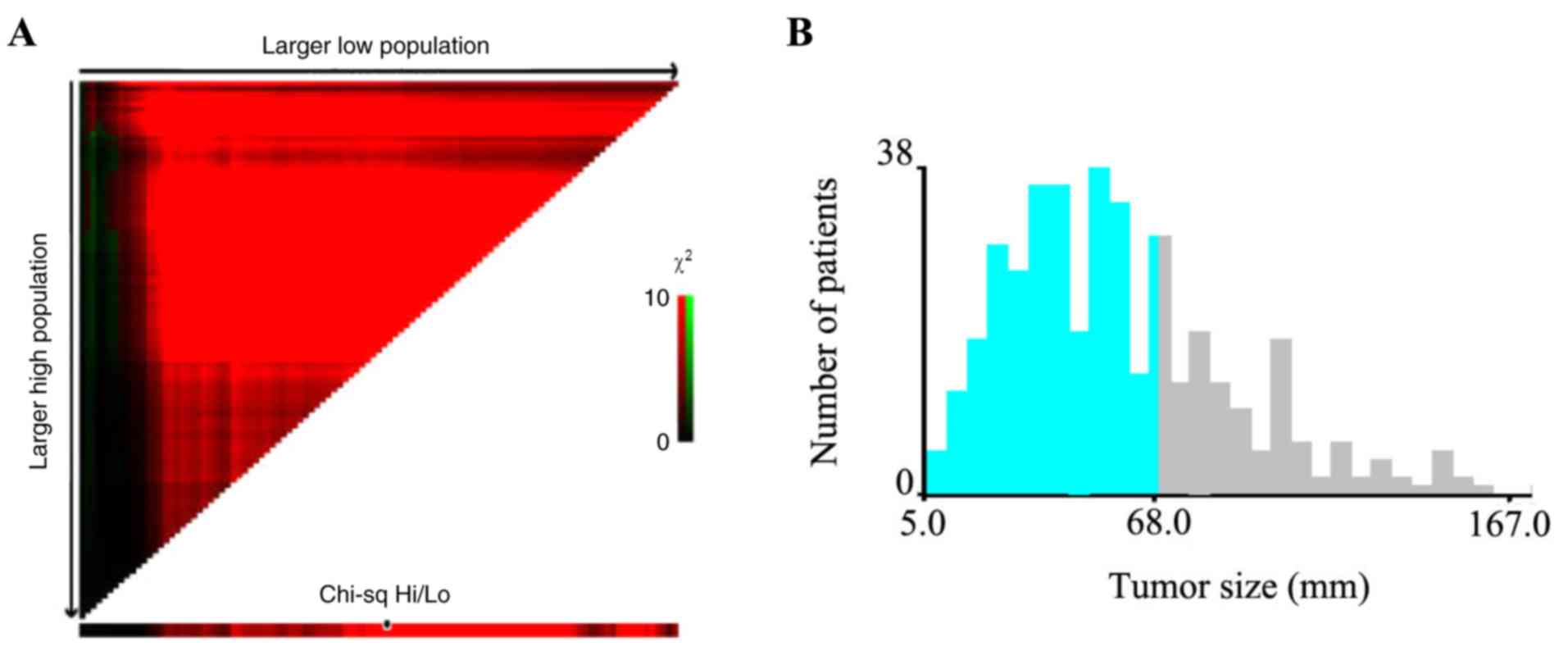
compared with that in patients with stage IB (Fig. 1; P=0.010). X-tile software was used
to investigate the association between tumor size and risk of
mortality (Fig. 2A and B). The plots
are created by dividing tumor size into two populations, randomly:
low and high. All possible cut-off points were assessed. The
brightest pixel (indicated by the black/white circle on the
χ2 high/low axis) denotes the optimal cut-off point. As
a result, the optimal cut-off value of tumor size was shown to be
6.8 cm. Thus 7 cm was used as an integer divider to redefine the
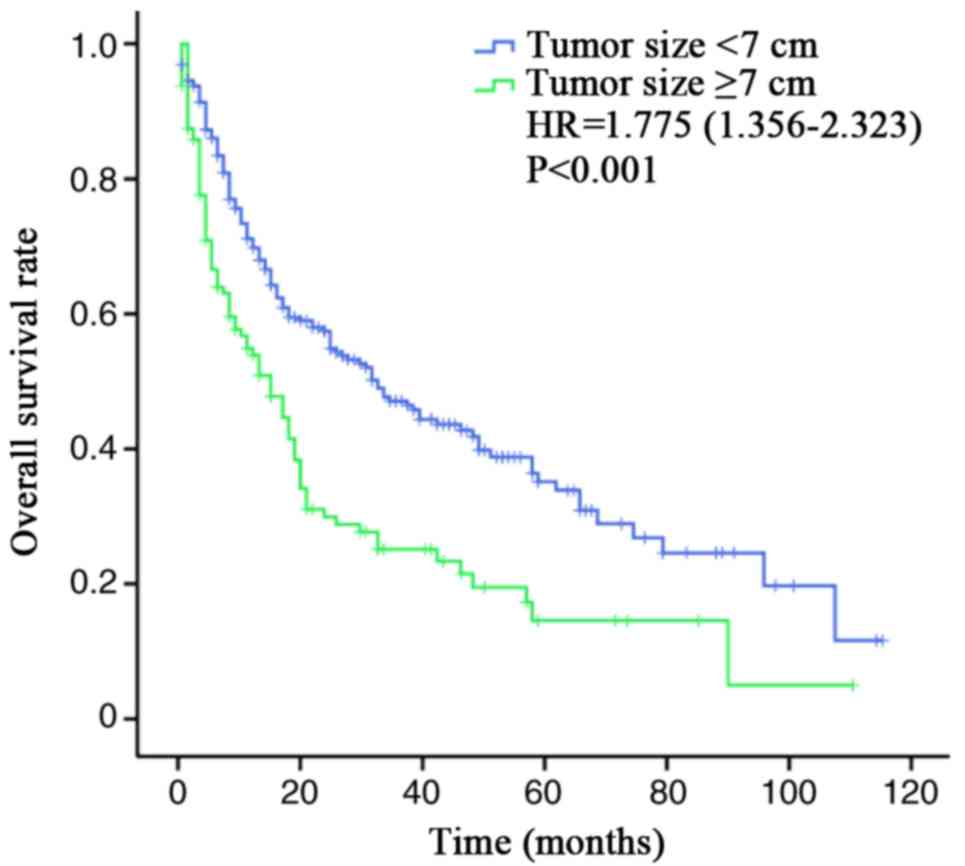
subclassifications of T1 (T1a, <7 cm; T1b, ≥7cm). The survival
curves of modified stage IA and IB are presented in Fig. 3 (P<0.001). Tumor size with a
cut-off value of 7 cm could better stratify patients by risk
compared with 5 cm (7 cm, HR, 1.775; 95% CI, 1.356–2.323; 5 cm, HR,
1.402; 95% CI, 1.078–1.824).
Discussion
ICC is a relatively uncommon cancer; however, some
patients miss their interventional operative opportunity due to
delayed diagnosis (12). The present
study demonstrated that the proportion of patients with stage IA
receiving operations was much higher than those with stage IB (64.3
vs. 49.0%), indicating that tumor size was a prominent factor in
decisions about surgical treatment. Besides surgery, the other
common prognostic factor for both stage IA and IB was age, which
was in agreement with many previous studies (13–16). Age
was significantly associated with OS time (Table III).
Notably, poor tumor differentiation has also been
considered to be a risk factor for ICC in several studies with
large sample sizes (16–18). Spolverato et al (8) identified that the incidence of poor
tumor differentiation was significantly higher in large tumors
(<3 cm, 9.7%; 3–5 cm, 19.8%; 5–7 cm, 24.2%; 7–15 cm, 21.1%;
>15 cm, 31.6%), which was similar to the present results
(Table I). The present study
indicated that grade was not an independent prognostic factor for
patients with stage IA (P=0.284; Table
III). However, grade was nearly an independent prognostic
factor for patients with stage IB (P=0.05; Table III). This is likely explained by
the high proportion of patients with stage IA receiving surgery,
resulting in better outcomes, regardless of the degree of tumor
differentiation.
Survival outcomes were significantly different
between stage IA and IB, suggesting the sub-classification of stage
I by tumor size is necessary. The present findings demonstrated the
most appropriate cut-off value for tumor size is 7 cm rather than 5
cm. In a large, multi-institutional study, Hyder et al
(19) also reported that the impact
of tumor size on the risk of mortality plateaued at a threshold
value of 7 cm in patients with resectable ICC. These findings
suggested that the optimal size cut-off value of the T1 category in
the 8th edition of AJCC staging system was worth considering to
better predict the outcomes of patients with ICC.
It should be noted that the present study was
limited by using retrospective clinical data. For this reason, the
optimal cut off value of 7 cm should be validated by external data
and therefore more prospective studies should be performed in a
larger cohort of patients with ICC in future research. A total of
129 cases with unknown grade information were excluded in the
univariate and multivariate Cox regression analysis, which may
impact the results to some extent. Additionally, the SEER database
does not include genetic information of tumors. Therefore, the
potential mechanism of large tumor size leading to poor prognosis
remains to be elucidated through further basic laboratory
research.
Acknowledgements
Not applicable.
Funding
The present study was supported by the Tianjin
Municipal Health Bureau of Science and Technology Fund Projects
(grant no. 2015KZ034).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the SEER database (https://seer.cancer.gov/).
Authors' contributions
FD and YL designed the research and critically
revised the manuscript for important intellectual content. CT and
BZ carried out administrative support and performed the collection,
assembly and interpretation of data. All authors performed the
research, analyzed the data and wrote the paper.
Ethics approval and consent to
participate
This study was approved by the institutional review
board of Gansu Provincial Hospital, China.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ikai I, Arii S, Okazaki M, Okita K, Omata
M, Kojiro M, Takayasu K, Nakanuma Y, Makuuchi M, Matsuyama Y, et
al: Report of the 17th Nationwide Follow-up Survey of Primary Liver
Cancer in Japan. Hepatol Res. 37:676–691. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Hu J, Chen FY, Zhou KQ, Zhou C, Cao Y, Sun
HC, Fan J, Zhou J and Wang Z: Intrahepatic cholangiocarcinoma
patients without indications of lymph node metastasis not benefit
from lymph node dissection. Oncotarget. 8:113817–113827. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Aljiffry M, Abdulelah A, Walsh M,
Peltekian K, Alwayn I and Molinari M: Evidence-based approach to
cholangiocarcinoma: A systematic review of the current literature.
J Am Coll Surg. 208:134–147. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Poultsides GA, Zhu AX, Choti MA and Pawlik
TM: Intrahepatic cholangiocarcinoma. Surg Clin North Am.
90:817–837. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lin XH and Luo JC: The risk factors and
prognostic factors of intrahepatic cholangiocarcinoma. J Chin Med
Assoc. 80:121–122. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Amin MB, Greene FL, Edge SB, Compton CC,
Gershenwald JE, Brookland RK, Meyer L, Gress DM, Byrd DR and
Winchester DP: The Eighth Edition AJCC Cancer Staging Manual:
Continuing to build a bridge from a population-based to a more
‘personalized’ approach to cancer staging. CA Cancer J Clin.
67:93–99. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Yamashita YI, Shirabe K, Beppu T, Eguchi
S, Nanashima A, Ohta M, Ueno S, Kondo K, Kitahara K, Shiraishi M,
et al: Surgical management of recurrent intrahepatic
cholangiocarcinoma: predictors, adjuvant chemotherapy, and surgical
therapy for recurrence: A multi-institutional study by the Kyushu
Study Group of Liver Surgery. Ann Gastroenterol Surg. 1:136–142.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Spolverato G, Ejaz A, Kim Y, Sotiropoulos
GC, Pau A, Alexandrescu S, Marques H, Pulitano C, Barroso E, Clary
BM, et al: Tumor size predicts vascular invasion and histologic
grade among patients undergoing resection of intrahepatic
cholangiocarcinoma. J Gastrointest Surg. 18:1284–1291. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Fritz A, Percy C, Jack A, Shanmugaratnam
K, Sobin L and Parkin DM: International classification of diseases
for oncology (ICD-O)3ed. Geneva: World Health Organization;
2013
|
|
10
|
Lee AJ and Chun YS: Intrahepatic
cholangiocarcinoma: The AJCC/UICC 8th edition updates. Chin Clin
Oncol. 7:522018. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Camp RL, Dolled-Filhart M and Rimm DL:
X-tile: A new bio-informatics tool for biomarker assessment and
outcome-based cut-point optimization. Clin Cancer Res.
10:7252–7259. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kim Y, Moris DP, Zhang XF, Bagante F,
Spolverato G, Schmidt C, Dilhoff M and Pawlik TM: Evaluation of the
8th edition American Joint Commission on Cancer (AJCC) staging
system for patients with intrahepatic cholangiocarcinoma: A
surveillance, epidemiology, and end results (SEER) analysis. J Surg
Oncol. 116:643–650. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Wang Y, Li J, Xia Y, Gong R, Wang K, Yan
Z, Wan X, Liu G, Wu D, Shi L, et al: Prognostic nomogram for
intrahepatic cholangiocarcinoma after partial hepatectomy. J Clin
Oncol. 31:1188–1195. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Clark CJ, Wood-Wentz CM, Reid-Lombardo KM,
Kendrick ML, Huebner M and Que FG: Lymphadenectomy in the staging
and treatment of intrahepatic cholangiocarcinoma: A
population-based study using the National Cancer Institute SEER
database. HPB (Oxford). 13:612–620. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Bunsiripaiboon P, Sornmayura P,
Wilasrusmee C and Lertsithichai P: The prognostic significance of
microvessel density in intrahepatic cholangiocarcinoma. J Med Assoc
Thai. 93:66–72. 2010.PubMed/NCBI
|
|
16
|
Tamandl D, Herberger B, Gruenberger B,
Puhalla H, Klinger M and Gruenberger T: Influence of hepatic
resection margin on recurrence and survival in intrahepatic
cholangiocarcinoma. Ann Surg Oncol. 15:2787–2794. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Ribero D, Pinna AD, Guglielmi A, Ponti A,
Nuzzo G, Giulini SM, Aldrighetti L, Calise F, Gerunda GE, Tomatis
M, et al: Surgical approach for long-term survival of patients with
intrahepatic cholangiocarcinoma: A multi-institutional analysis of
434 patients. Arch Surg. 147:1107–1113. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Fisher SB, Patel SH, Kooby DA, Weber S,
Bloomston M, Cho C, Hatzaras I, Schmidt C, Winslow E, Staley CA
III, et al: Lymphovascular and perineural invasion as selection
criteria for adjuvant therapy in intrahepatic cholangiocarcinoma: A
multi-institution analysis. HPB (Oxford). 14:514–522. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Hyder O, Marques H, Pulitano C, Marsh JW,
Alexandrescu S, Bauer TW, Gamblin TC, Sotiropoulos GC, Paul A,
Barroso E, et al: A nomogram to predict long-term survival after
resection for intrahepatic cholangiocarcinoma: An Eastern and
Western experience. JAMA Surg. 149:432–438. 2014. View Article : Google Scholar : PubMed/NCBI
|