Introduction
In immune cell infiltration in breast cancer tissue,
the expression of tumour-related immune cells differed greatly
among different breast cancer subtypes and patients (1). Lymphocyte-predominant breast cancer
(LPBC) is defined as a presentation wherein at least 50% of the
tumour tissue is invaded by tumour-infiltrating lymphocytes (TILs).
LPBC was observed in 20% of triple-negative breast cancers, 16% of
HER2-positive tumours and 6% of the hormonal receptor (HR)-positive
tumours (1). Since the 1970s, studies
have attempted to understand the basic function of TILs in cancer
as immune response in cancer tissue has been driven by the specific
functions of TILs (2). Moreover, the
variety of immune cells is believed to contribute to drug
sensitivity and prognosis in breast cancer patients. In 2006, Galon
et al were the first to report that in situ TIL
expression could serve as a strong prognostic marker for colorectal
and breast cancer (3). Thereafter,
many retrospective studies reported that TIL expression in breast
cancer could predict the efficacy of drug therapy and prognosis
(4–9).
Although the methods to quantify TIL expression and cut-off TIL
values in breast cancer tissues varied among studies and have not
been clearly standardised, the International Working Group of TILs
published the first guidelines for a TIL evaluation in 2014
(10). Accordingly, mononuclear
immune cells located between tumour nests, i.e., within the tumour
stroma, are defined as stromal TILs (str-TILs). The International
TILs Working Group recommended that str-TIL expression should be
graded as low (str-TILs: <10%), intermediate (str-TILs: ≥10 and
≤40%) and high (str-TILs: >40%) based on their relative
abundance within the tumour stroma. However, there is no sufficient
evidence to support the efficacy of this classification. In the
present study, we evaluated the relationship of TIL grades with
clinicopathological characteristics of breast cancer patients and
prognosis based on the guidelines of the International TILs Working
Group.
Patients and methods
Patient background
A total of 294 consecutive female patients,
diagnosed as invasive breast cancer who underwent breast-conserving
surgery or modified radical mastectomy without neoadjuvant
treatment at Saitama Cancer Centre between January 2000 and
December 2001, were enrolled in this retrospective study. After the
evaluation of intrinsic subtypes, patients with bilateral breast
cancer were excluded from the study. Clinicopathological data on
pathological tumour size, the status of pathological lymph node
metastasis and clinical course were extracted from the patient
medical records. This study was conducted in accordance with the
Declaration of Helsinki and after the approval by the Institutional
Review Board of the Saitama Cancer Centre (nos. 231, 483 and 534).
All patients enrolled provided written comprehensive informed
consent.
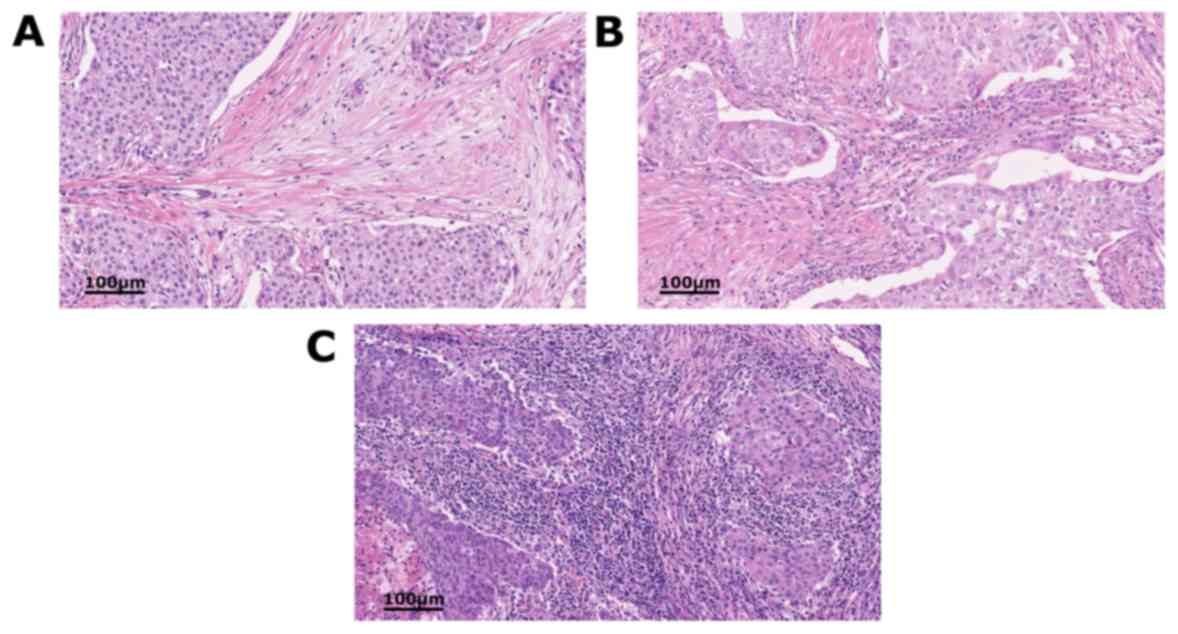
Evaluation of str-TILs
Surgical specimens were fixed in buffered formalin
solution, cut to 4-µm-thick slices and stained with haematoxylin
and eosin. Using an optical microscope with ×200 and ×400
magnification, a surgical pathologist specialising in breast
pathology (MK) quantified str-TILs. Str-TIL expression was
classified into the following three grades per the International
TILs Working Group (10) criteria:
Low (str-TILs: <10%), intermediate (str-TILs: ≥10 and ≤40%) and
high (str-TILs: >40%; Fig.
1A-C).
Procedures and evaluation of the
expression of oestrogen receptor (ER), progesterone receptor and
HER2
The following antibodies were used for
immunostaining: 1D5 (Dako, Glostrup, Denmark) for ER, PgR636 (Dako)
for progesterone receptor (PgR) and Hercep Test (Dako) for HER2.
For evaluation of HER2 gene amplification, dual in situ
hybridisation (DISH) was performed with INFORM HER2 Dual ISH DNA
Probe Cocktail assay (Ventana Medical Systems, Inc., Tuscon, AZ,
USA). ER, PgR and HER2 expression were evaluated in accordance with
the American Society of Clinical Oncology and College of American
Pathologists (11,12) criteria. In addition, the degree of ER
and PgR staining ≥1% and the specimen was determined as positive.
The proportional scores of cells membrane HER2 staining intensity
were as follows: scores 0, 1+, 2+ and 3+. HER2 immunostaining with
a score of 2+ was subjected to a DISH assay to assess the gene
amplification of HER2. A HER2 score of 2+/DISH positive or 3+ was
defined as HER2-positive cancer. Patients with ER-positive and/or
PgR-positive breast cancer were defined as a hormonal receptor
(HR)-positive breast cancer.
Statistical analysis
The relationship between TIL grades and various
clinicopathological factors, including ER, PgR and HER2 expression
was analysed by Chi-square and Fisher's exact tests. The log-rank
test and Kaplan-Meier method were used to estimate relapse-free
survival (RFS) and cancer-specific survival (CSS). RFS was defined
as the length of time from the day of surgery to any tumour
recurrence (including locoregional recurrence). CSS was defined as
the period from the day of surgery until the time of death caused
by the progression of breast cancer. In the multivariate analysis,
95% confidence intervals for the relationship between TIL grades
and clinicopathological factors were obtained using a logistic
regression test. The relationship between TIL grades and prognosis
were obtained using a Cox proportional hazards regression model.
Statistical analyses were performed using the SPSS v22.0 software
(IBM Corp., Armonk, NY, USA). P<0.05 was considered to indicate
a statistically significant difference.
Results
Patient and tumour
characteristics
The median age of the 294 patients enrolled in the
study was 55 years (age range, 25–87 years). Of these patients, 171
(58.2%) were in postmenopausal state, 134 (45.6%) had positive
pathological nodes (pN), 162 (55.1%) had a histological grade 3
tumour, 213 (72.4%) had HR-positive breast cancer, 176 (59.8%)
underwent adjuvant endocrine therapy, 158 (53.7%) underwent
adjuvant chemotherapy and 47 (16.0%) were diagnosed with
HER2-positive breast cancer (Table
I). There were no patients with HER2-positive who received
adjuvant trastuzumab therapy since adjuvant trastuzumab
administration had not been approved in Japan before 2008.
 | Table I.Patient characteristics. |
Table I.
Patient characteristics.
| Characteristics | Total |
|---|
| Age, years |
|
|
<40 | 26 |
| ≥40 and
<60 | 158 |
| ≥60 | 110 |
| Menopause status |
|
| Pre- | 123 |
|
Post- | 171 |
| Type of breast
surgery |
|
|
Breast-conserving surgery | 227 |
|
Mastectomy | 67 |
| Axillary
surgery |
|
|
Sentinel lymph node (biopsy
alone) | 149 |
|
Axillary lymph node
(dissection) | 142 |
| No
surgery | 4 |
| Pathological tumour
size |
|
|
pT1 | 152 |
|
pT2 | 116 |
|
pT3 | 17 |
|
pT4 | 9 |
| Pathological nodal
status |
|
|
pN0 | 156 |
|
pN1 | 78 |
|
pN2 | 34 |
|
pN3 | 22 |
| No
surgery | 4 |
| Pathological TNM
stage |
|
| I | 98 |
|
IIA | 96 |
|
IIB | 35 |
|
IIIA | 30 |
|
IIIB | 9 |
|
IIIC | 22 |
| Not
evaluated | 4 |
| Histological
grade |
|
| Grade
1 | 45 |
| Grade
2 | 87 |
| Grade
3 | 162 |
| Oestrogen
receptor |
|
|
Positive | 207 |
|
Negative | 87 |
| Progesterone
receptor |
|
|
Positive | 179 |
|
Negative | 115 |
| HER2 status |
|
|
Positive | 47 |
|
Negative | 247 |
Relationship between TIL expression
and clinicopathological characteristics
Of the patients assessed, 32 (10.9%), 44 (15.0%) and
218 (74.1%) patients have high, intermediate and low TIL
expression, respectively. In both the HER2-negative and
HER2-positive patients, only 3.3% had high TIL expression. In the
HR-negative group, 30.9% had high TIL expression (Table II). The rate of high TIL expression
was significantly higher in the HR-negative group than in the
HR-positive group (P<0.001). A univariate analysis identified
that the ER (P<0.001), PgR (P<0.001) and HER2 (P=0.004)
status and histological grade (P<0.001) were significant
(Table III). High TIL expression
was significantly associated with ER-negative, PgR-negative,
HER2-positive and histological grade 3 tumours. On the other hand,
multivariate analysis confirmed that TIL expression was
significantly higher in patients with ER-negative (P<0.001) and
histological grade 3 (P=0.03) tumours (Table III).
| Table II.Patient distribution by TIL grades in
each breast cancer subtype. |
Table II.
Patient distribution by TIL grades in
each breast cancer subtype.
|
| Patients, no.
(%) |
|
|---|
|
|
|
|
|---|
| Subtype | High TIL group | Intermediate TIL
group | Low TIL group | Total |
|---|
| HR+/HER2- | 6 (3.1) | 24 (12.2) | 166 (84.7) | 196 |
| HR+/HER2+ | 1 (5.9) | 5 (29.4) | 11 (64.7) | 17 |
| HR-/HER2+ | 9 (30.0) | 6 (20.0) | 15 (50.0) | 30 |
| HR-/HER2- | 16 (31.4) | 9 (17.6) | 26 (50.9) | 51 |
| Total | 32 (10.9) | 44 (15.0) | 218 (74.1) | 294 |
| Table III.The association between TIL grades
and clinicopathological characteristics. |
Table III.
The association between TIL grades
and clinicopathological characteristics.
|
| Patients, no. | Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|
|---|
| Clinicopathological
factor | Low TIL group | Intermediate TIL
group | High TIL group | P-value | P-value |
|---|
| ER status |
|
|
| <0.001 | <0.001 |
|
Positive | 175 | 27 | 5 |
|
|
|
Negative | 43 | 17 | 27 |
|
|
| PgR status |
|
|
| <0.001 | 0.31 |
|
Positive | 148 | 26 | 5 |
|
|
|
Negative | 70 | 18 | 27 |
|
|
| HER2 status |
|
|
| 0.004 | 0.61 |
|
Positive | 26 | 11 | 10 |
|
|
|
Negative | 192 | 33 | 22 |
|
|
| Tumour size |
|
|
| 0.16 |
|
|
T1-2 | 191 | 38 | 24 |
|
|
|
T3-4 | 27 | 6 | 8 |
|
|
| Nodal status |
|
|
| 0.14 |
|
|
Negative | 117 | 19 | 12 |
|
|
|
Positive | 101 | 25 | 20 |
|
|
| Menopausal
status |
|
|
| 0.31 |
|
|
Pre- | 87 | 23 | 13 |
|
|
|
Post- | 131 | 21 | 19 |
|
|
| Histological
grade |
|
|
| <0.001 | 0.03 |
|
1-2 | 116 | 11 | 5 |
|
|
| 3 | 102 | 33 | 27 |
|
|
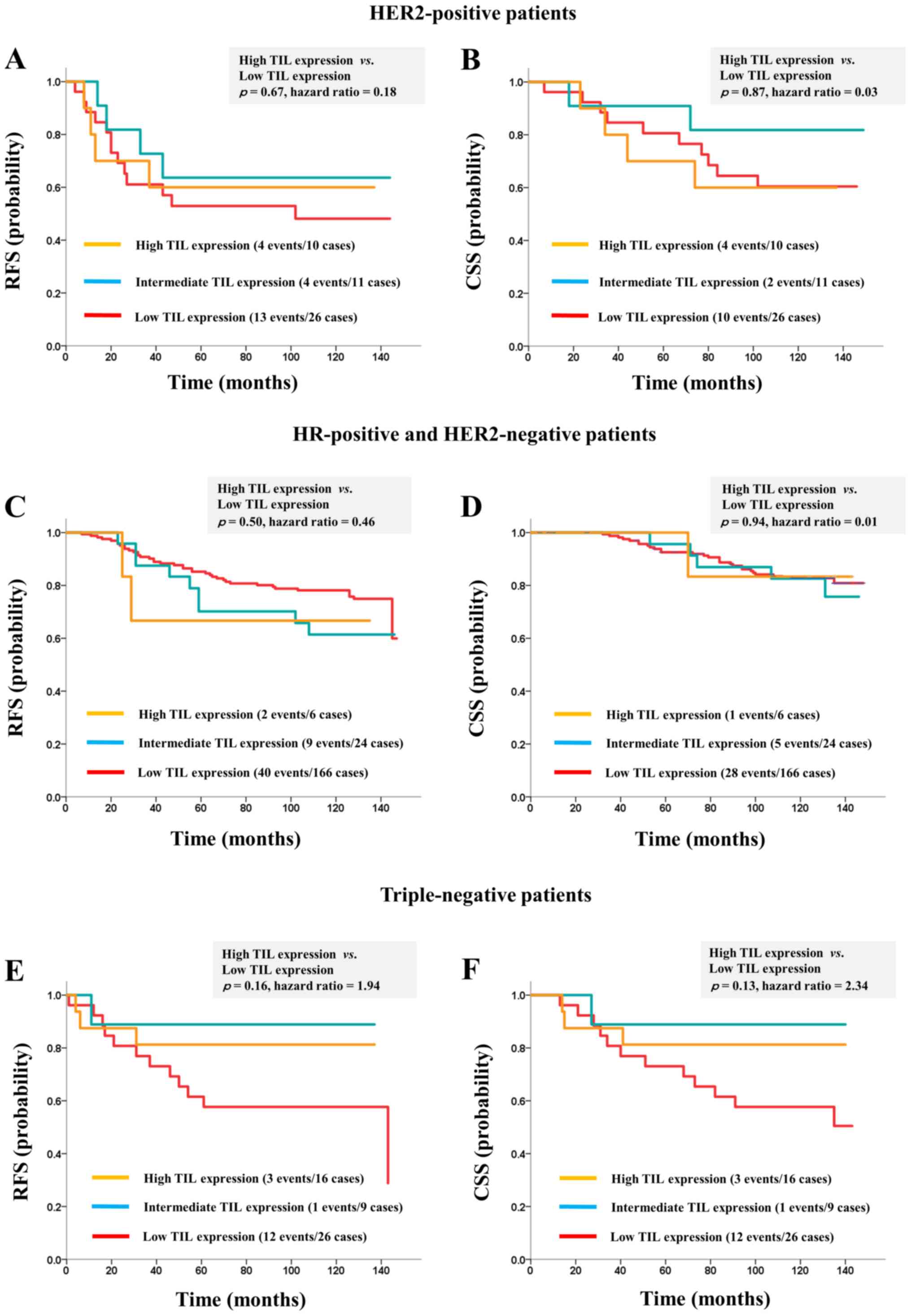
Prognostic significance of TIL
expression
The analysis identified that the median of RFS was
127 (range, 1–147 months), and median of CSS was 130 (range, 4–149
months). TIL expression was not a significant prognostic factor
when the analysis included the entire study cohort of breast cancer
patients. Multivariate analysis confirmed that high TIL expression
was not an independent prognostic marker (Table IV). TIL expression was not a
significant prognostic marker in the HER2-positive breast cancer
patient (RFS, P=0.67; CSS, P=0.87; Fig.
2A and B). Additionally, in the HR-positive and HER2-negative
breast cancer patients, no significant difference in survival was
recognised between the high- and low-grade TIL patients (RFS,
P=0.50; CSS, P=0.94; Fig. 2C and D).
Among the triple-negative breast cancer patients, the RFS and CSS
were higher in the high-grade TIL group compared with the low-TIL
group, although the difference was not significant (RFS, P=0.16;
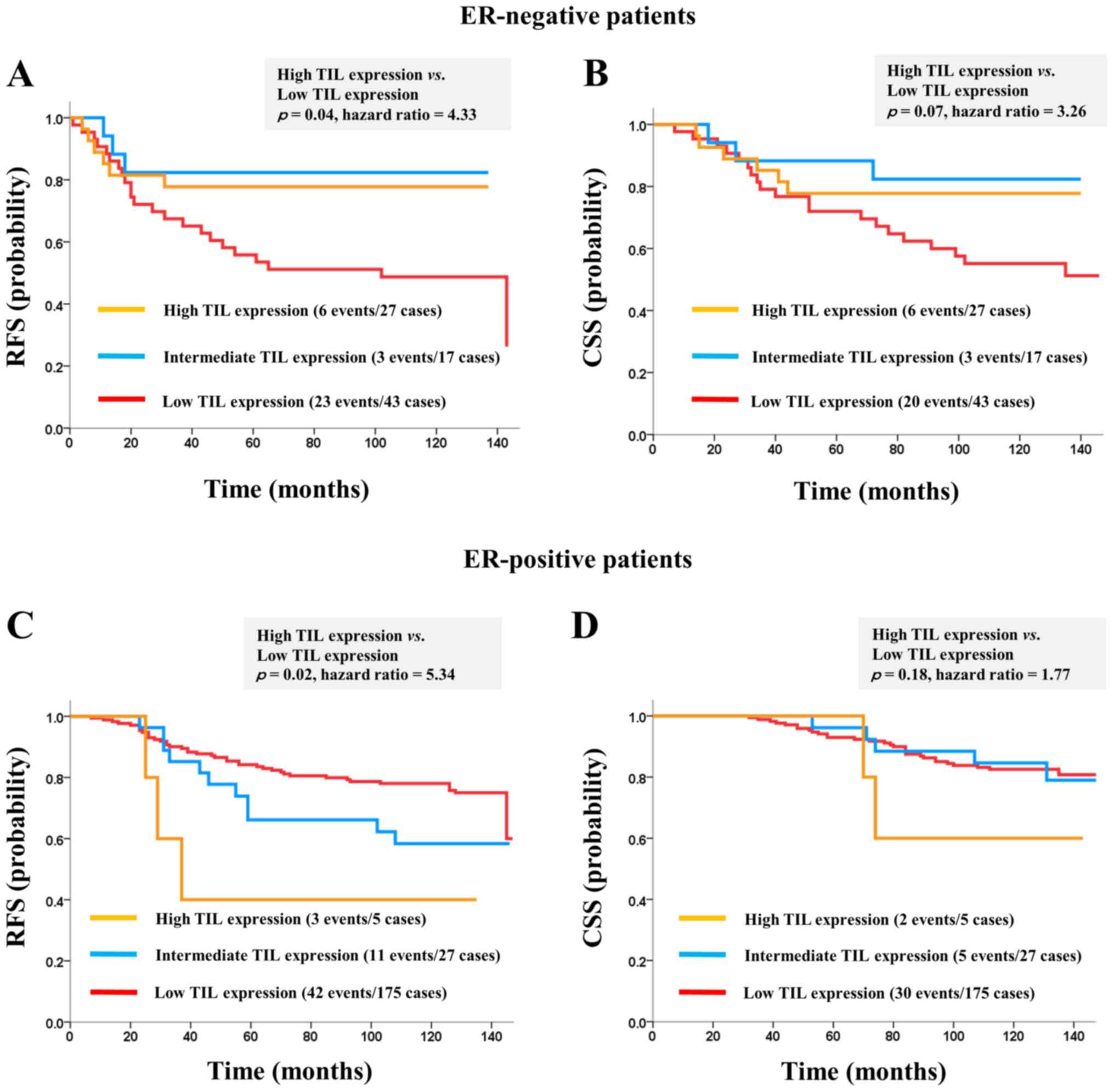
CSS, P=0.13; Fig. 2E and F). By
contrast, among the ER-negative breast cancer patients, the RFS was
significantly higher in the high-grade TIL group than in the
low-grade TIL group (RFS, P=0.04; CSS, P=0.07; Fig. 3A and B). Conversely, among the
ER-positive breast cancer patients, the RFS was significantly
higher in the low-grade TIL group than in the high-grade TIL group
with nonsignificant difference in the CSS (RFS, P=0.02; CSS,
P=0.18; Fig. 3C and D).
| Table IV.Results of univariate and
multivariate survival analyses on the influence of
clinicopathological variables, including the expression of
TILs. |
Table IV.
Results of univariate and
multivariate survival analyses on the influence of
clinicopathological variables, including the expression of
TILs.
| A, RFS |
|---|
|
|---|
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Clinicopathological
factor | Hazard ratio | P-value | Hazard ratio | 95% CI | P-value |
|---|
| TIL expression |
|
Low | Reference |
| Reference |
|
|
Intermediate | 0.050 | 0.82 | 0.88 | 0.49–1.61 | 0.69 |
|
High | 0.017 | 0.90 | 0.61 | 0.28–1.30 | 0.20 |
| ER status |
|
Positive | Reference |
| Reference |
|
|
Negative | 4.68 | 0.03 | 1.05 | 0.55–2.02 | 0.88 |
| PgR status |
|
Positive | Reference |
| Reference |
|
|
Negative | 8.01 | 0.005 | 1.68 | 0.92–3.07 | 0.09 |
| HER2 status |
|
Negative | Reference |
| Reference |
|
|
Positive | 9.49 | 0.002 | 1.52 | 0.88–2.61 | 0.13 |
| Tumour size |
| T
1–2 | Reference |
| Reference |
|
| T
3–4 | 15.13 | <0.001 | 1.79 | 0.99–3.23 | 0.05 |
| Nodal status |
|
Negative | Reference |
| Reference |
|
|
Positive | 29.80 | <0.001 | 3.04 | 1.88–4.92 | <0.001 |
| Histological
grade |
| Grade
1–2 | Reference |
| Reference |
|
| Grade
3 | 5.80 | 0.02 | 1.19 | 0.71–2.00 | 0.51 |
|
| B, CSS |
|
|
| Univariate
analysis | Multivariate
analysis |
|
|
|
|
|
Clinicopathological factor | Hazard
ratio | P-value | Hazard
ratio | 95% CI | P-value |
|
| TIL expression |
|
High | Reference |
| Reference |
|
|
Intermediate | 0.60 | 0.44 | 0.56 | 0.26–1.21 | 0.14 |
|
Low | 0.11 | 0.74 | 0.54 | 0.24–1.22 | 0.14 |
| ER status |
|
Positive | Reference |
| Reference |
|
|
Negative | 9.93 | 0.002 | 1.51 | 0.72–3.16 | 0.28 |
| PgR status |
|
Positive | Reference |
| Reference |
|
|
Negative | 11.28 | <0.001 | 1.60 | 0.78–3.29 | 0.20 |
| HER2 status |
|
Negative | Reference |
| Reference |
|
|
Positive | 4.84 | 0.03 | 1.09 | 0.59–2.02 | 0.79 |
| Tumour size |
|
T1-2 | Reference |
| Reference |
|
|
T3-4 | 11.51 | 0.001 | 1.95 | 1.00–3.81 | 0.05 |
| Nodal status |
|
Negative | Reference |
| Reference |
|
|
Positive | 17.93 | <0.001 | 2.60 | 1.49–4.52 | <0.001 |
| Histological
grade |
| Grade
1–2 | Reference |
| Reference |
|
| Grade
3 | 9.06 | 0.003 | 1.56 | 0.85–2.87 | 0.15 |
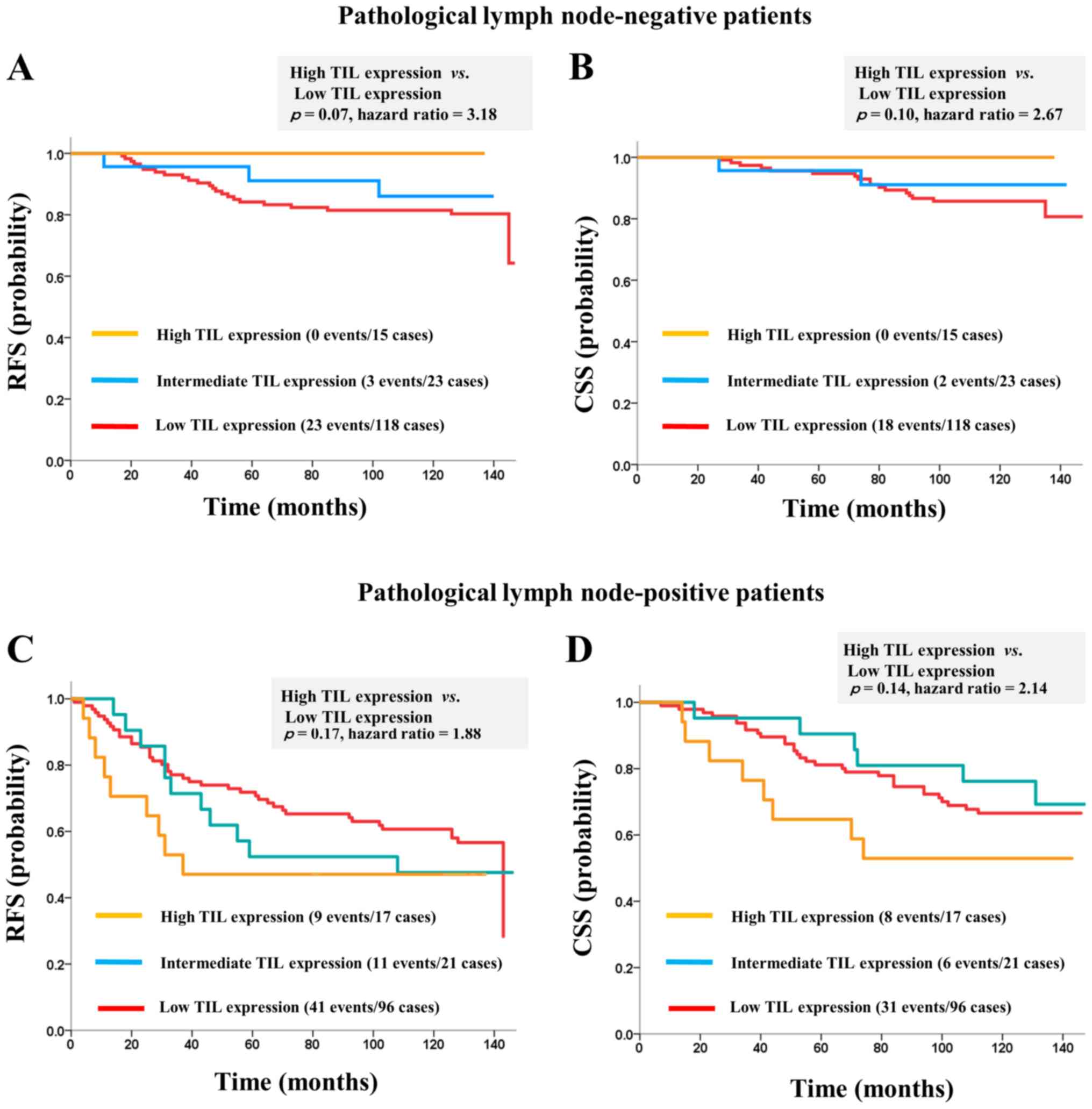
Among the pN-negative patients, none of the cases
with a high TIL score had recurrence. Moreover, the RFS and the CCS
tended to be higher in the high-grade TIL group than in the
low-grade TIL group (RFS, P=0.07; CSS, P=0.10; Fig. 4A and B). However, TIL expression was
not a prognostic indicator in the pN-positive patients (RFS,
P=0.17; CSS, P=0.14; Fig. 4C and D).
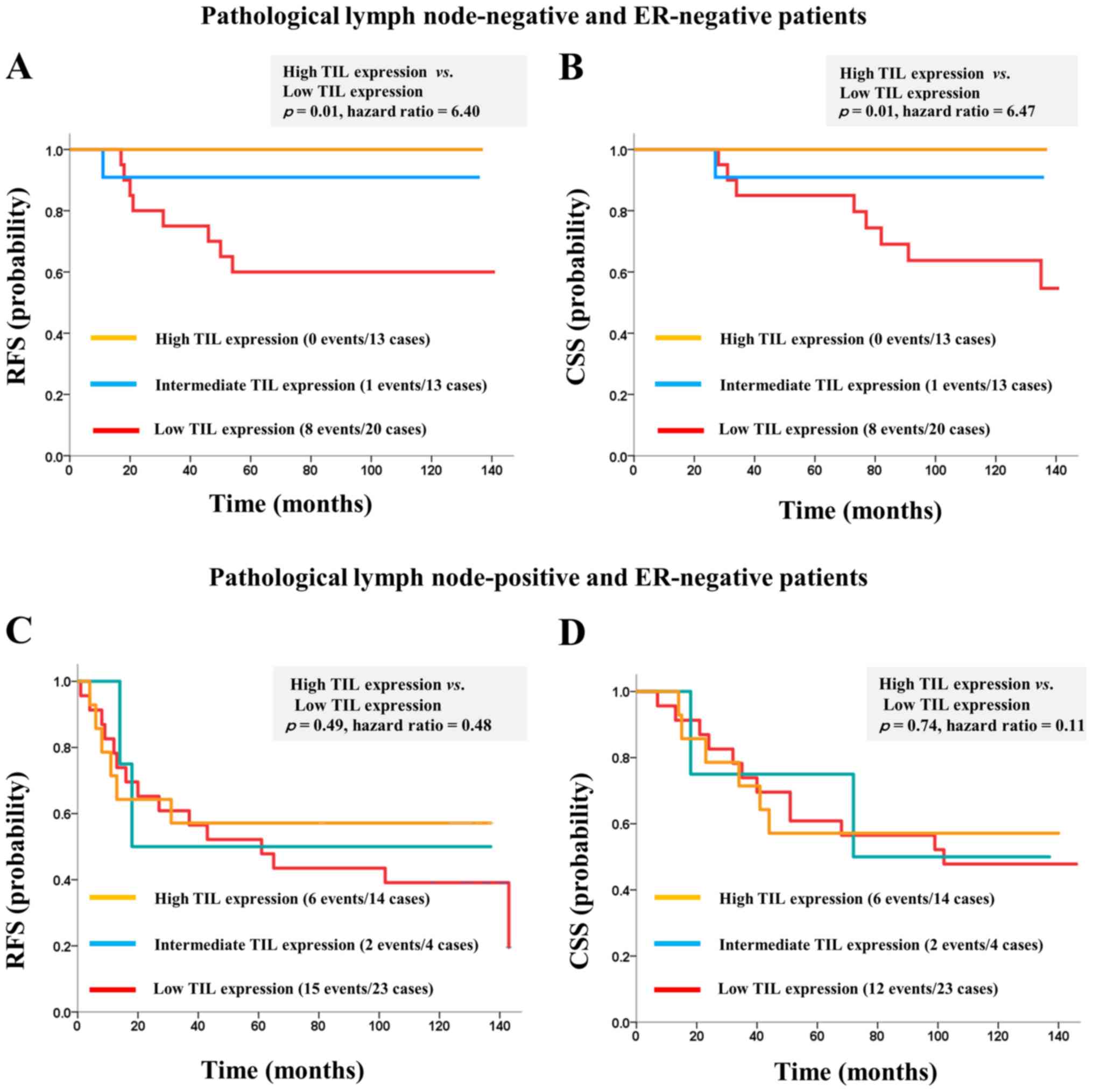
Among the ER-negative and pN-negative patients, the RFS and CCS
were significantly higher in the high-grade TIL group than in the
low-grade TIL group (RFS, P=0.01; CSS, P=0.01; Fig. 5A and B). Conversely, TIL expression
was not recognised as a prognostic factor in ER-negative and
pN-positive patients (RFS, P=0.49; CSS, P=0.74; Fig. 5C and D).
Discussion
It has been revealed that patients with invasive
breast cancer and high TIL expression, those with ER-negative and
high histological grade tumours were significantly more common.
Moreover, TIL expression level was a strong prognostic marker for
ER-negative breast cancer. Among different breast cancer subtypes,
ER-negative breast cancer and a subtype with high-grade malignancy
exhibit extremely high growth potential. In the Breast
International Group (BIG) 2–98 trial, Loi et al reported
that TIL expression was a prognostic marker for ER-negative
patients, especially those with triple-negative breast cancer
(13). Adams et al (14) demonstrated that TIL expression was a
strong prognostic marker for triple-negative breast cancer in the
Eastern Cooperative Oncology Group (ECOG) 2197 and ECOG 1199
trials. Loi et al (15)
conducted an meta-analysis of the efficacy of TIL expression as a
prognostic marker in triple-negative breast cancer patients
enrolled in large-scale trials, such as these trials and the
Finland Herceptin Trial (FinHER) (16) and reported that TIL expression was a
prognostic factor in triple-negative breast cancer. Therefore, most
of the studies that showed the efficacy of TIL expression, as a
predictor of prognosis and drug efficacy, were retrospective. We
believe that a prospective clinical trial is necessary to clarify
the real utility of TIL expression as a prognostic marker.
We found that survival was significantly higher in
the low-grade TIL group than in the high-grade TIL group among
ER-positive breast cancer patients. Recent studies on large cohorts
reported that high TIL expression was a poor prognostic factor in
ER-positive breast cancer (17).
Consistent with these studies, morphological TIL heterogeneity is
frequent in ER-positive patients compared with ER-negative patients
(18). It is possible that this
intra-tumour heterogeneity may affect the expression patterns of
immune cells, thereby underlying the difference in the prognostic
significance of TIL expression between ER-positive and ER-negative
breast cancer patient. To ascertain different roles associated with
various TIL types, immunohistochemical analysis of TILs is
necessary to determine the distribution of immune cells (19). In addition, the tumour mutational
burden is associated with tumour immunity (20) and a high level of the mutational load
is associated with poor outcomes in patients with ER-positive
tumours (21,22). ER is considered to play an important
role in tumour immunosuppression (23) as treatment options for ER-positive and
ER-negative breast cancer are distinct. Several clinical studies
demonstrated an association between TIL expression and response to
chemotherapy (19). Endocrine therapy
may modulate immune microenvironment of primary tumours (24); however, relationship of TILs with the
response to endocrine therapy in ER-positive breast cancer remains
controversial. A grade of ER expression and therapeutic options may
affect the extent and the pattern of infiltrating immune cells in
the tumour tissue as TIL expression may contribute to different
prognostic rates between ER-positive and ER-negative breast
cancers. However, there is no clear evidence to support this
biological mechanism and the prognostic power of TILs in
ER-positive patients with the luminal A and B subtypes. Therefore,
further investigation is needed to determine the prognostic utility
of TIL expression in ER-positive breast cancer.
It is noted that TIL expression was not a prognostic
marker in pN-positive patients. However, among pN-negative
patients, the prognosis was better in the high-grade TIL group than
in the low-grade TIL group. Lymph node metastasis is an important
factor in determining the prognosis of breast cancer patients and
the mechanism underlying lymph node metastasis in breast cancer
involves various factors. Nonetheless, we propose that a reduced
ability of immune cells within the tumour microenvironment, which
inhibits cancer cell metastasis is responsible for lymph node
metastasis. Programmed cell death protein-1 (PD-1) contributes to
the coexistence of cancer cells and immune cells. Moreover,
programmed cell death-ligand 1 (PD-L1) inhibits killer T cell
activity (25). PD-1 and PD-L1
inhibitors suppress these immune checkpoints, thereby promoting
tumour immune response by killer T cells and exhibiting an
anti-tumour effect (26–31). Recent studies were conducted to
determine the mechanism by which these molecules interact with
cancer invasion and metastasis (32).
The expression levels of TILs and immune checkpoint markers in
ductal carcinoma in situ provide important information on
tumour microenvironment before breast cancer invasion and
metastasis. Hendry et al (33)
suggested that ductal carcinoma in situ progression into
invasive breast cancer has a reduced ability of immune cells in the
tumour microenvironment, which inhibits cancer cell invasion caused
by PD-1 and PD-L1 activation. Furthermore, Tarhini et al
(34) reported that PD-L1 expression
in melanoma tumour cells contributed to the degree of
micrometastasis and sentinel lymph nodes. However, there is still
no clear evidence to support whether immune checkpoint factors,
such as PD-1 and PD-L1, are involved in axillary lymph node
metastasis of breast cancer. Thus, further investigation is
required to determine the relationship between lymph node
metastasis and tumour immunity in breast cancer.
In conclusions, high TIL expression correlated with
negative ER and high histological grade. Among ER-negative
patients, survival rate was higher in the high-grade TIL group than
the low-grade TIL group. Moreover, TIL expression might be a potent
prognostic marker in ER-negative and pN-negative patients.
Conversely, among the ER-positive breast cancer patients, survival
rate was significantly better in the low-grade TIL group than in
the high-grade TIL group. Thus, the biological association of TILs
with primary breast tumour might differ between ER-positive and
ER-negative breast cancer. The current study revealed that the RFS
and the CSS of triple-negative patients tended to be higher in the
high-grade TIL group than in the low-grade TIL group without
statistical significance. This cause might be due to several
factors, which include differences in patient background (race,
residence, and familial history) and differences in TIL evaluation
method. The number of triple-negative patients was not large in
this study. As such, a further study to validate the prognostic
utility of TILs based on breast cancer subtypes in large Japanese
cohorts is required.
Acknowledgements
The present study was selected for the Young
Investigator Award, 2015 Annual meeting of Japan Surgical
Society.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analysed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
All authors participated in the study design. SK
mainly performed image acquisition and statistical analyses. MK
assisted SK in histological examinations and evaluating results.
KI, HM and MK assisted in the production of the study design and
evaluating the results obtained. TF, JH, KS, TO and HK contributed
toward the statistical evaluation of results and theoretical
organization of the manuscript.
Ethics approval and consent to
participate
The present study was performed following approval
from the Institutional Review Board in Saitama Cancer Centre (nos.
231, 483 and 534). Furthermore, the study was performed in
accordance with the Declaration of Helsinki, and written informed
consent was obtained from all patients prior to inclusion in the
study.
Patient consent for publication
Written informed consent was obtained from all
patients prior to inclusion in the study.
Competing interests
JH received research funding from CHUGAI
Pharmaceutical Co., Ltd. and Taiho Pharmaceutical Co., Ltd. JH
received an honoraria from Astra Zeneca K.K. in Japan. All
remaining authors have declared that they have no competing
interests.
References
|
1
|
Stanton SE, Adams S and Disis ML:
Variation in incidence and magnitude of tumor-infiltrating
lymphocytes in breast cancer subtypes: A systematic review. JAMA
Oncol. 2:1354–1360. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Klein E, Becker S, Svedmyr E, Jondal M and
Vánky F: Tumor infiltrating lymphocytes. Ann N Y Acad Sci.
276:207–216. 1976. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Galon J, Angell HK, Bedognetti D and
Marincola FM: The continuum of cancer immunosurveillance:
Prognostic, predictive, and mechanistic signatures. Immunity.
39:11–26. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Savas P, Salgado R, Denkert C, Sotiriou C,
Darcy PK, Smyth MJ and Loi S: Clinical relevance of host immunity
in breast cancer: From TILs to the clinic. Nat Rev Clin Oncol.
13:228–241. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Salgado R, Denkert C, Campbell C, Savas P,
Nuciforo P, Aura C, de Azambuja E, Eidtmann H, Ellis CE, Baselga J,
et al: Tumor-infiltrating lymphocytes and associations with
pathological complete response and event-free survival in
HER2-positive early-stage breast cancer treated with lapatinib and
trastuzumab: A secondary analysis of the NeoALTTO Trial. JAMA
Oncol. 1:448–454. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Denkert C, Loibl S, Noske A, Roller M,
Müller BM, Komor M, Budczies J, Darb-Esfahani S, Kronenwett R,
Hanusch C, et al: Tumor-associated lymphocytes as an independent
predictor of response to neoadjuvant chemotherapy in breast cancer.
J Clin Oncol. 28:105–113. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Issa-Nummer Y, Darb-Esfahani S, Loibl S,
Kunz G, Nekljudova V, Schrader I, Sinn BV, Ulmer HU, Kronenwett R,
Just M, et al: Prospective validation of immunological infiltrate
for prediction of response to neoadjuvant chemotherapy in
HER2-negative breast cancer-a substudy of the neoadjuvant
GeparQuinto trial. PLoS One. 8:e797752013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Denkert C, von Minckwitz G, Brase JC, Sinn
BV, Gade S, Kronenwett R, Pfitzner BM, Salat C, Loi S, Schmitt WD,
et al: Tumor-infiltrating lymphocytes and response to neoadjuvant
chemotherapy with or without carboplatin in human epidermal growth
factor receptor 2-positive and triple-negative primary breast
cancers. J Clin Oncol. 33:983–991. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
West NR, Milne K, Truong PT, Macpherson N,
Nelson BH and Watson PH: Tumor-infiltrating lymphocytes predict
response to anthracycline-based chemotherapy in estrogen
receptor-negative breast cancer. Breast Cancer Res. 13:R1262011.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Salgado R, Denkert C, Demaria S, Sirtaine
N, Klauschen F, Pruneri G, Wienert S, Van den Eynden G, Baehner FL,
Penault-Llorca F, et al: The evaluation of tumor-infiltrating
lymphocytes (TILs) in breast cancer: Recommendations by an
International TILs Working Group 2014. Ann Oncol. 26:259–271. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hammond ME, Hayes DF, Dowsett M, Allred
DC, Hagerty KL, Badve S, Fitzgibbons PL, Francis G, Goldstein NS,
Hayes M, et al: American Society of Clinical Oncology/College Of
American Pathologists guideline recommendations for
immunohistochemical testing of estrogen and progesterone receptors
in breast cancer. J Clin Oncol. 28:2784–2795. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Wolff AC, Hammond ME, Hicks DG, Dowsett M,
McShane LM, Allison KH, Allred DC, Bartlett JM, Bilous M,
Fitzgibbons P, et al: Recommendations for human epidermal growth
factor receptor 2 testing in breast cancer: American Society of
Clinical Oncology/College of American Pathologists clinical
practice guideline update. Arch Pathol Lab Med. 138:241–256. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Loi S, Sirtaine N, Piette F, Salgado R,
Viale G, Van Eenoo F, Rouas G, Francis P, Crown JP, Hitre E, et al:
Prognostic and predictive value of tumor-infiltrating lymphocytes
in a phase III randomized adjuvant breast cancer trial in
node-positive breast cancer comparing the addition of docetaxel to
doxorubicin with doxorubicin-based chemotherapy: BIG 02–98. J Clin
Oncol. 31:860–867. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Adams S, Gray RJ, Demaria S, Goldstein L,
Perez EA, Shulman LN, Martino S, Wang M, Jones VE, Saphner TJ, et
al: Prognostic value of tumor-infiltrating lymphocytes in
triplenegative breast cancers from two phase III randomized
adjuvant breast cancer trials: ECOG 2197 and ECOG 1199. J Clin
Oncol. 32:2959–2966. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Loi S, Drubay D, Adams S, Francis PA,
Joensuu H, Dieci MV, Badve S, Demaria S, Gray R, Piccart MJ, et al:
Pooled individual patient data analysis of stromal tumor
infiltrating lymphocytes in primary triple negative breast cancer
treated with anthracyclinebased chemotherapy. Cancer Res. 76
(suppl):abstr S1-03. 2016. View Article : Google Scholar
|
|
16
|
Loi S, Michiels S, Salgado R, Sirtaine N,
Jose V, Fumagalli D, Kellokumpu-Lehtinen PL, Bono P, Kataja V,
Desmedt C, et al: Tumor infiltrating lymphocytes are prognostic in
triple negative breast cancer and predictive for trastuzumab
benefit in early breast cancer: Results from the FinHER trial. Ann
Oncol. 25:1544–1550. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Denkert C, von Minckwitz G, Darb-Esfahani
S, Lederer B, Heppner BI, Weber KE, Budczies J, Huober J, Klauschen
F, Furlanetto J, et al: Tumour-infiltrating lymphocytes and
prognosis in different subtypes of breast cancer: A pooled analysis
of 3771 patients treated with neoadjuvant therapy. Lancet Oncol.
19:40–50. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Heindl A, Sestak I, Naidoo K, Cuzick J,
Dowsett M and Yuan Y: Relevance of Spatial Heterogeneity of Immune
Infiltration for Predicting Risk of Recurrence After Endocrine
Therapy of ER+ Breast Cancer. J Natl Cancer Inst.
110:2018. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kurozumi S, Fujii T, Matsumoto H, Inoue K,
Kurosumi M, Horiguchi J and Kuwano H: Significance of evaluating
tumor-infiltrating lymphocytes (TILs) and programmed cell
death-ligand 1 (PD-L1) expression in breast cancer. Med Mol
Morphol. 50:185–194. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Goodman AM, Kato S, Bazhenova L, Patel SP,
Frampton GM, Miller V, Stephens PJ, Daniels GA and Kurzrock R:
Tumor mutational burden as an independent predictor of response to
immunotherapy in diverse cancers. Mol Cancer Ther. 16:2598–2608.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Pereira B, Chin SF, Rueda OM, Vollan HK,
Provenzano E, Bardwell HA, Pugh M, Jones L, Russell R, Sammut SJ,
et al: The somatic mutation profiles of 2,433 breast cancers
refines their genomic and transcriptomic landscapes. Nat Commun.
7:114792016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Haricharan S, Bainbridge MN, Scheet P and
Brown PH: Somatic mutation load of estrogen receptor-positive
breast tumors predicts overall survival: An analysis of genome
sequence data. Breast Cancer Res Treat. 146:211–220. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Svoronos N, Perales-Puchalt A, Allegrezza
MJ, Rutkowski MR, Payne KK, Tesone AJ, Nguyen JM, Curiel TJ,
Cadungog MG, Singhal S, et al: Tumor cell-independent estrogen
signaling drives disease progression through mobilization of
myeloid-derived suppressor cells. Cancer Discov. 7:72–85. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Montagna E, Vingiani A, Maisonneuve P,
Cancello G, Contaldo F, Pruneri G and Colleoni M: Unfavorable
prognostic role of tumor-infiltrating lymphocytes in
hormone-receptor positive, HER2 negative metastatic breast cancer
treated with metronomic chemotherapy. Breast. 34:83–88. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Topalian SL, Taube JM, Anders RA and
Pardoll DM: Mechanism-driven biomarkers to guide immune checkpoint
blockade in cancer therapy. Nat Rev Cancer. 16:275–287. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Larkin J, Chiarion-Sileni V, Gonzalez R,
Grob JJ, Cowey CL, Lao CD, Schadendorf D, Dummer R, Smylie M,
Rutkowski P, et al: Combined nivolumab and ipilimumab or
monotherapy in untreated melanoma. N Engl J Med. 373:23–34. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Brahmer J, Reckamp KL, Baas P, Crinò L,
Eberhardt WE, Poddubskaya E, Antonia S, Pluzanski A, Vokes EE,
Holgado E, et al: Nivolumab versus docetaxel in advanced
squamous-cell nonsmall-cell lung cancer. N Engl J Med. 373:123–135.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Motzer RJ, Rini BI, McDermott DF, Redman
BG, Kuzel TM, Harrison MR, Vaishampayan UN, Drabkin HA, George S,
Logan TF, et al: Nivolumab for metastatic renal cell carcinoma:
Results of a randomized phase II trial. J Clin Oncol. 33:1430–1437.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Nanda R, Chow LQ, Dees EC, Berger R, Gupta
S, Geva R, Pusztai L, Pathiraja K, Aktan G, Cheng JD, et al:
Pembrolizumab in patients with advanced triple-negative breast
cancer: Phase Ib KEYNOTE-012 study. J Clin Oncol. 34:2460–2467.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Gibney GT, Weiner LM and Atkins MB:
Predictive biomarkers for checkpoint inhibitor-based immunotherapy.
Lancet Oncol. 17:e542–e551. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Zhang M, Sun H, Zhao S, Wang Y, Pu H, Wang
Y and Zhang Q: Expression of PD-L1 and prognosis in breast cancer:
A meta-analysis. Oncotarget. 8:31347–31354. 2017.PubMed/NCBI
|
|
32
|
Soliman H, Khalil F and Antonia S: PD-L1
expression is increased in a subset of basal type breast cancer
cells. PLoS One. 9:e885572014. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Hendry S, Pang JB, Byrne DJ, Lakhani SR,
Cummings MC, Campbell IG, Mann GB, Gorringe KL and Fox SB:
Relationship of the breast ductal carcinoma in situ immune
microenvironment with clinicopathological and genetic features.
Clin Cancer Res. 23:5210–5217. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Tarhini AA, Zahoor H, Yearley JH, Gibson
C, Rahman Z, Dubner R, Rao UN, Sander C and Kirkwood JM: Tumor
associated PD-L1 expression pattern in microscopically tumor
positive sentinel lymph nodes in patients with melanoma. J Transl
Med. 13:3192015. View Article : Google Scholar : PubMed/NCBI
|