Introduction
Glypican-3 (GPC3) is a cell-surface heparin sulfate
proteoglycan that binds to the cell surface membrane through a
glycosyl-phosphatidylinositol anchor (1). It expresses predominantly during
development, tissue- and stage-specifically in the fetal liver,
kidney, vertebrae, and genital system, but not in most of the
mature normal organs (2). As GPC3 is
located in chromosome Xq26, its loss-of-function mutation in the
human GPC3 gene results in Simpson-Golabi-Behmel syndrome,
which is an X-linked disorder characterized by pre- and postnatal
overgrowth that is accompanied by a high risk of the development of
embryonal tumors such as hepatoblastoma, neuroblastoma (NB),
gonadoblastoma, Wilms tumor, and hepatocellular carcinoma (3,4).
Malignant small round cell tumors are histologically
characterized by a proliferation of small round tumor cells with
scant cytoplasm, and they are often difficult to distinguish by
standard histology or additional immunohistochemistry. However, the
quick initiation of treatment is needed for individuals with such
tumors.
GPC3 expression was recently reported in several
pediatric malignancies as well as in adult malignancies, and thus
its potential usefulness as a novel diagnostic marker is being
recognized. It is commonly known that GPC3 is expressed in
hepatocellular carcinoma, and the expression of GPC3 in many
primary liver tumors has been investigated (5–8). Kinoshita
et al examined the GPC3 expression in pediatric malignant
solid tumors, and they demonstrated that yolk sac tumor and
hepatoblastoma showed a high frequency of GPC3 expression (9).
In the present study, we immunohistochemically
analyzed the GPC3 protein expression in several types of malignant
small round cell tumors: Rhabdomyosarcoma (RMS), NB, Ewing sarcoma
(EWS), and desmoplastic small round cell tumors (DSRCT). We
determined the GPC3 protein expression in order to assess the
utility of GPC3 as a diagnostic marker in these tumors. We also
examined the mRNA expression of GPC3 in frozen samples by
performing a reverse transcription-quantitative polymerase chain
reaction (RT-qPCR) and by determining the serum-soluble GPC3 level
in preoperative blood samples with an enzyme-linked immunosorbent
assay (ELISA).
Patients and methods
Patients and tissue specimens
We collected 183 formalin-fixed paraffin-embedded
specimens from the soft-tissue tumor files registered between 1976
and 2007 at the Department of Anatomic Pathology, Graduate School
of Medical Sciences, Kyushu University, Fukuoka, Japan (Table I). These samples included 84 RMSs (44
alveolar RMSs and 40 embryonal RMSs), 62 EWSs, 35 NBs, and two
DSRCTs. In addition, 86 frozen samples (66 tumor frozen samples and
20 samples of surrounding non-tumorous skeletal muscle from
patients who had undergone surgery for various types of sarcoma)
were snap-frozen in liquid nitrogen at the time of the surgical
procedure and stored at −80°C until use. These 66 frozen tumor
samples included 23 RMSs, 28 EWSs and 15 NBs.
 | Table I.Clinical characteristics of malignant
small round cell tumors. |
Table I.
Clinical characteristics of malignant
small round cell tumors.
| Characteristics | Alveolar
rhabdomyosarcoma, n=44 | Embryonal
rhabdomyosarcoma, n=40 | Ewing sarcoma,
n=62 | Neuroblastoma,
n=35 | Desmoplastic round
cell tumors, n=2 |
|---|
| Sex |
|
|
|
|
|
| Male | 23 | 19 | 27 | 20 | 2 |
|
Female | 21 | 21 | 35 | 15 | 0 |
| Age, years |
|
|
|
|
|
|
<15 | 22 | 32 | 26 | 35 | 1 |
| ≥15 | 22 | 8 | 36 | 0 | 1 |
We also analyzed the serum levels of GPC3 in
preoperative blood samples from 10 patients (eight with NBs and two
with RMSs). Our study included the RMS and NB cases from a previous
study of GPC3 expression in pediatric malignant solid tumors by
Kinoshita et al (9). The
institutional review board at Kyushu University approved this study
(approval no. 25-143).
Immunohistochemistry for GPC3
Immunohistochemistry was performed by the
streptavidin-biotin-peroxidase method (Histofine; Nichirei, Tokyo)
using a mouse monoclonal antibody against GPC3 (clone 1G12, 1:200;
BioMosaics, Burlington, VT, USA). We considered the cytoplasmic or
membrane staining pattern positive. The immunoreactivity for GPC3
was assessed independently by three pathologists (K.M., K.K., Y.Y.)
in a blinded fashion with the use of the labeling index (LI). The
GPC3-LI was determined using the number of positively stained tumor
cells among ≥500 tumor cells. We classified the protein expression
in the tumor tissues into three categories according to the LI
percentage: negative, <1%; focally positive, 1–10%; and
positive, >10% as described (10).
We categorized the RMS samples into a GPC3-positive
and focally positive expression group and a negative-expression
group. A log-rank based survival analysis was conducted for the
comparison of the overall survival of the patients in the two
groups.
TaqMan PCR to detect GPC3 mRNA
expression
We performed RT-qPCR for GPC3 and analyzed
the results using TaqMan assay reagents (GPC3 Hs00170471_m1;
GAPDH Hs99999905_m1) and an ABI Prism 7700 Sequence
Detection system (all Applied Biosystems, Foster City, CA, USA).
The PCR reaction was carried out according to the manufacturer's
protocol. The obtained data were standardized using data of the
international housekeeping gene, GAPDH. All of the reactions
for the standard samples and the patients' samples were performed
in triplicate. The data were averaged from the values obtained in
each reaction. The final numerical value (V) in each sample was
calculated as follows: V=GPC3 mRNA value ×
106/GAPDH mRNA value.
Detection of the serum-soluble GPC3 by
ELISA
Preoperative blood serum samples were available in
10 patients (the eight NB and two RMS patients). The GPC3 serum
levels were determined by a commercial ELISA kit (BioMosaics)
following the manufacturer's protocol. Based on the data of healthy
adult samples with the standard deviation, we set the cut-off level
for GPC3 at 178 ng/ml, as described (9).
Statistical analyses
JMP® 13 (SAS Institute, Inc., Cary, NC,
USA) was used for the statistical analysis. The data regarding the
relative expressions of GPC3 mRNA and protein are presented as the
mean ± standard deviation of at least three independent
experiments. Univariate survival analysis was conducted according
to the Kaplan-Meier method, and the difference between the survival
curves was analyzed with the log-rank test. P<0.05 was
considered to indicate a statistically significant difference.
Results
Immunoreactivity for GPC3
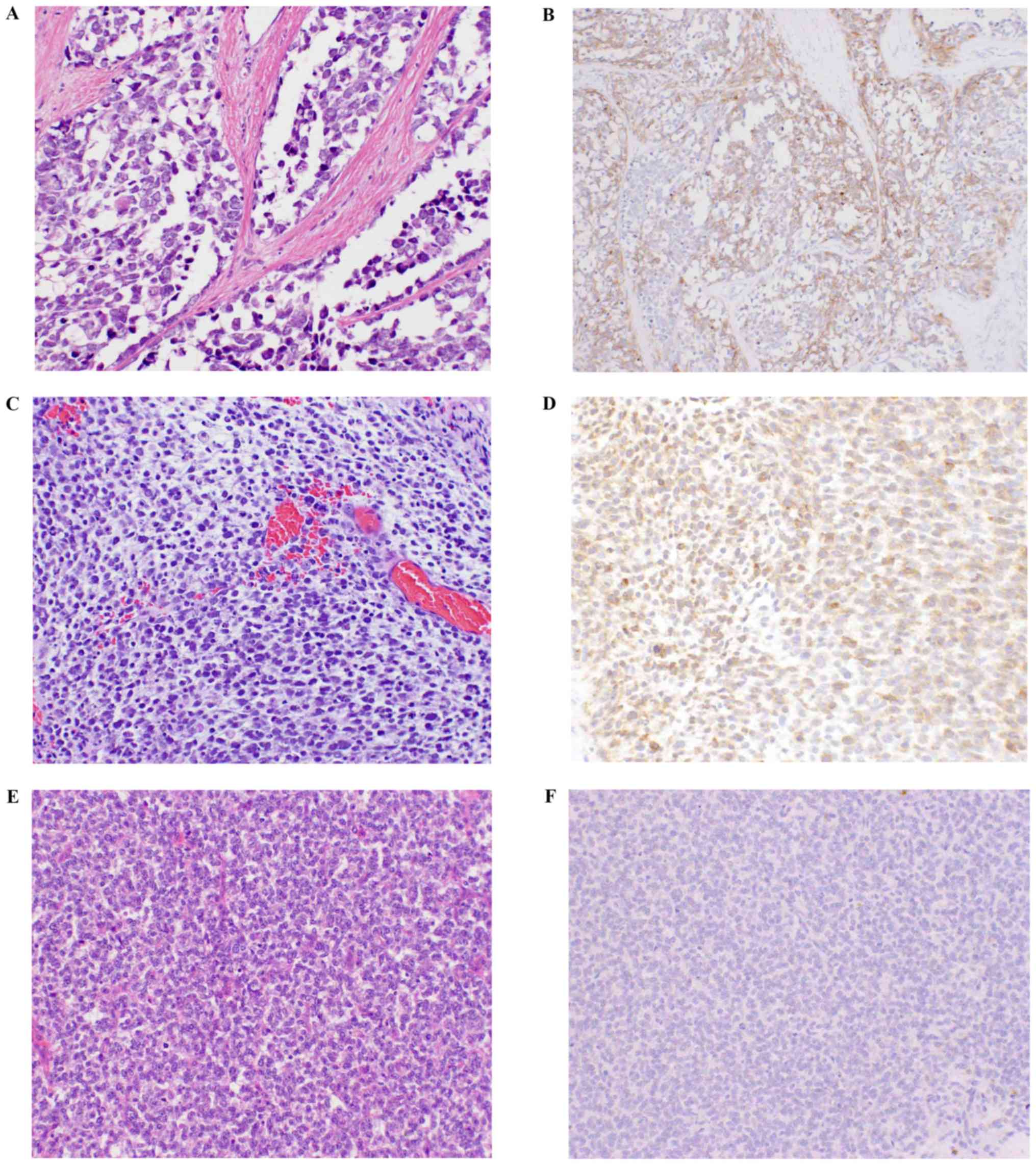
The results of the immunohistochemical analysis are
summarized in Table II. In the RMS
group, 19.0% (16/84) showed positive immunoreactivity for GPC3 and
6.0% (5/84) showed focally positive staining. The embryonal RMSs
and alveolar RMSs showed approximately the same proportion of
GPC3-positive immunoreactivity. In contrast, none of the EWS or
DSRCT cases showed GPC3 expression. Only a single NB showed GPC3
protein expression (Fig. 1).
| Table II.Glypican 3 expression in small round
cell tumors. |
Table II.
Glypican 3 expression in small round
cell tumors.
| Small round cell
tumor subtype | GPC3 (+) (%) | GPC3 (±) (%) | GPC3 (−) (%) |
|---|
| RMS, n=84 | 16 (19.0) | 5 (6.0) | 63 (75.0) |
| Alveolar RMS,
n=44 | 8 (18.2) | 1 (2.3) | 35 (79.5) |
| Embryonal RMS,
n=40 | 8 (20.0) | 4 (10.0) | 28 (70.0) |
| EWS, n=62 | 0 | 0 | 62 (100) |
| NB, n=35 | 1 (2.9) | 0 | 34 (97.1) |
| DSRCT | 0 | 0 | 2 (100) |
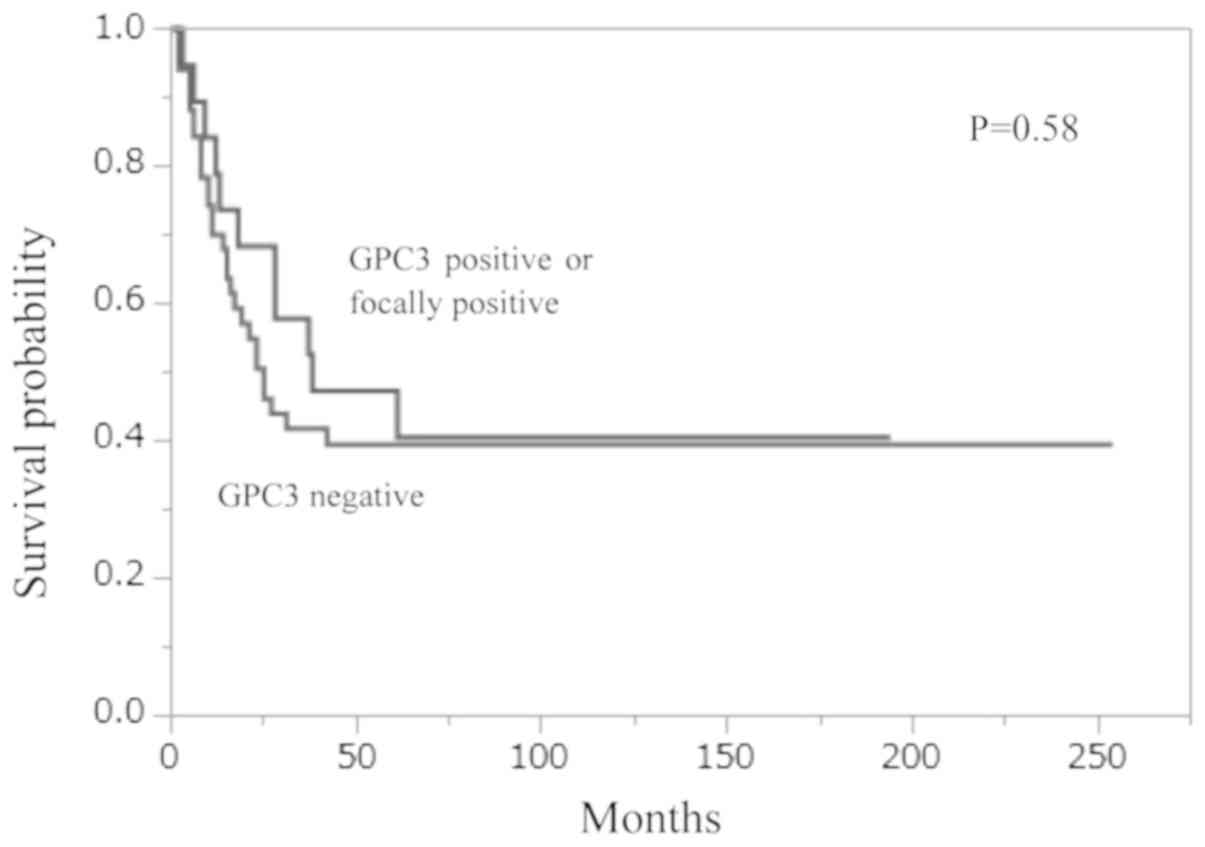
Survival analysis of RMS
Survival data were available in 70 of the 84 RMSs
(36 ARMSs and 34 ERMSs), and the follow-up periods of these cases
ranged from 2 to 254 months (average 62 months). We divided the RMS
patients into the immunohistochemically GPC3-positive or focally
positive and -negative groups. The survival rate of the negative
GPC3 expression group was considerably lower than that of the
positive/focally positive group, though the difference was not
significant (P=0.58, Fig. 2).
GPC3 mRNA expression by TaqMan
PCR
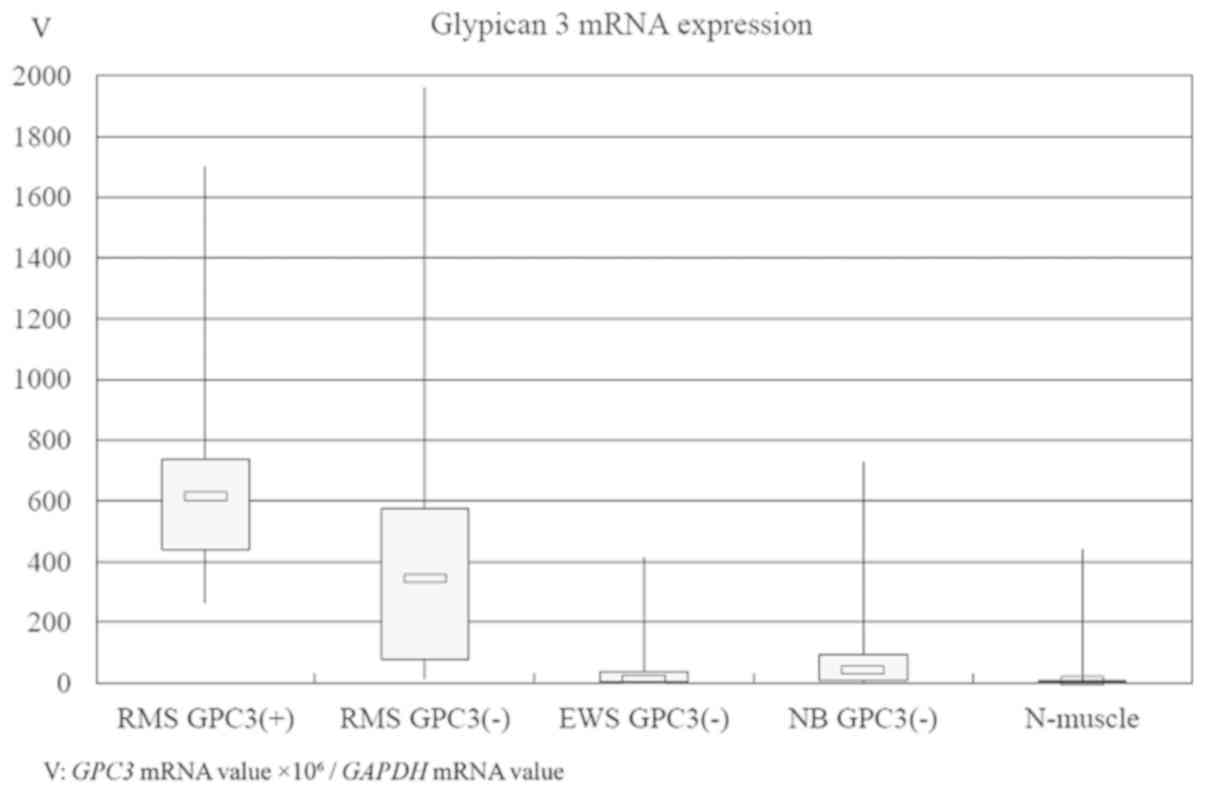
Fig. 3 provides the
boxplots of GPC3 mRNA expression and the median values
according to: the two groups of RMSs with immunohistochemically
positive GPC3 expression (615.23), the RMSs with negative GPC3
expression (345.18), the EWSs (12.03), the NBs (43.43), and
non-tumorous skeletal muscle (7.47). The GPC3 mRNA
expression level of the RMSs with positive GPC3 expression was
significantly higher than those of the EWS, NB, and non-tumorous
skeletal muscle groups (P=0.0003, 0.0024 and 0.0004,
respectively).
Serum-soluble GPC3 protein level
Regarding the malignant small round cell tumors'
serum-soluble GPC3 protein levels, our analyses revealed that
although neither of the tumors showed immunoreactivity for GPC3,
three cases of NBs showed high serum levels of GPC3.
Discussion
GPC3 is widely known to express in many malignancies
such as embryonal tumors (Wilms tumor, hepatoblastoma, and NB)
(11), germ cell tumors (yolk sac
tumor, immature teratoma, and embryonal carcinoma) (12), carcinomas (hepatocellular carcinoma
and pulmonary squamous cell carcinoma) (6,13),
sarcomas (malignant rhabdoid tumor and RMS) (10,14) and
malignant melanoma (15). In the
present study, we observed the overexpression of GPC3 in 25%
(21/84) of the RMSs but no expression in the EWSs, which was
similar to the results reported by Thway, who described the
frequency of GPC3 immunoreactivity among 213 RMSs as 34.7% (n=74)
(14).
Our observations of a high expression of GPC3 mRNA
in RMSs and a low expression in EWSs and DSRCTs are similar to the
results reported by Baer et al (16). Therefore, the evaluation of GPC3
expression may have the potential to be an ancillary parameter in
the differential diagnosis of RMS from EWS and DSRCT.
Some of the GPC3-negative RMSs in the present
analysis showed a high expression of GPC3 mRNA. We speculate that
GPC3 protein expression may be regulated by other
post-transcriptional regulatory mechanisms such as microRNA.
Studies by Nakatsura et al revealed the high
expression of GPC3 mRNA and protein in hepatocellular
carcinoma and melanoma (6,15). They also noted that GPC3 peptides may
be suitable for cancer immunotherapy for GPC3-expressing tumors,
because of its low expression in most other normal tissues in
adults. Nakatsura's group reported the results of a phase I
clinical trial regarding the immune and clinical responses of
advanced hepatocellular carcinoma (HCC) patients treated with a
GPC3-derived peptide vaccine (17).
In our present series, approx. 20% of the 29 cases
of ARMS, known as a poor-prognosis malignancy, showed positivity
for GPC3 and a high GPC3 mRNA level in tumor tissue. Thus,
GPC3 peptide immunotherapy may have a beneficial role for ARMS
patients.
Several studies revealed the poorer prognosis of HCC
patients with GPC3 overexpression compared to those with no or low
GPC3 expression (18,19). GPC3 is necessary for HCC cell growth,
adhesion, and migration by upregulating canonical Wnt signaling and
insulin-like growth factor-2 in vitro (20). In the present study, we assessed the
prognosis of RMS with the positive vs. negative status of GPC3
expression in tumor tissue, and the results of our analyses showed
a tendency for a poor prognosis in the negative status, but our
findings did not reveal a significant prognostic difference between
the two groups. The cause of the difference between the prognosis
of HCC and that of RMS is unclear. GPC3 expression may thus have
limited use as a prognostic indicator in RMS.
It was a predictable result that most of our NB
cases (n=35) showed no GPC3 immunoreactivity, and also showed low
GPC3 mRNA expression levels. Chan et al reported that
the immunohistochemical GPC3 expression was entirely negative in
clinical samples of NB (21), whereas
Saikali and Sinnett reported increased GPC3 mRNA expression
levels in most of the 10 NB cell lines they examined (11). Further studies using a larger number
of NB cases are required to confirm the correlation between GPC3
immunoreactivity and the mRNA expression level.
The serum level of GPC3 was proposed as a novel
tumor marker for HCC, along with its significant correlations with
the protein and mRNA expression levels (6). We observed high GPC3 serum levels in
three present NB patients, although these patients had
immunohistochemically GPC3-negative tumors. It is unclear what
caused this contradiction. The usefulness of the serum level of
GPC3 as a novel marker was not clarified in the present study.
Investigations of larger numbers of cases are necessary to test its
applicability.
In summary, our findings demonstrated GPC3
overexpression in RMS, whereas other malignant small round cell
tumors (i.e., EWS, DSRCT, and most of the NB cases) showed no GPC3
expression. This difference in expression status could be useful in
the differential diagnosis of small round cell tumors. GPC3
immunotherapy could be a beneficial approach for RMSs with GPC3
overexpression.
Acknowledgements
Not applicable.
Funding
The present study was supported by the Japan Society
for the Promotion of Science KAKENHI (grants no. 25293088 and
26460435).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
YS, KM, KK, HY and YO designed the study. YS, KM and
MK performed the experiments. YK and TT collected the clinical
information. YS and KM wrote the manuscript. KK, HY and YO reviewed
and checked the manuscript. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The present study was approved by the Kyushu
University Committee of Bioethics (approval no. 29-429; 2017).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that there are no competing
interests.
References
|
1
|
Filmus J: Glypicans in growth control and
cancer. Glycobiology. 11:19R–23R. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Iglesias BV, Centeno G, Pascuccelli H,
Ward F, Peters MG, Filmus J, Puricelli L and de Kier Joffé EB:
Expression pattern of glypican-3 (GPC3) during human embryonic and
fetal development. Histol Histopathol. 23:1333–1340.
2008.PubMed/NCBI
|
|
3
|
DeBaun MR, Ess J and Saunders S: Simpson
Golabi Behmel syndrome: Progress toward understanding the molecular
basis for overgrowth, malformation, and cancer predisposition. Mol
Genet Metab. 72:279–286. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lapunzina P: Risk of tumorigenesis in
overgrowth syndromes: A comprehensive review. Am J Med Genet C
Semin Med Genet. 137C:53–71. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Schirwani S, Novelli A, Digilio MC, Bourn
D, Wilson V, Roberts C, Dallapiccola B and Hobson E: Duplications
of GPC3 and GPC4 genes in symptomatic female carriers of
simpson-golabi-behmel syndrome type 1. Eur J Med Genet pii.
S1769-7212:30203–30209. 2018.
|
|
6
|
Nakatsura T, Yoshitake Y, Senju S, Monji
M, Komori H, Motomura Y, Hosaka S, Beppu T, Ishiko T, Kamohara H,
et al: Glypican-3, overexpressed specifically in human
hepatocellular carcinoma, is a novel tumor marker. Biochem Biophys
Res Commun. 306:16–25. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Levy M, Trivedi A, Zhang J, Miles L,
Mattis AN, Kim GE, Lassman C, Anders RA, Misdraji J, Yerian LM, et
al: Expression of glypican-3 in undifferentiated embryonal sarcoma
and mesenchymal hamartoma of the liver. Hum Pathol. 43:695–701.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Xing XL, Qin H, Yan SQ, Zhou LS, Chen P
and Zhao D: Expression of glypican-3 is highly associated with
pediatric hepatoblastoma: A systemic analysis. Asian Pac J Cancer
Prev. 16:1029–1031. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kinoshita Y, Tanaka S, Souzaki R, Miyoshi
K, Kohashi K, Oda Y, Nakatsura T and Taguchi T: Glypican 3
expression in pediatric malignant solid tumors. Eur J Pediatr Surg.
25:138–144. 2015.PubMed/NCBI
|
|
10
|
Kohashi K, Nakatsura T, Kinoshita Y,
Yamamoto H, Yamada Y, Tajiri T, Taguchi T, Iwamoto Y and Oda Y:
Glypican 3 expression in tumors with loss of SMARCB1/INI1 protein
expression. Hum Pathol. 44:526–533. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Saikali Z and Sinnett D: Expression of
glypican 3 (GPC3) in embryonal tumors. Int J Cancer. 89:418–422.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ota S, Hishinuma M, Yamauchi N, Goto A,
Morikawa T, Fujimura T, Kitamura T, Kodama T, Aburatani H and
Fukayama M: Oncofetal protein glypican-3 in testicular germ-cell
tumor. Virchows Arch. 449:308–314. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Aviel-Ronen S, Lau SK, Pintilie M, Lau D,
Liu N, Tsao MS and Jothy S: Glypican-3 is overexpressed in lung
squamous cell carcinoma, but not in adenocarcinoma. Mod Pathol.
21:817–825. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Thway K, Selfe J, Missiaglia E, Fisher C
and Shipley J: Glypican-3 is expressed in rhabdomyosarcomas but not
adult spindle cell and pleomorphic sarcomas. J Clin Pathol.
64:587–591. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Nakatsura T, Kageshita T, Ito S, Wakamatsu
K, Monji M, Ikuta Y, Senju S, Ono T and Nishimura Y: Identification
of glypican-3 as a novel tumor marker for melanoma. Clin Cancer
Res. 10:6612–6621. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Baer C, Nees M, Breit S, Wakamatsu K,
Monji M, Ikuta Y, Senju S, Ono T and Nishimura Y: Profiling and
functional annotation of mRNA gene expression in pediatric
rhabdomyosarcoma and Ewing's sarcoma. Int J Cancer. 110:687–694.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sawada Y, Yoshikawa T, Nobuoka D,
Shirakawa H, Kuronuma T, Motomura Y, Mizuno S, Ishii H, Nakachi K,
Konishi M, et al: Phase I trial of a glypican-3-derived peptide
vaccine for advanced hepatocellular carcinoma: Immunologic evidence
and potential for improving overall survival. Clin Cancer Res.
18:3686–3696. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Shirakawa H, Suzuki H, Shimomura M, Kojima
M, Gotohda N, Takahashi S, Nakagohri T, Konishi M, Kobayashi N,
Kinoshita T and Nakatsura T: Glypican-3 expression is correlated
with poor prognosis in hepatocellular carcinoma. Cancer Sci.
100:1403–1407. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Zhang J, Zhang M, Ma H, Song X, He L, Ye X
and Li X: Overexpression of glypican-3 is a predictor of poor
prognosis in hepatocellular carcinoma: An updated meta-analysis.
Medicine (Baltimore). 97:e1111302018.
|
|
20
|
Midorikawa Y, Ishikawa S, Iwanari H,
Imamura T, Sakamoto H, Miyazono K, Kodama T, Makuuchi M and
Aburatani H: Glypican-3, overexpressed in hepatocellular carcinoma,
modulates FGF2 and BMP-7 signaling. Int J Cancer. 103:455–465.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Chan ES, Pawel BR, Corao DA, Venneti S,
Russo P, Santi M and Sullivan LM: Immunohistochemical expression of
glypican-3 in pediatric tumors: An analysis of 414 cases. Pediatr
Dev Pathol. 16:272–277. 2013. View Article : Google Scholar : PubMed/NCBI
|