Introduction
Renal cell carcinoma (RCC) is the most common renal
malignancy, causing approximately 99200 new cases and almost 39100
deaths in Europe in 2018 (1). Clear
cell renal cell carcinoma (ccRCC) is the most common pathological
type of RCC, accounting for 80–90% of total cases globally in 2016
(2). Although surgical resection is
an effective treatment option for early ccRCC, the prognosis for
patients with metastatic ccRCC is poor (3). Targeted therapy is a promising
anticancer strategy (4) and the
identification of novel hub genes specific to ccRCC may improve
targeted treatment and confer significant benefit on patients.
MYB protooncogene-like 2 (MYBL2), a member of
the myeloblastosis family of transcription factors, influences
numerous factors affecting cell cycle progression (5). Recently, an increasing number of
studies have demonstrated that MYBL2 expression is
significantly associated with various carcinomas. For example,
upregulated MYBL2 expression was identified in gastric
cancer and predicted a poor prognosis, indicating that MYBL2
may serve as a promising biomarker (6). Overexpressed MYBL2 promotes
proliferation and inhibits apoptosis of breast cancer cells
targeted by miR-143-3p (7).
Moreover, MYBL2 knockdown suppressed the growth of
esophageal squamous cell and colorectal carcinoma cells via
regulation of the cell cycle (8). In
other cancer types, including hepatocellular carcinoma (HCC)
(9), non-small cell lung cancer
(NSCLC) (10) and pancreatic ductal
adenocarcinoma (11), high
MYBL2 expression also promoted the progression of tumors and
resulted in a poorer prognosis. However, the influence of
MYBL2 expression on ccRCC is yet to be elucidated.
Therefore, MYBL2 expression was analyzed in
ccRCC, and the association between MYBL2 and the prognosis
of patients with ccRCC was determined in the current study.
Moreover, gene set enrichment analysis (GSEA) was performed to
investigate the biological functions of MYBL2 in ccRCC.
According to previous studies, it was hypothesized that
MYBL2 may independently predict the prognosis of ccRCC
patients and may represent a novel therapeutic target.
Materials and methods
Patient samples
The mRNA expression data and corresponding clinical
data from patients with ccRCC were downloaded from the official
website of The Cancer Genome Atlas database (National Institutes of
Health), dataset TCGA-Kidney Renal Clear Cell Carcinoma. A total of
611 gene expression data profiles and 537 clinical data profiles
were retrieved from TCGA ccRCC database in July 2019. The 611 gene
expression data profiles were used to evaluate the differential
expression of MYBL2 between tumor (539) and healthy tissues
(72). Subsequently, patients lacking gene expression data or all
clinicopathological characteristics were excluded, 530 ccRCC
profiles with both gene expression and clinical data were included
for further analysis. Some patients had incomplete
clinicopathological characteristics data, such as T stage (12), therefore these patients were included
in analysis of clinical information they possessed, but excluded in
the analysis of clinicopathological characteristics they lacked.
Hence, some variables in Table I do
not total 530.
 | Table I.Clinicopathological characteristics
of patients with clear cell renal cell carcinoma, retrieved from
The Cancer Genome Atlas database. |
Table I.
Clinicopathological characteristics
of patients with clear cell renal cell carcinoma, retrieved from
The Cancer Genome Atlas database.
| Clinical
characteristics | Value |
|---|
| Median age at
diagnosis, years (range) | 61 (21–90) |
| Sex, % |
|
|
Female | 35.1 |
|
Male | 64.9 |
| Histological
gradea, % |
|
| I |
2.7 |
| II | 43.5 |
|
III | 39.5 |
| IV | 14.3 |
| Clinical
stagea, % |
|
| I | 50.3 |
| II | 10.8 |
|
III | 23.3 |
| IV | 15.6 |
| T
stagea, % |
|
| T1 | 51.1 |
| T2 | 13.1 |
| T3 | 33.8 |
| T4 | 0.02 |
| Lymph node
metastasis N stagea,
% |
|
| N0 | 93.7 |
| N1 |
6.3 |
| Distant metastasis
M stagea, % |
|
| M0 | 84.3 |
| M1 | 15.7 |
GSEA
GSEA was used to investigate the potential functions
of MYBL2 in ccRCC. The pretense of GSEA is to use predefined
gene sets (usually from functional annotation or results of
previous studies) to rank genes according to the degree of
differential expression in two types of samples, and then test
whether the preselected gene sets are enriched at the top or bottom
of this ranking table. In the present study, the
‘c2.cp.kegg.v6.2.symbols.gmt’ gene sets from the Molecular
Signatures Database (software.broadinstitute.org/gsea/msigdb/index.jsp)
were analyzed using GSEA 3.0 software (BROAD Institute). To obtain
normalized enrichment scores (NESs), the nominal P-value and false
discovery rate (FDR) q-value were determined. The number of gene
set permutations for each analysis was set at 1,000, and the
phenotype label was the expression level of MYBL2. Gene sets
with a nominal P-value of <0.05 and an FDR q-value of <0.25
were considered significantly enriched (13).
Statistical analysis
The Mann-Whitney U test was used to compare MYBL2
expression in tumor and healthy tissues. The Wilcoxon signed-rank
test was used to compare MYBL2 expression in paired tissues. To
examine the association between clinicopathological factors and
MYBL2 expression (after excluding healthy tissue sample data) the
Mann-Whitney U test was performed for comparison between two groups
(sex, lymph node metastasis and distant metastasis), and the
Kruskal-Wallis test and Bonferroni's post-hoc test was performed
for multi-group comparison [tumor (T) stage, clinical stage and
histological grade] (12), then
logistic regression was conducted for further analysis. The median
value of MYBL2 expression was selected as the cutoff value, and
patients with ccRCC were subsequently divided into high- and
low-expression groups. Kaplan-Meier survival curves were
constructed and log rank tests performed to evaluate the
association between MYBL2 expression and overall survival (OS). A
univariate Cox regression analysis was performed to explore the
association of clinicopathological factors and MYBL2 expression
with OS, and a multivariate Cox regression analysis was performed
to investigate whether MYBL2 can independently influence prognosis.
All statistical analyses were performed using R version 3.5.3
software (14), Statistical Product
and Service Solutions (SPSS) 26.0 software (IBM Corp.) and GraphPad
Prism 8.0.2 software (GraphPad Software).
Results
Patient characteristics
Of the 530 included patients, the median patient age
was 61 years (range, 26–90), and there were 14, 227, 206 and 75
patients with histological grade I, II, III and IV, respectively. A
total of 265, 57, 123 and 82 patients presented with clinical stage
I, II, III and IV, respectively. There were also 271, 69, 179 and
11 patients with T1, T2, T3 and T4, respectively. Notably, 239 and
16 patients presented with node (N)0 and N1, respectively, and
there were 420 and 78 patients with metastasis (M)0 and M1,
respectively. The characteristics of the included patients with
ccRCC are summarized in Table I. A
number of samples retrieved from TCGA had incomplete
clinicopathological characteristics, therefore, samples lacking
specific clinicopathological characteristics will be excluded when
these clinicopathological characteristics were counted.
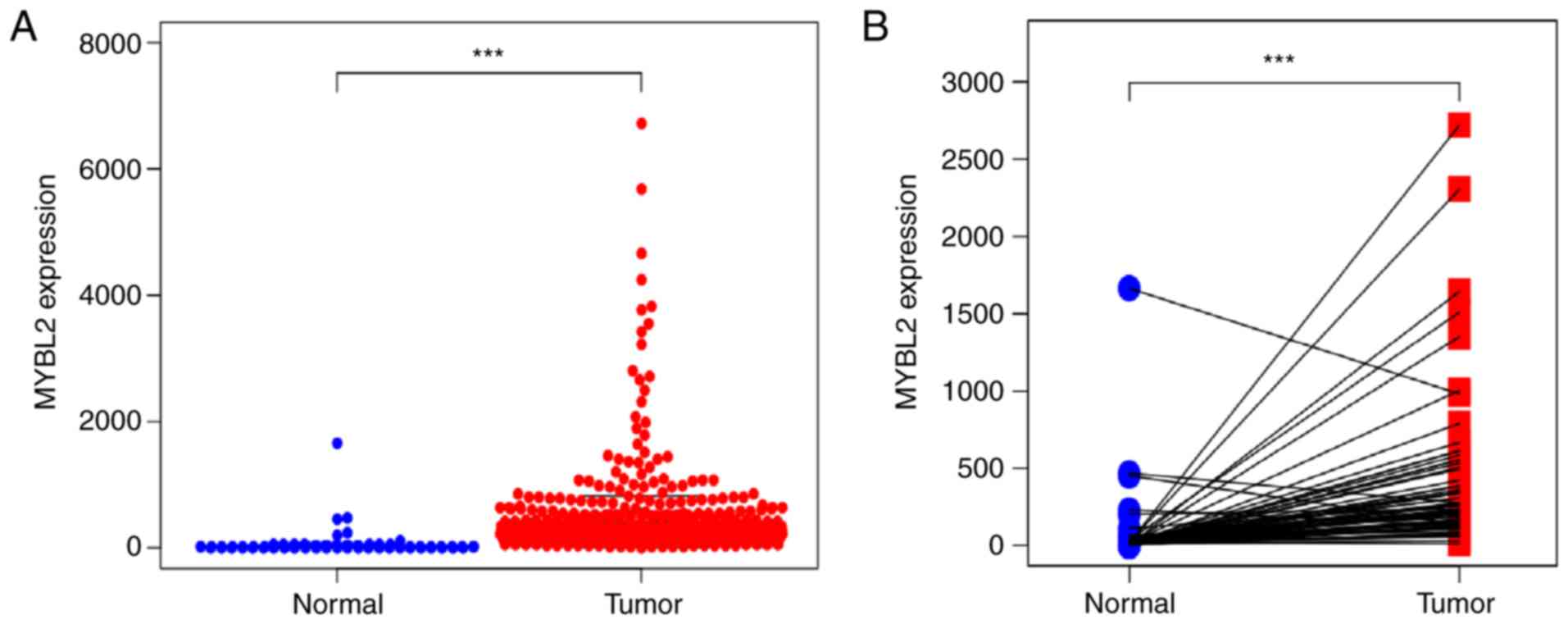
Upregulation of MYBL2
It was revealed that MYBL2 was significantly
upregulated in ccRCC tissues (P<0.001; Fig. 1A). In addition, MYBL2 was also
significantly upregulated in ccRCC tissues compared with paired
healthy tissues (P<0.001; Fig.
1B). The data from Fig. 1A and B
were derived from TCGA.
Association of MYBL2 expression and
clinicopathological factors
The median value of MYBL2 expression was
selected as the cut-off value and patients with ccRCC were divided
into high- and low-expression groups. The median follow-up times
for the high- and low-MYBL2 expression groups were 967 and
951 months, respectively. As indicated in Fig. 2A-F, the upregulation of MYBL2
was significantly associated with sex, an advanced T stage, lymph
node metastasis, distant metastasis, clinical stage and
histological grade. Logistic regression demonstrated that increased
MYBL2 expression was significantly associated with age, sex,
histologic grade, clinical stage, T stage, lymph node metastasis
and distant metastasis (Table II).
The data from Fig. 2A-F was derived
from TCGA.
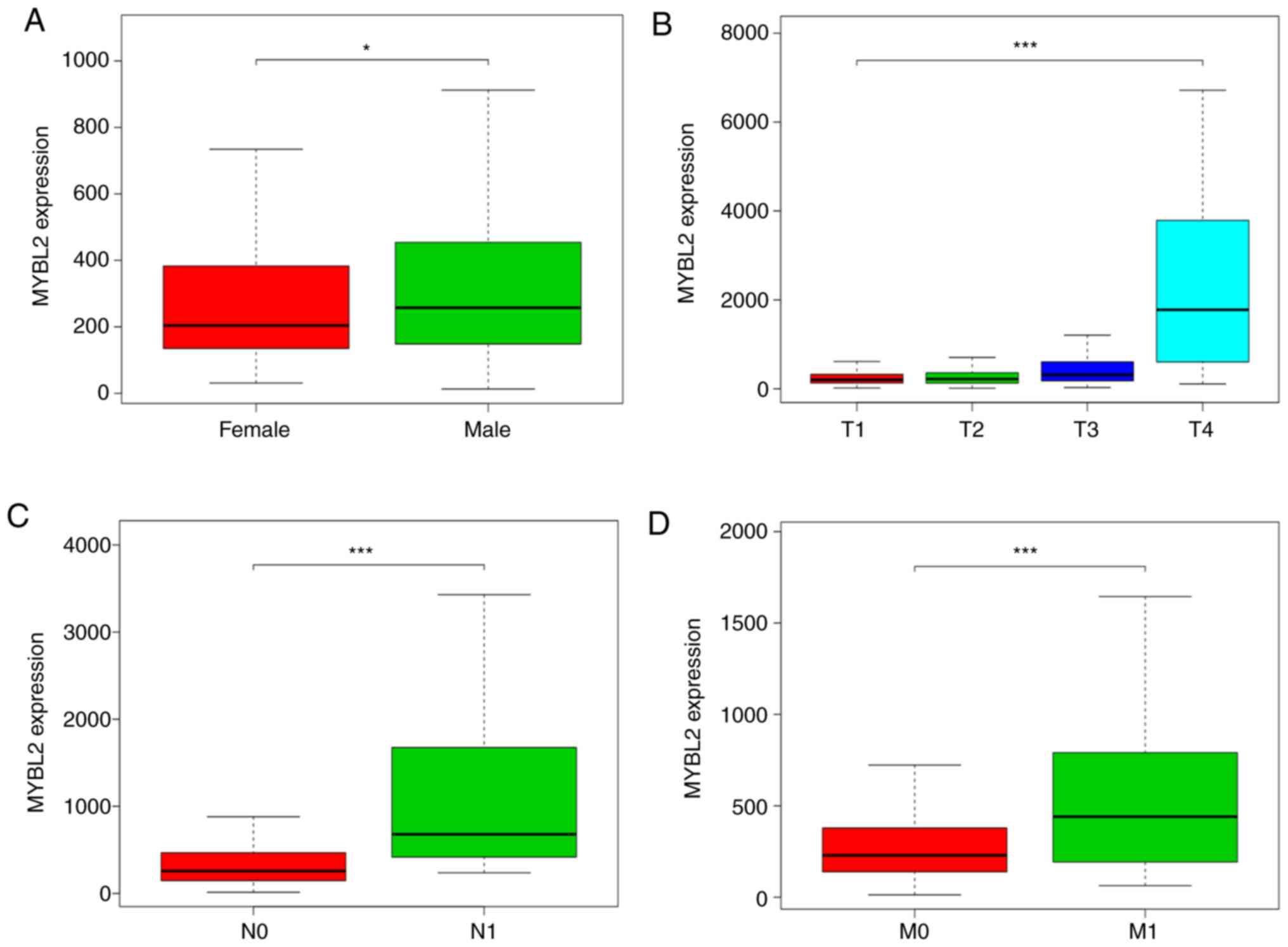 | Figure 2.Analysis of TGCA datasets was
conducted to determine expression of MYBL2 and its
association with clinicopathological variables. The median value of
MYBL2 expression was considered the cutoff value. To examine
the association between clinicopathological factors and
MYBL2 expression after excluding normal sample data, the
Mann-Whitney U test was performed for comparison between two groups
[sex, N stage and M stage (12)],
the Kruskal-Wallis test was used for multigroup comparison [T
stage, clinical stage and histological grade (12)]. The association between MYBL2
expression and OS was estimated using Kaplan-Meier survival curves.
(A) Sex; (B) T stage; (C) N stage; (D) M stage; (E) histological
grade; and (F) clinical stage. (G) Kaplan-Meier curves revealed
that the prognosis of patients with ccRCC with high MYBL2
expression was poorer than that of patients with ccRCC with low
MYBL2 expression. *P<0.05, ***P<0.001 TGCA, The Cancer
Genome Atlas; ccRCC, clear cell renal cell carcinoma; MYBL2,
MYB protooncogene-like 2; T, tumor; N, node; M, metastasis. |
| Table II.Association of MYB protooncogene-like
2 expression levels with the clinicopathological factors of
patients using logistic regression analysis. |
Table II.
Association of MYB protooncogene-like
2 expression levels with the clinicopathological factors of
patients using logistic regression analysis.
| Clinical
characteristics | Total, n | Odds ratio for
MYBL2 expression (Confidence Interval) | P-value |
|---|
| Age, years | 530 | 0.98
(0.96–0.99) | 0.003b |
| Sex, male vs.
female | 530 | 1.54
(1.08–2.21) | 0.018a |
| Histological
graded, IV vs. I | 89 | 22.15
(5.36–151.97) |
<0.001c |
| Clinical
staged, IV vs. I | 347 | 2.99
(1.78–5.11) |
<0.001c |
| T
staged, T4 vs. T1 | 530 | 6.19
(1.56–41.15) | 0.021a |
| N
staged, N1 vs. N0 | 255 | 4.91
(1.54–21.83) | 0.015a |
| M
staged, M1 vs. M0 | 498 | 3.85
(1.39–2.29) | 0.001b |
MYBL2 can be considered a prognostic
factor for ccRCC
Kaplan-Meier analysis revealed that patients with
ccRCC with high MYBL2 expression exhibited a poorer OS rate
compared with the low-expression group (Fig. 2G). Moreover, the univariate Cox
regression analysis indicated that high MYBL2 expression was
strongly associated with a poor prognosis. Other clinical
variables, such as age, grade, stage, T stage, lymph node
metastasis and distant metastasis were all associated with OS.
Moreover, multivariate analysis revealed that high MYBL2
expression, age and distant metastasis were independently
associated with a poor prognosis (Table III). Therefore, MYBL2 may be
an independent prognostic biomarker for patients with ccRCC.
| Table III.Association of OS and
clinicopathological characteristics in patients from TCGA database
using Cox regression. |
Table III.
Association of OS and
clinicopathological characteristics in patients from TCGA database
using Cox regression.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
|
Characteristics | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Age, years | 1.02 | 1.00–1.04 | 0.012a | 1.03 | 1.01–1.05 | 0.001b |
| Sex, male vs.
female | 1.01 | 0.67–1.54 | 0.951 | 1.11 | 0.71–1.73 | 0.657 |
| MYB
protooncogene-like 2 expression, high vs. low | 1.52 | 1.29–1.78 |
<0.001c | 1.29 | 1.08–1.55 | 0.004b |
| Histological
graded | 2.24 | 1.68–2.99 |
<0.001c | 1.27 | 0.91–1.79 | 0.164 |
| Clinical
staged | 1.86 | 1.54–2.25 |
<0.001c | 1.11 | 0.71–1.74 | 0.645 |
| T
staged | 3.31 | 2.17–5.06 |
<0.001c | 1.61 | 0.77–3.38 | 0.208 |
| N
staged | 2.93 | 1.52–5.67 | 0.001b | 1.31 | 0.64–2.68 | 0.456 |
| M
staged | 4.07 | 2.63–6.30 |
<0.001c | 2.25 | 1.03–4.79 | 0.041a |
Biological pathogenesis of MYBL2 in
ccRCC
GSEA revealed that the ‘intestinal immune network
for IgA production’, ‘primary immunodeficiency’, ‘the janus kinase
(JAK)-signal transducer and activator of transcription (STAT)
signaling pathway’, ‘the cytosolic DNA-sensing pathway’, ‘the p53
signaling pathway’ and ‘the chemokine signaling pathway’ (Fig. 3A-F) were enriched in the high
MYBL2 expression datasets (Table
IV).
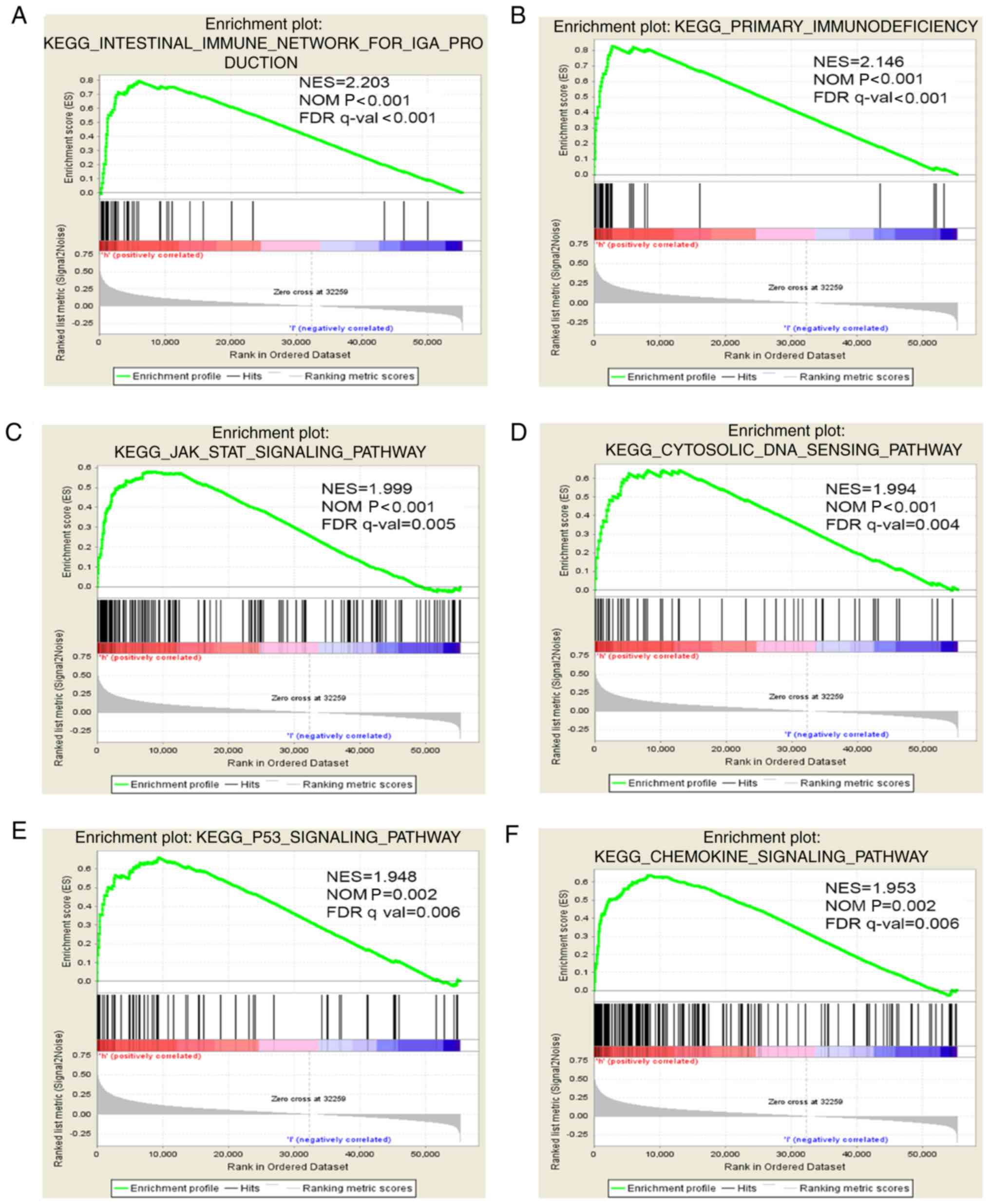 | Figure 3.Enrichment plots from GSEA. GSEA was
conducted to identify the differentially activated signaling
pathways in the high MYBL2 expression ccRCC datasets. GSEA
revealed that (A) ‘the intestinal immune network for IgA
production’, (B) ‘primary immunodeficiency’, (C) ‘the janus kinase
(JAK)-signal transducer and activator of transcription (STAT)
signaling pathway’, (D) ‘the cytosolic DNA-sensing pathway’, (E)
‘the p53 signaling pathway’ and (F) ‘the chemokine signaling
pathway’ were significantly enriched in patients with upregulated
MYBL2 expression. The data from (A-F) were derived from
GSEA. ccRCC, clear cell renal cell carcinoma; MYBL2, MYB
protooncogene-like 2; GSEA, gene set enrichment analysis; NES,
normalized enrichment score; NOM, nominal; FDR, false discovery
rate; q-val, q-value. |
| Table IV.Gene sets enriched in the high-MYB
protooncogene-like 2 expression phenotypes. |
Table IV.
Gene sets enriched in the high-MYB
protooncogene-like 2 expression phenotypes.
| Gene set name | NES | NOM P-value | FDR q-value |
|---|
|
KEGG_INTESTINAL_IMMUNE_NETWORK_FOR_IGA_PRODUCTION | 2.202 |
<0.001b | <0.001 |
|
KEGG_PRIMARY_IMMUNODEFICIENCY | 2.146 |
<0.001b | <0.001 |
|
KEGG_JAK_STAT_SIGNALING_PATHWAY | 1.999 |
<0.001b | 0.005 |
|
KEGG_CYTOSOLIC_DNA_SENSING_PATHWAY | 1.993 |
<0.001b | 0.004 |
|
KEGG_CHEMOKINE_SIGNALING_PATHWAY | 1.953 | 0.002a | 0.006 |
|
KEGG_P53_SIGNALING_PATHWAY | 1.948 | 0.002a | 0.006 |
Discussion
In the present study, analyzing the data from TCGA
provided a direction for further research and generated genomic and
statistical evidence to support novel candidate cancer targets for
therapeutic and diagnostic development. In the current study, it
was revealed that the upregulation of MYBL2 was significantly
associated with sex, high histological grade, advanced clinical
stage, T stage, lymph node metastasis, distant metastasis and poor
OS rate, and may therefore be used as an independent prognostic
factor for patients with ccRCC, according to data from TCGA.
Furthermore, the results of GSEA demonstrated that MYBL2
upregulation was significantly associated with classical
tumor-associated pathways and immune-associated pathways.
Previous findings have demonstrated that
MYBL2 regulates the progression of malignant tumors by
inhibiting the cell cycle and activating tumor-associated genes and
pathways via transcription factor activity (15). The upregulation of MYBL2 has
been reported in various cancer types, suggesting that MYBL2
may promote tumorigenesis. For example, the upregulation of
MYBL2 was revealed to promote progression of the G1-S phase
transition by suppressing insulin-like growth factor-binding
protein 3; thus, MYBL2 may represent a novel therapeutic
biomarker in NSCLC (16). Other
findings indicated that MYBL2 regulated breast cancer cell
proliferation and apoptosis via the targeting of microRNA-143-3p
(7). Therefore, MYBL2 may
serve as an effective therapeutic target. Notably, the high
expression and carcinogenic effects of MYBL2 in ccRCC were
described in detail in the present study.
GSEA was then performed; it is able to detect the
expression changes in gene sets rather than in individual genes and
is considered more flexible and reliable than traditional methods,
such as Gene Ontology and Kyoto Encyclopedia of Genes and Genomes,
making it one of the most commonly used pathway analysis methods to
study the biological function of tumors (17). However, for genes with complex
interactions and insufficient annotation information, the
sensitivity of GSEA is reduced due to functional class scoring, the
approach of GSEA (18). GSEA
demonstrated that MYBL2 is involved in various pathways
associated with tumor progression, such as the intestinal immune
network for IgA production, primary immunodeficiency, the JAK/STAT
signaling pathway, the cytosolic DNA-sensing pathway, the p53
signaling pathway and the chemokine signaling pathway. Some of
these pathways have been reported to be associated with other
cancer types. In HCC cells, increased apolipoprotein B mRNA editing
enzyme catalytic subunit 3F expression promoted cell proliferation
and migration, which were mediated by immune-associated pathways
(19). Moreover, a high incidence of
cancer, especially lymphoma, has been reported in subjects with
primary immunodeficiency (20).
Numerous studies have reported the association between JAK/STAT and
various malignancies and inflammatory pathologies, suggesting that
JAK-targeted drugs may be successful for the treatment of cancer
and immune-mediated diseases (21–27). A
previous study indicated that the downregulation of MYBL2
caused cell cycle arrest at the G2/M phase via the
p53-p21-DREAM-CDE/CHR pathway (28).
However, there were still certain limitations to the
current study. Notably, the number of normal tissues was
significantly lower than the number of tumorous tissues retrieved
from TCGA database. The factors associated with patient prognosis,
such as the use of drugs, surgical treatment and surgical details,
were lacking. Moreover, the protein levels or direct mechanisms
underlying the role of MYBL2 in ccRCC could not be assessed
using TCGA database. Therefore, accounting for various confounding
factors to more accurately assess the association between
MYBL2 and OS, and exploring the specific molecular
mechanisms involved represent a promising focus for future
research.
In conclusion, it was revealed that the upregulation
of MYBL2 in ccRCC was associated with certain advanced
clinical factors and was able to independently predict a poor
prognosis, indicating that MYBL2 expression may represent a
promising biomarker and potential therapeutic target for the
treatment of patients with ccRCC. However, the protein expression
levels of MYBL2 and the specific molecular mechanisms underlying
poor prognosis of ccRCC need to be further explored in future
research.
Acknowledgements
Not applicable.
Funding
The present study was supported by the National
Natural Science Foundation of China (grant no. 81302841) and the
University Outstanding Talent Support Plan Foundation of Liaoning
Province (grant no. LJQ2014086).
Availability of data and materials
The datasets generated and/or analyzed during the
current study are available in The Cancer Genome Atlas repository,
(portal.gdc.cancer.gov/).
Authors' contributions
JYL and YF designed this research project. SSS and
YF contributed to data collection, analysis and interpretation. All
authors participated in writing of the manuscript for the relevant
sections. All authors read and approved the final manuscript, and
agree to be accountable for all aspects of the research in ensuring
that the accuracy or integrity of any part of the work is
appropriately investigated and resolved.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
RCC
|
renal cell carcinoma
|
|
ccRCC
|
clear cell renal cell carcinoma
|
|
TCGA
|
The Cancer Genome Atlas
|
|
GSEA
|
gene set enrichment analysis
|
|
NES
|
normalized enrichment score
|
|
FDR
|
false discovery rate
|
|
OS
|
overall survival
|
|
HCC
|
hepatocellular carcinoma
|
References
|
1
|
Ferlay J, Colombet M, Soerjomataram I,
Dyba T, Randi G, Bettio M, Gavin A, Visser O and Bray F: Cancer
incidence and mortality patterns in Europe: Estimates for 40
countries and 25 major cancers in 2018. Eur J Cancer. 103:356–387.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ljungberg B, Albiges L, Abu-Ghanem Y,
Bensalah K, Dabestani S, Fernández-Pello S, Giles RH, Hofmann F,
Hora M, Kuczyk MA, et al: European association of urology
guidelines on renal cell carcinoma: The 2019 update. Eur Urol.
75:799–810. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Motzer RJ, Jonasch E, Agarwal N, Bhayani
S, Bro WP, Chang SS, Choueiri TK, Costello BA, Derweesh IH, Fishman
M, et al: Kidney cancer, version 2.2017, NCCN clinical practice
guidelines in oncology. J Natl Compr Canc Netw. 15:804–834. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Gore ME and Larkin JM: Challenges and
opportunities for converting renal cell carcinoma into a chronic
disease with targeted therapies. Br J Cancer. 104:399–406. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Iness AN, Felthousen J, Ananthapadmanabhan
V, Sesay F, Saini S, Guiley KZ, Rubin SM, Dozmorov M and Litovchick
L: The cell cycle regulatory DREAM complex is disrupted by high
expression of oncogenic B-Myb. Oncogene. 38:1080–1092. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Jia Y, Gao Y, Li J, Chang Z, Yan J and Qin
Y: Prognostic implications of MYBL2 in resected Chinese gastric
adenocarcinoma patients. Onco Targets Ther. 12:1129–1135. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Chen J and Chen X: MYBL2 is targeted by
miR-143-3p and regulates breast cancer cell proliferation and
apoptosis. Oncol Res. 26:913–922. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Qin H, Li Y, Zhang H, Wang F, He H, Bai X
and Li S: Prognostic implications and oncogenic roles of MYBL2
protein expression in esophageal squamous-cell carcinoma. Onco
Targets Ther. 12:1917–1927. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Guan Z, Cheng W, Huang D and Wei A: High
MYBL2 expression and transcription regulatory activity is
associated with poor overall survival in patients with
hepatocellular carcinoma. Curr Res Transl Med. 66:27–32. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Jin Y, Zhu H, Cai W, Fan X, Wang Y, Niu Y,
Song F and Bu Y: B-Myb is up-regulated and promotes cell growth and
motility in non-small cell lung cancer. Int J Mol Sci. 18(pii):
E8602017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Yu R, Li C, Lin X, Chen Q, Li J, Song L,
Lin L, Liu J, Zhang Y, Kong W, et al: Clinicopathologic features
and prognostic implications of MYBL2 protein expression in
pancreatic ductal adenocarcinoma. Pathol Res Pract. 213:964–968.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Amin MB, Edge SB, Greene FL, Byrd DR,
Brookland RK, Washington MK, Gershenwald JE, Compton CC, Hess KR,
Sullivan DC, et al: AJCC Cancer Staging Manual. 8th. Springer; pp.
751–752. 2017
|
|
13
|
Wu H and Zhang J: Decreased expression of
TFAP2B in endometrial cancer predicts poor prognosis: A study based
on TCGA data. Gynecol Oncol. 149:592–597. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Team RC: R: A language and environment for
statistical computing. R foundation for statistical computing,
version 2.15.1; Vienna, Austria: 2012
|
|
15
|
Musa J, Aynaud MM, Mirabeau O, Delattre O
and Grünewald TG: MYBL2 (B-Myb): A central regulator of cell
proliferation, cell survival and differentiation involved in
tumorigenesis. Cell Death Dis. 8:e28952017. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Fan X, Wang Y, Jiang T, Cai W, Jin Y, Niu
Y, Zhu H and Bu Y: B-Myb mediates proliferation and migration of
non-small-cell lung cancer via suppressing IGFBP3. Int J Mol Sci.
19(pii): E14792018. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Subramanian A, Tamayo P, Mootha VK,
Mukherjee S, Ebert BL, Gillette MA, Paulovich A, Pomeroy SL, Golub
TR, Lander ES and Mesirov JP: Gene set enrichment analysis: A
knowledge-based approach for interpreting genome-wide expression
profiles. Proc Natl Acad Sci USA. 102:15545–15550. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Khatri P, Sirota M and Butte AJ: Ten years
of pathway analysis: Current approaches and outstanding challenges.
PLoS Comput Biol. 8:e10023752012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Yang Z, Tao Y, Xu X, Cai F, Yu Y and Ma L:
Bufalin inhibits cell proliferation and migration of hepatocellular
carcinoma cells via APOBEC3F induced intestinal immune network for
IgA production signaling pathway. Biochem Biophys Res Commun.
503:2124–2131. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Mayor PC, Eng KH, Singel KL, Abrams SI,
Odunsi K, Moysich KB, Fuleihan R, Garabedian E, Lugar P, Ochs HD,
et al: Cancer in primary immunodeficiency diseases: Cancer
incidence in the United States immune deficiency network registry.
J Allergy Clin Immunol. 141:1028–1035. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Villarino AV, Kanno Y and O'Shea JJ:
Mechanisms and consequences of Jak-STAT signaling in the immune
system. Nat Immunol. 18:374–384. 2017. View
Article : Google Scholar : PubMed/NCBI
|
|
22
|
Cui C, Cheng X, Yan L, Ding H, Guan X,
Zhang W, Tian X and Hao C: Downregulation of TfR1 promotes
progression of colorectal cancer via the JAK/STAT pathway. Cancer
Manag Res. 11:6323–6341. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Toh TB, Lim JJ, Hooi L, Rashid MBMA and
Chow EK: Targeting Jak/Stat pathway as a therapeutic strategy
against SP/CD44+ tumorigenic cells in
Akt/β-catenin-driven hepatocellular carcinoma. J Hepatol.
72:104–118. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Wang X, Liao X, Yu T, Gong Y, Zhang L,
Huang J, Yang C, Han C, Yu L, Zhu G, et al: Analysis of clinical
significance and prospective molecular mechanism of main elements
of the JAK/STAT pathway in hepatocellular carcinoma. Int J Oncol.
55:805–822. 2019.PubMed/NCBI
|
|
25
|
Mendez Luque LF, Blackmon AL, Ramanathan G
and Fleischman AG: Key role of inflammation in myeloproliferative
neoplasms: Instigator of disease initiation, progression, and
symptoms. Curr Hematol Malig Rep. 14:145–153. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Cornez I, Yajnanarayana SP, Wolf AM and
Wolf D: JAK/STAT disruption induces immuno-deficiency: Rationale
for the development of JAK inhibitors as immunosuppressive drugs.
Mol Cell Endocrinol. 451:88–96. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Welsch K, Holstein J, Laurence A and
Ghoreschi K: Targeting JAK/STAT signalling in inflammatory skin
diseases with small molecule inhibitors. Eur J Immunol.
47:1096–1107. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Fischer M, Quaas M, Steiner L and Engeland
K: The p53-p21-DREAM-CDE/CHR pathway regulates G2/M cell cycle
genes. Nucleic Acids Res. 44:164–174. 2016. View Article : Google Scholar : PubMed/NCBI
|