Introduction
Hypopharyngeal squamous cell carcinoma (HPSCC) is
associated with one of the worst prognoses of all types of upper
aerodigestive tract cancer based on the U.S. population-based
analysis (1,2). Due to a rich network of lymphatic
vessels and the late presentation of symptoms, HPSCC is usually
detected at an advanced stage (3).
Surgery and radiotherapy alone, or in conjunction with
chemoradiation, is the standard treatment for HPSCC. However, the
overall 5-year survival rate for hypopharyngeal cancer is
unsatisfactory (37.5-41.3%) (2). The
identification of novel prognostic biomarkers may optimize the risk
stratification systems of HPSCC and, thus, may improve clinical
decision-making to ultimately improve patient survival.
Type I collagen is an important member of the
collagen family, which is a key structural component of the
extracellular matrix (4). Type I
collagen typically consists of a heterotrimer of two chains of
collagen type I α 1 (COL1A1) and one chain of collagen type I α 2
(COL1A2) (5). Type I collagen is
considered to influence tumor invasion and progression (6,7).
Recently, abnormal expression levels of COL1A1 and COL1A2 have been
reported in several types of cancer (8–10).
COL1A2 is downregulated in melanoma and bladder cancer, while
COL1A1 and COL1A2 mRNA expression levels are upregulated in
colorectal cancer and medulloblastoma (5,10–12). In
addition, Misawa et al (13)
reported that the methylation of the COL1A2 gene was an independent
adverse prognostic factor in head and neck cancer (13); however, this group have not
investigated the prognostic significance of COL1A2 in
hypopharyngeal squamous cell carcinoma, in detail.
In the present study, immunohistochemistry (IHC) was
used to evaluate the protein expression levels of COL1A1 and COL1A2
in hypopharyngeal squamous cell carcinoma tissues and to explore
the prognostic significance of these proteins in HPSCC.
Materials and methods
Patients and specimens
Between April 2012 and March 2017, 67 patients, who
were newly diagnosed with primary HPSCC and underwent radical
surgery at the Sun Yat-sen Memorial Hospital (Guangzhou, China),
were enrolled in the present study. The mean age of the patients
was 58.3 years (range of 41.0-74.0 years) with 97 and 3% males and
females, respectively. The cases selected were based on the
following criteria: i) No previous malignant disease or a second
primary tumor; and ii) no previous history of treatment with
radiotherapy, chemotherapy or surgery before HPSCC was diagnosed.
The pathological Tumor-Node-Metastasis (TNM) stage was defined
based on the 2017 edition of the TNM classification of the American
Joint Committee on Cancer (14). All
the experiments carried out in this study were approved by The
Ethics Committee of Sun Yat-sen Memorial Hospital, Sun Yat-sen
University (Guangzhou, China).
Tissue samples were obtained during the radical
surgery and were dehydrated at 4°C (70, 80, 90 and 95% ethanol, 3 h
for each step, and followed by 100% ethanol twice, 2 h for each
step), and vitrified (100% xylene twice, 0.5 h for each step).
Subsequently, tissue samples were immersed in melting paraffin at
56-58°C for 0.5 h and three times and then embedded in
paraffin.
Tissue microarray construction
The paraffin-embedded tissue blocks were cut into
4-µm thick sequential sections and the slides were dried,
deparaffinized in xylene at 20°C, rehydrated using a graded ethanol
series (100, 95, 80 and 70% ethanol followed by ddH2O, 2
min for each step) and immersed in hematoxylin (Sigma-Aldrich;
Merck KGaA) at 20°C for 10 min followed by ddH2O for 2
min. Subsequently, the slides were differentiated with acidic
ethanol for 15 sec and washed in running water for 30 min. The
slides were sequentially immersed in eosin at 20°C for 2 min
followed by ddH2O for 2 min. Finally, the sections were
dehydrated (70, 80, 90 and 100% ethanol, 2 min for each step),
vitrified (100% ethanol, followed by 50% ethanol and 50% xylene,
then 100% xylene) and mounted with resinene (Biosharp Life
Sciences). Hematoxylin and eosin-stained slides were reviewed and
the tumor zone in the paraffin-embedded specimens was selected for
tissue microarray (TMA) construction. Tissue microarrays were
constructed in accordance with a previously described method
(15). For each case, two cores
taken from the selected tumor area were used to construct the TMA.
A hollow needle was used to punch and remove bipartite cylinders
tissue cores (1.0 mm diameter) from selected donor tissue regions.
Further, the punched tissue cores were inserted into a recipient
paraffin block with a precisely spaced array pattern, using a
manual tissue arraying instrument according to the manufacturer's
protocol (Beecher Instruments, Silver Spring, Maryland, USA).
Immunohistochemistry (IHC)
IHC was performed using the standard EnVision method
(16). The paraffin-embedded tissue
blocks were cut into 4-µm thick sequential sections and the slides
were dried, deparaffinized in xylene at 20°C, rehydrated using a
graded ethanol series (100, 95, 80 and 70% ethanol and followed by
ddH2O) and immersed in 3% hydrogen peroxide for 10 min
at 20°C to block endogenous peroxidase activity. Antigens were
retrieved by pressure cooking at 120°C for 3 min in citrate buffer
(pH 6). The slides were then incubated with 5% BSA at 20°C for 15
min to prevent the non-specific reaction. Subsequently, the slides
were incubated with a primary antibody at 4°C overnight. The slides
were sequentially incubated with a secondary antibody for 30 min in
an incubator at 37°C and stained with 3,3′-diaminobenzidine.
Finally, the sections were counterstained with Mayer's hematoxylin
(Sigma-Aldrich; Merck KGaA), dehydrated (70, 80, 90 and 100%
ethanol, 2 min for each step), vitrified (100% ethanol, followed by
50% ethanol and 50% xylene, then 100% xylene) and mounted with
resinene (Biosharp Life Sciences). A negative control was obtained
by replacing the primary antibody with a normal rabbit
immunoglobulin G.
The primary antibodies used in the present study
were polyclonal rabbit anti-human COL1A2 (cat. no. YT1019; 1:200)
and monoclonal mouse anti-human COL1A1 (1:200; cat. no. YM3767)
(both ImmunoWay Biotechnology Company).
IHC evaluation
The positively stained cells were brown or yellow in
color. Immune reactivity was scored by evaluating the number of
positive cells and the positive intensity score using light
microscopy at ×100 magnification. The percentage of positive tumor
cells corresponded to the following scores: i) 0, staining in
<1% of tumor cells; ii) 1, staining in 1-25%; iii) 2, staining
in 26-50%; iv) 3, staining in 51-75%; and v) 4, staining in >75%
of tumor cells. The positive intensity score was defined as
follows: i) 0, no expression; ii) 1, weak; iii) 2, mild; iv) 3,
moderate; and v) 4, strong. The total score, ranging from 0-16, was
obtained by multiplying the proportion and intensity scores. The
IHC results were defined as negative with a total score of 0, mild
positive with a total score of 1-8 and strong positive with a total
score of 9-16. Two researchers who were blinded to the information
of the patients performed the scoring. If the results differed, a
third researcher would then participate to confirm the score.
Statistical analysis
Qualitative variables were summarized as absolute
and relative frequency (percentage). Quantitative variables were
summarized as means and standard deviations (mean ± standard
deviation). SPSS software (version 21.0; IBM Corp) was used to
perform the analysis. Pearson's χ2 or the Fisher's exact
test were applied to evaluate the association between COL1A1/COL1A2
expression levels and the categorical clinicopathological variables
of patients with HPSCC (data not shown). One-way ANOVA was applied
to evaluate the association between COL1A1/COL1A2 expression levels
with the quantitative variables of the clinicopathological features
of patients with HPSCC. If significant association was found,
Scheffe post hoc test would be performed (data not shown). The
follow-up time was defined as the time period between the day of
surgery and the end of follow-up or death. The follow up was
conducted in outpatient department. The frequency of follow up was
once every 3 months during the first two years, once every 6 months
during the third to fifth year, and once every year after 5 years.
The follow-up period ranged from 5-61 months, with a median
follow-up period of 18 months. Cox proportional hazard models were
used to investigate the associations between tumor
recurrence/survival rate and certain risk factors. Kaplan-Meier
survival analysis was also performed with log-rank tests based on
different COL1A2 staining. P<0.05 was considered to indicate a
statistically significant difference.
Results
Patient characteristics
The characteristics and pathological features of the
patients are presented in Table I.
Overall, 46/67 (68.7%) of the patients were smokers and 34/67
(50.7%) were positive for alcohol consumption. The primary tumors
of 44/67 (65.7%) of the patients were staged as T3-4 according to
the final pathological results. Histological grades in 53/67
(79.1%) of patients were grade 1 or 2. Excisional margins in 80.6%
of the patients were clear margins, whereas those in 3.0% patients
were involved margins. The regional lymph node stage of 38 (56.7%)
of the patients was N2. The anatomic stage of 89.6% the patients
was Stage III–IV. Overall, 71.6% of patients had undergone adjuvant
radiotherapy or/and chemotherapy. The 5-year locoregional
recurrence and distant metastasis rate were 38 and 50%,
respectively. The 5-year overall survival rate was 37%, while the
5-year disease-free survival rate was 22%.
 | Table I.Clinicopathological characteristics of
patients with hypopharyngeal squamous cell carcinoma (n=67). |
Table I.
Clinicopathological characteristics of
patients with hypopharyngeal squamous cell carcinoma (n=67).
| Parameter | Value |
|---|
| Age, years, mean ±
standard deviation | 58.3±8.0 |
| Sex, n (%) |
|
| Male | 65 (97.0) |
|
Female | 2 (3.0) |
| Hypertension, n
(%) |
|
| Yes | 10 (14.9) |
| No | 57 (85.1) |
| Diabetes Mellitus, n
(%) |
|
| Yes | 1 (1.4) |
| No | 66 (98.6) |
| Smoker, n (%) |
|
| Yes | 46 (68.7) |
| No | 21 (31.3) |
| Alcohol consumption,
n (%) |
|
| Yes | 34 (50.7) |
| No | 33 (49.3) |
| T classification, n
(%) |
|
| T1 | 8 (11.9) |
| T2 | 15 (22.4) |
| T3 | 24 (35.8) |
|
T4a | 17 (25.4) |
|
T4b | 3 (4.5) |
| Histological grade,
n (%) |
|
| G1 | 24 (35.8) |
| G2 | 29 (43.3) |
| G3 | 13 (19.4) |
| G4 | 1 (1.5) |
| Lymphovascular
invasion, n (%) |
|
|
Yes | 11 (16.4) |
| No | 56 (83.6) |
| Margin of removed
primary lesion, n (%) |
|
| Clear
margin | 54 (80.6) |
| Close
margin | 11 (16.4) |
|
Involved margin | 2 (3.0) |
| N classification, n
(%) |
|
| N0 | 16 (23.9) |
| N1 | 12 (17.9) |
|
N2a | 1 (1.5) |
|
N2b | 19 (28.4) |
|
N2c | 18 (26.8) |
| N3 | 1 (1.5) |
| Stage, n (%) |
|
| I | 4 (6.0) |
| II | 3 (4.5) |
|
III | 39 (58.2) |
|
Iva | 20 (29.9) |
|
Ivb | 1 (1.5) |
| Treatment, n
(%) |
|
Sx+CRT | 34 (50.7) |
|
Sx+RT | 9 (13.4) |
|
Sx+CT | 5 (7.5) |
| Sx | 19 (28.4) |
COL1A1 and COL1A2 expression patterns
in HPSCC tissues
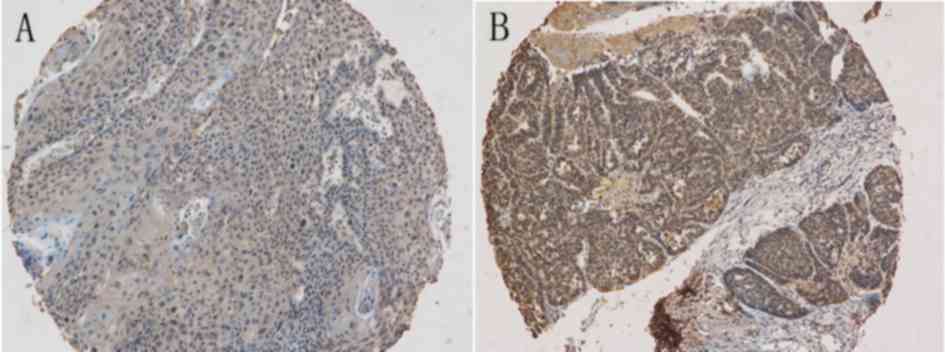
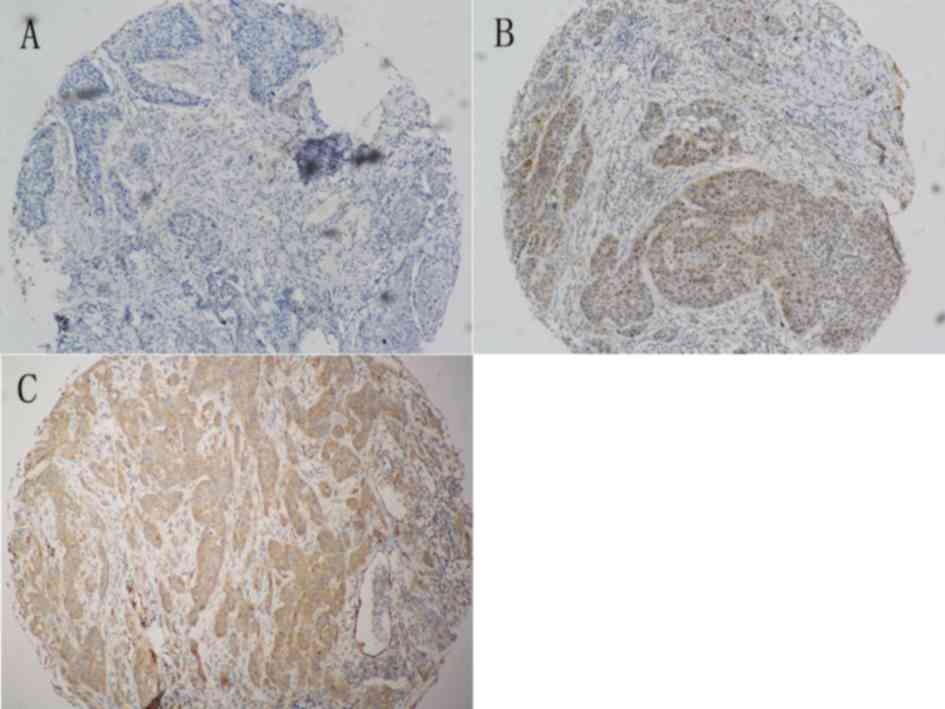
Both COL1A1 and COL1A2 expression levels were
evaluated in the tumor parenchyma component, which were primarily a
cytoplasmic pattern. COL1A1 expression was mildly positive in 40
(59.7%) of the tumors, while 27 (40.3%) of the tumors had a strong
COL1A1 expression. COL1A2 did not express in 16 (23.9%) of the
tumors, while 47 (70.1%) of the tumors had a mild COL1A2 expression
and 4 (6.0%) had a strong COL1A2 expression. Representative
immunohistochemical images of COL1A1 and COL1A2 expression in HPSCC
tissues are presented in Figs. 1 and
2.
Association of COL1A1/COL1A2
expression levels with the clinicopathological features and
survival of the patients with HPSCC
Pearson's χ2, Fisher's exact test and
one-way ANOVA test revealed no significant associations between
COL1A1/COL1A2 expression levels and patient clinicopathological
features (data not shown). Univariate cox regression analysis
revealed that the expression level of COL1A2 was a significant
prognostic factor for locoregional recurrence and disease-free
survival rate (P=0.042 and 0.020, respectively). N status was not
significantly associated with disease-free survival rate or overall
survival rate (P=0.094 and 0.075, respectively). COL1A2 expression
levels were not significantly associated with overall survival rate
(P=0.052). No other clinicopathological features significantly
predicted locoregional recurrence, distant metastasis, disease-free
survival rate or overall survival rate (Table II).
| Table II.Univariate Cox regression analysis
results for clinicopathological characteristics of patients with
hypopharyngeal squamous cell carcinoma. |
Table II.
Univariate Cox regression analysis
results for clinicopathological characteristics of patients with
hypopharyngeal squamous cell carcinoma.
|
| Locoregional
recurrence | Distant
metastasis | Disease-free
survival rate | Overall survival
rate |
|---|
|
|
|
|
|
|
|---|
| Clinicopathological
characteristic | HR (95% CI) | P-value | HR (95% CI) | P-value | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age | 1.027
(0.964-1.094) | 0.414 | 1.014
(0.920-1.117) | 0.784 | 1.009
(0.963-1.057) | 0.713 | 1.007
(0.953-1.063) | 0.811 |
| Sex | 21.326 (0.000–
8.272×106) | 0.641 | 20.923
(0.000-2.178×1013) | 0.829 | 0.834
(0.111-6.243) | 0.859 | 0.582
(0.076-4.444) | 0.602 |
| T
classification | 0.804
(0.491-1.317) | 0.386 | 1.098
(0.479-2.518) | 0.825 | 0.790
(0.536-1.166) | 0.235 | 0.934
(0.591-1.477) | 0.770 |
| Histological
grade | 1.044
(0.535-2.038) | 0.899 | 2.508
(0.583-10.791) | 0.217 | 1.347
(0.783-2.317) | 0.282 | 1.479
(0.722-2.834) | 0.238 |
| Lymphovascular
invasion | 1.716
(0.474-6.207) | 0.410 | 2.962
(0.489-17.940) | 0.237 | 1.508
(0.560-4.065) | 0.417 | 0.781
(0.178-3.430) | 0.743 |
| Margin of removed
primary lesion | 1.137
(0.717-1.804) | 0.585 | 0.865
(0.274-2.728) | 0.805 | 1.191
(0.828-1.713) | 0.347 | 1.321
(0.901-1.936) | 0.154 |
| N
classification | 1.182
(0.848-1.648) | 0.323 | 1.051
(0.651-1.698) | 0.837 | 1.240
(0.964-1.596) | 0.094 | 1.319
(0.972-1.789) | 0.075 |
| Hypertension | 0.760
(0.169-3.417) | 0.721 | 2.927
(0.557-15.384) | 0.205 | 0.923
(0.341-2.498) | 0.875 | 0.501
(0.114-2.192) | 0.359 |
| Smoking | 3.548
(0.460-27.352) | 0.224 | 0.520
(0.092-2.924) | 0.458 | 1.047
(0.390-2.813) | 0.927 | 0.960
(0.313-2.948) | 0.943 |
| Alcohol
consumption | 1.647
(0.552-4.918) | 0.371 | 1.263
(0.227-7.013) | 0.789 | 1.562
(0.686-3.558) | 0.288 | 1.809
(0.675-4.846) | 0.239 |
| Chemotherapy | 1.246
(0.426-3.639) | 0.688 | 1.954
(0.349-10.946) | 0.446 | 1.541
(0.685-3.469) | 0.296 | 1.005
(0.393-2.570) | 0.992 |
| Radiotherapy | 0.805
(0.277-2.339) | 0.690 | 0.999
(0.182-5.490) | 0.999 | 0.926
(0.413-2.073) | 0.851 | 0.616
(0.243-1.562) | 0.308 |
| COL1A1 | 1.000
(0.866-1.154) | 0.996 | 1.008
(0.779-1.304) | 0.954 | 0.957
(0.857-1.069) | 0.440 | 0.997
(0.857-1.114) | 0.732 |
| COL1A2 | 1.197
(1.006-1.425) | 0.042a | 1.106
(0.801-1.525) | 0.541 | 1.175
(1.026-1.345) | 0.020a | 1.168
(0.998-1.365) | 0.052 |
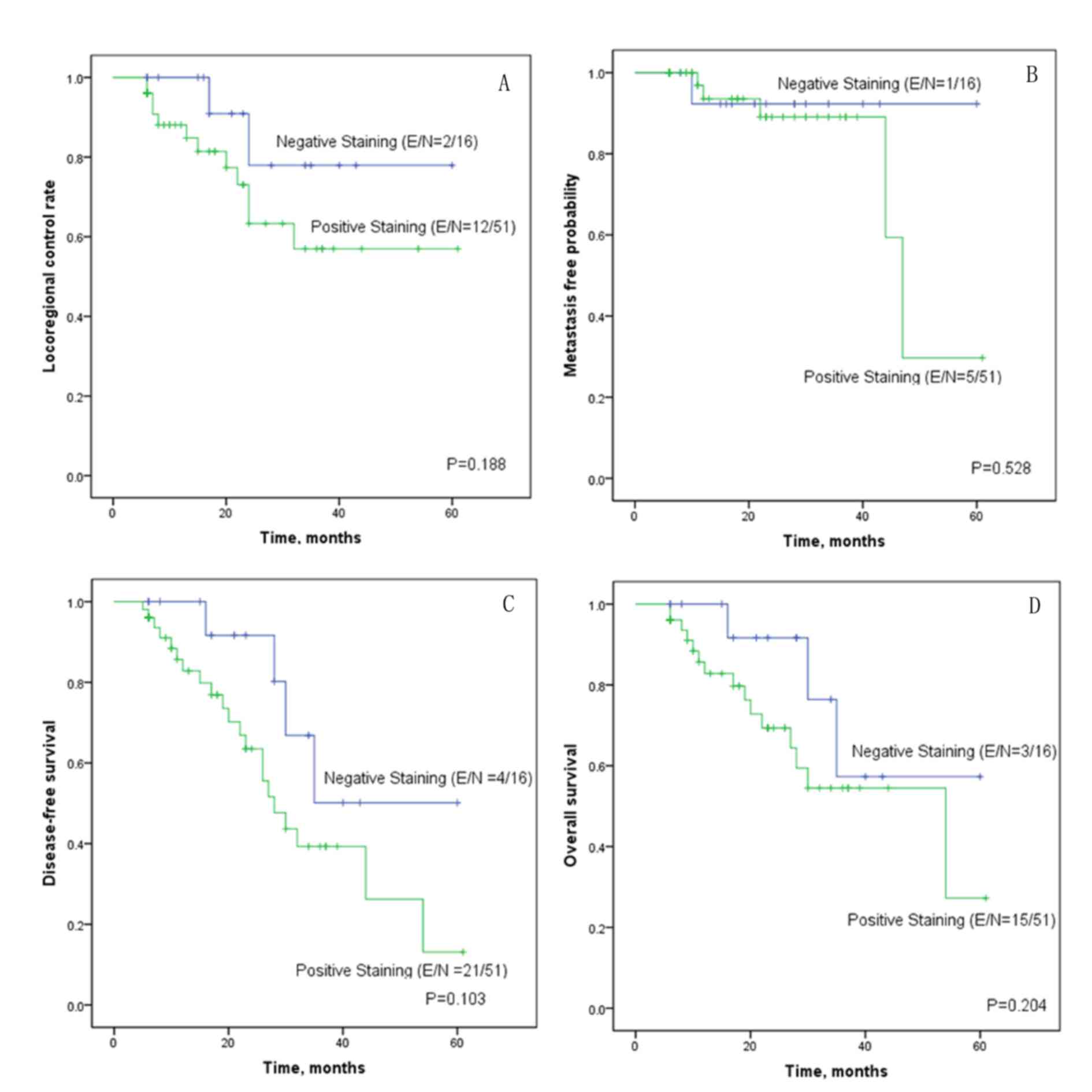
The Kaplan-Meier survival curves revealed that the
curves were separated between the negative and positive COL1A2
staining curves for locoregional control rate and disease-free
survival rate, although Log-rank tests revealed no statistical
significance (Fig. 3A-D). As the
COL1A2 staining results were calculated as a binary variable in
Kaplan-Meier survival analysis using log-rank tests, the test was
not as reliable as the Cox regression analysis, in which the COL1A2
staining results were calculated as a continuous variable.
Discussion
Although the hypopharynx is one of the least common
subsites for head and neck cancer, HPSCC has a poor prognosis
(5-yeaer survival rate, 37.5-41.3%) (2,17). Since
the hypopharynx is rich in highly anastomotic regional lymphatics,
HPSCC disseminates into the nodal basins of the neck quickly
(18). Thus, these tumors often
present at an advanced stage. In published studies, the 5-year
survival rates of patients with HPSCC have been reported to range
from 24-33% post-surgery alone and from 35-52% for post-combined
surgery and radiation therapy (19,20).
Advances in treatment techniques may improve the survival rate;
however, risk stratification is also important in developing an
individualized treatment management schedule. To date, researchers
have made efforts to identify prognostic factors, including
clinical features (21), cellular
adverse factors (22,23) and molecular markers (24,25).
This information can be used to identify patients with high-risk
HNSCC who may benefit from more aggressive therapy and frequent
follow-up following primary treatment.
Recently, the role of the microenvironment in
tumorigenesis and tumor progression has been a focus of research.
It is hypothesized that epithelial cell functions, including
cellular differentiation, migration and invasion, are regulated via
interaction with the extracellular matrix (ECM) (26). Type I collagen is a major structural
component of the ECM. It has been reported that type I collagen
remodeling in the ECM microenvironment accompanies stromal invasion
and epithelial tumorigenesis in various types of cancer (27). Type I collagen is composed of an α1
chain and α2 chain. Abnormal expression of the α1 chain and/or α2
chain impairs the function of type I collagen and tissue
homeostasis (5). The role of COL1A2
in various types of cancer remains controversial. On the one hand,
Bonazzi et al (28) and Mori
et al (5) reported that
COL1A2 was downregulated in melanoma and bladder cancer. On the
other hand, COL1A2 was observed to be upregulated in colorectal
cancer (11), gastric cancer
(29,30), breast cancer (31) and medulloblastoma (12). Koga et al (4) reported that COL1A2 methylation was
predominantly detected in advanced stage melanoma tumors. Mori
et al (5) reported that CpG
hypermethylation inactivated the COL1A2 gene and promoted the
proliferative and migratory activity of bladder cancer. In a study
by Misawa et al (13),
hypermethylation of the COL1A2 promoter occurred with a high
frequency and the expression levels of COL1A2 was downregulated in
HNSCC cell lines. In addition, disease-free survival rate was
significantly less favorable in patients with methylation in
COL1A2. However, in the present study, the upregulated expression
of COL1A2 was revealed to be associated with a high locoregional
recurrence and a less favorable disease-free survival rate in
HPSCC. One of the main differences between the two studies was that
the present study primarily focused on patients with HPSCC, while
Misawa et al (13) grouped
HPSCC with oropharyngeal, laryngeal and other types of cancer, and
HPSCC compiled 25% of cases. This may have resulted in the
different conclusion of the two studies.
There were certain limitations to the present study.
As a preliminary study, the present study only assessed the
expression levels of COL1A1 and COL1A2 using IHC in HPSCC and
analyzed the association between the expression levels of
COL1A1/COL1A2 and the clinicopathological characteristics, relapse
and survival rate of the patients. Yet, previous studies have
demonstrated a reciprocal interaction between urothelial carcinoma
cells and the stromal compartment, which modulates the epithelial
differentiation and progression of bladder cancer via paracrine
signaling pathways, such as the Sonic hedgehog and Wnt/bone
morphogenic pathways (6,7). The mechanisms via which COL1A2
expression influences the locoregional recurrence and disease-free
survival rate in HPSCC, and whether it reacts with other
biomarkers, remains unclear; thus, further studies are required to
elucidate these mechanisms. In the near future, in vivo and
in vitro experiments should be performed to investigate
whether regulation of COL1A2 expression could influence expression
of other proteins and affect cancer cell migration, invasion and
tumor progression. Due to the relative rarity of hypopharyngeal
types of cancer, the patients included in the present study were
relatively small in number and certain results should be confirmed
in further studies with a larger population size.
In conclusion, the expression levels of COL1A2 have
value as a prognostic factor of HPSCC in risk stratification and
may assist in individual clinical management for patients with
HPSCC in the future.
Acknowledgements
Not applicable.
Funding
The present study was supported by The National
Natural Science Foundation of China (grant nos. 81570935 and
81771018).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
PL and PT designed the study, analyzed the data and
wrote the manuscript. JP and LL acquired the general data of the
patients and assisted in the analysis of data. GH and YS performed
tissue microarray construction, immunohistochemical staining and
scoring. YZ was involved in designing the study, analyzing the data
and reviewing the manuscript. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
The present study was approved by The Ethics
Committee of Sun Yat-sen Memorial Hospital, Sun Yat-sen University
(approval no. SYSEC-KY-KS-2018-155). Patients who participated in
this research had complete clinical data. Written informed consent
was provided by the patients or their guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Pingree TF, Kim DR, Owen R and Larry D:
Treatment of hypopharyngeal carcinoma: A 10-year review of 1,362
cases. Laryngoscope. 97:901–904. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Newman JR, Connolly TM, Illing EA, Kilgore
ML, Locher JL and Carroll WR: Survival trends in hypopharyngeal
cancer: A population-based review. Laryngoscope. 125:624–629. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chu PY and Chang SY: Reconstruction of the
hypopharynx after surgical treatment of squamous cell carcinoma. J
Chin Med Assoc. 72:351–355. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Koga Y, Pelizzola M, Cheng E, Krauthammer
M, Sznol M, Ariyan S, Narayan D, Molinaro AM, Halaban R and
Weissman SM: Genome-wide screen of promoter methylation identifies
novel markers in melanoma. Genome Res. 19:1462–1470. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Mori K, Enokida H, Kagara I, Kawakami K,
Chiyomaru T, Tatarano S, Kawahara K, Nishiyama K, Seki N and
Nakagawa M: CpG hypermethylation of collagen type I alpha 2
contributes to proliferation and migration activity of human
bladder cancer. Int J Oncol. 34:1593–1602. 2009.PubMed/NCBI
|
|
6
|
Shin K, Lim A, Zhao C, Sahoo D, Pan Y,
Spiekerkoetter E, Liao JC and Beachy PA: Hedgehog signaling
restrains bladder cancer progression by eliciting stromal
production of urothelial differentiation factors. Cancer Cell.
26:521–533. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Shin K, Lee J, Guo N, Kim J, Lim A, Qu L,
Mysorekar IU and Beachy PA: Hedgehog/Wnt feedback supports
regenerative proliferation of epithelial stem cells in bladder.
Nature. 472:110–114. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Gao F, Li M, Xiang R, Zhou X, Zhu L and
Zhai Y: Expression of CLDN6 in tissues of gastric cancer patients:
Association with clinical pathology and prognosis. Oncol Lett.
17:4621–4625. 2019.PubMed/NCBI
|
|
9
|
Zhai JM, An YH, Wang W, Fan YG and Yao GL:
IL-32 expression indicates unfavorable prognosis in patients with
colon cancer. Oncol Lett. 17:4655–4660. 2019.PubMed/NCBI
|
|
10
|
Zhu YZ, Zhou K, Ruan LL, Sun F, Wang G and
Li WF: Metadherin overexpression in perihilar cholangiocarcinoma is
associated with lymph node metastasis and poor prognosis. Oncol
Lett. 17:4514–4520. 2019.PubMed/NCBI
|
|
11
|
Zou X, Feng B, Dong T, Yan G, Tan B, Shen
H, Huang A, Zhang X, Zhang M, Yang P, et al: Up-regulation of type
I collagen during tumorigenesis of colorectal cancer revealed by
quantitative proteomic analysis. J Proteomics. 94:473–485. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Liang Y, Diehn M, Bollen AW, Israel MA and
Gupta N: Type I collagen is overexpressed in medulloblastoma as a
component of tumor microenvironment. J Neurooncol. 86:133–141.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Misawa K, Kanazawa T, Misawa Y, Imai A,
Endo S, Hakamada K and Mineta H: Hypermethylation of collagen α2
(I) gene (COL1A2) is an independent predictor of survival in head
and neck cancer. Cancer Biomark. 10:135–144. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
National Comprehensive Cancer Network
(NCCN) clinical practice guidelines in oncology, . Head and Neck
Cancer. Version 1. 2019.
|
|
15
|
Kononen J, Bubendorf L, Kallioniemi A,
Bärlund M, Schraml P, Leighton S, Torhorst J, Mihatsch MJ, Sauter G
and Kallioniemi OP: Tissue microarrays for high-throughput
molecular profiling of tumor specimens. Nat Med. 4:844–847. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Chen J, Li S, Xiao Y, Zou X, Zhang X, Zhu
M, Cai M and Xie D: p53R2 as a novel prognostic biomarker in
nasopharyngeal carcinoma. BMC Cancer. 17:8462017. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Carvalho AL, Nishimoto IN, Califano JA and
Kowalski LP: Trends in incidence and prognosis for head and neck
cancer in the United States: A site-specific analysis of the SEER
database. Int J Cancer. 114:806–816. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Koo BS, Lim YC, Lee JS, Kim YH, Kim SH and
Choi EC: Management of contralateral N0 neck in pyriform sinus
carcinoma. Laryngoscope. 116:1268–1272. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kuo P, Chen MM, Decker RH, Yarbrough WG
and Judson BL: Hypopharyngeal cancer incidence, treatment, and
survival: Temporal trends in the United States. Laryngoscope.
124:2064–2069. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Wang YL, Feng SH, Zhu J, Zhu J, Zhu GP, Li
DS, Wang Y, Zhu YX, Sun GH and Ji QH: Impact of lymph node ratio on
the survival of patients with hypopharyngeal squamous cell
carcinoma: A population-based analysis. PLoS One. 8:e566132013.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Abrahão R, Anantharaman D, Gaborieau V,
Abedi-Ardekani B, Lagiou P, Lagiou A, Ahrens W, Holcatova I, Betka
J, Merletti F, et al: The influence of smoking, age and stage at
diagnosis on the survival after larynx, hypopharynx and oral cavity
cancers in Europe: The ARCAGE study. Int J Cancer. 143:32–44. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Yang J, Hsueh CY, Cao W and Zhou L:
Pretreatment lymphocyte-to-monocyte ratio as an independent
prognostic factor for hypopharyngeal squamous cell carcinoma. Acta
Otolaryngol. 138:734–740. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kuwahara T, Takahashi H, Sano D, Matsuoka
M, Hyakusoku H, Hatano T, Hiiragi Y and Oridate N: Fibrinogen and
neutrophil-to-lymphocyte ratio predicts survival in patients with
advanced hypopharyngeal squamous cell carcinoma. Anticancer Res.
38:5321–5330. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Chen Y, Liu Y, Ni H, Ding C, Zhang X and
Zhang Z: FoxM1 overexpression promotes cell proliferation and
migration and inhibits apoptosis in hypopharyngeal squamous cell
carcinoma resulting in poor clinical prognosis. Int J Oncol.
51:1045–1054. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wu H, Chen J, Wang Q, Yin Y, Da P, Le H,
Zhang Z and Qiu X: Abnormal expression of HAX-1 is associated with
cellular proliferation and migration in human hypopharyngeal
squamous cell carcinoma. Mol Med Rep. 16:4664–4670. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Lu P, Weaver VM and Werb Z: The
extracellular matrix: A dynamic niche in cancer progression. J Cell
Biol. 196:395–406. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Egeblad M, Rasch MG and Weaver VM: Dynamic
interplay between the collagen scaffold and tumor evolution. Curr
Opin Cell Biol. 22:697–706. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Bonazzi VF, Nancarrow DJ, Stark MS, Moser
RJ, Boyle GM, Aoude LG, Schmidt C and Hayward NK: Cross-platform
array screening identifies COL1A2, THBS1, TNFRSF10D and UCHL1 as
genes frequently silenced by methylation in melanoma. PLoS One.
6:e261212011. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Zhuo C, Li X, Zhuang H, Tian S, Cui H,
Jiang R, Liu C, Tao R and Lin X: Elevated THBS2, COL1A2, and SPP1
expression levels as predictors of gastric cancer prognosis. Cell
Physiol Biochem. 40:1316–1324. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Rong L, Huang W, Tian S, Chi X, Zhao P and
Liu F: COL1A2 is a novel biomarker to improve clinical prediction
in human gastric cancer: Integrating bioinformatics and
meta-analysis. Pathol Oncol Res. 24:129–134. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Lin J, Goldstein L, Nesbit A and Chen MY:
Influence of hormone receptor status on spinal metastatic lesions
in patients with breast cancer. World Neurosurg. 85:42–48. 2016.
View Article : Google Scholar : PubMed/NCBI
|