Introduction
Anti-programmed death 1 (PD-1)/anti-programmed death
1 ligand 1 (PD-L1) antibodies pembrolizumab, nivolumab and
atezolizumab are becoming promising new treatment options for a
broad range of refractory malignancies; this has resulted in their
approval by the US Food and Drug Administration for the treatment
of >14 different types of cancer, including non-small cell lung
cancer (NSCLC) (1), malignant
melanoma (2), renal cell carcinoma
(3), Hodgkin's lymphoma (4) and bladder cancer (5).
However, despite encouraging clinical effects,
PD-1/PD-L1-targeting agents have also been associated with a
spectrum of immune-related adverse events (irAEs), including skin
rashes, neurotoxicity, myocarditis, colitis, hepatitis, endocrine
dysfunction and pneumonitis (6).
Among these irAEs, pneumonitis is rare, but potentially
life-threatening. Immune-mediated pneumonitis, also termed
checkpoint inhibitor pneumonitis (CIP), was initially described in
a phase I trial of nivolumab in patients with different
malignancies, in which three (2%) patients died of severe
pneumonitis (7). CIP is defined as
the development of dyspnea and/or other respiratory symptoms
(including cough and hypoxia) in the presence of new pulmonary
infiltrates on chest imaging and in the absence of new infection
(8). To date, CIP has been reported
in ≤5% of patients in clinical trials, and the rates of grade 3/4
pneumonitis are similar across tumor types. However, due to
pneumonitis, patients with NSCLC appear to exhibit a higher
treatment-related mortality rate (9–16). The
real-world incidence of CIP may be even higher, especially as
immune checkpoint inhibitors (ICIs) are currently being widely used
in non-clinical trial settings. Thus, the occurrence of CIP in
NSCLC has become regarded as an area of special interest.
To date, the molecular mechanism of CIP has not been
fully elucidated. Current hypotheses suggest a dysregulated
interaction between effector and regulatory T cells (Tregs) in the
pulmonary interstitium, ultimately leading to an inflammatory
response (17). In 2013,
Barjaktarevic et al (18)
revealed an organizing pneumonia pattern in patients with
pneumonitis caused by an anti-cytotoxic T lymphocyte-associated
antigen-4 antibody. Naidoo et al (19) examined tissue samples from 11
patients treated with anti-PD-1/PD-L1 therapy at the Memorial Sloan
Kettering Cancer Center, and found that interstitial fibrosis
(4/11) and organizing pneumonia (3/11) were the most common
pathological manifestations. Despite the aforementioned studies, a
considerable lack of data has been reported in regard to the
etiology of CIP. Rapid clinical improvement upon administration of
corticosteroids indicates an immune-mediated mechanism, and
suggests that T cells may serve an important role in the
pathogenesis of CIP.
Interleukin (IL)-17 is an important cytokine for
regulating immune homeostasis, and the aberrant expression of IL-17
has been suggested to contribute to a number of pathologies,
including asthma, pneumonitis and the generation or exacerbation of
pulmonary fibrosis (20). IL-35, a
recently identified heterodimeric cytokine, has been implicated to
serve a crucial role in several immune-associated diseases, such as
autoimmune diseases and viral infections, as well as in tumors
(21). Higher levels of serum IL-35
are reportedly associated with pulmonary fibrosis (22). Thus, the present study aimed to
dynamically determine the alterations in the expression levels of
IL-17A and IL-35 in the peripheral blood and bronchoalveolar lavage
fluid (BALF) of patients with NSCLC-related CIP, as well as to
synchronically detect different subsets of T cells, including
helper T lymphocytes (Th)1, Th2 and Th17 cells, and
CD4+CD25+ forkhead box P3 (Foxp3)+
Tregs, in the peripheral blood.
Materials and methods
Patients
Blood specimens from 13 patients with NSCLC
diagnosed with CIP who received anti-PD-1/PD-L1 therapy between
July 2016 and December 2018 at the Department of Medical Oncology,
The First Affiliated Hospital of Zhejiang University (Hangzhou,
China), were collected within 2 weeks of immuno-oncology (IO)
treatment, prior to every two cycles of immunotherapy and upon
onset of CIP. A total of 9 patients underwent bronchoscopy and BALF
was collected at baseline and upon CIP diagnosis during
bronchoscopy examination; 20 patients with locally
advanced/metastatic NSCLC with available constitutive blood samples
during anti-PD-1/PD-L1 treatment were included as controls, and 10
of them received bronchoscopy examination both pre- (no more than
10 days before treatment) and post-ICI treatment (after 2–5 cycles
of ICI treatment). BALF was collected from the middle lobe in
control patients and a newly infiltrated area in patients with CIP
during bronchoscopy. The present study was a planned analysis with
a prospective observational protocol approved by the Ethical
Committee of The First Affiliated Hospital of Zhejiang University.
Written informed consent was obtained from all subjects.
Radiological and clinical
assessment
A chest computed tomography (CT) scan was mandatory
for all patients at baseline, during therapy, at follow-up and upon
clinical suspicion of CIP. According to the American Thoracic
Society/European Respiratory Society 2002 classification (23,24), the
occurrence of new and diffuse lung parenchymal abnormalities on CT
scans, such as ground-glass opacities, consolidations, interlobular
septal thickening and intralobular lines, micronodules,
bronchiectasis and architectural distortion, may correlate with
drug-induced interstitial pneumonitis.
The diagnosis of CIP was based on radiological data
and clinical symptoms following the guidelines of the European
Society for Medical Oncology, the Society for Immunotherapy of
Cancer, and the American Society for Clinical Oncology/National
Comprehensive Cancer Network, which include the use of imaging
(chest X-ray and/or CT), pulse oximetry and an infectious work-up
(including nasal swab, sputum, blood and urine cultures) (25–28).
Patients were only diagnosed with CIP after the exclusion of other
causes of pulmonary disorders, such as pulmonary infection,
progression of lung cancer or radiation pneumonitis based on a
multidisciplinary discussion between radiologists, oncologists,
pulmonologists and infectious disease specialists, although the
diagnostic criteria of CIP was inconsistent. CIP severity (G1-G5)
was defined according to the Common Terminology Criteria for
Adverse Events, version 4.0 (29).
Detection of IL-17A and IL-35 in serum
or BALF by ELISA
Peripheral blood and BALF samples were collected
from patients and stored at −80°C for subsequent experimentation;
the samples were analyzed within 90 days of collection. The
concentrations of IL-35 and IL-17A in patients with CIP and
controls were quantified using cytokine-specific ELISA kits (cat.
no. DY6456 for IL-35 and D1700 for IL-17A; R&D Systems, Inc.)
according to the manufacturer's protocols. Briefly, 100 µl serum or
BALF was added to microplate strips and incubated at room
temperature for 2–3 h. After a total of three washes, primary
antibodies for IL-35 or IL-17A were added and incubated for 1 h at
room temperature. The wash step was then repeated. Finally, after
incubation at room temperature with substrate solution for 30 min,
stop solution (acid stop solution provided with IL-17A kit and
2NH2SO4 with IL-35 kit (both R&D Systems,
Inc.) was added and the colorimetric density of each well was
determined at a wavelength of 450 nm using a Multimode Reader
(Tecan Infinite™ F200). All samples were assayed in
triplicate.
Flow cytometric detection of T-cell
subsets
The frequencies of different T-cell subsets in 13
patients with CIP and 20 control subjects were detected by flow
cytometry within 2 weeks prior to IO treatment, at every two cycles
of immunotherapy and at the onset of CIP. Peripheral blood
mononuclear cells (PBMCs) were isolated from fresh heparinized
blood by standard Ficoll-Hypaque density centrifugation (Biochrom,
Ltd.) at room temperature and 670 × g for 30 min. PBMC isolation
was performed ≤2 h after peripheral blood collection. To exclude
non-specific binding, isotype-matched antibodies (mouse IgG1
monoclonal κ antibody, cat. no. 554679, 1 µl/1 million cells, BD
Biosciences) were used as controls; ≥2×105 cells were
analyzed using a FC500 MPL flow cytometer and CXP-analysis version
2.2 (both Beckman Coulter, Inc.). For Treg analysis, cell surface
staining was performed with fluorescein isothiocyanate
(FITC)-conjugated anti-CD25 (cat. no. 560990, 20 µl/1 million
cells, BD Biosciences), phycoerythrin (PE)-conjugated anti-Foxp3
(cat. no. 560046, 20 µl/1 million cells, BD Biosciences),
PE-cy5-conjugated anti-CD4 (cat. no. 555348, 20 µl/1 million cells,
BD Biosciences) or the appropriate isotype controls (mouse IgG1
monoclonal κ antibody, cat. no. 554679, 1 µl/1 million cells, BD
Biosciences). The cells were incubated with the antibodies for 20
min at room temperature in the dark, followed by washing in PBS and
subsequent flow cytometric analysis. For cytotoxic and helper
T-cell subsets, the cells were incubated with PE-conjugated
anti-CD3 (cat. no. 555333, 20 µl/1 million cells, BD Biosciences)
and PE-cy5-conjugated anti-CD4/CD8 (cat. no. 555348, 20 µl/1
million cells for CD4 and cat. no. 557750, 5 µl/1 million cells for
CD8, both BD Biosciences) at 4°C for 15 min, fixed at 4°C for 10
min using fixation buffer (cat. no. 554714, BD Biosciences) and
permeabilized at room temperature for 15 min using permeabilization
wash buffer (cat. no. 554714, BD Biosciences). The cells were then
stained with FITC-conjugated anti-interferon-γ (IFN-γ, cat. no.
554551, 1 µl/1 million cells, BD Biosciences) or anti-IL-4
antibodies (cat. no. 559333, 20 µl/1 million cells, BD Biosciences)
at room temperature for 30 min and assessed by flow cytometry using
the FC500 MPX flow cytometer with MXP software version 2.2 (Beckman
Coulter, Inc.). The frequencies of Tregs
(CD4+CD25+Foxp3+), and Th1
(CD3+CD8−IFN-γ+) and Th2
(CD3+CD8−IL-4+) cells were
expressed as a percentage of the CD4+ T-cell population
by sequential gating on lymphocytes and CD4+ T
cells.
Statistical analysis
The data were analyzed using SPSS software version
22 (IBM Corp). Categorical data are summarized as counts and
percentages, and quantitative data are expressed as the mean ±
standard deviation or the median and quartile range according to
their distribution. The χ2 test was used to analyze the
baseline data of patients with NSCLC. The differences between
multiple groups were determined using Kruskal-Wallis with Dunn's
multiple comparisons test. The association between measures was
analyzed by Pearson's correlation with Bonferroni's correction.
P<0.05 (two-tailed) was considered to indicate a statistically
significant difference.
Results
Patient characteristics
A total of 13 patients with NSCLC developed CIP
during immunotherapy between July 2016 and December 2018; 20
patients with NSCLC without CIP were included as controls. All
patient baseline and treatment characteristics are presented in
Table I. The age of the patients
ranged between 36 and 82 years (mean, 66.8 years); the majority
were Eastern Cooperative Oncology Group performance status (ECOG
PS) (30) 0–1 (n=22; 66.7%) and
received single-agent anti-PD-1/PD-L1 therapy (n=29; 87.9%).
PD-1/PD-L1 antibodies included nivolumab (3 mg/kg; Bristol-Myers
Squibb), pembrolizumab (2 mg/kg; Merck Sharp & Dohme, Ltd.),
atezolizumab (1,200 mg; Roche Diagnostics) and camrelizumab (200
mg; Jiangsu Hengrui Medicine Co., Ltd.). In total, 4 patients
(12.1%) received immunotherapy combined with chemotherapy. PD-L1
was detected in 14 (58.3%) of the 24 patients for whom PD-L1
immunostaining (IHC 22C3 pharmDX, Agilent Technologies, Inc.) was
available. None of the considered variables (age, sex, ECOG PS,
smoking status, previous COPD, histological type, mutation status,
PD-L1 expression, metastatic sites, type of immunotherapy regimen
or previous treatment lines) were significantly different between
the patients with CIP and the controls (Table I).
 | Table I.Baseline characteristics of patients
with NSCLC. |
Table I.
Baseline characteristics of patients
with NSCLC.
|
Characteristics | Total (n=33) | Patients with CIP
(n=13) | Control patients
(n=20) |
P-valuea |
|---|
| Age, years |
|
|
| 0.930 |
|
≤65 | 20 | 8 | 12 |
|
|
>65 | 13 | 5 | 8 |
| Sex |
|
|
| 0.801 |
|
Male | 22 | 9 | 13 |
|
|
Female | 11 | 4 | 7 |
|
| ECOG PS |
|
|
| 0.614 |
|
0-1 | 22 | 8 | 14 |
|
| 2 | 11 | 5 | 6 |
|
| Smoking status |
|
|
| 0.960 |
|
Never | 3 | 1 | 2 |
|
|
Present | 7 | 3 | 4 |
|
|
History | 23 | 9 | 14 |
|
| Previous COPD |
|
|
| 0.829 |
|
Yes | 16 | 6 | 10 |
|
| No | 17 | 7 | 10 |
|
| Histological
type |
|
|
| 0.619 |
|
Squamous | 16 | 7 | 9 |
|
|
Non-squamous | 17 | 6 | 11 |
|
| Mutation
status |
|
|
| 0.343 |
|
EGFR | 4 | 2 | 2 |
|
|
ALK | 0 | 0 | 0 |
|
|
ROS1 | 0 | 0 | 0 |
|
|
KRAS | 5 | 1 | 4 |
|
| Previous target
therapy |
|
|
| 0.906 |
|
Yes | 4 | 2 | 2 |
|
| No | 0 | 0 | 0 |
|
| PD-L1 expression
(22C3) |
|
|
| 0.534 |
|
≤1% | 10 | 5 | 5 |
|
|
>1% | 14 | 4 | 10 |
|
| ND | 9 | 4 | 5 |
|
| Pathological
stage |
|
|
| 0.900 |
|
IIIB | 8 | 3 | 5 |
|
| IV | 25 | 10 | 15 |
|
| Metastatic sites,
n |
|
|
| 0.663 |
|
1-2 | 24 | 10 | 14 |
|
| ≥3 | 9 | 3 | 6 |
|
| Treatment line |
|
|
| 0.338 |
|
1st | 8 | 2 | 6 |
|
|
≥2nd | 25 | 11 | 14 |
|
| Immunotherapy |
|
|
| 0.886 |
|
Nivolumab | 8 | 3 | 5 |
|
|
Pembrolizumab | 10 | 5 | 5 |
|
|
Atezolizumab | 6 | 2 | 4 |
|
|
Camrelizumab | 5 | 1 | 4 |
|
| Pembro
+ Chemo | 4 | 2 | 2 |
|
Clinical features of patients with
CIP
Of the patients who developed CIP (n=13),
pneumonitis occurred after a median of 3 cycles of immunotherapy
(range, 1–6). The median time between initial immunotherapy and the
onset of CIP was 49.8 days (range, 18–140 days); 5 patients (38.5%)
initially presented with dyspnea, and 6 (46.2%) with a cough,
whereas 2 patients (15.4%) were asymptomatic. Most of the patients
exhibited grade 2–4 pneumonitis (11/13, 84.6%), with the exception
of 2 patients with grade 5 (15.4%). In addition, 11 patients
(84.6%) with pneumonitis were treated with systemic steroids for a
median of 24 days (range, 5–128 days). Of these patients, 4
completely recovered (30.8%) and 7 improved (53.8%), whereas 2 were
admitted to the intensive care unit and succumbed to pneumonitis
progression (15.4%) (Table II).
| Table II.Clinical features, treatment and
outcome of CIP. |
Table II.
Clinical features, treatment and
outcome of CIP.
| Variable | Patients with CIP
(n=13) |
|---|
| Immunotherapy
cycles, mean (range) | 3 (1–6) |
| Time to CIP, days,
mean (range) | 49.8 (18–140) |
| Clinical symptoms,
n (%) |
|
|
Dyspnea | 5 (38.5) |
|
Cough | 6 (46.2) |
|
Asymptotic | 2 (15.4) |
| Severity of CIP, n
(%) |
|
| G2 | 2 (15.4) |
| G3 | 5 (38.5) |
| G4 | 4 (30.8) |
|
G5, | 2 (15.4) |
|
Steroid, n (%) | 11 (84.6) |
| Outcome, n (%) |
|
|
Recovered | 4 (30.8) |
|
Improved | 7 (53.8) |
|
Succumbed | 2 (15.4) |
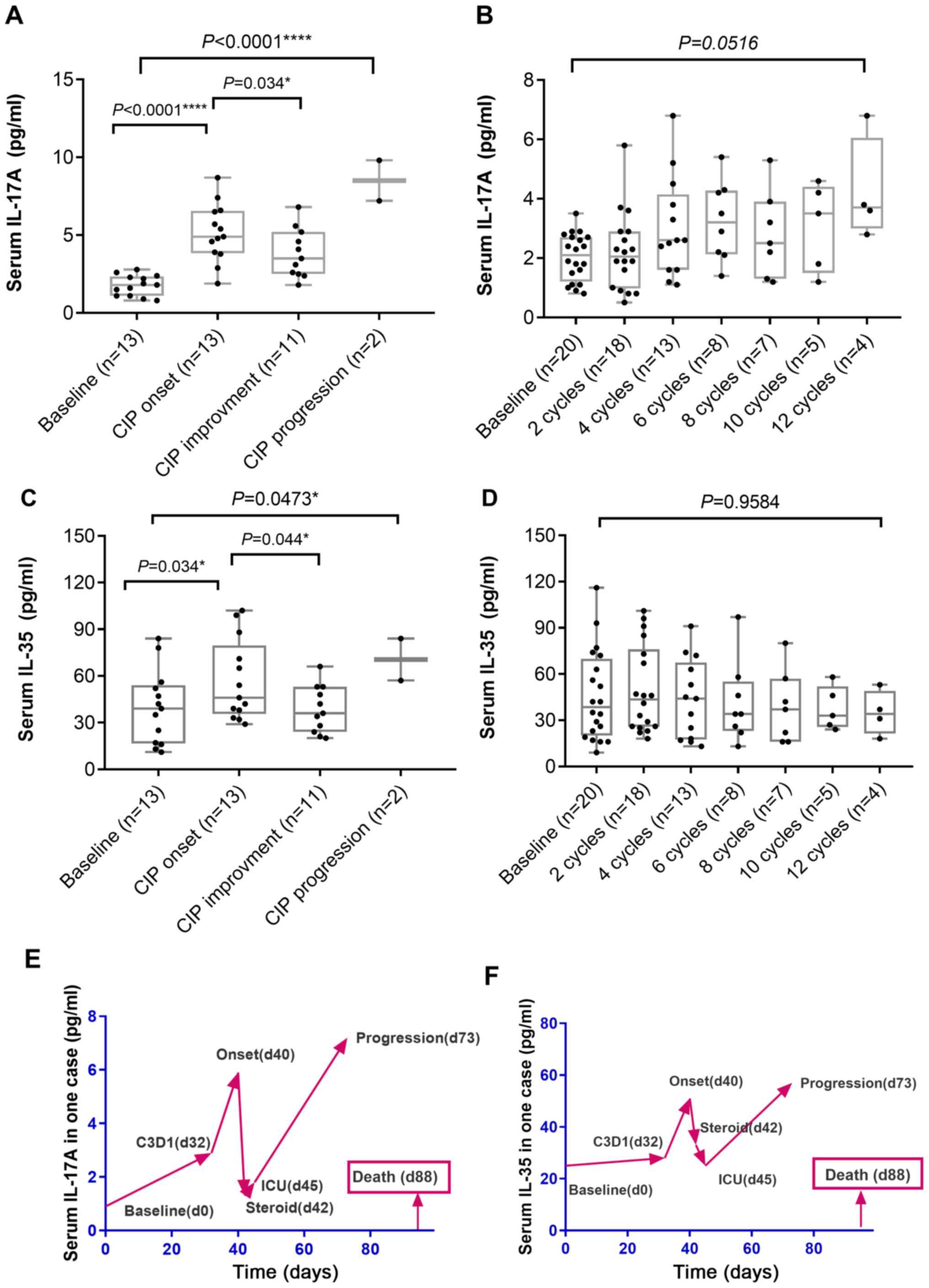
Alterations in the serum levels of
IL-17A and IL-35 are associated with CIP severity
The serum levels of IL-17A and IL-35 in the patients
with CIP and controls during immunotherapy were longitudinally
monitored within 2 weeks prior to IO treatment, at every two cycles
of immunotherapy and upon onset of CIP. In patients with CIP
(n=13), median serum IL-17A levels increased significantly at the
time of CIP diagnosis compared with baseline levels (P<0.001)
and significantly decreased upon clinical recovery or improvement
(n=11; P=0.034) (Fig. 1A). In 2 CIP
cases presenting with pneumonitis progression, the IL-17A level
decreased upon administration of systemic steroids compared with
CIP onset, but further increased at a later stage (Fig. 1E). Of note, the median serum levels
of IL-35 displayed the same pattern as those of IL-17A (Fig. 1C and F). In the control patients with
NSCLC who received ICI treatment (n=20), the median serum levels of
IL-17A and IL-35 increased slightly during immunotherapy compared
with the baseline; however, no significant elevation in serum
IL-17A or IL-35 levels was detected (Fig. 1B and D).
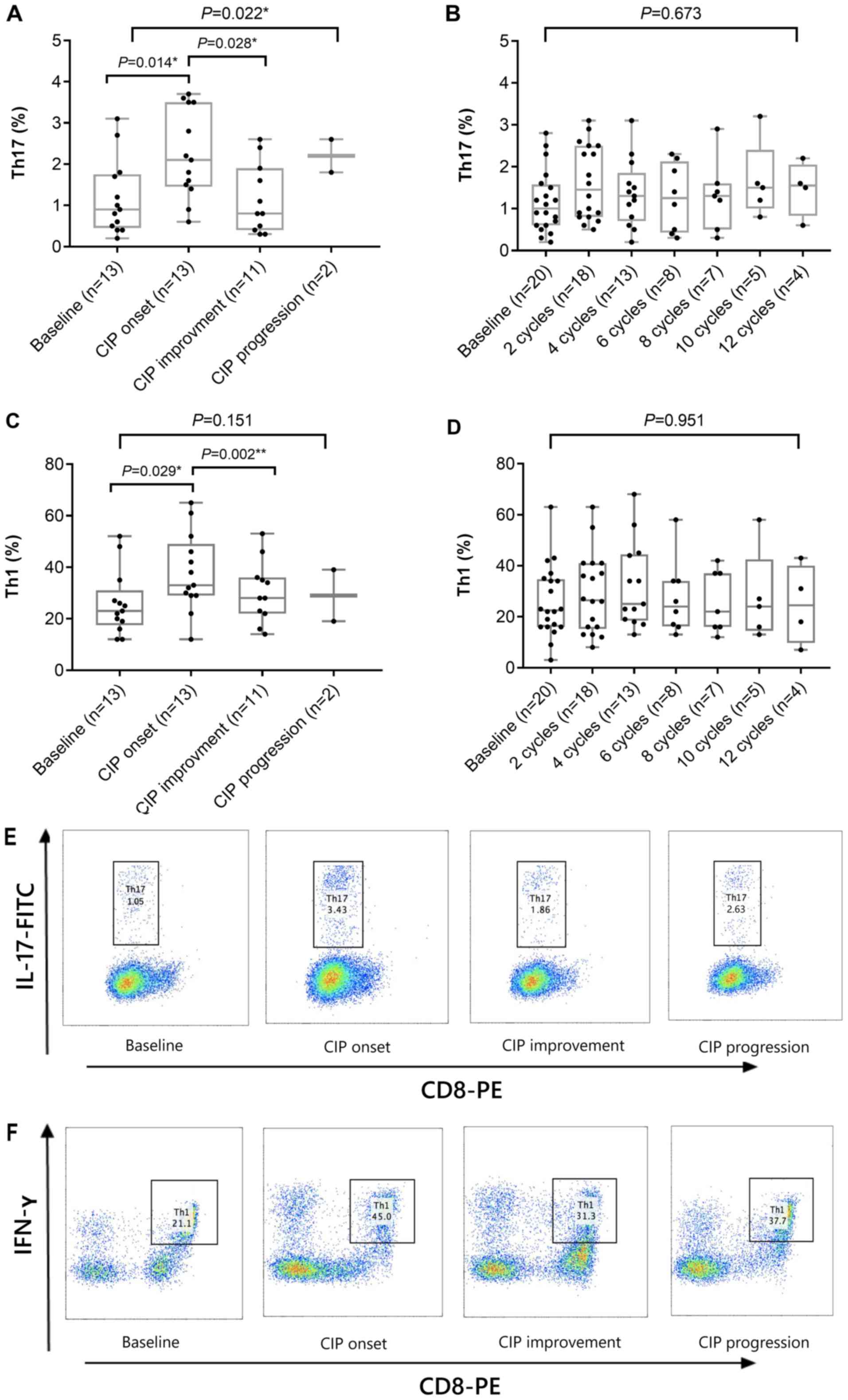
High frequencies of Th1 and Th17 cells
are associated with the development of CIP
Next, the frequencies of different T-cell subsets
were assessed by flow cytometry in 13 patients with CIP and 20
control subjects. As presented in Fig.
2, the percentages of Th17 and Th1 cells in patients with CIP
were significantly higher following the onset of CIP compared with
those at baseline (P=0.014 and P=0.029; Fig. 2A and C, respectively), whereas no
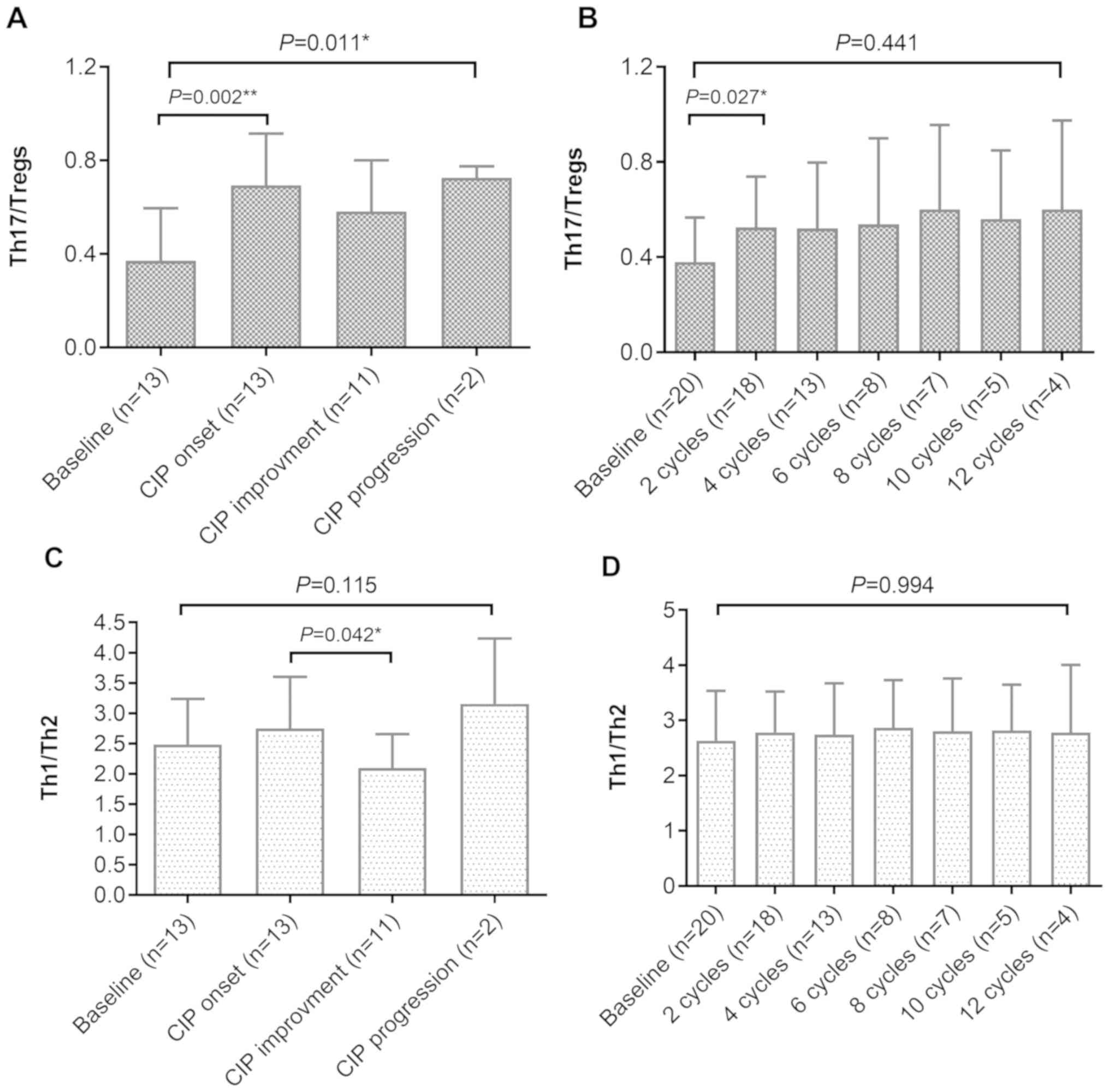
significant changes were detected in the control group (Fig. 2B and D). As a result, the ratios of
Th17 to Tregs in patients with CIP (upon onset of CIP) were
significantly higher compared with those at baseline (P=0.002;
Fig. 3A), and the ratios of Th1 to
Th2 were significantly higher compared with those following
improvement (P=0.042; Fig. 3C). In
the control group, the ratio of Th17 to Tregs in patients with
NSCLC also increased following ICI treatment compared with that at
baseline (P=0.441; Fig. 3B);
however, no increased ratios of Th1 to Th2 were observed in these
patients (Fig. 3D). These results
suggested that higher frequencies of Th1 and Th17 cells, as well as
higher ratios of Th17 to Tregs and Th1 to Th2 cells, may be
associated with the development of CIP in patients with NSCLC.
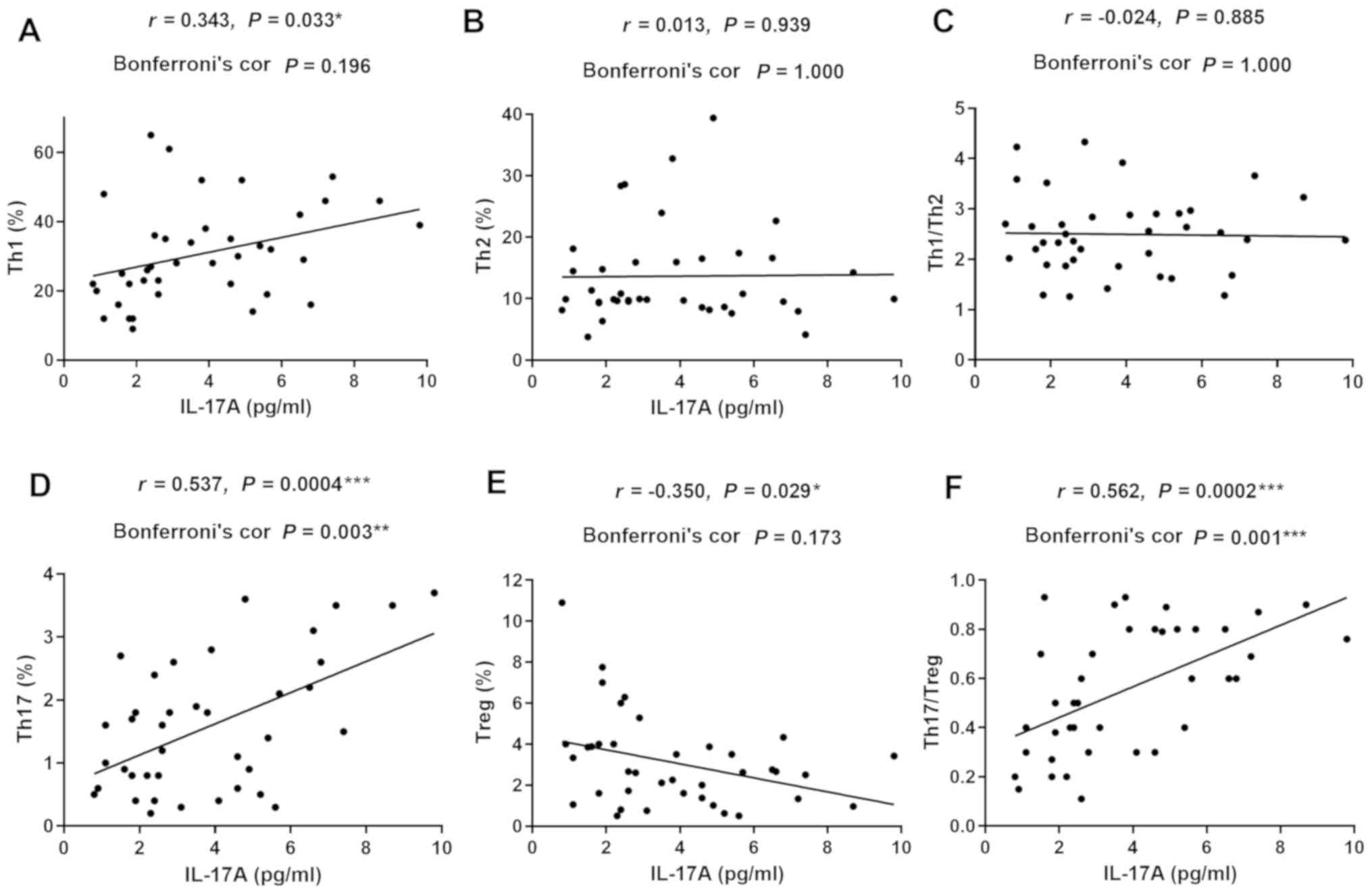
Association between serum IL-17A and
IL-35 levels and the percentages of different T-cell subsets in
patients with NSCLC and CIP
To further clarify the roles of IL-17A and IL-35 in
CIP, the correlation between the serum levels of these cytokines
and the percentages of different T-cell subsets were investigated
in patients with NSCLC and CIP (Fig.
4 for IL-17A and Fig. 5 for
IL-35). The levels of serum IL-17A were positively correlated with
the percentage of Th17 cells (r=0.537; P=0.003; Fig. 4D) and the ratio of Th17 to Tregs
(r=0.562; P=0.001; Fig. 4F). Serum
IL-17A levels displayed no significant correlation with the
frequency of Th1, Th2, Tregs or the ratio of Th1 to Th2 cells in
patients with CIP (r=0.343; P=0.196; Fig. 4A; r=0.013; P=1.000; Fig. 4B; r=−0.350; P=0.173; Fig. 4E; and r=−0.024; P=1.000; Fig. 4C). The levels of serum IL-35 were
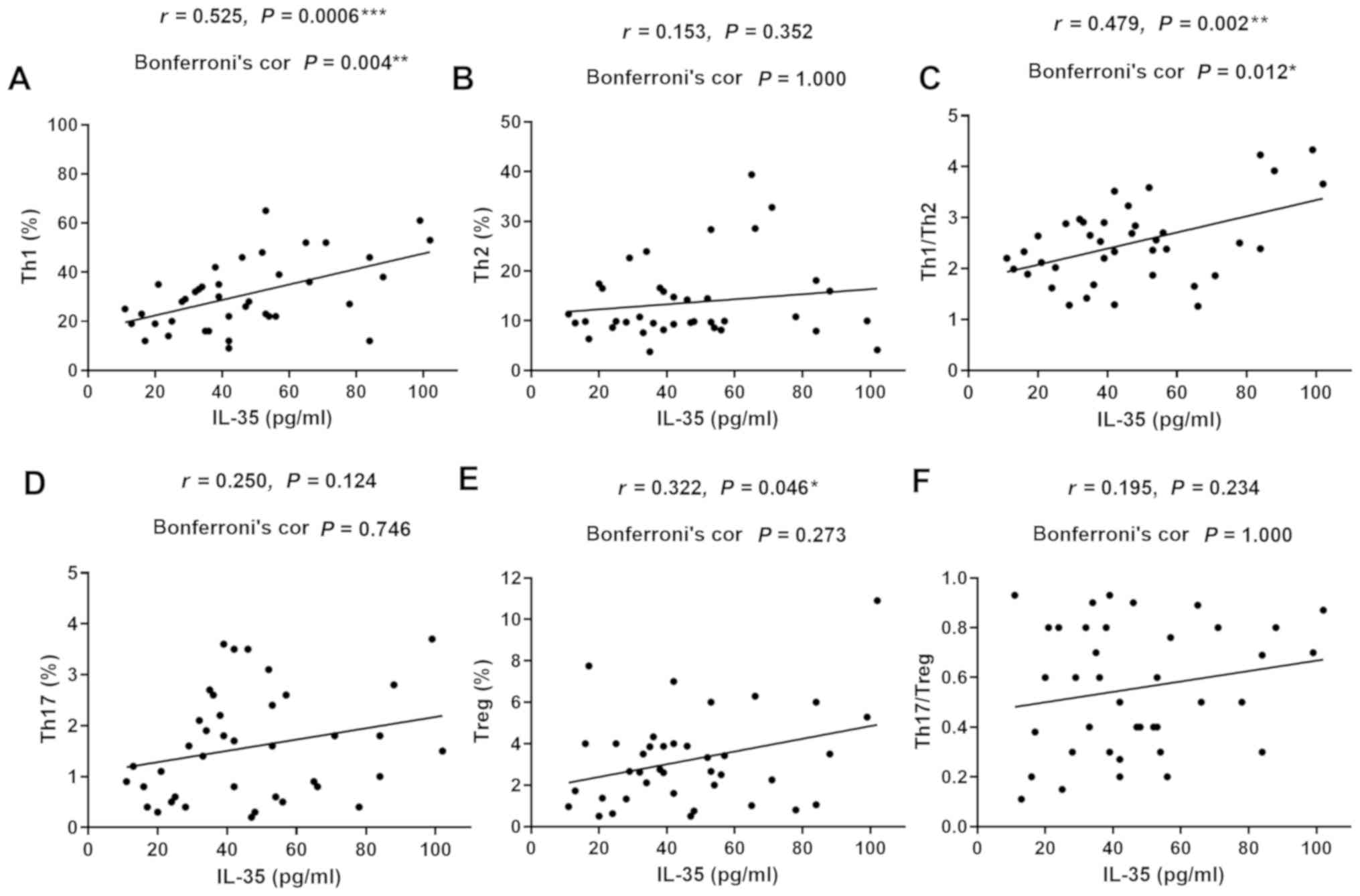
positively correlated with the percentages of Th1 (r=0.525;
P=0.004; Fig. 5A) and the ratio of
Th1 to Th2 cells (r=0.479; P=0.012; Fig.
5C) in patients with CIP. However, no correlation was detected
between serum IL-35 levels and frequency of Th2, Th17, Tregs or the
ratio of Th17 to Treg cells in patients with CIP (r=0.153; P=1.000;
Fig. 5B; r=0.250; P=0.746; Fig. 5D; r=0.322; P=0.273; Fig. 5E; and r=0.195; P=1.000; Fig. 5F). These data suggested that the
activation of Th1 and Th17 cells, as well as the inhibition of
Tregs may contribute to the imbalanced ratio of Th1 to Th2 and Th17
to Tregs, thus leading to increased secretion of serum IL-17A and
IL-35, and ultimately, the development of CIP.
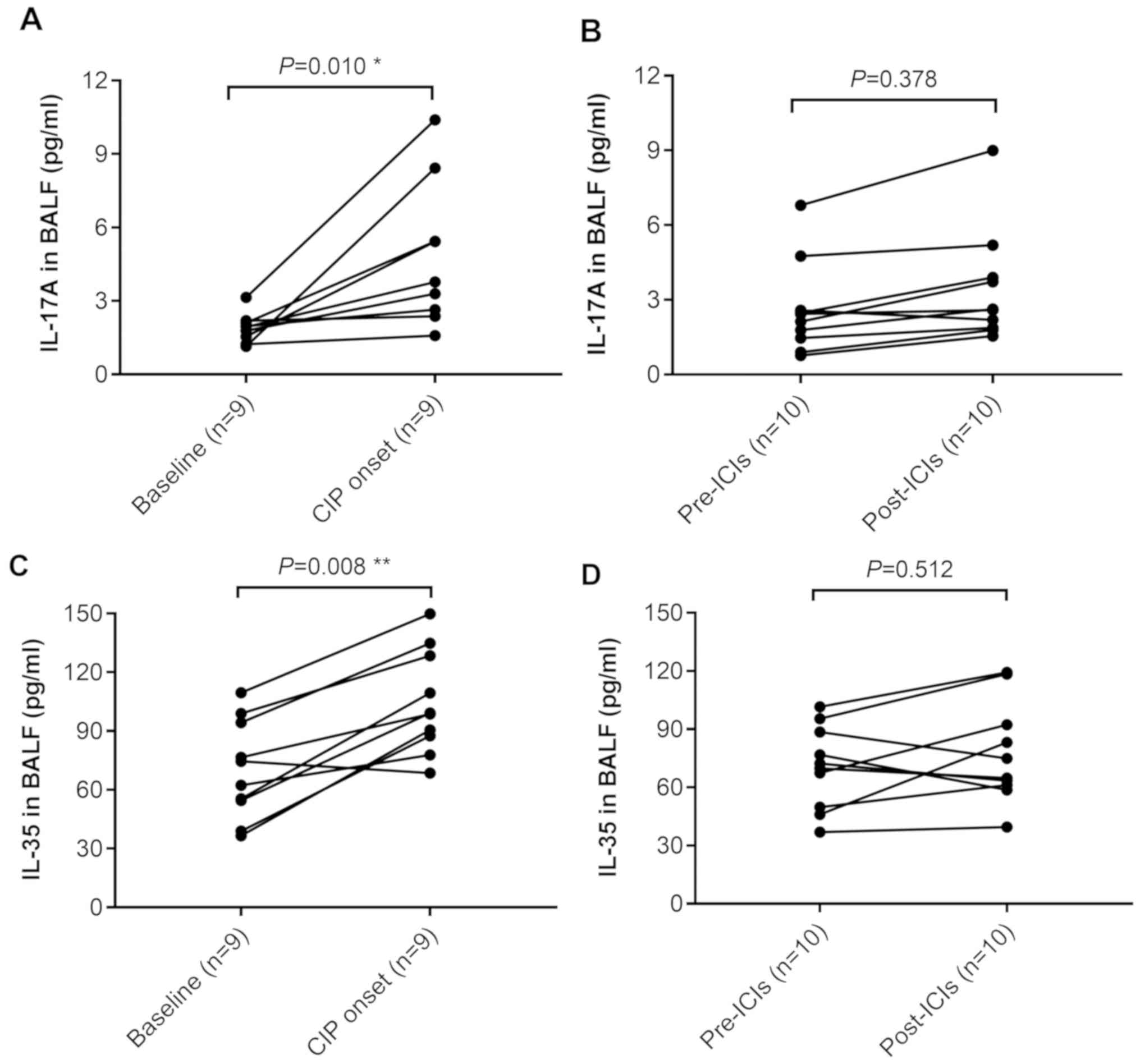
Increased levels of IL-17A and IL-35
in the BALF and serum of patients with NSCLC and CIP
To further confirm the roles that IL-17A and IL-35
serve in the development of CIP, the levels of these cytokines were
detected in the BALF of patients with CIP and the control patients
during immunotherapy. In patients with CIP (n=9), BALF IL-17A
levels increased significantly at the time of CIP diagnosis
compared with baseline levels (P=0.010; Fig. 6A), but no significant alteration was
observed in the BALF of the control patients with NSCLC (n=10;
Fig. 6B). Levels of IL-35 in the
BALF were also increased at the onset of CIP compared with those at
the baseline (P=0.008; Fig. 6C).
However, in 10 control patients with NSCLC who received ICI
treatment, no significant elevation of IL-35 was detected in the
BALF (Fig. 6D).
Discussion
Due to the wide spectrum of irAEs and the complexity
of normal physiological interactions between the immune system and
non-diseased tissues, the identification of biomarkers for irAEs is
challenging. The underlying mechanism of CIP has not been fully
elucidated; however, specific hyperactivation of the T-cell immune
response and/or increased levels of inflammatory cytokines appear
to be involved in the pathogenesis of irAEs (31). Largely on the basis of theory,
current treatments of CIP include discontinuing medication,
systemic corticosteroids and/or additional immune-suppressive
medication, such as infliximab, mycophenolate mofetil,
cyclophosphamide or intravenous immunoglobulins (26–28,32).
However, considering the complexity of CIP, the optimal guidelines
for the management of CIP are still to be established.
IL-17A has been extensively studied as a crucial
inflammatory cytokine, which is associated with autoimmune
conditions (33,34). Considering its essential role in
mediating several acute and chronic respiratory pathologies, such
as asthma (35) and idiopathic
pulmonary fibrosis (36,37), it may be hypothesized that IL-17A may
participate in the autoimmune-pathological processes involved in
CIP. In addition, as an inhibitory cytokine that can modulate
activated T cells in immune dysfunctions, IL-35 has also been
associated with pulmonary fibrosis, which is a characteristic
pathogenic process of systemic sclerosis, a chronic systemic
autoimmune disease (22,38). However, although interstitial
pneumonitis has been reported to be the most common pattern of CIP
(19), which shares similar
pathogenesis with pulmonary fibrosis, limited evidence exists to
clarify the roles of IL-17A and IL-35 in the development of
CIP.
In the present study, IL-17A and IL-35 were
dynamically detected in a cohort of 13 patients with CIP and 20
controls with NSCLC alone. The results indicated that serum levels
of these cytokines significantly increased at the time of CIP
diagnosis compared with the baseline, and decreased upon clinical
recovery or improvement. In 2 CIP cases presenting with severe
pneumonitis progression, markedly elevated levels of IL-17A and
IL-35 were observed in the final stages of disease. Increased
levels of IL-17A and IL-35 compared with baseline were also
observed in the BALF of patients with CIP. PD-1/PD-L1 inhibitors
disrupt immune tolerance, increasing the activation of T cells and
immune responses (39). Therefore,
the elevated levels of IL-17A in the plasma and the BALF may
suggest a second wave of autoreactive T cells, which mediate not
only tumor elimination, but also off-target pulmonary destruction
in CIP. Notably, in NSCLC patients with CIP onset during
immunotherapy, increased levels of IL-35 seem to be insufficient to
maintain immune tolerance or regulate reactive T cells for elevated
levels of IL-17A were also observed. It is likely that the
upregulation of IL-35 reflects a compensatory response to the
PD-1/PD-L1 axis blockage, as well as an anti-inflammatory response
to counteract IL-17A during the development of CIP. Functionally,
both IL-17A and IL-35 have been reported to regulate pulmonary
fibrosis (40,41); thus, the aforementioned data support
the cooperation of IL-35 and IL-17A in promoting CIP.
In the current study, different subtypes of T cells
were dynamically detected, and a higher frequency of Th1 and Th17
cells, as well as higher ratios of Th17 to Tregs and Th1 to Th2,
were associated with the development of CIP. In patients with NSCLC
and CIP, the level of serum IL-17A was positively correlated with
the percentage of Th17 cells and the ratio of Th17 to Tregs, and
negatively associated with the frequency of Tregs. Concurrently,
the levels of serum IL-35 were positively correlated with the
percentage of Th1 and the ratio of Th1 to Th2 cells. These results
support the notion that the activation of the IL-17/Th17 pathway is
involved in the pathogenesis of CIP. In addition, Treg depletion
promotes increased susceptibility of host cells to autoimmunity
(42). Taken together, the
activation of Th17 contributes to the imbalanced ratio of Th17 to
Tregs, and ultimately results in the increased secretion of IL-17A.
IL-17A then stimulates the secretion of tumor growth factor-β1
(43), which induces IL-35
expression (40); together with the
elevated levels of IL-17A, this in turn activates resting
fibroblasts and contributes to the progression of autoimmune
pneumonitis.
An enhanced Th1 response has been observed in the
development of CIP during immunotherapy. The Th1 immune response is
considered a key player in cell-mediated immunity (44), and Th1 dysfunction may promote cancer
progression. A shift in the Th1 to Th2 ratio towards Th2
predominance indicates impairment of cell-mediated immunity, and is
frequently observed in the advanced stages of malignancy (45), while Th1 dominance is reportedly
associated with high survival and low recurrence rates in patients
with cancer (46). Therefore, Th1
polarization in patients with CIP may trigger an excessive T-cell
response, yet to some extent, it also implies a more effective
defense against NSCLC.
In conclusion, the results of the current study
indicate that significantly higher levels of IL-17A and IL-35 in
the plasma and BALF are associated with the severity of
pneumonitis. Furthermore, the level of serum IL-17A was positively
correlated with Th1 and Th17 percentages, and the ratio of Th17 to
Tregs, whereas that of IL-35 was positively associated with the
percentage of Th1 and Tregs, and the ratio of Th1 to Th2 cells in
patients with CIP. Thus, IL-17A, together with IL-35, may
contribute to the pathogenesis of pulmonary fibrosis during the
development of CIP. The levels of IL-17A and IL-35 may be effective
indicators of not only the development, but also the severity of
pulmonary impairment in CIP. Notably, due to the relatively low
incidence of CIP, these analyses focused on PD-1/PD-L1
antibody-related pneumonitis, and thus included a limited number of
subjects. Further investigation is required to confirm these
results and to determine more appropriate biomarkers for predicting
the risk of this rare, but fatal adverse effect. Additional
research will also improve our understanding of such regulatory
systems and may yield insights for more effective therapeutic
approaches to irAEs.
Acknowledgements
The authors are grateful to Dr Wei Wu from State Key
Laboratory of Infectious Disease Diagnosis and Treatment, First
Affiliated Hospital, Zhejiang University School of Medicine, for
assistance with manuscript preparation and literature searches.
Funding
This study was funded by grants from Zhejiang
Provincial Natural Science Foundation of China (grant no.
LY16H160006) and Hangzhou Science and Technology Bureau (grant no.
20160533 B72).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
HC conceived and designed the study. YW and DFL also
helped design the study. WJ and WG performed the experiments and
collected the data. DYL and JD analyzed and interpreted the data.
YW and DFL wrote the manuscript and revised it for important
intellectual content. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
Human samples were provided by the Department of
Medical Oncology, The First Affiliated Hospital, Zhejiang
University School of Medicine, following approval by the
Institutional Review Board of the Cancer Research Institute.
Written informed consent was obtained from all patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
BALF
|
bronchoalveolar lavage fluid
|
|
CIP
|
checkpoint inhibitor pneumonitis
|
|
CT
|
computed tomography
|
|
IL
|
interleukin
|
|
IFN
|
interferon
|
|
irAEs
|
immune-related adverse events
|
|
NSCLC
|
non-small cell lung cancer
|
|
PD-1
|
programmed death receptor 1
|
|
PD-L1
|
programmed death receptor ligand 1
|
|
Th
|
helper T lymphocyte
|
|
Tregs
|
regulatory T cells
|
References
|
1
|
Peters S, Kerr KM and Stahel R: PD-1
blockade in advanced NSCLC: A focus on pembrolizumab. Cancer Treat
Rev. 62:39–49. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Gentzler R, Hall R, Kunk PR, Gaughan E,
Dillon P, Slingluff CL Jr and Rahma OE: Beyond melanoma: Inhibiting
the PD-1/PD-L1 pathway in solid tumors. Immunotherapy. 8:583–600.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Massari F, Santoni M, Ciccarese C, Santini
D, Alfieri S, Martignoni G, Brunelli M, Piva F, Berardi R,
Montironi R, et al: PD-1 blockade therapy in renal cell carcinoma:
Current studies and future promises. Cancer Treat Rev. 41:114–121.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wang Y, Wu L, Tian C and Zhang Y:
PD-1-PD-L1 immune-checkpoint blockade in malignant lymphomas. Ann
Hematol. 97:229–237. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Zhou TC, Sankin AI, Porcelli SA, Perlin
DS, Schoenberg MP and Zang X: A review of the PD-1/PD-L1 checkpoint
in bladder cancer: From mediator of immune escape to target for
treatment. Urol Oncol. 35:14–20. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Johnson DB, Chandra S and Sosman JA:
Immune checkpoint inhibitor toxicity in 2018. JAMA. 320:1702–1703.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Topalian SL, Hodi FS, Brahmer JR,
Gettinger SN, Smith DC, McDermott DF, Powderly JD, Carvajal RD,
Sosman JA, Atkins MB, et al: Safety, activity, and immune
correlates of anti-PD-1 antibody in cancer. N Engl J Med.
366:2443–2454. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Balaji A, Verde F, Suresh K and Naidoo J:
Pneumonitis from anti-PD-1/PD-L1 therapy. Oncology (Williston
Park). 31:739–746. 2017.PubMed/NCBI
|
|
9
|
Ribas A, Puzanov I, Dummer R, Schadendorf
D, Hamid O, Robert C, Hodi FS, Schachter J, Pavlick AC, Lewis KD,
et al: Pembrolizumab versus investigatorchoice chemotherapy for
ipilimumab-refractory melanoma (KEYNOTE-002): A randomised,
controlled, phase 2 trial. Lancet Oncol. 16:908–918. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hamid O, Robert C, Daud A, Hodi FS, Hwu
WJ, Kefford R, Wolchok JD, Hersey P, Joseph RW, Weber JS, et al:
Safety and tumor responses with lambrolizumab (anti-PD-1) in
melanoma. N Engl J Med. 369:134–144. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Borghaei H, Paz-Ares L, Horn L, Spigel DR,
Steins M, Ready NE, Chow LQ, Vokes EE, Felip E, Holgado E, et al:
Nivolumab versus docetaxel in advanced nonsquamous non-small-cell
lung cancer. N Engl J Med. 373:1627–1639. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Brahmer J, Reckamp KL, Baas P, Crinò L,
Eberhardt WE, Poddubskaya E, Antonia S, Pluzanski A, Vokes EE,
Holgado E, et al: Nivolumab versus docetaxel in advanced
squamous-cell non-small-cell lung cancer. N Engl J Med.
373:123–135. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Herbst RS, Baas P, Kim DW, Felip E,
Pérez-Gracia JL, Han JY, Molina J, Kim JH, Arvis CD, Ahn MJ, et al:
Pembrolizumab versus docetaxel for previously treated,
PD-L1-positive, advanced nonsmall-cell lung cancer (KEYNOTE-010): A
randomised controlled trial. Lancet. 387:1540–1550. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Robert C, Long GV, Brady B, Dutriaux C,
Maio M, Mortier L, Hassel JC, Rutkowski P, McNeil C,
Kalinka-Warzocha E, et al: Nivolumab in previously untreated
melanoma without BRAF mutation. N Engl J Med. 372:320–330. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Robert C, Schachter J, Long GV, Arance A,
Grob JJ, Mortier L, Daud A, Carlino MS, McNeil C, Lotem M, et al:
Pembrolizumab versus ipilimumab in advanced melanoma. N Engl J Med.
372:2521–2532. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Weber JS, D'Angelo SP, Minor D, Hodi FS,
Gutzmer R, Neyns B, Hoeller C, Khushalani NI, Miller WH Jr, Lao CD,
et al: Nivolumab versus chemotherapy in patients with advanced
melanoma who progressed after anti-CTLA-4 treatment (CheckMate
037): A randomised, controlled, open-label, phase 3 trial. Lancet
Oncol. 16:375–384. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Pardoll DM: The blockade of immune
checkpoints in cancer immunotherapy. Nat Rev Cancer. 12:252–264.
2012. View
Article : Google Scholar : PubMed/NCBI
|
|
18
|
Barjaktarevic IZ, Qadir N, Suri A,
Santamauro JT and Stover D: Organizing pneumonia as a side effect
of ipilimumab treatment of melanoma. Chest. 143:858–861. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Naidoo J, Wang X, Woo KM, Iyriboz T,
Halpenny D, Cunningham J, Chaft JE, Segal NH, Callahan MK, Lesokhin
AM, et al: Pneumonitis in patients treated with antiprogrammed
death-1/programmed death ligand 1 therapy. J Clin Oncol.
35:709–717. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Iwanaga N and Kolls JK: Updates on T
helper type 17 immunity in respiratory disease. Immunology.
156:3–8. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Collison LW, Workman CJ, Kuo TT, Boyd K,
Wang Y, Vignali KM, Cross R, Sehy D, Blumberg RS and Vignali DA:
The inhibitory cytokine IL-35 contributes to regulatory T-cell
function. Nature. 450:566–569. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Tang J, Lei L, Pan J, Zhao C and Wen J:
Higher levels of serum interleukin-35 are associated with the
severity of pulmonary fibrosis and Th2 responses in patients with
systemic sclerosis. Rheumatol Int. 38:1511–1519. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Konishi J, Yamazaki K, Kinoshita I, Isobe
H, Ogura S, Sekine S, Ishida T, Takashima R, Nakadate M, Nishikawa
S, et al: Analysis of the response and toxicity to gefitinib of
non-small cell lung cancer. Anticancer Res. 25:435–441.
2005.PubMed/NCBI
|
|
24
|
Grande C, Villanueva MJ, Huidobro G and
Casal J: Docetaxel- induced interstitial pneumonitis following
non-small-cell lung cancer treatment. Clin Transl Oncol. 9:578–581.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Delaunay M, Cadranel J, Lusque A, Meyer N,
Gounant V, Moro-Sibilot D, Michot JM, Raimbourg J, Girard N,
Guisier F, et al: Immune-checkpoint inhibitors associated with
interstitial lung disease in cancer patients. Eur Respir J.
50:17000502017. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Brahmer JR, Lacchetti C, Schneider BJ,
Atkins MB, Brassil KJ, Caterino JM, Chau I, Ernstoff MS, Gardner
JM, Ginex P, et al: National comprehensive cancer network.
Management of immune-related adverse events in patients treated
with immune checkpoint inhibitor therapy: American society of
clinical oncology clinical practice guideline. J Clin Oncol.
36:1714–1768. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Haanen JBAG, Carbonnel F, Robert C, Kerr
KM, Peters S, Larkin J, Jordan K and ESMO Guidelines Committee:
Management of toxicities from immunotherapy: ESMO clinical practice
guidelines for diagnosis, treatment and follow-up. Ann Oncol. 29
(Suppl 4):iv264–iv266. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Puzanov I, Diab A, Abdallah K, Bingham CO
III, Brogdon C, Dadu R, Hamad L, Kim S, Lacouture ME, LeBoeuf NR,
et al: Society for immunotherapy of cancer toxicity management
working group. Managing toxicities associated with immune
checkpoint inhibitors: Consensus recommendations from the society
for immunotherapy of cancer (SITC) toxicity management working
group. J Immunother Cancer. 5:952017. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
US Department of Health and Human
Services, National Institutes of Health, National Cancer Institute,
. Common Terminology Criteria for Adverse Events (CTCAE) Version
4.0. https://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03/Archive/CTCAE_4.0_2009-05-29_QuickReference_8.5×11.pdfMay
28–2009
|
|
30
|
Oken MM, Creech RH, Tormey DC, Horton J,
Davis TE, McFadden ET and Carbone PP: Toxicity and response
criteria of the eastern cooperative oncology group. Am J Clin
Oncol. 5:649–655. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Postow MA, Sidlow R and Hellmann MD:
Immune-related adverse events associated with immune checkpoint
blockade. N Engl J Med. 378:158–168. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Friedman CF, Proverbs-Singh TA and Postow
MA: Treatment of the immune-related adverse effects of immune
checkpoint inhibitors: A review. JAMA Oncol. 2:1346–1353. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Park H, Li Z, Yang XO, Chang SH, Nurieva
R, Wang YH, Wang Y, Hood L, Zhu Z, Tian Q and Dong C: A distinct
lineage of CD4 T cells regulates tissue inflammation by producing
interleukin 17. Nat Immunol. 6:1133–1141. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Miossec P and Kolls JK: Targeting IL-17
and TH17 cells in chronic inflammation. Nat Rev Drug Discov.
11:763–376. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Cosmi L, Liotta F and Annunziato F: Th17
regulating lower airway disease. Curr Opin Allergy Clin Immunol.
16:1–6. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Wilson MS, Madala SK, Ramalingam TR,
Gochuico BR, Rosas IO, Cheever AW and Wynn TA: Bleomycin and
IL-1beta-mediated pulmonary fibrosis is IL-17A dependent. J Exp
Med. 207:535–552. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Zhang J, Wang D, Wang L, Wang S, Roden AC,
Zhao H, Li X, Prakash YS, Matteson EL, Tschumperlin DJ and Vassallo
R: Profibrotic effect of IL-17A and elevated IL-17RA in idiopathic
pulmonary fibrosis and rheumatoid arthritis-associated lung disease
support a direct role for IL-17A/IL-17RA in human fibrotic
interstitial lung disease. Am J Physiol Lung Cell Mol Physiol.
316:L487–L497. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Dantas AT, Gonçalves SM, Pereira MC,
Gonçalves RS, Marques CD, Rego MJ, Pitta Ida R, Duarte AL and Pitta
MG: Increased IL-35 serum levels in systemic sclerosis and
association with pulmonary interstitial involvement. Clin
Rheumatol. 34:1621–1625. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Makkouk A and Weiner GJ: Cancer
immunotherapy and breaking immune tolerance: New approaches to an
old challenge. Cancer Res. 75:5–10. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Galati D, De Martino M, Trotta A, Rea G,
Bruzzese D, Cicchitto G, Stanziola AA, Napolitano M, Sanduzzi A and
Bocchino M: Peripheral depletion of NK cells and imbalance of the
Treg/Th17 axis in idiopathic pulmonary fibrosis patients. Cytokine.
66:119–126. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Tomcik M, Zerr P, Palumbo-Zerr K,
Storkanova H, Hulejova H, Spiritovic M, Kodet O, Stork J, Becvar R,
Vencovsky J, et al: Interleukin-35 is upregulated in systemic
sclerosis and its serum levels are associated with early disease.
Rheumatology (Oxford). 54:2273–2282. 2015.PubMed/NCBI
|
|
42
|
Tanaka A and Sakaguchi S: Regulatory T
cells in cancer immunotherapy. Cell Res. 27:109–118. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Mi S, Li Z, Yang HZ, Liu H, Wang JP, Ma
YG, Wang XX, Liu HZ, Sun W and Hu ZW: Blocking IL-17A promotes the
resolution of pulmonary inflammation and fibrosis via
TGF-beta1-dependent and -independent mechanisms. J Immunol.
187:3003–3014. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Kaiko GE, Horvat JC, Beagley KW and
Hansbro PM: Immunological decision making: How does the immune
system decide to mount a helper T-cell response? Immunology.
123:326–338. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Munn DH: Blocking IDO activity to enhance
anti-tumor immunity. Front Biosci (Elite Ed). 4:734–745. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Tosolini M, Kirilovsky A, Mlecnik B,
Fredriksen T, Mauger S, Bindea G, Berger A, Bruneval P, Fridman WH,
Pagès F and Galon J: Clinical impact of different classes of
infiltrating T cytotoxic and helper cells (Th1, th2, treg, th17) in
patients with colorectal cancer. Cancer Res. 71:1263–1271. 2011.
View Article : Google Scholar : PubMed/NCBI
|