Introduction
Skin squamous cell carcinoma (SCC) is one of the
commonest non-melanoma skin cancers worldwide (1,2). SCC is
a type of malignant tumor originating from epidermis or adnexal
keratinocytes, which often manifests in light exposed areas, such
as the scalp, the face and the dorsum of the hand. In Europe and
the United States, the incidence rate of SCC ranks second and
increases yearly, preceding basal cell carcinoma (3). In China, the incidence rate of SCC is
the highest among non-melanoma skin tumors (29.4%) and is slightly
higher than that of basal cell carcinoma (28%) (4). At present, the incidence rate of SCC
increases annually by 2.6% with the increased population age in
China, and 10–15% patients develop metastasis (5,6). Once
metastasis occurs or when the disease develops rapidly, the
follow-up treatment becomes less efficient and the prognosis of
patients is poor. At present, surgical resection remains the best
clinical treatment for SCC, followed by radiotherapy and
chemotherapy (7). Skin is constantly
exposed to chemical stress and ultraviolet radiation, which lead to
the overproduction of reactive oxygen species (ROS) (8). Increased oxidative stress can deplete
and destroy the skin's non-enzymatic and enzymatic antioxidant
defense systems, leading to increased oxidative stress and
photosensitivity (9). Increased
oxidative stress induces protein oxidation and lipid peroxidation,
leading to numerous physiological dysfunctions, including tumor
formation and aging (10).
Ring finger protein 2 (RNF2), a member of the
polycomb genes family, is an ubiquitinated ligase with finger ring
structure (11,12). As one of the core members of the
polycomb family, RNF2 gene is highly expressed in a variety
of human tumors (13–15), and its expression is associated with
the degree of malignancy and the prognosis of patients. In
addition, RNF2 expression was reported to promote tumor
growth and metastasis (16). Bosch
et al (13) demonstrated that
RNF2 expression in breast cancer tissues is significantly
increased compared with normal breast tissues and promotes breast
cancer cell invasive ability. Chen et al (14) reported that RNF2 knockdown
inhibits the proliferation and invasive ability of pancreatic
cancer cells. Li et al (15)
demonstrated that RNF10 may be the central target for the
regulation of diabetic vascular remodeling due to its
anti-hyperproliferative, pro-apoptotic anti-inflammatory
activities. However, RNF2 expression in SCC remains
unknown.
Investigating the association between RNF2
expression and the occurrence and development of SCC may therefore
provide novel insights for diagnosis, treatment option and
prevention of SCC. The present study aimed to evaluate the role of
RNF2 expression in SCC by using immunohistochemistry (IHC), western
blot analysis and semi-quantitative reverse transcription (RT) PCR,
in order to determine a potential prognostic and diagnostic
biomarker for patients with SCC.
Materials and methods
Patients and controls
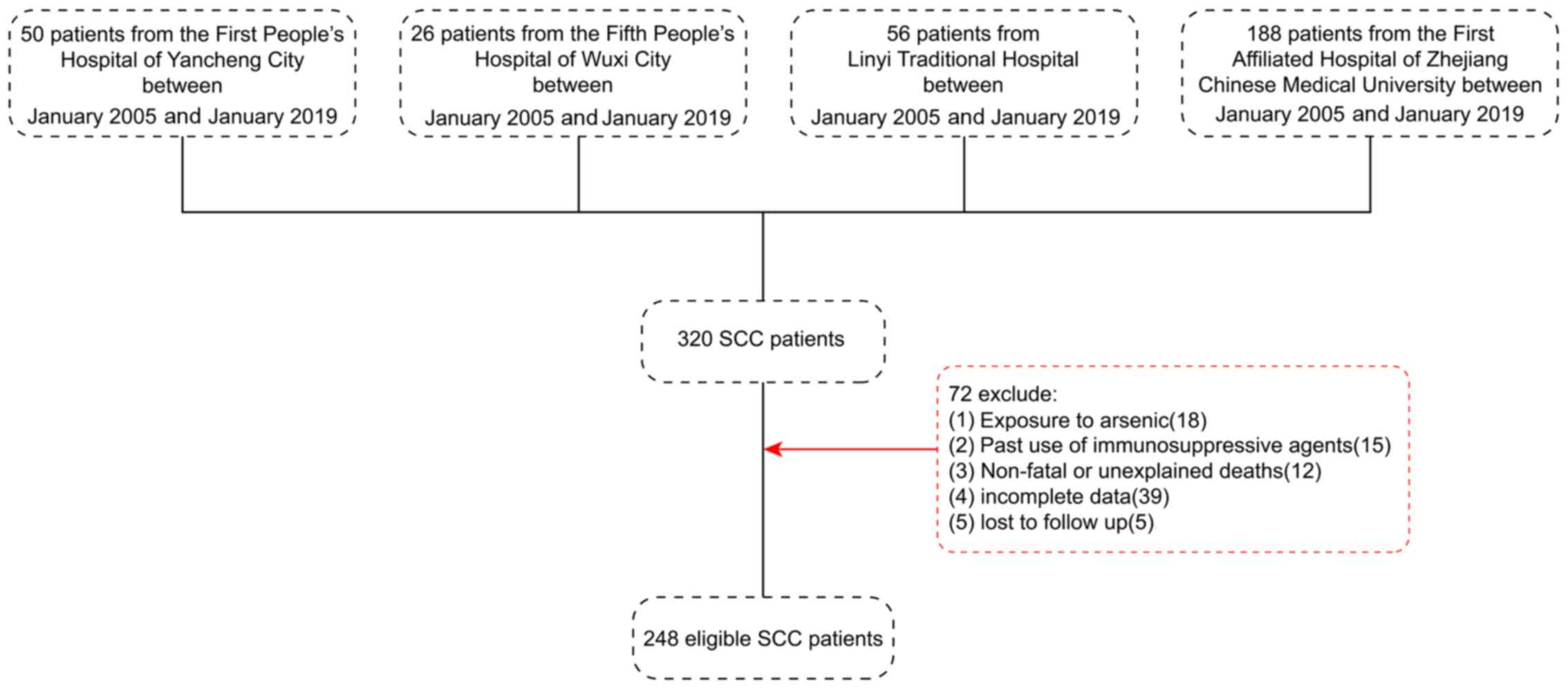
The present study retrospectively analyzed a
cross-section of 248 eligible patients with SCC from a total of 320
patients from the First People's Hospital of Yancheng City, The
Fifth People's Hospital of Wuxi, Linyi Traditional Hospital and the
First Affiliated Hospital of Zhejiang Chinese Medical University
between January 2005 and January 2019. The flow chart for patients
screening is presented in Fig. 1.
All patients underwent surgical resection. The inclusion criteria
were as follows: i) Clinicopathological diagnosis of SCC; ii) no
radiotherapy or chemotherapy was administered prior to surgery;
iii) clinicopathological and follow-up data were complete; and iv)
the location was exposed to at least one of the following: Head,
face and neck. The exclusion criteria were as follows: i) Exposure
to arsenic; ii) prior-use of immunosuppressive agents; iii)
non-fatal or unexplained deaths; iv) incomplete clinicopathological
and follow-up data; and v) patients lost to follow up.
The 248 patients with SCC included 140 men and 108
women (age range, 25–86 years; mean age, 57 years). The tumor
locations were as follows: 119 samples from the head, 77 samples
from the face and 52 cases from the neck. Furthermore, the tumor
size was <5 cm for 104 cases and >5 cm for 144 cases. A total
of 190 cases exhibited poor differentiation and 58 cases showed a
high-to-moderate differentiation. According to Broders'
pathological grading criteria for SCC (17), 68 cases were grades I and II and 180
cases were grades III and IV. Adjacent tissue specimens were
collected by surgical resection from 248 individuals to serve as a
control group (age range, 27–81 years; mean age, 55 years).
The follow-up results from the 248 patients enrolled
in the present study were obtained via medical records (laboratory
data, imaging data and clinical characteristics of the patient
during hospitalization) and telephone interviews (follow-up data
after discharge: Including survival time, treatment and laboratory
data.) Postoperative follow-up was performed every three months
during the first year, every four months during the second year,
every six months during the third year and every eight months until
patient succumbed to the disease. All participants provided oral
informed consent. The present study was approved by the Ethics
Committee of the First People's Hospital of Yancheng City (approval
no. 2017044) and of the Fifth People's Hospital of Wuxi [approval
no. HMU (Ethics) 2017-k-133].
IHC
IHC was used to detect RNF2 distribution by using
the Envision and DAB chromogenic reagent kit (cat. no. MAX-002
MAX007TM). Sections were fixed with 4% paraformaldehyde for 24 h at
room temperature. The dehydration was then carried out under a
gradually increasing ethanol gradient at room temperature. Tissues
were immersed in 70% ethanol, 80% ethanol, 95% ethanol I, 95%
ethanol II, anhydrous ethanol I, anhydrous ethanol II and anhydrous
ethanol III for 1 h each. Xylene was subsequently added to make the
tissues transparent, then immersed in paraffin and finally embedded
into wax blocks. Sections were embedded in paraffin and cut into
5-µm-thick sections. Subsequently, sections were dewaxed with
xylene I, xylene II and xylene III for 10 min at room temperature,
respectively, and then immersed in anhydrous ethanol I, anhydrous
ethanol II respectively for 2 min at room temperature, and rinsed
with distilled water three times (30 sec/wash). Antigen repair was
performed with 0.01 citrate buffer, pH 6.0 at 90°C for 1 h, and
incubated with 0.3% hydrogen peroxide (Sigma-Aldrich; Merck KGaA)
at room temperature for 30 min to inhibit peroxidase activity.
Sections were incubated with the primary rabbit anti-human RNF2
monoclonal antibody (1:100; cat. no. EPR12245; Upstate,
Biotechnology, Inc.) overnight at 4°C, washed 3 times with PBS
solution (PH 7.4, 1:100v/v; 3 min/wash) and then incubated with
polymer-HRP secondary antibody (1:200; cat. no. KXX0022; Dako;
Agilent Technologies, Inc.) for 20 min at room temperature. The
sections were washed 3 times with PBS solution (3 min/wash) and
subsequently incubated with DAB solution (OriGene Technologies,
Inc.) at room temperature for 5 min. Tissues were subsequently
stained with Improved Harris Hematoxylin Dye Solution (2 g
hematoxylin, 5 g aluminum sulfate, 0.2 g potassium iodate, 250 ml
95% ethanol, 750 ml distilled water, 50.0 ml glycerol and 0.3 g
citric acid; BASO Biotechnology Co., Ltd.; http://www.baso.com.cn) for 20 sec at room
temperature. The positive staining was observed by using a light
microscope (magnification, ×400) and the proportion of positive
area was calculated.
IHC staining scores were determined by two blinded
independent pathologists. The positively stained cells in SCC
tissues and adjacent tissues were observed in 10 randomly selected
high-power fields of view and 100 tumor cells were counted. RNF2
was located in the nucleus under light microscopy. The staining
score was determined as follows: Negative (−), no brown-yellow
positive staining in tumors or glandular epithelial cells; weakly
positive (+), <25% positive cells; positive (++), 25–50%
positive cells; strong positive (+++), >50% positive cells. For
statistical analysis, negative (−) or weakly positive (+) were
defined as low expression, whereas positive (++) or strong positive
(+++) were defined as high expression.
Detection of RNF2 expression by
western blot analysis
Tissue samples were homogenized, lysed with tissue
lysate RIPA lysis buffer (Beijing Solarbio Science & Technology
Co., Ltd.), centrifuged at 12,000 × g for 5 min at 4°C, and the
supernatan t containing the total proteins was collected. Protein
concentration was determined using the BCA kit (Pierce; Thermo
Fisher Scientific, Inc.), according to the manufacturer's protocol.
A total of 20 µg protein/lane was separated via SDS-PAGE on a 10%
gel and electrotransferred onto polyvinylidene difluoride membranes
for 1–2 h. Membranes were blocked with 5% skimmed milk for 1 h at
room temperature, and incubated with the following antibodies:
Rabbit RNF2 (1:2,000; cat. no. ab101273; Abcam) and rabbit β-actin
(1:10,000; cat. no. BS1002; Bioworld Technology, Inc.) overnight at
4°C, followed by incubation with anti-rabbit IgG secondary antibody
(1:2,000; cat. no. ab205718; Abcam) at room temperature for 1–2 h.
The membranes were analyzed using the Dolphin-Doc Plus gel imaging
system (25×25 cm; Wealtec Corp.).
Detection of RNF2 mRNA expression
levels by RT-CR
Total RNA was isolated from tissues using
TRIzol® and quantified by Nanodrop spectrophotometer.
Total RNA (10 µg/sample) was isolated and used to generate
complementary DNA. cDNA was amplified by semi-quantitative PCR and
normalized to the internal reference gene β-actin. The sequences of
primers used were as follows: RNF2, forward
5′-AGCACAATAATCAGCAAGCACTC-3′, reverse
5′-GCTCCACTACCATTTTCAATCTG-3′; and β-actin, forward
5′-TGGCATCCACGAAACTACC3-3′ and reverse 5′-GTGTTGGCGTACAGGTCTT-3′.
The thermocycling conditions were as follows: Pre-denaturation at
95°C for 30 sec, 95°C for 5 sec and 60°C for 30 sec, 40 cycles, and
final extension at 60°C for 30 sec. Amplification of RNF2 by PCR
was examined by 1.0% agarose gel electrophoresis using a
Quantity-One electrophoresis apparatus. The absorbance (a) value of
the belt and the reference were read, and the results were
expressed by the ratio (sample value/reference value). If the ratio
of the SCC value was greater than the reference value, it was
positively expressed. Otherwise, it was negatively expressed.
Statistical analysis
SPSS 13.0 (SPSS, Inc.) software was used for
statistical analysis. The χ2 test was used to compare
the association between the expression status of RNF2 mRNA and
protein levels and the clinicopathological characteristics of
patients in adjacent and cancer tissues. Kaplan-Meier survival
analysis was used to determine the disease-specific and
disease-free survival rates. The log-rank test was used to analyze
the difference in survival curves. Multivariable regression
analysis was performed to determine the prognostic factors by using
the Cox proportional-hazards model. P<0.05 was considered to
indicate a statistically significant difference.
Results
RNF2 protein expression in SCC and
adjacent tissues
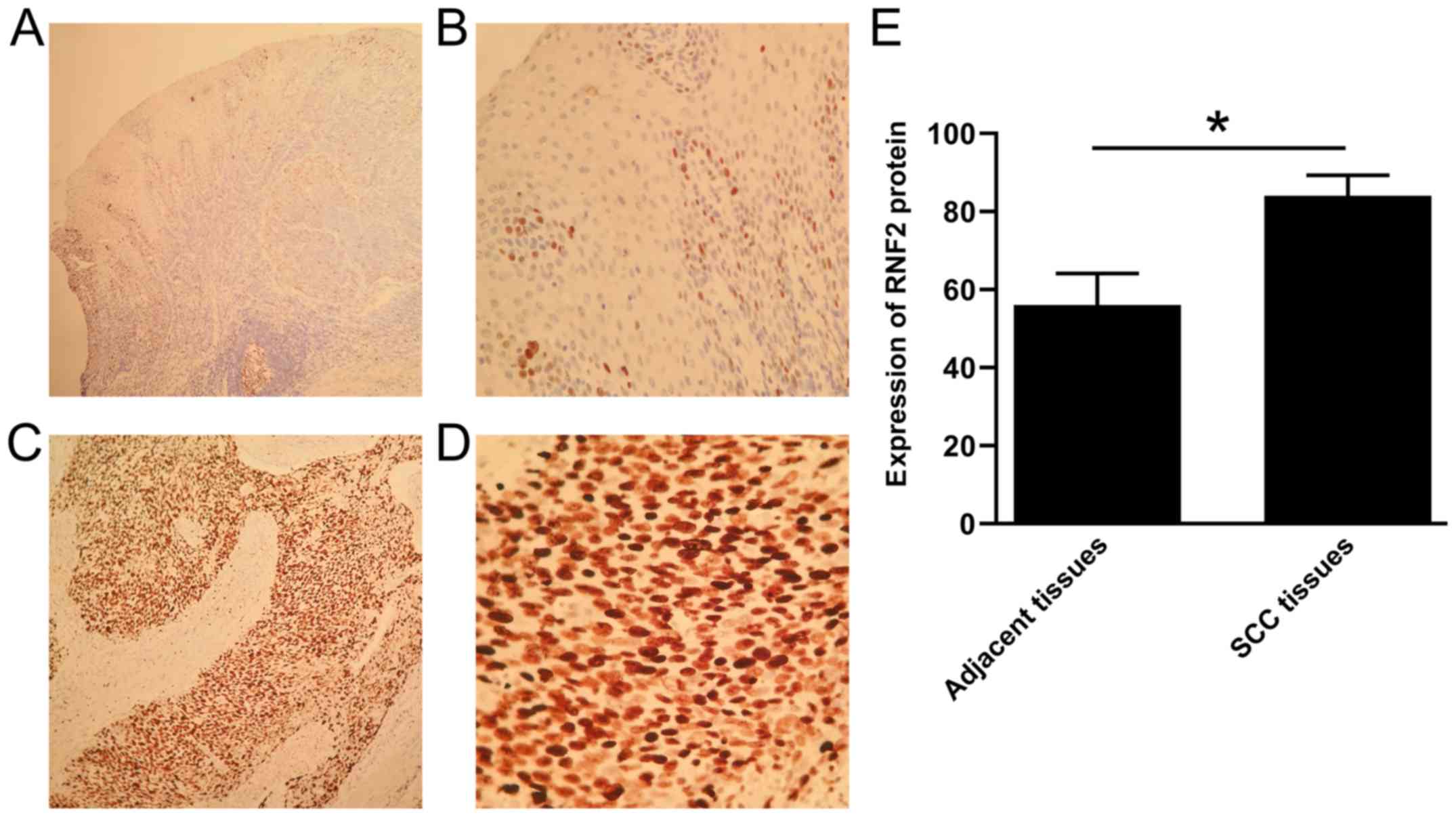
IHC was used to detect the expression of RNF2 in SCC
tissues and adjacent tissues. The results demonstrated that RNF2
was mainly expressed in the nucleus of SCC tissue cells. A small
amount of RNF2 was found in the cytoplasm (Fig. 2A-D). Furthermore, RNF2 expression in
SCC tissues was significantly higher compared with adjacent tissues
(P<0.05; Fig. 2). The positive
expression rate of RNF2 protein was 84.68% (210/248) and 56.05%
(139/248) in SCC tissues and in adjacent tissues, respectively. The
results from western blot analysis also revealed that RNF2
expression in SCC tissues was significantly higher compared with
that in the adjacent tissues (P<0.05; Fig. 3A-B).
RNF2 mRNA expression in SCC and
adjacent tissues
RNF2 expression level in SCC and adjacent
tissues was evaluated by semi-quantitative RT-PCR. The results
demonstrated that the positive rate of RNF2 mRNA in SCC tissues was
81.05% (201/248), which was significantly higher compared with
adjacent tissues 54.44% (135/248; P<0.05; Fig. 3C).
Association between RNF2 mRNA and
protein expression and the clinicopathological characteristics in
patients with SCC
The expression of RNF2 mRNA and protein were both
higher in SCC tissues compared with adjacent tissues. The results
from single factor analysis demonstrated that RNF2 mRNA and protein
expression was not associated with sex, age or tumor site
(P>0.05). However, they were significantly associated with tumor
diameter, degree of tumor differentiation, tumor stage and tumor
metastasis (P<0.05; Table I).
 | Table I.Association between RNF2 protein and
mRNA expression and the clinicopathological characteristics of
patients with SCC. |
Table I.
Association between RNF2 protein and
mRNA expression and the clinicopathological characteristics of
patients with SCC.
| Characteristic | n | RNF2 protein
positive rate | χ2 | P-value | RNF2 mRNA positive
rate | χ2 | P-value |
|---|
| Sex |
|
|
|
|
|
|
|
|
Male | 140 | 119 (85.00) | 0.155 | 0.586 | 115 (82.14) | 0.022 | 0.878 |
|
Female | 108 | 91 (84.26) |
|
| 86 (79.63) |
|
|
| Age (years) |
|
|
|
|
|
|
|
|
<40 | 49 | 41 (83.67) | 0.192 | 0.675 | 39 (79.59) | 0.039 | 0.943 |
|
≥40 | 199 | 169 (84.92) |
|
| 162 (81.41) |
|
|
| Tumor diameter
(cm) |
|
|
|
|
|
|
|
|
<5 | 104 | 80 (76.92) | 0.145 | 0.010 | 75 (72.12) | 0.113 | 0.021 |
| ≥5 | 144 | 130 (90.28) |
|
| 126 (87.50) |
|
|
| Degree of tumor
differentiation |
|
|
|
|
|
|
|
| High
and moderate differentiation | 58 | 28 (48.28) | 0.499 | 0.002 | 27 (46.55) | 0.441 | 0.003 |
| Poor
differentiation | 190 | 182 (95.79) |
|
| 174 (91.58) |
|
|
| Tumor stage |
|
|
|
|
|
|
|
|
I–II | 68 | 41 (60.29) | 7.131 | 0.004 | 37 (54.41) | 6.928 | 0.005 |
|
III–IV | 180 | 169 (93.89) |
|
| 164 (91.11) |
|
|
| Lymph node
metastasis |
|
|
|
|
|
|
|
|
Yes | 86 | 81 (94.19) | 0.219 | 0.032 | 79 (91.86) | 0.201 | 0.031 |
| No | 162 | 129 (79.63) |
|
| 122 (75.31) |
|
|
| Tumor site |
|
|
|
|
|
|
|
|
Head | 119 | 103 (86.55) | 0.209 | 0.912 | 99 (83.19) | 0.129 | 0.372 |
|
Face | 77 | 64 (83.12) |
|
| 61 (79.22) |
|
|
|
Neck | 52 | 43 (82.69) |
|
| 41 (78.85) |
|
|
Prognostic value of RNF2 expression
status for the overall survival of postoperative patients with
SCC
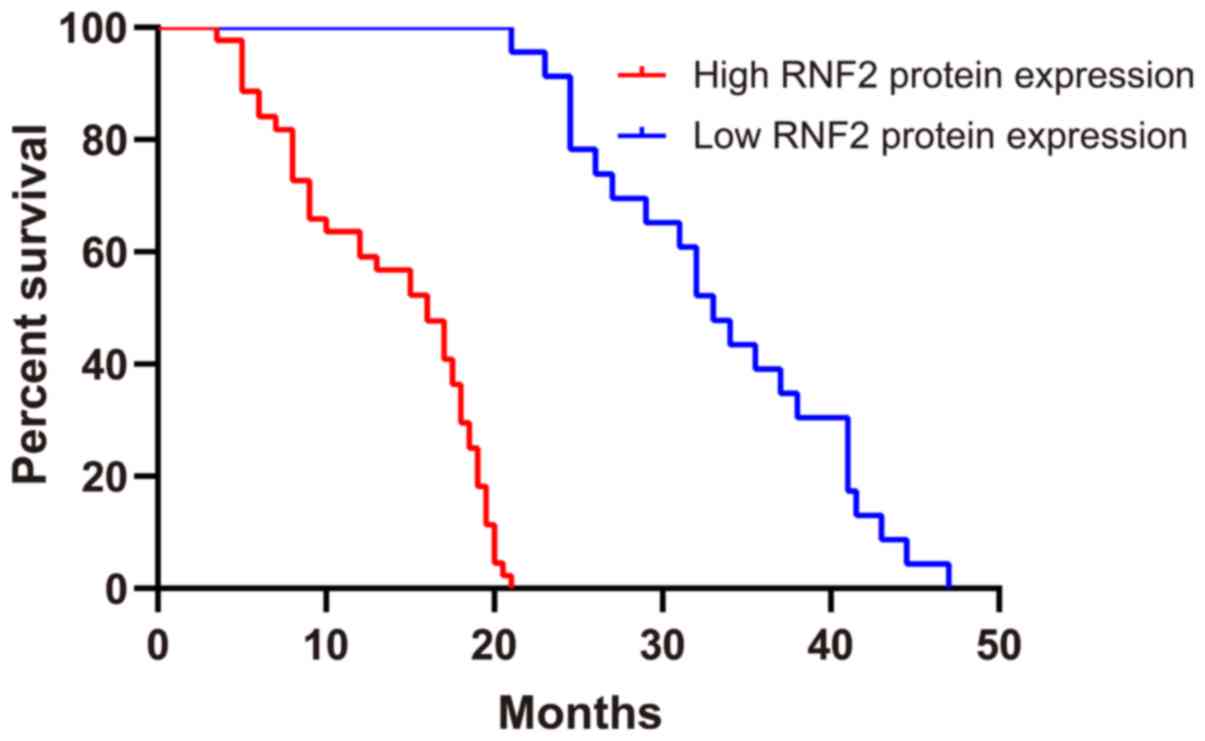
The follow-up examination of patients with SCC was
performed up until 80 months. Patients with high RNF2 expression in
SCC tissues had a significantly shorter disease-specific survival
rate compared with patients with low RNF2 expression. Kaplan-Meier
survival analysis demonstrated that there was a significant
difference between RNF2 high and RNF2 low patients (P<0.0001;
Fig. 4). High RNF2 expression in SCC
tissues was associated with a significantly shorter
disease-specific survival rate than those with low RNF2 expression.
Among the 210 patients exhibiting high RNF2 protein expression in
SCC tissues, 195 patients succumbed to the disease and 15 patients
survived. Among the 38 patients with low RNF2 protein expression,
16 patients succumbed and 22 patients survived. The median survival
time of patients with higher and lower expression of RNF2 was
14.5±1.3 and 25.5±7.5 months, respectively. These findings
indicated that high RNF2 expression may affect the prognosis of
patients with SCC.
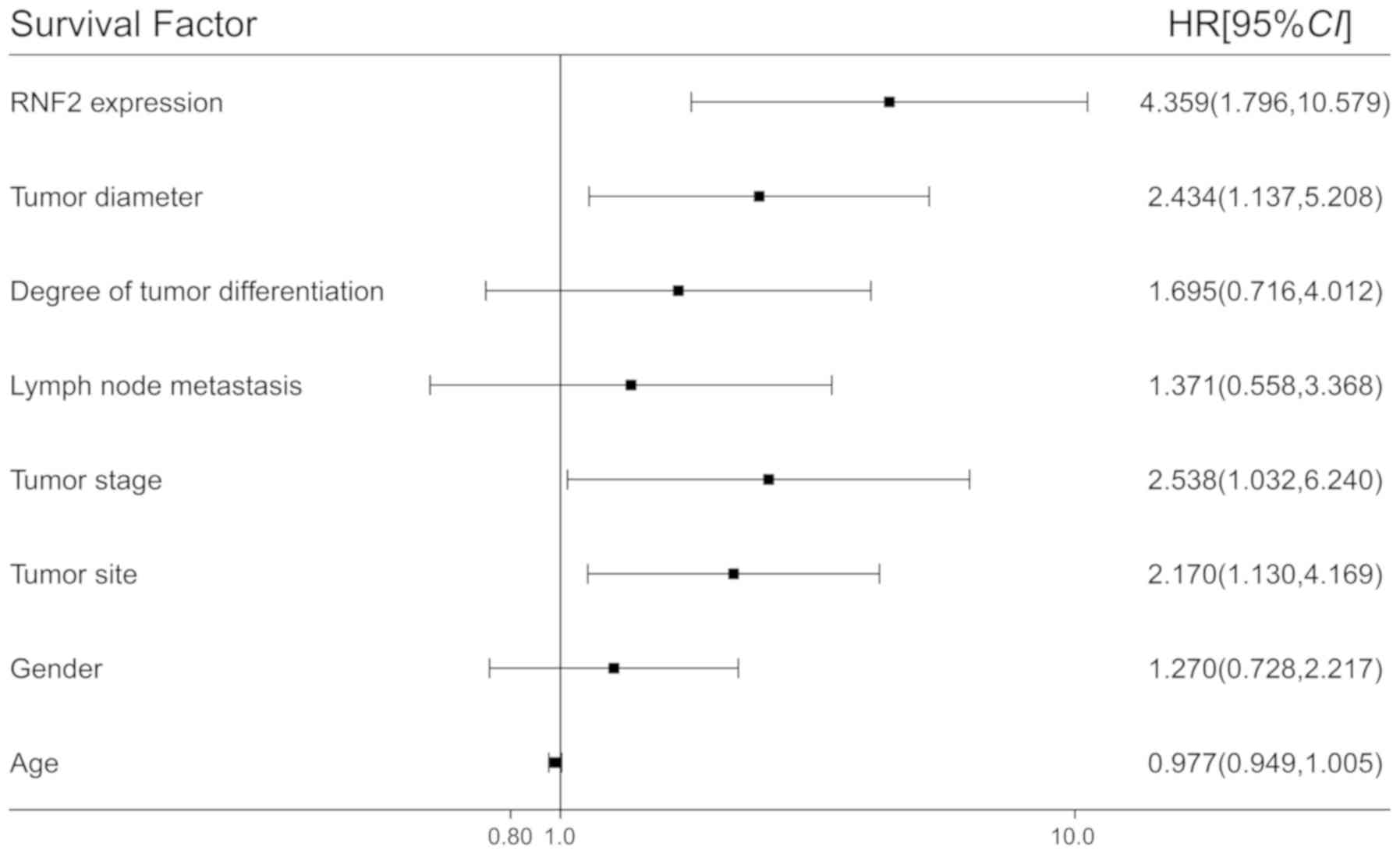
The results from multifactor Cox survival analysis
demonstrated that RNF2 protein expression, tumor diameter, tumor
site and tumor stage were independent prognostic factors affecting
the overall survival of patients with SCC following surgery.
However, sex, age, tumor differentiation degree and tumor
metastasis were not independent prognostic factors affecting the
overall survival of patients with SCC (Fig. 5).
Discussion
RNF2 is a member of the protein-coding genes
(PCGs) also known as RING1B (18).
PCGs were first discovered in Drosophila melanogaster and
are reported to maintain the expression level of growth regulators
such as Hox, promote histone deacetylation and block ATP-dependent
chromosome remodeling, inhibiting therefore gene transcription
(19,20). Furthermore, PCGs are involved in
numerous biological processes, including cell cycle regulation,
cancer progression, aging, X chromosome inactivation, cell fate and
stem cell differentiation (21). In
mammals, PCGs consist of two core components: Polycomb inhibitory
complexes (PRC) 1 and PRC2. PCGs mainly inhibit the activity of
target genes through epigenetic events, thus participating in the
occurrence, development and regulation of cancer via DNA
methylation, histone demethylation, macrohistone H2A linkage and
histone deacetylation (22). An
important member of PRC1, RNF2, has a ring finger domain (23). This ring finger has E3 ligase, which
helps RNF2 catalyze the universalization of histone H2A 119 lysine,
then silence genes by compressing chromatin and inhibiting the
extension of transcription (24).
Due to its E3 ligase, RNF2 catalyzes the universalization of
histone H2A 119 lysine, which can silence genes by compressing
chromatin and therefore inhibit the extension of transcription
(25). RNF2 serves a role in the
proliferation and differentiation of stem cells, maintaining their
ability of self-renewal and the occurrence and development of
tumors (26). Curatti et al
(27) demonstrated that RNF1 serves
a crucial role in the existence of a redox regulatory mechanism in
A. vinelandii, and controls the rate of expression and
maturation of nitrogenase by the activity of the Rnf protein
complexes.
Recent studies reported that RNF2 is highly
expressed in malignant tumors and serves a role in promoting cancer
(28,29). For example, previous studies
demonstrated that RNF2 protein is highly expressed in esophageal,
pancreatic, bladder, breast and ovarian cancers, and that RNF2 is
manly located in tumor cell nucleus (11,30,31).
Yang et al (16) reported a
significantly higher RNF2 protein expression in esophageal cancer
compared with adjacent tissue, which was associated with tumor
size, tumor-node-metastasis (TNM) stage and lymph node metastasis;
however, RNF2 expression is not associated with the prognosis of
patients. Chen et al (30)
demonstrated that the high RNF2 protein and mRNA expression in
invasive ovarian cancer tissues following IHC and fluorescence in
situ hybridization is associated with TNM stage, histological
grade, FIGO stage and Ki-67 proliferation index. Li et al
(31) also reported that RNF2
protein and gene expression in bladder urothelial carcinoma is
significantly increased compared with that in bladder mucosa, and
high RNF2 expression is associated with tumor TNM stage and lymph
node metastasis. However, no association was indicated with poor
prognosis of patients with bladder mucosa (30). Chen et al (15) reported that RNF2 protein is localized
in the nucleus of pancreatic cancer tissues where it is highly
expressed. However, low RNF2 expression in normal pancreatic
tissues adjacent to cancer, and high RNF2 expression in cancer
tissues are negatively correlated with the 5-year survival rate of
patients.
The present study confirmed that RNF2 protein was
localized in the nucleus of SCC tissues cells. The results from the
present study demonstrated that RNF2 expression in SCC was
significantly higher compared with adjacent tissue, suggesting an
association between the occurrence and development of tumor and a
higher expression of RNF2. In the present study, the RNF2
mRNA expression in SCC tissues was significantly higher compared
with that in adjacent tissues. The association between RNF2
expression and the clinicopathological characteristics of patients
with SCC was consistent, whereby the protein level was consistent
with the gene level. The present study demonstrated that RNF2
protein and gene expression in SCC tissues were not associated with
sex, age or tumor site. However, RNF2 protein and gene expression
were associated with tumor diameter, tumor stage, tumor metastasis
and the degree of tumor differentiation in SCC tissues. In
addition, the protein and gene expression of RNF2 in the poor
differentiation group and the lymph node metastasis group was
significantly higher compared with the high and moderate
differentiation group and the non-metastasis lymph node group.
These findings suggested that higher expression of RNF2 may serve a
crucial role in the development, invasion and metastasis of
SCC.
The present study also examined the association
between the expression of RNF2 and overall survival rate of
postoperative patients with SCC. The median survival time for
patients with higher RNF2 expression was significantly shorter
compared with patients with low RNF2 expression in SCC. Multifactor
Cox survival stage demonstrated that RNF2 protein expression, tumor
diameter, tumors site and tumor stage were independent prognostic
factors affecting the overall survival of postoperative patients
with SCC. All these results revealed that high expression of RNF2
was associated with the prognosis of patients with SCC, which were
also approved the results of studies by Choi et al (32) and Li et al (31).
The present study had some limitations. Firstly,
although this study was, to the best of our knowledge, one of the
largest-scale studies on RNF2 protein expression in SCC, further
validation is required through recruitment of a larger sample size.
Secondly, the underlying mechanism of RNF2 as a predictor for the
prognosis of patients with SCC requires further investigation
through large samples and multi centers.
In summary, the present study demonstrated that the
protein and gene expression of RNF2 in SCC tissues may be
associated with the occurrence, development and prognosis of SCC,
which may further assist in the development of novel therapeutic
and diagnostic strategies for patients with SCC.
Acknowledgements
Not applicable.
Funding
The present study was supported by the Youth Medical
Talent of Jiangsu Province (grant no. QNRC2016163) granted to
JL.
Availability of data and materials
All data generated or analyzed during this study are
included in the published article.
Authors' contributions
BaL, MY and BiL contributed to the conception and
design of the study, acquisition of data, analysis and
interpretation of data, and drafting of the manuscript. JL, BJ and
WW contributed to the statistical analysis. GL contributed to the
conception and supervision of the study, and the critical revision
of the manuscript. BaL and BJ contributed to the study conception
and design, study supervision and critical revision of the
manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of the First People's Hospital of Yancheng City (approval
no. 2017044) and of the Fifth People's Hospital of Wuxi [approval
no. HMU (Ethics) 2017-k-133], and was performed in accordance with
the Declaration of Helsinki.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
IHC
|
immunohistochemistry
|
|
RT-PCR
|
reverse transcription polymerase chain
reaction
|
|
SCC
|
skin squamous cell carcinoma
|
|
RNF2
|
ring finger protein 2
|
|
PCGs
|
protein-coding genes
|
References
|
1
|
Drucker AM, Adam GP, Rofeberg V, Gazula A,
Smith B, Moustafa F, Weinstock MA and Trikalinos TA: Treatments for
primary squamous cell carcinoma and squamous cell carcinoma in situ
of the skin: A systematic review and network meta-analysis: Summary
of an Agency for Healthcare Research and Quality Comparative
Effectiveness Review. J Am Acad Dermatol. 82:479–482. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Wu J, Lu WY and Cui LL: Clinical
significance of STAT3 and MAPK phosphorylation, and the protein
expression of cyclin D1 in skin squamous cell carcinoma tissues.
Mol Med Rep. 12:8129–8134. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bashline B: Skin cancer: Squamous and
basal cell carcinomas. FP Essent. 481:17–22. 2019.PubMed/NCBI
|
|
4
|
Wu J, Guo NZ, Cui LL, Wang W, Xiong CQ and
Zhang XY: Correlation between tripartite motif-containing protein
44 protein expression and the prognosis of postoperative patients
exhibiting skin squamous cell carcinoma. Medicine (Baltimore).
97:e130212018. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Zhang L, Shan X, Chen Q, Xu D, Fan X, Yu
M, Yan Q and Liu J: Downregulation of HDAC3 by ginsenoside Rg3
inhibits epithelial-mesenchymal transition of cutaneous squamous
cell carcinoma through c-Jun acetylation. J Cell Physiol.
234:22207–22219. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Lansbury L, Bath-Hextall F, Perkins W,
Stanton W and Leonardi-Bee J: Interventions for non-metastatic
squamous cell carcinoma of the skin: Systematic review and pooled
analysis of observational studies. BMJ. 347:f61532013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lailheugue A, Gibier JB, Lassailly G,
Truant S, Pruvot FR and El Amrani M: Primary squamous cell
carcinoma of the peristomal skin of gastrostomy in a transplant
patient: A first case report. J Gastrointest Oncol. 10:573–576.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Emmert H, Patel H and Brunton VG:
Kindlin-1 protects cells from oxidative damage through activation
of ERK signalling. Free Radic. Biol Med. 108:896–903. 2017.
|
|
9
|
Zhang QL, Li XM, Lian DD, Zhu MJ, Yim SH,
Lee JH, Jiang RH and Kim CD: Tumor Suppressive function of NQO1 in
cutaneous squamous cell carcinoma (SCC) cells. Biomed Res Int.
2019:20765792019. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ciani F, Tafuri S, Troiano A, Cimmino A,
Fioretto BS, Guarino AM, Pollice A, Vivo M, Evidente A, Carotenuto
D and Calabrò V: Anti-proliferative and pro-apoptotic effects of
Uncaria tomentosa aqueous extract in squamous carcinoma cells. J
Ethnopharmacol. 211:285–294. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Yang J, Yu F, Guan J, Wang T, Liu C, Wang
Y, Liu G and Zhu S: Knockdown of RNF2 enhances the radiosensitivity
of squamous cell carcinoma in lung. Biochem Cell Biol. 97:589–599.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
An R, Cheng L, Chen L and Du J: Plk1
interacts with RNF2 and promotes its ubiquitin-dependent
degradation. Oncol Rep. 39:2358–2364. 2018.PubMed/NCBI
|
|
13
|
Bosch A, Panoutsopoulou K, Corominas JM,
Gimeno R, Moreno-Bueno G, Martín-Caballero J, Morales S, Lobato T,
Martínez-Romero C, Farias EF, et al: The Polycomb group protein
RING1B is overexpressed in ductal breast carcinoma and is required
to sustain FAK steady state levels in breast cancer epithelial
cells. Oncotarget. 5:2065–2076. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Chen S, Chen JZ, Zhang JQ, Chen HX, Yan
ML, Huang L, Tian YF, Chen YL and Wang YD: Hypoxia induces
TWIST-activated epithelial-mesenchymal transition and proliferation
of pancreatic cancer cells in vitro and in nude mice. Cancer Lett.
383:73–84. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Li S, Yu G, Huang W, Wang R, Pu P and Chen
M: RING finger protein 10 is a potential drug target for diabetic
vascular complications. Mol Med Rep. 20:931–938. 2019.PubMed/NCBI
|
|
16
|
Yang XX, Ma M, Sang MX, Wang XX, Song H,
Liu ZK and Zhu SC: Radiosensitization of esophageal carcinoma cells
by knockdown of RNF2 expression. Int J Oncol. 48:1985–1996. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Vasconcelos L, Melo JC, Miot HA, Marques
ME and Abbade LP: Invasive head and neck cutaneous squamous cell
carcinoma: Clinical and histopathological characteristics,
frequency of local recurrence and metastasis. An Bras Dermatol.
89:562–568. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Chrispijn ND, Elurbe DM, Mickoleit M, Aben
M, de Bakker DEM, Andralojc KM, Huisken J, Bakkers J and Kamminga
LM: Loss of the Polycomb group protein Rnf2 results in derepression
of tbx-transcription factors and defects in embryonic and cardiac
development. Sci Rep. 9:43272019. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Sui Y, Ju C and Shao B: A lymph node
metastasis-related protein-coding genes combining with long
noncoding RNA signature for breast cancer survival prediction. J
Cell Physiol. 234:20036–20045. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Zhang Y, Tao Y, Ji H, Li W, Guo X, Ng DM,
Haleem M, Xi Y, Dong C, Zhao J, et al: Genome-wide identification
of the essential protein-coding genes and long noncoding RNAs for
human pan-cancer. Bioinformatics. 35:4344–4349. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Guo JC, Li CQ, Wang QY, Zhao JM, Ding JY,
Li EM and Xu LY: Protein-coding genes combined with long non-coding
RNAs predict prognosis in esophageal squamous cell carcinoma
patients as a novel clinical multi-dimensional signature. Mol
Biosyst. 12:3467–3477. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Dempsey J, Zhang A and Cui JY: Coordinate
regulation of long non-coding RNAs and protein-coding genes in
germ-free mice. BMC Genomics. 19:8342018. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Zhu S, Zhao D, Yan L, Jiang W, Kim JS, Gu
B, Liu Q, Wang R, Xia B, Zhao JC, et al: BMI1 regulates androgen
receptor in prostate cancer independently of the polycomb
repressive complex 1. Nat Commun. 9:5002018. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Zhang J, Sun Z, Han Y, Yao R, Yue L, Xu Y
and Zhang J: Rnf2 knockdown reduces cell viability and promotes
cell cycle arrest in gastric cancer cells. Oncol Lett.
13:3817–3822. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Koike H, Ueno Y, Naito T, Shiina T, Nakata
S, Ouchi R, Obana Y, Sekine K, Zheng YW, Takebe T, et al: Ring1B
promotes hepatic stem/progenitor cell expansion through
simultaneous suppression of Cdkn1a and Cdkn2a in mice. Hepatology.
60:323–333. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Román-Trufero M, Méndez-Gómez HR, Pérez C,
Hijikata A, Fujimura Y, Endo T, Koseki H, Vicario-Abejón C and
Vidal M: Maintenance of undifferentiated state and self-renewal of
embryonic neural stem cells by Polycomb protein Ring1B. Stem Cells.
27:1559–1570. 2009. View
Article : Google Scholar : PubMed/NCBI
|
|
27
|
Curatti L, Brown CS, Ludden PW and Rubio
LM: Genes required for rapid expression of nitrogenase activity in
Azotobacter vinelandii. Proc Natl Acad Sci USA.
102:6291–6296. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Li Q, Li S, Yang X, Zhang X, Song C and
Zhu S: Association between RNF2+P-AKT expression in pretreatment
biopsy specimens, and poor survival following radiotherapy in
patients with esophageal squamous cell carcinoma. Oncol Lett.
18:3734–3742. 2019.PubMed/NCBI
|
|
29
|
Wu J, Wang H, Li Q, Guo QY, Tao SQ, Shen
YX and Wu ZS: The oncogenic impact of RNF2 on cell proliferation,
invasion and migration through EMT on mammary carcinoma. Pathol Res
Pract. 215:1525232019. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Chen Y, Cao XY, Li YN, Qiu YY, Li YN, Li W
and Wang H: Reversal of cisplatin resistance by
microRNA-139-5p-independent RNF2 downregulation and MAPK inhibition
in ovarian cancer. Am J Physiol Cell Physiol. 315:C225–C235. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Li XD, Chen SL, Dong P, Chen JW, Wang FW,
Guo SJ, Jiang LJ, Zhou FJ, Xie D, Liu ZW, et al: Overexpression of
RNF2 is an independent predictor of outcome in patients with
urothelial carcinoma of the bladder undergoing radical cystectomy.
Sci Rep. 6:208942016. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Choi D, Lee SJ, Hong S, Kim IH and Kang S:
Prohibitin interacts with RNF2 and regulates E2F1 function via dual
pathways. Oncogene. 27:1716–1725. 2008. View Article : Google Scholar : PubMed/NCBI
|