Introduction
Ovarian cancer (OC) is one of the common malignant
tumors in the female reproductive system. Its incidence rate ranks
third below cervical cancer and carcinoma of corpus uteri, and its
mortality rate ranks first among all kinds of gynecologic tumors,
posing a serious threat to women's health (1). As the ovary is located in the deep part
of the pelvic cavity, early symptoms are not typical. Most patients
have developed middle and late stage OC when they seek medical
treatment, missing the best treatment opportunity (2).
At present, the conventional methods for clinical
screening of OC are trans-abdominal sonography and the
determination of serum tumor marker carbohydrate antigen 125
(CA125). However, trans-abdominal sonography has many influencing
factors, and the ratio of false positive and false negative in
diagnosis of OC are high, resulting in poor stability and accuracy.
The detection of serum CA125 alone has poor sensitivity and
accuracy, so the early diagnosis of OC is not ideal (3). In recent years, transvaginal color
doppler ultrasound (TV-CDS) technology is an emerging examination
method, which can obtain clearer mass morphology, internal echo and
blood flow images, providing reference for the diagnosis of OC by
measuring blood flow parameters (4).
At the same time, with the rapid development of molecular biology,
an increasing number of tumor markers are closely related to OC,
such as CA125, vascular endothelial growth factor (VEGF), and
osteopontin (OPN).
In this study, TV-CDS combined with serum CA125,
VEGF and OPN were selected to diagnose OC, so as to provide basis
for early diagnosis, monitor of disease progression and evaluation
of prognosis of OC.
Patients and methods
Clinical materials
From July 2017 to December 2018, 106 patients with
ovarian cancer (MTG) and 50 patients with benign ovarian diseases
(BCG) who received initial treatment in The Third People's Hospital
of Qingdao (Qingdao, China) were selected as the study subjects.
Patients in MTG were aged 35-83 years, with an average age of
56.72±9.34. Clinical staging referred to the Federation
International of Gynecology and Obstetrics (FIGO) staging standard
in 2009: A total of 11 cases in stage I, 39 cases in stage II, 44
cases in stage III and 12 cases in stage IV. The histopathological
types were 69 cases of ovarian serous adenocarcinoma, 19 cases of
ovarian mucinous adenocarcinoma, 11 cases of endometrial carcinoma
and 7 cases of clear cell carcinoma. According to WHO
classification criteria, there were 23 cases of well
differentiated, 35 cases of middle differentiation and 48 cases of
undifferentiated. Patients in BCG were 34-86 years of age, with an
average age of 57.26±10.98, including 29 cases of serous
cystadenoma, 10 cases of mucinous cystadenoma, 6 cases of ovarian
teratoma and 5 cases of endometrial cyst.
Inclusion criteria were: i) Patients treated for the
first time without radiotherapy and chemotherapy or endocrine
therapy; ii) patients who underwent TV-CDS, serum CA125, VEGF and
OPN; iii) patients who underwent surgery or laparoscopic treatment
in the hospital and were diagnosed by pathology and iv) patients
with complete follow-up data.
Exclusion criteria were: i) Incomplete medical
history data; ii) other important organ dysfunction and iii)
combined with other tumors.
The study was approved by the Ethics Committee of
The Third People's Hospital of Qingdao. All patients who
participated in this research had complete clinical data. Patients
provided a signed informed consent and volunteered to participate
in the study. Age and other baselines of the two groups were not
statistically significant, and thus, the groups were
comparable.
TV-CDS examination
PHILIPS iU22 (Koninklijke Philips N.V.) was used for
color doppler ultrasound diagnosis, with a transducer frequency of
5-7 MHz. The patient was instructed to empty the bladder before
examination. During examination, the patient lay on the back in a
lithotomy position. The transvaginal ultrasound probe was covered
with a disposable latex cot or condom. The cot was coated with
disinfectant couplant. The probe was placed in the deepest part of
the vagina. The size, morphology, boundary, internal echo,
calcification, side-acoustic images and other imaging conditions of
the lesion were explored (5). Then
the blood flow were observed using color doppler flow imaging
(CDFI) technology, including flow classification, resistance index
(RI) and pulsability index (PI). Flow classification (6): Grade 0: there was no blood flow signal;
Grade I: There was punctiform or short line blood flow around the
tumor but there was no blood flow signal inside the tumor. Class
II: There was punctiform or short line blood flow inside the tumor,
with regular blood vessel course; Class III: the blood flow inside
the tumor was dendritic and reticular, with abundant short and long
blood flow, tortuosity and disordered blood vessels. RI and PI were
directly read out and counted by ultrasonic instruments. The
ultrasonography, recording and image diagnosis of all patients were
determined by two deputy directors of the ultrasonography
department.
Examination of serum tumor
markers
A total of 4 ml fasting elbow venous blood was
extracted from OC patients before treatment and at 3 months after
treatment, and from the subjects in the BCG group at 6.00-9.00 in
the morning. The serum was self-coagulated at room temperature, and
then centrifuged using DT5-4 automatic decap centrifuge (Beijing
Era Beili Centrifuge Co., Ltd.) at 2,264 × g, at room temperature
for 30 min. CA125 was detected by electrochemiluminescence using
Roche ELecsys-2010 and Roche original reagents. VEGF and OPN were
detected by enzyme-linked immunosorbent assay (ELISA). Reagents
were provided by R&D Systems, Inc. Tecan Infinite M1000 PRO
multi-function enzyme-labeling instrument (Tecan Group, Ltd.) was
used according to the manufacturer's instructions. The reference
values were CAl25 ≤35.00 U/ml, VEGF ≤148.60 pg/ml and OPN ≤49.90
ng/ml.
Result estimation
One or more positives in the combined examination
were considered positive. All negatives were considered as
negative.
Evaluation index
The standard method of diagnostic test evaluation:
Subjects were divided into patients and non-patients by gold
standard diagnosis, a certain test method was used to measure the
positive and negative results, and then various statistical
analysis were carried out. Based on this, the evaluation indexes
commonly used in diagnostic tests can be calculated. The results of
the test diagnosis were divided into (a) true positive, (b) false
positive, (c) false negative and (d) true negative. Calculation
formula: Sensitivity = a/(a+c); Specificity = d/(d+b); Accuracy =
(a+d)/(a+b+c+d); Positive predictive value = a/(a+b); Negative
predictive value = d/(d+c).
Statistical analysis
Excel 2007 was used to establish a database.
SPSS17.0 statistical software, t-test and χ2 test were
applied. The concentration level of the measured data was expressed
as mean ± standard deviation (SD). The comparison of the mean
number between groups was conducted by independent sample t-test.
The comparison of the counting data rate was conducted by
χ2 test, with statistical significance (P<0.05).
Results
Sonographic comparison of OC and
benign ovarian diseases by TV-CDS
According to the histopathological ‘gold standard’
and the diagnostic value of TV-CDS for benign and malignant ovarian
tumors, the sensitivity of TV-CDS in the diagnosis of OC was 75.47%
(80/106) and the specificity was 90.00% (45/50). TV-CDS showed that
the incidence of lesions in conventional two-dimensional ultrasound
including irregular morphology, unclear boundary, uneven echo,
microcalcification and side-acoustic images in OCG was
significantly higher than that in BCG (P<0.01), as shown in
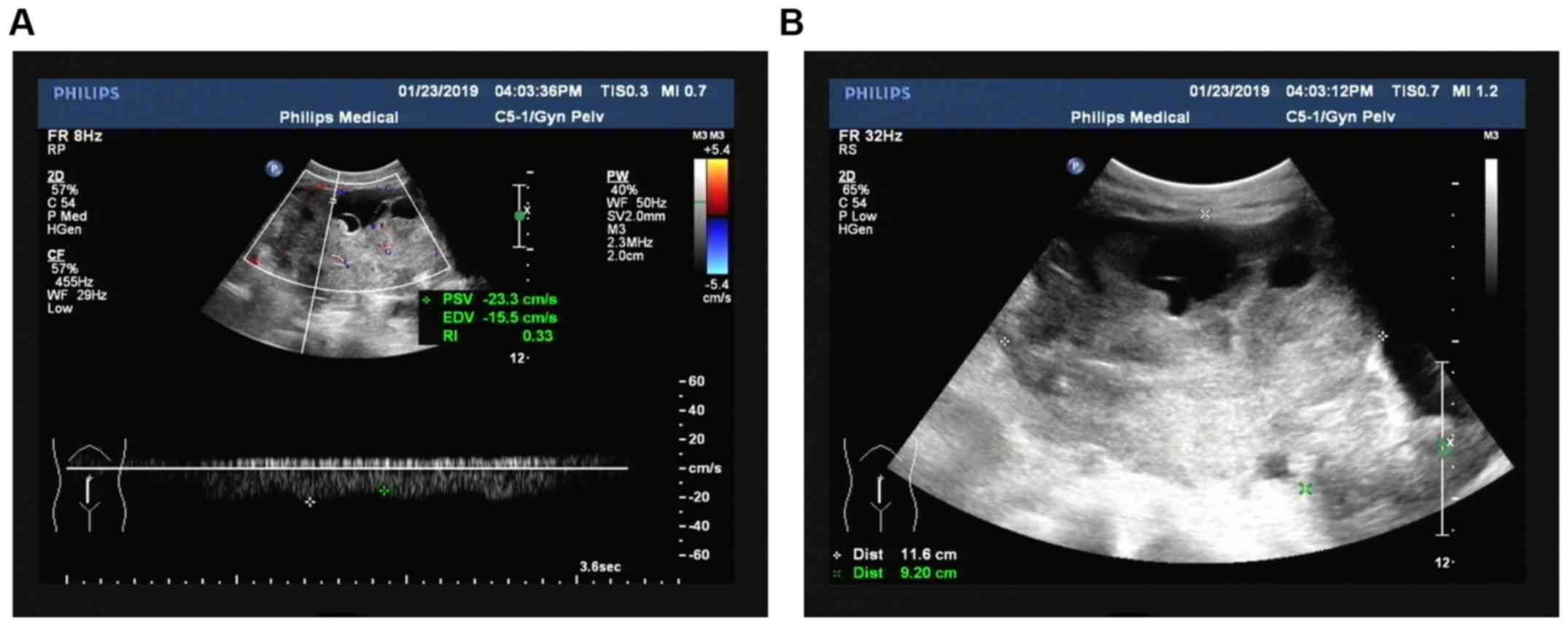
Table I. Regarding blood flow
grading, most patients in the MTG were in grade II and III, while
most patients in the BCG were in grade 0. Compared with RI
(0.73±0.09) and PI (1.25±0.15) in BCG, RI (0.38±0.04) and PI
(0.63±0.09) in the OCG were significantly decreased (t= −3.893,
−3.883, P<0.01) (Table II). The
ultrasonic acoustic and blood flow display images of OC are shown
in Fig. 1.
 | Table I.Comparison of conventional
ultrasonographic features of lesion location of patients in the two
groups [n (%)]. |
Table I.
Comparison of conventional
ultrasonographic features of lesion location of patients in the two
groups [n (%)].
| Group | Cases | Irregular
morphology | Unclear boundary | Uneven echo |
Micro-calcification | Side-acoustic
images |
|---|
| MTG | 106 | 100
(94.34)a | 77
(72.64)a | 76
(71.70)a | 73
(68.87)a | 70
(66.04)a |
| BCG | 50 | 3 (6.00) | 2 (4.00) | 3 (6.00) | 1 (2.00) | 2 (4.00) |
| χ2 |
| 118.195 | 64.041 | 58.666 | 60.924 | 52.614 |
| P-value |
| <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Table II.Comparison of serum CDFI of patients
between OCG and the control group. |
Table II.
Comparison of serum CDFI of patients
between OCG and the control group.
|
|
|
|
| Blood flow grading [n
(%)] |
|---|
|
|
|
|
|
|
|---|
| Group | Cases | RI (mean ± SD) | PI (mean ± SD) | 0 | I | II | III |
|---|
| MTG | 106 |
0.38±0.04a |
0.63±0.09a | 0 (0)a | 10
(9.43)a | 61
(57.55)a | 35
(33.02)a |
| BCG | 50 | 0.73±0.09 | 1.25±0.15 | 35 (70.00) | 12 (24.00) | 3 (6.00) | 0 (0.00) |
Comparison of serum CA125, VEGF, OPN
levels of patients between OCG and the control group
The levels of serum CA125, VEGF and OPN of patients
in OCG were significantly higher than those in BCG, with
statistically significant difference (P<0.01) (Table III).
| Table III.Comparison of serum CA125, VEGF and
OPN levels of patients between OCG and the control group (mean ±
SD). |
Table III.
Comparison of serum CA125, VEGF and
OPN levels of patients between OCG and the control group (mean ±
SD).
| Group | Cases | CA125 (U/ml) | t-test | P-value | VEGF (pg/ml) | t-test | P-value | OPN (ng/ml) | t-test | P-value |
|---|
| MTG | 106 |
169.82±26.38a | 5.981 | 0.001 |
679.62±57.83a | 10.288 | <0.001 |
216.87±34.95a | 5.645 | 0.001 |
| BCG | 50 | 22.83±7.29 |
|
| 123.54±16.68 |
|
| 36.62±8.73 |
|
|
Comparison of expression levels of
serum CA125, VEGF and OPN in different clinicopathological factors
of OC
The expression levels of serum CA125, VEGF and OPN
in OC patients with clinical high stage (stage III and IV), poorly
differentiated, ascites, recurrence and metastasis were
significantly higher than those in patients with clinical low stage
(stage I and II), well differentiated, no ascites and no recurrence
and metastasis (P<0.05). With the disappearance of the tumor or
the decrease of tumor load, the serum marker levels after treatment
were significantly lower than those before treatment (P<0.05)
(Table IV).
| Table IV.Comparison of expression levels of
serum CA125, VEGF and OPN in different clinicopathological factors
of ovarian cancer (mean ± SD). |
Table IV.
Comparison of expression levels of
serum CA125, VEGF and OPN in different clinicopathological factors
of ovarian cancer (mean ± SD).
| Variables | Cases | CA125 (U/ml) | t-test | P-value | VEGF (pg/ml) | t-test | P-value | OPN (ng/ml) | t-test | P-value |
|---|
| Clinical stage |
| Stage
I+II | 50 | 121.68±17.63 | 2.590 | 0.041 | 553.26±45.37 | 3.286 | 0.017 | 125.48±14.82 | 4.680 | 0.003 |
| Stage
III+IV | 56 |
213.65±35.32a |
|
|
792.22±65.61a |
|
|
298.24±38.67a |
|
|
| Differentiation
degree | 58 |
|
|
|
|
|
|
|
|
|
| Well
and middle |
| 115.52±22.68. | 3.116 | 0.021 | 493.25±36.54 | 5.119 | 0.002 | 135.69±15.67 | 4.421 | 0.004 |
|
Poor | 48 |
235.85±36.54a |
|
|
865.31±71.24a |
|
|
315.26±42.85a |
|
|
| Ascites |
|
|
|
|
|
|
|
|
|
|
| No | 42 | 110.59±13.11 | 3.194 | 0.019 | 567.28±43.29 | 2.671 | 0.037 | 142.69±20.81 | 3.737 | 0.010 |
|
Yes | 64 |
208.65±31.37a |
|
|
753.62±63.55a |
|
|
265.87±36.39a |
|
|
| Lymph node
metastasis |
|
|
|
|
|
|
|
|
|
|
| No | 39 | 99.84±18.30 | 3.161 | 0.020 | 530.29±37.26 | 3.228 | 0.018 | 148.52±16.87 | 3.074 | 0.022 |
|
Yes | 67 |
210.28±34.31a |
|
|
766.35±71.41a |
|
|
256.74±35.12a |
|
|
| Distant
metastasis |
|
|
|
|
|
|
|
|
|
|
| No | 94 | 138.42±17.31 | 5.302 | 0.002 | 559.25±37.70 | 6.932 | <0.001 | 122.35±17.41 | 6.013 | <0.001 |
|
Yes | 12 |
412.35±54.01a |
|
|
1,623.65±108.71a |
|
|
546.92±54.05a |
|
|
| Recurrence |
|
|
|
|
|
|
|
|
|
|
| No | 81 | 39.87±8.81 | 8.076 | <0.001 | 153.21±19.82 | 8.367 | <0.001 | 56.82±11.18 | 9.125 | <0.001 |
|
Yes | 25 |
423.86±52.41a |
|
|
1,365.02±79.51a |
|
|
436.82±41.27a |
|
|
| Treatment |
|
|
|
|
|
|
|
|
|
|
|
Before | 106 |
169.82±26.38a | 5.330 | 0.002 |
679.62±57.83a | 9.214 | <0.001 |
216.87±34.95a | 4.558 | 0.004 |
|
After | 106 | 41.27±10.67 |
|
| 162.36±23.06 |
|
| 65.01±12.25 |
|
|
Comparison of diagnostic value of
transvaginal ultrasound, CA125, VEGF, OPN single and combined
examination in OC
The sensitivity, accuracy and negative predictive
value of the combination of transvaginal ultrasound, CA125, VEGF
and OPN in the diagnosis of OC were significantly improved compared
with those of individual and partial combination tests. The
differences were statistically significant (P<0.05) (Table V).
| Table V.Diagnostic value of transvaginal
ultrasound, CA125, VEGF, OPN single and combined examination in
ovarian cancer [% (ratio)]. |
Table V.
Diagnostic value of transvaginal
ultrasound, CA125, VEGF, OPN single and combined examination in
ovarian cancer [% (ratio)].
| Detection
indexes | Sensitivity | Specificity | Accuracy | Positive predictive
value | Negative predictive
value |
|---|
| Ultrasound | 75.47 (80/106) | 90.00 (45/50) | 80.12
(125/156) | 94.12 (80/85) | 63.38 (45/71) |
| CA125 | 60.38 (64/106) | 94.00 (47/50) | 71.15
(111/156) | 95.52 (64/67) | 52.81 (47/89) |
| VEGF | 58.49 (62/106) | 96.00 (48/50) | 70.51
(110/156) | 96.88 (62/64) | 52.17 (48/92) |
| OPN | 55.66 (59/106) | 92.00 (46/50) | 67.31
(105/156) | 93.65 (59/63) | 49.46 (46/93) |
| CA125+VEGF+OPN | 80.19 (85/106) | 88.00 (44/50) | 82.69
(129/156) | 93.41 (85/91) | 67.69 (44/65) |
| Ultrasound+CA125
+VEGF+OPN | 97.17
(103/106)a | 84.00 (43/50) | 93.59
(146/156)a | 96.26
(103/107) | 93.48
(43/46)a |
Discussion
Compared with the traditional transvaginal color
Doppler imaging (TV-CDS), the transvaginal ultrasound is closer to
the ovary. The frequency of the probe is higher without
interference from abdominal wall fat and flatulence, which
significantly improves image quality and resolution and makes it
more objective and accurate to judge whether the ovarian tumors are
benign or malignant. Schelling et al (4) stated that two important factors for the
diagnosis of OC by ultrasound are the determination of the solid
component of the lesion and the presence of blood flow signals in
the solid component. The benign and malignant ovarian masses were
judged by color Doppler ultrasound two-dimensional image and blood
flow imaging (7). The results of
this study showed that the incidence of irregular lesion shape,
unclear boundary, uneven internal echo, microcalcification and
lateral sound shadow in the OC group was significantly higher than
that in the benign lesion group. Due to the lack of muscle layer in
the neovasal wall of ovarian malignant tumor, the neovasal wall is
highly permeable and the vascular wall is thin, presenting a
low-resistance spectrum, and the RI and PI of OC are significantly
lower than those of benign ovarian tumors (8). Kurjak et al (9) proposed that the sensitivity of RI≤0.4
in the diagnosis of ovarian malignancy was 86.4%. The results of
this study showed that the sensitivity of TV-CD in the diagnosis of
OC was 75.47%, slightly lower than those in previous reports, which
may be related to the low threshold of RI (≤0.35). A study on early
detection of OC screening was carried out in the United States,
4,526 women at high risk of developing OC were screened by
transvaginal ultrasound. The value of single detection method of
screening was limited, in particular, early ovarian patients with
low blood flow was easily misdiagnosed (10). Therefore, combined detection with
other markers is needed.
The detection of serum tumor markers is a common
detection method in the diagnosis of malignant tumors, because it
is simple and inexpensive, and the samples are easy to collect.
CA125 is still the most commonly used biomarker for the diagnosis
and efficacy monitoring of OC, providing valuable information for
the determination of the benign and malignant ovarian tumors
(11). It has been reported that
CA125 is elevated in the serum of most ovarian epithelial
carcinoma, and continuous elevation of CA125 level indicates a
relatively poor prognosis (12). It
was better in the prognosis of patients where CA125 level declined
to normal after 3 months of treatment, compared with those who did
not return to normal. The sensitivity of CA125 in the diagnosis of
OC in this study was 60.38%, which was relatively lower than the
73.60% reported by Schummer et al (13), which may be related to the difference
in selected cases. The expression level of CA125 in mucous ovarian
epithelial carcinoma is low, which is prone to false negatives. In
female inflammatory diseases, ovarian chocolate cyst, follicular
cyst, pregnancy and menstruation, CA125 is increased to different
degrees (14), which affects the
accurate diagnosis of OC and results in false positive, indicating
that the value of CA125 alone is limited. VEGF is a cytokine that
regulates angiogenesis and acts specifically on vascular
endothelial cells. The role of VEGF in tumors is not limited to the
formation of blood vessels and the regulation of vascular
permeability (15). Previous
research has shown that the presence of VEGF regulatory signal is
found in tumor cells, which not only acts on the formation of tumor
cells, but also plays a certain role in the formation of tumor stem
cells and tumor metastasis (16).
VEGF plays an important role in the formation of lymphatic vessels
(17). As an important factor of
tumor angiogenesis, VEGF plays a very important role in the
occurrence, progression and invasion of tumors (16). Serum expression level is
significantly correlated with the clinical stage, invasion,
recurrence and metastasis of tumors (18). The results of this study showed that
the sensitivity of VEGF in the diagnosis of OC was 58.49%. Li et
al (19) reported that the
sensitivity of VEGF in the diagnosis of OC was 77.00% in the
combined detection of VEGF and CA125, indicating that the value of
VEGF alone was limited.
OPN is a glycosylated phosphorylated protein that is
associated with the development, invasion and metastasis of tumors.
Its expression is significantly up-regulated in a variety of
malignant tumor tissues (20). In
terms of the mechanism of tumor angiogenesis, VEGF can play a
synergistic role with OPN to promote the generation of granulation
tissue and induce angiogenesis. The establishment of new blood
vessels can promote cell migration, adhesion and prevent cell
apoptosis, which is conducive to tumor cell generation (21). The increase of OPN level in
peripheral blood of advanced OC is more obvious, and the serum
expression level is positively correlated with clinical stage
(22). As for the mechanism of tumor
invasion, metastasis and relapse, cell adhesion - GRGDS sequence in
OPN may interact with integrin and cancer cell surface adhesion
molecule CD44 to inhibit endothelial cell apoptosis, and cause a
variety of protein dissolving enzyme synthesis and secretion, so as
to dissolve the extracellular matrix barrier to tumorigenesis of
invasion and metastasis (23).
Relevant research has shown that OPN is closely correlated with the
development of OC (21). Kim et
al (24) studied 107 plasma
samples by cDNA array and found that there was a significantly high
level of OPN expression in invasive OC and ovarian junction tumors.
It has been pointed out that OPN positive expression could be
detected in OC patients with negative CA125, and the detection of
OPN was complementary (25). The
results of this study showed that the sensitivity of OPN in the
diagnosis of OC was 55.66%, indicating that the value of detection
alone was limited. Combined detection with other markers can
enhance the value.
The results of this study showed that transvaginal
ultrasound and serum CA125, TSGF and VEGF have their respective
advantages and disadvantages in the diagnosis of OC, and the
sensitivity and accuracy are not high, which is far from the
clinical requirements. Because the combined parallel method was
used, that is, if any of the indicators is positive, it is
determined to be positive. Although the specificity decreased
(84.00%), the sensitivity, accuracy and negative predictive value
(97.17, 93.59, and 93.48%, respectively) were significantly higher
than those of individual examinations, thereby missed diagnosis was
reduced.
In conclusion, TV-CDS combined with serum CA125,
TSGF, and VEGF can be used as an effective method for the diagnosis
of OC. The selected sample size for this study was limited.
Therefore, research on larger sample size and prognostic follow-up
will be necessary.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
CY was involved in the conception of the study and
wrote the manuscript. TD and YL collected and analyzed the general
data of the patients. RL assisted with the statistical analysis.
All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
The Third People's Hospital of Qingdao (Qingdao, China). All
patients who participated in this research had complete clinical
data. Signed informed consents were obtained from the patients
and/or guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ulusoy S, Akbayir O, Numanoglu C, Ulusoy
N, Odabas E and Gulkilik A: The risk of malignancy index in
discrimination of adnexal masses. Int J Gynaecol Obstet.
96:186–191. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Menon U, Talaat A, Rosenthal AN, Macdonald
ND, Jeyerajah AR, Skates SJ, Sibley K, Oram DH and Jacobs IJ:
Performance of ultrasound as a second line test to serum CA125 in
ovarian cancer screening. BJOG. 121:35–39. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Schelling M, Braun M, Kuhn W, Bogner G,
Gruber R, Gnirs J, Schneider KT, Ulm K, Rutke S and Staudach A:
Combined transvaginal B-mode and color Doppler sonography for
differential diagnosis of ovarian tumors: Results of a multivariate
logistic regression analysis. Gynecol Oncol. 77:78–86. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Goldberger S, Tepper R, Markov S and Beyth
Y: Transvaginal sonographic characterization of ovarian disease:
Evaluation of a new scoring system to predict ovarian malignancy.
Obstet Gynecol. 78:1151–1152. 1991.PubMed/NCBI
|
|
6
|
Kupesic S and Kurjak A: Contrast-enhanced,
three-dimensional power Doppler sonography for differentiation of
adnexal masses. Obstet Gynecol. 96:452–458. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Benjapibal M, Sunsaneevitayakul P,
Boriboonhirunsarn D, Sutanthavibul A and Chakorngowit M: Color
Doppler ultraso-nography for prediction of malignant ovarian
tumors. J Med Assoc Thai. 85:709–715. 2002.PubMed/NCBI
|
|
8
|
Sawicki W, Spiewankiewicz B, Cendrowski K
and Stelmachów J: Preoperative discrimination between malignant and
benign adnexal masses with transvaginal ultrasonography and colour
blood flow imaging. Eur J Gynaecol Oncol. 22:137–142.
2001.PubMed/NCBI
|
|
9
|
kurjak A, Kupesic S, Sparac V, Prka M and
Bekavac I: The detection of stage I ovarian cancer by
three-dimensional sonography and power Doppler. Gynecol Oncol.
90:258–264. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Fishman DA, Cohen L, Blank SV, Shulman L,
Singh D, Bozorgi K, Tamura R, Timor-Tritsch I and Schwartz PE: The
role of ultrasound evaluation in the detection of early-stage
epithelial ovarian cancer. Am J Obstet Gynecol. 192:1214–1221,
discussion 1221-1222. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gupta KK, Gupta VK and Naumann RW: Ovarian
cancer: Screening and future directions. Int J Gynecol Cancer.
29:195–200. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yang Z, Zhao B and Li L: The significance
of the change pattern of serum CA125 level for judging prognosis
and diagnosing recurrences of epithelial ovarian cancer. J Ovarian
Res. 9:572016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Schummer M, Drescher C, Forrest R, Gough
S, Thorpe J, Hellström I, Hellström KE and Urban N: Evaluation of
ovarian cancer remission markers HE4, MMP7 and Mesothelin by
comparison to the established marker CA125. Gynecol Oncol.
125:65–69. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Dorigo O and Berek JS: Personalizing CA125
levels for ovarian cancer screening. Cancer Prev Res (Phila).
4:1356–1359. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Goel HL and Mercurio AM: VEGF targets the
tumour cell. Nat Rev Cancer. 13:871–882. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Vempati P, Popel AS and MacGabhann F:
Formation of VEGF isoform-specific spatial distributions governing
angiogenesis: Computational analysis. BMC Syst Biol. 5:592011.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wada H, Ura S, Kitaoka S, Satoh-Asahara N,
Horie T, Ono K, Takaya T, Takanabe-Mori R, Akao M, Abe M, et al:
Distinct characteristics of circulating vascular endothelial growth
factor-A and C levels in human subjects. PLoS One. 6:e293512011.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Wang X, Chen X, Fang J and Yang C:
Overexpression of both VEGF-A and VEGF-C in gastric cancer
correlates with prognosis, and silencing of both is effective to
inhibit cancer growth. Int J Clin Exp Pathol. 6:586–597.
2013.PubMed/NCBI
|
|
19
|
Li L, Wang L, Zhang W, Tang B, Zhang J,
Song H, Yao D, Tang Y, Chen X, Yang Z, et al: Correlation of serum
VEGF levels with clinical stage, therapy efficacy, tumor metastasis
and patient survival in ovarian cancer. Anticancer Res.
24:1973–1979. 2004.PubMed/NCBI
|
|
20
|
Lan Z, Fu D, Yu X and Xi M: Diagnostic
values of osteopontin combined with CA125 for ovarian cancer: A
meta-analysis. Fam Cancer. 15:221–230. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ramchandani D and Weber GF: Interactions
between osteopontin and vascular endothelial growth factor:
Implications for cancer. Biochim Biophys Acta. 1855:202–222.
2015.PubMed/NCBI
|
|
22
|
Wang YD, Chen H, Liu HQ and Hao M:
Correlation between ovarian neoplasm and serum levels of
osteopontin: A meta-analysis. Tumour Biol. 35:11799–11808. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Rao G, Wang H, Li B, Huang L, Xue D, Wang
X, Jin H, Wang J, Zhu Y, Lu Y, et al: Reciprocal interactions
between tumor-associated macrophages and CD44-positive cancer cells
via osteopontin/CD44 promote tumorigenicity in colorectal cancer.
Clin Cancer Res. 19:785–797. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kim JH, Skates SJ, Uede T, Wong KK,
Schorge JO, Feltmate CM, Berkowitz RS, Cramer DW and Mok SC:
Osteopontin as a potential diagnostic biomarker for ovarian cancer.
JAMA. 287:1671–1679. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Tilli TM, Franco VF, Robbs BK, Wanderley
JL, da Silva FR, de Mello KD, Viola JP, Weber GF and Gimba ER:
Osteopontin-c splicing isoform contributes to ovarian cancer
progression. Mol Cancer Res. 9:280–293. 2011. View Article : Google Scholar : PubMed/NCBI
|