Introduction
Adenoid cystic carcinoma (ACC) is a rare type of
cancer that occurs primarily in the major and minor salivary glands
(up to 50 and 35%, respectively), but it may also be located at
other sites, including the oropharyngeal and nasopharyngeal spaces,
external ear, trachea, breast, lacrimal gland, skin and lower
female genital tract (1). ACC is
most frequently detected in younger- and middle-aged adults, but
individuals of any age may be affected, including children. Certain
studies have determined a median age of ~60 years and a greater
prevalence in female patients (up to 60% of cases) (1,2). ACC
usually presents in a localized manner and is limited to the
primary sites, but a small proportion of patients exhibit regional
lymph node involvement and distant organ metastasis at diagnosis,
particularly in the lungs. To date, the biological behavior of ACC
has remained poorly understood, and clinically, it is primarily
treated by surgery, with or without adjuvant radiation therapy.
Case report
A 46-year-old male patient visited the First
Affiliated Hospital of Army Medical University (Chongqing, China)
in May 2016 with recurring asymptomatic large irregular red lumps
on the right temple for ~6 years. The patient also complained of
slight breathlessness on exertion for half a year. The patient's
medical history was provided by the patient and the patient's
daughter. In early 2006, a slow-growing red nodule arose on the
right auricle. It was gradually enlarged to the size of a pigeon
egg and was surgically excised at a separate hospital (The First
Affiliated Hospital of Chongqing Medical University; Chongqing,
China) in January 2010. The histopathological diagnosis was ACC and
there was no obvious evidence of spread elsewhere during the
general physical examination. After a few months, indurated plaques
appeared on the right temple and gradually enlarged over time. For
economic reasons, the patient did not seek any medical help until
April 2016. The patient refused operative treatment once again. In
the recent half year, the tumors on the right temple increased
markedly and the patient experienced slight breathlessness after
activity and he then visited a hospital.
The patient was underweight (Body Mass Index, 16.7),
but appeared reasonably energetic. Physical examination indicated
no obvious abnormality besides the skin lesions. There was no
associated cervical lymphadenopathy. On local examination, a
solitary non-tender proliferative growth, measuring ~5×4 cm with an
uneven surface and irregular margins, was arising on the right
temple without erosion or bleeding. There were obviously dilated
capillaries on the surface. The upper part of the right auricle was
absent due to the previous surgery (Fig.
1).
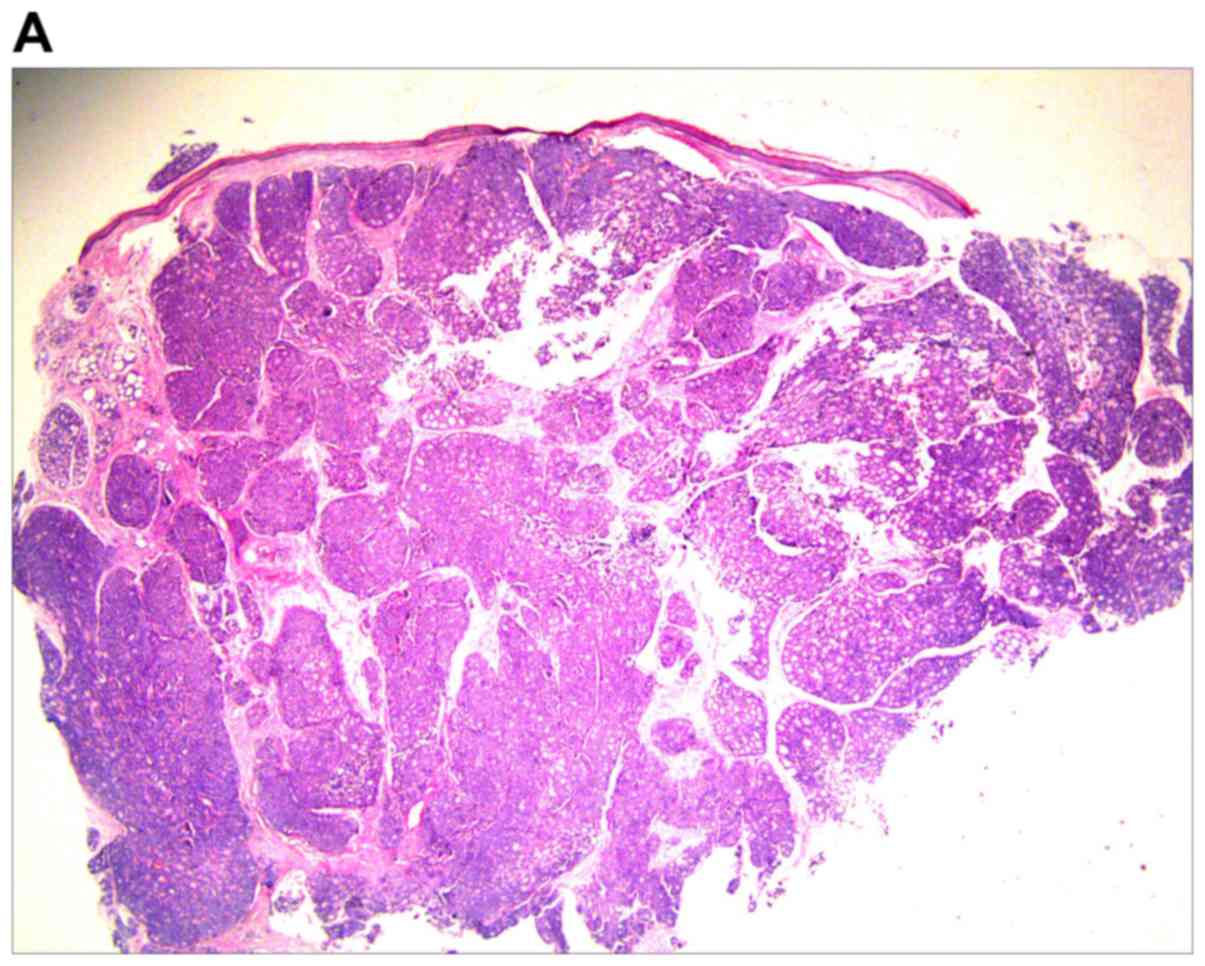
An excision biopsy from the center of tumors on the
right temple was performed. Histopathological examination revealed
a neoplasm that was sharply demarcated from surrounding the normal
parenchyma by reactive gliosis (Fig.
2A). The epithelial tumor cells proliferated with a tubular and
cribriform pattern, in certain places forming ductular structures
lined by stratified cuboidal cells (Fig.
2B-D). There was a certain amount of hyaline or mucinous
material within the tubules and acini or around them. Tubules and
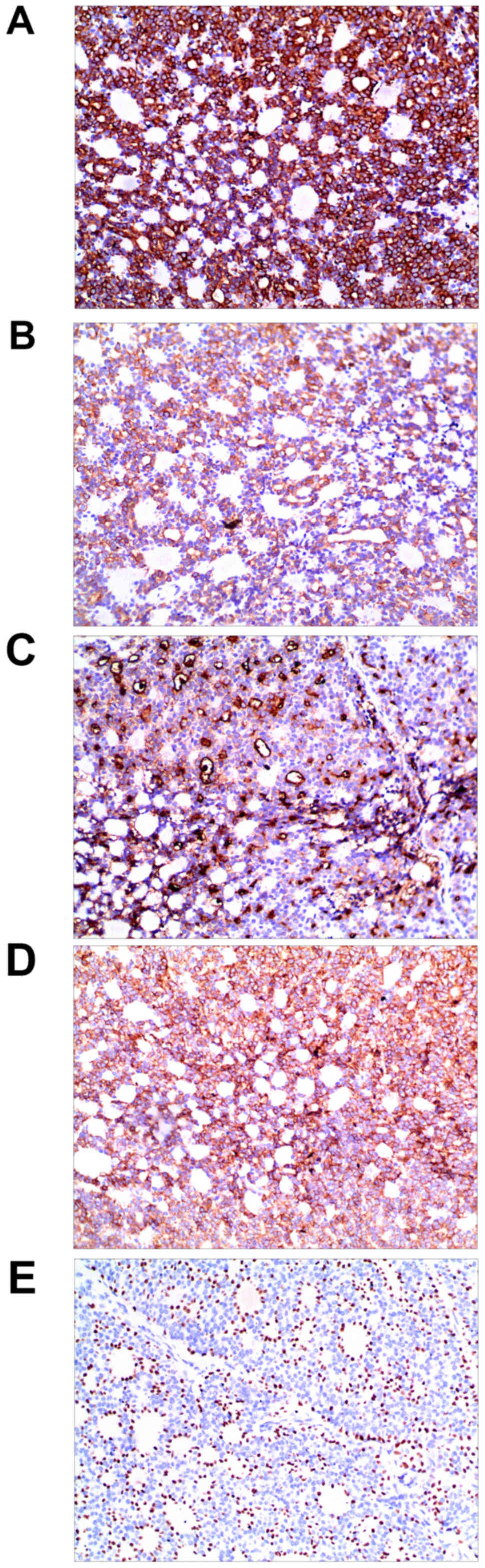
acini were highlighted by periodic acid-Schiff stain (Fig. 2E). Immunohistochemistry for
cytokeratin (CK)20, carcinoembryonic antigen, S100, thyroid
transcription factor 1 and CDX-2 was negative, and thus,
neuroendocrine and visceral metastatic adenocarcinoma was excluded.
The tumor cells tested positive for CK7, CAM5.2, epithelial
membrane antigen and CD117, and the tumor cells in the medial
margin of the glandular cavity were positive for P63 (Fig. 3).
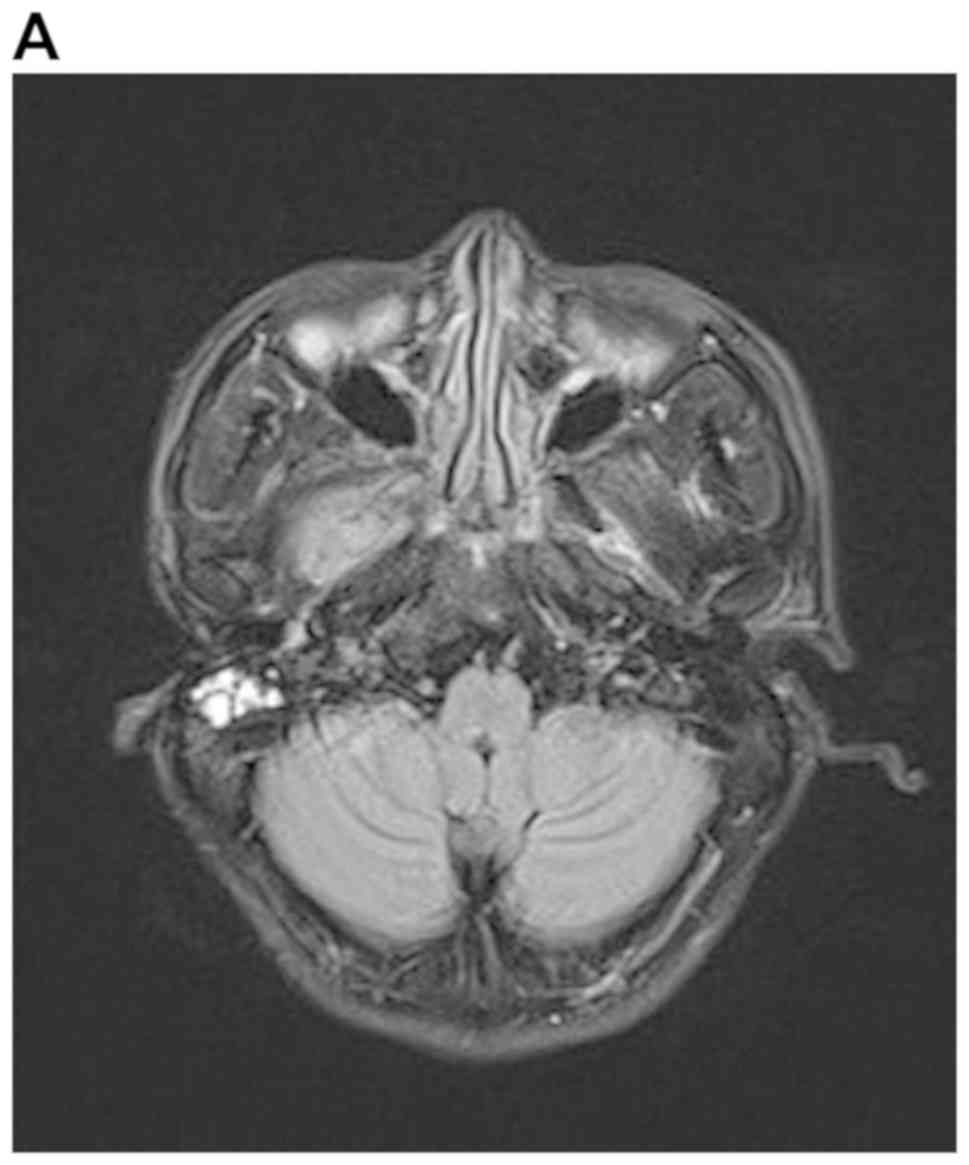
A detailed evaluation of the patient was performed.
Hematological and biochemical parameters were within normal limits.
Cranial MRI revealed multiple mass lesions in the right pharynx,
inferior temporal fossa, middle cranial fossa and right
frontotemporal subcutaneous, which was hyper-intense on T1-weighted
or T2-weighted MRI. The lesion was again enhanced heterogeneously
on contrast and the largest mass measured 4.0×3.0×3.5 cm. In the
right mastoid process, an enhanced T2 signal indicated the presence
of right mastoid process inflammation (Fig. 4A-D). Chest CT (plain and contrast)
revealed multiple metastases in both sides of the lungs (Fig. 4E) and it was hyper-densely situated
in the mediastinum, suggesting calcification. Ultrasonography of
the abdomen indicated no obvious abnormalities. After receiving
radiotherapy one time at a local hospital, the patient exhibited no
significant clinical improvement and refused further treatment. At
a follow-up time of ~2 years, the patient appeared in good spirits,
but refused further medical examination and treatment, and had
become more frail. The patient was then lost to follow-up.
Discussion
ACC is a rare, slow-growing form of high-grade
adenocarcinoma that begins in glandular tissues. ACC occurs
primarily in the head and neck, most commonly in the salivary
glands, and accounts for 1–2% of all cases of head and neck cancer,
~10% of all salivary neoplasms and ~22% of all salivary gland
malignancies (3–5). ACC may also occur in other locations in
the body, including the tracheobronchial tree, breast, foot and
cervix (6–10). ACC of the external ear is rare, and
to the best of our knowledge, only a few cases have been reported
in the literature in the English language. The incidence rate
ranges from 5 to 10% in the external auditory canal (11,12). To
date, the incidence rate of ACC of the external ear has not been
reported in China. According to previous studies, ACC of the
external auditory canal was most commonly diagnosed in the fifth
decade of life and was more common in females (11,13).
The clinical symptoms of ACC depend on the location
of the tumor. As the tumor growth of ACC is frequently slow,
numerous patients may live asymptomatically for a long time, even
with metastatic lesions. ACC is rarely associated with regional
lymph node involvement and there is only a 13% rate of nodal
metastasis in patients with ACC of the external ear (13), which is similar to the 5–10% rate
reported for ACC in other head and neck subsites (14). According to the literature, delayed
hematogenous metastases occur in 25–50% of patients with ACC and
the most common locations of metastases are the lungs and bones
(15). Distant metastasis frequently
occurs without local recurrence. The patient described in the
present case report was a 46-year-old male. While skull base
infiltration and lung metastases have been previously observed, no
nodal metastasis was detected in this patient. This may be
explained by the fact that ACC tends to spread along nerves, known
as a perineural invasion, or through the bloodstream (15). In clinical practice, the majority of
ACCs in the skin are therefore primary neoplasms. Cutaneous ACC may
also represent a direct extension from an underlying salivary gland
primary neoplasm. Metastasis from a more distant site has rarely
been observed (10). The lesions of
the patient in the present case report appeared on the right
external ear at first, and subsequently, skull base and lung
metastases were detected. As a consequence, the ACC on the right
external ear may arise from the underlying ceruminous gland or
adjacent salivary gland. ACC is known for having long periods of no
growth, or indolence, followed by growth spurts. However, ACC may
present as aggressive forms in certain patients, making the course
of the ACC unpredictable (10). The
long period of the cancer evolving was reflected in the patient of
the present case report.
A biopsy is essential for the diagnosis of ACC. It
has a characteristic cribiform or sieve-like pattern, in which
bundles of epithelial cells surround ducts or glandular structures
(16,17). In cutaneous ACC, the tumor tissue is
rarely attached to the epidermis or hair follicles. Mitotic
activity is rare and peripheral palisading is uncommon (17). Immunohistochemistry is useful for the
diagnosis of ACC (16,18). ACC is characterized by slow
progression but has a high propensity to invade and metastasize,
particularly via perineural invasion, which occurs in ≤70% of ACC
cases (19). ACC involving the skull
base (orbital contents/bone, sinonasal cavities, nasopharynx,
cavernous sinus, clivus, pterygopalatine fossa and infratemporal
fossa) is usually identified via novel imaging techniques (20). Clinically, imaging techniques,
primarily MRI or CT scan, are useful in order to determine the size
and location of the tumor (9,21), and a
positron emission tomography scan may also be used to detect
metastatic lesions early (22).
The primary treatment modalities are surgery and
radiation therapy. Surgical removal of the tumor is the best
treatment for ACC as long as it is performed safely and is likely
to have a good outcome. Radiation therapy, as an adjuvant therapy
following surgery, is particularly effective for ACC by eliminating
microscopic cancer cells. Certain studies have indicated that
surgery alone was associated with improved overall survival
compared with a combination of surgery and radiotherapy, while
radiotherapy alone was associated with comparatively worse overall
survival (13). It is uncertain
whether chemotherapy alters the natural course of metastatic ACC at
any site (23,24). With further study on the pathogenesis
of ACC, more and more gene mutations have been detected, including
epidermal growth factor receptor (EGFR), ALK receptor tyrosine
kinase (25) and notch receptor 1
(NOTCH1) (26). At present, targeted
therapies are being developed that may be useful in the treatment
of ACC, including ALK-targeted gold nanoparticles and EGFR-tyrosine
kinase inhibitor gefitinib (6,7).
Previous studies have demonstrated that lung ACC is associated with
EGFR mutation and that it exhibited a good response to gefitinib
(6,7). Distant metastasis is a poor prognostic
factor, but nodal metastasis had no impact on overall survival.
Local recurrence is another common poor prognostic factor. Local
recurrences are frequent and may present as early as 2 years after
initial treatment, or after a number of years from the initial
treatment (5). In addition, a solid
pattern, higher age, black ethnicity and male sex are also poor
prognostic factors (11). The
survival rate for people with ACC at 5 years was reported to be
80.4–89.1% (20,27). Local recurrence and distant
metastasis result in poor long-term survival, with 80–90% of
patients succumbing to the disease within 10–15 years (28). According to the literature, skull
base metastasis is a predictor of lower overall survival and higher
rate of local recurrence (25).
Further molecular-level investigations are required in order to
improve the current understanding of the unique recurrence and
metastasis in ACC. Recently, B-cell-specific moloney murine
leukemia virus insertion region (Bmi)-1 mRNA levels were revealed
to be markedly elevated in ACC tissues compared with those in the
adjacent non-cancerous salivary gland tissues. Further study
suggested that Bmi-1 may have a crucial role in ACC progression
through interaction with the epithelial-to-mesenchymal
transition-associated markers, and may predict poor survival
(29).
In conclusion, ACC is an uncommon disease that
primarily arises from a salivary gland low-grade malignancy that
presents with unpredictable growth and poorly understood prognostic
factors. It is imperative for patients to receive an early
diagnosis and surgery to remove the tumor in a timely manner, which
may markedly improve the survival of these patients.
Acknowledgements
Not applicable.
Funding
The present study was partly supported by the
education training research project of the First Affiliated
Hospital of Army Medical University (grant no. SWH2015JY07y to
ZZ).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
ZZ was responsible for the conception, design,
content and writing of the manuscript. JH was responsible for
acquisition, analysis and interpretation of the images. YY made
substantial contributions to conception, design, drafting and
revising the manuscript. XY made substantial contributions to
acquisition, analysis and interpretation of data and revising the
manuscript critically for important intellectual content. ZS made
substantial contributions to conception and design, revising and
proofreading the manuscript and gave final approval of the version
to be published. All authors have read and approved the final
manuscript.
Ethics approval and consent to
participate
Ethics approval for the present study was obtained
from the Ethics Committee of the Southwest Hospital of Chongqing
(The First Affiliated Hospital of Army Medical University;
Chongqing, China). Informed consent was obtained from the
patient.
Patient consent for publication
The patient provided written informed consent for
publication of the present case report.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ko JJ, Siever JE, Hao D, Simpson R and Lau
HY: Adenoid cystic carcinoma of head and neck: Clinical predictors
of outcome from a Canadian centre. Curr Oncol. 23:26–33. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ellington CL, Goodman M, Kono SA, Grist W,
Wadsworth T, Chen AY, Owonikoko T, Ramalingam S, Shin DM, Khuri FR,
et al: Adenoid cystic carcinoma of the head and neck: Incidence and
survival trends based on 1973–2007 surveillance, epidemiology, and
end results data. Cancer. 118:4444–4451. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Brookstone MS, Huvos AG and Spiro RH:
Central adenoid cystic carcinoma of the mandible. J Oral Maxillofac
Surg. 48:1329–1333. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zhang CY, Xia RH, Han J, Wang BS, Tian WD,
Zhong LP, Tian Z, Wang LZ, Hu YH and Li J: Adenoid cystic carcinoma
of the head and neck: Clinicopathologic analysis of 218 cases in a
Chinese population. Oral Surg Oral Med Oral Pathol Oral Radiol.
115:368–375. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bradley PJ: Adenoid cystic carcinoma of
the head and neck: A review. Curr Opin Otolaryngol Head Neck Surg.
12:127–132. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Fujita M, Matsumoto T, Hirano R, Uchino J,
Hirota T, Yamaguchi E, Kubo A, Yokoi T, Nabeshima K and Watanabe K:
Adenoid cystic carcinoma of the lung with an EGFR mutation. Intern
Med. 55:1621–1624. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Huo Z, Wu H, Li S and Liang Z: Molecular
genetic studies on EGFR, KRAS, BRAF, ALK, PIK3CA, PDGFRA, and DDR2
in primary pulmonary adenoid cystic carcinoma. Diagn Pathol.
10:1612015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Agunbiade MM, Lalehparvar S and Khaladj M:
Cutaneous adenoid cystic carcinoma with perineural invasion
diagnosed in the foot: A case report. J Am Podiatr Med Assoc.
107:457–460. 2017. View
Article : Google Scholar : PubMed/NCBI
|
|
9
|
Treitl D, Radkani P, Rizer M, EI Hussein
S, Paramo JC and Mesko TW: Adenoid cystic carcinoma of the breast,
20 years of experience in a single center with review of
literature. Breast Cancer. 25:28–33. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Rais M, Kharmoum J, Ech-Charif S and EI
Khannoussi B: Adenoid cystic carcinoma of the uterine cervix: A
report of 2 cases. Case Rep Pathol. 2017:84017412017.PubMed/NCBI
|
|
11
|
Dong F, Gidley PW, Ho T, Luna MA,
Gingsberg LE and Sturgis FM: Adenoid cystic carcinoma of external
auditory canal. Laryngoscope. 118:1591–1596. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ouaz K, Robier A, Lescanne E, Bobillier C,
Morinière S and Bakhos D: Cancer of the external auditory canal.
Eur Ann Otorhinolaryngol Head Neck Dis. 130:175–182. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Green RW and Megwalu UC: Adenoid cystic
carcinoma of the external ear: A population based study. Am J
Otolaryngol. 37:346–350. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Min R, Siyi L, Wenjun Y, Ow A, Lizheng W,
Minjun D and Chenping Z: Salivary gland adenoid cystic carcinoma
with cervical lymph node metastasis: A preliminary study of 62
cases. Int J Oral Maxillofac Surg. 41:952–927. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ferlito A, Shaha AR, Silver CE, Rinaldo A
and Mondin V: Incidence and sites of distant metastases from head
and neck cancer. ORL J Otorhinolaryngol Relat Spec. 63:202–207.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Arps DP, Chan MP, Patel RM and Andea AA:
Primary cutaneous cribriform carcinoma: Report of six cases with
clinicopathologic data and immunohistochemical profile. J Cutan
Pathol. 42:379–387. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Ramakrishnan R, Chaudhry IH, Ramdial P,
Lazar AJ, McMenamin ME, Kazakov D, Brenn T and Calonje E: Primary
cutaneous adenoid cystic carcinoma: A clinicopathologic and
immunohistochemical study of 27 cases. Am J Surg Pathol.
37:1603–1611. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
van Weert S, Bloemena E, van der Waal I,
de Bree R, Rietveld DH, Kuik JD and Leemans CR: Adenoid cystic
carcinoma of the head and neck: A single-center analysis of 105
consecutive cases over a 30-year period. Oral Oncol. 49:824–829.
2013. View Article : Google Scholar
|
|
19
|
Alkan BI, Bozdogan O, Karadeniz M and
Bozdoğan N: Two different cell populations is an important clue for
diagnosis of primary cutaneous adenoid cystic carcinoma:
Immunohistochemical study. Case Rep Pathol.
2017:79493612017.PubMed/NCBI
|
|
20
|
Jang S, Patel PN, Kimple RJ and McCulloch
TM: Clinical outcomes and prognostic factors of adenoid cystic
carcinoma of the head and neck. Anticancer Res. 37:3045–3052.
2017.PubMed/NCBI
|
|
21
|
Kumar PP, Patil AA, Ogren FP, Johansson SL
and Reeves MA: Intracranial skip metastasis from parotid and facial
skin tumors: Mechanism, diagnosis, and treatment. J Natl Med Assoc.
85:369–374. 1993.PubMed/NCBI
|
|
22
|
Girelli L, Locati L, Galeone C, Scanagatta
P, Duranti L, Licitra L and Pastorino U: Lung metastasectomy in
adenoid cystic cancer: Is it worth it? Oral Oncol. 65:114–118.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Honings J, van Dijck JA, Verhagen AF, van
der Heijden HF and Marres HA: Incidence and treatment of tracheal
cancer: A nationwide study in the Netherlands. Ann Surg Oncol.
14:968–969. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Laurie SA, Ho AL, Fury MG, Sherman E and
Pfister DG: Systemic therapy in the management of metastatic or
locally recurrent adenoid cystic carcinoma of the salivary glands:
A systematic review. Lancet Oncol. 12:815–824. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Hazkani I, Motiei M, Betzer O, Sadan T,
Bragilovski D, Lubimov L, Mizrachi A, Hadar T, Levi M, Ben-Aharon
I, et al: Can molecular profiling enhance radiotherapy? Impact of
personalized targeted gold nanoparticles on radiosensitivity and
imaging of adenoid cystic carcinoma. Theranostics. 7:3962–3971.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ferrarotto R, Mitani Y, Diao L, Guijarro
I, Wang J, Zweidler-McKay P, Bell D, William WN Jr, Glisson BS,
Wick MJ, et al: Activating NOTCH1 mutations define a distinct
subgroup of patients with adenoid cystic carcinoma who have poor
prognosis, propensity to bone and liver metastasis, and potential
responsiveness to Notch1 inhibitors. J Clin Oncol. 35:352–360.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Cao C, Ge M, Chen X, Xu J and Chen C:
Clinical outcomes and prognostic factors of salivary gland adenoid
cystic carcinomas: A case control study. Oral Surg Oral Med Oral
Pathol Oral Radiol. 123:531–535. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Thompson L: World health organization
classification of tumours: Pathology and genetics of head and neck
tumours. Ear Nose Throat J. 85:742006. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Yi C, Li BB and Zhou CX: Bmi-1 expression
predicts prognosis in salivary adenoid cystic carcinoma and
correlates with epithelial-mesenchymal transition-related factors.
Ann Diagn Pathol. 22:38–44. 2016. View Article : Google Scholar : PubMed/NCBI
|