Introduction
Previous studies have, demonstrate that immune cell
infiltration in human gastrointestinal cancers is associated with
cancer progression and is a favorable prognostic predictor
(1–5). Both cellular composition and
organization of tumor infiltrating lymphocytes (TILs) are crucial
for inhibiting cancer progression and are implicated in the success
of cancer immunotherapy (1,2,6).
Tertiary lymphoid structure (TLSs) are an important source of TILs,
characterized by ectopic aggregated lymphocytes with high
endothelial venules and have a similar function to secondary
lymphoid organs (SLOs). The lymphocytes in TLSs have easy access to
tumor antigens as TLSs are not encapsulated and embedded within the
tumor microenvironment (5). The
numbers of both TILs and TLSs within solid tumor tissues can be
used for the assessment of tumor immune surveillance and are
important prognostic factors for cancer (7–11).
Although TLSs are thought to be associated with
anti-tumor immune responses (12–15), the
functional role of their cellular components remains unclear. TLSs
are divided into B- and T-zones, which consist of follicular
dendritic cells (FDCs) and fibroblastic reticular cells (FRCs),
respectively (16). TLSs can be
further defined as primary and secondary TLSs, based on the absence
or presence of a germinal center in B-cell follicles. Following
stimulation by tumor antigens, B cells differentiate and form the
germinal center, which is the site of B cell proliferation, class
switching and somatic hyper mutation (17–19).
CD4+ CXCR5+ T follicular helper (Tfh) cells
are a subtype of CD4+ helper T cells, principally
located in germinal centers, and play critical roles in recruiting,
activating and regulating the germinal center (20–22).
Previous studies suggested that Tfh cells mediate follicular and
germinal center formation in TLSs (23,24). In
recent studies, CXCR5+ CD8+ T cells were
found within the lymphoid follicle, primarily within the germinal
center, where they controlled viral replication during chronic HIV
and lymphocytic choriomeningitis virus (LMCV) infection (25,26). The
CD20+ B cells and CD8+ T cells co-localize in
the tumor nest (20) and TLSs
(21). This distribution pattern of
follicular CD8+ T cells might be involved in antitumor
immune responses.
The present study investigated follicular
CD8+ T cells in the tumor tissues of patients with
gastric cancer (GC). In addition, germinal center CD8+
(gcCD8+) TILs were quantified. The relationship between
tumoral immune parameters such as TILs, TLSs, TILs-TLSs and
gcCD8+ TILs and clinical pathological parameters was
determined.
Materials and methods
Patients and tissue samples
The present study retrospectively analyzed data of
patients admitted to the Department of Pathology, Third Affiliated
Hospital of Soochow University between 2006 to 2008. The patients
were enrolled according to the following criteria: i)
Pathologically-confirmed diagnosis of primary GC (adenocarcinoma);
ii) did not receive pre-operative chemotherapy or radiotherapy;
iii) presence of adequate paraffin-embedded fixed tissue blocks;
iv) at least one slide contained the invasive margin of the tumor;
and v) availability of complete medical records and follow-up
information. A total of 63 patients with GC were included in this
present study. Tumor clinical and pathological staging system was
based on the Eighth Edition of the Union for International Cancer
Control/American Joint Committee on Cancer. Three slides contain
cancer tissue were available for each patient, and a total of 189
slides were reviewed in the present study. Patient survival data
were available until the end of November 2011. Patient clinical
data are presented in Table I. The
present study was approved by the Ethics Committee of Soochow
University, and complied with the Declaration of Helsinki. Informed
consent to use the tissue sample for scientific research was
obtained from all patients.
 | Table I.Details of parameters in the study
cohort. |
Table I.
Details of parameters in the study
cohort.
|
| Total study
cohort |
|---|
|
|
|
|---|
| Parameters | n | % |
|---|
| Sex |
|
|
|
Male | 49 | 77.8 |
|
Female | 14 | 22.2 |
| Age, years |
|
|
|
≤50 | 8 | 12.7 |
|
>50 | 55 | 87.3 |
| Tumor size |
|
|
| ≤5
cm | 39 | 61.9 |
| >5
cm | 24 | 38.1 |
| Nerve invasion |
|
|
|
Yes | 25 | 39.7 |
| No | 38 | 60.3 |
| Tumor thrombus |
|
|
|
Yes | 22 | 34.9 |
| No | 41 | 65.1 |
| Nodal
metastasis |
|
|
|
Yes | 36 | 57.1 |
| No | 27 | 42.9 |
| Histological
grade |
|
|
|
I–II | 30 | 47.6 |
|
III | 33 | 52.4 |
| pTN stage |
|
|
| I | 23 | 36.5 |
| II | 13 | 20.6 |
|
III | 27 | 42.9 |
| TILs |
|
|
|
High | 44 | 69.8 |
|
Low | 19 | 30.2 |
| TLSs |
|
|
|
High | 43 | 68.3 |
|
Low | 20 | 31.7 |
| TILs and TLSs |
|
|
|
High | 32 | 50.8 |
|
Low | 31 | 49.2 |
| gcCD8+
TILsa |
|
|
|
High | 23 | 41.8 |
|
Low | 32 | 58.2 |
Pathomorphological evaluation of TILs
and TLSs
Cancer tissue was fixed in 10% (v/v) formalin and
embedded in paraffin until use. The H&E stained slides of the
resected GC tissues were reviewed and scored independently by two
pathologists who were blinded to the clinical data and prognosis of
the patients. The pathologists were trained in the
pathomorphological evaluation of TILs and TLSs, and any problematic
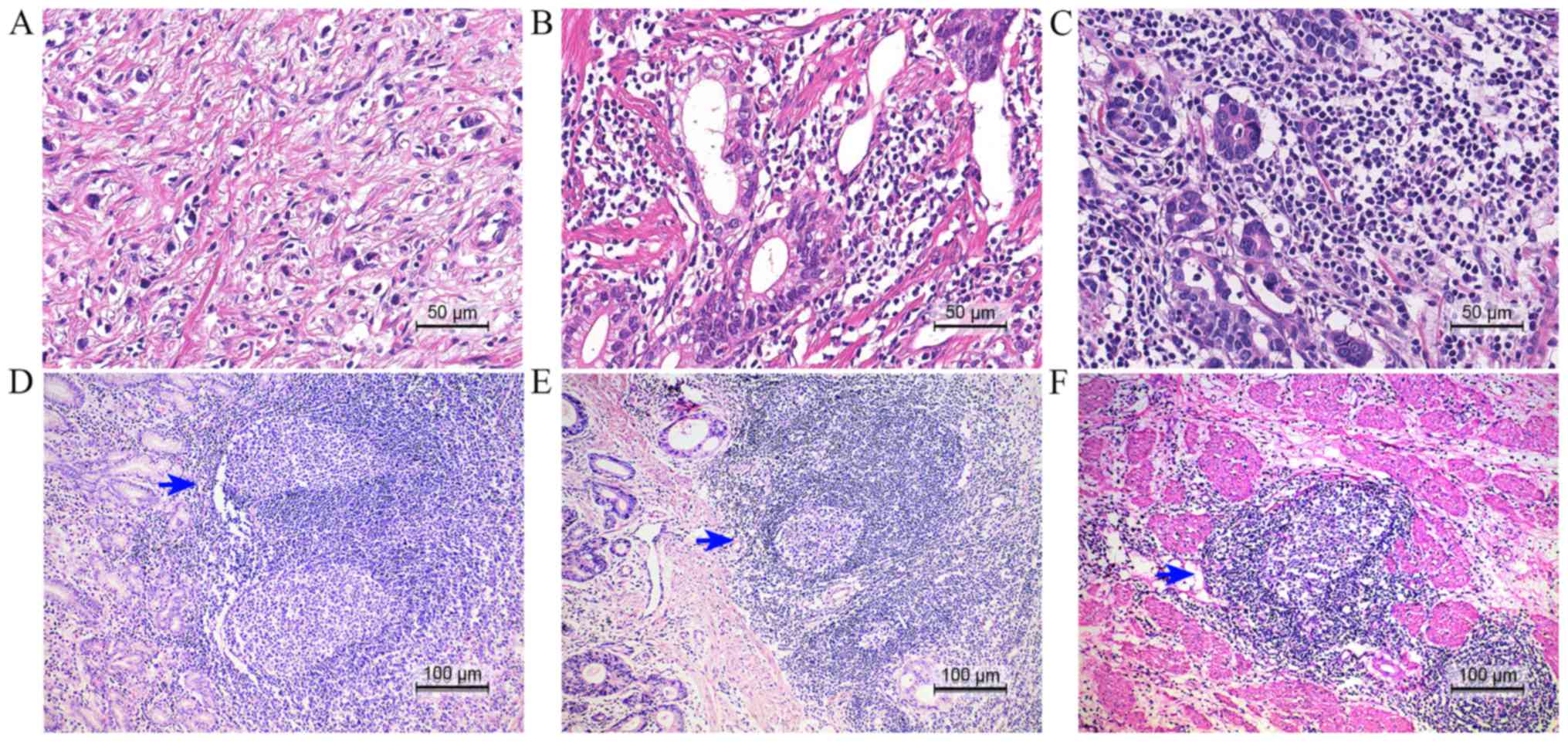
cases were discussed with them during subsequent scoring. The TILs
and TLSs in the center of the tumor (CT) and the invasive margin
(IM) were examined (11,27,28). The
TILs scoring system incorporated two aspects: i) The number of
infiltrating lymphocytes; score 0, no infiltration; score 1, mild
infiltration; score 2, moderate infiltration; score 3, extensive
infiltration (Fig. 1); and ii) the
percentage of the tumor area containing TILs in the CT or IM. The
CT-TILs and IM-TILs location scores were defined as the number of
infiltrating lymphocytes multiplied by the percentage, and then,
the final score was computed by summation of the CT- and IM-TILs
scores. TLSs were also evaluated in the CT and IM by measuring two
factors: The number of TLSs (aggregates of lymphocytes with and
without germinal centers were counted) and the percentage, similar
to the TILs, in the CT or IM (29,30). The
CT-TLSs and IM-TLSs location scores were defined as the numbers
multiplied by the percentage, and then, the final score of TLSs was
computed by summation of the CT- and IM-TLS scores.
Immunohistochemistry and evaluation of
the gcCD8+ T cells
Formalin-fixed and paraffin-embedded (FFPE) tissues
were cut into 4 µm thick consecutive sections deparaffinized in
xylene and rehydrated in graded ethanol solutions. Monoclonal mouse
antibody against human CD8 (MAB-0021, ready to use, Maixin
Biotechnology Limited Corporation) was used to stain the T
lymphocytes. The CD8 antigen was retrieved by boiling the slides in
citrate buffer (10 mmol/l; pH 6.0) under high pressure for 2 min.
Then, the sections were immersed in 3% hydrogen peroxide for 10 min
to block endogenous peroxidase activity, rinsed three times in PBS,
and then incubated with primary antibodies at 4°C overnight. The
negative control was performed with PBS. The sections were
incubated with horseradish peroxidase-labeled goat anti-mouse
secondary antibody (ready to use, Maixin Biotechnology Limited
Corporation). Diaminobenzene was used as the chromogen and
hematoxylin as the nuclear counterstain. The scoring system for
gcCD8+ TILs was assessed in every slide. The number of
germinal centers and gcCD8+ TILs in each germinal center
were counted. The average values were subsequently obtained.
Statistical analysis
Statistical analyses were performed using SPSS
(version 24.0; IBM Corp.) and GraphPad Prism software (version 6;
GraphPad Software, Inc.). Data were analyzed using the
χ2 test, Kaplan-Meier method and Cox regression analysis
as appropriate. All tests were two-sided and P<0.05 was
considered to indicate a statistically significant difference.
Results
Relationship between tumoral immune
parameters and clinical pathological parameters
The TILs, TLSs, and gcCD8+ TILs were
defined as tumoral immune parameters in the present study (Tables I and II). In order to make the scoring system
more facilitative to statistical analysis, these variables were
converted into binary variables. TILs were sub-grouped by the TIL
final score: TILhi 44 cases, score >0.45 [area under
the receiver operating characteristic curve (AUC)=0.35;
sensitivity, 82.1%; specificity, 50.0%], and TILlow 19
cases, score ≤0.45 (Table I;
Fig. 1A-C). TLSs were sub-grouped by
the TLS final score: TLShi 43 cases, score >0.42
(AUC=0.39; sensitivity, 79.5%; specificity, 50.0%), and
TLSlow 20 cases, score ≤0.42 (Table I; Fig.
1D-F). Considering the combination of TILs and TLSs, the
samples were divided into two groups. The TIL-TLShi
group (32 cases) consisted of samples that scored as both
TILhi and TLShi. The TIL-TLSlow
group (31 cases) consisted of samples that scored as
TILhi-TLSlow,
TILlow-TLShi and
TILlow-TLSlow (Table I). Based on the density of
gcCD8+ TILs, 55 samples (specimens from eight cases were
excluded due to absence of germinal centers) were divided into two
groups: gcCD8hi TIL, 23 cases, score >6.93 (AUC=0.19;
sensitivity, 59.5%; specificity, 94.4%; Fig. 2A-F), and gcCD8low TIL, 32
cases, score ≤6.93 (Table I;
Fig. 2G-L).
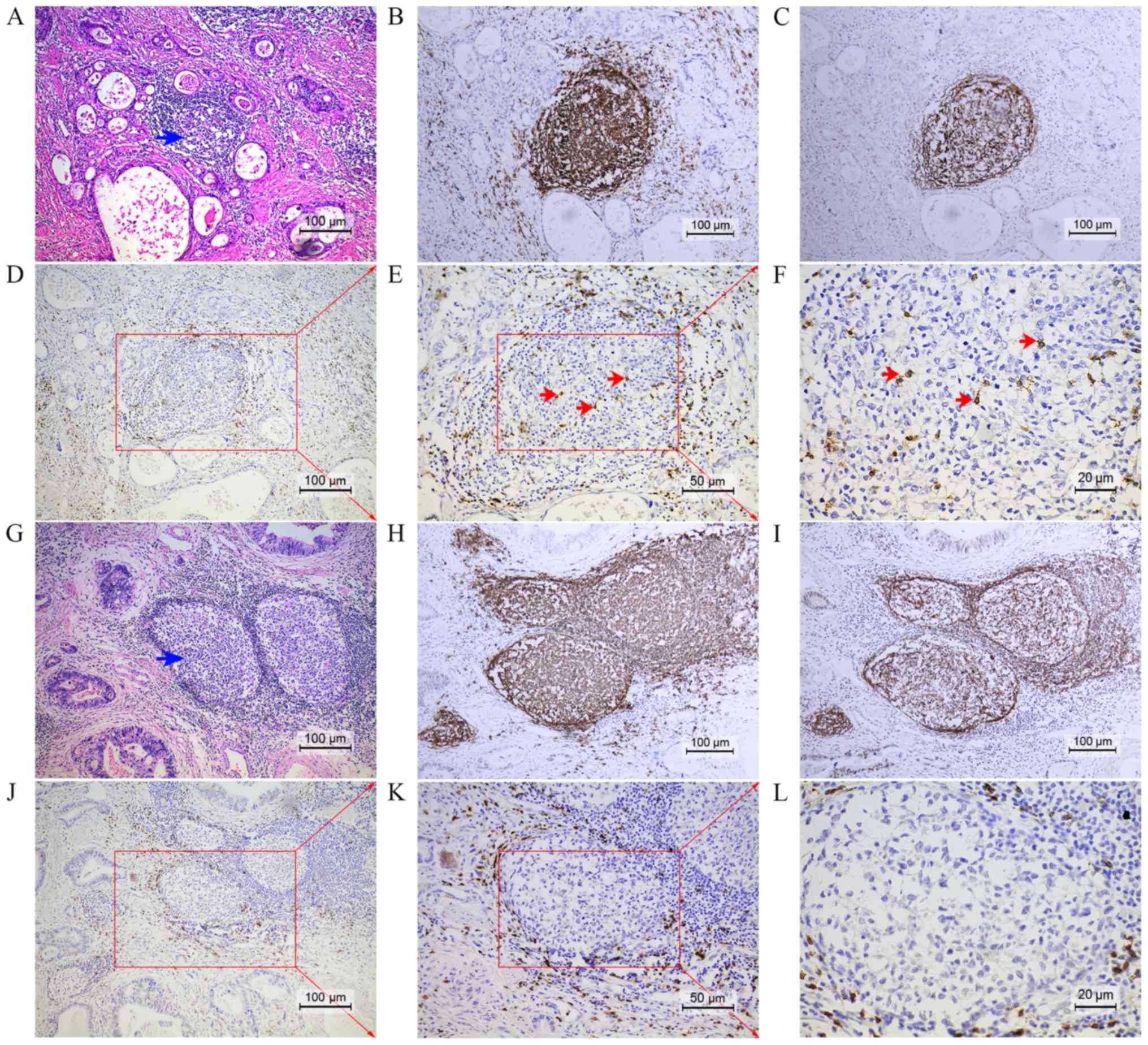 | Figure 2.Two cases of (A-F) gcCD8hi
TILs and (G-L) gcCD8low TILs were presented. (A) Case 1
had the TLS with a follicle and germinal center (marked with blue
arrow) in HE slides. (B) CD20 staining revealed B lymphocyte
aggregation and the germinal center. (C) CD21 staining revealed the
follicular dendritic cell network in the germinal center. (D)
Enlarged images of the red square area revealed follicular
CD8+ TILs around the germinal center. (E and F)
gcCD8+ TILs were detected in the germinal center (red
arrows). (G) TLS marked with a blue arrow were also observed in
Case 2. (H-J) The same expression pattern of CD20, CD21 and CD8 was
observed. (K-L) Conversely, there were no gcCD8+ TILs
that infiltrated into the germinal center. (A-D and G-J)
Magnification, ×100; scale bar, 100 µm. (E and K) Magnification,
×200; scale bar, 50 µm. (F and L) Magnification, ×400; scale bar,
20 µm. TLS, tertiary lymphoid structure; CD, cluster of
differentiation; HE, hematoxylin and eosin; TILs, tumor
infiltrating lymphocytes. |
| Table II.Association between
clinicopathological parameters and tumoral immune parameters. |
Table II.
Association between
clinicopathological parameters and tumoral immune parameters.
|
| gcCD8+
TILs |
|
| TILs |
|
| TLSs |
|
| TILs-TLSs |
|
|
|---|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|---|
| Parameters | Low | High | χ2 | P-value | Low | High | χ2 | P-value | Low | High | χ2 | P-value | Low | High | χ2 | P-value |
|---|
| Sex |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Male | 23 | 19 | 0.854 | 0.355 | 17 | 32 | 2.153 | 0.142 | 15 | 34 | 0.131 | 0.718 | 26 | 23 | 1.311 | 0.252 |
|
Female | 9 | 4 |
|
| 2 | 12 |
|
| 5 | 9 |
|
| 5 | 9 |
|
|
| Age (years) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
≤50 | 6 | 0 | 4.841 | 0.028 | 4 | 4 | 1.713 | 0.191 | 3 | 5 | 0.140 | 0.708 | 5 | 3 | 0.648 | 0.421 |
|
>50 | 26 | 23 |
|
| 15 | 40 |
|
| 17 | 38 |
|
| 26 | 29 |
|
|
| Tumor size |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| ≤5
cm | 18 | 17 | 1.804 | 0.179 | 7 | 32 | 7.246 | 0.007 | 12 | 27 | 0.045 | 0.832 | 16 | 23 | 2.741 | 0.098 |
| >5
cm | 14 | 6 |
|
| 12 | 12 |
|
| 8 | 16 |
|
| 15 | 9 |
|
|
| Nerve invasion |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes | 12 | 8 | 0.043 | 0.836 | 14 | 11 | 13.140 |
<0.001 | 10 | 15 | 1.303 | 0.254 | 18 | 7 | 8.616 | 0.003 |
| No | 20 | 15 |
|
| 5 | 33 |
|
| 10 | 28 |
|
| 13 | 25 |
|
|
| Tumor thrombus |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes | 13 | 4 | 3.383 | 0.066 | 10 | 12 | 3.755 | 0.053 | 10 | 12 | 2.932 | 0.087 | 16 | 6 | 7.483 | 0.006 |
| No | 19 | 19 |
|
| 9 | 32 |
|
| 10 | 31 |
|
| 15 | 26 |
|
|
| Nodal
metastasis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes | 20 | 9 | 2.932 | 0.087 | 16 | 20 | 8.139 | 0.004 | 12 | 24 | 0.098 | 0.755 | 22 | 14 | 4.763 | 0.029 |
| No | 12 | 14 |
|
| 3 | 24 |
|
| 8 | 19 |
|
| 9 | 18 |
|
|
| Histological
grade |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I–II | 11 | 16 | 6.631 | 0.010 | 5 | 25 | 4.950 | 0.026 | 8 | 22 | 0.682 | 0.409 | 10 | 20 | 5.773 | 0.016 |
|
III | 21 | 7 |
|
| 14 | 19 |
|
| 12 | 21 |
|
| 21 | 12 |
|
|
| pTN stage |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| I | 9 | 13 | 6.053 | 0.048 | 2 | 21 | 8.072 | 0.018 | 6 | 17 | 0.642 | 0.725 | 7 | 16 | 5.399 | 0.067 |
| II | 6 | 5 |
|
| 5 | 8 |
|
| 5 | 8 |
|
| 7 | 6 |
|
|
|
III | 17 | 5 |
|
| 12 | 15 |
|
| 9 | 18 |
|
| 17 | 10 |
|
|
The TILs were significantly associated with the
tumor size, nerve invasion, lymph nodal metastasis, histological
grade and pTN stage (P=0.007, 0.001, 0.004, 0.026 and 0.018,
respectively; Table II). The data
showed that the TLSs were not significantly associated with
clinical pathological parameters. The combination of TILs-TLSs was
significantly associated with nerve invasion, tumor thrombus, lymph
nodal metastasis and histological grade (P=0.003, 0.006, 0.029 and
0.016, respectively; Table II). The
data also showed the gcCD8+ TILs was significantly
associated with patient age, histological grade and pTN stage
(P=0.028, 0.010 and 0.048, respectively; Table II). The higher levels of
gcCD8+ TILs were associated with lower histological
grade and lower pTN stage. These data suggested that the
gcCD8+ TILs might be involved in antitumor immunity in
GC.
Association between tumoral immune
parameters and patient prognosis
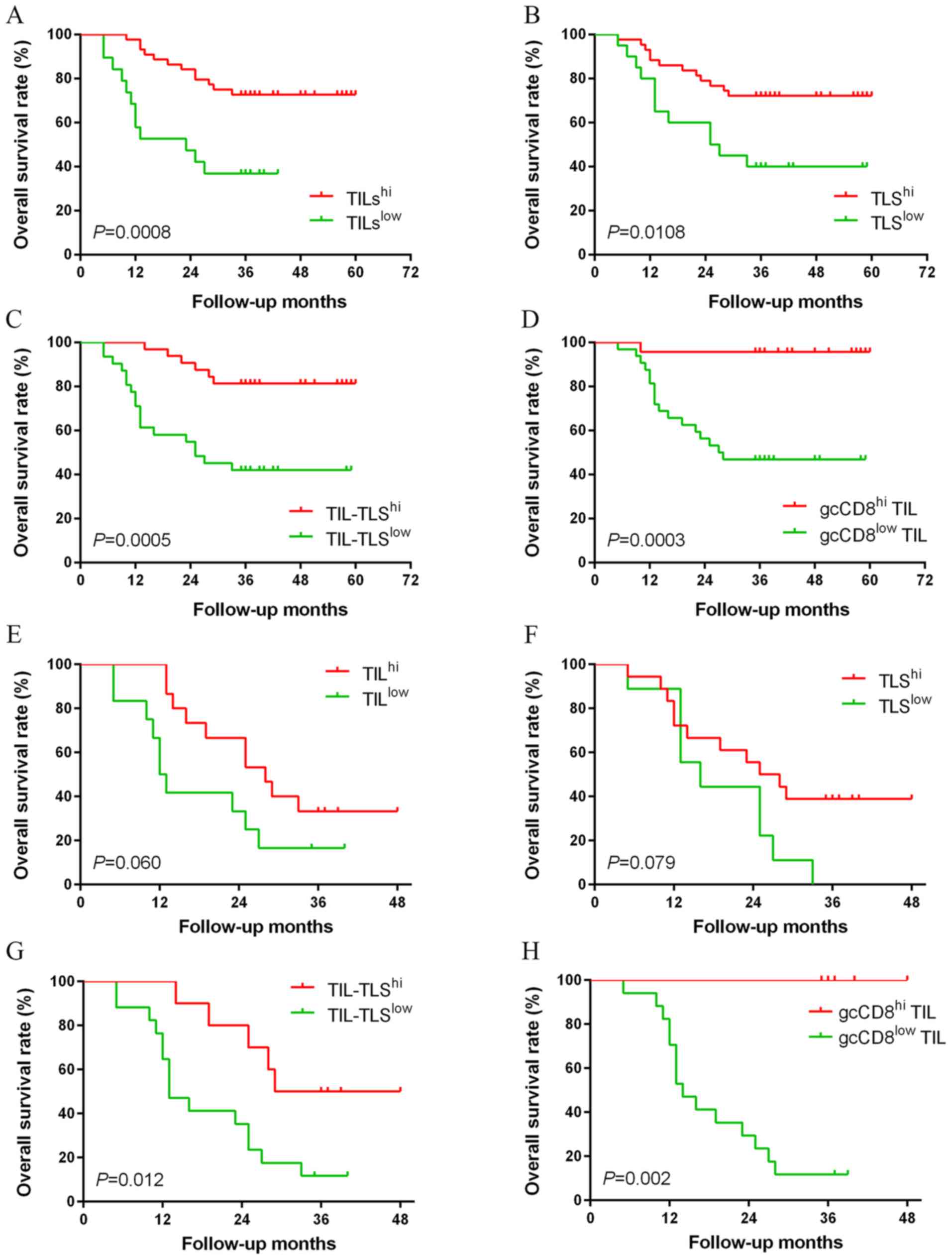
Kaplan-Meier survival analysis showed that the
patients with TILhi, TLShi,
TIL-TLShi or gcCD8hi TIL had favorable
prognosis than those with lower levels (P=0.0008, 0.0108, 0.0005
and 0.0003, respectively; Fig.
3A-D). The prognostic value of tumoral immune parameters in
patients with advanced GC (pTN III stage) was investigated. The
patients in the TIL-TLShi and gcCD8hi TIL
groups had an improved overall survival (OS) compared with patients
in the TIL-TLSlow and gcCD8low TIL groups
(P=0.012 and 0.002; Table III;
Fig. 3G and H).
| Table III.Kaplan-Meier analysis of tumoral
immune parameters. |
Table III.
Kaplan-Meier analysis of tumoral
immune parameters.
| A, Tumoral immune
parameters in all cases |
|---|
|
|---|
| Parameters | Cases, n | Status of
death | Mean OS,
months | Log-Rank
χ2 | P-value |
|---|
| TILs |
|
|
|
|
|
|
High | 44 | 12 | 49.25 | 11.198 | 0.001 |
|
Low | 19 | 12 | 24.21 |
|
|
| TLSs |
|
|
|
|
|
|
High | 43 | 12 | 48.14 | 6.501 | 0.011 |
|
Low | 20 | 12 | 33.40 |
|
|
| TILs-TLSs |
|
|
|
|
|
|
High | 32 | 6 | 53.03 | 12.148 |
<0.001 |
|
Low | 31 | 18 | 33.42 |
|
|
| gcCD8+
TILs |
|
|
|
|
|
|
High | 23 | 1 | 57.83 | 13.322 |
<0.001 |
|
Low | 32 | 17 | 36.16 |
|
|
|
| B, Tumoral
immune parameters in pTN III stage cases |
|
|
Parameters | Cases,
n | Status of
death | Mean OS,
months | Log-Rank
χ2 | P-value |
|
| TILs |
|
|
|
|
|
|
High | 12 | 10 | 30.33 | 3.527 | 0.06 |
|
Low | 15 | 10 | 18.58 |
|
|
| TLSs |
|
|
|
|
|
|
High | 18 | 11 | 19.11 | 3.089 | 0.079 |
|
Low | 9 | 9 | 18.89 |
|
|
| TILs-TLSs |
|
|
|
|
|
|
High | 10 | 5 | 35.50 | 6.310 | 0.012 |
|
Low | 17 | 15 | 19.00 |
|
|
| gcCD8+
TILs |
|
|
|
|
|
|
High | 5 | 0 | – | 9.334 | 0.002 |
|
Low | 17 | 15 | 18.65 |
|
|
In the univariate Cox regression analysis
(analysisa), smaller tumor size, lower histological
grade, absence of tumor thrombus or lymph nodal metastasis, lower
pTN stage and higher levels of tumoral immune parameters were
favorable prognostic factors for OS (Table IV). Considering the possible
interference among TILs, TLSs and TILs-TLSs, we did a cohort of
multivariate Cox regression analysis. Multivariate Cox regression
analysisb (based on the clinicopathological feature,
TILs, TLSs and gcCD8+ TILs) revealed that the
gcCD8+ TILs were the only independent prognostic factor
for OS (HR=0.087; 95% CI: 0.011–0.692; P=0.021; Table IV). Multivariate Cox regression
analysisc (based on the clinicopathological feature,
TILs-TLSs and gcCD8+ TILs) demonstrated that TILs-TLSs
and gcCD8+ TILs were independent prognostic factors
(HR=0.247, 95% CI: 0.069–0.882, P=0.031; HR=0.067, 95% CI:
0.008–0.561, P=0.013, respectively). Moreover, the multivariate Cox
regression analysisd was designed to determine the
association between tumoral immune parameters (TILs, TLSs and
gcCD8+ TILs). The result showed TILs and
gcCD8+ TILs could be used as independent prognostic
factors (HR=0.322, 95% CI: 0.124–0.835, P=0.020; HR=0.059, 95% CI:
0.008–0.451, P=0.006, respectively). The tumoral immune parameters
exhibited an HR <1 in the Cox regression analysis, suggesting
that may protect against tumor progression.
| Table IV.Univariate and multivariate Cox
regression analyses of clinicopathological parameters and tumoral
immune parameters. |
Table IV.
Univariate and multivariate Cox
regression analyses of clinicopathological parameters and tumoral
immune parameters.
| A, Univariate
analysis |
|---|
|
|---|
| Variables |
Unfavorable/favorable | HR | 95% CI | P-value |
|---|
| Sex | Male/Female | 0.863 | 0.343–2.176 | 0.755 |
| Age, years | ≤50/>50 | 0.747 | 0.255–2.187 | 0.594 |
| Tumor size, cm | ≤5/>5 | 3.643 | 1.587–8.363 | 0.002 |
| Histological
grade | I–II/III | 4.624 | 1.722–12.421 | 0.002 |
| Neural
Invasion | No/Yes | 2.168 | 0.969–4.847 | 0.060 |
| Tumor thrombus | No/Yes | 6.619 | 2.716–16.134 | 0.001 |
| Lymphatic
metastasis | No/Yes | 11.528 | 2.702–49.184 | 0.001 |
| pTN stage | I–II/III | 18.732 | 2.525–138.976 | 0.004 |
| TILs | High/Low | 0.279 | 0.125–0.623 | 0.002 |
| TLSs | High/Low | 0.370 | 0.166–0.825 | 0.015 |
| gcCD8+
TILs | High/Low | 0.062 | 0.008–0.470 | 0.007 |
| TILs-TLSs | High/Low | 0.376 | 0.222–0.636 | 0.000 |
|
| B, Multivariate
Cox regression analysis |
|
Variables |
Unfavorable/favorable | HR | 95% CI | P-value |
|
| Tumor size, cm | ≤5/>5 | 0.896 | 0.198–4.046 | 0.886 |
| Histological
grade |
I–II/III | 1.009 | 0.277–3.671 | 0.990 |
| Tumor thrombus | No/Yes | 2.227 | 0.482–10.748 | 0.299 |
| Lymphatic
metastasis | No/Yes | 1.251 | 0.135–11.560 | 0.844 |
| pTN stage | I–II/III | 5.594 | 0.336–93.237 | 0.230 |
| TILs | High/Low | 0.503 | 0.169–1.492 | 0.215 |
| TLSs | High/Low | 0.609 | 0.203–1.831 | 0.377 |
| gcCD8+
TILs | High/Low | 0.087 | 0.011–0.692 | 0.021 |
|
| C, Multivariate
Cox regression analysis |
|
|
Variables |
Unfavorable/favorable | HR | 95% CI | P-value |
|
| Tumor size, cm | ≤5/>5 | 1.208 | 0.273–5.355 | 0.803 |
| Histological
grade | I–II/III | 0.806 | 0.208–3.116 | 0.754 |
| Tumor thrombus | No/Yes | 1.742 | 0.381–7.970 | 0.474 |
| Lymphatic
metastasis | No/Yes | 0.980 | 0.103–9.296 | 0.986 |
| pTN stage | I–II/III | 7.159 | 0.419–122.410 | 0.174 |
| gcCD8+
TILs | High/Low | 0.067 | 0.008–0.561 | 0.013 |
| TILs-TLSs | High/Low | 0.247 | 0.069–0.882 | 0.031 |
|
| D, Multivariate
Cox regression analysis |
|
|
Variables |
Unfavorable/favorable | HR | 95% CI | P-value |
|
| TILs | High/Low | 0.322 | 0.124–0.835 | 0.020 |
| TLSs | High/Low | 0.396 | 0.148–1.056 | 0.064 |
| gcCD8+
TILs | High/Low | 0.059 | 0.008–0.451 | 0.006 |
Discussion
The present study demostrated that patients with GC
with higher levels of TILs, or TLSs, or gcCD8+ TILs had
an improved OS. Multivariate Cox regression analysis revealed that
TILs-TLSs and gcCD8+ TILs were independent prognostic
factors. In addition, gcCD8+ TILs were significantly
associated with patient age, histological grade and pTN stage.
Higher levels of TILs-TLSs was positively associated with the nerve
invasion, tumor thrombus, lymph nodal metastasis and histological
grade. The data obtained in the present study suggested that high
levels of tumoral immune parameters were associated with improved
prognosis in patients with GC.
Cancer progression is a multi-step process that
involves genetic, epigenetic, as well as histopathological change
(3,31–33).
Infiltrating immune cells play an important role in preventing or
promoting cancer progression (34).
Previous studies have demonstrated that high levels of TILs may
inhibit the progression of breast and colorectal cancer (8,31,35). The
present study revealed that a high level of TILs was associated
with improved prognosis in patient with GC. Univariate and
multivariate Cox regression analyses revealed that TILs could be
used as an independent favorable prognostic factor.
Previous studies demonstrated that TLSs are required
for the development of the T- and B-cell mediated immune response
against human cancer and various other diseases (25,26,31,36,37).
TLSs have been previously described in several types of cancer,
such as lung cancer and breast cancer, and are associated with
patient prognosis (10,17,29).
TLSs are organization by heterotopic lymphoid tissues, and exhibit
similar organization and functionality to SLOs. The basic
components of TLSs include the T-zone, comprising of T cells and
FRCs, and the B-zone, comprising of B cells and FDCs. TLSs are
involved in establishing a systemic memory response to protect
patients against circulating metastatic cancer cells, therefor
inhibiting tumor recurrence for several years (8,31). The
present study revealed that the high levels of TLSs were associated
with improved outcome in patients with GC, and could therefor be
used as an independent prognostic factor. The combination of TILs
and TLSs is superior to TILs or TLSs alone for predicting survival.
In advanced cancer, the high levels of TILs-TLSs were associated
with improved OS. Based on the results obtained in the present
study, TLSs are an important niche in which tumor antigen specific
T and B cells are generated.
Despite the association of gcCD8+ T cells
with improved prognosis, the role of gcCD8+ T cells in
antitumor immune responses and germinal center B cell responses
remains unknow. Previous studies investigating chronic infection
with LMCV and HIV revealed that there are two subsets of
CD8+ effector T cells, namely CXCR5+
PD-1+ CD8+ T and CXCR5−
PD-1+ CD8+ T cells (26,38). The
CXCR5+ subset exhibits stem cell-like properties and is
localized in the B cell follicle and germinal center during chronic
infection. The CXCR5+ subset undergo self-renewal and
can differentiate into CXCR5− CD8+ T cells.
The de novo converted CXCR5− subset exhibits
increased cytotoxicity and removes virus infected cells. Hornquist
et al (39) studied the role
of CD8+ T cells in the regulation of gut mucosal immune
responses and showed that CD8+ T cells inhibited local B
cell responses. By contrast, B cells and plasma cells have been
shown to impede T cell-mediated antitumor immune responses
(40–42). Based on the aforementioned findings,
gcCD8+ T cells are likely to promote cell-mediate
antitumor immune responses and inhibit humoral immunity. A
diagrammatic representation based on two hypotheses is presented in
Fig. S1. Based on the results
obtained from studies investigating chronic HIV or LMCV infection
(43,44), it is hypothesized that
PD1+ CD8+ TILs may be further divided into
CXCR5+ and CXCR5− subsets, which are
regulated by the inhibitor of DNA binding 2 (ID2)/transcription
factor E2-α axis. The CXCR5+ subset located in the B
cell follicle and the germinal center. The follicular
CXCR5+ CD8+ T cells subset can undergo
proliferation and differentiate into the CXCR5− subset
following ID2 upregulation. 2. According to the studies by
Hornquist et al (39) and Li
et al (44), germinal center
CXCR5+ CD8+ T cells can exert a suppressive
effect on germinal B cell responses and inhibit the generation of
plasma cells. Some mechanisms in these hypotheses were
demonstrated. Elimination of immunosuppressive B cells expressing
IgA, IL-10 and PD-L1 allows CD8+ cytotoxic T cells
eradication of oxaliplatin-resistance prostate cancer (40). The expression of CXCR5 on
CD8+ T cells was necessary for T cells infiltrating into
B-cells follicular (43). The
present study revealed that the phenotype of TILs, TLSs and
gcCD8+ TILs exhibited significant heterogeneity in
patients with GC. TILs, TLSs and gcCD8+ TILs may be had
the potential function associated with GC immunotherapy. Further
investigation is required to validate the hypotheses proposed in
the present study.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
This work was supported by grants from the National
Natural Science Foundation of China (No. 31701111), Key R&D
Project of Science and Technology Department of Jiangsu Province
(BE2015633). Changzhou Health and Family Planning Commission Youth
Talent Science and Technology Project (QN201709). This work was
also supported in part by Roswell Park Cancer Institute/University
of Pittsburgh Cancer Institute Ovarian Cancer Specialized Programs
of Research Excellence Grants (P50CA159981).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
QL, DZ and WH designed the study and wrote the
manuscript. DZ, TC, ZY, XG and LC performed all of the experiments.
XZ and BX performed the statistical analysis. BL and JJ conceived
and designed the study, guided the experiments and revised the
manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of Soochow University, and complied with the Declaration
of Helsinki. Informed consent to use the tissue sample for
scientific research was obtained from all patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
TILs
|
tumor infiltrating lymphocytes
|
|
TLSs
|
tertiary lymphoid structures
|
|
GC
|
gastric cancer
|
|
Tfc
|
follicular CD8+ cytotoxic T
cells
|
|
gcCD8+ TILs
|
germinal center CD8+
TILs
|
|
SLO
|
secondary lymphoid organs
|
|
TME
|
tumor microenvironment
|
|
FDC
|
follicular dendritic cell
|
|
FRC
|
fibroblastic reticular cell
|
|
CT
|
center of the tumor
|
|
IM
|
invasive margin
|
|
pTN
|
pathological tumor and lymph node
|
|
AUC
|
area under the receiver operating
charatcteristic curve
|
References
|
1
|
Chen LJ, Sun J, Wu HY, Zhou SM, Tan Y, Tan
M, Shan BE, Lu BF and Zhang XG: B7-H4 expression associates with
cancer progression and predicts patient's survival in human
esophageal squamous cell carcinoma. Cancer Immunol Immunother.
60:1047–1055. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chen LJ, Zheng X, Shen YP, Zhu YB, Li Q,
Chen J, Xia R, Zhou SM, Wu CP, Zhang XG, et al: Higher numbers of
T-bet(+) intratumoral lymphoid cells correlate with better survival
in gastric cancer. Cancer Immunol Immunother. 62:553–561. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Xu Y, Chen L, Xu B, Xiong Y, Yang M, Rui
X, Shi L, Wu C, Jiang J and Lu B: Higher numbers of T-Bet+
tumor-infiltrating lymphocytes associate with better survival in
human epithelial ovarian cancer. Cell Physiol Biochem. 41:475–483.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zhu Y, Ju S, Chen E, Dai S, Li C, Morel P,
Liu L, Zhang X and Lu B: T-bet and eomesodermin are required for T
cell-mediated antitumor immune responses. J Immunol. 185:3174–3183.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Pimenta EM and Barnes BJ: Role of tertiary
lymphoid structures (TLS) in anti-tumor immunity: Potential
tumor-induced cytokines/chemokines that regulate TLS formation in
epithelial-derived cancers. Cancers (Basel). 6:969–997. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Singer M, Wang C, Cong L, Marjanovic ND,
Kowalczyk MS, Zhang H, Nyman J, Sakuishi K, Kurtulus S, Gennert D,
et al: A distinct gene module for dysfunction uncoupled from
activation in tumor-infiltrating T cells. Cell. 166:1500–1511.e9.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Dieu-Nosjean MC, Antoine M, Danel C,
Heudes D, Wislez M, Poulot V, Rabbe N, Laurans L, Tartour E, de
Chaisemartin L, et al: Long-term survival for patients with
non-small-cell lung cancer with intratumoral lymphoid structures. J
Clin Oncol. 26:4410–4417. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Galon J, Costes A, Sanchez-Cabo F,
Kirilovsky A, Mlecnik B, Lagorce-Pagès C, Tosolini M, Camus M,
Berger A, Wind P, et al: Type, density, and location of immune
cells within human colorectal tumors predict clinical outcome.
Science. 313:1960–1964. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Pagès F, Berger A, Camus M, Sanchez-Cabo
F, Costes A, Molidor R, Mlecnik B, Kirilovsky A, Nilsson M, Damotte
D, et al: Effector memory T cells, early metastasis, and survival
in colorectal cancer. N Engl J Med. 353:2654–2666. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Goc J, Fridman WH, Sautès-Fridman C and
Dieu-Nosjean MC: Characteristics of tertiary lymphoid structures in
primary cancers. Oncoimmunology. 2:e268362013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Zhang D, He W, Wu C, Tan Y, He Y, Xu B,
Chen L, Li Q and Jiang J: Scoring system for tumor-infiltrating
lymphocytes and its prognostic value for gastric cancer. Front
Immunol. 10:712019. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Martinet L, Filleron T, Le Guellec S,
Rochaix P, Garrido I and Girard JP: High endothelial venule blood
vessels for tumor-infiltrating lymphocytes are associated with
lymphotoxin beta-producing dendritic cells in human breast cancer.
J Immunol. 191:2001–2008. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Cipponi A, Mercier M, Seremet T, Baurain
JF, Théate I, van den Oord J, Stas M, Boon T, Coulie PG and van
Baren N: Neogenesis of lymphoid structures and antibody responses
occur in human melanoma metastases. Cancer Res. 72:3997–4007. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
de Chaisemartin L, Goc J, Damotte D,
Validire P, Magdeleinat P, Alifano M, Cremer I, Fridman WH,
Sautès-Fridman C and Dieu-Nosjean MC: Characterization of
chemokines and adhesion molecules associated with T cell presence
in tertiary lymphoid structures in human lung cancer. Cancer Res.
71:6391–6399. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Bergomas F, Grizzi F, Doni A, Pesce S,
Laghi L, Allavena P, Mantovani A and Marchesi F: Tertiary
intratumor lymphoid tissue in colo-rectal cancer. Cancers (Basel).
4:1–10. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Joshi NS, Akama-Garren EH, Lu Y, Lee DY,
Chang GP, Li A, DuPage M, Tammela T, Kerper NR, Farago AF, et al:
Regulatory T cells in tumor-Associated tertiary lymphoid structures
suppress anti-tumor T cell responses. Immunity. 43:579–590. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Goc J, Germain C, Vo-Bourgais TK, Lupo A,
Klein C, Knockaert S, de Chaisemartin L, Ouakrim H, Becht E,
Alifano M, et al: Dendritic cells in tumor-associated tertiary
lymphoid structures signal a Th1 cytotoxic immune contexture and
license the positive prognostic value of infiltrating CD8+ T cells.
Cancer Res. 74:705–715. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Gu-Trantien C, Loi S, Garaud S, Equeter C,
Libin M, de Wind A, Ravoet M, Le Buanec H, Sibille C,
Manfouo-Foutsop G, et al: CD4+ follicular helper T cell
infiltration predicts breast cancer survival. J Clin Invest.
123:2873–2892. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Gottlin EB, Bentley RC, Campa MJ, Pisetsky
DS, Herndon JE II and Patz EF Jr: The association of intratumoral
germinal centers with early-stage non-small cell lung cancer. J
Thorac Oncol. 6:1687–1690. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
McHeyzer-Williams LJ and McHeyzer-Williams
MG: Antigen-specific memory B cell development. Annu Rev Immunol.
23:487–513. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Bos R and Sherman LA: CD4+ T-cell help in
the tumor milieu is required for recruitment and cytolytic function
of CD8+ T lymphocytes. Cancer Res. 70:8368–8377. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Bos R, Marquardt KL, Cheung J and Sherman
LA: Functional differences between low- and high-affinity CD8(+) T
cells in the tumor environment. Oncoimmunology. 1:1239–1247. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kroenke MA, Eto D, Locci M, Cho M,
Davidson T, Haddad EK and Crotty S: Bcl6 and Maf cooperate to
instruct human follicular helper CD4 T cell differentiation. J
Immunol. 188:3734–3744. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Wang C, Hillsamer P and Kim CH: Phenotype,
effector function, and tissue localization of PD-1-expressing human
follicular helper T cell subsets. BMC Immunol. 12:532011.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Petrovas C, Ferrando-Martinez S, Gerner
MY, Casazza JP, Pegu A, Deleage C, Cooper A, Hataye J, Andrews S,
Ambrozak D, et al: Follicular CD8 T cells accumulate in HIV
infection and can kill infected cells in vitro via bispecific
antibodies. Science translational medicine. 9:eaag22852017.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
He R, Hou S, Liu C, Zhang A, Bai Q, Han M,
Yang Y, Wei G, Shen T, Yang X, et al: Follicular CXCR5- expressing
CD8(+) T cells curtail chronic viral infection. Nature.
537:412–428. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Galon J, Mlecnik B, Bindea G, Angell HK,
Berger A, Lagorce C, Lugli A, Zlobec I, Hartmann A, Bifulco C, et
al: Towards the introduction of the ‘Immunoscore’ in the
classification of malignant tumours. J Pathol. 232:199–209. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Hennequin A, Derangère V, Boidot R, Apetoh
L, Vincent J, Orry D, Fraisse J, Causeret S, Martin F, Arnould L,
et al: Tumor infiltration by Tbet+ effector T cells and CD20+ B
cells is associated with survival in gastric cancer patients.
Oncoimmunology. 5:e10545982016. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Lee HJ, Park IA, Song IH, Shin SJ, Kim JY,
Yu JH and Gong G: Tertiary lymphoid structures: Prognostic
significance and relationship with tumour-infiltrating lymphocytes
in triple-negative breast cancer. J Clin Pathol. 69:422–430. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Carney JA: Gastric mucosal lymphoid
follicles: Histology, distribution, frequency, and etiologic
features. Am J Surg Pathol. 34:1019–1024. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Dieu-Nosjean MC, Giraldo NA, Kaplon H,
Germain C, Fridman WH and Sautes-Fridman C: Tertiary lymphoid
structures, drivers of the anti-tumor responses in human cancers.
Immunol Rev. 271:260–275. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Geng Y, Shao Y, He W, Hu W, Xu Y, Chen J,
Wu C and Jiang J: Prognostic role of tumor-infiltrating lymphocytes
in lung cancer: A meta-analysis. Cell Physiol Biochem.
37:1560–1571. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Li J, Chen L, Xiong Y, Zheng X, Xie Q,
Zhou Q, Shi L, Wu C, Jiang J and Wang H: Knockdown of PD-L1 in
human gastric cancer cells inhibits tumor progression and improves
the cytotoxic sensitivity to CIK therapy. Cell Physiol Biochem.
41:907–920. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Zou W and Chen L: Inhibitory B7-family
molecules in the tumour microenvironment. Nat Rev Immunol.
8:467–477. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Lee HJ, Kim JY, Park IA, Song IH, Yu JH,
Ahn JH and Gong G: Prognostic significance of tumor-infiltrating
lymphocytes and the tertiary lymphoid structures in HER2-positive
breast cancer treated with adjuvant trastuzumab. Am J Clin Pathol.
144:278–288. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Gu-Trantien C, Migliori E, Buisseret L, de
Wind A, Brohée S, Garaud S, Noël G, Dang Chi VL, Lodewyckx JN,
Naveaux C, et al: CXCL13-producing TFH cells link immune
suppression and adaptive memory in human breast cancer. JCI
Insight. 2:e914872017. View Article : Google Scholar
|
|
37
|
Schweiger T, Berghoff AS, Glogner C,
Glueck O, Rajky O, Traxler D, Birner P, Preusser M, Klepetko W and
Hoetzenecker K: Tumor-infiltrating lymphocyte subsets and tertiary
lymphoid structures in pulmonary metastases from colorectal cancer.
Clin Exp Metastasis. 33:727–739. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Im SJ, Hashimoto M, Gerner MY, Lee J,
Kissick HT, Burger MC, Shan Q, Hale JS, Lee J, Nasti TH, et al:
Defining CD8+ T cells that provide the proliferative burst after
PD-1 therapy. Nature. 537:417–421. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Hornquist E, Grdic D, Mak T and Lycke N:
CD8-deficient mice exhibit augmented mucosal immune responses and
intact adjuvant effects to cholera toxin. Immunology. 87:220–229.
1996. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Shalapour S, Font-Burgada J, Di Caro G,
Zhong Z, Sanchez-Lopez E, Dhar D, Willimsky G, Ammirante M,
Strasner A, Hansel DE, et al: Immunosuppressive plasma cells impede
T-cell-dependent immunogenic chemotherapy. Nature. 521:94–98. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Shalapour S, Lin XJ, Bastian IN, Brain J,
Burt AD, Aksenov AA, Vrbanac AF, Li W, Perkins A, Matsutani T, et
al: Inflammation-induced IgA+ cells dismantle anti-liver cancer
immunity. Nature. 551:340–345. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Lampropoulou V, Hoehlig K, Roch T, Neves
P, Calderón Gómez E, Sweenie CH, Hao Y, Freitas AA, Steinhoff U,
Anderton SM and Fillatreau S: TLR-activated B cells suppress T
cell-mediated autoimmunity. J Immunol. 180:4763–4773. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Ayala VI, Deleage C, Trivett MT, Jain S,
Coren LV, Breed MW, Kramer JA, Thomas JA, Estes JD, Lifson JD and
Ott DE: CXCR5-dependent entry of CD8 T cells into rhesus macaque
B-Cell follicles achieved through T-cell engineering. J Virol.
91:2017. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Li S, Folkvord JM, Rakasz EG, Abdelaal HM,
Wagstaff RK, Kovacs KJ, Kim HO, Sawahata R, MaWhinney S, Masopust
D, et al: Simian immunodeficiency virus-producing cells in
follicles are partially suppressed by CD8+ cells in vivo. J Virol.
90:11168–11180. 2016. View Article : Google Scholar : PubMed/NCBI
|