Introduction
Invasive micropapillary carcinoma (IMPC) is a type
of mammary epithelial tumor that was added in the 2003 World Health
Organization (WHO) classification (1). IMPC was first described by Siriaunkgul
and Tavassoli and was reported to account for 0.7–3% of all breast
cancer cases (2). The pathological
morphology of IMPC is unique, and immunohistochemistry has
demonstrated that the positive portion of the epithelial membrane
antigen is located on the outside of the pseudopapillary neoplasm
or glandular tube (3). Most cases of
IMPC appear mixed with other pathological types of invasive breast
carcinoma, most commonly with invasive ductal carcinoma (4).
Lymphatic invasion and lymph node metastasis are
common in IMPC, with an incidence of nodal metastases of 24.9%,
leading to frequent recurrence and poor prognosis in patients, with
a 5-year overall survival rate of 87.5% (5). Even when the proportion of
micropapillary structures is <10%, the invasive ability of the
cancer is significantly higher compared with that of the same
pathological type of breast cancer without IMPC components
(6,7). Diagnosis of this cancer type before
surgery is of great value for determining the optimal treatment
strategy (6), including the choice
of surgical methods and the follow-up treatment plan to improve the
prognosis of patients.
To date, the majority of studies have focused on the
pathological features and ultrasonographic findings of IMPC
(8,9). In previous reports, most IMPCs
presented as an irregular mass with a high density and a
non-circumscribed margin on the mammography, and as an irregular
spiculated mass on magnetic resonance imaging (MRI) (10–16).
These are typical features of malignant breast cancers (17); however, they are of limited
significance for the diagnosis of IMPC. In addition, only several
MRI features were investigated in each study, and thus, the results
did not provide enough information for clinical use (10–14).
Therefore, the present retrospective study was performed to
characterize the MRI and pathological features of IMPC for
comprehensive preoperative assessment of IMPC cases.
Patients and methods
Ethics approval
The present study was approved by the Ethics
Committee of Sir Run Run Shaw Hospital, Zhejiang University School
of Medicine (Hangzhou, China). All procedures involving human
participants were performed in accordance with the ethical
standards of the Institutional and/or National Research Committee,
the 1964 Helsinki Declaration and its later amendments or
comparable ethical standards. Informed consent was waived due to
the retrospective nature of the study.
Patients
A total of nine cases of IMPC, confirmed
pathologically after surgical resection or ultrasound-guided
core-needle breast biopsy at Sir Run Run Shaw Hospital, Zhejiang
University School of Medicine between August 2011 and January 2018,
were included in the present study. A total of six patients
underwent both MRI and mammography, two patients underwent MRI only
and one patient underwent mammography only. None of the patients
had received radiotherapy or undergone biopsy before MRI
examination, and complete immunohistochemical data were available
for all lesions.
Imaging
Preoperative mammography was performed in seven
cases using a GE Senographe DS digital mammography machine (GE
Healthcare) in the routine craniocaudal and mediolateral oblique
position.
Preoperative MRI was performed in eight cases with a
GE Signa HD Excite 1.5T/HD or 3.0T superconducting MRI scanner (GE
Healthcare), with an 8-channel breast phased array surface coil.
Patients were in a prone position, and bilateral breasts were
hanging naturally in the coil. The plain cross-sectional T2WI fat
suppression sequence and fast spin-echo T2WI sequence were scanned
at a layer thickness of 4.0 mm with a layer spacing of 1.0 mm. The
sagittal T2WI fat suppression sequence was scanned at a layer
thickness of 4.0/5.0 mm with a layer spacing of 1.0 mm, a matrix of
512×512 and number of excitations (NEX)2. Diffusion-weighted
imaging was performed using single-shot plane echo-planar imaging
technology with a matrix of 256×256, layer thickness of 4.0 mm,
layer spacing of 1.0 mm, NEX6 and diffusion sensitivity coefficient
b values of 0 and 800 sec/mm2.
Dynamic enhanced scanning was performed using
breast-optimized parallel acquisition of 3D fast gradient echo
sequences (volume imaging for breast assessment). The dynamic
enhancement was performed before the masking, and 0.2 mmol/kg of
the contrast agent Gd-DTPA was injected via a high-pressure syringe
through the elbow vein at a rate of 3.0 ml/sec, followed by the
injection of 15–20 ml saline. Scanning was performed immediately. A
total of seven phases were continuously collected, and the scanning
time per phase was 60 sec. Imaging was performed with a reverse
angle of 15°, a matrix of 512×512, and NEX2. All patients' dynamic
enhanced scans were post-processed on the GE AW4.5 workstation
using Functool software (both from GE Healthcare). On each scan,
the region of interest (ROI) was selected in the most obvious area
of lesion enhancement, avoiding the necrotic cystic region, and the
TIC was plotted.
Pathological examination
All IMPC tissue specimens were fixed in 10% neutral
formalin for 12 h at room temperature, embedded in paraffin and
serially sectioned with a layer thickness of 4 µm. Subsequently,
they were stained with hematoxylin for 5 min and eosin for 3 min at
room temperature. Immunohistochemical staining was performed using
the EnVision (cat. no. K5007; Dako; Agilent Technologies, Inc.)
method. Briefly, 4% goat serum (OriGene Technologies, Inc.) was
added dropwise for blocking at room temperature for 30 min.
Subsequently, different primary antibodies, namely anti-estrogen
receptor (ready to use; cat. no. 790-4325; Roche Diagnostics),
anti-progesterone receptor (ready to use; cat. no. 790-4296; Roche
Diagnostics), anti-human epidemic growth factor receptor 2 (ready
to use; cat. no. 790-4493; Roche Diagnostics) and anti-Ki67 (1:800;
cat. no. M7240; Dako; Agilent Technologies, Inc.), were added and
incubated at room temperature for 2 h. After washing with PBS, one
drop of EnVision secondary antibody (ready to use; cat. no. K5007;
Dako; Agilent Technologies, Inc.) bound to horseradish peroxidase
was added at 37°C for 30 min. All stained sections were observed
under a light microscope (magnifications ×40 and ×100).
Image analysis
All mammography and MRI scans were reviewed by two
physicians with >5 years of experience in breast lesion
diagnosis, who were blinded to the pathological results. All signs
were described in accordance with the 2013 version of the Breast
Imaging Reporting and Data System (BI-RADS) proposed by the
American College of Radiology (18).
The features of mammography included lesion type (only mass, mass
with suspected malignant calcification, only suspected malignant
calcification, focal asymmetry or structural distortion) and mass
characteristics (shape and edge). MRI analysis included
determination of the lesion size, plain scanning signal intensity
(low, equal and high signal compared with that in normal glands),
enhanced lesion morphology, edge morphology, internal enhancement
mode, early enhancement rate and the TIC. Lesion size was evaluated
using the maximum diameter as the reference index. If multiple
lesions were present, the diameter of the largest lesion was
measured.
TICs were generated by the post-processing
workstation. According to the 2013 BI-RADS, the enhancement rate
was based on the first phase enhancement rate as follows:
(SIpost-SIpre)/SIpre ×100%, where
SIpost is the intensity of the first phase signal after
lesion enhancement, and SIpre is the signal intensity
before enhanced scanning. The enhancement rate was classified into
three modes: Slow (<50%), medium (50-100%) and fast (>100%).
The delay period was recorded after the appearance of the peak,
with the progressive type recorded as type I, the platform type
recorded as type II and the outflow type recorded as type III. For
lesions with complicated or non-tumor enhancement, numerous points
were repeatedly evaluated, and multiple TICs were considered
together.
The ADC map was automatically generated by the
workstation and used to artificially measure the ADC value. A
visibly solid part of the lesion was selected, and the ROI was
manually selected according to the size of the lesion. The ROI was
usually drawn slightly smaller than the lesion range, avoiding the
cystic change and hemorrhagic or necrotic areas. ROIs were measured
3–5 times for the calculation of the mean value.
All pathological sections were reviewed by two
pathologists with 5 years of experience in the diagnosis of breast
diseases, and agreement was achieved through discussion when the
diagnoses were inconsistent. According to the 4th edition of the
WHO classification of breast tumors published in 2012 (19), IMPC was identified by clusters of
cells in a pseudo-papillary structure without a fibrous vascular
axis that were surrounded by interstitial spaces. In addition, the
examination included the presence of associated ductal carcinoma
in situ (DCIS), lymphatic vessel infiltration, axillary
lymph node status, proliferation index (Ki-67), and the expression
of estrogen receptor (ER), progesterone receptor (PR) and human
epidermal growth factor receptor 2 (HER2). Molecular subtype was
determined based on ER, PR, HER2 and Ki-67 expression and
categorized as follows: Luminal A was ER+ and/or
PR+, HER2− and Ki-67−; luminal B
was ER+ and/or PR+, HER2− and
Ki-67+; luminal-HER2-positive was ER+ and/or
PR+ and HER2+; HER2-rich was ER−,
PR− and HER2+; and triple negative was
ER−, PR− and HER2−.
Results
Clinical characteristics
All nine patients were female with an average age of
52.11 years (range, 40–65 years). Among them, seven patients were
postmenopausal. The initial manifestations were a palpable breast
mass in 8 (89%) patients and a gradually enlarged breast mass in
two patients. Three patients reported mild tenderness of the mass,
and two patients reported ipsilateral breast pain. Eight (80%)
lesions were located in the left breast. The mean lesion diameter
was 34.44±25.68 mm, and the range between the minimum and maximum
diameter was 13.2–85.4 mm, with a median value of 18.3 mm. The
patient clinical characteristics are shown in Table I.
 | Table I.Clinical characteristics of the
patients. |
Table I.
Clinical characteristics of the
patients.
| Patient no. | Age, years | Menopause | Symptoms and
physical examination findings | Stage and molecular
type |
|---|
| 1 | 52 | + | A mass in the right
upper quadrant of the breast was occasionally noticed, starting 302
days previously. | pT1N0M0/luminal
B |
|
|
|
| PE: Mass in the
right breast at 10 o'clock and 2.5 cm from the nipple, 1.8×1.5 cm,
hard, with uneven surface, unclear edge, and dimple sign (+). |
|
| 2 | 50 | + | A mass was detected
by mammography 33 days previously. PE: Mass in the upper left
quadrant of the left breast, 1.5 cm in diameter, hard, with unclear
edge. | pT1N1M0/luminal
B |
| 3 | 65 | + | Two years
previously, a mass was inadvertently discovered by touch, which
gradually increased in size. The patient reported pain in the left
breast, discomfort and itchy skin on the surface, with local
ulceration 1 month previously. PE: Mass in the left breast at 3
o'clock, 4×3 cm, hard, with unclear boundary and unmovable. | ypT2N2M0/luminal
A |
| 4 | 50 | + | A mass in the left
breast was discovered by self-examination, with slight tenderness
to touch. PE: Mass of medium texture in the left breast at 12
o'clock, 3 cm away from the areola, 1.5×1.5 cm, with unclear edge
and dimple sign (+). | pT1N1M0/luminal
B |
| 5 | 51 | + | A mass was
occasionally felt, starting 35 days previously. PE: Mass in the
upper outer quadrant of the left breast at 1–3 o'clock, 7×5 cm,
hard, with unclear boundary and unmovable. |
ypT4N2M0/luminal-HER2 |
| 6 | 60 | + | One lesion was
discovered by self-examination that was painful, but tolerable and
without periodicity. PE: Two masses in the left breast at 3
o'clock, 2 and 3 cm away from the areola, respectively, 2×1.5 and
1×1 cm, respectively, moderate, with unclear boundary and
movable. | pT1N1M0/luminal
A |
| 7 | 48 | – | One lesion was
discovered by self-examination 123 days previously, with
tenderness, which became larger in the past 0.5 month. PE: Mass in
the right breast at 2 o'clock, 4 cm outside the areola, 2×2 cm,
hard, clear, with smooth surface and not easy to push. | pT1N0M0/luminal
A |
| 8 | 40 | – | A left axillary
mass was discovered by self-examination due to discomfort at the
left axillary, starting 14 days previously. PE: Left axillary
discomfort, mass in the left breast at 1–2 o'clock, 1×1 cm, hard,
with unclear boundary, general activity, and a second left axillary
mass, 2×1 cm, hard, with general activity. | pT1N3M0/luminal
B |
| 9 | 53 | + | A mass was
inadvertently felt by palpation in the left breast with local
tenderness 32 days previously. |
pT1N1M0/luminal-HER2 |
|
|
|
| PE: Local
tenderness of a mass in the left breast at 6 o'clock, 1.5×1 cm,
hard, with unclear boundary, poor activity and suspicious dimple
sign. |
|
Pathological manifestations
Regarding the pathological manifestations of the
nine cases, there were three cases accompanied by DCIS, seven cases
with lymph node metastasis (including one case of lymph node
metastasis in the supraclavicular region), three cases with
lymphatic invasion, one case with vascular tumor thrombus, two
cases with invasion of the nipple and one case with invasion of the
pectoralis major. According to the immunohistochemical staining
analysis, three cases were luminal A (ER+ and
PR+), four cases were luminal B (four cases were
ER+ and three cases were PR+), and two cases
were luminal-HER2-positive (ER+, PR+,
HER2+ and Ki-67+) (Table I).
Imaging
Mammography features
A total of seven patients underwent mammography
before surgery, and internal mammary gland lesions were identified
in six patients. A total of five cases exhibited high-density
masses with an oval or irregular shape and blurring or spiculation
and partially visible lobes. Among them, two cases had small dense
or polymorphic suspicious malignant calcifications with segmental
distribution, including one case with calcification around the
mass; two cases exhibited local skin thickening or invagination;
and one case had multiple enlarged axillary lymph nodes with
disappearance of the hilum of the lymph nodes. One case presented
with structural asymmetry, small pleomorphic calcification with
regional distribution, localized skin thickening, nipple
retraction, multiple lymph nodes with axillary fossa and
disappearance of the hilum. No abnormalities were observed in the
mammary gland of one patient; instead, only enlarged axillary lymph
nodes were detected (Table II).
| Table II.Mammography, MRI and pathological
characteristics of 9 cases of IMPC. |
Table II.
Mammography, MRI and pathological
characteristics of 9 cases of IMPC.
|
|
|
|
| Pathology |
|---|
|
|
|
|
|
|
|---|
| Patient no. | Diameter, mm | Mammography | ADC of MRI,
×10−3 mm2/sec | LVI | LNM | IC components |
Immunohistochemistry |
|---|
| 1 | 13.2 | High density,
irregular shape, burr edge | 0.681 | – | – | – | ER+,
PR−, Her-2−, Ki-67 (30%) |
| 2 | 19.2 | N/A | 0.882 | – | + | – | ER+,
PR+, Her-21+, Ki-67 (30%) |
| 3 | 64.2 (largest of 3
lesions) | High density,
lobulated, unclear edge, thickened adjacent skin, depression | 0.613 | + | + | – | ER+,
PR+, Her-22+, Ki-67 (10%), no HER2
amplification FISH |
| 4 | 15 | High density,
irregular shape, blurry edges | 0.849 | – | + | + | ER+,
PR+, Her-2−, Ki-67 (15%) |
| 5 | 85.4 | Large pieces of
asymmetrical and dense lesions, with regional distribution of fine
pleomorphic calcification, thickened local skin, nipple
retraction | 0.989 | + | + | – | ER+,
PR+, Her-22+, Ki-67 (70-80%), HER2
amplification on FISH |
| 6 | 44.9 | High density,
irregular shape, burr edge, visible fine calcification of the
segmental distribution | 0.838 | – | + | + | ER+,
PR+, Her-2−, Ki-67 (10%) |
| 7 | 16.2 | N/A | 0.778 | – | – | + | ER+,
PR+, Her-2−, Ki-67 (10%) |
| 8 | 17.4 | Under the left
armpit, increased density, unclear edges, several lymph nodes
displayed around | 0.955 | + | + | – | ER+,
PR+, Her-22+, Ki-67 (20%), no HER2
amplification on FISH |
| 9 | 27.7 | High density,
irregular shape, unclear edge, small pleomorphic calcification
around the segment, thickening near the local areola skin | N/A | – | + | – | ER+,
PR+, Her-23+, Ki-67 (20%) |
MRI
On plain T2WI, seven cases had slightly high
heterogeneous signal and one had a high signal. With a b value of
800 sec/mm2, the average, maximum, minimum and median
ADC values were 0.823±0.12×10−3, 0.989×10−3,
0.613×10−3 and 0.844×10−3 mm2/sec,
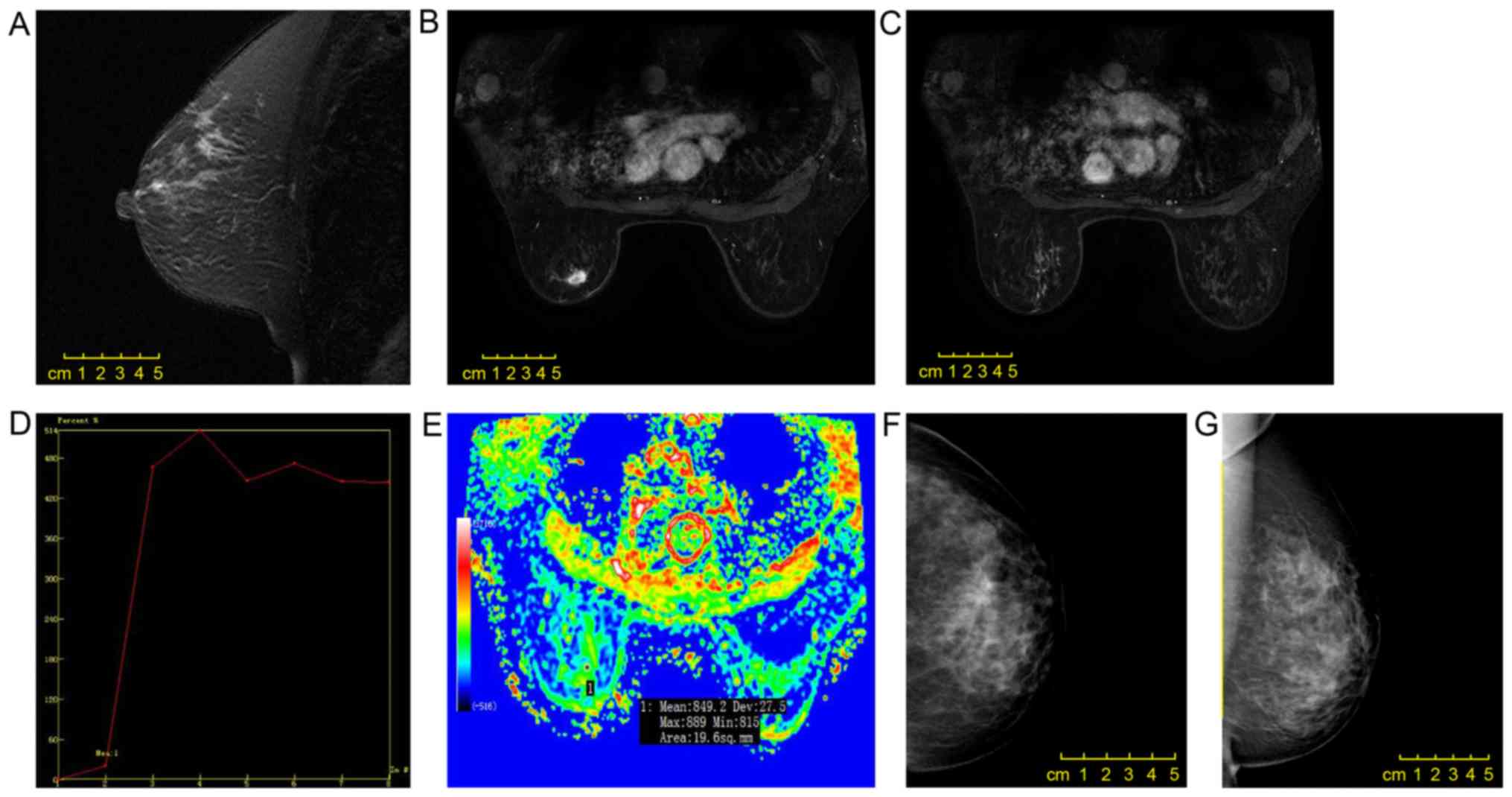
respectively. In the enhanced scanning, four cases exhibited
mass-like enhancement, including one case (three lesions) with
oval-shaped ring enhancement, one case with irregular shape
heterogeneity enhancement and one case with irregular shape uniform
enhancement. The margins were clear in one case (three lesions),
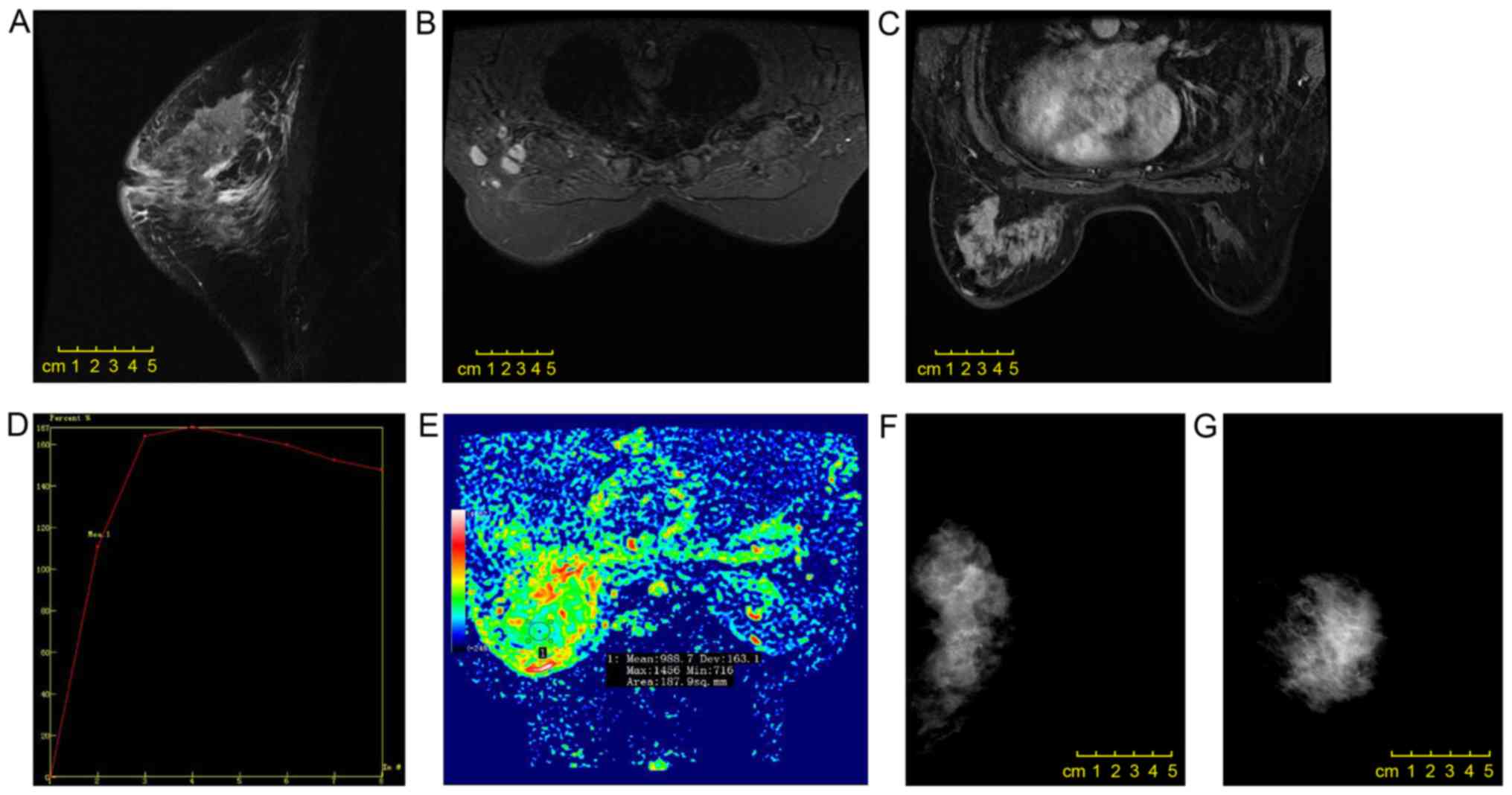
irregular in two cases and spiculated in one case (Fig. 1). A total of four cases exhibited
non-mass enhancement, including two cases with a focal
distribution, one case with linear distribution and one case with
regional distribution. Regarding the internal enhancement, these
four cases included one case with clustering, one case with
heterogeneity and two cases with uniformity (Fig. 2). The average, maximum, minimum and
median early enhancement rates were 116.96±45.26, 190.1, 20.3 and
126.1%, respectively. TICs were of type III in all cases. IMPC was
accompanied by skin edema thickening in one case, local skin
depression in one case and nipple depression in one case. Axillary
lymphadenopathy with enhancement was observed in three cases. The
sensitivity, specificity, positive predictive value, negative
predictive value and overall accuracy of MRI for axillary lymph
node metastasis diagnosis were 50, 100, 100, 40 and 62.5%,
respectively (Table III).
| Table III.MRI characteristics of pure breast
IMPC. |
Table III.
MRI characteristics of pure breast
IMPC.
| Features | n (%) |
|---|
| Mass-like
enhancement | 4 |
|
Shape |
|
|
Oval | 1 (25) |
|
Irregular
shape | 3 (75) |
|
Edge |
|
|
Clear | 1 (25) |
|
Irregular | 2 (50) |
|
Burr | 1 (25) |
|
Internal enhancement
feature |
|
|
Uniform | 1 (25) |
|
Inhomogeneous | 2 (50) |
|
Edge
enhancement | 1 (25) |
| Non-mass
enhancement | 4 |
|
Distribution |
|
|
Linear | 1 (25) |
|
Focal | 2 (50) |
|
Regional | 1 (25) |
|
Internal enhancement
feature |
|
|
Uniform | 2 (50) |
|
Inhomogeneous | 1 (25) |
|
Cluster-like | 1 (25) |
| TIC | 8 |
| Early
stage |
|
|
Slow | 1 (12.5) |
|
Medium | 1 (12.5) |
|
Fast | 6 (75) |
| Delay
stage |
|
|
Outflow type | 8 (100) |
| Axillary lymph node
metastasis | 6 |
| (+) on
MRI | 3 (50) |
| (−) on
MRI | 3 (50) |
| Metastatic lymph
nodes detected by MRI | 8 |
| Sensitivity | 50% |
| Specificity | 100% |
| Positive predictive
value | 100% |
| Negative predictive
value | 40% |
| Overall
accuracy | 62.5% |
| Invasion of the
nipple, chest wall or skin | 2 (25) |
Discussion
IMPC is a highly invasive type of breast cancer
(20). The incidence of IMPC is very
low accounting for 0.76–3.8% of breast carcinomas (21–23);
however, the degree of malignancy is high. In the present study,
the clinical manifestations, pathological changes and imaging
results in cases of IMPC were investigated, including mammography
and MRI findings. The most common clinical manifestations were
palpable masses that were presented in 89% (8/9) of the cases
studied, and this percentage was slightly lower than compared with
the 94% reported by Günhan-Bilgen et al (17). Among the observed lesions, the site
with the most frequent IMPC occurrence was the left breast (80%,
8/10), which was consistent with the finding of 60.5% of lesions
(23/38) in the left breast reported by Kim et al (24). In most cases, axillary lymph node
metastasis was present at the time of diagnosis, and axillary
lymphadenopathy was noticed before the primary tumor was identified
in one case of the present study.
The mammography results of all patients in the
present study suggested malignant tumors, and the characteristics
were mostly consistent with those observed in the literature
(17,25–28),
including a mass (54.2–74.4%), irregular high density and
microcalcification (38.5–66.7%). In the study by Lim et al
(13), microcalcification was
observed around the edge of the mass. As reported be Adrada et
al (10) and Alsharif et
al (12), the common
morphological features of microcalcification were polymorphism
(57%, 11/19) and polymorphism or fine branch morphology (86.7%,
13/15). Microcalcification is the most common mammographic feature
of DCIS (29), and these imaging
features are highly suggestive of malignant tumors.
Previous studies have reported that IMPC exhibits an
irregular mass with an irregular or spiculated edge on MRI
(10,13). The enhanced scanning curve is
outflow-type and the internal enhancement mode is very different,
with 16.7–38.9% probability of surrounding non-mass-enhanced
lesions (10–14). Secondly, 22–39% of cases presented
with non-mass enhancement in these studies (10–14).
Kubota et al (15) compared
the MRI features of eight IMPC lesions and 22 invasive ductal
carcinomas and demonstrated that IMPC was more likely to exhibit a
characteristic irregular mass. In the present study, 50% of IMPC
cases exhibited mass-like enhancement, and the other 50% exhibited
non-mass enhancement. The incidence of non-mass enhancement was
higher compared with that reported in the literature, which was
possibly due to the increase of the pathological micro-nipple
component. This needs to be confirmed by analysis of more cases.
Among the four cases of mass-like enhanced lesions and the four
cases of non-mass enhanced lesions, one case in each set had
non-mass enhancement of segmental distribution, which was
pathologically confirmed to be accompanied by DCIS. In the four
lesions with non-mass enhancement, two cases had a focal
distribution, one case had a linear distribution and one case had a
regional distribution, which differed from previous reports. Yun
et al (11) reported seven
cases with segmental distribution, and Jones et al (14) reported that most lesions with
non-mass enhancement had a diffuse distribution. The internal
enhancement patterns in the present study also differed, and TICs
were of type III in all cases, which was consistent with a previous
study (14). In addition, the ADC
with a b value of 800 sec/mm2 was determined, and a mean
ADC value of 0.823±0.12×10−3 mm2/sec was
observed, which indicated malignant tumors (16). The enhancement rate in the first
phase was mostly the rapid enhancement mode (75%, 6/8) according to
the 2013 version of the BI-RADS (19), and the average was 116.96±45.26%.
Although the standard deviation for the mean enhancement rate was
large, the early rapid enhancement mode also suggested the
differentiation of malignant tumors. MRI demonstrated higher
sensitivity for lesion detection compared with that of mammography,
especially for the detection of lesions with non-mass enhancement
and for precise definition of the lesion (13,14).
Kubota et al (15) concluded
that radiography, including MRI, can be carefully interpreted to
determine the boundary of the lesion, and additional resection can
be performed at the positive edge (cells close to the edge of the
previously resected specimen).
Previous studies have reported that IMPC is often
associated with DCIS, with an incidence as high as 78.6% (10,13,25).
Among the patients in the present study, only three cases (33%) had
IMPC mixed with DCIS, and the incidence was lower than previously
reported. The rate of axillary lymph node metastasis in IMPC has
been reported to range between 56 and 90.5% (12–14,26,27), and
lymphatic vascular invasion has been demonstrated to be an
independent factor for poor prognosis and a marker of lymph node
metastasis (4,24). Zekioglu et al (4) observed lymphatic invasion in 75% of
cases of IMPC, of which 82% exhibited lymph node metastasis. In the
present study, lymphatic invasion was identified in three cases
(33.3%, 3/9), whereas axillary lymph node metastasis was observed
in seven cases (77.8%, 7/9). The longest lesion diameter in a case
with lymphatic infiltration and simultaneous intravascular tumor
thrombus lesions was 17.4 mm, and the initial clinical
manifestation was palpable axillary lymphadenopathy, indicating
that the size of IMPC was not directly related to tumor invasion
and histological characteristics, including histological grade;
thus, lymphatic vessel density and lymphocytic infiltration of IMPC
may be more relevant than lesion size (28). MRI revealed that three cases (37.5%,
3/8) had axillary lymph node metastasis. The sensitivity,
specificity, positive predictive value, negative predictive value
and overall accuracy of MRI for axillary lymph node metastasis
diagnosis were 50, 100, 100, 40 and 62.5%, respectively. These
results suggested that the possibility of axillary lymph node
metastasis in patients with IMPC was high regardless of the MRI
findings, and pathological examination of lymphatic vessels and
regional lymph nodes was needed.
The molecular phenotype of lesions in the present
study was mainly luminal type (78%, 7/9), and no cases were triple
negative, which was similar to the findings presented in previous
reports (4,11). Positivity for hormone receptors is
usually observed in better differentiated tumors, and the prognosis
is better in these cases. This seems to contrast with the high
rates of biological invasion and recurrence and poor prognosis in
IMPC. It is speculated that IMPC has unique histological features.
In the present study, 2 cases (22%, 2/9) were luminal-HER2
positive, and this frequency of HER2-positive cases was lower than
those previously reported (4,10,11).
Previous studies have confirmed that HER2 gene amplification and/or
upregulation of HER2 protein expression is associated with poor
prognosis in patients with invasive breast cancer (26,30). In
the present study, one patient with the luminal-HER2-positive type
presented with metastasis to the ipsilateral chest wall 2 years
after treatment with chemoradiotherapy, modified radical mastectomy
and endocrine therapy. After changing the chemotherapy regimen,
multiple liver, lung and contralateral breast cancer metastases
were observed. Retrospective analysis of the molecular phenotype in
this case, in addition to HER22+ and HER2 gene
amplification by fluorescence in situ hybridization and
Ki-67 index measurement (~70-80%, indicating a high cell
proliferation index), indicated accelerated tumor metastasis. In
the present study, the negative predictive value of MRI for
axillary lymph node metastasis was only 40%, indicating that
regardless of the clinical and imaging findings for lymph nodes,
patients with IMPC should undergo biopsy of the axillary lymph
nodes.
Complete surgical resection of the lesion is an
important therapy in IMPC (5).
However, IMPC is typically irregular in shape on MRI and the border
is unclear (8,10). Thus, the possibility of residual
cancer cells remaining in the breast after breast-conserving
surgery is high. If a rapid pathological analysis performed during
surgery reveals the presence of cancer cells at the margin of the
resected specimen, re-expansion of the resection is required, and a
prolonged operative time and re-expanded resection increase the
probability of postoperative complications.
The present study had several limitations. First,
the sample size was small, and more cases are needed. Second, the
study was a retrospective analysis, and not all patients underwent
both mammography and MRI examinations. Third, pathology was not
classified according to the WHO guidelines. A multicenter study is
the next step to expand the sample size and compare the MRI
features, pathological grades and molecular phenotypes to identify
effective imaging features for preoperative evaluation and
prognosis prediction.
In conclusion, the MRI features of IMPC included
typical malignant tumor characteristics with ready invasion of
lymphatic vessels. Among the IMPC cases presented, frequent nodal
metastases and high likelihood of luminal type lesions were
observed. These characteristics provide valuable insight for the
diagnosis of IMPC.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
CHH and HJH designed/performed the majority of the
experiments and data analysis, and wrote the manuscript. ZBG
provided pathological assistance. WGY and JH contributed to the
analysis and the interpretation of the data. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Sir Run Run Shaw Hospital, Zhejiang University School of Medicine
(Hangzhou, China). All procedures involving human participants were
performed in accordance with the ethical standards of the
Institutional and/or National Research Committee, the 1964 Helsinki
Declaration and its later amendments. All data published here are
under the consent for publication.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
IMPC
|
invasive micropapillary carcinoma
|
|
WHO
|
World Health Organization
|
|
MRI
|
magnetic resonance imaging
|
|
ROI
|
region of interest
|
|
ADC
|
apparent diffusion coefficient
|
|
TIC
|
time-intensity curve
|
|
BI-RADS
|
Breast Imaging Reporting and Data
System
|
|
DCIS
|
ductal carcinoma in situ
|
|
ER
|
estrogen receptor
|
|
PR
|
progesterone receptor
|
|
HER2
|
human epidermal growth factor receptor
2
|
References
|
1
|
Tavassoli FA and Devilee P: Pathology and
genetics of tumors of the breast and female genital organs. World
Health Organization classification of tumors. IARC Press. 2003.
|
|
2
|
Siriaunkgul S and Tavassoli FA: Invasive
micropapillary carcinoma of the breast. Mod Pathol. 6:660–662.
1993.PubMed/NCBI
|
|
3
|
Luna-More S, Gonzalez B, Acedo C, Rodrigo
I and Luna C: Invasive micropapillary carcinoma of the breast. A
new special type of invasive mammary carcinoma. Pathol Res Pract.
190:668–674. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zekioglu O, Erhan Y, Ciris M, Bayramoglu H
and Ozdemir N: Invasive micropapillary carcinoma of the breast:
High incidence of lymph node metastasis with extranodal extension
and its immunohistochemical profile compared with invasive ductal
carcinoma. Histopathology. 44:18–23. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lewis GD, Xing Y, Haque W, Patel T,
Schwartz M, Chen A, Farach A, Hatch S, Butler EB, Chang J and Teh
BS: Prognosis of lymphotropic invasive micropapillary breast
carcinoma analyzed by using data from the national cancer database.
Cancer Commun (Lond). 39:602019. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Li W, Han Y, Wang C, Guo X, Shen B, Liu F,
Jiang C, Li Y, Yang Y, Lang R, et al: Precise pathologic diagnosis
and individualized treatment improve the outcomes of invasive
micropapillary carcinoma of the breast: A 12-year prospective
clinical study. Mod Pathol. 31:956–964. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kaya C, Uçak R, Bozkurt E, Ömeroğlu S,
Kartal K, Yazıcı P, Idiz UO and Mihmanli M: The impact of
micropapillary component ratio on the prognosis of patients with
invasive micropapillary breast carcinoma. J Invest Surg. 1–9.
2018.
|
|
8
|
Kamitani K, Kamitani T, Ono M, Toyoshima S
and Mitsuyama S: Ultrasonographic findings of invasive
micropapillary carcinoma of the breast: Correlation between
internal echogenicity and histological findings. Breast Cancer.
19:349–352. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Mizushima Y, Yamaguchi R, Yokoyama T, Ogo
E and Nakashima O: Recurrence of invasive micropapillary carcinoma
of the breast with different ultrasound features according to
lesion site: Case report. Kurume Med J. 58:81–85. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Adrada B, Arribas E, Gilcrease M and Yang
WT: Invasive micropapillary carcinoma of the breast: Mammographic,
sonographic, and MRI features. AJR Am J Roentgenol. 193:W58–W63.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Yun SU, Choi BB, Shu KS, Kim SM, Seo YD,
Lee JS and Chang ES: Imaging findings of invasive micropapillary
carcinoma of the breast. J Breast Cancer. 15:57–64. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Alsharif S, Daghistani R, Kamberoğlu EA,
Omeroglu A, Meterissian S and Mesurolle B: Mammographic,
sonographic and MR imaging features of invasive micropapillary
breast cancer. Eur J Radiol. 83:1375–1380. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lim HS, Kuzmiak CM, Jeong SI, Choi YR, Kim
JW, Lee JS and Park MH: Invasive micropapillary carcinoma of the
breast: MR imaging findings. Korean J Radiol. 14:551–558. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Jones KN, Guimaraes LS, Reynolds CA, Ghosh
K, Degnim AC and Glazebrook KN: Invasive micropapillary carcinoma
of the breast: Imaging features with clinical and pathologic
correlation. AJR Am J Roentgenol. 200:689–695. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kubota K, Ogawa Y, Nishioka A, Murata Y,
Itoh S, Hamada N, Morio K, Maeda H and Tanaka Y: Radiological
imaging features of invasive micropapillary carcinoma of the breast
and axillary lymph nodes. Oncol Rep. 20:1143–1147. 2008.PubMed/NCBI
|
|
16
|
Peng YX, Cai HM and CY C: Vulation the
differential value of diffusion-weighted imaging and dynamic
contrast-enhanced magnetic resonance in breast lesions. Chinese
Journal. 11:1–4. 2014.
|
|
17
|
Günhan-Bilgen I, Zekioglu O, Ustün EE,
Memis A and Erhan Y: Invasive micropapillary carcinoma of the
breast: Clinical, mammographic, and sonographic findings with
histopathologic correlation. AJR Am J Roentgenol. 179:927–931.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Allarakha A, Gao Y, Jiang H and Wang PJ:
Prediction and prognosis of biologically aggressive breast cancers
by the combination of DWI/DCE-MRI and immunohistochemical tumor
markers. Discov Med. 27:7–15. 2019.PubMed/NCBI
|
|
19
|
American College of Radiology, Breast
Imaging Reporting and Data System (BI-RADS). (4th). American
College of Radiology. (Reston). 563–570. 2013.
|
|
20
|
Onder S, Fayda M, Karanlık H, Bayram A,
Şen F, Cabioglu N, Tuzlalı S, İlhan R and Yavuz E: Loss of ARID1A
expression is associated with poor prognosis in invasive
micropapillary carcinomas of the breast: A clinicopathologic and
immunohistochemical study with long-term survival analysis. Breast
J. 23:638–646. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Shi WB, Yang LJ, Hu X, Zhou J, Zhang Q and
Shao ZM: Clinico-pathological features and prognosis of invasive
micropapillary carcinoma compared to invasive ductal carcinoma: A
population-based study from China. PLoS One. 9:e1013902014.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Gokce H, Durak MG, Akin MM, Canda Y, Balci
P, Ellidokuz H, Demirkan B, Gorken IB, Sevinc AI, Kocdor MA, et al:
Invasive micropapillary carcinoma of the breast: A
clinicopathologic study of 103 cases of an unusual and highly
aggressive variant of breast carcinoma. Breast J. 19:374–381. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Hashmi AA, Aijaz S, Mahboob R, Khan SM,
Irfan M, Iftikhar N, Nisar M, Siddiqui M, Edhi MM, Faridi N and
Khan A: Clinicopathologic features of invasive metaplastic and
micropapillary breast carcinoma: Comparison with invasive ductal
carcinoma of breast. BMC Res Notes. 11:5312018. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kim MJ, Gong G, Joo HJ, Ahn SH and Ro JY:
Immunohistochemical and clinicopathologic characteristics of
invasive ductal carcinoma of breast with micropapillary carcinoma
component. Arch Pathol Lab Med. 129:1277–1282. 2005.PubMed/NCBI
|
|
25
|
Ross JS, Fletcher JA, Linette GP, Stec J,
Clark E, Ayers M, Symmans WF, Pusztai L and Bloom KJ: The her-2/neu
gene and protein in breast cancer 2003: Biomarker and target of
therapy. Oncologist. 8:307–325. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kuroda H, Sakamoto G, Ohnisi K and Itoyama
S: Clinical and pathologic features of invasive micropapillary
carcinoma. Breast Cancer. 11:169–174. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Nassar H, Wallis T, Andea A, Dey J, Adsay
V and Visscher D: Clinicopathologic analysis of invasive
micropapillary differentiation in breast carcinoma. Mod Pathol.
14:836–841. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Guo X, Chen L, Lang R, Fan Y, Zhang X and
Fu L: Invasive micropapillary carcinoma of the breast: Association
of pathologic features with lymph node metastasis. Am J Clin
Pathol. 126:740–746. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Evans A, Pinder S, Wilson R, Sibbering M,
Poller D, Elston C and Ellis I: Ductal carcinoma in situ of the
breast: Correlation between mammographic and pathologic findings.
AJR Am J Roentgenol. 162:1307–1311. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Ferretti G, Felici A, Papaldo P, Fabi A
and Cognetti F: HER2/neu role in breast cancer: From a prognostic
foe to a predictive friend. Curr Opin Obstet Gynecol. 19:56–62.
2007. View Article : Google Scholar : PubMed/NCBI
|