Introduction
Papillary thyroid carcinoma (PTC) is a common
endocrine malignant tumor, that has a high incidence worldwide
(1,2). PTC usually develops slowly, and most
patients with PTC have a high overall survival (3). However, ~10% of PTC cases are
characterized by aggressive characteristics and high mortality
rates (4–6). Recently, various studies have
emphasized the importance of risk stratification in order to design
individualized treatments for patients with aggressive PTC
(7–9). Therefore, it is important to identify
novel molecular biomarkers to improve the accurate identification
of high-risk patients with early-stage PTC.
B-Raf proto-oncogene (BRAF), a major human
oncogene, has been identified in various cancers, including thyroid
carcinoma (10,11). The mitogen-activated protein kinase
(MAPK) signaling pathway may be activated by the BRAF V600E
mutation and subsequently contribute to the tumorigenesis of
thyroid cancer (12). Mutations in
BRAF occur in ~50% of patients with PTC and have been
reported to be associated with the aggressiveness-associated
features of PTC, including older age, lymph node metastasis, larger
tumor size and advanced tumor stage (13–16).
However, contrasting results have been reported, and no significant
associations between BRAF mutations and high-risk PTC
characteristics were detected in several studies (17–19).
Human telomerase reverse transcriptase (TERT)
is an important gene involved in the maintenance of chromosomal
integrity and genome stability (20). TERT encodes the catalytic
reverse transcriptase subunit of the telomerase enzyme (20). In total, two common mutations in the
TERT promoter are located at positions −124 and −146 bp
upstream of its translation start site, and are characterized by a
C>T mutation at position 1,295,228 (C228T) and 1,295,250 of
chromosome 5 (C250T), respectively. Mutations in the TERT
promoter lead to TERT overexpression by creating an extra
E26 binding motif, thus facilitating cancer growth (21,22).
This novel genetic alteration occurs in PTC with a prevalence of
7.5-27% (23–26). Interestingly, mutations in
BRAF and the TERT promoter could co-exist in PTC
(25). Several studies have reported
that mutations in the TERT promoter are associated with
aggressive clinicopathological characteristics, especially when
BRAF V600E mutations were also identified (27–29).
However, another study found contrasting results (30). Therefore, the significance of
TERT promoter mutations in predicting the aggressiveness of
PTC is inconclusive and requires further investigation.
In the present study, the incidence and
clinicopathological significance of BRAF and TERT
promoter mutations were analyzed in patients with PTC. Additional
studies on TERT and BRAF mutations may clarify
whether these molecular factors could be used as biomarkers for the
diagnosis and/or prognosis of patients with PTC.
Materials and methods
Patients and tissue samples
In the present study, 205 patients with PTC were
enrolled at The Affiliated Yantai Yuhuangding Hospital of Qingdao
University from January 2015 to December 2016. The surgical
procedures for patients with PTC, including conventional papillary
thyroid carcinoma (CPTC) and papillary thyroid microcarcinoma
(PTMC), were based on the Guidelines for the diagnosis and
treatment of thyroid nodules and differentiated thyroid cancer
(31). According to the surgical
procedure recommended in the guidelines, patients with thyroid
papillary carcinoma underwent total thyroidectomy or thyroid gland
combined with isthmus resection, and routine central lymph node
dissection at the tumor site. Based on the preoperative and
intraoperative conditions, it was decided whether to perform lymph
node dissection of the contralateral neck area. In addition, the
selection of routine use of radioactive iodine after surgery was
also based on the aforementioned guidelines. According to the World
Health Organization classification criteria, 118 patients were
diagnosed with CPTC and 87 patients with PTMC. The American Joint
Committee on Cancer staging system (32) was used for the classification of the
TNM stage. After institutional review board approval and informed
patient consent, thyroid tumor specimens were obtained for genetic
analysis and clinicopathological data was retrospectively
collected. All mutational analyses were performed after surgery,
and the results had no influence on the surgical procedures.
Patients who declined genetic testing or lacked clinicopathological
data were excluded from the study. The clinicopathological data of
the patients enrolled in the present study are presented in
Table I.
 | Table I.Association between BRAF V600E
or TERT promoter mutations and clinicopathological
characteristics in patients with papillary thyroid carcinoma. |
Table I.
Association between BRAF V600E
or TERT promoter mutations and clinicopathological
characteristics in patients with papillary thyroid carcinoma.
|
| BRAF
V600E | TERT
promoter mutation |
|---|
|
|
|
|
|---|
| Clinicopathological
features | Mutated, n=169 | Wild type,
n=36 | OR (95% CI) | P-value | Mutated, n=8 | Wild type,
n=197 | OR (95% CI) | P-value |
|---|
| Sex |
|
|
|
|
|
|
|
|
|
Female | 133 | 28 | 0.947 | 0.903 | 5 | 156 | 2.283 | 0.373 |
|
Male | 36 | 8 | (0.398-2.256) |
| 3 | 41 | (0.524-9.950) |
|
| Age at diagnosis
(years) |
|
|
|
|
|
|
|
|
|
≤45 | 90 | 16 | 0.702 | 0.337 | 1 | 105 | 7.989 | 0.030a |
|
>45 | 79 | 20 | (0.341-1.448) |
| 7 | 92 | (1.001-66.154) |
|
| Tumor size
(mm) |
|
|
|
|
|
|
|
|
|
≤10 | 74 | 12 | 0.642 | 0.248 | 1 | 85 | 5.312 | 0.142 |
|
>10 | 95 | 24 | (0.301-1.368) |
| 7 | 112 | (0.641-44.002) |
|
| Extrathyroidal
invasion |
|
|
|
|
|
|
|
|
| No | 87 | 24 | 1.885 | 0.097 | 1 | 110 | 8.851 | 0.025a |
|
Yes | 82 | 12 | (0.885-4.014) |
| 7 | 87 | (1.069-73.300) |
|
| Multifocality |
|
|
|
|
|
|
|
|
|
Single | 85 | 24 | 1.976 | 0.074 | 1 | 108 | 8.494 | 0.027a |
|
Multifocal | 84 | 12 | (0.928-4.208) |
| 7 | 89 | (1.026-70.344) |
|
| Lymph node
metastasis |
|
|
|
|
|
|
|
|
| No | 69 | 22 | 2.277 | 0.026a | 2 | 89 | 2.472 | 0.305 |
|
Yes | 100 | 14 | (1.090-4.759) |
| 6 | 108 | (0.487-12.551) |
|
| TNM stage |
|
|
|
|
|
|
|
|
|
I–II | 100 | 23 | 1.221 | 0.600 | 1 | 122 | 11.387 | 0.007a |
|
III–IV | 69 | 13 | (0.579-2.574) |
| 7 | 75 | (1.374-94.385) |
|
Genomic DNA isolation
Genomic DNA in the formalin-fixed and
paraffin-embedded specimens was extracted using a DNA Extraction
kit (Promega Corporation) according to the manufacturer's
instructions.
Mutational analysis of BRAF V600E and
the TERT promoter
A human BRAF mutant gene detection kit (Amoy
Diagnostics Co., Ltd.) was used for the detection of BRAF
V600E mutation, as previously described (33). DNA was further analyzed using an
ABI7500 real-time PCR thermocycler (Promega Corporation). The
5-carboxyfuorescein (FAM) and 5-hexachloro-fuorescein (HEX)
contained in the BRAF mutant gene detection kit was used.
The thermocycling conditions were as follows: 95°C For 5 min, 15
cycles of 95°C for 25 sec, 64°C for 20 sec, 72°C for 20 sec, and
then 31 cycles of 93°C for 25 sec, 60°C for 35 sec, 72°C for 20
sec. The primers used were the following: Forward,
5′-TCATAATGCTTGCTCTGATAGGA-3′ and reverse,
5′-GGCCAAAAATTTAATCAGTGGA-3′. The mutation plot was determined by
the cycle threshold values of FAM according to the manufacturer's
instructions. The quality of the extracted DNA was verified by the
amplification of a housekeeping gene, which was reported in the HEX
channel. PCR was used to amplify the TERT promoter
containing the C228T and C250T mutation hotpots, and the PCR
products were sequenced for the detection of TERT promoter
mutations, as previously reported (34,35). Taq
polymerase was used and purchased from Kapa Biosystems; Roche
Diagnostics. The primers for TERT promoter region were the
following 5′-AGTGGATTCGCGGGCACAGA-3′ (sense) and
5′-CAGCGCTGCCTGAAACTC-3′ (antisense) and the PCR conditions were
95°C for 3 min, followed by 10 cycles of 95°C for 30 sec, 55°C for
30 sec and 68°C for 1 min. This was then followed by 30 cycles of
the same settings except for elongation for an additional 5 sec in
each cycle. The PCR was completed with a final elongation step at
68°C for 7 min.
Statistical analysis
Statistical analysis was performed using SPSS
(version 19.0; IBM Corp.). Fisher's exact test and χ2
tests were used for analyzing the relationship between mutations
and clinicopathological features of patients with PTC. P<0.05
was considered to indicate a statistically significant
difference.
Results
Prevalence of mutations in BRAF and
the TERT promoter in patients with PTC
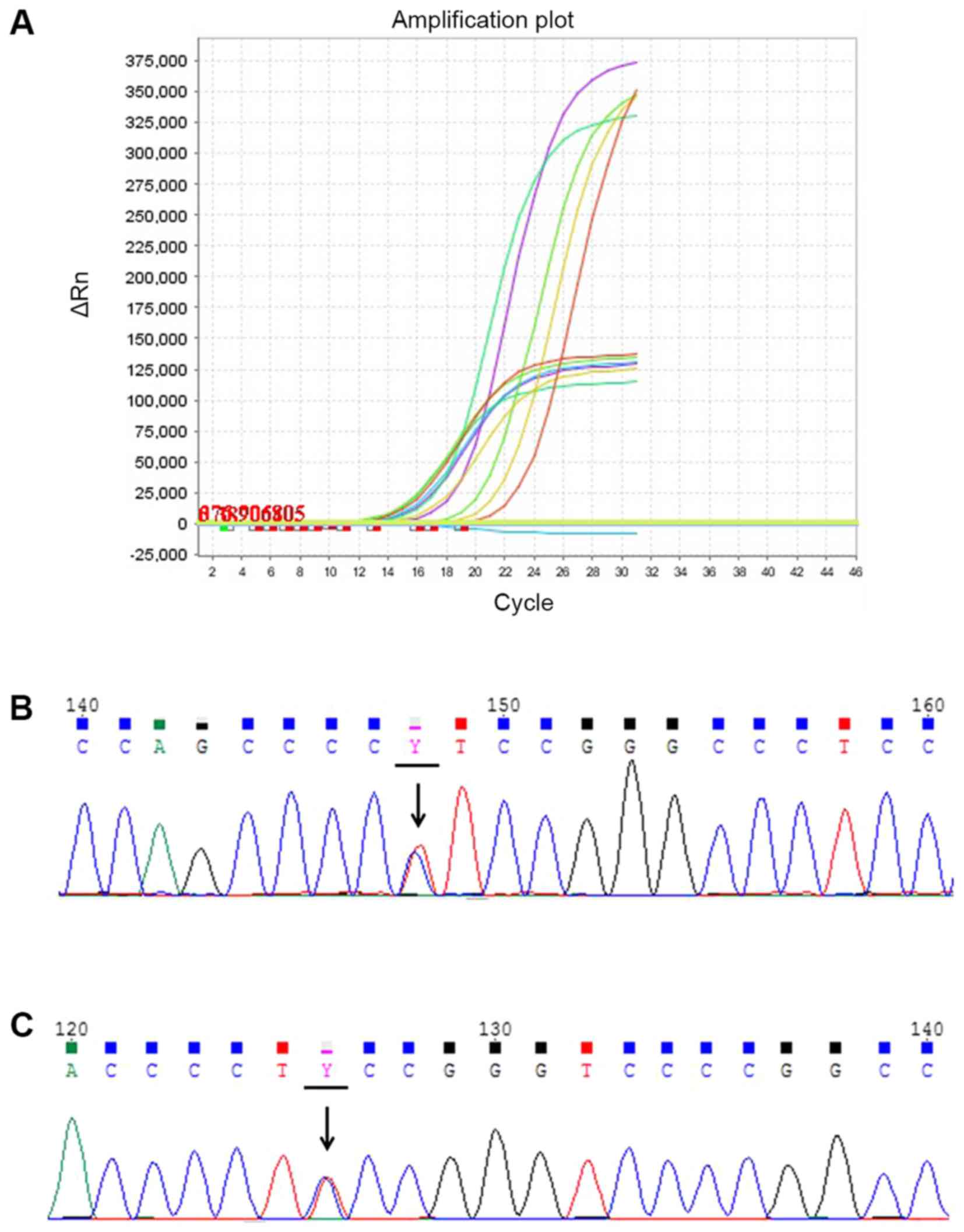
Mutations in BRAF and the TERT
promoter were investigated in 205 PTC patients (161 females and 44
males). Mutations in BRAF and the TERT promoter were
analyzed with quantitative PCR and Sanger DNA sequencing,
respectively (Fig. 1). In total, 169
patients exhibited BRAF V600E mutations, accounting for
82.4% (169/205) of patients with PTCs. Mutations of the TERT
promoter were found in eight patients, with a prevalence of 3.9%
(8/205; Table I). Of the eight cases
analyzed, seven presented a C228T mutation (7/8) and the remaining
patient exhibited a C250T mutation. According to previous studies,
only one type of TERT promoter mutation is commonly found
(34). No cases of simultaneous
mutations (C228T and C250T) were found in the present study. In
addition, among the eight patients with TERT promoter
mutations, six presented with the BRAF V600E mutation (6/8).
In total, 118 patients with CPTC and 87 patients with PTMC was
involved in the present study. The mutation prevalence of
BRAF V600E and TERT promoter was different in these
two histological subtypes. In patients with CPTC, the mutation rate
of BRAF V600E and TERT promoter was 79.66 and 5.93%,
while in patients with PTMC the mutation rate was 86.21 and 1.15%
(data not shown).
Correlation between mutations in BRAF
or the TERT promoter and clinicopathological features of PTC
In the present study, the association between
mutations in BRAF or the TERT promoter and the
clinicopathological parameters of PTC was investigated. As shown in
Table I, a significant difference in
lymph node metastasis was detected between patients with the
BRAF V600E mutation and patients without BRAF
mutations (P=0.026). However, no significant associations were
observed between the BRAF V600E mutation and patient sex,
age at diagnosis, tumor multifocality, extrathyroidal invasion or
tumor/node/metastasis (TNM) stage. Compared with the group without
mutations in the TERT promoter, mutations of the TERT
promoter were significantly associated with an older age at
diagnosis, tumor multifocality, extrathyroidal invasion and
advanced TNM stage (P=0.03, P=0.027, P=0.025 and P=0.007,
respectively), but not with tumor size, sex or lymph node
metastasis.
In order to determine the significance of mutations
in BRAF and the TERT promoter in risk stratification,
patients with PTC were divided into the following three subgroups:
i) Negative for mutations in both BRAF and the TERT
promoter (BRAF−/TERT−); ii)
only positive for the BRAF V600E mutation,
(BRAF+/TERT−); and iii) with or
without the BRAF V600E mutation and positive for TERT
promoter mutations,
(BRAF+/−/TERT+). Compared with
the BRAF−/TERT−group, the
BRAF+/TERT− group was
significantly associated with tumor multifocality (P=0.042) and
lymph node metastasis (P=0.012), while the
BRAF+/−/TERT+ group showed a
significant association with extrathyroidal invasion (P=0.004) and
advanced TNM stage (P=0.013), and tumor multifocality (P=0.004),
and trend towards an increase in lymph node metastasis (P=0.05;
Table II). Interestingly, the
BRAF+/−/TERT+ group showed
significant association with extrathyroidal invasion (P=0.032) and
TNM stage (P=0.009) in comparison with the
BRAF+/TERT− group (Table II). Importantly, the
BRAF+/−/TERT+ group had a
higher incidence of recurrence and distant metastasis compared with
both BRAF−/TERT− and
BRAF+/TERT− groups (Table III). Collectively, these two
molecular biomarkers, and in particular, mutations in the
TERT promoter, may be useful for the identification and
management of patients with poor outcome.
| Table II.Association of BRAF
V600E/TERT promoter mutation status with clinicopathological
characteristics in patients with papillary thyroid carcinoma. |
Table II.
Association of BRAF
V600E/TERT promoter mutation status with clinicopathological
characteristics in patients with papillary thyroid carcinoma.
|
|
|
|
|
| 1 vs. 2 | 1 vs. 3 | 2 vs. 3 |
|---|
|
|
|
|
|
|
|
|
|
|---|
| Clinicopathological
features | BRAF
−/TERT − (1) n=34 | BRAF
+/TERT − (2) n=163 | BRAF
+/−/TERT + (3) n=8 | P-value | OR (95% CI) | P-value | OR (95% CI) | P-value | OR (95% CI) | P-value |
|---|
| Sex |
|
|
|
|
|
|
|
|
|
|
|
Female | 26 | 130 | 5 | 0.484 | 0.825
(0.342-1.988) | 0.668 | 1.950
(0.380-10.013) | 0.412 | 2.364
(0.537-10.399) | 0.367 |
|
Male | 8 | 33 | 3 |
|
|
|
|
|
|
|
| Age at diagnosis
(years) |
|
|
|
|
|
|
|
|
|
|
|
≤45 | 16 | 89 | 1 | 0.056 | 0.739
(0.352-1.550) | 0.423 | 6.222
(0.689-56.203) | 0.114 | 8.419
(1.013-69.989) | 0.028a |
|
>45 | 18 | 74 | 7 |
|
|
|
|
|
|
|
| Tumor size
(mm) |
|
|
|
|
|
|
|
|
|
|
|
≤10 | 12 | 73 | 1 | 0.135 | 0.672
(0.312-1.450) | 0.309 | 3.818
(0.419-34.812) | 0.398 | 5.678
(0.683-47.204) | 0.140 |
|
>10 | 22 | 90 | 7 |
|
|
|
|
|
|
|
| Extrathyroidal
invasion |
|
|
|
|
|
|
|
|
|
|
| No | 24 | 86 | 1 | 0.009a | 2.149
(0.966-4.779) | 0.057 | 16.800
(1.822-154.894) | 0.004a | 7.818
(1.041-64.987) | 0.032a |
|
Yes | 10 | 77 | 7 |
|
|
|
|
|
|
|
| Multifocality |
|
|
|
|
|
|
|
|
|
|
|
Single | 24 | 84 | 1 | 0.008a | 2.257
(1.015-5.019) | 0.042a | 16.800
(1.822-154.894) | 0.004a | 7.443
(0.895-61.866) | 0.064 |
|
Multifocal | 10 | 79 | 7 |
|
|
|
|
|
|
|
| Lymph node
metastasis |
|
|
|
|
|
|
|
|
|
|
| No | 22 | 67 | 2 | 0.022a | 2.627
(1.217-5.670) | 0.012a | 5.500
(1.021-31.589) | 0.050 | 2.094
(0.410-10.691) | 0.303 |
|
Yes | 12 | 96 | 6 |
|
|
|
|
|
|
|
| TNM stage |
|
|
|
|
|
|
|
|
|
|
|
I–II | 23 | 99 | 1 | 0.015a | 1.352
(0.617-2.961) | 0.450 | 14.636
(1.598-134.097) | 0.013a | 10.828
(1.301-90.097) | 0.009a |
|
III–IV | 11 | 64 | 7 |
|
|
|
|
|
|
|
| Table III.Association between BRAF
V600E/TERT promoter mutation status and recurrences or
distant metastasis in patients with papillary thyroid
carcinoma. |
Table III.
Association between BRAF
V600E/TERT promoter mutation status and recurrences or
distant metastasis in patients with papillary thyroid
carcinoma.
|
|
| 1 vs. 2 | 1 vs. 3 | 2 vs. 3 |
|---|
|
|
|
|
|
|
|---|
| Mutation
status | No. of recurrences
or distant metastasis/no. patients | OR (95% CI) | P-value | OR (95% CI) | P-value | OR (95% CI) | P-value |
|---|
|
BRAF−/TERT−
(1) | 1/34 |
|
|
|
|
|
|
|
BRAF+/TERT−
(2) | 4/169 | 0.800
(0.087-7.388) | 1.000 | 19.800
(1.707-129.643) | 0.018a | 24.750
(4.338-141.205) | 0.002a |
|
BRAF+/−/TERT+
(3) | 3/8 |
|
|
|
|
|
|
Discussion
In the present study, mutations in the TERT
promoter showed a greater association with the aggressive
clinicopathological features of PTC compared with the BRAF
V600E mutation. Moreover, patients with TERT promoter
mutations had a poorer outcome, as assessed by recurrence and
distant metastasis rates.
The prevalence of the BRAF V600E mutation in
the present study was 82.4%, which was relatively high compared
with the average worldwide prevalence of ~45%. Several studies have
shown that the prevalence of the BRAF V600E mutation in
patients from Asian countries, including Japan, South Korea and
China, is higher than that of Western countries (16,27,36,37). The
present study found that the frequency of mutations in the
TERT promoter was lower than that of BRAF mutations.
These differences in the mutation frequency can be caused by
various factors, including iodide intake, endocrine disruptors,
analysis of ethnically diverse groups and environmental factors in
certain geographical areas, such as radiation and increased
exposure to asbestos amphibole fluoroedenite in the volcanic areas
(38–41). Moreover, it has been reported that
the prevalence of the BRAF V600E mutation is increasing in
China (27). Another important
reason is that the distribution of BRAF mutation is
associated with the distinct histological subtypes of PTC (40,41). The
present study included 118 patients with CPTC and 87 patients with
PTMC. In a prior study, the distribution of mutations in
BRAF and the TERT promoter displayed a clear
subtype-related pattern (25). In
the present study, the mutation prevalence of BRAF V600E in
patients with CPTC and PTMC was 79.66 and 86.21%, respectively. In
addition, the mutation rate of the TERT promoter was 5.93
and 1.15% in patients with CPTC and PTMC, respectively.
It has been reported in several previous studies
that the BRAF V600E mutation is associated with high-risk
clinicopathological characteristics (15,42–45).
However, some studies have shown no significant association between
BRAF V600E mutations and any clinicopathological features of
PTC (17,18,46–48). A
modest association between BRAF V600E mutations and PTC
clinicopathological features was reported in the present study. Due
to the high prevalence of BRAF V600E, it is difficult to use
this marker to improve the risk stratification and identify
high-risk patients with poor outcome. Therefore, in addition to
BRAF V600E, additional studies are required to identify
novel gene mutations associated with aggressive PTC phenotypes.
In the present study, mutations in the TERT
promoter were significantly associated with aggressive
clinicopathological features compared with patients without
mutations or the BRAF V600E mutation alone, such as the
presence of extrathyroidal invasion and advanced TNM stage.
Furthermore, patients harboring TERT promoter mutations
showed a higher possibility of recurrence and distant metastasis.
The present data suggested that mutations in the TERT
promoter may be a promising genetic molecular biomarker associated
with aggressive PTC. The present findings are in line with previous
studies, and suggest that mutations in the TERT promoter may
enhance the aggressiveness of PTC (24,29,49).
Mutations in BRAF and the TERT promoter co-existed in
6/8 patients with BRAF V600E in the present study. The
BRAF V600E mutation may upregulate the expression of
TERT by activating the MAPK pathway (25). Whether mutations in BRAF and
TERT are directly related to PTC oncogenesis, and if these
gene mutations have synergistic or additive effects on PTC, will
require further investigation.
Genetic testing of thyroid cancer is of great
significance for the diagnosis and prognosis assessment of patients
with PTC and may facilitate follow-up treatments. Importantly,
genetic testing can be used as an auxiliary means for pre-operative
fine needle aspiration biopsy to diagnose unidentified thyroid
nodules, thereby improving the accuracy of diagnosis (50). BRAF V600E plays an important
role as a driving mutation in the early stage of tumorigenesis and
has become an ideal biomarker for thyroid cancer (51). Moreover, BRAF V600E has been
used as one of the prognostic indicators in patients with PTC in
the 2015 edition of the American Thyroid Association (ATA)
Guidelines (52). Previous studies
have shown that TERT promoter mutation is involved in the
pathogenesis of tumors and is associated with tumor aggressiveness
(20). However, whether TERT
promoter mutations could be used as a prognostic indicator for
patients with PTC remains unclear, and the present study has
contributed towards further understanding of this. The detection of
TERT promoter mutations may be helpful to improve the ATA
risk stratification system and guide clinicians to select
appropriate treatments for patients with PTC.
One of the main limitations of the present study is
that no follow-up data was obtained for the patients exhibiting
these mutations, partly due to the short time period after the
diagnosis and the better 5-year survival rate of PTC patients. In
future studies, it would be useful to investigate whether
TERT promoter mutations were of complementary value to the
ATA risk stratification system, and could help identify the
high-risk patients and guide appropriate treatments of them. In
addition, the findings of the present study need to be further
confirmed with a larger sample size, as the prevalence of
TERT mutations was relatively low. Moreover, although
TERT promoter mutations may be a promising molecular
biomarker for identifying aggressive PTC, the therapeutic potential
of simultaneous mutations in BRAF and the TERT
promoter requires further investigation.
In conclusion, mutations in the TERT promoter
may have a low prevalence, but a high value in improving the risk
stratification system and management of patients with aggressive
PTC. The aggressiveness of PTC may be cooperatively driven by
TERT promoter and other gene mutations, and the implication
of TERT promoter mutations for the prognosis and treatment
of patients with PTC should be further investigated.
Acknowledgements
Not applicable.
Funding
The present work was supported by the Natural
Science Fund of Shandong Province, China (grant no.
ZR2016HL37).
Availability of data and materials
The data used and/or analyzed in the present study
are available from the corresponding author on reasonable
request.
Authors' contributions
RL, YuL and CS conceived the study. RL, YuL, WC, JC,
ZZ, LM, LC, HX, YZ, YoL, YX, QY and XY designed the experiments,
provided reagents and collected data. ZZ conducted the experiments.
YuL performed data analysis and wrote the manuscript. All authors
read and approved the final version of the paper.
Ethics approval and consent to
participate
The study protocol was approved by the ethics
committee of The Affiliated Yantai Yuhuangding Hospital of Qingdao
University. Written informed consent was provided by each patient.
When the patient was <18 years of age, informed consent was
provided by the patient's legal guardian.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Davies L and Welch HG: Current thyroid
cancer trends in the United States. JAMA Otolaryngol Head Neck
Surg. 140:317–322. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
La Vecchia C, Malvezzi M, Bosetti C,
Garavello W, Bertuccio P, Levi F and Negri E: Thyroid cancer
mortality and incidence: A global overview. Int J Cancer.
136:2187–2195. 2015. View Article : Google Scholar
|
|
3
|
Ito Y, Kudo T, Kihara M, Takamura Y,
Kobayashi K, Miya A and Miyauchi A: Improvement of lymph node
recurrence rate, but not distant recurrence and carcinoma death
rates, in patients with papillary thyroid carcinoma after
disease-free survival for 5 years. Endocr J. 59:895–901. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Brown RL, de Souza JA and Cohen EE:
Thyroid cancer: Burden of illness and management of disease. J
Cancer. 2:193–199. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Mazzaferri EL and Jhiang SM: Long-term
impact of initial surgical and medical therapy on papillary and
follicular thyroid cancer. Am J Med. 97:418–428. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Durante C, Montesano T, Torlontano M,
Attard M, Monzani F, Tumino S, Costante G, Meringolo D, Bruno R,
Trulli F, et al: Papillary thyroid cancer: Time course of
recurrences during postsurgery surveillance. J Clin Endocrinol
Metab. 98:636–642. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Xing M, Haugen BR and Schlumberger M:
Progress in molecular-based management of differentiated thyroid
cancer. Lancet. 381:1058–1069. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ahn D, Park JS, Sohn JH, Kim JH, Park SK,
Seo AN and Park JY: BRAFV600E mutation does not serve as a
prognostic factor in Korean patients with papillary thyroid
carcinoma. Auris Nasus Larynx. 39:198–203. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Nikiforov YE and Nikiforova MN: Molecular
genetics and diagnosis of thyroid cancer. Nat Rev Endocrinol.
7:569–580. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kimura ET, Nikiforova MN, Zhu Z, Knauf JA,
Nikiforov YE and Fagin JA: High prevalence of BRAF mutations in
thyroid cancer: Genetic evidence for constitutive activation of the
RET/PTC-RAS-BRAF signaling pathway in papillary thyroid carcinoma.
Cancer Res. 63:1454–1457. 2003.PubMed/NCBI
|
|
11
|
Cohen Y, Xing M, Mambo E, Guo Z, Wu G,
Trink B, Beller U, Westra WH, Ladenson PW and Sidransky D: BRAF
mutation in papillary thyroid carcinoma. J Natl Cancer Inst.
95:625–627. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Davies H, Bignell GR, Cox C, Stephens P,
Edkins S, Clegg S, Teague J, Woffendin H, Garnett MJ, Bottomley W,
et al: Mutations of the BRAF gene in human cancer. Nature.
417:949–954. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Li C, Lee KC, Schneider EB and Zeiger MA:
BRAF V600E mutation and its association with clinicopathological
features of papillary thyroid cancer: A meta-analysis. J Clin
Endocrinol Metab. 97:4559–4570. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Xing M: BRAF mutation in papillary thyroid
cancer: Pathogenic role, molecular bases, and clinical
implications. Endocr Rev. 28:742–762. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Xing M, Westra WH, Tufano RP, Cohen Y,
Rosenbaum E, Rhoden KJ, Carson KA, Vasko V, Larin A, Tallini G, et
al: BRAF mutation predicts a poorer clinical prognosis for
papillary thyroid cancer. J Clin Endocrinol Metab. 90:6373–6379.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Xing M, Alzahrani AS, Carson KA, Viola D,
Elisei R, Bendlova B, Yip L, Mian C, Vianello F, Tuttle RM, et al:
Association between BRAF V600E mutation and mortality in patients
with papillary thyroid cancer. JAMA. 309:1493–1501. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Brzezianska E, Pastuszak-Lewandoska D,
Wojciechowska K, Migdalska-Sek M, Cyniak-Magierska A, Nawrot E and
Lewiński A: Investigation of V600E BRAF mutation in papillary
thyroid carcinoma in the Polish population. Neuro Endocrinol Lett.
28:351–359. 2007.PubMed/NCBI
|
|
18
|
Henke LE, Pfeifer JD, Ma C, Perkins SM,
DeWees T, El-Mofty S, Moley JF, Nussenbaum B, Haughey BH, Baranski
TJ, et al: BRAF mutation is not predictive of long-term outcome in
papillary thyroid carcinoma. Cancer Med. 4:791–799. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Nasirden A, Saito T, Fukumura Y, Hara K,
Akaike K, Kurisaki-Arakawa A, Asahina M, Yamashita A, Tomomasa R,
Hayashi T, et al: In Japanese patients with papillary thyroid
carcinoma, TERT promoter mutation is associated with poor
prognosis, in contrast to BRAF (V600E) mutation. Virchows Arch.
469:687–696. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Alzahrani AS, Alsaadi R, Murugan AK and
Sadiq BB: TERT promoter mutations in thyroid cancer. Horm Cancer.
7:165–177. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Vinagre J, Almeida A, Populo H, Batista R,
Lyra J, Pinto V, Coelho R, Celestino R, Prazeres H, Lima L, et al:
Frequency of TERT promoter mutations in human cancers. Nat Commun.
4:21852013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Huang FW, Hodis E, Xu MJ, Kryukov GV, Chin
L and Garraway LA: Highly recurrent TERT promoter mutations in
human melanoma. Science. 339:957–959. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Liu X, Bishop J, Shan Y, Pai S, Liu D,
Murugan AK, Sun H, El-Naggar AK and Xing M: Highly prevalent TERT
promoter mutations in aggressive thyroid cancers. Endocr Relat
Cancer. 20:603–610. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Liu T, Wang N, Cao J, Sofiadis A, Dinets
A, Zedenius J, Larsson C and Xu D: The age- and shorter
telomere-dependent TERT promoter mutation in follicular thyroid
cell-derived carcinomas. Oncogene. 33:4978–4984. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Liu R and Xing M: TERT promoter mutations
in thyroid cancer. Endocr Relat Cancer. 23:R143–R155. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Marques IJ, Moura MM, Cabrera R, Pinto AE,
Simoes-Pereira J, Santos C, Menezes FD, Montezuma D, Henrique R,
Rodrigues Teixeira M, et al: Identification of somatic TERT
promoter mutations in familial nonmedullary thyroid carcinomas.
Clin Endocrinol (Oxf). 87:394–399. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Jin L, Chen E, Dong S, Cai Y, Zhang X,
Zhou Y, Zeng R, Yang F, Pan C, Liu Y, et al: BRAF and TERT promoter
mutations in the aggressiveness of papillary thyroid carcinoma: A
study of 653 patients. Oncotarget. 7:18346–18355. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Liu X, Qu S, Liu R, Sheng C, Shi X, Zhu G,
Murugan AK, Guan H, Yu H, Wang Y, et al: TERT promoter mutations
and their association with BRAF V600E mutation and aggressive
clinicopathological characteristics of thyroid cancer. J Clin
Endocrinol Metab. 99:E1130–E1136. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Xing M, Liu R, Liu X, Murugan AK, Zhu G,
Zeiger MA, Pai S and Bishop J: BRAF V600E and TERT promoter
mutations cooperatively identify the most aggressive papillary
thyroid cancer with highest recurrence. J Clin Oncol. 32:2718–2726.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
de Biase D, Gandolfi G, Ragazzi M,
Eszlinger M, Sancisi V, Gugnoni M, Visani M, Pession A, Casadei G,
Durante C, et al: TERT promoter mutations in papillary thyroid
microcarcinomas. Thyroid. 25:1013–1019. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
American Thyroid Association (ATA)
Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid
Cancer, . Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL,
Mandel SJ, Mazzaferri EL, McIver B, Pacini F, et al: Revised
American thyroid association management guidelines for patients
with thyroid nodules and differentiated thyroid cancer. Thyroid.
19:1167–1214. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Amin MB ES, Greene FL, Byrd DR, Brookland
RK and Washington MK: AJCC Cancer Staging Manual. (8th). (New
York). Springer International. 2017. View Article : Google Scholar
|
|
33
|
Liu R, Hao S, Zhang H, Ma J, Liu X, Xu J,
Liu X, Ning J, Sun Y, Jiang L, et al: Correlation of thyroid
stimulating hormone receptor mRNA expression levels in peripheral
blood with undesirable clinicopathological features in papillary
thyroid carcinoma patients. Oncotarget. 8:74129–74138. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Ren H, Shen Y, Hu D, He W, Zhou J, Cao Y,
Mao Y, Dou Y, Xiong W, Xiao Q, et al: Co-existence of BRAF(V600E)
and TERT promoter mutations in papillary thyroid carcinoma is
associated with tumor aggressiveness, but not with lymph node
metastasis. Cancer Manag Res. 10:1005–1013. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Sun J, Zhang J, Lu J, Gao J, Ren X, Teng
L, Duan H, Lin Y, Li X, Zhang B and Liang Z: BRAF V600E and TERT
Promoter Mutations in Papillary Thyroid Carcinoma in Chinese
Patients. PLoS One. 11:e01533192016. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Song YS, Lim JA, Choi H, Won JK, Moon JH,
Cho SW, Lee KE, Park YJ, Yi KH, Park DJ and Seo JS: Prognostic
effects of TERT promoter mutations are enhanced by coexistence with
BRAF or RAS mutations and strengthen the risk prediction by the ATA
or TNM staging system in differentiated thyroid cancer patients.
Cancer. 122:1370–1379. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Matsuse M, Yabuta T, Saenko V, Hirokawa M,
Nishihara E, Suzuki K, Yamashita S, Miyauchi A and Mitsutake N:
TERT promoter mutations and Ki-67 labeling index as a prognostic
marker of papillary thyroid carcinomas: Combination of two
independent factors. Sci Rep. 7:417522017. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Argyropoulou M, Veskoukis AS, Karanatsiou
PM, Manolakelli A, Kostoglou-Athanassiou I, Vilaras G, Karameris A
and Liadaki K: Low Prevalence of TERT Promoter, BRAF and RAS
Mutations in Papillary Thyroid Cancer in the Greek Population.
Pathol Oncol Res. 26:347–354. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Kim HJ, Park HK, Byun DW, Suh K, Yoo MH,
Min YK, Kim SW and Chung JH: Iodine intake as a risk factor for
BRAF mutations in papillary thyroid cancer patients from an
iodine-replete area. Eur J Nutr. 57:809–815. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Frasca F, Nucera C, Pellegriti G, Gangemi
P, Attard M, Stella M, Loda M, Vella V, Giordano C, Trimarchi F, et
al: BRAF(V600E) mutation and the biology of papillary thyroid
cancer. Endocr Relat Cancer. 15:191–205. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Schulten HJ, Salama S, Al-Mansouri Z,
Alotibi R, AlGhamdi K, Al-Hamour OA, Sayadi H, Al-Aradati H,
Al-Johari A, Huwait E, et al: BRAF mutations in thyroid tumors from
an ethnically diverse group. Hered Cancer Clin Pract. 10:102012.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Elisei R, Ugolini C, Viola D, Lupi C,
Biagini A, Giannini R, Romei C, Miccoli P, Pinchera A and Basolo F:
BRAF(V600E) mutation and outcome of patients with papillary thyroid
carcinoma: A 15-year median follow-up study. J Clin Endocrinol
Metab. 93:3943–3949. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Oler G and Cerutti JM: High prevalence of
BRAF mutation in a Brazilian cohort of patients with sporadic
papillary thyroid carcinomas: Correlation with more aggressive
phenotype and decreased expression of iodide-metabolizing genes.
Cancer. 115:972–980. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Elisei R, Viola D, Torregrossa L, Giannini
R, Romei C, Ugolini C, Molinaro E, Agate L, Biagini A, Lupi C, et
al: The BRAF(V600E) mutation is an independent, poor prognostic
factor for the outcome of patients with low-risk intrathyroid
papillary thyroid carcinoma: Single-institution results from a
large cohort study. J Clin Endocrinol Metab. 97:4390–4398. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Xing M, Alzahrani AS, Carson KA, Shong YK,
Kim TY, Viola D, Elisei R, Bendlová B, Yip L, Mian C, et al:
Association between BRAF V600E mutation and recurrence of papillary
thyroid cancer. J Clin Oncol. 33:42–50. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Ito Y, Yoshida H, Maruo R, Morita S,
Takano T, Hirokawa M, Yabuta T, Fukushima M, Inoue H, Tomoda C, et
al: BRAF mutation in papillary thyroid carcinoma in a Japanese
population: Its lack of correlation with high-risk
clinicopathological features and disease-free survival of patients.
Endocr J. 56:89–97. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Nam JK, Jung CK, Song BJ, Lim DJ, Chae BJ,
Lee NS, Park WC, Kim JS, Jung SS and Bae JS: Is the BRAF(V600E)
mutation useful as a predictor of preoperative risk in papillary
thyroid cancer? Am J Surg. 203:436–441. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Fugazzola L, Puxeddu E, Avenia N, Romei C,
Cirello V, Cavaliere A, Faviana P, Mannavola D, Moretti S, Rossi S,
et al: Correlation between B-RAFV600E mutation and
clinico-pathologic parameters in papillary thyroid carcinoma: Data
from a multicentric Italian study and review of the literature.
Endocr Relat Cancer. 13:455–464. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Muzza M, Colombo C, Rossi S, Tosi D,
Cirello V, Perrino M, De Leo S, Magnani E, Pignatti E, Vigo B, et
al: Telomerase in differentiated thyroid cancer: Promoter
mutations, expression and localization. Mol Cell Endocrinol.
399:288–295. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Yin L, Tang Y, Yu S, Wang C, Xiao M, Wang
Y, Liu SJ, Gao L, Huang K and Jin L: The role of BRAF V600E in
reducing AUS/FLUS diagnosis in thyroid fine needle aspiration.
Endocr Pathol. 30:312–317. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Aubhishek Z, Wei W and Trever GB:
Targeting Oncogenic BRAF: Past, Present, and Future. Cancers
(Basel). 11:11972019. View Article : Google Scholar
|
|
52
|
Li XY, Zhang B and Lin YS: The
Interpretation of 2015 American thyroid association management
guidelines for adult patients with thyroid nodules and
differentiated thyroid cancer. Zhonghua Er Bi Yan Hou Tou Jing Wai
Ke Za Zhi. 52:309–315. 2017.(In Chinese). PubMed/NCBI
|