Introduction
Lung cancer has been reported as the leading cause
of cancer-associated mortality globally in the past 10 years
(1,2). Non-small cell lung cancer (NSCLC) has
been indicated to account for 80–85% of cancer cases, and the
majority of patients have advanced stage or metastatic NSCLC at
diagnosis (3,4). From the eastern cooperative oncology
group 1594 trial, it was indicated that the overall survival (OS)
rate of patients with NSCLC is 8–10 months if patients with
advanced disease received chemotherapy alone (5). It has been reported that
first-generation small molecule tyrosine kinase inhibitors (TKI) of
the epidermal growth factor receptor (EGFR) are a notable factor in
the treatment of advanced or metastatic NSCLC in patients with
inhibitor-sensitive EGFR mutations (6,7).
Numerous phase III studies demonstrated that compared with
traditional chemotherapy, EGFR-TKIs, as first-line treatments,
contributed to the protraction of progression-free survival (PFS)
rate and to an increased response rate (RR) in patients with
inhibitor-sensitive EGFR mutation (8–13).
Furthermore, a previous study demonstrated that the median OS time
was prolonged to 30 months, when patients with EGFR
sensitive-mutations received chemotherapy and TKIs, compared with
an OS time of 10 months in patients who were treated with
chemotherapy alone (14). It has
been reported that inhibitor-sensitive EGFR mutations are an
important indicator of NSCLC response to TKI therapy (15). Therefore, the determination of EGFR
mutation status is important for the optimization of NSCLC
treatment. However, it has also been indicated that limited tissue
size prevents determination of EGFR mutation status. It has been
reported that, in 2013, only 32.8% of patients with NSCLC in China
exhibited EGFR mutations (16). The
population exhibiting optimal response to TKI treatment has been
reported to be in non-smoking Asian female patients with
adenocarcinoma (16). However, it
has been indicated that 36% of patients exhibiting ≥3 of the
aforementioned features did not develop an EGFR mutation (16). Therefore, it is imperative to
identify novel prognostic indicators for the non-invasive detection
of EGFR-mutation status.
Carcinoembryonic antigen (CEA) was first identified
in 1965 in human colon cancer (17).
It has been reported that 30–70% of patients with NSCLC,
particularly those with advanced lung adenocarcinoma, exhibit
elevated serum CEA levels (18–23).
Previous studies reported that following gefitinib treatment,
patients with NSCLC who exhibited increased CEA levels (>50
ng/ml) had an increased OS time (20). However, it has also been reported
that an increased pre-treatment serum CEA level was associated with
poor outcome in patients with NSCLC treated with erlotinib
(18). Other studies indicated that
CEA may be associated with EGFR mutation status (24–26).
Thus far, researchers have not reached a consensus on the
feasibility of serum CEA level as a predictor for the EGFR mutation
status and the prognosis of NSCLC.
18F-fluorodeoxyglucose positron emission
tomography (FDG PET) in addition to reduced dose computed
tomography (CT) has been effectively employed for the staging of
NSCLC (27). Furthermore, it has
been reported that the primary maximum standardized uptake value
(SUVmax) is associated with the status of EGFR mutation
and that the tumor FDG uptake is a notable prognostic factor for
NSCLC (28,29). Despite the SUVmax value
being reported to be increased (≥6) in patients exhibiting
wild-type EGFR, compared with patients exhibiting an EGFR mutation
(26), no significant difference has
been observed in 18F-FDG PET/CT uptake between patients
exhibiting EGFR mutation and their wild-type counterparts
(30).
The association of EGFR mutation status with FDG
uptake and serum CEA level in NSCLC requires further investigation.
The present study examined 18F-FDG PET/CT uptake and the
CEA level in patients with NSCLC exhibiting different EGFR
mutations, in order to predict the EGFR mutation status and
optimize NSCLC treatment.
Materials and methods
Patients
A total of 454 patients with NSCLC were tested for
CEA level and SUVmax in the Wuhan Cancer Center (Wuhan,
China) and 167 were staged by using 18F-FDG PET/CT.
Patient information (n=167) was collected by chart review,
including age, sex, smoking status, pre-treatment serum CEA level
(normal range, 0–5 ng/ml), histological type and clinical stage of
the patient's tumors. The sample included 87 males (52.1%) and 80
females (47.9%), with their age ranging from 28–82 years (mean ±
standard deviation 58.4±10.3 years). A total of 86 cases were
<60 years of age and 81 cases were >60 years of age. The most
common histological type was adenocarcinoma (97.0%), followed by
squamous cell carcinoma (3.0%). The histopathological diagnoses
were confirmed by means of CT-guided core-needle biopsy,
ultrasound-guided percutaneous biopsy or bronchoscopic biopsy
performed in the Wuhan Cancer Center. Tumor-Node-Metastasis (TNM)
stages were recorded in all patients in accordance with the 7th
edition of the American Joint Committee on Cancer (AJCC) staging
manual (31). Patients with stage
I–IV NSCLC were examined for EGFR mutation status, serum CEA level
and subjected to PET/CT for 18F-FDG uptake between
January 2010 and October 2011 at the Cancer Center of the Union
Hospital (Wuhan, China).
Patients with NSCLC were enrolled in the present
study under the following inclusion criteria: i) Histological
confirmation of NSCLC; ii) stage I–IV demonstrated by PET/CT and/or
brain magnetic resonance imaging, and iii) underwent EGFR mutation
detection and serum CEA level detection at diagnosis. Patients with
active pneumonia or other types of infection and diabetes, which
could have confounded the analysis, were not included in the
present study. Patients were also categorized according to the
exons of EGFR mutations. The EGFR mutations at exons 18–21 were
detected using an EGFR 29 Mutations Detection kit (ADx-EG01; Amoy
Diagnostics Co., Ltd.), according to the manufacturer's protocol.
The present study was approved by the Ethics Committee of Union
Hospital, Tongji Medical College, Huazhong University of Science
and Technology (Wuhan, China) and written informed consent was
obtained from each participant prior to the initiation of any
study-associated procedures.
18F-FDG PET/CT image
acquisition and analysis
In accordance with the protocol of Union Hospital of
Tongji Medical College, whole-body 18F-FDG PET/CT scans
were conducted (32). All patients
were asked to fast for ≥6 h prior to intravenous injection of 370
MBq of 18F-FDG and whole-body emission scans were
obtained. The acquired PET data were reconstructed to volumetric
images with a 2D-OSEM algorithm (2 iterations/16 subsets) in the
Discovery LS PET/CT scanner (GE Healthcare) and (2 iterations/8
subsets) in the Biograph PET-CT scanner (Siemens Healthineers).
Images were reconstructed with attenuation correction
(CT-based).
All PET/CT scans were analyzed at the Union Hospital
of Tongji Medical College by a radiologist and a nuclear physician
with 8 and 5 years of PET experience, respectively. For each
involved site, including the primary tumor, the metastatic lymph
nodes and the distant metastases, a region of interest (ROI) was
carefully drawn around the site of suspected lesions. The SUV was
calculated using the standard formula normalized by body weight:
SUV=cdc/(di/w), where cdc is the decay-corrected tracer tissue
concentration (Bq/g), di is the injected dose (Bq), and w is the
body weight of the patient (g). The physiological SUVs of lung
tissue were 0.37–1.29, similar to those previously reported
(33–35). The numerical value is associated with
the differentiation of tumor cells, in addition to the activity and
the degree of malignancy (36–38). In
order to minimize variation and ensure reproducibility, sites where
increased SUV value was considered as physiological uptake were
excluded and the maximal pixel activity in the ROI was the
SUVmax (34,35).
Metastatic lymph nodes were defined as lymph nodes
with increased metabolic activity against the background of
mediastinal structures, based on qualitative visual inspection.
Only lesions with the longest axis ≥1.0 cm were included in the
analysis to avoid partial volume effect. For patients with multiple
metastatic lymph nodes, the mean SUVmax of all lymph
nodes was used for subgroup analyses.
DNA extraction and quantitative
PCR
The formalin-fixed and paraffin-embedded tumor
tissues were collected from patients and DNA extraction performed
with the QIAamp DNA Mini kits (Qiagen GmbH) according to the
manufacturer's protocol. The tyrosine kinase domain of the EGFR
coding sequence, i.e., exons 19 and exon 21, were amplified by
independent rounds of PCR. The sequences of the primers used are
presented in Table I. PCR was
performed with an ADx-EG01 kit (Amoy Diagnostics Co., Ltd.)
according to the manufacturer's protocol. A LightCycler®
480 real-time PCR machine (Roche Diagnostics) with the following
thermocycling conditions: 95°C, 5 min; 95°C, 10 min; 15 cycles of
95°C, 25 sec; 64°C, 20 sec; and 72°C, 20 sec; followed by 31 cycles
of 93°C, 25 sec 60°C, 35 sec; and 72°C, 20 sec. The relative
expression levels were normalized to endogenous control and were
expressed as 2−ΔΔct (39).
 | Table I.Sequences of the primers used for
PCR. |
Table I.
Sequences of the primers used for
PCR.
| Name | Sequences |
|---|
| Exon 19 |
|
|
Forward |
5′-GCAATATCAGCCTTAGGTGCGGCTC-3′ |
|
Reverse |
5′-GCAATATCAGCCTTAGGTGCGGCTC-3′ |
| Exon 21 |
|
|
Forward |
5′-CTAACGTTCGCCAGCCATAAGTCC-3′ |
|
Reverse |
5′-GCTGCGAGCTCACCCAGAATGTCTGG-3′ |
EGFR mutation analysis by
immunohistochemistry
In the majority of cases, pathological tissue
specimens for EGFR mutation analysis were obtained via surgical
resection (n=8/167, 4.8%) and CT-guided core-needle biopsy
(n=120/167, 71.9%). The remaining samples were harvested by
ultrasound-guided percutaneous biopsy (n=18/167, 10.8%), and
bronchoscopic biopsy (n=21/167, 12.6%). Immunohistochemical
examination proceeded according to the standard
avidin-biotin-peroxidase complex method using monoclonal rabbit
antibodies against the exon 21 L858R EGFR mutation (cat. no. 3197)
and the 15-bp E746-750 deletion in exon 19 (cat. no. 2085) (both
from Cell Signaling Technology Inc.). Tissues were fixed in 4%
formalin at room temperature for 8 h, and dehydrated by using
increasing graded alcohol solutions (70, 90 and 100%) and xylene
for 30 mins at room temperature before being embedded in paraffin.
The paraffin-embedded tissue sections (5 mm thickness) were
deparaffinized with xylene and rehydrated by using decreasing
graded ethanol solutions (100, 95, 80 and 70%) for 30 min at room
temperature. Antigens were retrieved by microwave for 15 min in
EDTA buffer (pH 9.0). Sections were washed with TBS/Tween-20 (TBST)
and then blocked with 5% bovine serum albumin at room temperature
for 1 h. The rabbit monoclonal antibodies were applied as the
primary antibody at a dilution of 1:100 at 4°C overnight. Slides
were washed for 5 min in TBST and incubated at room temperature for
1 h with the respective horseradish peroxidase-conjugated
anti-rabbit secondary antibody (cat. no. ab6721; Abcam) diluted
with TBS in a ratio of 1:200. After washing, slides were incubated
with 3,3′-diaminobenzidine tetrahydrochloride (Sigma-Aldrich; Merck
KGaA) and immediately washed under running water after color
development. Slides were counterstained with hematoxylin at room
temperature for 3 min, mounted with dibutyl phthalate xylene and
were observed under a light microscope at a ×100 magnification
(Zeiss AG). Particular care was taken to ensure sufficient tumor
tissues or cells, in terms of quality and quantity (>100 tumor
cells), were available for later mutation detection.
A total of 29 mutations in 4 exons were observed,
including 3 mutations in exon 18 (G719A, G719S and G719C), 19
deletions in exon 19, 2 mutations in exon 20 (S768I and T790M), 3
insertions in exon 20 and 2 mutations in exon 21 (L858R and L861Q).
The EGFR mutation status of each patient was recorded as follows:
Mutant (≥1 mutation) and wild-type (no mutation).
CEA level measurement
The serum CEA level was measured within 1 week prior
to the initial diagnosis of NSCLC. Venous blood (5 ml) was drawn
from all the patients with NSCLC early in the morning, and
specimens were then promptly sent to the clinical laboratory of the
Cancer Center of the Union Hospital, Tongji Medical College, within
30 min. Serum CEA level was quantitatively measured using the Roche
Cobas E601 analyzer (Roche Diagnostics), by
electro-chemiluminescence immunoassay following serum separation,
according to the manufacturer's protocol. After serum separation,
serum CEA level was quantitatively measured using
electro-chemiluminescence immunoassay (ECLIA) kits, according to
the manufacturer's instructions (Roche Diagnostics). The CEA level
was categorized as normal when CEA <5 ng/ml and abnormal when
CEA≥5 ng/l.
Statistical analyses
Statistical analyses were performed using SPSS 19.0
software (IBM Corp.). All data are expressed as the mean ± standard
deviation. Age was a continuous variable and normally distributed,
while SUVmax and CEA were abnormally distributed and
expressed as the median and range. The smoking status, sex and AJCC
stage were categorical variables. The Mann-Whitney U test was used
to make comparisons between 2 groups and the χ2 test to
compare the difference between patients with EGFR-mutant and EGFR
wild-type. Receiver operating characteristic (ROC) curve analysis
was conducted to obtain a cut-off value for SUV and CEA. On the
basis of this value, SUV and CEA were categorized as low or high.
To determine the prognostic markers, multivariate analyses were
performed by using the logistic regression model on the basis of
SUVmax and CEA. The odd ratios, at 95% confidence
intervals (CI) were calculated and the P-values were derived from
two-sided tests. P<0.05 was considered to indicate a
statistically significant difference.
Results
Patient characteristics
The demographic and clinical features of the 167
patients are indicated in Table II.
According to the AJCC staging, 3 patients were classified as stage
I, 5 as stage II, 16 as stage III and 143 as stage IV. Among the
167 subjects, 73 (43.7%) were positive for EGFR mutation and 94
(56.3%) for EGFR wild-type. The mutation subtypes included the
L858R point mutation in exon 21 (n=40; 54.8%), followed by the exon
19 deletion (n=33; 45.2%). The medians for SUVmax were
as follows: Primary lesion, 9.9 (7.3-16.1); and metastatic lymph
nodes, 8.1 (5.7-11.3). The median CEA value was 7.3 (3.5-43.5). Of
the 167 patients, 160 presented with lymph node metastases, of
which 77 had an EGFR mutation and 83 did not. Additionally, among
these 160 cases, 146 patients had mediastinal lymph node
metastasis, 4 had cervical lymph node metastasis, 8 had
supraclavicular lymph node metastasis and 2 had retroperitoneal
lymph node metastasis.
| Table II.Clinicopathological characteristics
of patients. |
Table II.
Clinicopathological characteristics
of patients.
|
Characteristics | Patients, n (%)
(n=167) | Wild-type, n (%)
(n=94) | Mutation, n (%)
(n=73) | P-value |
|---|
| Mean age ± SD,
years | 58.4±10.3 | 58.3±9.8 | 58.5±10.7 | 0.904 |
| Age, years |
|
|
| 0.756 |
|
≤60 | 86 (51.5) | 49 (52.1) | 36 (49.3) |
|
|
>60 | 81 (48.5) | 45 (47.9) | 37 (50.7) |
|
| Sex |
|
|
| 0.876 |
|
Male | 87 (52.1) | 48 (51.1) | 39 (53.4) |
|
|
Female | 80 (47.9) | 46 (48.9) | 34 (46.6) |
|
| Smoking status |
|
|
| <0.001 |
| Never
smoked | 102 (61.1) | 44 (46.8) | 58 (79.5) |
|
| Regular
smoker | 39 (23.3) | 33 (35.1) | 10 (13.7) |
|
|
Ex-smoker | 26 (15.6) | 17 (18.1) | 5 (6.8) |
|
| AJCC stage |
|
|
| 0.202 |
| I | 3 (1.8) | 0 (0.0) | 3 (4.1) |
|
| II | 5 (3.0) | 1 (1.1) | 4 (5.5) |
|
|
III | 16 (9.6) | 11 (11.7) | 5 (6.8) |
|
| IV | 143 (85.6) | 82 (87.2) | 61 (83.6) |
|
| Histology type |
|
|
| <0.001 |
|
Squamous cell carcinoma | 5 (3.0) | 4 (4.3) | 1 (1.4) |
|
|
Adenocarcinoma | 162 (97.0) | 90 (95.7) | 72 (98.6) |
|
| Median
SUVmax, primary lesion | 9.9 | 15.3 | 8.1 | <0.001 |
| SUVmax
range, primary lesion | 7.3-16.1 | 9.7-19.0 | 5.1-9.8 | <0.001 |
|
SUVmax≤5 | 20 (12.0) | 6 (30.0) | 14 (70.0) |
|
|
5<SUVmax≤10 | 53 (31.7) | 23 (43.3) | 30 (56.6) |
|
|
10<SUVmax≤15 | 40 (24.0) | 14 (35.0) | 26 (65.0) |
|
|
SUVmax>15 | 54 (32.3) | 51 (94.4) | 3 (5.6) |
|
| Median
SUVmax, metastatic lymph nodes | 8.1 | 10.1 | 6.5 | <0.001 |
| SUVmax
range, metastatic lymph nodes | 5.7-11.3 | 6.9-14.5 | 3.6-8.7 | <0.001 |
|
SUVmax≤5 | 32 (19.2) | 8 (25.0) | 24 (75.0) |
|
|
5<SUVmax≤10 | 76 (45.5) | 39 (51.3) | 37 (48.7) |
|
|
SUVmax>10 | 54 (32.3) | 47 (87.0) | 7 (13.0) |
|
| Median CEA,
ng/ml | 7.3 | 6.0 | 12.5 | 0.001 |
| CEA range,
ng/ml | 3.5-43.5 | 3.4-29.5 | 4.3-76.0 | <0.001 |
|
CEA≤5 | 59 (35.3) | 41 (69.5) | 18 (30.5) |
|
|
5<CEA≤10 | 31 (18.6) | 24 (77.4) | 7 (22.6) |
|
|
10<CEA≤15 | 10 (6.0) | 1 (10.0) | 9 (90.0) |
|
|
CEA>15 | 66 (39.5) | 28 (42.4) | 38 (57.6) |
Association between clinical factors
and EGFR mutation status
Among 73 patients, EGFR mutations were identified in
39 male patients (53.4%) and 34 female patients (46.6%). Among the
94 EGFR-wild-type patients (56.3%), 48 were male (51.1%) and 46
were female (48.9%) (Table II). A
χ2 test showed there were no significant differences in
EGFR mutation proportion between sex (P=0.876) and among different
age groups (P=0.904), stages (P=0.202). Adenocarcinoma histology
type tended to express EGFR mutations (P<0.001). In addition,
EGFR mutation was associated with decreased SUVmax
levels and increased CEA levels in non-smoking subjects, compared
with EGFR-wild-type (P<0.001; Table
II).
Multivariate analysis of predictive
factors of EGFR mutation
Univariate analysis demonstrated that the
histological type was associated with EGFR mutation, and patients
with adenocarcinoma exhibited a significantly increased frequency
of EGFR mutations (P<0.001; Table
II). This increase may be due to the unbalanced patient number
in the squamous cell carcinoma and adenocarcinoma groups. The
multivariate logistic regression analysis revealed that smoking
status, SUVmax in primary lesions, SUVmax in
metastatic lymph nodes, and CEA classification were independent
predictors of EGFR mutation. Additionally, non-smoking status and
the high CEA value (10–15 ng/ml) were the most significant
predictors of EGFR mutation (Table
III). Patients with SUVmax >15 in primary lesions
and SUVmax >10 in metastatic lymph nodes were less
prone to mutation (P<0.001; Table
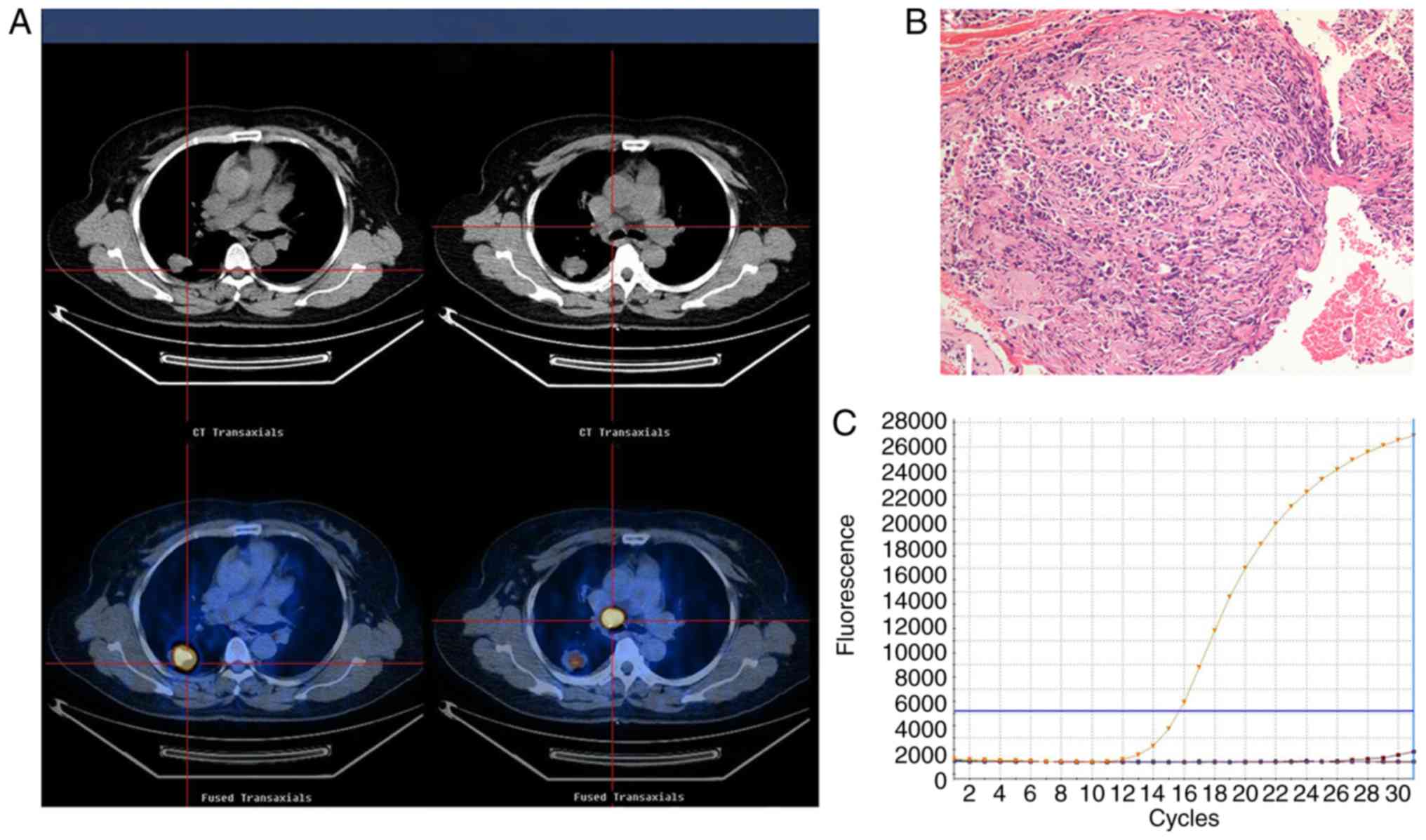
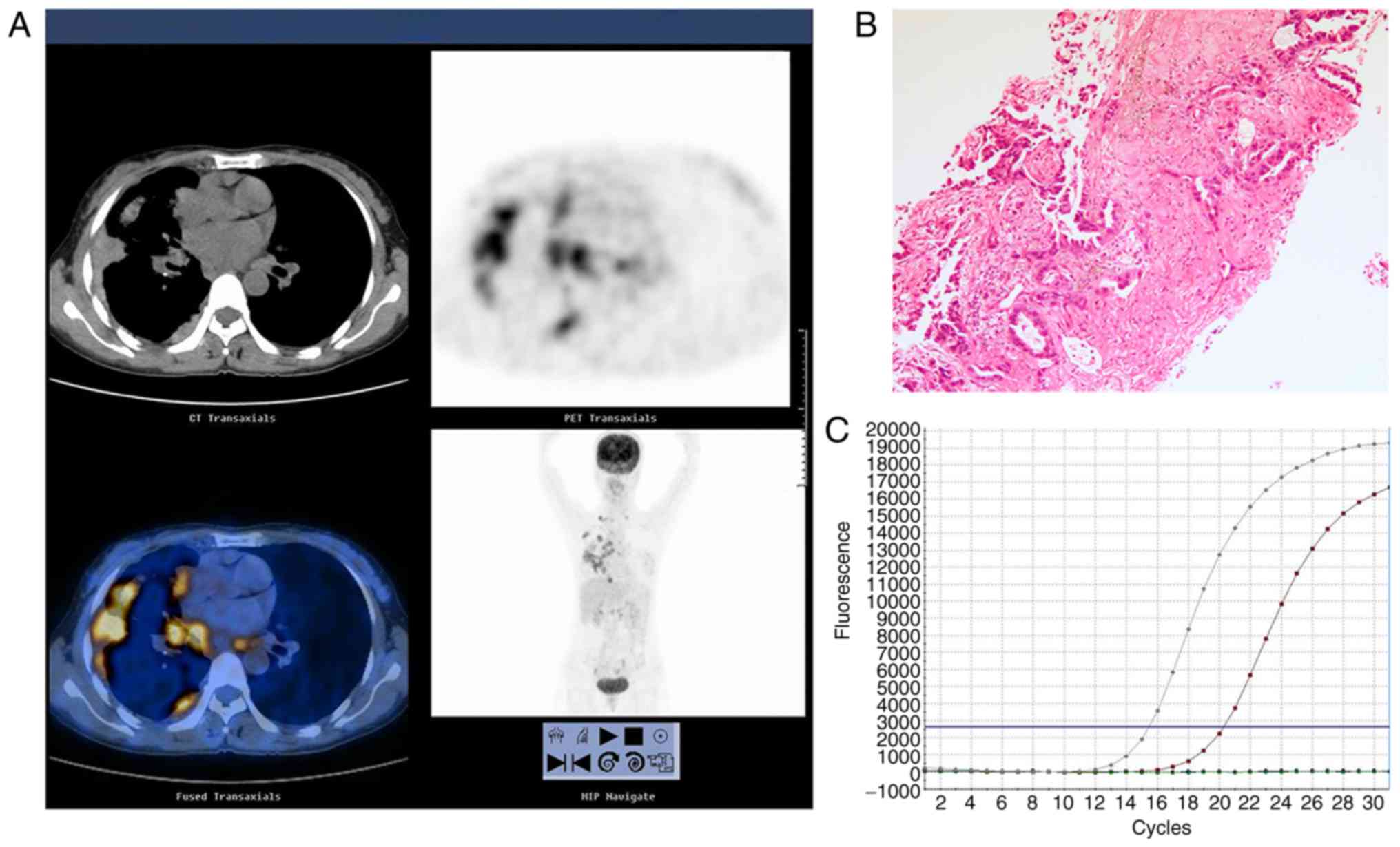
III). 18F-FDG PET/CT images, histological and
immunohistochemical results in a representative patient with EGFR
status are indicated in Figs.
1–3.
| Table III.Multivariate analysis for predictive
factors of epidermal growth factor receptor mutation. |
Table III.
Multivariate analysis for predictive
factors of epidermal growth factor receptor mutation.
| Factor | Hazard ratio | 95% CI | P-value |
|---|
| Smoking status |
|
|
|
|
Never-smokeda | 1.00 | – | – |
|
Ex-smoker | 0.85 | 0.07-1.97 | 0.245 |
| Regular
smoker | 0.71 | 0.11-1.70 | 0.224 |
| SUVmax,
primary lesion |
|
|
|
|
SUVmax≤5a | 1.00 | – | – |
|
5<SUVmax≤10 | 3.68 | 0.01-1.05 | 0.055 |
|
10<SUVmax≤15 | 6.33 | 0.01-0.52 | 0.012 |
|
SUVmax>15 | 19.50 | 0.00-0.02 | <0.001 |
| SUVmax,
metastatic lymph nodes |
|
|
|
|
SUVmax≤5a | 1.00 | – | – |
|
5<SUVmax≤10 | 0.66 | 0.06-0.88 | 0.032 |
|
SUVmax>10 | 0.85 | 0.02-0.64 | 0.013 |
| CEA, ng/ml |
|
|
|
|
CEA≤5a | 1.00 | – | – |
|
5<CEA≤10 | 0.73 | 1.00-1.73 | 0.227 |
|
10<CEA≤15 | 1.16 | 0.61-56.94 | 0.127 |
|
CEA>15 | 0.64 | 0.66-8.03 | 0.193 |
| Histology type |
|
|
|
| Squamous cell
carcinomaa | 1.00 | – | – |
|
Adenocarcinoma | 3.20 | 0.35-29.26 | 0.303 |
Association between EGFR status and
serum CEA level
The median value of CEA of the EGFR wild-type group
was significantly decreased compared with the EGFR mutation group
(6.0 vs. 12.5; P=0.001). To evaluate whether the pre-treatment CEA
level was associated with the EGFR status, patients were divided
into four groups according to their pre-treatment CEA levels
(CEA≤5, 5<CEA≤10, 10<CEA≤15 and CEA>15 ng/ml). A trend
towards an increased incidence of EGFR mutation was observed in
patients with increased CEA values (P<0.001; Table II).
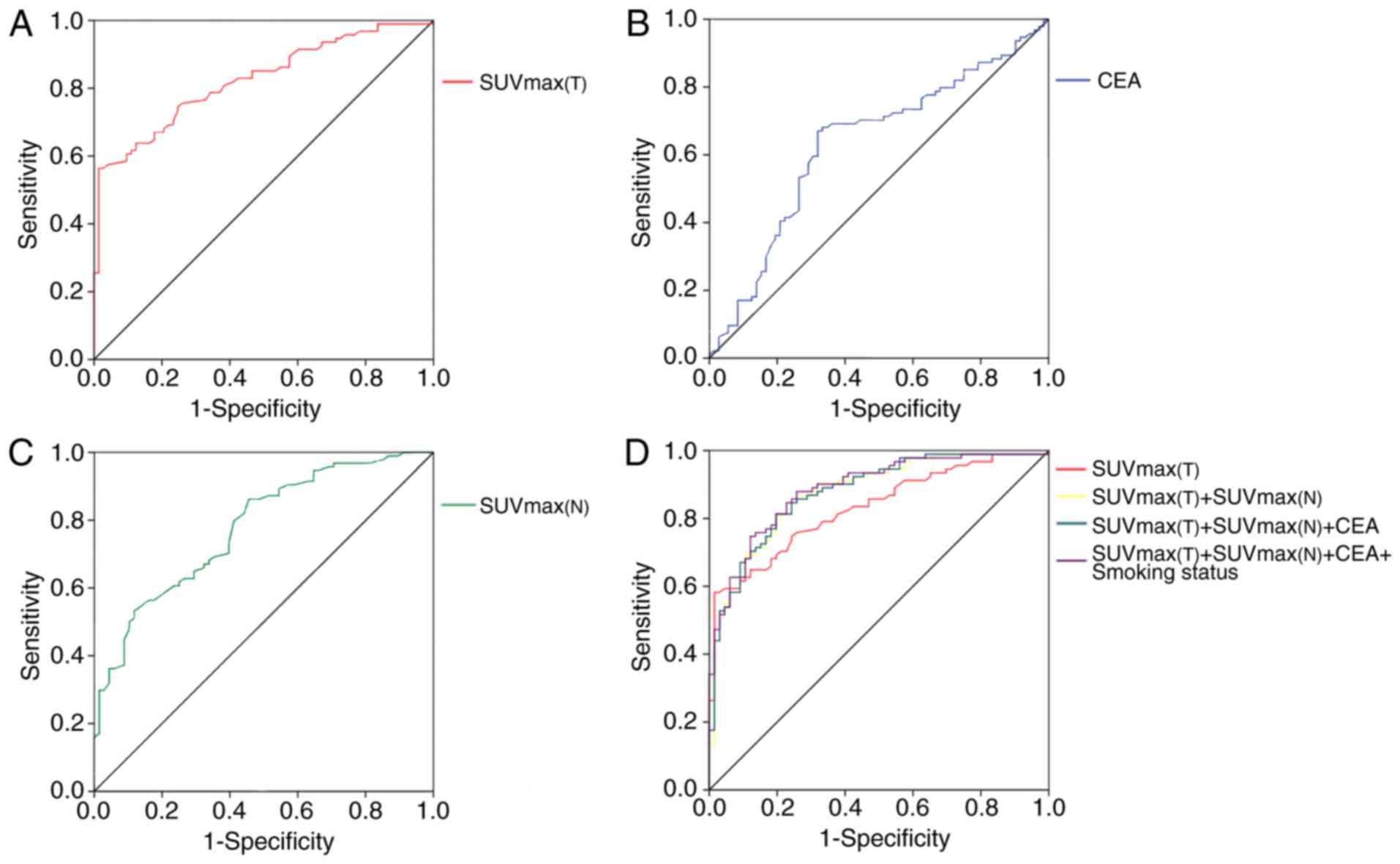
A ROC curve was analyzed to select a cut-off value
for CEA level, which could be used to identify patients with an
increased risk of EGFR mutations. A cut-off value of 9.6 was
determined and ROC analysis of CEA levels indicated a sensitivity
of 67.0%, a specificity of 68.1% and an area under the curve (AUC)
of 0.632 (95% CI, 0.546–0.719) (Table
IV). The frequency of EGFR mutations was increased in patients
with CEA overexpression, compared with patients with decreased CEA
level (40% vs. 11%; P=0.0010; Fig.
4B).
| Table IV.Comparative receiver operating
characteristic analysis of predictive factors to discriminate
epidermal growth factor receptor mutation. |
Table IV.
Comparative receiver operating
characteristic analysis of predictive factors to discriminate
epidermal growth factor receptor mutation.
| Predictive
factors | AUC | 95% CI | Sensitivity, % | Specificity, % | P-value |
|---|
|
SUVmax(T) | 0.830 | 0.768-0.892 | 87.7 | 63.8 | <0.001 |
|
SUVmax(N) | 0.777 | 0.634-0.842 | 88.2 | 53.2 | <0.001 |
| CEA | 0.632 | 0.546-0.719 | 68.1 | 67.0 | <0.001 |
|
SUVmax(T)+SUVmax(N) | 0.876 | 0.821-0.930 | 82.4 | 81.3 | <0.001 |
|
SUVmax(T)+SUVmax(N)+CEA | 0.877 | 0.824-0.931 | 85.3 | 75.1 | <0.001 |
|
SUVmax(T)+SUVmax(N)+CEA+smoking
status | 0.886 | 0.835-0.937 | 82.1 | 80.3 | <0.001 |
Association between EGFR mutation and
the SUVmax in primary lesions
The median value of SUVmax in primary
lesions [SUVmax(T)] was significantly increased in the
EGFR wild-type group, compared with the EGFR mutant group (15.3 vs.
8.1; P<0.001). ROC curve analysis was performed to select a
cut-off value for SUVmax(T), in order to identify
patients with increased probability of EGFR mutations (Fig. 4A). ROC analysis indicated a cut-off
value of 11.5 for SUVmax(T) with a specificity of 87.7%,
a sensitivity of 63.8% and an AUC of 0.830 (95% CI,
0.768–0.892).
Association between EGFR status and
metastatic lymph nodes
The median SUVmax values in metastatic
lymph nodes of the EGFR wild-type group and mutation group were
10.1 and 6.5, respectively (P<0.001; Table II). The SUVmax of
metastatic lymph nodes [SUVmax(N)] was a predictive
value for EGFR gene mutation. ROC analysis was performed and a
cut-off value of 9.8 for SUVmax(N) with specificity of
53.2%, a sensitivity of 88.2% and an AUC of 0.777 was determined
(P<0.001; Table IV; Fig. 4C). When four factors which were
SUVmax(T), SUVmax(N), CEA level and smoking
status were all included, the AUC was increased to 0.886, compared
with the AUC of primary tumor SUVmax, indicating that
these factors can predict EGFR mutation status (Table IV; Fig.
4D).
The differences in CEA and
SUVmax between EGFR gene mutations in exon 19 and
21
The association between each individual factor and
the two types of EGFR mutation was analyzed. No significant
difference was noted between the two mutation groups in terms of
sex, age, smoking status, histological type or serum CEA levels. A
significant difference in the SUVmax in primary lesions
existed between the two groups (P=0.021; Table V). The median SUVmax was
10.6 in the EGFR exon 19 mutation group and 8.7 in the exon 21
mutation group in primary lesions.
| Table V.Association between clinical factors
and epidermal growth factor receptor mutation status in exon 19 and
21. |
Table V.
Association between clinical factors
and epidermal growth factor receptor mutation status in exon 19 and
21.
|
Characteristics | Exon 19 mutation, n
(%) (n=33) | Exon 21 mutation, n
(%) (n=40) | P-value |
|---|
| Age, years |
|
|
|
|
≤60 | 17 (51.5) | 19 (47.5) | 0.816 |
|
>60 | 16 (48.5) | 21 (52.5) |
|
| Sex |
|
| 0.876 |
|
Male | 20 (60.6) | 19 (47.5) |
|
|
Female | 13 (39.4) | 21 (52.5) |
|
| Smoking status |
|
| 0.805 |
| Never
smoked | 26 (78.8) | 31 (77.5) |
|
| Regular
smoker | 7 (21.2) | 7 (17.5) |
|
|
Ex-smoker | 0 (0.0) | 2 (5.0) |
|
| AJCC stage |
|
| 0.880 |
| I | 1 (3.0) | 2 (5.0) |
|
| II | 2 (6.1) | 2 (5.0) |
|
|
III | 3 (9.1) | 2 (5.0) |
|
| IV | 27 (81.8) | 34 (85.0) |
|
| Histology type |
|
| 0.268 |
|
Squamous cell carcinoma | 1 (3.0) | 0 (0.0) |
|
|
Adenocarcinoma | 32 (97.0) | 40 (100.0) |
|
| Median
SUVmax, primary lesion | 10.6 | 8.7 | 0.021 |
| SUVmax
range, primary lesion | 7.2-12.7 | 5.0-10.2 | 0.057 |
|
SUVmax≤5 | 4 (28.6) | 10 (71.4) |
|
|
5<SUVmax≤10 | 12 (40.0) | 18 (60.0) |
|
|
10<SUVmax≤15 | 14 (53.8) | 12 (46.2) |
|
|
SUVmax>15 | 3 (100.0) | 0 (0.0) |
|
| Median
SUVmax, metastatic lymph nodes | 6.7 (3.6-8.3) | 6.9 (4.0-9.5) | 0.960 |
| SUVmax
range, metastatic lymph nodes |
|
| 0.920 |
|
SUVmax≤5 | 11 (45.8) | 13 (54.2) |
|
|
5<SUVmax≤10 | 15 (40.5) | 22 (59.5) |
|
|
SUVmax>10 | 3 (42.9) | 4 (57.1) |
|
| Median CEA,
ng/ml | 22.5 | 24.9 | 0.771 |
| CEA range,
ng/ml | 5.6-53.0 | 4.5-91.2 | 0.780 |
|
CEA≤5 | 8 (40.0) | 12 (60.0) |
|
|
5<CEA≤10 | 6 (60.0) | 4 (40.0) |
|
|
10<CEA≤15 | 5 (45.5) | 6 (54.5) |
|
|
CEA>15 | 14 (45.2) | 17 (54.8) |
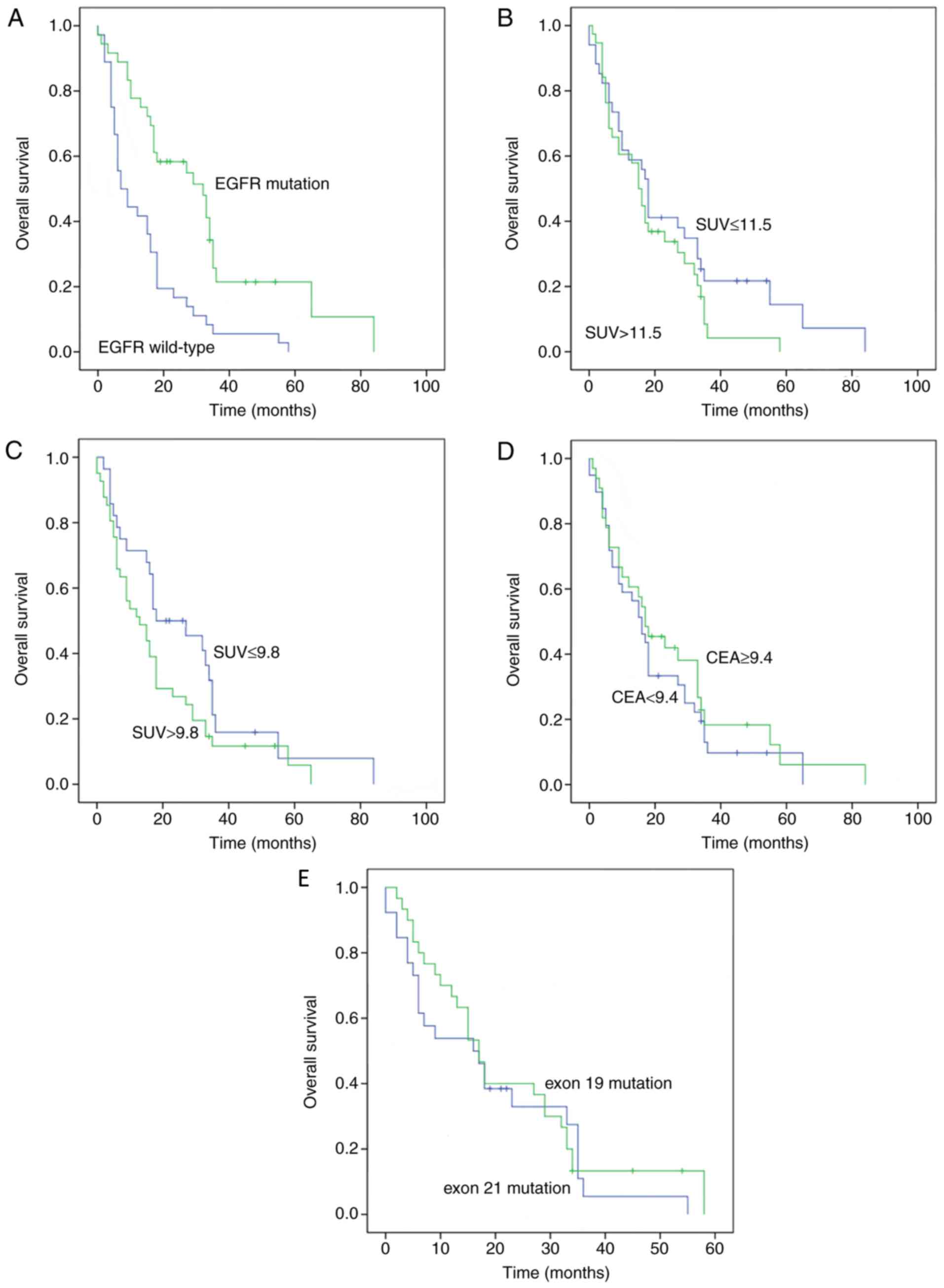
SUVmax and OS time
A total of 88 patients received EGFR-TKI treatment,
and 73 patients developed EGFR mutations. The median OS time of all
patients was 17.08 months. Patients with EGFR mutations had an
increased OS time, compared with their EGFR wild-type counterparts
(32.8 months vs. 7.8 months; P=0.001; Fig. 5). In terms of the SUVmax
values in primary lesions (SUVmax ≤11.5 vs.
SUVmax >11.5), the median OS time in the
SUVmax ≤11.5 group was increased, compared with the
SUVmax >11.5 group, but the difference was not
statistically significant (18.6 months vs. 16.1 months; P=0.179).
In terms of SUVmax values in metastatic lymph nodes
(SUVmax ≤9.8 vs. SUVmax >9.8), the median
OS time in the SUVmax ≤9.8 group was increased, compared
with the SUVmax >9.8 group, but the difference was
not significant (19.3 months vs. 13.1 months; P=0.079). The median
OS time in the CEA ≤9.4 group was reduced, compared with the group
with CEA level >9.4, but the difference was not statistically
significant (16.4 months vs. 17.4 months; P=0.418). In terms of
EGFR mutation type, the median OS time was increased in patients
with the in-frame deletion in exon 19, compared with patients with
exon 21 mutation (27.5 months vs. 24.3 months; P=0.532).
Discussion
In the present study, it was demonstrated that
18F-FDG PET/CT SUVmax and serum CEA levels
prior to initial treatment were associated with EGFR mutations in
patients with NSCLC. Patients with a reduced SUVmax in
the primary lesions were more significantly associated with EGFR
mutation, compared with the control group. The ROC analysis
indicated that SUVmax serves as a predictor for EGFR
mutation. Increased 18F-FDG PET/CT uptake (SUV≥11.5) may
serve as a predictor of the wild-type EGFR genotype, whereas a
reduced SUVmax (SUV<11.5) may be indicative of EGFR
mutations. The present study demonstrated that metastatic lymph
nodes in patients with EGFR mutations had significantly reduced
SUVmax, compared with patients with EGFR wild-type. ROC
analysis demonstrated that increased CEA levels (CEA≥9.4) were
associated with EGFR gene mutation. Furthermore, multivariate
analysis revealed that non-smoking status, low SUVmax of
the primary lesions and high CEA levels were significantly
associated with EGFR mutation status.
EGFR is a transmembrane receptor present on the cell
surface (40). It has been reported
that EGFR mutations occur in exon 19 and 21, and a number of
studies have reported that EGFR mutation is associated with
improved prognosis in TKI-treated patients (8,9,13). According to the Iressa Pan-Asian
study, the objective RR was 71.2% when patients with EGFR-sensitive
mutations received TKI treatment, while the RR was only 1.1% in
patients with EGFR-wild-type receiving TKI treatment (8). A previous study indicated that the
median OS time was prolonged to 30 months when patients with EGFR
mutations received chemotherapy and TKIs, compared with 10 months
in patients receiving chemotherapy alone (13). Therefore, the identification of the
EGFR genotype is notable and may optimize treatment for patients
with lung adenocarcinoma. However, it is sometimes difficult to
obtain sufficient tumor tissues for genetic tests and, in some
cases, invasive tests are not feasible. In these scenarios,
non-invasive EGFR mutation detection is clinically desirable.
Previous studies reported different variations in
the EGFR mutation rate according to region. Western countries have
exhibited an EGFR mutation rate of 10%, while Asian countries have
reported an EGFR mutation rate as high as 51.4% (41–43).
Furthermore, an increased rate of EGFR mutation has been reported
in non-smokers (60.7%) and females (61.1%). In the present study,
it was indicated that among 167 patients with NSCLC, 73 (43.7%)
exhibited EGFR mutations and 94 (56.3%) did not. The smoking status
was demonstrated to be significantly associated with EGFR mutation
frequency.
It was also indicated in the present study that the
SUVmax of the primary lesion in 73 patients with EGFR
mutation was significantly decreased (median SUVmax,
8.1), compared with the 94 patients with EGFR wild-type (median
SUVmax, 15.3). ROC analysis revealed that high
18F-FDG PET/CT uptake (SUVmax ≥11.5) may
serve as a predictor of the wild-type EGFR genotype. Nonetheless,
the results of the present study were inconsistent with that of
Putora et al (44), which
reported that in 28 patients with lung adenocarcinoma, including 14
patients with EGFR mutation and 14 patients with wild-type EGFR,
the mean SUVmax was 10.7 for EGFR-mutated adenocarcinoma
cases and 9.9 for wild-type tumor cases. The study did not
demonstrate any association between SUVmax values and
EGFR mutation status. This could be due to the small size of the
study. In the study by Ko et al (26), involving 132 patients with pulmonary
adenocarcinoma, including 69 patients with EGFR mutation, it was
reported that patients with SUVmax ≥6 had an increased
probability of exhibiting EGFR mutations. In the study by Huang
et al (45), which enrolled
77 patients with adenocarcinoma, including 49 patients with EGFR
mutation and 28 patients with wild-type EGFR tumors,
18F-FDG PET/CT uptake was significantly increased in
tumors with EGFR mutation (mean SUVmax, 10.5±4.7),
compared with tumors with EGFR wild-type (mean SUVmax,
8.0±3.3). The ROC analysis of the aforementioned study indicated a
cut-off value of SUVmax ≥9.5, which was predictive of
EGFR mutation status. In contrast, the study by Mak et al
(46) examined 100 patients with
NSCLC, including 24 patients with EGFR mutations and patients with
stage I–IV tumors (4 with stage IA, 2 with stage IB, 2 with stage
IIIA, 5 with stage IIIB and 11 with stage IV), and demonstrated
that patients with decreased SUVs had an increased probability of
exhibiting EGFR mutations, compared with those with increased SUVs.
Another study reported that increased SUVmax in the
primary lesions was associated with EGFR wild-type, compared with
their mutant counterparts (47). The
multivariate analysis of the aforementioned study indicated that
decreased SUVmax of the primary tumor was predictive of
EGFR mutation (47). Furthermore,
the ROC curve analysis of the study by Choi et al (47) identified a cut-off value of ≥5.0 to
distinguish wild-type from mutant tumors. The present study
demonstrated that low SUVmax (SUVmax ≤11.5)
was associated with EGFR mutation and this result was in line with
the data of two aforementioned studies (46,47).
Additionally, the present study also demonstrated that the exon 19
mutation (median SUVmax, 10.6) was strongly associated
with high SUVmax in comparison with the exon 21 mutation
(median SUVmax, 8.7). However, this observation does not
coincide with the results of Choi et al (47), which indicated that SUVmax
is significantly decreased in the exon 19 mutation group, compared
with the exon 21 mutation group.
One of the strengths of the present study was the
inclusion of reliable clinical, tumor markers and imaging criteria
for the prediction of EGFR mutation. In previous studies, the
calculated AUC of SUVmax was 0.62–0.74 (48,49).
Diagnostic efficiency of SUVmax alone has been reported
to be insufficient, as Cho et al (49) indicated that the highest sensitivity
of SUVmax alone was 79.3%. In the present study, ROC
curve analyses were further applied to evaluate the diagnostic
efficiency of SUVmax, CEA level and the combination of
SUVmax, CEA level and smoking status, in order to
differentiate between the EGFR mutation group and the wild-type
group. In terms of EGFR mutation status prediction, the sensitivity
and specificity of SUVmax, CEA level and smoking status
alone did not exceed 80%. However, by combining clinical or serum
factors with SUVmax to increase the AUC to 0.886, the
sensitivity and specificity were >80%. It was also reported that
patients with EGFR mutations had an increased OS time, compared
with those with EGFR wild-type (32.8 months vs. 7.8 months;
P=0.001). These observations were in accordance with those of
previous studies (13,47,50–52).
The present study is different from previous studies
in a number of aspects. Firstly, patients enrolled were primarily
at stage III and IV of the disease, because EGFR-TKI treatment is
used for late-stage tumors (12,53).
Secondly, the data was analyzed in terms of different mutation
types and were consistent with a previous study (54). The research of the present study
demonstrated that following EGFR-TKI treatment, patients with
advanced NSCLC with exon 19 deletion had an increased OS time,
compared with those with L858R mutation of exon 21. Thirdly, the
present data was collected from mainland China, in which EGFR
mutation rate has been reported to be 43.7%, in contrast to
previous studies conducted in the Taiwan region of China or Korea
where a ~20% EGFR mutation rate in adenocarcinoma has been reported
(26,45,46). The
data of the present study were consistent with a previous study,
which indicated that in 1,482 patients from Asian countries, the
EGFR mutation rate was ~51.4% (41).
Lastly, it was indicated that the SUVmax of primary
pulmonary lesions and metastatic lymph nodes in mediastinal,
supraclavicular regions and pelvic cavity was decreased in the EGFR
mutation group, compared with the EGFR wild-type group. It has been
reported that inter-tumor heterogeneity in EGFR mutations is a
potential explanation for this phenomenon (55).
Serum CEA is frequently reported to be overexpressed
in patients with NSCLC, particularly in adenocarcinoma cases.
Additionally, patients with adenocarcinoma exhibit significantly
increased mutation rates of EGFR, compared with their
non-adenocarcinoma counterparts (56,57). The
present study also revealed that patients with increased-serum CEA
levels (≥12.5 ng/ml) at initial diagnosis were the ideal patient
population for EGFR-TKI therapy, because this population was
indicated to have an increased inhibitor-sensitive mutation rate
(58). In a study involving 113
Chinese patients with adenocarcinoma, including 59 with EGFR
mutations and 54 EGFR wild-type tumors, CEA level was significantly
increased in tumors with EGFR mutations, compared with tumors with
EGFR wild-type (55).
In the present study, the results were categorized
by type of EGFR mutation and it was indicated that the mean
SUVmax was significantly increased in the exon 19 group,
compared with the exon 21 group. ROC analysis also demonstrated
that increased CEA levels (CEA ≥9.4) were associated with EGFR gene
mutation. A limitation of the present study was that it was of
retrospective design, therefore selection bias was unavoidable and
further investigation is required. Furthermore, indexes of
SUVmax and CEA levels cannot replace conventional
EGFR-mutation detection when adequate tumor tissue is available for
DNA analysis. In conclusion, the present study indicated that in
patients with advanced NSCLC, particularly Chinese patients, a
decreased SUVmax and an increased CEA level are
associated with EGFR mutation and may serve as predictors for
responsiveness to EGFR-TKI therapy.
Acknowledgements
Not applicable.
Funding
The present study was supported by the National
Nature Science Foundation of China (grant nos. 30800283 and
81172595), the Postdoctoral foundation of China (grant no.
20100480905) and by the Postdoctoral special foundation of China
(grant no. 201104440).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
XG and CW analyzed the patient data and wrote the
manuscript. RZ made substantial contributions to quality control of
the study, and analyzed and described the figures. QC, YH and FT
acquired the data and were involved in drafting the manuscript. JD
and GW interpreted the data. XD conceived and designed the study.
All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of Union Hospital, Tongji Medical College, HUST (China).
All procedures performed in studies involving human participants
were in accordance with the ethical standards of the institutional
and/or national research committee and with the 1964 Declaration of
Helsinki and its later amendments or comparable ethical standards.
Informed consent was obtained from all individual participants
included in the study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chen W, Zheng R, Zeng H and Zhang S:
Epidemiology of lung cancer in China. Thorac Cancer. 6:209–215.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ettinger DS, Akerley W, Bepler G, Chang A,
Cheney RT, Chirieac LR, D'Amico TA, Demmy TL, Feigenberg SJ, Figlin
RA, et al: Non-small cell lung cancer. J Natl Compr Canc Netw.
6:228–269. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Molina JR, Yang P, Cassivi SD, Schild SE
and Adjei AA: Non-small cell lung cancer: Epidemiology, risk
factors, treatment, and survivorship. Mayo Clin Proc. 83:584–594.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Schiller JH, Harrington D, Belani CP,
Langer C, Sandler A, Krook J, Zhu J and Johnson DH; Eastern
Cooperative Oncology Group, : Comparison of four chemotherapy
regimens for advanced non-small-cell lung cancer. N Engl J Med.
346:92–98. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Bria E, Milella M, Cuppone F, Novello S,
Ceribelli A, Vaccaro V, Sperduti I, Gelibter A, Scagliotti GV,
Cognetti F and Giannarelli D: Outcome of advanced NSCLC patients
harboring sensitizing EGFR mutations randomized to EGFR tyrosine
kinase inhibitors or chemotherapy as first-line treatment: A
meta-analysis. Ann Oncol. 22:2277–2285. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Loong HH, Kwan SS, Mok TS and Lau YM:
Therapeutic strategies in EGFR mutant non-small cell lung cancer.
Curr Treat Options Oncol. 19:582018. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Mok TS, Wu YL, Thongprasert S, Yang CH,
Chu DT, Saijo N, Sunpaweravong P, Han B, Margono B, Ichinose Y, et
al: Gefitinib or carboplatin-paclitaxel in pulmonary
adenocarcinoma. N Engl J Med. 361:947–957. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Han JY, Park K, Kim SW, Lee DH, Kim HY,
Kim HT, Ahn MJ, Yun T, Ahn JS, Suh C, et al: First-SIGNAL:
First-line single-agent iressa versus gemcitabine and cisplatin
trial in non-smokers with adenocarcinoma of the lung. J Clin Oncol.
30:1122–1128. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Maemondo M, Inoue A, Kobayashi K, Sugawara
S, Oizumi S, Isobe H, Gemma A, Harada M, Yoshizawa H, Kinoshita I,
et al: Gefitinib or chemotherapy for non-small-cell lung cancer
with mutated EGFR. N Engl J Med. 362:2380–2388. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Mitsudomi T, Morita S, Yatabe Y, Negoro S,
Okamoto I, Tsurutani J, Seto T, Satouchi M, Tada H, Hirashima T, et
al: Gefitinib versus cisplatin plus docetaxel in patients with
non-small-cell lung cancer harbouring mutations of the epidermal
growth factor receptor (WJTOG3405): An open label, randomised phase
3 trial. Lancet Oncol. 11:121–128. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Rosell R, Carcereny E, Gervais R,
Vergnenegre A, Massuti B, Felip E, Palmero R, Garcia-Gomez R,
Pallares C, Sanchez JM, et al: Erlotinib versus standard
chemotherapy as first-line treatment for European patients with
advanced EGFR mutation-positive non-small-cell lung cancer
(EURTAC): A multicentre, open-label, randomised phase 3 trial. The
Lancet. Oncology. 13:239–246. 2012.PubMed/NCBI
|
|
13
|
Zhou C, Wu YL, Chen G, Feng J, Liu XQ,
Wang C, Zhang S, Wang J, Zhou S, Ren S, et al: Erlotinib versus
chemotherapy as first-line treatment for patients with advanced
EGFR mutation-positive non-small-cell lung cancer (OPTIMAL,
CTONG-0802): A multicentre, open-label, randomised, phase 3 study.
Lancet. Oncol. 12:735–742. 2011.
|
|
14
|
Xue C, Hu Z, Jiang W, Zhao Y, Xu F, Huang
Y, Zhao H, Wu J, Zhang Y, Zhao L, et al: National survey of the
medical treatment status for non-small cell lung cancer (NSCLC) in
China. Lung Cancer. 77:371–375. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gazdar AF: Activating and resistance
mutations of EGFR in non-small-cell lung cancer: Role in clinical
response to EGFR tyrosine kinase inhibitors. Oncogene. 28 (Suppl
1):S24–S31. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Jackman DM, Miller VA, Cioffredi LA, Yeap
BY, Jänne PA, Riely GJ, Ruiz MG, Giaccone G, Sequist LV and Johnson
BE: Impact of epidermal growth factor receptor and KRAS mutations
on clinical outcomes in previously untreated non-small cell lung
cancer patients: Results of an online tumor registry of clinical
trials. Clin Cancer Res. 15:5267–5273. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Gold P and Freedman SO: Demonstration of
tumor-specific antigens in human colonic carcinomata by
immunological tolerance and absorption techniques. J Exp Med.
121:439–462. 1965. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Fiala O, Pesek M, Finek J, Benesova L,
Minarik M, Bortlicek Z and Topolcan O: Predictive role of CEA and
CYFRA 21-1 in patients with advanced-stage NSCLC treated with
erlotinib. Anticancer Res. 34:3205–3210. 2014.PubMed/NCBI
|
|
19
|
Yang ZM, Ding XP, Pen L, Mei L and Liu T:
Analysis of CEA expression and EGFR mutation status in non-small
cell lung cancers. Asian Pac J Cancer Prev. 15:3451–3455. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Qin HF, Qu LL, Liu H, Wang SS and Gao HJ:
Serum CEA level change and its significance before and after
Gefitinib therapy on patients with advanced non-small cell lung
cancer. Asian Pac J Cancer Prev. 14:4205–4208. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Muley T, Dienemann H and Ebert W: CYFRA
21-1 and CEA are independent prognostic factors in 153 operated
stage I NSCLC patients. Anticancer Res. 24:1953–1956.
2004.PubMed/NCBI
|
|
22
|
Barlesi F, Gimenez C, Torre JP, Doddoli C,
Mancini J, Greillier L, Roux F and Kleisbauer JP: Prognostic value
of combination of Cyfra 21-1, CEA and NSE in patients with advanced
non-small cell lung cancer. Respir Med. 98:357–362. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Molina R, Filella X, Auge JM, Fuentes R,
Bover I, Rifa J, Moreno V, Canals E, Viñolas N, Marquez A, et al:
Tumor markers (CEA, CA 125, CYFRA 21-1, SCC and NSE) in patients
with non-small cell lung cancer as an aid in histological diagnosis
and prognosis. Comparison with the main clinical and pathological
prognostic factors. Tumour Bio. 24:209–218. 2003. View Article : Google Scholar
|
|
24
|
Tomita M, Shimizu T, Ayabe T and Onitsuka
T: Maximum SUV on positron emission tomography and serum CEA level
as prognostic factors after curative resection for non-small cell
lung cancer. Asia Pac J Clin Oncol. 8:244–247. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Chiu CH, Shih YN, Tsai CM, Liou JL, Chen
YM and Perng RP: Serum tumor markers as predictors for survival in
advanced non-small cell lung cancer patients treated with
gefitinib. Lung Cancer. 57:213–221. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ko KH, Hsu HH, Huang TW, Gao HW, Shen DH,
Chang WC, Hsu YC, Chang TH, Chu CM, Ho CL and Chang H: Value of
18F-FDG uptake on PET/CT and CEA level to predict
epidermal growth factor receptor mutations in pulmonary
adenocarcinoma. Eur J Nucl Med Mol Imaging. 41:1889–1897. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Lardinois D, Weder W, Hany TF, Kamel EM,
Korom S, Seifert B, von Schulthess GK and Steinert HC: Staging of
nonsmall-cell lung cancer with integrated positron-emission
tomography and computed tomography. N Engl J Med. 348:2500–2507.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Sasaki R, Komaki R, Macapinlac H, Erasmus
J, Allen P, Forster K, Putnam JB, Herbst RS, Moran CA, Podoloff DA,
et al: [18F]fluorodeoxyglucose uptake by positron emission
tomography predicts outcome of non-small-cell lung cancer. J Clin
Onco. 23:1136–1143. 2005. View Article : Google Scholar
|
|
29
|
Hoang JK, Hoagland LF, Coleman RE, Coan
AD, Herndon JE II and Patz EF Jr: Prognostic value of fluorine-18
fluorodeoxyglucose positron emission tomography imaging in patients
with advanced-stage non-small-cell lung carcinoma. J Clin Oncol.
26:1459–1464. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Caicedo C, Garcia-Velloso MJ, Lozano MD,
Labiano T, Vigil Diaz C, Lopez-Picazo JM, Gurpide A, Zulueta JJ,
Richter Echevarria JA and Perez Gracia JL: Role of
[18F]FDG PET in prediction of KRAS and EGFR mutation
status in patients with advanced non-small-cell lung cancer. Eur J
Nucl Med Mol Imaging. 41:2058–2065. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Edge SB and Compton CC: The American Joint
Committee on Cancer: The 7th edition of the AJCC cancer staging
manual and the future of TNM. Ann Surg Oncol. 17:1471–1474. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Lan XL, Zhang YX, Wu ZJ, Jia Q, Wei H and
Gao ZR: The value of dual time point (18)F-FDG PET imaging for the
differentiation between malignant and benign lesions. Clin Radiol.
63:756–764. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Wang Y, Chiu E, Rosenberg J and Gambhir
SS: Standardized uptake value atlas: Characterization of
physiological 2-deoxy-2-[18F]fluoro-D-glucose uptake in normal
tissues. Mol Imaging Biol. 9:83–90. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Higashi K, Ueda Y, Ayabe K, Sakurai A,
Seki H, Nambu Y, Oguchi M, Shikata H, Taki S, Tonami H, Katsuda S
and Yamamoto I: FDG PET in the evaluation of the aggressiveness of
pulmonary adenocarcinoma: Correlation with histopathological
features. Nucl Med Commun. 21:707–714. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Vesselle H, Schmidt RA, Pugsley JM, Li M,
Kohlmyer SG, Vallires E and Wood DE: Lung cancer proliferation
correlates with [F-18] fluorodeoxyglucose uptake by positron
emission tomography. Clin Cancer Res. 6:3837–3844. 2000.PubMed/NCBI
|
|
36
|
Song JY, Lee YN, Kim YS, Kim SG, Jin SJ,
Park JM, Choi GS, Chung JC, Lee MH, Cho YH, et al: Predictability
of preoperative 18F-FDG PET for histopathological differentiation
and early recurrence of primary malignant intrahepatic tumors. Nucl
Med Commun. 36:319–327. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Ahn SJ, Park MS, Lee JD and Kang WJ:
Correlation between 18F-fluorodeoxyglucose positron emission
tomography and pathologic differentiation in pancreatic cancer. Ann
Nucl Med. 28:430–435. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Purandare NC, Puranik A, Shah S, Agrawal
A, Gupta T, Moiyadi A, Shetty P, Shridhar E, Jalali R and
Rangarajan V: Common malignant brain tumors: Can 18F-FDG PET/CT aid
in differentiation? Nucl Med Commun. 38:1109–1116. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Herbst RS: Review of epidermal growth
factor receptor biology. Int J Radiat Oncol Biol Phys. 59:21–26.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Shi Y, Au JS, Thongprasert S, Srinivasan
S, Tsai CM, Khoa MT, Heeroma K, Itoh Y, Cornelio G and Yang PC: A
prospective, molecular epidemiology study of EGFR mutations in
Asian patients with advanced non-small-cell lung cancer of
adenocarcinoma histology (PIONEER). J Thorac Oncol. 9:154–162.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Dearden S, Stevens J, Wu YL and Blowers D:
Mutation incidence and coincidence in non small-cell lung cancer:
Meta-analyses by ethnicity and histology (mutMap). Ann Oncol.
24:2371–2376. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Pao W and Girard N: New driver mutations
in non-small-cell lung cancer. Lancet Oncol. 12:175–180. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Putora PM, Fruh M and Muller J: FDG-PET
SUV-max values do not correlate with epidermal growth factor
receptor mutation status in lung adenocarcinoma. Respirology.
18:734–735. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Huang CT, Yen RF, Cheng MF, Hsu YC, Wei
PF, Tsai YJ, Tsai MF, Shih JY, Yang CH and Yang PC: Correlation of
F-18 fluorodeoxyglucose-positron emission tomography maximal
standardized uptake value and EGFR mutations in advanced lung
adenocarcinoma. Med Oncol. 27:9–15. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Mak RH, Digumarthy SR, Muzikansky A,
Engelman JA, Shepard JA, Choi NC and Sequist LV: Role of
18F-fluorodeoxyglucose positron emission tomography in predicting
epidermal growth factor receptor mutations in non-small cell lung
cancer. Oncologist. 16:319–326. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Choi YJ, Cho BC, Jeong YH, Seo HJ, Kim HJ,
Cho A, Lee JH, Yun M, Jeon TJ, Lee JD and Kang WJ: Correlation
between (18F)-fluorodeoxyglucose uptake and epidermal growth factor
receptor mutations in advanced lung cancer. Nuclear Medicine
Molecular Imaging. 46:169–175. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Lee EY, Khong PL, Lee VH, Qian W, Yu X and
Wong MP: Metabolic phenotype of stage IV lung adenocarcinoma:
Relationship with epidermal growth factor receptor mutation. Clin
Nucl Med. 40:e190–e195. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Cho A, Hur J, Moon YW, Hong SR, Suh YJ,
Kim YJ, Im DJ, Hong YJ, Lee HJ, Kim YJ, et al: Correlation between
EGFR gene mutation, cytologic tumor markers, 18F-FDG uptake in
non-small cell lung cancer. BMC Cancer. 16:2242016. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Zhang XT, Li LY, Mu XL, Cui QC, Chang XY,
Song W, Wang SL, Wang MZ, Zhong W and Zhang L: The EGFR mutation
and its correlation with response of gefitinib in previously
treated Chinese patients with advanced non-small-cell lung cancer.
Ann Oncol. 16:1334–1342. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Faehling M, Achenbach J, Staib P, Steffen
U, Tessen HW, Gaillard VE and Brugger W: Erlotinib in routine
clinical practice for first-line maintenance therapy in patients
with advanced non-small cell lung cancer (NSCLC). J Cancer Res Clin
Oncol. 144:1375–1383. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Kobayashi K and Hagiwara K: Epidermal
growth factor receptor (EGFR) mutation and personalized therapy in
advanced nonsmall cell lung cancer (NSCLC). Target Oncol. 8:27–33.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Sequist LV, Martins RG, Spigel D, Grunberg
SM, Spira A, Jänne PA, Joshi VA, McCollum D, Evans TL, Muzikansky
A, et al: First-line gefitinib in patients with advanced
non-small-cell lung cancer harboring somatic EGFR mutations. J Clin
Oncol. 26:2442–2449. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Chen ZY, Zhong WZ, Zhang XC, Su J, Yang
XN, Chen ZH, Yang JJ, Zhou Q, Yan HH, An SJ, et al: EGFR mutation
heterogeneity and the mixed response to EGFR tyrosine kinase
inhibitors of lung adenocarcinomas. Oncologist. 17:978–985. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Wang WT, Li Y, Ma J, Chen XB and Qin JJ:
Serum carcinoembryonic antigen levels before initial treatment are
associated with EGFR mutations and EML4- ALK fusion gene in lung
adenocarcinoma patients. Asian Pac J Cancer Prev. 15:3927–3932.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Vincent RG, Chu TM, Fergen TB and
Ostrander M: Carcinoembryonic antigen in 228 patients with
carcinoma of the lung. Cancer. 36:2069–2076. 1975. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Vincent RG, Chu TM and Lane WW: The value
of carcinoembryonic antigen in patients with carcinoma of the lung.
Cancer. 44:685–691. 1979. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Yang ZM, Ding XP, Pen L, Mei L and Liu T:
Analysis of CEA expression and EGFR mutation status in non-small
cell lung cancers. Asian Pac J Cancer Prev. 15:3451–3455. 2014.
View Article : Google Scholar : PubMed/NCBI
|