Introduction
Breast cancer is the most common type of malignancy
in females and >90% of mortalities are due to
metastasis-associated complications (1). An estimated 5–10% of patients have
metastasis at the time-point of diagnosis and 20–40% of those who
did not have any metastasis at the time-point of diagnosis
eventually experience recurrence after treatment and metastasis;
once recurrence and metastasis occur, the overall prognosis is
generally poor (2,3).
The status of hormone receptors (HRs) is closely
linked to the treatment and prognosis of breast cancer. Certain
studies have explored the association between molecular subtypes
and sentinel lymph node metastasis and risk factors of metastasis
(4–14). However, breast cancer is a highly
heterogeneous disease at the molecular level and the metastatic
behavior of different subtypes of breast cancer, including
metastatic sites and the number of metastases, as well as the
prognosis difference between primary and metastatic breast cancer
patients of different subtypes, have remained to be fully
defined.
In the present study, the possible association
between molecular subtypes and metastatic behavior was
retrospectively explored in a single-center sample of 166 patients
with metastatic breast cancer from Hunan Provincial People's
Hospital (Changsha, China) between January 2012 and December 2018,
and the results were further supported by analysis of a large
dataset from the Surveillance, Epidemiology, and End Results (SEER)
database with 15,322 cases of metastatic breast cancer among
329,770 patients with primary breast cancer. Furthermore,
differences in prognosis regarding overall survival (OS) of
patients with primary and with metastatic breast cancer with
different molecular subtypes were determined. The results of the
present study may be valuable to inform improved monitoring for
metastasis sites during follow-up. An understanding of the patterns
of metastatic spread will allow the clinician to make more
efficient surveillance decisions and select appropriate
examinations and therapies.
Materials and methods
Patients
The present study was a retrospective analysis.
First, 166 patients with metastatic breast cancer treated at Hunan
Provincial People's Hospital (Changsha, China) between January 2012
and December 2018 were collected. All patients underwent primary
tumor resection and the tumors were pathologically confirmed as
breast cancer. The age at diagnosis was 25–79 years. Each patient
included had a complete medical record and preserved pathological
specimens. The study protocol was approved by the Ethics Committee
of Hunan Provincial People's Hospital and The First Affiliated
Hospital of Hunan Normal University (Changsha, China).
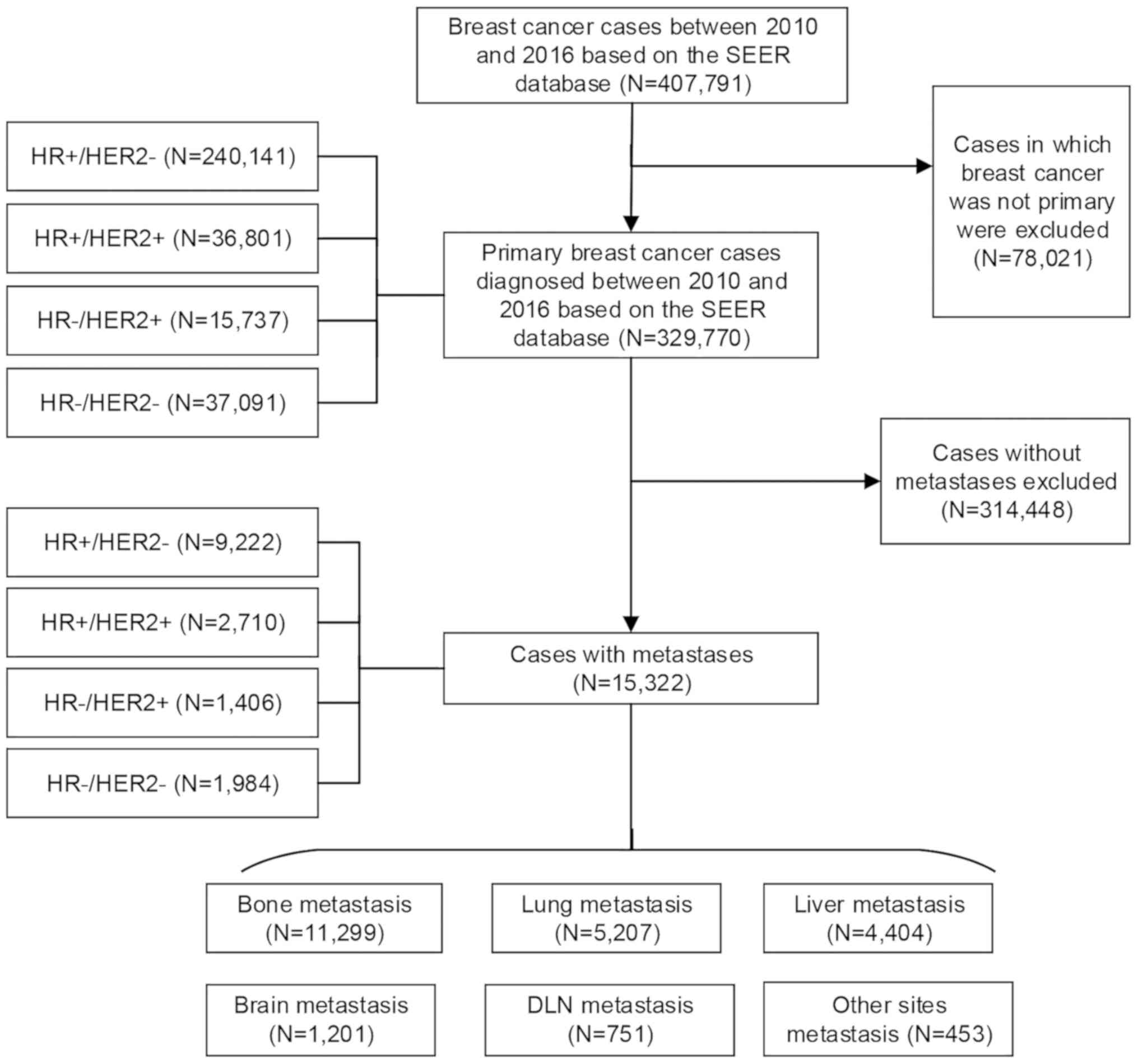
Furthermore, data were extracted from the SEER
database (https://seer.cancer.gov/) on 407,791
patients who were diagnosed with malignant breast cancer between
2010 and 2016 and had known HR and human epidermal growth factor
receptor 2 (HER2) statuses. After excluding non-primary breast
cancer cases, there were 329,770 primary breast cancer patients, of
which 15,322 cases had metastatic breast cancer. The number of
HR+/HER2− metastatic cases was 9,222, compared with 2,710 HR+/HER2+
metastatic cases, 1,406 HR-/HER2+ metastatic cases and 1,984
HR-/HER2- metastatic cases. Bone metastasis was present in 11,299
cases, as compared with 5,207 cases with lung metastasis, 4,404
with liver metastasis, 1,201 with brain metastasis and 751 with
distant lymph node (DLN) metastasis, as well as 453 cases that
involved other metastatic sites (Fig.
1).
Characterization of specimens
Tumor specimen samples were processed by routine
detection methods. First, tumor samples were fixed, after which
they were consecutively sliced to a thickness of 4 µm and then
stained with H&E, followed by immunohistochemistry (IHC)
staining. Fluorescence in situ hybridization (FISH) was
performed when necessary. After staining, the HR and HER2 statuses
of all specimens were assessed by two senior pathologists based on
the same criteria as those used by the hospital.
For evaluation, the following specific standards
were used: A total of 5 high-power fields were randomly selected to
count >500 cells and the number of positive cells and staining
intensity were used for scoring. Samples were considered HR+ if
>1% of cells exhibited IHC staining (15). HER2 expression was only present on
the cell membrane or in the cell plasma, and samples scored 3+
(overexpression) via IHC were classified as HER2+. For those
samples scoring as HER2 1–2+, 2+ and 2–3+ on IHC, FISH was further
performed by hybridization of fluorescent DNA probes to the HER2
gene and chromosome 17. The result was considered HER2+ status when
the HER2/centromeric probe for chromosome 17 (Cep17) ratio was ≥2
on average for 60 cells and detection of gene amplification was
interpreted as HER2+ status (16).
Study design
The patients were divided into four groups according
to molecular subtypes: HR+/HER2−, HR+/HER2+, HR-/HER2+ and
HR-/HER2-. First, 166 patients with metastatic breast cancer with
HR and HER2 expression data were assessed. The associations between
molecular subtypes and the sites of and the number of metastases
were examined.
Furthermore, 15,322 metastatic cases among 329,770
patients with primary breast cancer from the SEER database were
analyzed. The possible impact of molecular subtypes on the sites
and number of metastases was studied based on data from the SEER
database. In addition, the possible impact of molecular subtypes on
the OS of patients with primary and with metastatic breast cancer
was evaluated. OS was defined as the time from the date of
diagnosis to death from any cause.
Statistical analysis
All data were analyzed by using SPSS version 22.0
(IBM Corp.), where ratio variables were compared using the
χ2 test or Fisher's exact test as appropriate. Survival
rates were calculated with the Kaplan-Meier method and survival
curves were drawn. The log-rank test was performed to perform
univariate analysis. The statistical analyses were two-sided and
P<0.05 was considered to indicate statistical significance.
Results
Major characteristics of patients with
different molecular subtypes of breast cancer
A total of 166 patients with metastatic breast
cancer from the Hunan Provincial People's Hospital (Changsha,
China) and 15,322 metastatic breast cancer cases from the SEER
database were identified. The major baseline features of the breast
cancer molecular subtypes are presented in Tables I and II. In 166 patients with metastases, the
HR+/HER2−, HR+/HER2+, HR-/HER2+ and HR-/HER2- cases accounted for
55.4, 15.7, 12.6 and 16.3%, respectively; all of the patients were
female, with a mean age of 51.4 years (range, 25–79 years). For the
15,322 metastatic breast cancer cases from the SEER database, the
mean age was 60.7 years (range, 19–103 years); the HR+/HER2−,
HR+/HER2+, HR-/HER2+ and HR-/HER2- cases accounted for 60.2, 17.7,
9.2 and 12.9%, respectively. In both datasets, HR+/HER2− accounted
for the largest proportion of molecular subtypes, while HR-/HER2+
had the smallest proportion. There was no statistically significant
difference in the proportion of molecular subtypes between the two
datasets (P=0.196; Table III).
 | Table I.Major characteristics of the patients
with metastatic breast cancer from the present cohort study
(n=166). |
Table I.
Major characteristics of the patients
with metastatic breast cancer from the present cohort study
(n=166).
| Main
characteristics | HR+/HER2− (n=92) | HR+/HER2+ (n=26) | HR-/HER2+ (n=21) | HR-/HER2- (n=27) |
|---|
| Age (years) |
|
<40 | 19 (20.6) | 5 (19.2) | 2 (9.5) | 1 (3.7) |
|
40-49 | 26 (28.3) | 8 (30.8) | 3 (14.3) | 9 (33.3) |
|
50-59 | 26 (28.3) | 6 (23.1) | 9 (42.9) | 11 (40.8) |
|
≥60 | 21 (22.8) | 7 (26.9) | 7 (33.3) | 6 (22.2) |
| Menopausal
status |
|
|
|
|
|
Premenopause | 41 (44.6) | 12 (46.2) | 5 (23.8) | 9 (33.3) |
|
Postmenopause | 51 (55.4) | 14 (53.8) | 16 (76.2) | 18 (66.7) |
| Tumor stage |
|
|
|
|
| T1 | 9 (9.8) | 5 (19.2) | 4 (19.1) | 8 (29.6) |
| T2 | 55 (59.8) | 11 (42.3) | 8 (38.1) | 15 (55.6) |
| T3 | 18 (19.6) | 9 (34.6) | 7 (33.3) | 3 (11.1) |
| T4 | 10 (10.8) | 1 (3.9) | 2 (9.5) | 1 (3.7) |
| TNM stage |
|
|
|
|
| I | 7 (7.6) | 4 (15.4) | 0 (0) | 3 (11.1) |
| II | 34 (37.0) | 7 (26.9) | 6 (28.6) | 12 (44.4) |
|
III | 51 (55.4) | 15 (57.7) | 15 (71.4) | 12 (44.4) |
| Lymph node
status |
|
|
|
|
|
Positive | 65 (70.7) | 19 (73.1) | 19 (90.5) | 16 (59.3) |
|
Negative | 27 (29.3) | 7 (26.9) | 2 (9.5) | 11 (40.7) |
| Histopathological
type |
|
|
|
|
|
Invasive ductal carcinoma | 75 (81.5) | 23 (88.5) | 18 (85.7) | 25 (92.6) |
|
Invasive lobular
carcinoma | 4 (4.3) | 0 (0) | 0 (0) | 1 (3.7) |
| Ductal
carcinoma in situ | 2 (2.2) | 2 (7.7) | 1 (4.8) | 0 (0) |
|
Other | 11 (12.0) | 1 (3.8) | 2 (9.5) | 1 (3.7) |
| Table II.Major characteristics of patients
with metastatic breast cancer from the Surveillance, Epidemiology
and End Results dataset (n=15,322). |
Table II.
Major characteristics of patients
with metastatic breast cancer from the Surveillance, Epidemiology
and End Results dataset (n=15,322).
| Main
characteristics | HR+/HER2−
(n=9,222) | HR+/HER2+
(n=2,710) | HR-/HER2+
(n=1,406) | HR-/HER2-
(n=1,984) |
|---|
| Age (years) |
|
|
|
|
|
<40 | 553 (6.0) | 298 (11.0) | 169 (12.0) | 160 (8.1) |
|
40-49 | 1,193 (12.9) | 430 (15.9) | 227 (16.2) | 289 (14.6) |
|
50-59 | 2,178 (23.6) | 765 (28.2) | 411 (29.2) | 512 (25.8) |
|
≥60 | 5298 (57.5) | 1,217 (44.9) | 599 (42.6) | 1,023 (51.5) |
| Sex |
|
|
|
|
|
Female | 9,107 (98.8) | 2,673 (98.6) | 1,403 (99.8) | 1969 (99.2) |
|
Male | 115 (1.2) | 37 (1.4) | 3 (0.2) | 15 (0.8) |
| Tumor stage |
|
|
|
|
| T0 | 110 (1.2) | 23 (0.8) | 15 (1.1) | 26 (1.3) |
| T1 | 819 (8.9) | 224 (8.3) | 99 (7.0) | 133 (6.7) |
| T2 | 2,287 (24.8) | 668 (24.6) | 278 (19.8) | 416 (21.0) |
| T3 | 1,188 (12.9) | 345 (12.7) | 190 (13.5) | 301 (15.2) |
| T4 | 2,244 (24.3) | 713 (26.3) | 449 (31.9) | 617 (31.1) |
|
Unknown | 2,574 (27.9) | 737 (27.3) | 375 (26.7) | 491 (24.7) |
| Lymph node
status |
|
|
|
|
|
Positive | 8,919 (96.7) | 2,563 (94.6) | 1,296 (92.2) | 1,819 (91.7) |
|
Negative | 303 (3.3) | 147 (5.4) | 110 (7.8) | 165 (8.3) |
| Grade |
|
|
|
|
| I | 894 (9.7) | 62 (2.3) | 7 (0.5) | 23 (1.2) |
| II | 3,855 (41.8) | 891 (32.9) | 310 (22.0) | 296 (14.9) |
|
III | 2,604 (28.2) | 1,326 (48.9) | 839 (59.7) | 1,333 (67.2) |
| IV | 34 (0.4) | 16 (0.6) | 11 (0.8) | 25 (1.3) |
|
Unknown | 1,835 (19.9) | 415 (15.3) | 239 (17.0) | 307 (15.4) |
| Radiation
therapy |
|
|
|
|
| Prior
to surgery | 146 (1.6) | 37 (1.4) | 20 (1.4) | 22 (1.1) |
| After
surgery | 1,343 (14.6) | 409 (15.1) | 209 (14.9) | 315 (15.9) |
| Prior
to and after surgery | 39 (0.4) | 8 (0.3) | 7 (0.5) | 7 (0.4) |
|
None | 7,678 (83.3) | 2,250 (83.0) | 1,166 (82.9) | 1,636 (82.4) |
|
Other | 16 (0.1) | 6 (0.2) | 4 (0.3) | 4 (0.2) |
| Chemotherapy |
|
|
|
|
| No | 5,058 (54.8) | 748 (27.6) | 288 (20.5) | 553 (27.9) |
|
Yes | 4,164 (45.2) | 1,962 (72.4) | 1,118 (79.5) | 1,431 (72.1) |
| Table III.Similarities and differences of
molecular subtypes between the two datasets. |
Table III.
Similarities and differences of
molecular subtypes between the two datasets.
| Molecular
subtype |
Single-centerdataset (n=166) | Surveillance,
Epidemiology and End Results dataset (n=15,322) | χ2 | P-value |
|---|
| HR+/HER2− | 92 (55.4) | 9,222 (60.2) | 4.605 | 0.196 |
| HR+/HER2+ | 26 (15.7) | 2,710 (17.7) |
|
|
| HR-/HER2+ | 21 (12.6) | 1,406 (9.2) |
|
|
| HR-/HER2− | 27 (16.3) | 1,984 (12.9) |
|
|
Molecular subtypes and distribution of
metastatic sites in the two datasets
Among the 166 cases of the present single-center
study, the molecular subtypes were significantly associated with
the prevalence of DLN metastasis (P=0.010), but not significantly
associated with the prevalence of any other sites of metastasis.
Bone metastasis was more common in the HR+/HER2+ and HR-/HER2+
subtypes compared to the other subtypes and their rates of
occurrence were 50.0 and 42.9%, respectively. Lung metastasis was
more common in the HR+/HER2− and HR-/HER2+ subtypes, and their
rates of occurrence were 23.9 and 23.8% respectively; furthermore,
pleural metastasis was more common in the HR+/HER2− and
HR-/HER2-subtypes, and their rates of occurrence were 19.6 and
18.5%, respectively. Liver metastasis was more common in the
HR-/HER2+ and HR+/HER2+ subtypes and their rates of occurrence were
33.3 and 30.8%, respectively. Brain metastasis was more common in
the HR+/HER2+ and HR+/HER2− subtypes and their rates of occurrence
were 11.5 and 5.4% respectively; DLN metastasis was also more
common in the HR-/HER2- and HR-/HER2+ subtypes and their rates of
occurrence were 44.4 and 23.8%, respectively (Table IV).
| Table IV.Molecular subtypes and metastatic
sites in the patients with metastatic breast cancer from the
present cohort study (n=166). |
Table IV.
Molecular subtypes and metastatic
sites in the patients with metastatic breast cancer from the
present cohort study (n=166).
| Metastatic
site | HR+/HER2−
(n=92) | HR+/HER2+
(n=26) | HR-/HER2+
(n=21) | HR-/HER2-
(n=27) | P-value |
|---|
| Bone |
|
|
|
| 0.165 |
|
Metastasis | 31 (33.7) | 13 (50.0) | 9 (42.9) | 6 (22.2) |
|
| No
metastasis | 61 (66.3) | 13 (50.0) | 12 (57.1) | 21 (77.8) |
|
| Lung |
|
|
|
| 0.779 |
|
Metastasis | 22 (23.9) | 4 (15.4) | 5 (23.8) | 5 (18.5) |
|
| No
metastasis | 70 (76.1) | 22 (84.6) | 16 (76.2) | 22 (81.5) |
|
| Pleural |
|
|
|
| 0.330 |
|
Metastasis | 15 (19.6) | 1 (3.8) | 2 (9.5) | 5 (18.5) |
|
| No
metastasis | 77 (80.4) | 25 (96.2) | 19 (90.5) | 22 (81.5) |
|
| Liver |
|
|
|
| 0.438 |
|
Metastasis | 18 (19.6) | 8 (30.8) | 7 (33.3) | 6 (22.2) |
|
| No
metastasis | 74 (80.4) | 18 (69.2) | 14 (66.7) | 21 (77.8) |
|
| Brain |
|
|
|
| 0.425 |
|
Metastasis | 5 (5.4) | 3 (11.5) | 0 (0.0) | 1 (3.7) |
|
| No
metastasis | 87 (94.6) | 23 (88.5) | 21 (100.0) | 26 (96.3) |
|
| DLN |
|
|
|
| 0.010 |
|
Metastasis | 18 (19.6) | 2 (7.7) | 5 (23.8) | 12 (44.4) |
|
| No
metastasis | 74 (80.4) | 24 (92.3) | 16 (76.2) | 15 (55.6) |
|
Among the 15,322 metastatic cases from the SEER
database, the metastasis sites were significantly different among
the different molecular subtypes (bone, lung, liver, brain and DLN;
P<0.001). Bone metastasis was more common in the HR+/HER2− and
HR+/HER2+ than in the other subgroups, with rates of occurrence of
82.0 and 71.3%, respectively. Lung metastasis was more common in
the HR-/HER2+ and HR-/HER2- subtypes and the rates of occurrence
were 40.8 and 47.7%, respectively. Liver metastasis was more common
in the HR-/HER2+ and HR+/HER2+ subtypes, with rates of occurrence
of 51.6 and 39.2%, respectively; brain metastasis was more common
in the HR-/HER2+ and HR-/HER2- subtypes and the rates of occurrence
were 12.7 and 12.9%, respectively. DLN metastasis was more common
in the HR-/HER2- and HR-/HER2+ subtypes, with rates of occurrence
of 6.4 and 6.9%, respectively (Table
V).
| Table V.Molecular subtypes and metastatic
sites in patients with metastatic breast cancer from the
Surveillance, Epidemiology and End Results dataset (n=15,322). |
Table V.
Molecular subtypes and metastatic
sites in patients with metastatic breast cancer from the
Surveillance, Epidemiology and End Results dataset (n=15,322).
| Metastatic
sites | HR+/HER2−
(n=9,222) | HR+/HER2+
(n=2,710) | HR-/HER2+
(n=1,406) | HR-/HER2-
(n=1,984) | P-value |
|---|
| Bone |
|
|
|
| <0.001 |
|
Metastasis | 7,563 (82.0) | 1,931 (71.3) | 762 (54.2) | 1,043 (52.6) |
|
| No
metastasis | 1,659 (18.0) | 779 (28.7) | 644 (45.8) | 941 (47.4) |
|
| Lung |
|
|
|
| <0.001 |
|
Metastasis | 2,787 (30.2) | 901 (33.2) | 573 (40.8) | 946 (47.7) |
|
| No
metastasis | 6,435 (69.8) | 1,809 (66.8) | 833 (59.2) | 1,038 (52.3) |
|
| Liver |
|
|
|
| <0.001 |
|
Metastasis | 1,965 (21.3) | 1,062 (39.2) | 726 (51.6) | 651 (32.8) |
|
| No
metastasis | 7,257 (78.7) | 1,648 (60.8) | 680 (48.4) | 1,333 (67.2) |
|
| Brain |
|
|
|
| <0.001 |
|
Metastasis | 542 (5.9) | 226 (8.3) | 178 (12.7) | 255 (12.9) |
|
| No
metastasis | 8,680 (94.1) | 2,484 (91.7) | 1,228 (87.3) | 1,729 (87.1) |
|
| DLN |
|
|
|
| <0.001 |
|
Metastasis | 363 (3.9) | 165 (6.1) | 97 (6.9) | 126 (6.4) |
|
| No
metastasis | 8,859 (96.1) | 2,545 (93.9) | 1,309 (93.1) | 1,858 (93.6) |
|
In summary, bone metastasis was more likely to occur
in the HR+/HER2+ subtype patients according to the single-center
data as well as the dataset from the SEER database. Lung metastasis
was more likely to occur in patients of the HR-/HER2+ subtype in
both datasets. Liver metastasis was more likely to occur in the
HR-/HER2+ and HR+/HER2+ patients in both datasets. DLN metastasis
was more likely to occur in the HR-/HER2- and HR-/HER2+ patients in
both datasets.
Molecular subtypes and the number of
metastatic sites in both datasets
In the 166 cases from the single-center cohort,
molecular subtypes were not significantly associated with the
prevalence of the number of metastatic sites (P=0.221). A single
site of metastasis was more frequent in the HR+/HER2− and HR-/HER2+
patients than in the other subgroups, with frequencies of 59.8 and
57.1%, respectively. Furthermore, two sites of metastasis were more
common in the HR-/HER2- and HR+/HER2+ patients and the rates of
occurrence were 37.0 and 30.8%, respectively. In addition, three
sites of metastasis were more frequent in HR+/HER2+ and
HR+/HER2−patients, with rates of occurrence of 19.2 and 10.9%,
respectively. Finally, ≥4 sites of metastasis were more frequent in
the HR-/HER2- and HR-/HER2+ subtypes and the rates of occurrence
were 14.8 and 14.3%, respectively (Table VI).
| Table VI.Molecular subtypes and the number of
metastatic sites in patients with metastatic breast cancer from the
present cohort study (n=166). |
Table VI.
Molecular subtypes and the number of
metastatic sites in patients with metastatic breast cancer from the
present cohort study (n=166).
| Number of
metastatic sites | HR+/HER2−
(n=92) | HR+/HER2+
(n=26) | HR-/HER2+
(n=21) | HR-/HER2-
(n=27) | χ2 | P-value |
|---|
| 1 | 55 (59.8) | 12 (46.2) | 12 (57.1) | 13 (48.2) | 11.328 | 0.221 |
| 2 | 20 (21.7) | 8 (30.8) | 4 (19.1) | 10 (37.0) |
|
|
| 3 | 10 (10.9) | 5 (19.2) | 2 (9.5) | 0 (0) |
|
|
| ≥4 | 7 (7.6) | 1 (3.8) | 3 (14.3) | 4 (14.8) |
|
|
Among the 15,322 metastatic cases from the SEER
database, the molecular subtypes were significantly associated with
the prevalence of the number of metastatic sites (P<0.001). A
single site of metastasis was more common in the HR+/HER2− and
HR-/HER2- patients than in the other subgroups, with rates of
occurrence of 65.5 and 60.5%, respectively. Furthermore, two sites
of metastasis were more frequent in the HR+/HER2+ and HR-/HER2+
patients and the rates of occurrence were 28.6 and 28.4%,
respectively. In addition, three sites of metastasis were more
common in the HR-/HER2+ and HR+/HER2+ subtypes, with rates of
occurrence of 13.0 and 11.5%, respectively. Finally, ≥4 sites of
metastasis were more common for the HR-/HER2+ and HR-/HER2-subtypes
(4.5 and 3.5%, respectively; Table
VII).
| Table VII.Molecular subtypes and the number of
metastatic sites in patients with metastatic breast cancer from the
Surveillance, Epidemiology and End Results dataset (n=15,322). |
Table VII.
Molecular subtypes and the number of
metastatic sites in patients with metastatic breast cancer from the
Surveillance, Epidemiology and End Results dataset (n=15,322).
| Number of
metastatic sites | HR+/HER2−
(n=9,222) | HR+/HER2+
(n=2,710) | HR-/HER2+
(n=1,406) | HR-/HER2-
(n=1,984) | χ2 | P-value |
|---|
| 1 | 6,042 (65.5) | 1,546 (57) | 761 (54.1) | 1,200 (60.5) | 160.329 | <0.001 |
| 2 | 2,289 (24.8) | 774 (28.6) | 399 (28.4) | 541 (27.3) |
|
|
| 3 | 722 (7.8) | 312 (11.5) | 183 (13.0) | 173 (8.7) |
|
|
| ≥4 | 169 (1.8) | 78 (2.9) | 63 (4.5) | 70 (3.5) |
|
|
The results of both datasets all suggested that the
number of metastatic sites was diverse across the molecular
subtypes. A single site of metastasis was more likely in
HR+/HER2−patients, while 2–3 sites of metastases were more likely
in HR+/HER2+ patients. Furthermore, ≥4 sites of metastasis were
more likely in patients with the HR-/HER2+ and HR-/HER2-
subtype.
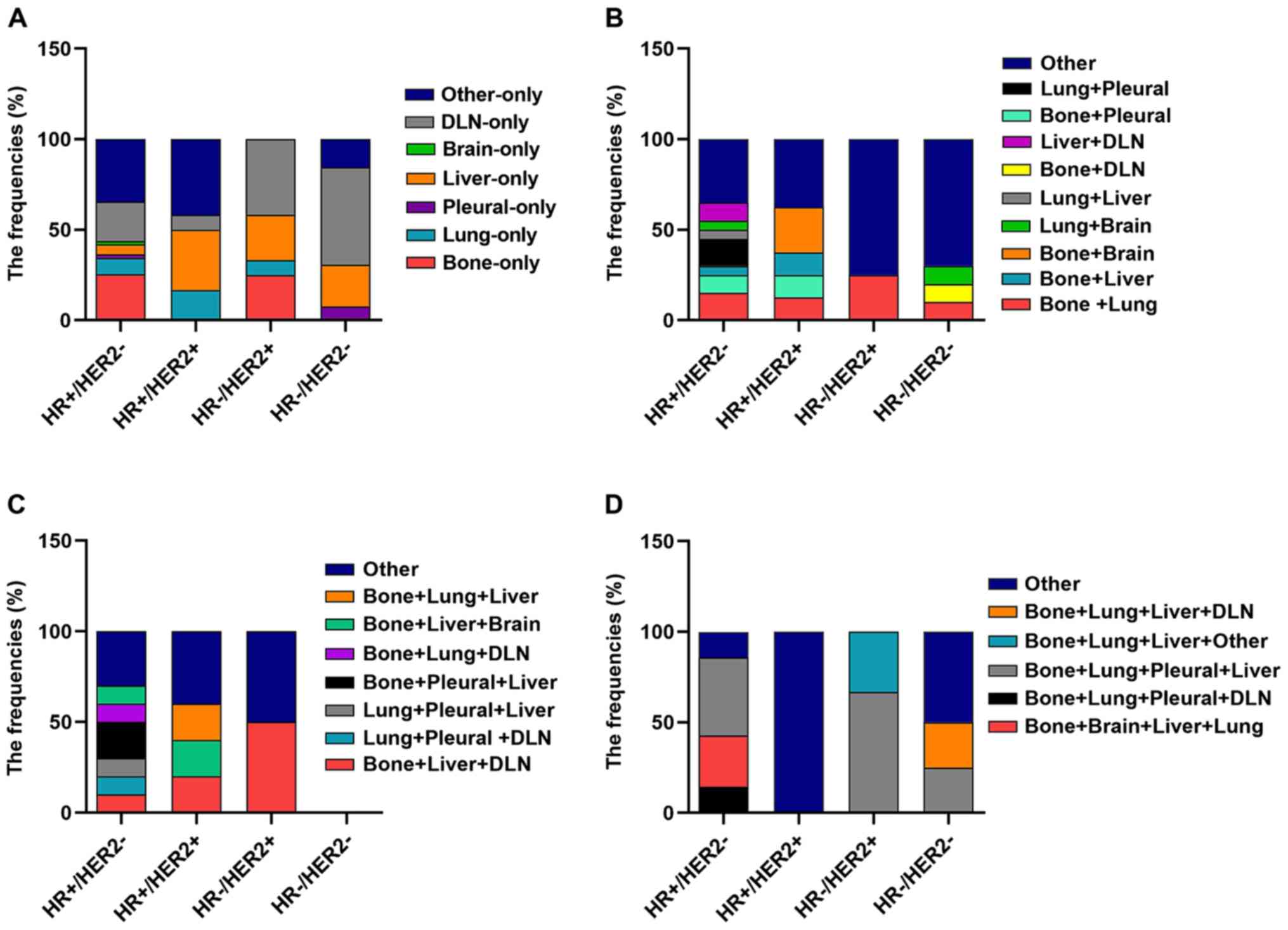
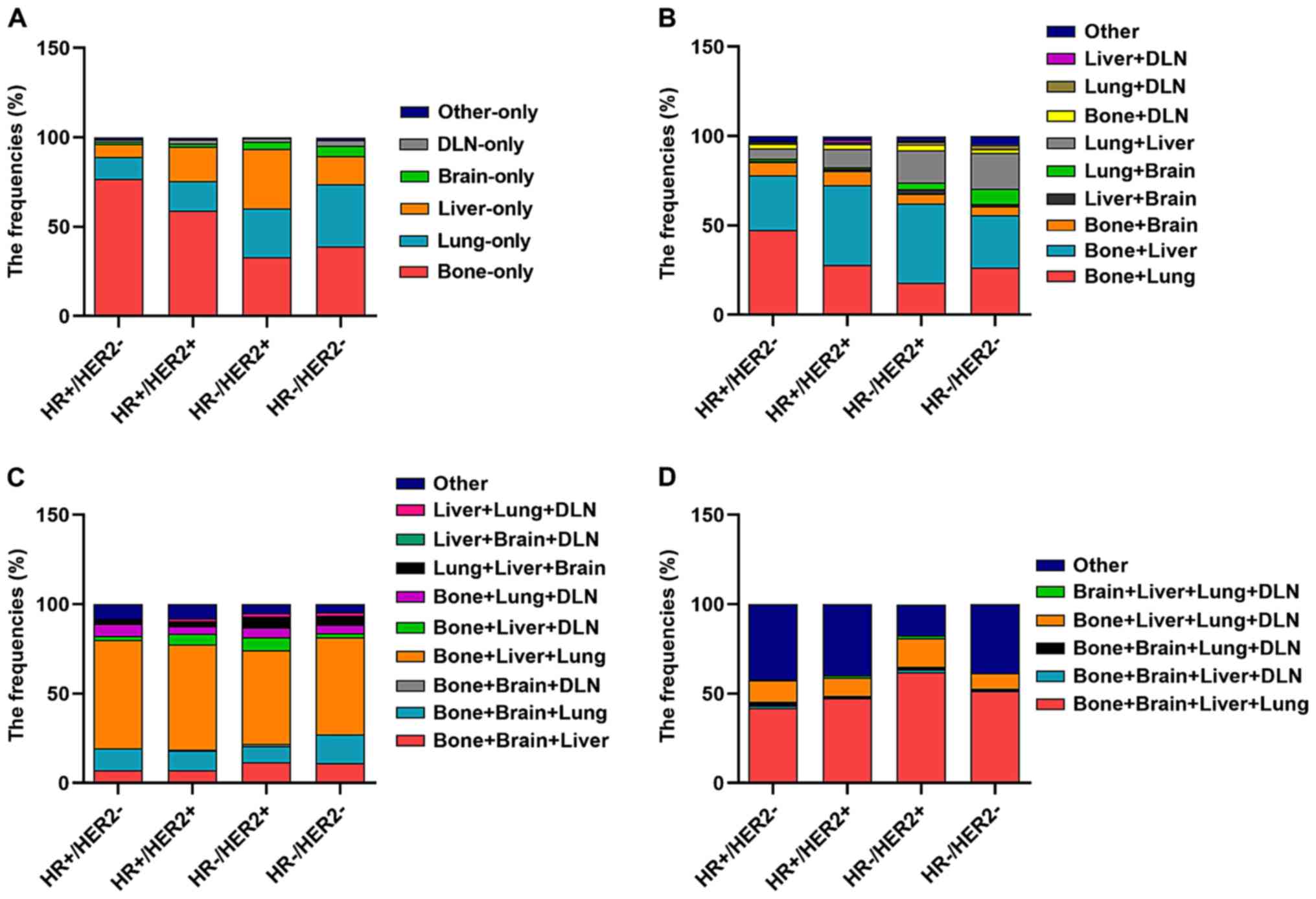
Subsequently, the information on all combinations of
different distant metastases was further analyzed in the subtypes
of patients in both datasets. In both datasets, it was indicated
that regarding single distant metastasis, bone-only metastasis was
more common in the HR+/HER2−subtype (P<0.05) and liver-only
metastasis was more common in the HR+/HER2+ and HR-/HER2+ subtypes
(P<0.05), while DLN-only metastasis was more common in HR-/HER2-
patients (P<0.05). Regarding the combinations of distant
metastases to two different sites, bone + liver metastases were
more common in the HR+/HER2+ subtype and bone + brain metastases
were also more common in the HR+/HER2+ subtype, while lung + brain
metastases were more common in the HR-/HER2- subtype. For
combinations of metastasis to three different distant sites, bone +
lung + DLN metastases were more common in the HR+/HER2− subtype
(Figs. 2 and 3; Tables SI
and SII).
Molecular subtypes and the OS of
patients with primary and metastatic breast cancer based on the
SEER database
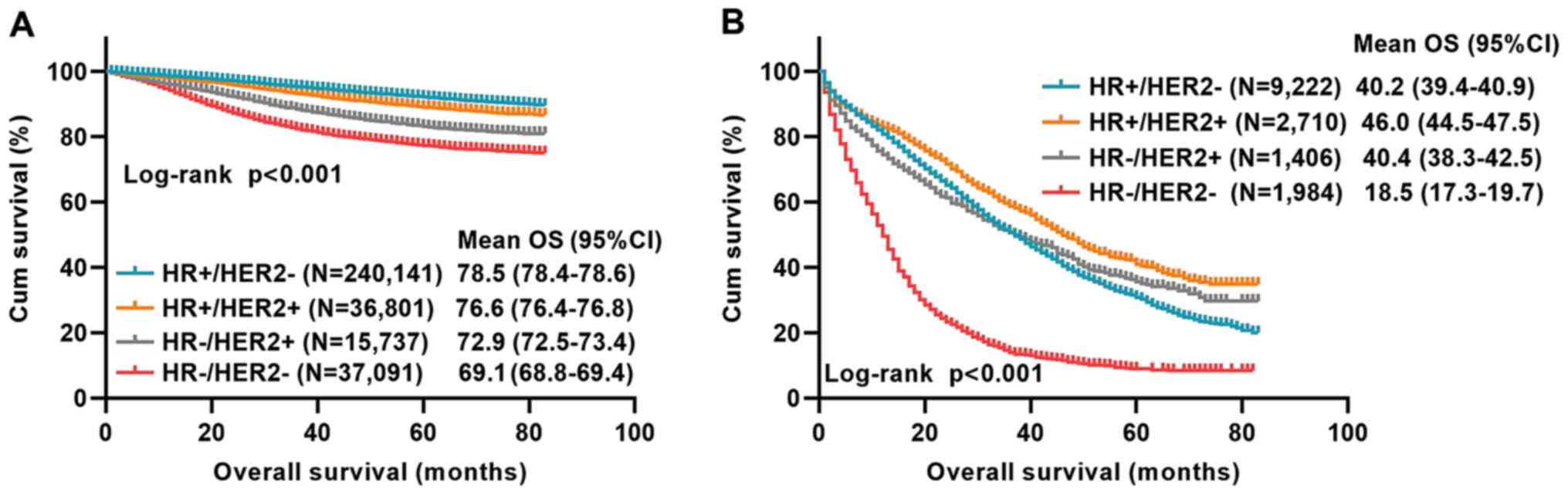
Based on the results discussed in the previous
section, the influence of the molecular subtype on the OS of
329,770 primary breast cancer patients from the SEER database
between 2010 and 2016 was first analyzed. There was a statistical
difference in OS among the molecular subtypes with primary breast
cancer (P<0.001). The mean OS period of HR+/HER2− patients was
78.5 months and the mean OS period of HR+/HER2+, HR-/HER2+ and
HR-/HER2- patients was 76.6, 72.9 and 69.1 months, respectively
(Fig. 4A).
Furthermore, the association between molecular
subtypes of the 15,322 metastatic breast cancer patients from the
SEER database between 2010 and 2016 and OS was determined. There
was a statistically significant difference in OS among the
different molecular subtypes with metastasis (P<0.001). The mean
OS of patients with metastasis of the HR+/HER2−type was 40.2
months, while that of the HR+/HER2+, HR-/HER2+ and HR-/HER2-types
was 46.0, 40.4 and 18.5 months, respectively (Fig. 4B).
Discussion
In most cases, the generation of breast cancer
metastatic lesions may last for months, years or even decades prior
to becoming a clinically detectable metastasis (17). While the underlying mechanisms remain
to be fully elucidated, it is known that metastasis is a process
that begins with the detachment of tumor cells from the primary
tumor (18). According to the St.
Gallen International Expert Consensus on the Primary Therapy of
Early Breast Cancer in 2011 (19),
given the limitation of molecular profiling studies in routine
clinical practice, the combination of the HR and HER2 status with
or without an accompanying Ki-67 proliferation index has been
recently used as an indicator for molecular subtypes. Different
molecular subtypes have distinctive biological features and
clinical outcomes (20). Molecular
subtypes remain the most important prognostic determinants in
breast cancer (21). The goal of the
present study was to explore the possible impact of molecular
subtypes on metastatic behavior and OS in a single-center study
combined with a large cohort study from the SEER database.
Monitoring the biological behavior of breast cancer may benefit a
patient by allowing for the implementation of a personalized
treatment strategy (22).
The present study indicated that bone metastasis is
more frequent in HR+/HER2+ patients, while metastasis to the lung
is more frequent in the HR-/HER2+ subtype as compared to the other
molecular subtypes of patients with breast cancer. Smid et
al (6) also determined that bone
metastasis is most abundant in the luminal subtypes. Largely in
accordance with these observations, tissue microarray analysis
suggested that the HER2 subtype exhibited higher rates of lung
metastasis compared with luminal A cancers (7). The luminal B subtype was less
frequently associated with lung metastasis than the HER2 subtype
(23). The liver was a common organ
involved in breast cancer metastasis. A previous study reported
that liver metastasis was more frequently observed in the HER2
subtype than the luminal A and triple-negative breast cancer (TNBC)
subtypes (23). Similarly, the
present study indicated that liver metastasis was more likely to be
present in the HR-/HER2+ and HR+/HER2+ subtypes from both datasets.
However, only a small number of previous studies have investigated
pleural metastases. One previous study reported that the luminal A
and B subtypes were both less frequently associated with pleural
metastasis than the TNBC subtype (23). In the present study, the HR+/HER2−
and HR-/HER2- subtypes had an increased likelihood to have pleural
metastasis in the single-center cohort. Since the metastatic sites
recorded in the SEER database did not include the pleura, it was
not possible to use those big data to further support this result.
The brain metastasis of breast cancer is not common (6); the present study indicated that
metastasis to the brain was less common than metastasis to other
organs. In the present study, the HR-/HER2+ and HR-/HER2-subtypes
were observed to have relatively more brain metastasis than the
other two subtypes. This result is consistent with a previous
study, which indicated that the HR-/HER2+ subtype had a higher risk
of brain metastasis (5).
There may be various reasons why different molecular
subtypes of breast cancer exhibit differences in metastatic sites.
A previous study reported that downregulation of E-cadherin was
crucial to the dissemination and invasion of cancer cells, which
may augment breast cancer metastasis to the bone (24). Zhang et al (25) recently identified differentially
expressed DEGs and signaling pathways that may make a contribution
towards the understanding of the pathological mechanisms of bone
metastasis from breast cancer. For example, integrin binding
sialoprotein, matrix metallopeptidase, TNF α-induced protein 6,
dehydrogenase/reductase 3, receptor interacting serine/threonine
kinase 4, and CD200 had a diagnostic value for patients with breast
cancer bone metastasis. There was evidence that the ability of
breast cancer cells to activate osteoclasts is similar to that of
normal glandular tissue of mammary epithelial cells during
lactation; therefore, breast cancer cells have intrinsic properties
that allow them to metastasize to bone tissue (26). Sphingosine kinase 1 (SPHK1) promoted
lung metastasis by transcriptionally upregulating the expression of
the metastasis-promoting gene fascin actin-building protein 1 via
NF-κB activation, and targeting SPHK1 and NF-κB using
clinically-applicable inhibitors significantly inhibited aggressive
mammary tumor growth and spontaneous lung metastasis in orthotopic
syngeneic HR-/HER2- subtype mouse models (27). The mechanism for the tendency of
HER2+ tumors to appear in the liver remains elusive. C-X-C motif
chemokine receptor 4, a chemokine receptor enhanced by HER2
activation, has been proposed to be involved in promoting invasion
of these cells to visceral organs (28). In addition, a previous study
indicated that hepatic steatosis may serve as an independent factor
to decrease liver metastasis in patients with breast cancer
(29). The biological mechanisms of
brain metastasis are currently unclear in breast cancer. A study
reported that the WNT pathway was associated with relapse of breast
cancer or metastasis to the brain (6). Future studies should investigate the
metastatic mechanism in breast cancer across the different subtypes
and develop strategies of how to reduce the overall risk of
metastasis.
To date, the association of molecular subtypes with
the number of metastatic sites in patients with breast cancer has
been rarely investigated. In the present study, analysis of the
single-center cohort and the SEER dataset both indicated that the
the number of metastatic sites of the HR+/HER2− subtype patients
was lower than in patients with the other three subtypes after
those patients had experienced metastases, while the number of
metastatic sites of the HR-/HER2+ and HR-/HER2- subtypes patients
was higher. The present study lacks mechanistic evidence to explain
why the molecular subtype affected the number of metastatic sites.
Future work by our group will continue to explore the reasons for
this and attempt to identify a possible mechanism.
Numerous studies have demonstrated different
survival rates between molecular subtypes (30–32).
However, the difference in prognosis between primary and metastatic
tumors of different molecular subtypes remains to be fully
elucidated. In the present study, there was a statistically
significant difference in OS among the different molecular subtypes
of patients with distant metastatic primary breast cancer between
2010 and 2016 from the SEER database. The patients of the HR+/HER2−
subtype had the longest mean OS compared with the other three
subtypes. HR-/HER2- was associated with a significantly poorer OS,
whether in primary breast cancer or the subset of metastatic breast
cancer patients. The Notch signaling pathway has emerged as a
regulatory factor in the pathogenesis and tumor progression of TNBC
(33). A previous study also
reported that in a survival analysis of females diagnosed with
de novo metastasis, the mortality risk relative to the
HR+/HER2− subtype was twice as high for HR-/HER2- and slightly
lower for HR+/HER2+; HER2+ metastatic breast cancers had relatively
better survival in recent years (34). The present study also determined that
the mean OS of metastatic patients of the HR+/HER2+ subtype was the
longest (46.0 months). Previous studies have indicated that the
median survival time of patients with metastatic breast cancer was
~2–4 years (3) and the 5-year
survival rate was only ~25% (35).
This was consistent with the present study.
As a limitation of the present study, no
Kaplan-Meier analysis was performed for the present single-center
cohort. As a proportion of metastatic breast cancer patients
enrolled in the present single-center study between 2012 and 2016
were initially treated at Hunan Provincial People's Hospital
(Changsha, China), when they were diagnosed with metastases later
here, then they went back to their local hospitals for final
treatment and some of them were lost to follow-up. In addition,
some metastatic breast cancer patients enrolled in the present
single-center study between 2017 and 2018 were still alive at the
end of the follow-up that their total time until death could not be
determined. Thus, considering the large amount of censored data in
the present dataset, no corresponding prognostic survival analysis
of the cases collected at Hunan Provincial People's Hospital
(Changsha, China) was performed.
The present results may assist clinicians in the
treatment of patients to select appropriate and standardized
treatments. Although the results for the single-center cohort were
not always consistent with the results obtained with the SEER data
due to limited samples in the single-center cohort, the present
results may be valuable for developing appropriate follow-up
strategies and to guide personalized care.
In conclusion, the present study indicated that
different molecular subtypes of breast cancer have different
metastatic behaviors. The subtypes exhibited differences regarding
the sites and number of metastases. The survival was different
among the different molecular subtypes with metastasis. These
results may assist clinicians in the prediction of metastatic
behavior of breast cancers and develop more efficient follow-up
monitoring strategies to further improve OS.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
This study was supported by The National Natural
Science Foundation of China (grant no. 81572966).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
Study design and supervision, as well as data
curation were performed by WW. The manuscript was drafted by HY.
Pathological work was performed by JZ and WG. Data collection and
processing were performed by HY, RW, FRZ, SLP, YYM, SYC, SJD and
LHZ. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
All procedures performed in this study were in
accordance with the ethical standards of the institutional and
national research committee and with the 1964 Helsinki declaration
and its later amendments or comparable ethical standards. It was
approved by the Medical Ethical Committee of Hunan Provincial
People's Hospital and The First Affiliated Hospital of Hunan Normal
University (Changsha, China) and written informed consent was
provided by all of the participating patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Santa-Maria CA, Nye L, Mutonga MB, Jain S
and Gradishar WJ: Management of Metastatic HER2-positive breast
cancer: Where are we and where do we go from here? Oncology
(Williston Park). 30:148–155. 2016.PubMed/NCBI
|
|
3
|
Puglisi F, Rea D, Kroes MA and Pronzato P:
Second-line single-agent chemotherapy in human epidermal growth
factor receptor 2-negative metastatic breast cancer: A systematic
review. Cancer Treat Rev. 43:36–49. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Gerratana L, Fanotto V, Bonotto M,
Bolzonello S, Minisini AM, Fasola G and Puglisi F: Pattern of
metastasis and outcome in patients with breast cancer. Clin Exp
Metastasis. 32:125–133. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sihto H, Lundin J, Lundin M, Lehtimäki T,
Ristimäki A, Holli K, Sailas L, Kataja V, Turpeenniemi-Hujanen T,
Isola J, et al: Breast cancer biological subtypes and protein
expression predict for the preferential distant metastasis sites: A
nationwide cohort study. Breast Cancer Res. 13:R872011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Smid M, Wang Y, Zhang Y, Sieuwerts AM, Yu
J, Klijn JG, Foekens JA and Martens JW: Subtypes of breast cancer
show preferential site of relapse. Cancer Res. 68:3108–3114. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kennecke H, Yerushalmi R, Woods R, Cheang
MC, Voduc D, Speers CH, Nielsen TO and Gelmon K: Metastatic
behavior of breast cancer subtypes. J Clin Oncol. 28:3271–3277.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Berman AT, Thukral AD, Hwang WT, Solin LJ
and Vapiwala N: Incidence and patterns of distant metastases for
patients with early-stage breast cancer after breast conservation
treatment. Clin Breast Cancer. 13:88–94. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Heitz F, Harter P, Lueck HJ,
Fissler-Eckhoff A, Lorenz-Salehi F, Scheil-Bertram S, Traut A and
du Bois A: Triple-negative and HER2-overexpressing breast cancers
exhibit an elevated risk and an earlier occurrence of cerebral
metastases. Eur J Cancer. 45:2792–2798. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Metzger-Filho O, Sun Z, Viale G, Price KN,
Crivellari D, Snyder RD, Gelber RD, Castiglione-Gertsch M, Coates
AS, Goldhirsch A and Cardoso F: Patterns of Recurrence and outcome
according to breast cancer subtypes in lymph node-negative disease:
Results from international breast cancer study group trials VIII
and IX. J Clin Oncol. 31:3083–3090. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Paluch-Shimon S, Ben-Baruch N, Wolf I,
Zach L, Kopolovic J, Kruglikova A, Modiano T, Yosepovich A, Catane
R and Kaufman B: Hormone receptor expression is associated with a
unique pattern of metastatic spread and increased survival among
HER2-overexpressing breast cancer patients. Am J Clin Oncol.
32:504–508. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Dent R, Hanna WM, Trudeau M, Rawlinson E,
Sun P and Narod SA: Pattern of metastatic spread in triple-negative
breast cancer. Breast Cancer Res Treat. 115:423–428. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Minisini AM, Moroso S, Gerratana L,
Giangreco M, Iacono D, Poletto E, Guardascione M, Fontanella C,
Fasola G and Puglisi F: Risk factors and survival outcomes in
patients with brain metastases from breast cancer. Clin Exp
Metastasis. 30:951–956. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Sperduto PW, Kased N, Roberge D, Chao ST,
Shanley R, Luo X, Sneed PK, Suh J, Weil RJ, Jensen AW, et al: The
effect of tumor subtype on the time from primary diagnosis to
development of brain metastases and survival in patients with
breast cancer. J Neurooncol. 112:467–472. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hammond ME, Hayes DF, Wolff AC, Mangu PB
and Temin S: American society of clinical oncology/college of
american pathologists guideline recommendations for
immunohistochemical testing of estrogen and progesterone receptors
in breast cancer. J Oncol Pract. 6:195–197. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Wolff AC, Hammond ME, Hicks DG, Dowsett M,
McShane LM, Allison KH, Allred DC, Bartlett JM, Bilous M,
Fitzgibbons P, et al: Recommendations for human epidermal growth
factor receptor 2 testing in breast cancer: American Society of
Clinical Oncology/College of American Pathologists clinical
practice guideline update. J Clin Oncol. 31:3997–4013. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kimbung S, Loman N and Hedenfalk I:
Clinical and molecular complexity of breast cancer metastases.
Semin Cancer Biol. 35:85–95. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Chaffer CL and Weinberg RA: A perspective
on cancer cell metastasis. Science. 331:1559–1564. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Goldhirsch A, Wood WC, Coates AS, Gelber
RD, Thurlimann B and Senn HJ; Panel members, : Strategies for
subtypes-dealing with the diversity of breast cancer: Highlights of
the St. Gallen international expert consensus on the primary
therapy of early breast cancer 2011. Ann Onco. 22:1736–1747. 2011.
View Article : Google Scholar
|
|
20
|
Ongaro E, Gerratana L, Cinausero M,
Pelizzari G, Poletto E, Giangreco M, Andreetta C, Pizzolitto S, Di
Loreto C, Minisini AM, et al: Comparison of primary breast cancer
and paired metastases: Biomarkers discordance influence on outcome
and therapy. Future Oncol. 14:849–859. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Killelea BK, Gallagher EJ, Feldman SM,
Port E, King T, Boolbol SK, Franco R, Fei K, Le Roith D and Bickell
NA: The effect of modifiable risk factors on breast cancer
aggressiveness among black and white women. Am J Surg. 218:689–694.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Fujii K, Watanabe R, Ando T, Kousaka J,
Mouri Y, Yoshida M, Imai T, Nakano S and Fukutomi T: Alterations in
three biomarkers (estrogen receptor, progesterone receptor and
human epidermal growth factor 2) and the Ki67 index between primary
and metastatic breast cancer lesions. Biomed Rep. 7:535–542.
2017.PubMed/NCBI
|
|
23
|
Soni A, Ren Z, Hameed O, Chanda D, Morgan
CJ, Siegal GP and Wei S: Breast cancer subtypes predispose the site
of distant metastases. Am J Clin Pathol. 143:471–478. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Schmalhofer O, Brabletz S and Brabletz T:
E-cadherin, beta-catenin, and ZEB1 in malignant progression of
cancer. Cancer Metastasis Rev. 28:151–166. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Zhang Y, He W and Zhang S: Seeking for
correlative genes and signaling pathways with bone metastasis from
breast cancer by integrated analysis. Front Oncol. 9:1382019.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Jones DH, Nakashima T, Sanchez OH,
Kozieradzki I, Komarova SV, Sarosi I, Morony S, Rubin E, Sarao R,
Hojilla CV, et al: Regulation of cancer cell migration and bone
metastasis by RANKL. Nature. 440:692–696. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Acharya S, Yao J, Li P, Zhang C, Lowery
FJ, Zhang Q, Guo H, Qu J, Yang F, Wistuba II, et al:
Sphingosine-kinase-1 signaling promotes metastasis of
triple-negative breast cancer. Cancer Res. 79:4211–4226. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Li YM, Pan Y, Wei Y, Cheng X, Zhou BP, Tan
M, Zhou X, Xia W, Hortobagyi GN, Yu D and Hung MC: Upregulation of
CXCR4 is essential for HER2-mediated tumor metastasis. Cancer Cell.
6:459–469. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Wu W, Chen J, Ye W, Li X and Zhang J:
Fatty liver decreases the risk of liver metastasis in patients with
breast cancer: A two-center cohort study. Breast Cancer Res Treat.
166:289–297. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Park HS, Kim S, Kim K, Yoo H, Chae BJ, Bae
JS, Song BJ and Jung SS: Pattern of distant recurrence according to
the molecular subtypes in Korean women with breast cancer. World J
Surg Oncol. 10:42012. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Carvalho ST, Stiepcich MM, Fregnani JH,
Nonogaki S, Rocha R and Soares FA: Evaluation of prognostic factors
in stage IIA breast tumors and their correlation with mortality
risk. Clinics (Sao Paulo). 66:607–612. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Zhang C, Wang S, Israel HP, Yan SX,
Horowitz DP, Crockford S, Gidea-Addeo D, Clifford Chao KS, Kalinsky
K and Connolly EP: Higher locoregional recurrence rate for
triple-negative breast cancer following neoadjuvant chemotherapy,
surgery and radiotherapy. Springer Plus. 4:3862015. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Giuli MV, Giuliani E, Screpanti I,
Bellavia D and Checquolo S: Notch signaling activation as a
hallmark for triple-negative breast cancer subtype. J Oncol.
2019:87070532019. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Press DJ, Miller ME, Liederbach E, Yao K
and Huo D: De novo metastasis in breast cancer: Occurrence and
overall survival stratified by molecular subtype. Clin Exp
Metastasis. 34:457–465. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Bonotto M, Gerratana L, Poletto E, Driol
P, Giangreco M, Russo S, Minisini AM, Andreetta C, Mansutti M, Pisa
FE, et al: Measures of outcome in metastatic breast cancer:
Insights from a real-world scenario. Oncologist. 19:608–615. 2014.
View Article : Google Scholar : PubMed/NCBI
|