Introduction
Cervical cancer is the second most common female
cancer in the world and the fourth most common cause of
cancer-related deaths (1). Infection
with human papillomavirus (HPV) is a prerequisite for the disease,
and approximately 80% of women will be infected with cervical HPV
by the age of 50, but not all infected individuals will develop the
disease (2,3). Among them, 13% of cervical cancer
patients are only diagnosed at an advanced stage. When cervical
cancer progresses to metastatic cervical cancer, the 5-year
survival rate is only 16.5%, with local cervical cancer accounting
for 91.5% of the total cases, and the 5-year survival rate of
patients past stage III is <40% (4). Therefore, early diagnosis and effective
prognosis prediction of cervical cancer patients will markedly
enhance the survival treatment of patients. However, to date,
cervical cancer does not have an effective biomarker for diagnosis
and prognosis, thus it is particularly important to identify a key
non-invasive molecular marker.
Long non-coding RNAs (lncRNAs) are a class of RNA
molecules with a transcription length >200 nt. Although they
lack protein-coding features, they are able to widely regulate the
expression of some genes and participate in cell proliferation,
differentiation, apoptosis as well as other processes, thereby
attracting the attention of several scientists in recent years
(5,6). With the progress in lncRNA research, it
has been revealed that lncRNAs are closely related to numerous
cancer diseases (7,8). For example, Misawa et al
(9) revealed that lncRNASOCS2-AS1
could inhibit apoptosis of prostate cancer cells through the
androgen receptor target gene. In addition, Chen et al
(10) demonstrated that the
expression of lncRNA n336928 in bladder cancer tissues was
significantly higher than that in adjacent tissues, and the total
survival time of bladder cancer patients with low expression of
lncRNA n336928 was also lower than that of patients with high
expression. lncRNA maternally expressed 3 (MEG3), a member of the
lncRNA family, is located in the imprinted region of DLK1-MEG3 on
chromosome 14, which contains multiple imprinted genes that exerts
inhibition in most cancers (11,12).
Studies have revealed that MEG3 expression in endometrial cancer
tissue is significantly lower than that in normal endometrial
tissue, and that overexpressed MEG3 inhibits proliferation,
invasion and metastasis of endometrial cancer cells, promotes
apoptosis. Moreover, the expression of MEG3 in ovarian cancer cells
has also been revealed to be significantly lower than normal
ovarian cells (13–15). However, the diagnostic value of
lncRNA MEG3 in cervical cancer and its impact on prognosis remain
poorly understood.
Therefore, by observing the serum lncRNA MEG3
expression of cancer patients, the present study aimed to elucidate
its diagnostic and prognostic value in cervical cancer, thus
providing direction and basis for clinical application.
Materials and methods
Clinical data
Eighty-four patients with cervical cancer, with an
average age of 51.0±6.3 years, were enrolled as the observation
group (OG) from February 2013 to March 2014 at Huangshi Central
Hospital. In addition, 58 female subjects with an average age of
50.7±5.8 years, who underwent physical examination at Huangshi
Central Hospital, concurrently, were assigned into the control
group (CG). The present study was approved by the Medical Ethics
Committee of Huangshi Central Hospital, and all patients provided
signed informed consent.
Inclusion and exclusion criteria
Patients pathologically diagnosed with cervical
cancer that could be staged according to the International
Federation of Gynecology and Obstetrics (FIGO) pathological staging
(16), who were informed of the
purpose of this study and signed the informed consent, and those
willing to cooperate with the follow-up, with complete clinical
data were included.
Patients complicated with other tumors or
gynecological diseases, who had received chemoradiotherapy before
this study or presented with congenital liver, kidney and heart
function defects, or those with a life expectancy of <3 months
were excluded.
Patient follow-up
The patients were followed-up for 5 years, with the
diagnosis time as the starting point, and the death of a patient
(due to cervical cancer and complications), loss of follow-up or
the end of the follow-up time as the end point. A reexamination was
carried out every 6 months. The follow-up was conducted by
telephone, door-to-door and outpatient reexamination. In the first
year of follow-up, the patients were followed-up every 3 months,
and every 6 months for the following 4 years.
Quantitative real-time polymerase
chain reaction (qPCR) detection
Fasting venous blood (5 ml) was collected from all
the research participants, and the serum was collected by
centrifugation (3,000 × g at 4°C for 10 min) in a pro-coagulation
tube. Then the total RNA in serum was extracted with a TRIzol kit
(Invitrogen; Thermo Fisher Scientific, Inc. cat. no. 15596018),
whose purity, concentration and integrity was then detected by UV
spectrophotometer and agarose gel electrophoresis. Subsequently,
reverse transcription was conducted using TransScript®
II Green Two-Step qRT-PCR SuperMix kit (cat. no. AQ301-01; Beijing
TransGen Biotech Co., Ltd.) in strict accordance with the
manufacturer's instructions. PCR amplification was then performed,
and the PCR reaction system was as follows: cDNA, 1 µl; upstream
and downstream primers, each 0.4 µl; 2X TransScript® Tip
Green qPCR, SuperMix 10 µl; Passive Reference Dye (50X), 0.4 µl,
and finally nuclease-free water was added for a total reaction
volume of 20 µl. The PCR reaction conditions were as follows:
Pre-denaturation at 94°C for 30 sec, denaturation at 94°C for 5
sec, annealing at 60°C for 30 sec, totaling 40 cycles. The primer
sequences for MEG3 and GAPDH are presented in Table I. Three replicate wells were set for
each sample and the experiment was performed in triplicate. GAPDH
was used as the internal reference, and the data was analyzed by
2−∆∆Cq in this experiment (17).
 | Table I.Primer sequences. |
Table I.
Primer sequences.
| Gene | Upstream primer | Downstream
primer |
|---|
| MEG3 |
5′-TCGCTCTTCTCCATCGAACCG-3′ |
5′-GTAGGGCGACGACTTTGAGT-3′ |
| GAPDH |
5′-ATGGTGAAGGTCGGT-GTGA-3′ |
5′-CCATGTAGTTGAG-GTCAATGAG-3′ |
Observation indicators
Primary endpoints
MEG3 expression was compared between the OG and the
CG. The 5-year survival of the patients was recorded, and
multivariate Cox regression was used to analyze the risk factors of
mortality according to the 5-year survival of the patients.
Receiver operating characteristic (ROC) curve was applied to
analyze the diagnostic and death-predicting value of MEG3 in
cervical cancer.
Secondary endpoints
The MEG3 expression between patients who survived
and those who succumbed to the disease, lymph node metastasis and
non-metastasis, FIGO stage III and IV and I and II were compared.
ROC was used to analyze the diagnostic value of MEG3 in lymph node
metastasis and FIGO staging.
Statistical analysis
The collected data were statistically analyzed by
SPSS 20.0 (Shanghai Cabit Information Technology Co., Ltd.), and
the acquired images were plotted using GraphPad Prism 7 (Shenzhen
Softhead Technology Co., Ltd., China). The counting data
represented by percentage (%) were compared using Chi-square and
expressed as χ2. While the measurement data were
expressed as the mean ± standard deviation (SD). All measurement
data were in line with normal distribution, and the comparison
between the two groups was compared by an independent sample
t-test, represented by t. The ability of MEG3 in diagnosing
cervical cancer, lymph node metastasis and FIGO staging, as well as
in predicting mortality was assessed by ROC. The 5-year survival of
patients was analyzed by Kaplan-Meier (K-M) survival analysis using
log-rank test. Cox regression was employed to analyze the factors
affecting the prognosis of patients. P<0.05 indicated a
statistically significant difference between the two groups.
Results
Clinical data
No significant difference was observed in the
clinical data of patients in the two groups in terms of age, BMI,
smoking history, alcohol history, place of residence, and
reproductive history (P>0.05; Table
II).
| Table II.Clinical data of patients. |
Table II.
Clinical data of patients.
| Factors | OG (n=84) | CG (n=58) |
t/χ2-value | P-value |
|---|
| Age (years) | 51.0±6.3 | 50.7±5.8 | 0.288 | 0.774 |
| BMI
(kg/m2) | 21.36±1.53 | 21.54±1.42 | 0.709 | 0.479 |
| Smoking history |
|
|
|
|
| Yes | 15 (17.86) | 11 (18.97) | 0.028 | 0.867 |
| No | 69 (82.14) | 47 (81.03) |
|
|
| Drinking history |
|
|
|
|
| Yes | 13 (15.48) | 7
(12.07) | 0.329 | 0.566 |
| No | 71 (84.52) | 51 (87.93) |
|
|
| Residence |
|
|
|
|
|
Urban | 67 (79.76) | 47 (81.03) | 0.035 | 0.851 |
|
Rural | 17 (20.24) | 11 (18.97) |
|
|
| Reproductive
history |
|
|
|
|
| Yes | 62 (73.81) | 48 (82.76) | 1.574 | 0.210 |
| No | 22 (26.19) | 10 (17.24) |
|
|
| Menopause |
|
|
|
|
| Yes | 48 (57.14) | 35 (60.34) | 0.145 | 0.704 |
| No | 36 (42.86) | 23 (39.66) |
|
|
| Tumor size |
|
|
|
|
| ≤2
cm | 45 (53.57) |
|
|
|
| >2
cm | 39 (46.43) |
|
|
|
| FIGO staging |
|
|
|
|
|
I+II | 51 (60.71) |
|
|
|
|
III+IV | 33 (39.29) |
|
|
|
| Histological
type |
|
|
|
|
|
Squamous cell carcinoma | 57 (67.86) |
|
|
|
|
Adenocarcinoma | 27 (32.14) |
|
|
|
| Vaginal
infiltration | 28 (33.33) |
|
|
|
| Parametrial
involvement | 24 (28.57) |
|
|
|
| Lymph node
metastasis | 31 (36.90) |
|
|
|
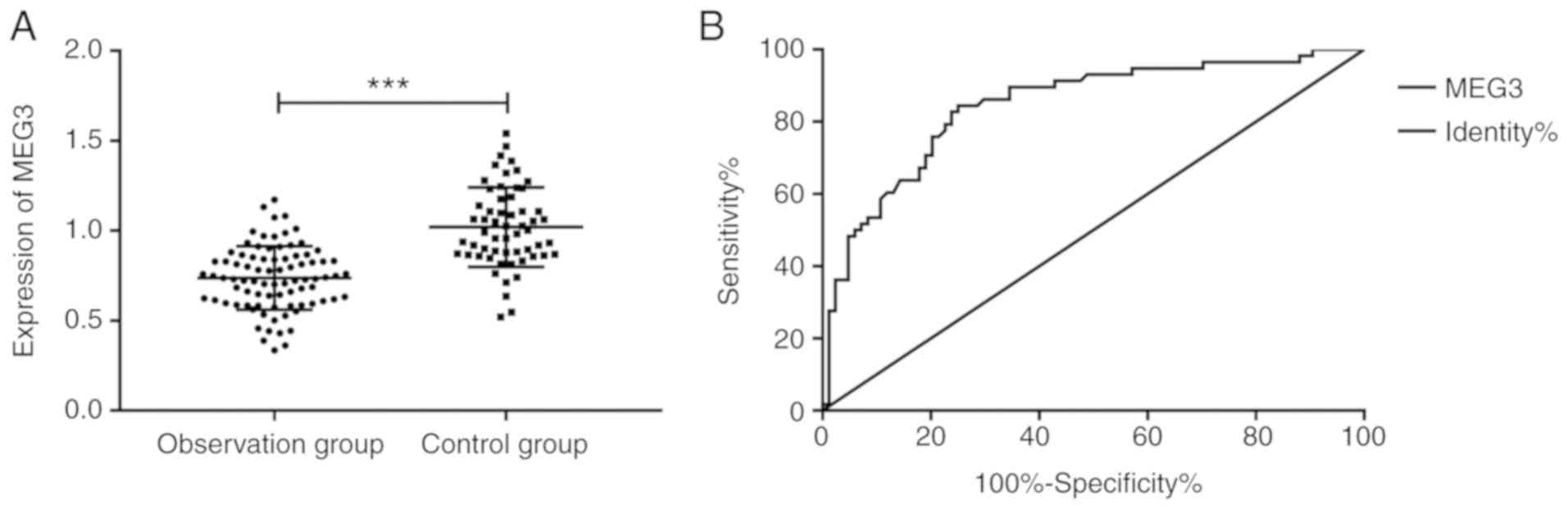
Comparison of MEG3 expression in the
two groups and its diagnostic value in cervical cancer
By observing the expression of MEG3, it was revealed
that the expression of MEG3 in the OG (0.74±0.20) was significantly
lower than that in the CG (1.02±0.22). The AUC of MEG3 in the
diagnosis of cervical cancer was 0.844, 95 CI%, 0.778–0.911. When
the cut-off point was 0.850, the specificity was 75.00%, the
sensitivity was 82.76%, and the Youden index was 57.76% (Fig. 1).
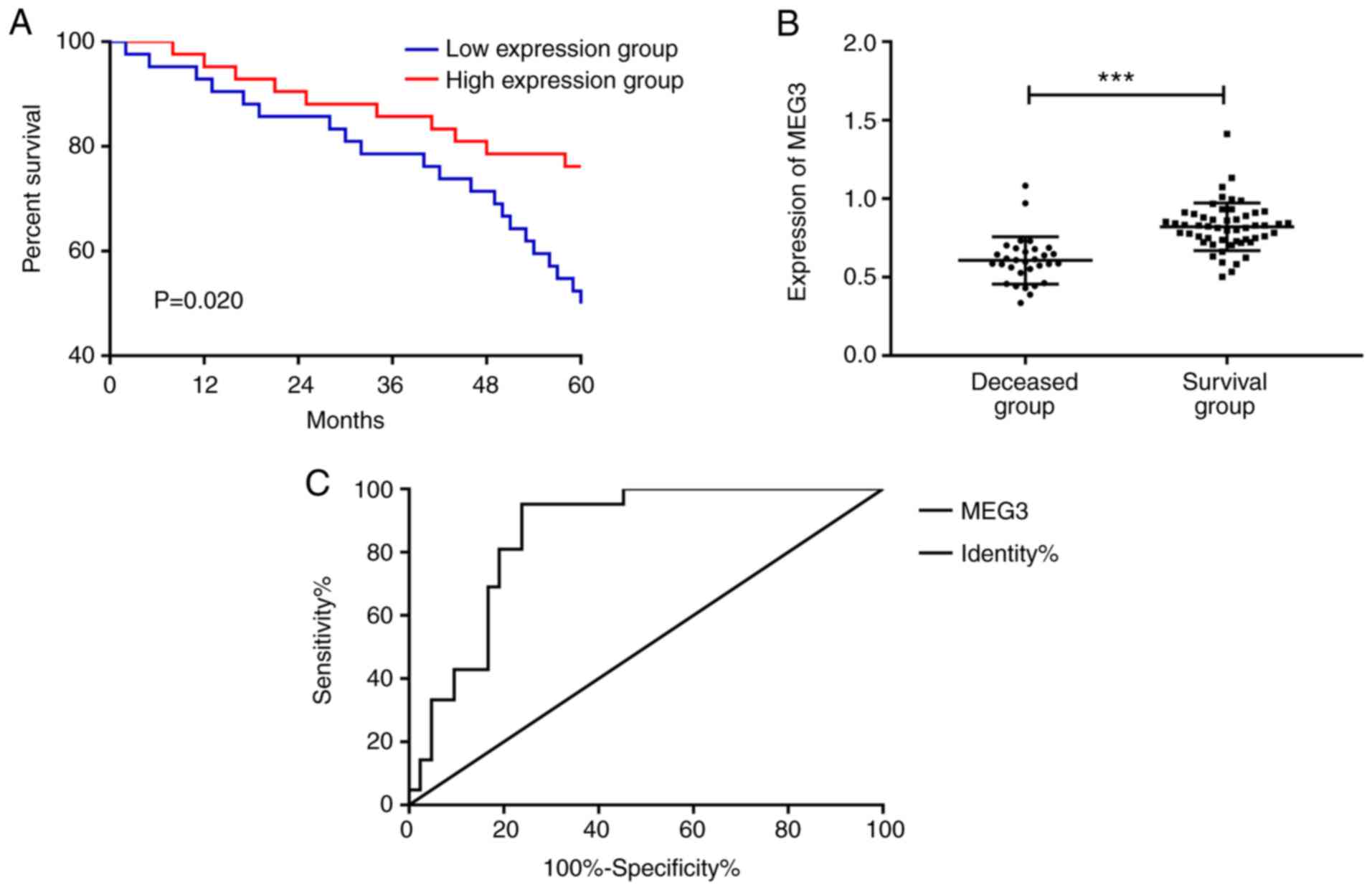
Survival and mortality prediction
value of patients with high and low expression of MEG3
Over the 5-year follow-up, 31 patients did not
survive while 53 survived in the OG, with a survival rate of
63.10%. All patients in the OG were divided into a high-expression
group and a low-expression group according to the median value of
MEG3 expression. It was determined that the survival of the
high-expression group was significantly increased compared to the
low-expression group, and MEG3 expression of the non-surviving
patients was significantly lower than that of the surviving
patients. The area under the ROC curve of MEG3 in predicting
cervical cancer death was 0.858, 95 CI%, 0.773–0.943. When the
cutoff point was 0.706, the specificity was 76.19%, the sensitivity
was 92.86%, and the Youden index was 69.05% (Fig. 2).
Cox analysis
The clinical data of patients were collected and
assigned, and then Cox regression and the Enter Regression method
were used for analysis. It was determined that FIGO staging,
vaginal infiltration, lymph node metastasis and MEG3 were
prognostic factors for cervical cancer patients. Then, backward
logistic regression (LR) was further selected for the multivariate
analysis of the factors with differences, which revealed that MEG3
(HR, 0.173; 95 CI%, 0.028–0.919), lymph node metastasis (HR, 2.259;
95 CI%, 1.004–5.025), and FIGO staging (HR, 0.008; 95 CI%,
1.453–6.248) were independent prognostic factors for cervical
cancer patients (Tables III and
IV).
| Table III.Factors and assignments of cervical
cancer. |
Table III.
Factors and assignments of cervical
cancer.
| Factors | Assignments |
|---|
| Age | ≥50 years old=1;
<50 years old=0 |
| BMI | ≥21
kg/m3=1; <21 kg/m3=0 |
| Reproductive
history | Yes=1; no=0 |
| Menopause | Yes=1; no=0 |
| Tumor size | >2 cm=1; ≤2
cm=0 |
| FIGO staging | III+IV=1;
I+II=0 |
| Histological
type | Squamous cell
carcinoma=1; adenocarcinoma=0 |
| Vaginal
infiltration | Yes=1; no=0 |
| Parametrial
involvement | Yes=1; no=0 |
| Lymph node
metastasis | With metastasis=1;
without metastasis=0 |
| MEG3 | Raw data analysis
for continuous variables. |
| Table IV.Cox regression. |
Table IV.
Cox regression.
|
| Univariate cox | Multivariate
cox |
|---|
|
|
|
|
|---|
| Factors | Exp(B) | 95 CI% | Sig. | Exp(B) | 95 CI% | Sig. |
|---|
| Age | 1.072 | 0.896–1.226 | 0.473 |
|
|
|
| BMI | 1.672 | 0.632–3.066 | 0.336 |
|
|
|
| Reproductive
history | 0.836 | 0.445–1.783 | 0.720 |
|
|
|
| Menopause | 1.053 | 0.572–1.94 | 0.868 |
|
|
|
| Tumor size | 1.274 | 0.937–1.725 | 0.173 |
|
|
|
| FIGO staging | 3.739 | 1.780–7.458 | <0.001 | 0.008 | 1.453–6.248 | 0.006 |
| Histological
type | 0.937 | 2.745–10.247 | 0.963 |
|
|
|
| Vaginal
infiltration | 2.136 | 1.037–4.227 | 0.036 | 0.583 | 0.185–1.649 | 0.365 |
| Parametrial
involvement | 0.146 | 0.061–0.351 | 0.400 |
|
|
|
| Lymph node
metastasis | 2.057 | 1.021–4.243 | 0.044 | 2.259 | 1.004–5.025 | 0.047 |
| MEG3 | 0.137 | 0.038–0.573 | 0.003 | 0.173 | 0.028–0.919 | 0.042 |
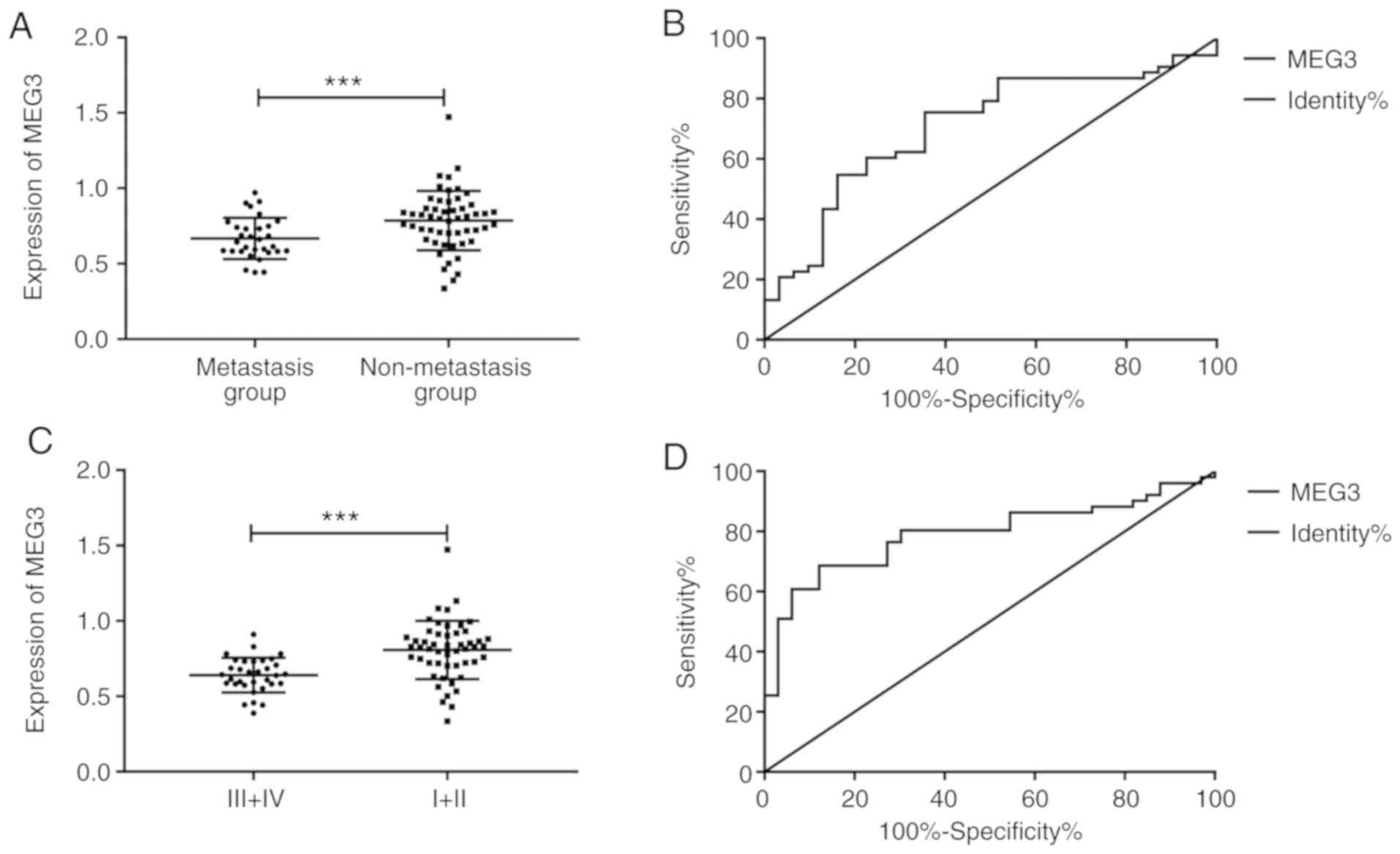
Diagnostic value of MEG3 for risk
factors
By comparing the expression of MEG3 in patients with
lymph node metastasis and non-metastasis and those with stage I and
II or III and IV, it was revealed that the expression of metastatic
patients was significantly lower than that of non-metastatic
patients. The area under the ROC curve for diagnosis of lymph node
metastasis was 0.707, 95 CI%, 0.592–0.821. When the cut-off point
was 0.750, the specificity was 77.42%, the sensitivity was 60.38%,
and the Youden index was 37.80%. In addition, the expression of
patients with stage III and IV was lower than that of patients with
stage I and II. The area under the ROC curve for the diagnosis of
FIGO staging was 0.791, 95 CI%, 0.694–0.889. When the cut-off point
was 0.755, the specificity was 87.88%, the sensitivity was 66.67%,
and the Youden index was 54.55%. (Fig.
3).
Discussion
The onset of cervical cancer is the contribution of
different complex factors, resulting in the formation of invasive,
chemoresistant and radiation-tolerant tumor masses in HPV-infected
cells, which are often caused by unstable mutations and disorders
of the genome (18). At present,
several lncRNAs have been demonstrated to play a relevant role in
the development and progression of cervical cancer, and are
expected to be new targets for the diagnosis, prognosis and
targeted therapy of the disease (19). Although there are different treatment
methods available customized to the different conditions of
cervical cancer patients, such as surgery, chemotherapy and
radiotherapy (20), if the actual
condition of patients can be accurately understood, more
appropriate individualized treatment programs can be applied for
treatment, thus improving the survival of patients (21,22).
In the present study, the expression of MEG3 was
first compared between two groups (OG and CG). It was revealed that
the OG presented markedly lower MEG3 expression than the CG, which
was in line with a previous study (23). Moreover, in a study by Chen and Qu
(24), MEG3 inhibited the survival
and migration of cervical cancer cells mainly by inhibiting Rac1.
Therefore, we hypothesized that MEG3 may be a diagnostic indicator
for cervical cancer patients. With the advantage of a ROC curve, it
was observed that the AUC of MEG3 in diagnosing cervical cancer was
0.844, and the corresponding specificity and sensitivity were 75.00
and 82.76% when the cut-off point was set as 0.850, which also
indicated that MEG3 may be a diagnostic marker for cervical cancer.
Then, the patients were followed-up for 5 years and it was revealed
that the survival rate was 63.10%. The survival curve demonstrated
that the survival rate of patients with low MEG3 expression was
significantly lower than that of patients with high MEG3
expression. In addition, by comparing the expression of MEG3
between the surviving and non-surviving patients, it was revealed
that the expression of MEG3 in the non-surviving patients was
significantly lower than that in surviving patients. Furthermore,
ROC curve revealed that the AUC of MEG3 in predicting cervical
cancer death was 0.858, and when the cut-off point was 0.706, the
specificity was 76.19% and the sensitivity was 92.86%, which
further indicated that MEG3 may be used as a predictor of mortality
of cervical cancer patients. Xiu et al (25) determined that the inhibition
mechanism of MEG3 in ovarian cancer was realized by regulating ATG3
activity and inducing autophagy, and they also reported that the
AUC was 0.763 by ROC curve detection, which revealed that MEG3 not
only had diagnostic value in ovarian cancer, but also had
diagnostic value in cervical cancer, while MEG3 may be more
suitable for the diagnosis of the latter.
Furthermore, by exploring the independent factors
affecting the prognosis of cervical cancer patients, we collected
the clinical data of the patients for multivariate Cox regression
analysis, and it was determined that lymph node metastasis, FIGO
stage III and IV, and a low MEG3 level were independent prognostic
factors for cervical cancer patients. Numerous studies have
reported that patients with high FIGO staging and lymph node
metastasis present poor prognosis (26,27). In
addition, since lymph node metastasis and high FIGO staging are
characteristics of high-risk patients, early diagnosis of lymph
node metastasis and high FIGO stage will also be helpful for the
treatment. Therefore, we compared the MEG3 level of these patients
and utilized ROC curve to assess the diagnostic value of MEG3 in
cervical cancer patients with lymph node metastasis and FIGO stage
III+IV. It revealed that the MEG3 level of patients with metastasis
was significantly lower than that of patients without metastasis.
The area under the ROC curve was 0.707, with a specificity of
77.42% and a sensitivity of 60.38% when the cut-off point was
0.750. Moreover, the MEG3 level of patients with FIGO stage III and
IV was significantly lower than that of patients with stage I and
II. Therefore, the detection of MEG3 levels may be conducive to
identify high-risk patients before treatment, in order to conduct
more effective treatment. However, there are some limitations in
the present study. First, the treatment methods were not
restricted, which may irrevocably lead to inconsistencies in the
treatment of patients, and the impact of these treatments is still
unclear. Secondly, we have not conducted any cell-based
experiments, and the specific regulatory mechanism of MEG3 as a
tumor suppressor gene in cervical cancer remains a subject of
investigation. Zhang et al (28) revealed that MEG3 inhibited the growth
of tumors in cervical cancer by regulating miR-21-5p. Hence, our
aim is to conduct corresponding basic experiments on MEG3 in the
future to study corresponding target genes and affected signaling
pathways, to verify whether it can be used as a target therapy.
Finally, an in-depth investigation has not yet been performed on
patients with recurrence, however, this will be carried out with
the relevant research in a follow-up study.
In summary, lncRNA MEG3, which possesses diagnostic
value for lymph node metastasis and FIGO staging, may serve as a
diagnostic marker and prognostic indicator for cervical cancer.
Furthermore, lymph node metastasis, FIGO stage III and IV, and a
low MEG3 level were revealed to be independent prognostic factors
for cervical cancer patients.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
SW wrote the manuscript, and analyzed and
interpreted the general data of patients. HZ performed PCR and was
responsible for observation indicator analysis. Both authors read
and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Medical Ethics
Committee of Huangshi Central Hospital. Patients who participated
in this research, provided signed informed consent and had complete
clinical data. Signed written informed consents were obtained from
the patients and/or guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Guo L, Lu X, Zheng L, Liu X and Hu M:
Association of long non-coding RNA HOTAIR polymorphisms with
cervical cancer risk in a Chinese population. PLoS One.
11:e01600392016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Hang D, Yin Y, Han J, Jiang J, Ma H, Xie
S, Feng X, Zhang K, Hu Z, Shen H, et al: Analysis of human
papillomavirus 16 variants and risk for cervical cancer in Chinese
population. Virology. 488:156–161. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Liang Y, Sun R, Li L, Yuan F, Liang W,
Wang L, Nie X, Chen P, Zhang L and Gao L: A functional polymorphism
in the promoter of MiR-143/145 is associated with the risk of
cervical squamous cell carcinoma in Chinese women: A case-control
study. Medicine (Baltimore). 94:e12892015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Li H, Wu X and Cheng X: Advances in
diagnosis and treatment of metastatic cervical cancer. J Gynecol
Oncol. 27:e432016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Jing H, Qu X, Liu L and Xia H: A novel
long noncoding RNA (lncRNA), LL22NC03-N64E9. 1, promotes the
proliferation of lung cancer cells and is a potential prognostic
molecular biomarker for lung cancer. Med Sci Monit. 24:43172018.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Xiao B, Huang Z, Zhou R, Zhang J and Yu B:
The prognostic value of expression of the long noncoding RNA
(lncRNA) small nucleolar RNA Host Gene 1 (SNHG1) in patients with
solid malignant tumors: A systematic review and meta-analysis. Med
Sci Monit. 24:5462–5472. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hao S, Yao L, Huang J, He H, Yang F, Di Y,
Jin C and Fu D: Genome-wide analysis identified a number of
dysregulated long noncoding RNA (lncRNA) in human pancreatic ductal
adenocarcinoma. Technol Cancer Res Treat. 17:15330346177484292018.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Fu XM, Guo W, Li N, Liu HZ, Liu J, Qiu SQ,
Zhang Q, Wang LC, Li F and Li CL: The expression and function of
long noncoding RNA lncRNA-ATB in papillary thyroid cancer. Eur Rev
Med Pharmacol Sci. 21:3239–3246. 2017.PubMed/NCBI
|
|
9
|
Misawa A, Takayama K, Urano T and Inoue S:
Androgen-induced long noncoding RNA (lncRNA) SOCS2-AS1 promotes
cell growth and inhibits apoptosis in prostate cancer cells. J Biol
Chem. 291:17861–17880. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Chen T, Xie W, Xie L, Sun Y, Zhang Y, Shen
Z, Sha N, Xu H, Wu Z, Hu H and Wu C: Expression of long noncoding
RNA lncRNA-n336928 is correlated with tumor stage and grade and
overall survival in bladder cancer. Biochem Biophys Res Commun.
468:666–670. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
He Y, Luo Y, Liang B, Ye L, Lu G and He W:
Potential applications of MEG3 in cancer diagnosis and prognosis.
Oncotarget. 8:73282–73295. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ghafouri-Fard S and Taheri M: Maternally
expressed gene 3 (MEG3): A tumor suppressor long non coding RNA.
Biomed Pharmacother. 118:1091292019. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Sun KX, Wu DD, Chen S, Zhao Y and Zong ZH:
lncRNA MEG3 inhibit endometrial carcinoma tumorigenesis and
progression through PI3K pathway. Apoptosis. 22:1543–1552. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wang J, Xu W, He Y, Xia Q and Liu S:
lncRNA MEG3 impacts proliferation, invasion, and migration of
ovarian cancer cells through regulating PTEN. Inflamm Res.
67:927–936. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Cui X, Jing X, Long C, Tian J and Zhu J:
Long noncoding RNA MEG3, a potential novel biomarker to predict the
clinical outcome of cancer patients: A meta-analysis. Oncotarget.
8:19049–19056. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Pecorelli S: Revised FIGO staging for
carcinoma of the vulva, cervix, and endometrium. Int J Gynaecol
Obstet. 105:103–104. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Migdalska-Sęk M, Karowicz-Bilińska A,
Pastuszak-Lewandoska D, Czarnecka KH, Nawrot E,
Domańska-Senderowska D, Kiszałkiewicz J and Brzeziańska-Lasota E:
Assessment of the frequency of genetic alterations (LOH/MSI) in
patients with intraepithelial cervical lesions with HPV infection:
A pilot study. Med Oncol. 33:512016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Peng L, Yuan X, Jiang B, Tang Z and Li GC:
lncRNAs: Key players and novel insights into cervical cancer.
Tumour Biol. 37:2779–2788. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
González-Quintana V, Palma-Berré L,
Campos-Parra AD, López-Urrutia E, Peralta-Zaragoza O, Vazquez-Romo
R and Pérez-Plasencia C: MicroRNAs are involved in cervical cancer
development, progression, clinical outcome and improvement
treatment response (Review). Oncol Rep. 35:3–12. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Landoni F, Colombo A, Milani R, Placa F,
Zanagnolo V and Mangioni C: Randomized study between radical
surgery and radiotherapy for the treatment of stage IB-IIA cervical
cancer: 20-year update. J Gynecol Oncol. 28:e342017. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kong TW, Piao X, Chang SJ, Paek J, Lee Y,
Lee EJ and Ryu HS: A predictive model for parametrial invasion in
patients with FIGO stage IB cervical cancer: Individualized
approach for primary treatment. Int J Gynecol Cancer. 26:184–191.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Qin R, Chen Z, Ding Y, Hao J, Hu J and Guo
F: Long non-coding RNA MEG3 inhibits the proliferation of cervical
carcinoma cells through the induction of cell cycle arrest and
apoptosis. Neoplasma. 60:486–492. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Chen X and Qu J: Long non-coding RNA MEG3
suppresses survival, migration, and invasion of cervical cancer.
Onco Targets Ther. 11:4999–5007. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Xiu YL, Sun KX, Chen X, Chen S, Zhao Y,
Guo QG and Zong ZH: Upregulation of the lncRNA Meg3 induces
autophagy to inhibit tumorigenesis and progression of epithelial
ovarian carcinoma by regulating activity of ATG3. Oncotarget.
8:31714–31725. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Zhang W, He W, Shi Y, Zhao J, Liu S, Zhang
F, Yang J, Xie C and Zhang Y: Aberrant TIMELESS expression is
associated with poor clinical survival and lymph node metastasis in
early-stage cervical carcinoma. Int J Oncol. 50:173–184. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Rofstad EK, Huang R, Galappathi K,
Andersen LM, Wegner CS, Hauge A, Gaustad JV and Simonsen TG:
Functional intratumoral lymphatics in patient-derived xenograft
models of squamous cell carcinoma of the uterine cervix:
Implications for lymph node metastasis. Oncotarget. 7:56986–56997.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Zhang J, Yao T, Wang Y, Yu J, Liu Y and
Lin Z: Long noncoding RNA MEG3 is downregulated in cervical cancer
and affects cell proliferation and apoptosis by regulating miR-21.
Cancer Biol Ther. 17:104–113. 2016. View Article : Google Scholar : PubMed/NCBI
|