Introduction
Gastric carcinoma (GC) is the fourth most common
cancer type worldwide and the third leading cause of
cancer-associated mortality (1).
According to an annual report on the status of cancer in China, GC
was recorded as the second most common cancer in terms of incidence
and mortality (2). As the majority
of patients are diagnosed at advanced stages with complications,
poorer prognoses, and limited treatment options, GC remains a major
clinical challenge (3). At present,
gastroscopy and biopsy remain the standard diagnostic methods in
populations at a high risk of GC. However, gastroscopy is difficult
to use as a first-line examination method due to its invasiveness
and cost, and limited medical resources, which limit its utility in
a large number of people. Therefore, a novel diagnostic strategy to
solve the aforementioned problems is urgently required. Plasma
tumor markers have become a common clinical screening method due to
their easy detection in recent years. Tumor markers, including
alpha-fetoprotein (AFP), carcinoembryonic antigen (CEA),
carbohydrate antigen (CA)125, and CA19-9 have been extensively used
as routine examination items in the diagnosis of GC (4,5), but
they have certain limitations under certain conditions. When these
markers are used alone in the diagnosis of GC, they tend to have
very low sensitivity and specificity. In recent years (6–8),
microRNAs (miRNAs) have worked as a DNA transcription regulator for
gene expression and have opened up a new use of tumor biomarkers
for early cancer diagnosis. For GC, miRNA-21, miRNA-218, miRNA-223,
miRNA-378 and miRNA-421 have been reported to function as tumor
biomarkers (9–11). Previously, our group reported that
miRNA-650 is significantly upregulated in GC plasma (unpublished
data). However, as an independent tumor marker, its diagnostic
efficacy may not be satisfactory.
A recent study reported that the use of AFP in
combination with CEA, CA125, and CAl9-9 may improve sensitivity for
the diagnosis of GC (12).
Therefore, we hypothesized that the combination of two types of
tumor markers may avoid inconsistencies and improve the sensitivity
of diagnostic rates. Therefore, in the present follow-up study, the
plasma levels of tumor markers CEA, CA125, CA211, CA50, and
miRNA-650 were detected in 90 patients with GC, 90 patients with
precancerous lesions (Pre) and 45 healthy controls. The aim of the
present study was to investigate the expression profiles of tumor
markers, CEA, CA125, CA211, CA50, and miRNA-650, and their
contribution to the diagnosis of gastric cancer.
Materials and methods
Study design
The present study consisted of three phases: The
screening phase, the candidate phase, and the validation phase
(Fig. S1). In the screening phase,
plasma samples were collected from 90 patients with GC, 90 patients
with Pre and 45 healthy controls, and the differential expression
levels of miRNA-650, CEA, CA125, CA211, and CA50 in the plasma
samples were statistically analyzed. In the candidate phase,
multiple logistic regression analysis was conducted to identify the
potential biomarkers. The results demonstrated that miRNA-650 and
CA211 were the markers for the prediction of the presence of GC.
Their diagnostic efficacy in GC and Pre was subsequently determined
using receiver operating characteristic (ROC) curves. To further
evaluate the diagnostic accuracy of the targeted biomarkers,
receiver-operating characteristic (ROC) curves were used to confirm
the diagnostic efficacy of the two markers in combination.
Patients
The present study consisted of 90 patients with GC
with a mean age of 65 (range, 36–89 years) years, including 68
males and 22 females, 90 Pre patients with a mean age of 61.5 years
(range, 29–88 years), including 48 males and 42 females, and 45
healthy controls with a mean age of 59 years (range, 39–80 years),
including 21 males and 24 females. All participants were recruited
from the Affiliated Liutie Central Hospital of Guangxi Medical
University between April 2014 and December 2018. Diagnoses of
gastric cancer and Pre were confirmed by histopathology. None of
the patients had undergone preoperative therapies, including
chemotherapy and radiotherapy. The tumor type and stage were
identified for patients with GC based on the Union of International
Cancer Control (UICC) Tumor-Node-Metastasis (TNM) system, 7th
edition (13). The histology of all
patients was evaluated according to World Health Organization (WHO)
criteria (14). Among the 90
patients with Pre, 80 had intestinal metaplasia, 6 had severe
atypical hyperplasia and 4 had chronic atrophic gastritis. A total
of 45 healthy subjects with normal biochemical indexes without a
previous history of tumors were selected as normal controls (NCs),
and their age, sex, and area of residence were matched with those
of the patients with GC or Pre. All participants or their guardians
provided written informed consent prior to participation in the
study. The Ethics Committee of the Affiliated Liutie Central
Hospital of Guangxi Medical University approved the present
study.
Sample collection and storage
Approximately 5 ml venous blood samples were
collected from the study participants in EDTA-anticoagulant tubes
(BD Biosciences) and centrifuged at 1,520 × g for 5 min at 4°C. The
plasma samples were transferred into RNase/DNase-free tubes and
frozen at −80°C for miRNA extraction. For conventional tumor marker
determination, the plasma samples were separated and kept at −20°C
until assayed.
Extraction of plasma total RNAs,
microRNA validation and reverse transcription-quantitative
polymerase chain reaction (RT-qPCR)
Total RNA was extracted from 200 µl plasma using a
Blood (serum/plasma) MicroRNA Extraction and Purification kit (spin
column; LN-0114B; Novland Co., Ltd.), according to the
manufacturer's protocol. The concentration and quality of RNA were
measured using the NanoQ Micro-Volume Spectrophotometer
(CapitalBio, Beijing, China). miR-16 was used as an internal
reference in the present study. The expression of the selected
plasma miRNA with an initial 2 µl template was determined using a
one-step Stemaim-it miR-RT-qPCR kit Quantitation (TaqMan Probes;
LK-0106B; Novland Co., Ltd.). The reaction was incubated in a
96-well plate under the following conditions: 45°C for 30 min for
reverse transcription, 94°C for 2 min for degeneration, 40 cycles
of 94°C for 15 sec, 55°C for 45 sec, and 72°C for 60 sec. The
primer sequences for PCR were as follows: miR-650 forward,
5′-AGAGGAGGCAGCGCTCT-3′ and reverse, 5′-CAGTGCGTGTCGTGGAGT-3′
(mature sequence of hsa-miR-650, 5′-AGGAGGCAGCGCUCUCAGGAC-3′).
Reference miRNA (hsa-miR-16): Forward,
5′-GTCGTATCCAGTGCAGGGTCCGAGTCGCACTGGATACGACCGCCAA-3′ and reverse,
5′-GTATCCAGTGCAGGGTCCGAGGT-3′. The expression levels of miR-650
were performed in the ABI-7500 PCR system and calculated by cycle
threshold (Ct) value with SDS 2.0 software (Applied Biosystems;
Thermo Fisher Scientific, Inc.). The relative expression of plasma
miRNA-650 was calculated using the 2−ΔΔCq method
(15), where ΔCq = Cq (miR-650)-Cq
(miR-16).
Conventional tumor markers
Conventional tumor markers were tested by
electrochemiluminescence immunoassay, according to the standard
procedure of Roche Company's kit, using the Roche E170 automatic
immunity analyzer (both Roche Diagnostic GmbH).
Statistical analysis
All statistical analyses and graphics were performed
using MedCalc statistical software v18.2.1(MedCalc Software Ltd.)
or GraphPad Prism 8.0 (GraphPad Software). Mean values of
quantitative variables were evaluated using Student's t-test or the
Mann-Whitney U test when the Student's t-test was not satisfied.
The diagnostic efficacy was assessed using ROC curve analysis. All
statistical tests were two-tailed, and P<0.05 was considered to
indicate a statistically significant difference.
Results
Differential expression levels of
potential biomarkers in the plasma of patients with GC or Pre and
health controls
A previous study demonstrated that oncogenic
miRNA-650 expression levels are significantly increased in GC
tissues compared with paired normal tissues (16). To assess whether miRNA-650 is a
potential circulating tumor marker for the early detection of GC,
RT-qPCR was performed on 90 patients with GC, 90 patients with Pre,
and 45 healthy controls. As shown in Table I, the expression levels of miRNA-650,
CEA, CA125, CA211, and CA50 were significantly increased in
patients with GC compared with patients with Pre and normal
controls (P<0.05), while no difference in miRNA-650, CEA and
CA125 expression were detected between the patients with Pre and
normal controls (P>0.05).
 | Table I.Differential expression levels of
biomarkers in plasma from patients with GC or Pre, and health
controls. |
Table I.
Differential expression levels of
biomarkers in plasma from patients with GC or Pre, and health
controls.
| Marker | n | GC, mean ± SD | n | Pre, mean ± SD | n | NC, mean ± SD | GC vs. Pre,
P-value | GC vs. NC,
P-value | Pre vs. NC,
P-value |
|---|
| CEA | 75 | 36.43±135.61 | 62 | 1.92±1.35 | 44 | 2.11±1.18 | <0.0001 | <0.0001 | 0.4706a |
| CA125 | 68 | 58.63±89.08 | 53 | 12.48±7.65 | 45 | 11.06±4.0 | 0.0075 | 0.0091 | 0.9363 |
| CA211 | 40 | 17.52±46.11 | 57 | 2.96±1.38 | 45 | 2.08±0.47 | 0.0011 | 0.0002 | <0.0001 |
| CA50 | 47 | 37.95±94.87 | 77 | 8.16±5.96 | 34 | 4.91±4.39 | 0.0456 | <0.0001 | 0.0101a |
| miR-650(ΔCt) | 90 | 1.17±2.91 | 90 | 2.94±3.02 | 45 | 2.87±0.77 | 0.0001a | <0.001 | 0.7186 |
Identification of candidate diagnostic
biomarkers for predicting GC
Next, whether the candidate biomarkers were able to
predict the presence of GC was assessed using multiple logistic
regression analysis. The results indicated that the increase in
miRNA-650 and CA211 levels were significantly associated with the
presence of GC (P<0.05; Table
II). The P-value of Hosmer-Lemeshow test was 0.979, indicating
that the model was a good fitted. Based on the ROC analysis, the
sensitivity, specificity, area under the ROC curve (AUC), Youden
index, accuracy, negative predictive value (NPV), positive
predictive value (PPV) and the cut-off values for detecting GC are
summarized in Table III. At a
cut-off 1.98, the AUC of miRNA-650 was 0.700 (moderate) with 93.3%
specificity and 62.2% sensitivity. CA211 had a greater AUC compared
with miRNA-650 for discriminating patients developing GC from
healthy controls (Fig. 1).
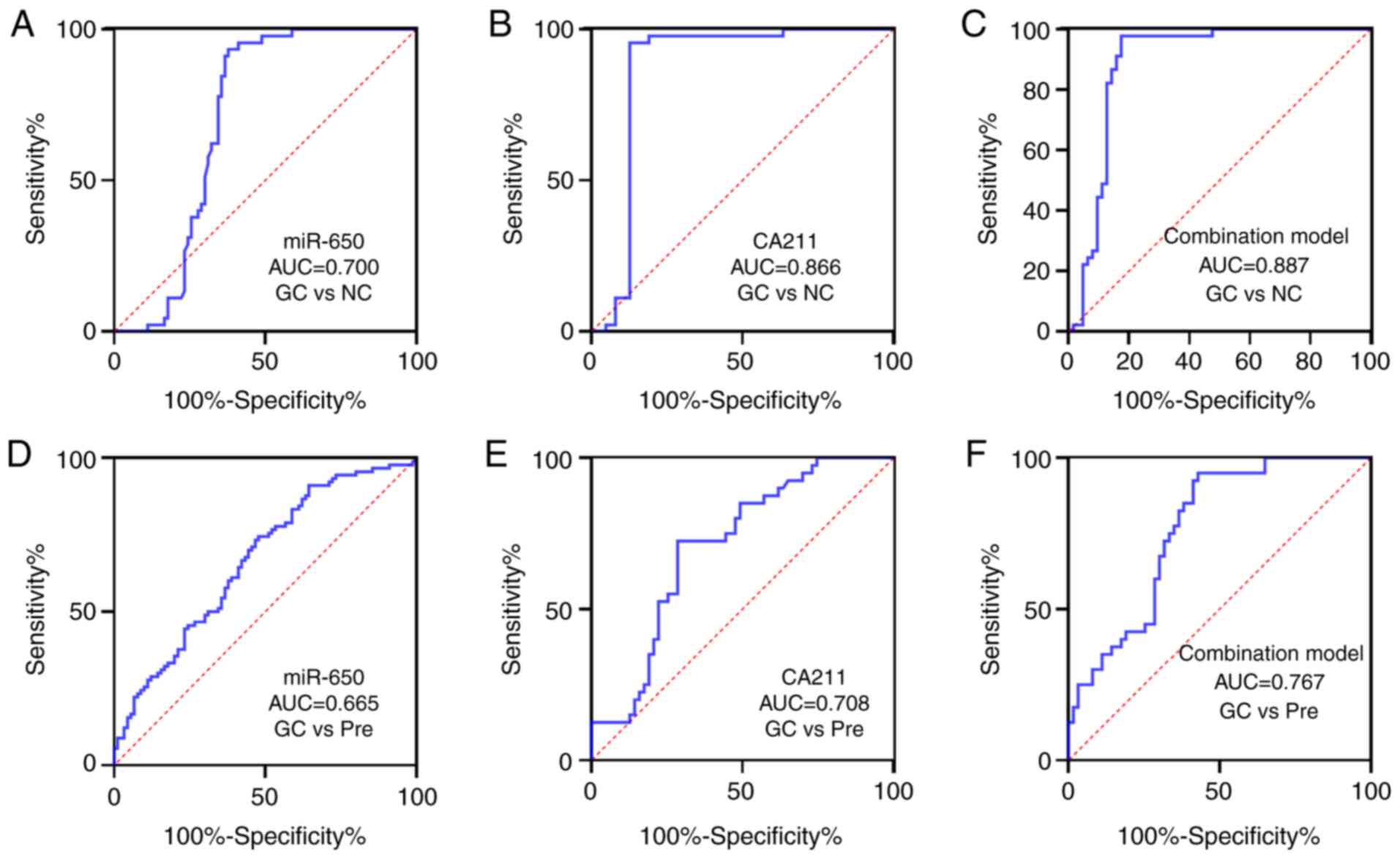 | Figure 1.AUC of markers, (A) miR-650, (B) CA211
and (C) combination model (miR-650 and CA211), to discriminate GC
from NC. AUC of markers, (D) miR-650, (E) CA211 and (F) combination
model (miR-650 and CA211), to discriminate GC from Pre. AUC, area
under the receiver operating characteristic curve; GC, gastric
carcinoma; NC, normal control; miR, microRNA; CA211, carbohydrate
antigen 211; Pre, precancerous lesions. |
| Table II.Candidate plasma markers independently
associated with the presence of GC. |
Table II.
Candidate plasma markers independently
associated with the presence of GC.
| Markers | Beta | S.E | OR | 95% CI | P-value |
|---|
| miR-650 (ΔCt) | −0.460 | 0.218 | 0.632 | 0.412–0.968 | 0.035 |
| CEA | 0.208 | 0.160 | 1.232 | 0.901–1.685 | 0.192 |
| CA211 | 1.326 | 0.450 | 3.767 | 1.558–9.106 | 0.003 |
| CA125 | 0.074 | 0.046 | 1.076 | 0.984–1.178 | 0.109 |
| CA50 | 0.155 | 0.088 | 1.168 | 0.982–1.389 | 0.079 |
| Table III.Performance of candidate metabolites
and blood markers for predicting GC. |
Table III.
Performance of candidate metabolites
and blood markers for predicting GC.
| Variable | AUC (95%CI) | Youden index | Cut-off | Sensitivity, % | Specificity, % | Accuracy, % | PPV, % | NPV, % | P-value |
|---|
| GC vs. Pre |
|
|
|
|
|
|
|
|
|
|
miR-650 | 0.665
(0.586–0.744) | 0.2267 | 1.06 | 52.2 | 74.4 | 63.3 | 24.04 | 68.51 | 0.0001 |
|
CA211 | 0.708
(0.608–0.807) | 0.4393 | 3.06 | 71.4 | 72.5 | 71.8 | 12 | 30.60 | 0.0004 |
|
Model | 0.767
(0.678–0.857) | 0.5214 | 0.671 | 57.1 | 95 | 71.8 | 3 | 39.40 | <0.0001 |
| GC vs. NC |
|
|
|
|
|
|
|
|
|
|
miR-650 | 0.700
(0.613–0.788) | 0.5556 | 1.98 | 62.2 | 93.3 | 72.5 | 4.01 | 43.21 | 0.0001 |
|
CA211 | 0.866
(0.785–0.947) | 0.8286 | 2.20 | 87.3 | 95.6 | 90.7 | 2.98 | 48.39 | <0.0001 |
|
Model | 0.887
(0.818–0.956) | 0.8032 | 0.49 | 82.5 | 97.7 | 88.8 | 1.99 | 47.99 | <0.0001 |
Diagnostic model using candidate
markers
To evaluate whether the combined application of
tumor markers may improve the diagnostic efficiency of GC, the
significant variables in univariate analysis were inserted into a
stepwise logistic regression analysis with consequent development
of a novel model that combined the most discriminatory factors
(miRNA-650 and CA211) for predicting GC. The model is illustrated
as follows: −0.277–0.588 × miR-650 (ΔCq) + 1.643×CA211 (ng/ml). The
AUC (95% CI) of the combination model was 0.887 (0.818–0.956) for
distinguishing patients with GC from healthy controls (sensitivity,
82.5% and specificity, 97.7%) and 0.767 (0.678–0.857) for gastric
precancerous lesions (sensitivity, 57.1% and specificity, 95%),
respectively (Table III; Fig. 1). When the two markers were combined,
there was a much stronger diagnostic value for GC (AUC=0.887;
P<0.0001) compared with when either was used separately.
Compared with the diagnostic efficiency of miRNA-650 alone,
combined detection improved the diagnostic efficiency of GC to a
certain extent (Table IV).
| Table IV.Diagnostic efficacy of tumor
markers. |
Table IV.
Diagnostic efficacy of tumor
markers.
|
| CA211 | miR-650 |
|---|
|
|
|
|
|---|
| ROC curve
comparison | Z | P-value | Z | P-value |
|---|
| Combination | 0.719 | 0.4722 | 2.868 | 0.0041 |
| miR-650 | 2.035 | 0.0418 | ‒ | ‒ |
Associations between miRNA-650 and
CA211 expression levels, and clinicopathological factors in
patients with GC
The associations between the expression of the
miRNA-650 and CA211, and clinicopathological parameters of patients
with GC were further elaborated. As shown in Table V, miRNA-650 expression levels were
not associated with the following characteristics of patients with
GC; age (P=0.1489), sex (P=0.7122), TNM stage (P=0.4769), or
histological type (P=0.2679). Similarly, the same result was
observed for CA211. The plasma levels of CA211 did not correlate
with age (P=0.0537), sex (P=0.9856), TNM stage
(P=0.1064) or histological type (P=0.7942).
| Table V.The associations between the
expression levels of miR-650 (2−ΔCt) and CA211 in plasma
and clinicopathological factors of patients with gastric
cancer. |
Table V.
The associations between the
expression levels of miR-650 (2−ΔCt) and CA211 in plasma
and clinicopathological factors of patients with gastric
cancer.
| Parameter | na |
miR-650a,
average fold-change ± SD |
P-valuea | nb | CA211b |
P-valueb |
|---|
| Age, median
years |
|
| 0.1489 |
|
| 0.0537 |
|
<60 | 30 | 23.23±48.69 |
| 11 | 2.795±1.25 |
|
|
≥60 | 60 | 6.83±10.09 |
| 29 | 3.89±40.95 |
|
| Sex |
|
| 0.7122 |
|
| 0.9856 |
|
Male | 68 | 15.04±31.14 |
| 31 | 4.63±44.67 |
|
|
Female | 22 | 26.15±62.19 |
| 9 | 3.09±57.66 |
|
| TNM stage |
|
| 0.4769 |
|
| 0.1064 |
| I | 22 | 15.72±25.86 |
| 6 | 0.67±1.86 |
|
| II | 8 | 13.21±26.40 |
| 5 | 3.09±0.78 |
|
|
III | 13 | 4.00±6.32 |
| 9 | 4.48±22.67 |
|
| IV | 47 | 14.94±33.96 |
| 20 | 3.89±58.55 |
|
| Histological
type |
|
| 0.6947 |
|
| 0.7942 |
| A | 63 | 3.42±47.52 |
| 28 | 3.415±45.56 |
|
|
Other | 27 | 4.01±10.43 |
| 12 | 3.26±1.33 |
|
Discussion
GC is one of the leading causes of cancer-associated
mortality due to late diagnosis and limited therapeutic strategies.
Circulating miRNAs are promising, noninvasive biomarkers for cancer
screening (17). The present study
reported an investigation on miR-650 expression in human GC. The
present study revealed that circulating miRNA-650, CEA, CA125,
CA211 and CA50 were differentially expressed in GC, compared with
healthy individuals. Furthermore, the increased expression levels
of miRNA-650 and CA211 were significantly associated with the
presence of GC. AUC analysis showed that plasma miRNA-650
association with CA211 improved the diagnostic efficiency of
GC.
The aberrant expression of miRNA-650 is associated
with the progression of glioma, breast cancer, colorectal cancer,
gastric cancer, osteosarcoma, and lung adenocarcinoma (18,19).
Previous studies have demonstrated that the positive expression of
miRNA-650 is a poor prognostic indicator in glioma (18). It has been reported that miRNA-650
may target ING4 to promote the development of GC (16). Lango-Chavarría et al (19) indicated that overexpression of
miRNA-650 is associated with the downregulated expression of tumor
suppressors, ING4 and NDRG2, in breast cancer (20). A clinical investigation on
osteosarcoma indicated that miRNA-650 serves an important role in
the synthesis of IL6, which is regulated by ING4 expression and
NF-κB signaling pathways (21).
Furthermore, a research study reported that upregulation of
miRNA-650 was correlated with enhanced malignant potential and poor
prognosis of patients with lung adenocarcinoma (22).
Different methods have been used to study the
expression profile of miRNAs in GC. Certain miRNAs, including
miR-21, miR-223, miR-218, miR-106 and miR-421 (19,23,24) have
been reported to exhibit significant upregulation or
downregulation. Notably, miR-106, miR-21 and miR-221 have been
reported as potential biomarkers for tumor diagnosis and prognosis
(25). The present study reported
that circulating miR-650 was highly expressed in patients with GC,
compared with those with Pre and healthy controls. However, whether
or not miRNA-650 is a potential biomarker for the diagnosis of GC
is yet to be reported. In order to address this, multiple logistic
regression and ROC curve analysis were performed. The results
indicated that the increase in miRNA-650 and CA211 expression
levels were significantly associated with the presence of GC. The
present study demonstrated that circulating miRNA-650 and CA211
levels were significantly associated with the presence of GC, and
the AUC of miR-650 alone was 0.70 for diagnosing GC, suggesting
that this miRNA may be a useful screening biomarker for GC.
As a classification of RNA, miRNAs are also unstable
and prone to degradation in the presence of RNA enzymes; therefore,
as an independent tumor marker, the diagnostic efficacy of miR-650
may not be satisfactory. Previous studies have demonstrated that
biomarker combinations may improve the diagnostic performance of a
model for various cancer types (26–28). To
further investigate this, a predictive logistic regression analysis
model called the Cancer Screening Model for diagnosing GC was
developed. This screening model had an AUC of 0.887 and indicated
that a combination of plasma miR-650 and CA211 was an effective and
novel diagnostic biomarker panel in the diagnosis of GC.
Prior to the present study, very little was known
regarding circulating miR-650 expression in GC, and its correlation
with the clinicopathological features of these patients. To address
these questions, miR-650 expression levels and the
clinicopathological characteristics of 90 patients with GC were
examined, but there was no association between miR-650 expression
and sex, histological type, differentiation grade or TNM stage.
However, whether miR-650 is abnormally expressed in the early
stages of GC and has significant value in the early diagnosis of GC
requires further study.
Although the results are novel, the present study
has certain limitations. To begin with, the TNM stages were not
divided into T1a and T1b, so there was no data relating to T1b.
Therefore, the significance of miR-650 in the early diagnosis of GC
requires further study. Another potential limitation of the present
study was that no specific genotyping was performed in the patients
with GC, and the miRNA expression may differ between gene subtypes.
Furthermore, the results of the present study may reflect biases
inherent in the acquisition of such clinical data; therefore, using
more external bioinformatics data for an external validation may be
a future direction.
In conclusion, miRNA-650, which is upregulated in
GC, may be a novel early diagnostic marker for GC. Furthermore, a
new screening model was developed in the present study, which
patients may be more willing to accept for detecting GC.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
The present study was funded by the National Natural
Science Foundation of China (grant no. 81760501); The Natural
Science Foundation of the Guangxi Zhuang Autonomous Region (grant
nos. 2017GXNSFAA198041 and 2018GXNSFAA294055); Liuzhou Scientific
Research and Technological Development Programs (grant no.
2014JC010); The Self-Funded Research Project of Guangxi Zhuang
Autonomous Region health and Family Planning Commission (grant no.
Z2014613).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author upon reasonable
request.
Authors' contributions
JC conceived, designed and performed the
experiments. JC, LW, YFS, CL and XC analyzed the data. LW, JD, GP,
CH and ZW contributed toward the collection of clinical samples,
and performed experiments and data analysis. JC wrote the
manuscript. YQS analysed and interpreted the data, was involved in
drafting and revision of the manuscript and gave final approval of
the version to be published. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
The present study was approved by The Ethical Review
Committee of Affiliated Liutie Central Hospital of Guangxi Medical
University (Liuzhou, China). All patients provided written informed
consent.
Patient consent for publication
All patients provided written informed consent for
publication.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Siegel R, Naishadham D and Jemal A: Cancer
statistics, 2013. CA Cancer J Clin. 63:11–30. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chen W, Zheng R, Baade PD, Zhang S, Zeng
H, Bray F, Jemal A, Yu XQ and He J: Cancer statistics in China,
2015. CA Cancer J Clin. 66:115–132. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Thrift AP and El-Serag HB: Burden of
gastric cancer. Clin Gastroenterol Hepatol. 18:534–542. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Feng F, Tian Y, Xu G, Liu Z, Liu S, Zheng
G, Guo M, Lian X, Fan D and Zhang H: Diagnostic and prognostic
value of CEA, CA19-9, AFP and CA125 for early gastric cancer. BMC
Cancer. 17:7372017. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wang YK, Shen L and Zhang XT: The
prognosis and clinicopathological characteristics of 70 gastric
cancer patients with elevated serum AFP. Zhonghua Zhong Liu Za Zhi.
39:514–517. 2017.PubMed/NCBI
|
|
6
|
Han Z, Li Y, Zhang J, Guo C, Li Q, Zhang
X, Lan Y, Gu W, Xing Z, Liang L, et al: Tumor-derived circulating
exosomal miR-342-5p and miR-574-5p as promising diagnostic
biomarkers for early-stage lung adenocarcinoma. Int J Med Sci.
17:1428–1438. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Satapathy S, Kumar C and Singh RK:
MicroRNAs as key regulators of ovarian cancers. Cell Med.
11:21551790198738492019. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hu M, Xiong S, Chen Q, Zhu S and Zhou X:
Novel role of microRNA-126 in digestive system cancers: From bench
to bedside. Oncol Lett. 17:31–41. 2019.PubMed/NCBI
|
|
9
|
Li BS, Zhao YL, Guo G, Li W, Zhu ED, Luo
X, Mao XH, Zou QM, Yu PW, Zuo QF, et al: Plasma microRNAs, miR-223,
miR-21 and miR-218, as novel potential biomarkers for gastric
cancer detection. PLoS One. 7:e416292012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Liu H, Zhu L, Liu B, Yang L, Meng X, Zhang
W, Ma Y and Xiao H: Genome-wide microRNA profiles identify miR-378
as a serum biomarker for early detection of gastric cancer. Cancer
Lett. 316:196–203. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Chen J, Wu L, Sun Y, Yin Q, Chen X, Liang
S, Meng Q, Long H, Li F, Luo C and Xiao X: Mir-421 in plasma as a
potential diagnostic biomarker for precancerous gastric lesions and
early gastric cancer. PeerJ. 7:e70022019. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
He CZ, Zhang KH, Li Q, Liu XH, Hong Y and
Lv NH: Combined use of AFP, CEA, CA125 and CAl9-9 improves the
sensitivity for the diagnosis of gastric cancer. BMC Gastroenterol.
13:872013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Catalano V, Sisti V, Spada D, Graziano F,
Giordani P, Alessandroni P, Baldelli A, Casadei V, Rossi D,
D'Emidio S, et al: The 7th edition of the tnm classification for
gastric cancer and a proposal of a new classification for D2
gastrectomy. Ann Oncol. 23:2012. View Article : Google Scholar
|
|
14
|
Bosman FT, Carneiro F, Hruban RH and
Theise ND: WHO Cassification of Tumours of the Digestive System. 3.
4th. World Health Organization Classification of Tumours; Lyon:
2010
|
|
15
|
Pan J, Zhou C, Zhao X, He J, Tian H, Shen
W, Han Y, Chen J, Fang S, Meng X, et al: A two-miRNA signature
(miR-33a-5p and miR-128-3p) in whole blood as potential biomarker
for early diagnosis of lung cancer. Sci Rep. 8:166992018.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Zhang X, Zhu W, Zhang J, Huo S, Zhou L, Gu
Z and Zhang M: MicroRNA-650 targets ING4 to promote gastric cancer
tumorigenicity. Biochem Biophys Res Commun. 395:275–280. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Santangelo A, Tamanini A, Cabrini G and
Dechecchi MC: Circulating microRNAs as emerging non-invasive
biomarkers for gliomas. Ann Transl Med. 5:2772017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Sun B, Pu B, Chu D, Chu X, Li W and Wei D:
MicroRNA-650 expression in glioma is associated with prognosis of
patients. J Neurooncol. 115:375–380. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Lango-Chavarría M, Chimal-Ramírez GK,
Ruiz-Tachiquín ME, Espinoza-Sánchez NA, Suárez-Arriaga MC and
Fuentes-Pananá EM: A 22q11.2 amplification in the region encoding
microRNA-650 correlates with the epithelial to mesenchymal
transition in breast cancer primary cultures of Mexican patients.
Int J Oncol. 50:432–440. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Feng L, Xie Y, Zhang H and Wu Y:
Down-regulation of NDRG2 gene expression in human colorectal cancer
involves promoter methylation and microRNA-650. Biochem Biophys Res
Commun. 406:534–538. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Yun JH, Moon S, Lee HS, Hwang MY, Kim YJ,
Yu HY, Kim Y, Han BG, Kim BJ and Kim JM: MicroRNA-650 in a copy
number-variable region regulates the production of interleukin 6 in
human osteosarcoma cells. Oncol Lett. 10:2603–2609. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Huang JY, Cui SY, Chen YT, Song HZ, Huang
GC, Feng B, Sun M, De W, Wang R and Chen LB: MicroRNA-650 was a
prognostic factor in human lung adenocarcinoma and confers the
docetaxel chemoresistance of lung adenocarcinoma cells via
regulating Bcl-2/Bax expression. PLoS One. 8:e726152013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Zhang Z, Li Z, Gao C, Chen P, Chen J, Liu
W, Xiao S and Lu H: miR-21 plays a pivotal role in gastric cancer
pathogenesis and progression. Lab Invest. 88:1358–1366. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Peng Q, Shen Y, Lin K, Zou L, Shen Y and
Zhu Y: Comprehensive and integrative analysis identifies
microRNA-106 as a novel non-invasive biomarker for detection of
gastric cancer. J Transl Med. 16:1272018. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Ishiguro H, Kimura M and Takeyama H: Role
of microRNAs in gastric cancer. World J Gastroenterol.
20:5694–5699. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Sun L, Tu H, Chen T, Yuan Q, Liu J, Dong N
and Yuan Y: Three-dimensional combined biomarkers assay could
improve diagnostic accuracy for gastric cancer. Sci Rep.
7:116212017. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Cheng J, Yang A, Cheng S, Feng L, Wu X, Lu
X, Zu M, Cui J, Yu H and Zou L: Circulating miR-19a-3p and
miR-483-5p as novel diagnostic biomarkers for the early diagnosis
of gastric cancer. Med Sci Monit. 26:e9234442020. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Alemar B, Izetti P, Gregório C, Macedo GS,
Castro MA, Osvaldt AB, Matte U and Ashton-Prolla P: miRNA-21 and
miRNA-34a Are potential minimally invasive biomarkers for the
diagnosis of pancreatic ductal adenocarcinoma. Pancreas. 45:84–92.
2016. View Article : Google Scholar : PubMed/NCBI
|














