Introduction
Tumors expressing PD-L1 bind to PD-1, an
immunoinhibitory receptor expressed on T cells, and inhibit T
cell-mediated immune responses (1).
Nivolumab (anti-PD-1 antibody) binds to PD-1 and blocks its
PD-1/PDL-1 interaction. Nivolumab has led to extremely significant
results in patients with terminally-progressed carcinomas who can
be administered several treatments. However, because nivolumab is
reported to have a low cure rate of 20–30%, many researchers have
been searching for biomarkers that can be used to distinguish
responders from non-responders. T cell exhaustion, a state of T
cell dysfunction characterized by reduced cytokine production,
impaired killing, and hypo-proliferation, was first characterized
in chronic lymphocytic choriomeningitis virus (LCMV) infection
(2,3). These T cell dysfunctions of exhausted T
cells are inversely correlated with decreased mitochondrial
function (3), which is caused by
progressive loss of peroxisome proliferator-activated receptor-γ
coactivator 1α (PGC1α), a regulator of mitochondrial replication
that is controlled by a variety of signaling pathways (Akt,
p38-MARK, AMPK, SIRT1, PRMT1) (4),
likely driven by chronic antigen exposure in the tumor
microenvironment (5). Honjo et
al, reported that mitochondrial activation chemicals such as
Bezafibrate, an activator of PGC1-α, synergize with nivolumab for T
cell-dependent antitumor activity (6), suggesting that T cells with severe
metabolic insufficiency equivalent to exhausted T cells are highly
involved in low clinical outcomes of nivolumab and reinvigoration
of exhausted T cells is incompletely achieved by checkpoint
blockade such as nivolumab only, and consequently, metabolic
reprogramming must be preceded for enhancement of checkpoint
blockade (5). Recently, we reported
that the proportion of PD-1+terminal CD8+ T
cells containing PDT+ and PDT- (exhausted CD8+ T cells)
in the peripheral blood of colorectal cancer patients was reduced
by hydrogen gas, an activator of PGC1-α, leading to better
prognosis (7). Furthermore, enforced
expression of PGC1α in exhausted T cells results in superior
antitumor T cell function (5,8). These
reports indicate that mitochondrial activation chemicals,
especially an activator of PGC1-α, such as hydrogen gas and
Bezafibrate, enhance nivolumab outcomes by restoring exhausted T
cells.
T cell immunoglobulin and mucin domain-containing
protein 3 (Tim-3) is a type I membrane glycoprotein. Its expression
can be found on terminally differentiated Th1 cells and innate
immune cells (9–11). Recently, Tim-3-expressing
PD-1+ terminal CD8+ T cells (PDT+)
were reported to have the most severe exhaustive phenotype and most
suppressive function compared with PD-1+
Tim-3−terminal CD8+ T cells (PDT−)
(12), suggesting that mitochondrial
dysfunction of PDT+ is more severe than that of
PDT− and thus may be more responsible for nivolumab's
clinical effects than exhausted T cells expressing only PD-1. Some
of Tim-3-expressing T cells have been recognized as senescent T
cells characteristic of their irreversible dysfunction, and so it
is doubtful whether hydrogen gas can restore PDT+ into active
CD8+ T cells like the PD-1+terminal
CD8+ T cells as described before. Restoring exhausted T
cells, including PDT+, represents an inspiring strategy
in cancer treatment with nivolumab and has yielded promising
results. In the patients with advanced carcinomas, exhausted T
cells are increased, resulting in low effectiveness of nivolumab
(about 20–30% response rate), because of their dysfunctional
cytotoxic activity. Hydrogen gas can restore the exhausted T cells
into active T cells, which will bring a higher clinical response
rate of nivolumab in the advanced cancer patients. Therefore, such
restoration of exhausted CD8+ T cells by hydrogen gas
has become a significant breakthrough in cancer immunotherapy with
nivolumab.
Molecular hydrogen (i.e., dihydrogen or
H2) was previously reported to efficiently neutralize
hydroxyl radicals (•OH), but not other reactive oxygen species,
such as superoxide anions (O2•-), hydrogen peroxide
(H2O2), and nitric oxide (NO•) (13). As hydrogen gas is reported to
activate PGC1-α (14), it is also
one of the mitochondrial activation mediators. Recently, we
reported that hydrogen gas could restore exhausted CD8+
T cells to active CD8+ T cells via mitochondrial
activation (7). This implies that
hydrogen gas may improve the clinical effects of nivolumab, as
reported by Chamoto et al (6). However, there is no direct evidence
that hydrogen gas activates mitochondria. Therefore, we have been
searching for methods that clinically and easily measure
mitochondrial function. Recently, coenzyme Q10 (CoQ10), a key
enzyme of the mitochondrial respiratory chain, became easily and
clinically measurable through the use of peripheral blood (15). CoQ10 transfers electrons from
complexes I and II into complex III, which is a critical process
for ATP production. CoQ10 supplementation was reported to activate
mitochondrial function (16), which
is reported to depend on the CoQ10 concentration in peripheral
blood (17). Such findings suggest
that the concentration of CoQ10 in peripheral blood is available as
a marker of mitochondrial function. Therefore, we sought to use
CoQ10 as a marker of mitochondrial function in this study.
Herein, we investigated whether hydrogen gas, an
activator of PGC1-α, is able to enhance the clinical effect of
nivolumab, and what its mechanism might be. Further, we
investigated whether the CoQ10 concentration in the peripheral
blood of cancer patients is available as a marker of mitochondrial
function.
Materials and methods
Patients, sample collection and
processing
All participants provided written informed consent
prior to enrollment. The study protocol was approved by the
Institutional Review Boards at the Tamana Regional Health Medical
Center (Tamana, Kumamoto, Japan). All methods and procedures were
consistent with Good Clinical Practice, the Declaration of
Helsinki, and local laws. In this prospective cohort study, 56
patients with histologically- and clinically-diagnosed stage IV
lung carcinoma, based on the unified Tumor-Node-Metastasis criteria
(18), were enrolled at Tamana
Regional Health Medical Center between July 2016 and July 2018. The
specific exclusion and inclusion criteria were: A performance
status of ≥2 and <2, hemoglobin of <8.0 and ≥8.0, WBC of
<2,000 and ≥2,000, platelet of <60,000 and ≥60,000,
respectively. Among the patients with lung carcinoma, 22 were men,
and 34 were women, ranging in age from 33 to 84 years (mean age of
63.6±1.88 years). Patients were continuously treated with nivolumab
(1 mg/kg) every 2 weeks. Patients also inhaled hydrogen gas 3 h
daily at their home through a cannula or mask that they rented or
purchased and connected to a Hycellvator ET 100 (Helix Japan, Co.,
Ltd.). None of the patients reported any complaints regarding the
daily 3-h hydrogen gas inhalation. Peripheral blood (10 ml) was
collected from patients prior to and every month after treatment
with hydrogen gas.
When the total patients number reached to about 30,
we found that the survival rate and QOL (Quality of life) of the
patients treated with both nivolumab and hydrogen gas were quite
better that those with nivolumab only. Therefore, then, we are
sorry to select the combined treatment of nivolumab and hydrogen
gas more preferably than the treatment of nivolumab only. That is
why the number of the patients treated with combined treatment was
more than those with nivolumab only. However, this result strongly
suggest that the combined treatment of nivolumab and hydrogen gas
is more clinically effective than the treatment with nivolumab
only.
Hydrogen gas treatment
The Hycellvator ET 100 (Helix Japan, Co., Ltd.)
generates 1.67 l/ min hydrogen gas (hydrogen purity, 99.99%) by
electrolysis. As measured by gas chromatography at Kureha Special
Laboratory, the gas generated 680,000 ppm hydrogen gas and 320,000
ppm oxygen gas. Recently, hydrogen gas inhalation was used in
patients with post-cardiac arrest syndrome, and adverse events were
not observed (19). Similarly, no
adverse events were observed in the 56 patients who inhaled
hydrogen gas for up to a maximum of 60 months in the present
study.
Antibodies and fluorescence-activated
cell sorting (FACS)
Briefly, Ficoll-Hypaque solution (20 ml) was placed
into a 50-ml conical centrifuge tube using a sterile pipette.
Anti-coagulated blood (10 ml) mixed with an equal volume of PBS was
then slowly layered over the Ficoll-Hypaque solution by gently
pipetting down the side of the tube. Samples were then centrifuged
at 400 × g and 22°C for 30–40 min. Mononuclear cells that
accumulated at the interface between the plasma (upper) and
Ficoll-Hypaque layers (bottom) were carefully recovered using a
Pasteur pipette and transferred to a 15-ml conical tube. Cells were
then analyzed on a BD FACSCalibur (Nippon Becton Dickinson) with BD
CellQuest software (v5.1) using anti-CD57 conjugated to fluorescein
isothiocyanate (clone NK-1; cat. no. 347393; Nippon Becton
Dickinson), mouse anti-human CD27 conjugated to APC (clone M-T271;
cat. no. B09983; Beckman Coulter), mouse anti-human PD-1 conjugated
to PE (clone EH12.1; cat. no. 557946; Nippon Beckton Dickinson),
mouse anti-human Tim-3 conjugated to PE (clone FAB2365C; cat. no.
344823; R&D system), and mouse anti-human CD8 conjugated to
PerCP (clone SK1; cat. no. 347314) (BD Pharmingen). The mixtures
were incubated at 4 C for 30 min after blocking with 1% γ-globulin
for 15 min at 4°C. To determine the independent contributions of
each marker to PFS and OS, FACS data were used to stratify patients
based on the proportion of early, intermediate, terminal, and end
PD-1+ and PD-1− CD8+ T cells. All
blood samples obtained from patients were transferred to SRL, Inc.
for lymphocyte separation and flow cytometry; the status of the
laboratory data, reliable protocols, and flow cytometry assays were
certified by SRL, Inc., one of the most reliable clinical
laboratory centers in Japan. The flow cytometry data were analyzed
using SPSS v19.0 for Windows (IBM Corp.).
Measurement of Coenzyme Q10
Serum ubiquinol content was determined by LC/MS/MS
(outsourced to Kaneka Techno Research Corporation). Briefly, 0.7 ml
of isopropanol was added to 0.1 ml of serum. The obtained mixture
was then centrifuged, and the resulting supernatant was filtered
through a membrane filter. The obtained filtrate was then used as
the sample for LC/MS/MS, which was performed on a Triple Quad5500
(AB SCIEX Company).
Study endpoints and assessments
Primary endpoints were PFS and OS time, and these
were measured from the date of randomization to the first
recurrence and mortality, regardless of cause, respectively.
Patients were monitored by dynamic computed tomography or magnetic
resonance imaging every 3 months from baseline up to 60 months, and
every 3–6 months thereafter. Two independent and blinded
radiologists, each with >5 years of experience, reviewed all
scans at each site. When there was discord, the radiologists
reviewed the images to reach the same conclusion following a
discussion. Adverse events were classified and graded every 2
months according to the Common Terminology Criteria for Adverse
Events v3.0 (National Cancer Institute) (20) from the day of consent until the end
of the study, at least 30 days after treatment. Multiple events
were counted once for each patient, of which the most severe was
noted.
Statistical analysis
Significant differences between two groups were
found using the (Mann-Whitney test). For persistent abnormal
distribution, the linear correlation between two continuous
variables was tested using Spearman's correlation coefficient.
Statistical analysis of Tables
I–III was performed using
χ2 test for comparing two groups. The receiver operating
characteristic (ROC) analysis was used to determine the optimal
cut-off values for continuous variables. The ROC curve shows
1-specificity on the x-axis and sensitivity on the y-axis. The
optimal cut-off value was calculated by maximizing the sensitivity
and specificity across various cut-off points on the ROC curve. The
probability of survival was estimated by the Kaplan-Meier method,
and differences in survival were evaluated by the log-rank test.
Prognostic factors were tested by univariate and multivariate Cox
regression analyses. All statistical analyses were performed using
SPSS version 19.0 for Windows (IBM Corp.). P<0.05 was considered
to indicate a statistically significant difference.
 | Table I.Comparison of clinicopathological
data between patients treated with Hydrogen gas + Nivolumab and
Nivolumab only. |
Table I.
Comparison of clinicopathological
data between patients treated with Hydrogen gas + Nivolumab and
Nivolumab only.
| Factor | Hydrogen gas +
Nivolumab (n=42) | Nivolumab only
(n=14) | P-value |
|---|
| Age | 63.6±12.2 | 62.7±8.68 | NS |
| Sex |
|
| NS |
|
Male | 14 | 8 |
|
|
Female | 28 | 6 |
|
| T factor |
|
| NS |
| T1 | 2 | 1 |
|
| T2 | 10 | 3 |
|
| T3 | 16 | 5 |
|
| T4 | 8 | 4 |
|
| Tx | 6 | 1 |
|
| N factor |
|
| NS |
| N0 | 6 | 2 |
|
| N1 | 12 | 2 |
|
| N2 | 6 | 3 |
|
| N3 | 8 | 3 |
|
| Nx | 10 | 4 |
|
| M factor |
|
| NS |
| M0 | 0 | 0 |
|
|
M1a | 30 | 10 |
|
|
M1b | 12 | 4 |
|
| Histology |
|
| NS |
|
Adenocarcinoma | 30 | 10 |
|
|
SCC | 12 | 4 |
|
| Table III.Comparison of clinicopathological
data between patients with high- and low-level of Coenzyme Q10. |
Table III.
Comparison of clinicopathological
data between patients with high- and low-level of Coenzyme Q10.
|
| Coenzyme Q10 |
|
|---|
|
|
|
|
|---|
| Factor | High (n=22) | Low (n=13) | P-value |
|---|
| Age | 60.5±11.4 | 66.8±13.7 | NS |
| Sex |
|
| NS |
|
Male | 8 | 4 |
|
|
Female | 14 | 9 |
|
| T factor |
|
| NS |
| T1 | 1 | 1 |
|
| T2 | 4 | 1 |
|
| T3 | 8 | 6 |
|
| T4 | 7 | 4 |
|
| Tx | 2 | 1 |
|
| N factor |
| N0 | 2 | 1 |
|
| N1 | 5 | 3 |
|
| N2 | 9 | 6 |
|
| N3 | 3 | 2 |
|
| Nx | 3 | 1 |
|
| M factor |
|
| NS |
| M0 | 0 | 0 |
|
|
M1a | 14 | 9 |
|
|
M1b | 8 | 4 |
|
| Histology |
|
| NS |
|
Adenocarcinoma | 14 | 10 |
|
|
SCC | 8 | 3 |
|
Results
Hydrogen gas extends the OS of
patients treated with hydrogen gas and nivolumab
Of the patients with stage IV lung cancer, 42 were
treated with hydrogen gas and nivolumab (HGN), while 14 were
treated with nivolumab only (NO). Table
I shows that a significant difference was not found in the
clinico-pathological parameters such as age, gender, T (Tumor)
factor (18), N (Node) factor
(18), M (Metastasis) factor
(18), and histology between the two
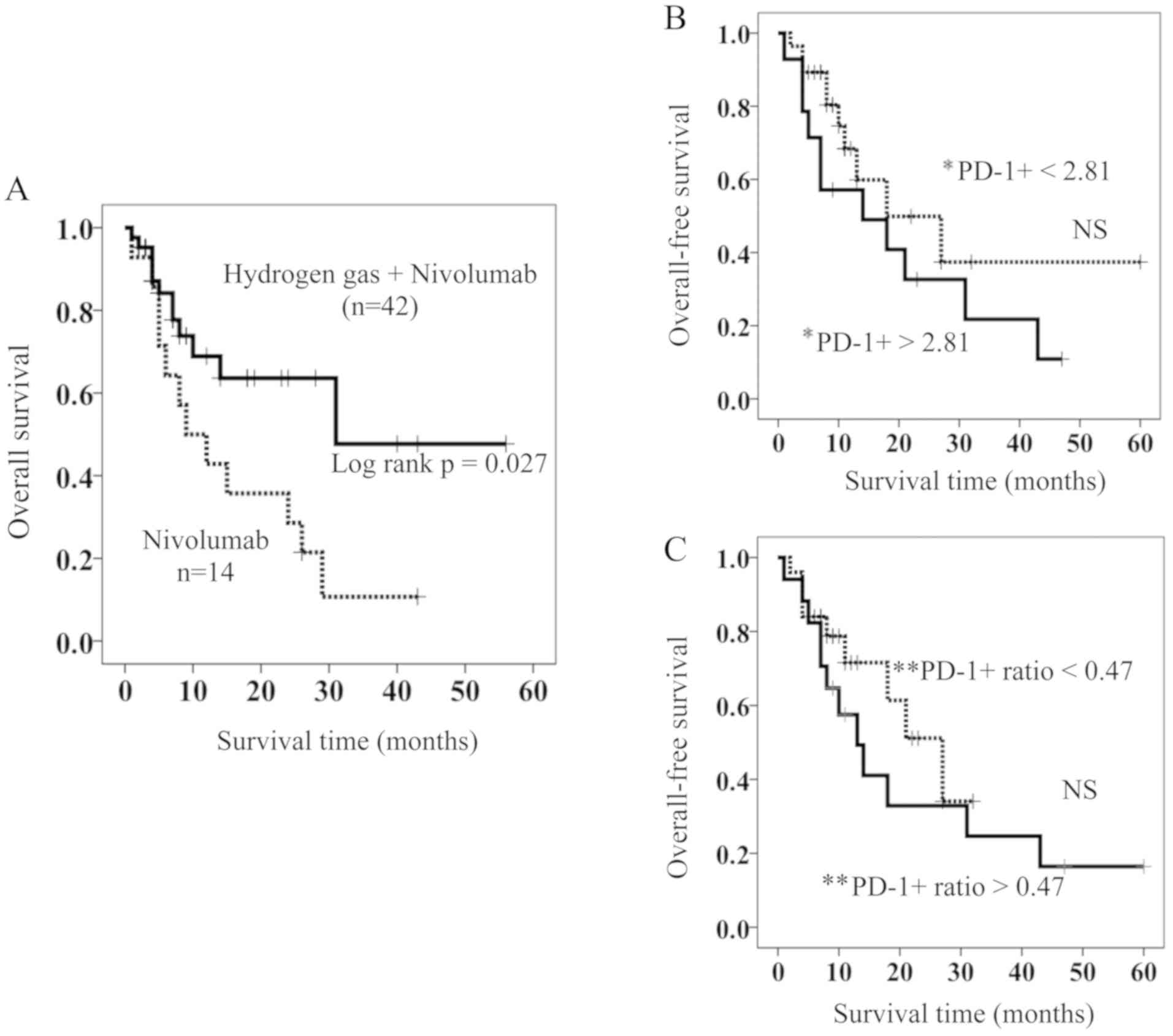
groups. Kaplan-Meyer analysis showed that the HGN-treated patients
had a significantly longer OS than those treated with NO (Fig. 1A). Median survival time (MST) for the
HGN-treated patients was 28 months, a length that is approximately
3-fold longer than that for NO-treated patients (MST 9 months)
(Fig. 1A).
Prognostic factors of HGN-treated
patients
It was recently reported that
PD-1+terminal CD8+ T cells are an independent
poor prognostic factor of colorectal cancer patients and hydrogen
gas brought them a better prognosis by reducing
PD-1+terminal CD8+ T cells probably and
increasing PD-1−terminal CD8+ T cells.
However, in the HGN-treated patients, the proportion of
PD-1+terminal CD8+ T cells and the change in
the rate of PD-1+terminal CD8+ T cells after
vs. before HGN (PD-1+ ratio) were not involved in overall survival
(Fig. 1B and C). As described in the
introduction, PD-1+terminal CD8+ T cells
(exhausted CD8+ T cells) are supposed to contain the
most exhausted CD8+ T cells
(PD-1+Tim-3+terminal CD8+ T cells,
PDT+) as well as
PD-1+Tim-3−terminal CD8+ T cells
(PDT-), and so we sought to determine whether the expression of
Tim-3 and/or PD-1 on populations of CD8+ T cells in
differentiation pathways is associated with their OS.
Cox proportional-hazards regression analysis was
used to identify PD-1+/− Tim-3+/−
CD8+ T cell subsets and the clinico-pathological factors
(age, sex, primary tumor (T), regional lymph nodes (N), distant
metastasis (M), and histology) associated with OS in patients with
stage IV lung cancer. By performing a univariate analysis of 17
factors, PD-1+Tim-3−intermediate
CD8+ T cells (HR, 1.035; 95% CI, 1.008–1.062; P=0.009),
PD-1+Tim-3+intermediate CD8+ T
cells (HR, 2.504; 95% CI, 1.472–4.262; P=0.001),
PD-1+terminal CD8+ T cells (HR, 1.092; 95%
CI, 1.005–1.188; P=0.038),
PD-1+Tim-3−terminal CD8+ T cells
(HR, 1.089; 95% CI, 1.013–1.170; P=0.021), and PDT+ (HR,
49.97; 95% CI, 6.369–392.1; P<0.0001) was found to be
significantly associated with poorer OS, while PD-1
Tim-3−intermediate CD8+ T cells (HR, 0.966;
95% CI, 0.942–0.991; P=0.008), PD-1−
Tim-3−terminal CD8+ T cells (HR, 0.922; 95%
CI, 0.8680.980; P=0.009), and CoQ10 (HR, 0.717; 95% CI,
0.541–0.949; P=0.020) with better OS. On the other hand, four types
of PD-1−Tim-3+early-, intermediate-,
terminal-, and end-diff. CD8+ T cells were not significantly
associated with OS. Based on multivariate Cox regression, terminal
PDT+ was more strongly associated with OS than others
(HR, 27.16; 95% CI, 3.152–233.9; P=0.003), and CoQ10 showed a
tendency to be associated with better prognosis (HR, 0.780; 95% CI,
0.602–1.012; P=0.062).
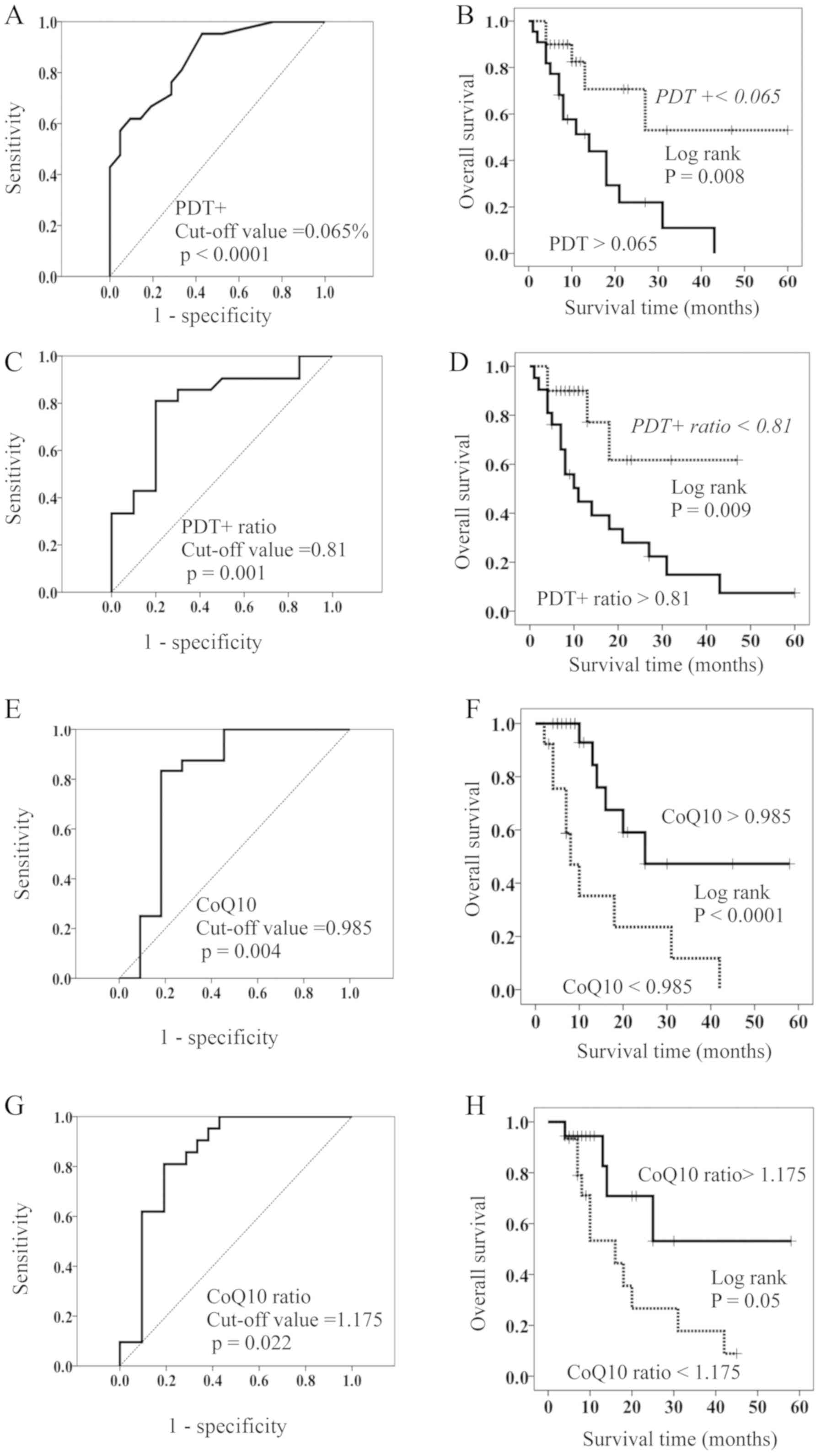
Based on the above results, patients were stratified
as having high and low PDT+ by using a cut-off value of 0.065% for
OS (ROC (Receiver Operating Characteristic) curve; AUC (Area Under
the curve)=0.858, Sensitivity=76.2%, Specificity=71.4%) (Fig. 2A). There were no significant
differences in the clinico-pathological factors between patients
with high and low PDT+ (Table II);
the resulting stratified OS curves are plotted in Fig. 2B. The curves demonstrated that
patients with low PDT+ had a significant increase in OS compared to
those with high PDT+. MST of OS was 11 months for patients with
high PDT+ and 60 months for those with low PDT+ (Fig. 2B).
| Table II.Comparison of clinicopathological
data between patients with high- and low-level of
PD-1+Tim-3+terminal CD8+ T cells
(PDT+). |
Table II.
Comparison of clinicopathological
data between patients with high- and low-level of
PD-1+Tim-3+terminal CD8+ T cells
(PDT+).
|
|
Tim-3+PD-1+terminal
CD8+ T cells (PDT+) |
|
|---|
|
|
|
|
|---|
| Factor | High (n=18) | Low (n=24) | P-value |
|---|
| Age | 62.7±14.3 | 64.3±10.57 | NS |
| Sex |
|
| NS |
|
Male | 5 | 9 |
|
|
Female | 13 | 15 |
|
| T factor |
|
| NS |
| T1 | 1 | 1 |
|
| T2 | 1 | 3 |
|
| T3 | 6 | 9 |
|
| T4 | 8 | 10 |
|
| Tx | 2 | 1 |
|
| N factor |
|
| NS |
| N0 | 2 | 3 |
|
| N1 | 4 | 5 |
|
| N2 | 8 | 8 |
|
| N3 | 2 | 4 |
|
| Nx | 3 | 4 |
|
| M factor |
|
| NS |
| M0 | 0 | 0 |
|
|
M1a | 12 | 16 |
|
|
M1b | 6 | 8 |
|
| Histology |
|
| NS |
|
Adenocarcinoma | 11 | 17 |
|
|
SCC | 7 | 7 |
|
Hydrogen gas reduces PDT+, leading to
better prognosis
Hydrogen gas decreased the proportion of PDT+ in 20
of the 42 patients (47.6%) and
PD-1+Tim3−terminal CD8+ T cells
(PDT-) in 23 of the 42 patients (54.8%). In contrast, it increased
the proportion of PD-1−Tim3−terminal
CD8+ T cells in 30 of the 42 patients (71.4%). We
calculated the change in ratio for the proportion of PDT+ after HG
vs. before HG (PDT+ ratio). The cut-off value of the PDT+ ratio was
0.81 according to ROC curve (AUC=0.796, Sensitivity=81.0%,
Specificity=80.0%) (Fig. 2C), and
patients with low PDT+ ratio showed a significantly longer OS than
those with a high PDT+ ratio (Fig.
2D). The MST of the latter patients was 10 months, while more
than 50% of the former are still alive (Fig. 2D).
Concentration of CoQ10 in the
peripheral blood is highly associated with OS
PDT+ is assumed to have a more progressive
exhaustion than PDT-, leading to a worse prognosis compared to
PDT-. As the two exhausted CD8+ T cell populations (PDT+
and PDT-) are naturally considered to have mitochondrial
dysfunction, with potential differences in their degree,
measurement of mitochondria function is very important. While we
are yet to derive a method that clinically and easily grasps
mitochondrial function, the CoQ10 concentration can already be
measured using peripheral blood. Because CoQ10 plays an important
role in the mitochondrial respiratory chain, its concentration in
peripheral blood may be an approximate value of mitochondrial
function. We measured the CoQ10 concentration in the 35 HGN-treated
patients with stage IV lung cancer and investigated its association
with OS. The cut-off value was found to be 0.985 µg/ml (ROC curve;
AUC=0.803, Sensitivity=83.3%, Specificity=81.8%, (Fig. 2E). Further, the 35 HGN-treated
patients were stratified as having high (>0.985 µg/ml) and low
(<0.985 µg/ml) CoQ10 concentrations. There were no significant
differences in the clinico-pathological factors between patients
with high and low CoQ10 (Table
III). Patients with high CoQ10 had a significantly longer OS
than those with low CoQ10 (Fig. 2F).
MST of patients with high CoQ10 was 25 months, while that of
patients with low CoQ10 was 8 months (Fig. 2F).
Following hydrogen gas treatment, the concentration
of CoQ10 was increased in 19 (46%) of 41 patients (Table IV). Hence, we proceeded to calculate
the rate of change of CoQ10 by hydrogen gas treatment (CoQ10
ratio=CoQ10 concentration after treatment/CoQ10 concentration
before treatment) and classified patients by high- and low-CoQ10
ratio using the cut-off value (1.175) (ROC curve; AUC=0.710,
Sensitivity=75.0%, Specificity=66.7%) (Fig. 2G). Patients with a high-CoQ10 ratio
survived significantly longer than those with a low-CoQ10 ratio, as
shown in Fig. 2H. MST of patients
with a high CoQ10 ratio was NR (not reached to 50% overall
survival), while that of patients with low CoQ10 was 9 months
(Fig. 2H).
| Table IV.aPDT+ ratio and CoQ10 ratio. |
Table IV.
aPDT+ ratio and CoQ10 ratio.
|
| CoQ10 ratio |
|
|
|---|
|
|
|
|
|
|---|
| Value | High | Low | Total |
P-valueb |
|---|
| PDT+ ratio |
|
|
| 0.007 |
|
High | 5 | 16 | 21 (51%) |
|
|
Low | 14 | 6 | 20 (49%) |
|
| Total | 19 (46%) | 22 (54%) | 41 |
|
Exhausted CD8+ T cells,
especially PDT+, are highly associated with CoQ10
PDT+ might be more exhausted than PDT- and may have
more severe mitochondrial dysfunction than PDT-. As described
above, if the concentration of CoQ10 in the peripheral blood of
patients can predict mitochondrial function to some extent, an
association between the proportion of PDT+ and the concentration of
CoQ10 may exist; this is because the most striking feature of PDT+
is mitochondrial dysfunction.
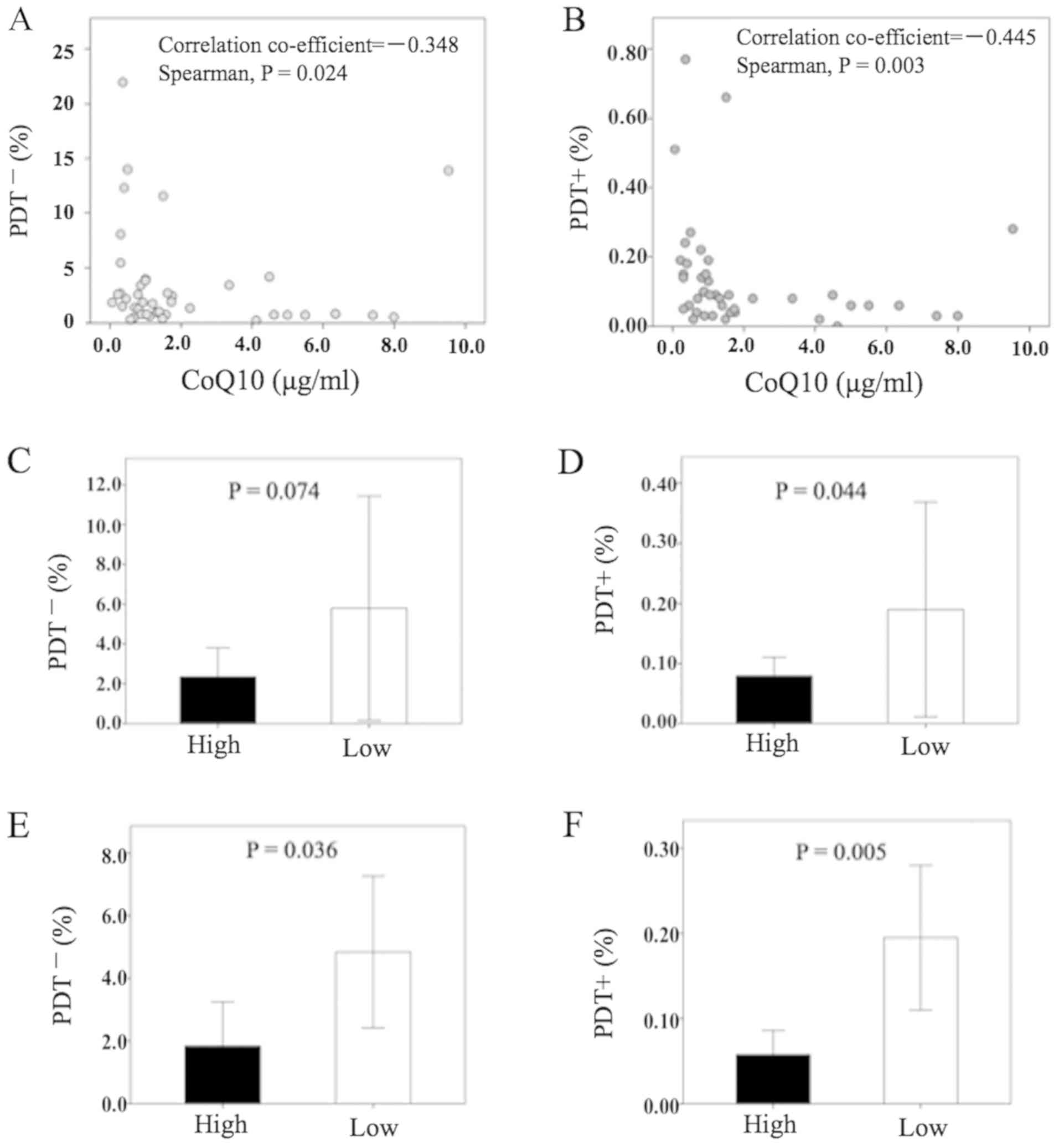
We found that PDT+ showed a moderate reverse
correlation to CoQ10, which was more significant than that of PDT-
(Fig. 3A and B). In patients with a
high level of CoQ10, the proportion of PDT+ was significantly lower
than in patients with low CoQ10 (Fig.
3D), while that of PDT- was not significant (Fig. 3C). Further, in patients with a
high-CoQ10 ratio (i.e., patients with increased CoQ10 concentration
after HGN-treatment), both of PDT- and PDT+ were significantly
lower than in patients with a low-CoQ10 ratio (Fig. 3E and F, respectively). Table IV shows that the CoQ10 ratio was
significantly low in patients with a high PDT+ ratio, while the
CoQ10 ratio was significantly high in those with a low PDT+
ratio.
Discussion
In the present study, we revealed that hydrogen gas
enhances the overall survival time of nivolumab-treated lung cancer
patients. The MST of the patients treated with nivolumab and
hydrogen gas (28 months) is about three times longer than that of
those treated with nivolumab only (9 months). Although
PD-1+terminal CD8+ T cells were an
independent poor prognostic factor in the stage IV colorectal
cancer patients as previously reported (7), the CD8+ T cells expressing
both PD-1 and Tim-3 (PDT+) were most significantly responsible for
OS of the patients treated with nivolumab and hydrogen gas,
suggesting that nivolumab masks an expression of PD-1 molecules on
CD8+ T cells and so measurement of Tim-3 molecules as
well as PD-1 on CD8+ T cells is required for an accurate
evaluation of prognosis of patients treated with nivolumab.
Contrary to our recent report on PD-1+terminal
CD8+ T cells (7), the
hydrogen-induced reduction of the proportion of
PD-1+terminal CD8+ T cells in this study did
not cause an improvement of overall survival, but hydrogen gas
decreased PDT+ and increased
PD-1−Tim-3−terminal CD8+ T cells,
which resulted in a better OS in HGN-treated patients. PDT+ is
supposed to be the most severely exhausted CD8+ T cells
possible exhibiting severe mitochondrial dysfunction, which is
caused by progressive loss of PGC1α, a regulator of mitochondrial
replication, which is controlled by a variety of signaling pathways
(Akt, p38-MARK, AMPK, SIRT1, PRMT1) (4), likely driven by constitutive chronic
antigen exposure in the tumor microenvironment (5). It was reported that hydrogen is
associated with these signaling pathways (21–24),
suggesting that it may improve PGC1-α through these pathways to
enhance the clinical effects of nivolumab by restoring exhausted
CD8+ T cells. Direct mitochondrial activators synergize
with PD-1 blockade therapy; however, none of the mitochondrial
activation chemicals alone exert any effects on tumor growth
(6). This indicates that the better
clinical effects observed in this study are not attributable to
hydrogen gas alone, and as such, nivolumab is also required. This
phenomenon may be explained by the fact that the reactive T cells
by hydrogen gas contact cancer cells and subsequently express PD-1
in response to PDL-1 expressed on tumor cells, and consequently,
nivolumab is required at the final stage of cancer attack. This is
only the best situation for nivolumab showing its own best
performance. Taken together, it is assumed that there are three
kinds of PD-1-expressing CD8+ T cells, namely 1)
CD8+ T cells transiently express PD-1 in response to
PDL-1 on tumor cells and have normal mitochondria (referred to as
suppressive CD8+ T cells, for convenience), 2) exhausted
CD8+ T cells have mitochondrial disorder driven by a
variety of signals from the cancer microenvironment and
consequently express PD-1 (exhausted CD8+ T cells), and
3) more exhaustive CD8+ T cells express both PD-1 and
Tim-3 and possess more severe mitochondrial disorder (PDT+).
Suppressive CD8+ T cells are nivolumab-responder type,
and both exhausted CD8+ T cells, especially PDT+, are
nivolumab-non-responder type, requiring mitochondrial activation
substances such as hydrogen gas for making nivolumab effective.
Because mitochondrial dysfunction of the two
exhausted CD8+ T cells described above is caused by loss
of PGC1-α and hydrogen gas activates PGC1-α, the hydrogen
gas-induced reduction of the two exhausted CD8+ T cells
(PDT- and PDT+) is assumed to be due to mitochondrial reactivation
by hydrogen gas. However, there is currently no appropriate method
to clinically and easily measure mitochondrial function. In this
study, we attempted to use, as a marker of mitochondrial function,
the concentration of CoQ10 in peripheral blood. This is because
CoQ10 plays an important role in the mitochondrial respiratory
chain, and it has recently become possible to easily measure its
concentration in peripheral blood. In this study, we found that the
CoQ10 concentration was highly associated with the better prognosis
of lung cancer patients (Fig. 2F),
which is the first report about an association of CoQ10 with the
prognosis of cancer patients. Moreover, the hydrogen gas-induced
increase in the CoQ10 concentration was found to result in an
improvement in prognosis (Fig. 2H).
The proportion of PDT+ was significantly lower in patients with a
high CoQ10 concentration than in those with a low concentration
(Fig. 3D). Additionally, when the
CoQ10 concentration increased, that of PDT+ significantly decreased
(Fig. 3F and Table IV). This finding suggests that the
proportion of PDT+ is influenced by CoQ10 concentration. CoQ10
concentration in the peripheral blood of lung cancer patients was
inversely associated with the proportion of PDT+, more
significantly than with the proportion of PDT- (Fig. 3A and B). These results are indicative
that the concentration of CoQ10 reflects mitochondrial function.
Furthermore, exhausted CD8+ T cells, especially PDT+,
may be an opposite marker of mitochondrial function. Consequently,
it is suggested that hydrogen gas activates the mitochondria
(CoQ10) to restore exhausted CD8+ T cells, including
PDT+, into the active form of CD8+ T cells, resulting in
better nivolumab outcomes. Our study revealed that nivolumab could
not exert clinical effects against exhausted CD8+ T
cells, especially PDT+, which is the major reason for the clinical
response rate of nivolumab being as low as 20–30% in patients with
advanced cancer. From this point of view, hydrogen gas has good
compatibility with nivolumab as it decreases exhausted
CD8+ T cells. Thus, PDT+ and CoQ10 might be reliable
negative and positive biomarkers of nivolumab, respectively.
Although coenzyme Q10 (CoQ10), a key enzyme of the mitochondrial
respiratory chain (15), is
suggested in this study to be a representative marker of
mitochondrial function, we did not measure other mitochondrial
enzymes such as nicotinamide adenine dinucleotide (NAD+), NADH,
flavin adenine dinucleotide (FAD), acetyl coA and ATP amount in
this study and so it is unclear yet whether a measurement of
peripheral CoQ10 concentration is most suitable marker of
mitochondrial function. Therefore, it will be required in the
future to investigate whether CoQ10 is more suitable mitochondrial
marker than other mitochondrial enzymes as described above. The
present study had limitations. Other mitochondrial enzymes such as
nicotinamide adenine dinucleotide (NAD+), NADH, flavin adenine
dinucleotide (FAD), acetyl coA and ATP amount were not investigated
in the present study and so it is unclear yet whether a measurement
of peripheral CoQ10 concentration is most suitable marker of
mitochondrial function.
Although pulmonary function tests before and after
hydrogen is an important subject to evaluate patients' prognosis,
we did not performed pulmonary function tests and will investigate
it in the future.
Hydrogen gas could not restore PDT+ in all of the
patients. PDT+ was not reduced in 21 of 41 patients (51.0%) by
hydrogen gas, and in 22 out of 41 patients (54%), hydrogen gas
could not increase the CoQ10 concentration (Table IV). In approximately half of the
lung cancer patients, hydrogen gas could not activate CoQ10
(mitochondria) and/or reduce PDT+. The existence of senescent
CD8+ T cells, which are known to show decreased
proliferation, defective mitochondrial function, and Tim-3
expression, has been reported (25).
In addition, it was recently understood that senescent
CD8+ T cells are not only dysfunctional CD8+
T cells, but they have an important role in altering the tissue
microenvironment and affecting neighboring cells via the production
and secretion of pro-inflammatory cytokines, chemokines, growth
factors, and proteases through paracrine signaling (26). The most striking feature of senescent
CD8+ T cells is that not only their T cell-dysfunction
but also their mitochondrial dysfunction should be irreversible as
reported before (25,27–29). In
this study, there also existed hydrogen-unresponsive PDT+, which
may be senescent CD8+ T cells. Nonetheless, recent
studies have shown that even senescent T cells could regain
function by inhibiting the p38 mitogen-activated protein kinase
(MAPK) pathway (30,31), which is one of the MAPK subfamilies
that regulate cell growth, differentiation, and stress responses
(32). Further, it was reported that
hydrogen gas inhibits the p-38 pathway (33,34),
suggesting that hydrogen gas may even restore senescent
CD8+ T cells (including hydrogen-unresponsive PDT+) into
active CD8+ T cells by inhibiting the p38 pathway. Our
hydrogen gas-related data revealed that the longer patients inhaled
hydrogen gas, the better their prognosis (data not shown). Such
finding suggests that a longer inhalation of hydrogen gas may cause
further effective recoveries of PDT+ even if they are senescent
CD8+ T cells. For example, there are few cases with a
10-h inhalation per day that demonstrate much better clinical
effects than those with the usual 3-h inhalation per day.
When the total patients number reached to about 30,
we found that the survival rate and QOL (Quality of life) of the
patients treated with both nivolumab and hydrogen gas were quite
better that those with nivolumab only. Therefore, then, we are
sorry to select the combined treatment of nivolumab and hydrogen
gas more preferably than the treatment of nivolumab only. That is
why the number of the patients treated with combined treatment was
more than those with nivolumab only. However, this result strongly
suggest that the combined treatment of nivolumab and hydrogen gas
is more clinically effective than the treatment with nivolumab
only.
In conclusion, hydrogen gas activates CoQ10
(mitochondria), thereby enhancing the outcomes of nivolumab via
reducing exhausted CD8+ T cells, especially PDT+. Our
findings also suggest that CoQ10 concentration in peripheral blood
is an available marker of mitochondrial function, while PDT+ and
CoQ10 are reliable biomarkers of nivolumab. It is assumed that
nivolumab is not effective for patients with predominant exhausted
CD8+ T cells in peripheral blood, which can be overcome
by hydrogen gas.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
HB interpreted the patient blood data. JA performed
the blood examination of the patients with lung cancer, analyzed
their data and was a major contributor in writing the manuscript.
All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The ethic review board of Tamana Regional Health
Medical Center approved the current study.
Patient consent for publication
All patients were provided with informed consent for
publication of any associated data and accompanying images.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
PDT+
|
PD-1+Tim3+terminal CD8+ T
cells
|
|
PDT-
|
PD-1+Tim3−terminal CD8+ T
cells
|
|
PD-1
|
programmed cell death 1
|
|
PGC-1α
|
peroxisome proliferator-activated
receptor γ coactivator 1α.
|
References
|
1
|
Zou W, Wolchok JD and Chen L: PD-L1
(B7-H1) and PD-1 pathway blockade for cancer therapy: Mechanisms,
response biomarkers, and combinations. Sci Transl Med.
8:328rv42016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Zajac AJ, Blattman JN, Murali-Krishna K,
Soudive DJ, Suresh M, Altman JD and Ahmed R: Viral immune evasion
due to persistence of activated T cells without effector function.
J Exp Med. 188:2205–2213. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Urbani S, Amadei B, Tola D, Massari M,
Schivazappa S, Missale G and Ferrari C: PD-1 expression in acute
hepatitis C virus (HCV) infection is associated with HCV-specific
CD8 exhaustion. J Virol. 80:11398–11403. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Fernandez-Marcos PJ and Auwerx J:
Regulation of PGC1-α, a nodal regulation of mitochondrial
biogenesis. Am J Clin Nutr. 93:884S–890S. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Scharping NE, Menk AV, Moreci RS,
Whetstone RD, Dadey RE, Watkins SC, Ferris RL and Delgoffe GM: The
tumor microenvironment represses T cell mitochondrial biogenesis to
drive intratumoral T cell metabolic insufficiency and dysfunction.
Immunity. 45:374–388. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Chamoto K, Chowdhury PS, Kumar A, Sonomura
K, Matsuda F, Fagarasan S and Honjo T: Mitochondrial activation
chemicals synergize with surface receptor PD-1 blockade for T
cell-dependent antitumor activity. Proc Natl Acad Sci USA.
114:E761–E770. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Akagi J and Baba H: Hydrogen gas restores
exhausted CD8+ T cells in patients with advanced colorectal cancer
to improve prognosis. Oncol Rep. 41:301–311. 2019.PubMed/NCBI
|
|
8
|
Lund AW: Re-energizing exhausted T cells?
Sci Transl Med. 8:353ec1352016. View Article : Google Scholar
|
|
9
|
Wang F, He W, Zhou H, Yuan J, Wu K, Xu L
and Chen ZK: The Tim-3 ligand galectin-9 negatively regulates CD8+
alloreactive T cell and prolongs survival of skin graft. Cell
Immunol. 250:68–74. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Anderson AC, Anderson DE, Bregoli L,
Hastings WD, Kassam N, Lei C, Chandwaskar R, Karman J, Su EW,
Hirashima M, et al: Promotion of tissue inflammation by the immune
receptor Tim-3 expressed on innate immune cells. Science.
318:1141–1143. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Jones RB, Ndhlovu LC, Barbour JD, Sheth
PM, Jha AR, Long BR, Wong JC, Satkunarajah M, Schweneker M, Chapman
JM, et al: Tim-3 expression defines a novel population of
dysfunctional T cells with highly elevated frequencies in
progressive HIV-1 infection. J Exp Med. 205:2763–2779. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sakuishi K, Apethoh L, Sullivan JM, Biazar
BR, Kuchroo VK and Anderson AC: Targeting Tim-3 and PD-1 pathways
to reverse T cell exhaustion and restore anti-tumor immunity. J Exp
Med. 207:2187–2194. 2011. View Article : Google Scholar
|
|
13
|
Ohsawa I, Ishikawa M, Takahashi K,
Watanabe M, Nishimaki K, Yamagata K, Katsura K, Katayama Y, Asoh S
and Ohta S: Hydrogen acts as a therapeutic antioxidant by
selectively reducing cytotoxic oxygen radicals. Nat Med.
13:688–694. 2007. View
Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kamimura N, Ichimiya H, Luchi K and Ohta
S: Molecular hydrogen stimulates the gene expression of
transcriptional coactivator PGC-1α to enhance fatty acid
metabolism. NPJ Aging Mech Dis. 2:160082016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hosoe K, Kitano M, Kishida H, Kubo H,
Fujii K and Kitahara M: Study on safety and bioavailability of
ubiquinol (Kaneka QH) after single and 4-week multiple oral
administration to healthy volunteers. Regul Toxicol Pharmacol.
47:19–28. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Tian G, Sawashita J, Kubo H, Nishio SY,
Hashimoto S, Suzuki N, Yoshimura H, Tsuruoka M, Wang Y, Liu Y, et
al: Ubiquinol-10 supplementation activates mitochondria functions
to decelerate senescence in senescence-accelerated mice. Antioxid
Redox Signal. 20:2606–2620. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Gyozdiakova A, Kucharska J, Sumbalova Z,
Nemec M, Chladekova A, Vancova O, Rausová Z, Kubalová M, Kuzmiaková
Z and Mojto V: Platelets mitochondrial function depends on CoQ10
concentration in winter, not in spring season. Gen Physiol Biophys.
38:325–334. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Sobin LH and Wittekind CH: UICC TNM
Classification of Malignant Tumors. John Wiley and Sons; New York,
NY: 1997
|
|
19
|
Tamura T, Hayashida K, Sano M, Suzuki M,
Shibusawa T, Yoshizawa J, Kobayashi Y, Suzuki T, Ohta S, Morisaki
H, et al: Feasibility and safety of hydrogen gas inhalation for
post-cardiac arrest syndrome-First-in-Human Pilot Study. Circ J.
80:1870–1873. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
National Cancer Institute: Cancer therapy
evaluation program, common terminology criteria for adverse events,
v3. Int J Clin Oncol. 9 (Supp III):1–82. 2004.
|
|
21
|
Wang M, Tang W and Zhu YZ: An update on
AMPK in hydrogen sulfide pharmacology. Front Pharmacol. 8:8102017.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Chi Q, Wang D, Hu X and Li S and Li S:
Hydrogen sulfide gas exposure induces necroptosis and promotes
inflammation through the MAPK/NF-κB pathway in broiler
spleen. Oxid Med Cell Longev. 2019:80618232019. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Li S, Fujino M, Ichimaru N, Kurokawa R,
Hirano S, Mou L, Takahara S, Takahara T and Li XK: Molecular
hydrogen protects against ischemia-reperfusion injury in a mouse
fatty liver model via regulating HO-1 and Sirt1 expression. Sci
Rep. 8:140192018. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Zhang B, Zhao Z, Meng X, Chen H, Fu G and
Xie K: Hydrogen ameliorates oxidative stress via PI3K-Akt signaling
pathway in UVB-induced HaCaT cells. Int J Mol Med. 41:3653–3661.
2018.PubMed/NCBI
|
|
25
|
Crespo J, Sun H, Welling TH, Tian Z and
Zou W: T cell anergy, exhaustion, senescence, and stemness in the
tumor microenvironment. Curr Opin Immunol. 25:214–221. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Callender LA, Carroll EC, Beal RWJ,
Chambers ES, Nourshargh S, Akbar AN and Henson SM: Human
CD8+ EMRA T cells display a senescence-associated
secretory phenotype regulated by p38 MAPK. Aging Cell.
17:e126752018. View Article : Google Scholar
|
|
27
|
Vallejo AN, Weyand CM and Goronzy ZJJ:
T-cell senescence: A culprit of immune abnormalities in chronic
inflammation and persistent infection. Trends Mol Med. 10:119–124.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Chappert P and Schwartz RH: Induction of T
cell anergy: Integration of environmental cues and infectious
tolerance. Curr Opin Immunol. 22:552–559. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Baitsch L, Fuertes-Marraco SA, Legat A,
Meyer C and Speiser DE: The three main stumbling blocks for
anticancer T cells. Trends Immunol. 33:364–372. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Lanna A, Henson SM, Escors D and Akbar AN:
The kinase p38 activated by the metablic regulator AMPK and
scaffold TAB1 drives the senescence of human T cells. Nat Immunol.
15:965–972. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Lanna A, Henson M and Akbar A: The
regulation of T cell senescence and metabolism by p38 map kinase
signaling. Innov Aging. 1 (Suppl 1):12542017. View Article : Google Scholar
|
|
32
|
Arthur JS and Ley SC: Mitogen-activated
protein kinases in innate immunity. Nat Rev Immunol. 13:679–692.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Zhou J, Yan P, Zhu XD and Yu KJ: Hydrogen
mitigates acute lung injury through upregulation of M2 and
downregulation of M1 macrophage phenotypes. Int J Clin Exp Med.
11:7927–7935. 2018.
|
|
34
|
Li D and Ai Y: Hydrogen saline suppresses
neuronal cell apoptosis and inhibit the p38 mitogen-activated
protein kinase-caspase-3 signaling pathway following cerebral
ischemia-reperfusion injury. Mol Med Rep. 16:5321–5325. 2017.
View Article : Google Scholar : PubMed/NCBI
|