Introduction
Intraductal papillary mucinous neoplasms (IPMNs) are
epithelial neoplasms composed of mucin-producing columnar cells,
and IPMNs are classified as 2 types: Main-duct type (MD-IPMN) and
branch-duct type IPMN (BD-IPMN). Since IPMN occasionally develops
into malignancy (IPMN-derived carcinoma: IPMC) (MD-IPMN: Range,
36–100%, BD-IPMN: Range, 6.3–46.5%), we need to develop a screening
strategy that can detect IPMN in the general population and
identify IPMC (1,2). For a reliable screening program,
establishment of diagnostic tests with low invasiveness, high
diagnostic yield and high reproducibility is essential. In this
context, biomarkers from body fluids can play an important role in
IPMN screening.
A considerable number of biomarker studies have
evaluated markers for use in detecting IPMCs among IPMN patients
(3–6). Carcinogenic antigen 19-9 (CA19-9) is
the only biomarker described in the guidelines; however, a recent
meta-analysis reported its diagnostic performance as highly
specific but not sensitive in identifying IPMC in IPMNs (7). Moreover, no biomarker has demonstrated
reliable diagnostic ability in detecting IPMNs in the general
population. To overcome this challenge, we need to establish new
biomarkers for IPMN screening.
Circulating microRNAs (miRNAs) have been shown to
have diagnostic potential as blood biomarkers for various tumors
(8–11). miRNAs are small, noncoding RNAs
(18–25 nucleotides in length) that regulate gene expression at the
posttranscriptional level by promoting the degradation of messenger
RNAs or by blocking messenger RNA translation. They can be loaded
into exosomes or other extracellular vesicles (extracellular
vesicle-encapsulated miRNA: EV-miRNA) or exist freely in the blood
circulation (circulating miRNA). Among these two forms, EV-miRNA
has several advantages over circulating miRNA: i) It can be
specifically released for cell-to-cell communication, and ii) lipid
membrane coverage protects miRNA from RNase degradation (12).
In this study, we aimed to determine whether serum
EV-miRNAs could be diagnostic markers of IPMNs in the general
population. In addition, the diagnostic yield of serum EV-miRNAs in
distinguishing IPMNs and IPMC was evaluated.
Materials and methods
Patients and treatments
First, we selected 4 patients with IPMNs (2 benign
IPMNs and 2 IPMCs) and 4 controls without any type of tumor for
microarray analysis to identify differences in the gene expression
of serum EV-miRNAs between these groups. To validate the microarray
results, we enrolled 38 consecutive patients who were diagnosed
with IPMNs by imaging modalities at Fukushima Medical University
Hospital and 21 patients without any neoplastic lesions as controls
between June 2015 and November 2019. The diagnostic criteria were
as follows: i) Dilation of the MD and/or a cystic dilation of the
BD, and ii) secretion of mucin from the major or minor papilla
identified by endoscopic retrograde cholangiopancreatography or
duodenoscopy.
Clinical data including age, sex, background
diseases in controls, presence of symptoms (jaundice, body weight
loss, etc.), history of diabetes mellitus, pancreatitis, smoking,
family history of pancreatic tumor, and serum tumor markers,
including carcinoembryonic antigen (CEA) and CA 19-9, were
retrieved from electronic medical records. Patients with
co-existing tumors or active infection (i.e., cholangitis or
cholecystitis) were excluded from the analysis. All recruited
patients were evaluated with CT or MRI, and the location of the
lesion, maximum diameter of cyst and main pancreatic duct (MPD),
and the presence of mural nodules were determined. Medical
management of the disease was also evaluated. Classification of
BD-IPMN and others was performed according to the 2017
International Consensus Guideline (1).
The study protocol conformed to the ethical
guidelines of the 1975 Declaration of Helsinki and was approved by
the institutional review board of Fukushima Medical University (IRB
#2387). All participants provided written informed consent.
Sample collection
To obtain the serum samples, 8 ml of blood was
collected and incubated at room temperature for at least 60 min to
allow clotting. Samples were then centrifuged at 1,000 × g for 10
min. The serum was collected and stored in aliquots at −80°C.
miRNA preparation and microarrays
Serum miRNA was extracted from serum using the
exoRNeasy Serum/Plasma Midi kit (Qiagen) according to the
manufacturer's protocol. RNA quantity and quality were determined
using an Agilent Bioanalyzer (Agilent Technologies), as
recommended. miRNA microarrays were manufactured by Agilent
Technologies. Briefly, RNA was dephosphorylated using calf
intestinal alkaline phosphatase (CIP) master mix incubated at 37°C
for 30 min. Dephosphorylated RNA was denatured with DMSO incubated
at 100°C for 5 min and then immediately transferred to ice for 2
min. These products were mixed with a ligation master mix for T4
RNA ligase and Cy3-pCp (Cyanine 3-Cytidine biphosphate) and
incubated at 16°C for 2 h. Labeled RNA was dried using a vacuum
concentrator at 55°C for 1.5 h. Cy3-pCp-labeled RNA was hybridized
on an Agilent SurePrint G3 Human miRNA 8×60K Rel.21 (design ID:
070156) array at 55°C for 20 h. After washing, microarrays were
scanned using an Agilent SureScan Microarray Scanner System
(G4900DA). The intensity values of each scanned feature were
quantified using Agilent Feature Extraction software version
12.1.1.1, which performs background subtractions. We only used
features that were flagged as no errors (detected flags) and
excluded features that were not positive, not significant, not
uniform, not above background, saturated, and population outliers
(not detected flags). These expression analyses were performed with
Agilent GeneSpring GX version 14.9.1.
Digital PCR
Digital PCR and quantification of the absolute
levels of serum miRNAs were performed using the Quant-Studio 3D
Digital PCR system (Thermo Fisher Scientific, Inc.). Data were
analyzed using QuantStudio 3D Analysis Suite Cloud Software (Thermo
Fisher Scientificc, Inc.). The digital PCR mixture contained 5.0 µl
of the RT product, 1.0 µl of nuclease-free H2O, 7.50 µl
of the QuantStudio™ 3D Digital PCR Master Mix, and 0.75 µl of the
TaqMan MiRNA Assay-1 (20X) for let-7d. Samples were individually
loaded onto the QuantStudio 3D digital PCR 20K chip kit v2 using
the QuantStudio 3D digital PCR Chip Loader. Digital PCR was
performed in a Proflex 2X flat block thermal cycler (Applied
Biosystems) using standard conditions: 96°C for 10 min followed by
39 cycles of 60°C for 2 min, 98°C for 30 sec, and 60°C for 2 min.
Chips were read on the QuantStudio 3D digital PCR instrument, and
the number of FAM-positive and FAM-negative (empty) wells was
quantified (13,14).
Target gene prediction and pathway
enrichment analyses
Target gene prediction was performed using
DIANA-miRPath software (15).
Specifically, we investigated whether tumor suppressor genes were
targeted by these 3 miRNAs because aberrant tumor suppressor gene
methylation was observed in malignant IPMN (16).
To predict cell signaling pathways that were
potentially influenced by the EV-miRNAs, Kyoto Encyclopedia of
Genes and Genomes (KEGG) pathway enrichment analyses were performed
via the Database for Annotation, Visualization and Integrated
Discovery (DAVID 6.8; http://david.abcc.ncifcrf.gov/) (17,18).
KEGG pathways with a P-value <0.05 were considered significantly
enriched.
Statistical analysis
Continuous variables (i.e., age, cyst size, serum
CEA and CA 19-9 levels and GS) are reported as the median and range
and were compared using Mann-Whitney analysis. Categorical
variables (i.e., sex and location of disease) were analyzed using
Fisher's exact test. The diagnostic yield of CEA and CA 19-9 levels
and EV-miRNAs in distinguishing whole IPMN (benign IPMN and IPMC)
from the control and IPMC from benign IPMN was assessed using the
area under the receiver operating characteristic (ROC) curve.
Statistical analyses were performed using SPSS version 26.0 for
Windows (IBM Corp.), and figures were generated with Prism 7
(GraphPad Software, Inc.). P<0.05 was considered to indicate
statistical significance.
Results
Identification of miRNAs for IPMN
screening
We first identified miRNAs showing altered
expression in 2 IPMNs,2 IPMCs and 4 controls (Table I). Among the 2588 mature miRNAs
evaluated in the microarray, we found 3 EV-miRNAs [hsa-miR-6132
(EV-miR-6132), hsa-miR-22-3p (EV-miR-22) and hsa-miR-4539
(EV-miR-4539)] that could discriminate IPMN, IPMC and control
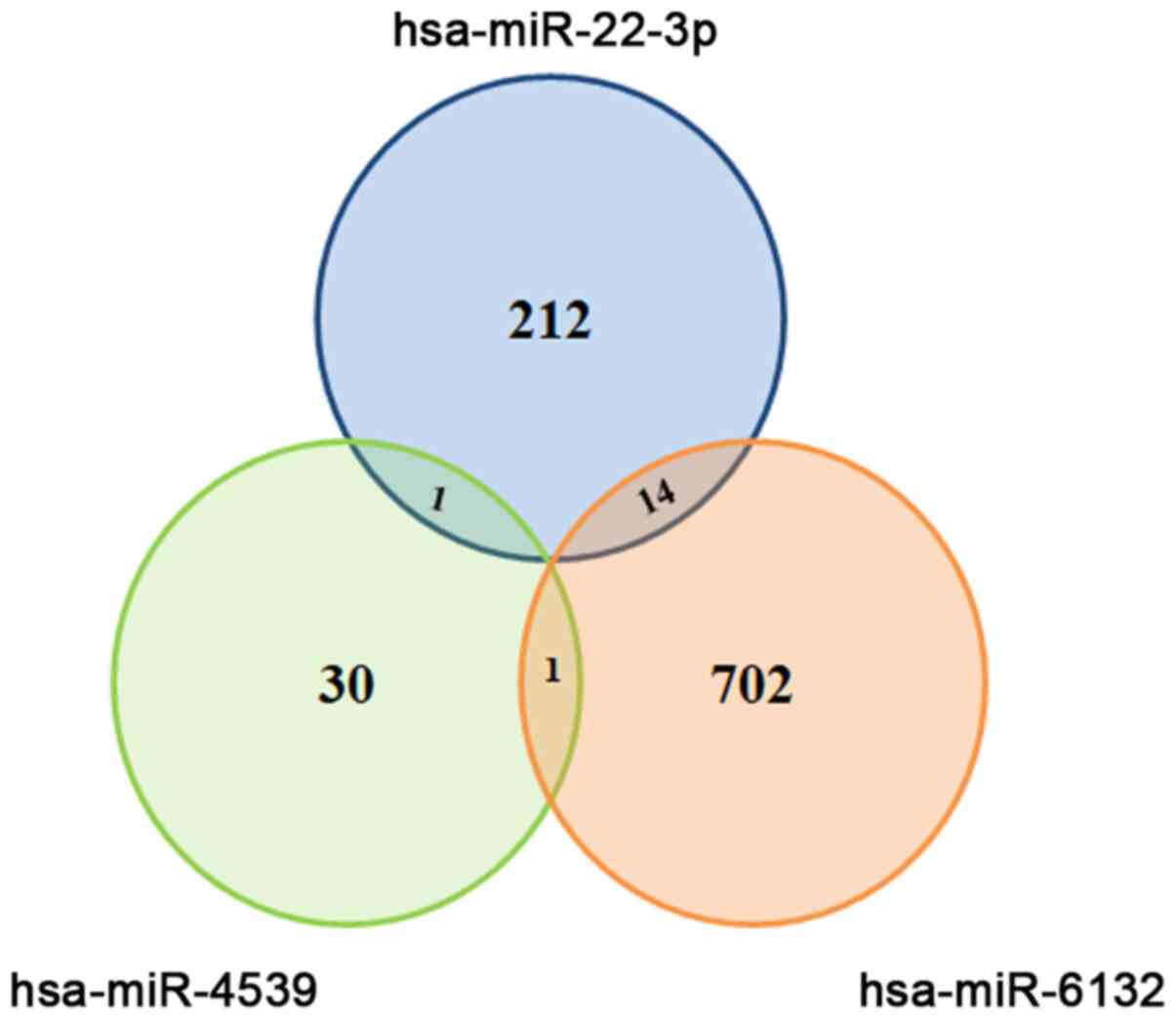
(Table II). As shown in Fig. 1, target prediction using
DIANA-miRPath software revealed that these 3 miRNAs could target
various genes. Regarding tumor suppressor genes, we found that
miR-22-3p could target TP53INP1 and mir-6132 could target 3 genes
(tuberous sclerosis complex 2: TSC2, tumor protein p53-inducible
protein 11: TP53I11 and protein phosphatase 2 regulatory subunit
B'Delta: PPP2R5D).
 | Table I.Background disease of patients in
microRNA array analysis. |
Table I.
Background disease of patients in
microRNA array analysis.
| Sample nos. | Disease | Group name |
|---|
| 1-4 | Control | A1 |
| 5 and 6 | IPMC | A2 |
| 7 and 8 | IPMN | A3 |
| Table II.Different expressions of miRNAs
between each group. |
Table II.
Different expressions of miRNAs
between each group.
| Systematic name | FC [(A2) vs.
(A3)] | Log FC [(A2) vs.
(A3)] | FC [(A2) vs.
(A1)] | Log FC [(A2) vs.
(A1)] | FC [(A3) vs.
(A1)] | Log FC [(A3) vs.
(A1)] |
|---|
| hsa-miR-6132 | 4.55 | 2.19 | 21.55 | 4.43 | 4.74 | 2.24 |
| hsa-miR-22-3p | 2.92 | 1.55 | 7.54 | 2.91 | 2.58 | 1.37 |
| hsa-miR-4539 | 2.94 | 1.56 | 7.54 | 2.91 | 2.56 | 1.36 |
| hsa-miR-6732-3p | 9.31 | 3.22 | 7.54 | 2.91 | −1.23 | −0.30 |
| hsa-miR-4534 | 2.16 | 1.11 | 2.30 | 1.20 | 1.06 | 0.09 |
| hsa-miR-3679-5p | 1.83 | 0.87 | 1.60 | 0.67 | −1.15 | −0.20 |
In addition, pathway enrichment analyses found that
these 3 miRNAs could influence the NOD-like receptor signaling
pathway (6 target genes involved), glycosphingolipid
biosynthesis-lacto and neolacto series-(1 target gene involved) and
fat digestion and absorption (5 target genes involved) (Table III).
| Table III.Results of KEGG pathway analysis. |
Table III.
Results of KEGG pathway analysis.
| KEGG pathways | P-value | Involved genes |
|---|
| KEGG pathway:
miR-22-3p and miR-6132 |
|
|
|
NOD-like receptor signaling
pathway | 0.04 | NF-kappa-B
inhibitor beta (NFKBIB), Caspase 1 (CASP1), NACHT, LRR and PYD
domains-containing protein 3 (NLRP3), mitogen-activated protein
kinase 11 (MAPK11), Suppressor of G2 allele of SKP1 homolog
(SUGT1), mitogen-activated protein kinase 1 (MAPK1) |
| KEGG pathway:
miR-22-3p and miR-4539 |
|
|
|
Glycosphingolipid
biosynthesis-lacto and neolacto series | 0.002 | Fucosyltransferase
9 (FUT9) |
| KEGG pathway:
miR-4539 and miR-6132 |
|
|
| Fat
digestion and absorption | 0.04 | Fatty acid binding
protein 1 (FABP1), Apolipoprotein A4 (APOA4), CD36, microsomal
triglyceride transfer protein (MTTP), Phospholipase A2 Group IIC
(PLA2G2C) |
Clinical characteristics of the
patients
To validate whether the 3 miRNAs could be diagnostic
markers for IPMN, we conducted a validation study using digital
PCR. The clinical characteristics of patients in the IPMN (n=38)
and control (n=21) groups are presented in Table IV. Briefly, there were no
significant differences in age, sex, absence of symptoms, history
of diabetes, pancreatitis, smoking, or family history of pancreatic
cancer between the IPMN group and the control group. With regard to
management, a total of 9 patients underwent surgery among 38 IPMN
patients. We confirmed the pathological diagnosis of the resected
cases according to the latest classification (1): Low-grade dysplasia (n=4), high-grade
dysplasia (n=1), and invasive carcinoma (n=4). Twenty-eight
patients did not require surgery and were continuously observed.
One patient was treated with chemotherapy.
| Table IV.Clinical characteristics of patients
with IPMN and controls. |
Table IV.
Clinical characteristics of patients
with IPMN and controls.
|
Characteristics | Control (n=21) | IPMN (n=38) | P-value |
|---|
| Median age, years
(range) | 71.0
(46.0–89.0) | 74.0
(47.0–91.0) | 0.51 |
| Sex, male (%) | 13 (61.9) | 19 (50.0) | 0.42 |
| Background
disease |
|
|
|
| Bile
duct stone, n (%) | 14 (66.7) |
|
|
| Chronic
pancreatitis, n (%) | 7
(33.3) |
|
|
| Presence of
symptoms, n (%) | 3
(14.2) | 7
(18.4) | 0.99 |
| Hx of diabetes
mellitus, n (%) | 4
(19.0) | 11 (28.9) | 0.53 |
| Hx of pancreatitis,
n (%) | 2
(9.5) | 2
(5.3) | 0.61 |
| Hx of smoking,
never/ever/current | 9/6/6 | 19/9/10 | 0.29 |
| Family Hx of
pancreatic tumor (%) | 0
(0.0) | 2
(5.3) | 0.53 |
| IPMN subtype,
branch-duct, n (%) |
| 25 (65.8) |
|
| IPMC, n (%) |
| 11 (28.9) |
|
| Management, n
(%) |
|
|
|
|
Follow-up | 21 (100.0) | 28 (73.6) |
|
|
Surgical resection |
| 9
(23.6) |
|
|
Chemotherapy |
| 1
(2.6) |
|
We also divided IPMNs into 2 groups, namely, IPMC
(n=11) and benign IPMN without any suspicious findings of
malignancy (n=27), and compared clinical characteristics as shown
in Table V. Clinical symptoms were
observed more frequently in IPMC than IPMN (36.3 vs. 0.0%,
P=0.0001). Additionally, the median diameter of the MPD was
significantly larger in IPMC than in IPMN (11.3 vs. 4.4 mm,
P=0.0003).
| Table V.Clinical characteristics of patients
with IPMC and IPMN. |
Table V.
Clinical characteristics of patients
with IPMC and IPMN.
|
Characteristics | Benign IPMN
(n=27) | IPMC (n=11) | P-value |
|---|
| Median age, years
(range) | 69.5
(48.0–89.0) | 74.5
(47.0–91.0) | 0.71 |
| Sex, male (%) | 11 (40.7) | 8 (63.6) | 0.15 |
| Presence of
symptoms, n (%) | 0
(0.0) | 7 (36.3) | 0.0001 |
| Hx of diabetes
mellitus, n (%) | 7
(33.3) | 4 (33.3) | 0.99 |
| Hx of pancreatitis,
n (%) | 2
(7.4) | 0 (0.0) | 0.99 |
| Hx of smoking,
never/ever/current | 15/5/7 | 5/5/1 | 0.29 |
| Family Hx of
pancreatic tumor (%) | 1
(3.7) | 1 (9.1) | 0.50 |
| Location of the
lesion, Ph/Pb/Pt/diffuse | 12/7/4/4 | 6/3/0/2 | 0.60 |
| Median cyst
diameter, mm (range) | 24.5
(12.0–63.0) | 31.0
(10.0–170.0) | 0.09 |
| Median MPD
diameter, mm (range) | 4.4 (1.5–13.0) | 11.2
(2.2–33.0) | 0.0003 |
| Median size of
mural nodule, mm (range) | 8.1 (3.0–15.0) | 18.0 (4.0–50) | 0.02 |
miRNAs as diagnostic markers for
IPMN
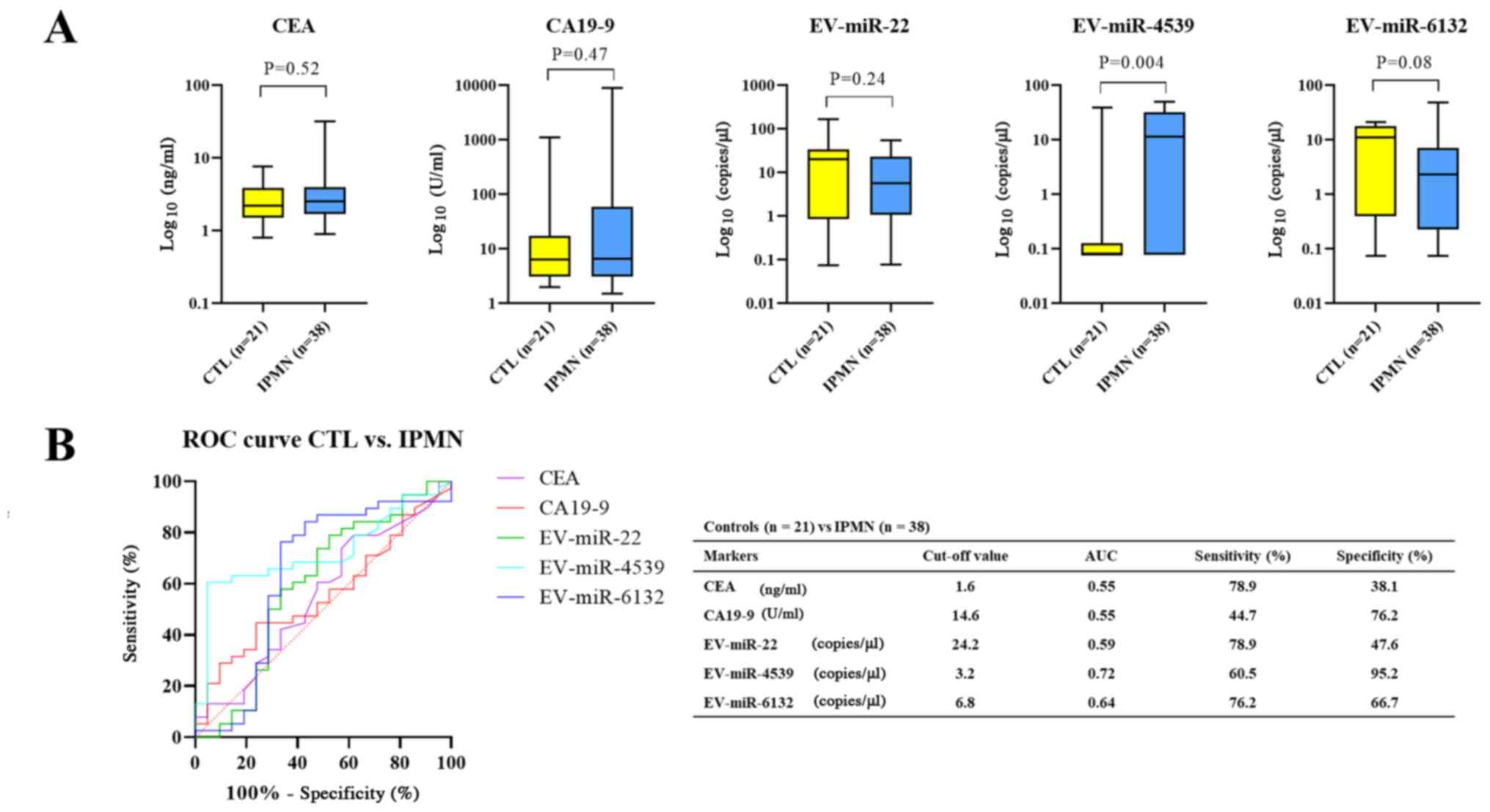
Fig. 2 shows the
differences in each biomarker between the control and IPMN (both
benign IPMN or IPMC) groups (Fig. 2)
and between benign IPMN and IPMC groups (Fig. 3). With regard to discriminating IPMNs
from control, only EV-miR-4539 showed a significant difference
(P=0.004) (Fig. 2A). ROC analysis
showed that 5 markers could discriminate patients with IPMN and
from control patients, with areas under the curve (AUCs) of 0.72
for EV-miR-4539 (95% confidence interval [CI]: 0.59–0.85), 0.55 for
CEA (95% CI, 0.39–0.71), 0.55 for CA19-9 (95% CI, 0.41–0.71), 0.59
for EV-miR-22 (95% CI, 0.42–0.76) and 0.64 for EV-miR-6132 (95% CI,
0.47–0.81). As shown in Fig. 2B,
EV-miR-4539 had the highest diagnostic yield compared with other
markers at the cutoff value of 3.2 copies/µl, and the sensitivity
and specificity were 60.5 and 95.2%, respectively (Fig. 2B).
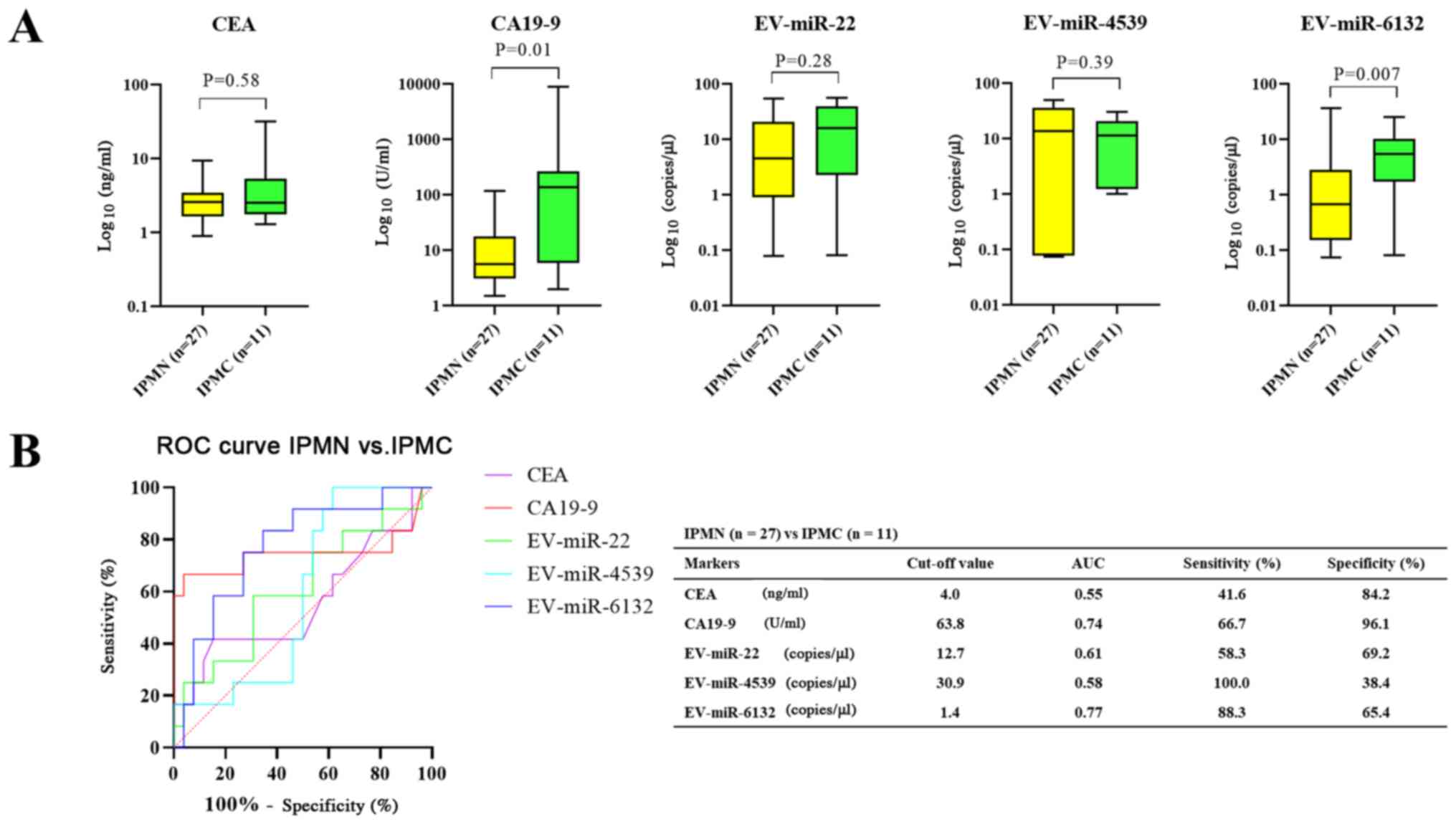
In the comparison between benign IPMN and IPMC,
CA19-9 and EV-miR-6132 showed significant differences (P=0.01 and
0.007, respectively) (Fig. 3A). ROC
analysis showed that the markers could discriminate patients with
IPMC from patients with benign IPMN, with an AUC of 0.77 for
EV-miR-6132 (95% CI, 0.61–0.93), 0.74 for CA19-9 (95% CI,
0.52–0.97), 0.61 for EV-miR-22 (95% CI, 0.41–0.81), 0.58 for
EV-miR-4539 (95% CI, 0.40–0.77) and 0.55 for CEA (95% CI,
0.34–0.77). EV-miR-6132 showed the highest diagnostic yield
compared with other markers at the cutoff value of 1.4 copies/µl
and the sensitivity and specificity were 88.3 and 65.4%,
respectively (Fig. 3B).
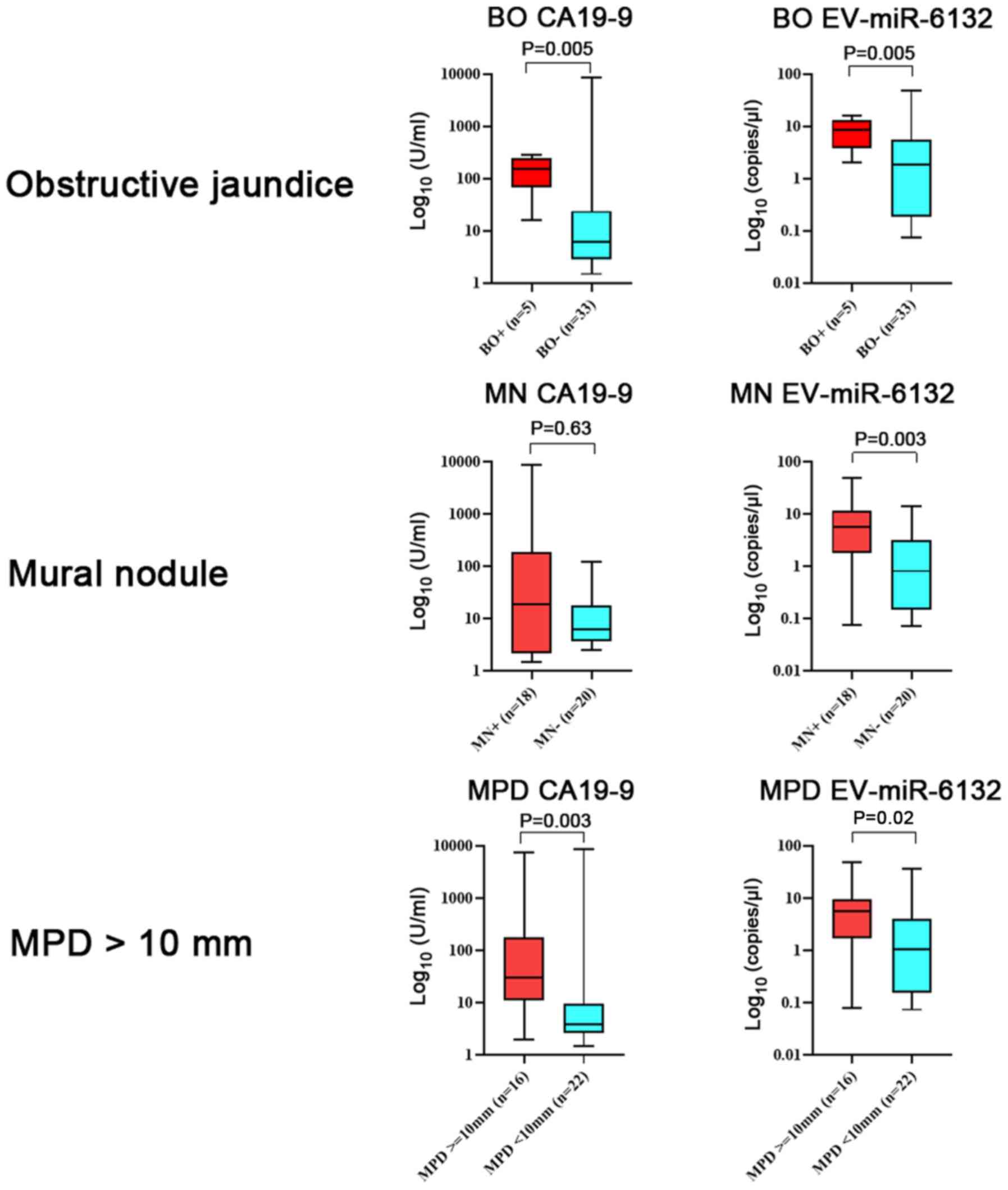
With regard to the serum levels of biomarkers and
the existence of high-risk indicators, the serum level of CA19-9
was higher in patients with obstructive jaundice (Fig. 4). The serum level of EV-miR-6132 was
higher in patients with high-risk indicators (mural nodules and MPD
diameter more than 10 mm) than in patients without them.
Discussion
In the present study, we aimed to confirm the
potentially useful EV-miRNAs (EV-miR-22, EV-miR-4539 and
EV-miR-6132) for IPMN and IPMC detection in microarray analysis. To
the best of our knowledge, this is the first study that suggested
the usefulness of EV-miRNAs in IPMN screening. It was found that
EV-miR-4539 was better at distinguishing IPMNs from non-tumor
controls than other biomarkers. While the diagnostic yield of
EV-miR-6132 to discriminate IPMNs and IPMC was comparable to that
of CA19-9, it had the advantage that the expression level was not
influenced by biliary obstruction.
miRNAs can play multifunctional roles in cancer
progression. With regard to IPMN, Habbe et al first reported
abnormal miRNA expression in IPMN (19). In this study, the expression of
miR-155 was found to be elevated in both IPMN tissue and pancreatic
juice. Authors suggested that miRNA could be a diagnostic marker
for pancreatic neoplasms. Subsequently, multiple studies focused on
the identification of high-risk IPMN, and the results suggested
that many miRNAs in the blood, pancreatic juice, and cystic fluid
could be useful diagnostic markers. More recently, some researchers
have attracted the attention of miRNAs encapsulated in EV-like
exosomes since they are supposed to be stabilized to avoid
degradation in the blood and highly enriched compared to
circulating miRNAs. Goto et al (20) compared the diagnostic yield of serum
circulating miRNAs and exosomal miRNAs in distinguishing control
tissues from IPMNs. Their study was quite informative as the
diagnostic yield of exosomal miRNAs was found to be 5–20% superior
to that of serum circulating miRNAs (e.g., exosomal miR-21: AUC
0.826, accuracy 80%). Circulating miRNA-21: AUC 0.653, accuracy
62.3%). Although they did not focus on discriminating IPMCs from
benign IPMNs, in contrast to our study, the results indicated the
superiority of encapsulated miRNAs over circulating miRNAs as
diagnostic markers.
While we cannot find any relevant data regarding
miR-6132 and tumors, the expression of miR-22 and miR-4539 in
cancer tissue has been studied in gastric cancer, rhabdomyosarcoma,
breast cancer, prostate cancer, osteosarcoma and papillary thyroid
cancer (21–30). Most studies have reported that, in
contrast to their expression levels in the blood, the expression
levels of these miRNAs are decreased in cancer tissue. Moreover,
in vivo and in vitro studies regarding the
biophysical properties of those miRNAs encapsulated in EVs have not
been conducted. Hence, the mechanism by which the 3 EV-miRNAs in
the blood contribute to IPMN progression has not been elucidated.
As in silico analysis suggests, inhibition of the NOD-like receptor
signaling pathway may be a cause of IPMN progression. NOD-like
receptors are genetically conserved proteins that belong to the
cellular pattern recognition receptor protein family. They are
important components in the innate immune system of mammals,
regulating the immune response and inflammatory response. Recently,
accumulative evidence has extended the concept that the NOD-like
receptor signaling pathway contributes to the activation of the
antitumor immune response by priming antitumor CD4+ and
CD8+ T cells (31).
Considering this result, increased expression of EV-miRNAs might be
attributable to suppression of the antitumor immune response and
progression of IPMN. Regarding the other 2 pathways,
glycosphingolipid biosynthesis-lacto and neolacto series- and fat
digestion and absorption, we could not find any relevant
studies.
Regarding progression of IPMN to IPMC, EV-miR-6132
may play an important role because its serum levels are higher in
IPMC patients than in benign IPMN patients. Further evaluation
revealed that 3 tumor suppressor genes (TSC2, TP53I11 and PPP2R5D)
were found among 717 target genes. Aberrant tumor suppressor gene
methylation which lead to gene suppression just like miRNA is often
found in IPMC, and we speculate that the high level of EV-miR-6132
in the serum of IPMC patients may influence tumor suppressor gene
activity as well (16).
Several limitations were found in this study. First,
this study was conducted in a single referral center, and the
results may not be generalizable to all patients with IPMNs and
IPMCs. The relatively small sample size also limited the
reliability of our statistical analysis. Second, only 9 of 38 IPMN
patients underwent surgical resection. The remaining 29 patients
were diagnosed with a benign IPMN or an IPMC based on the imaging
findings and clinical outcomes. Third, we did not investigate the
expression levels of the 3 miRNAs in the tumor tissue, and we do
not know whether the miRNAs directly contribute to carcinogenesis
or tumor progression. Therefore, we must conduct a further study
that includes a large number of patients with histopathological
evaluation.
In conclusion, we found that EV-miRNAs can be
diagnostic markers for use in detecting IPMNs in the general
population as well as in identifying IPMNs with high malignant
potential.
Acknowledgements
The authors would like to thank Ms. Chikako Sato and
Ms. Rie Hikichi (Department of Gastroenterology, Fukushima Medical
University School of Medicine) for their assistance in the
experiments.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during the present
study are included in the published article.
Authors' contributions
YS, RS and HO conceived and designed the
experiments. YS and RS performed the experiments. YS, RS, TT, MS
and HO collected and analyzed the data. YS, RS, TT, MS and HO
interpreted the results and wrote the manuscript. All authors read
and approved the manuscript, and agree to be accountable for all
aspects of the research and to guarantee for the accuracy and
integrity of any part of the work.
Ethics approval and consent to
participate
The study protocol conformed to the ethical
guidelines of the 1975 Declaration of Helsinki and was approved by
the institutional review board of Fukushima Medical University (IRB
#2387). All participants provided written informed consent for
participation.
Patient consent for publication
All participants provided written informed consent
for publication.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Tanaka M, Fernandez-Del Castillo C,
Kamisawa T, Jang JY, Levy P, Ohtsuka T, Salvia R, Shimizu Y, Tada M
and Wolfgang CL: Revisions of international consensus Fukuoka
guidelines for the management of IPMN of the pancreas.
Pancreatology. 17:738–753. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Oyama H, Tada M, Takagi K, Tateishi K,
Hamada T, Nakai Y, Hakuta R, Ijichi H, Ishigaki K, Kanai S, et al:
Long-term risk of malignancy in branch-duct intraductal papillary
mucinous neoplasms. Gastroenterology. 158:226–237 e5. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Al-Haddad M, DeWitt J, Sherman S, Schmidt
CM, LeBlanc JK, McHenry L, Coté G, El Chafic AH, Luz L, Stuart JS,
et al: Performance characteristics of molecular (DNA) analysis for
the diagnosis of mucinous pancreatic cysts. Gastrointest Endosc.
79:79–87. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Matthaei H, Wylie D, Lloyd MB, Dal Molin
M, Kemppainen J, Mayo SC, Wolfgang CL, Schulick RD, Langfield L,
Andruss BF, et al: mRNA biomarkers in cyst fluid augment the
diagnosis and management of pancreatic cysts. Clin Cancer Res.
18:4713–4724. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Takano S, Fukasawa M, Maekawa S, Kadokura
M, Miura M, Shindo H, Takahashi E, Sato T and Enomoto N: Deep
sequencing of cancer-related genes revealed GNAS mutations to be
associated with intraductal papillary mucinous neoplasms and its
main pancreatic duct dilation. PLoS One. 9:e987182014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Moris D, Damaskos C, Spartalis E,
Papalampros A, Vernadakis S, Dimitroulis D, Griniatsos J,
Felekouras E and Nikiteas N: Updates and critical evaluation on
novel biomarkers for the malignant progression of intraductal
papillary mucinous neoplasms of the pancreas. Anticancer Res.
37:2185–2194. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Tanaka M, Heckler M, Liu B, Heger U,
Hackert T and Michalski CW: Cytologic analysis of pancreatic juice
increases specificity of detection of malignant IPMN-A systematic
review. Clin Gastroenterol Hepatol. 17:2199–2211 e21. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Reddy KB: MicroRNA (miRNA) in cancer.
Cancer Cell Int. 15:382015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Peng Y and Croce CM: The role of microRNAs
in human cancer. Signal Transduct Target Ther. 1:150042016.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Jansson MD and Lund AH: MicroRNA and
cancer. Mol Oncol. 6:590–610. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hayes J, Peruzzi PP and Lawler S:
MicroRNAs in cancer: Biomarkers, functions and therapy. Trends Mol
Med. 20:460–469. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
de Miguel Perez D, Rodriguez Martinez A,
Ortigosa Palomo A, Delgado Ureña M, Garcia Puche JL, Robles Remacho
A, Exposito Hernandez J, Lorente Acosta JA, Ortega Sánchez FG and
Serrano MJ: Extracellular vesicle-miRNAs as liquid biopsy
biomarkers for disease identification and prognosis in metastatic
colorectal cancer patients. Sci Rep. 10:39742020. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Conte D, Verri C, Borzi C, Suatoni P,
Pastorino U, Sozzi G and Fortunato O: Novel method to detect
microRNAs using chip-based QuantStudio 3D digital PCR. BMC
Genomics. 16:8492015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Suzuki R, Asama H, Waragai Y, Takagi T,
Hikichi T, Sugimoto M, Konno N, Watanabe K, Nakamura J, Kikuchi H,
et al: Fibrosis-related miRNAs as serum biomarkers for pancreatic
ductal adenocarcinoma. Oncotarget. 9:4451–4460. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Vlachos IS, Zagganas K, Paraskevopoulou
MD, Georgakilas G, Karagkouni D, Vergoulis T, Dalamagas T and
Hatzigeorgiou AG: DIANA-miRPath v3.0: Deciphering microRNA function
with experimental support. Nucleic Acids Res. 43((W1)): W460–W466.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
House MG, Guo M, Iacobuzio-Donahue C and
Herman JG: Molecular progression of promoter methylation in
intraductal papillary mucinous neoplasms (IPMN) of the pancreas.
Carcinogenesis. 24:193–198. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Huang da W, Sherman BT, Zheng X, Yang J,
Imamichi T, Stephens R and Lempicki RA: Extracting biological
meaning from large gene lists with DAVID. Curr Protoc
Bioinformatics Chapter. 13:Unit 13 11. 2009.doi:
10.1002/0471250953.bi1311s27.
|
|
18
|
Huang da W, Sherman BT and Lempicki RA:
Bioinformatics enrichment tools: Paths toward the comprehensive
functional analysis of large gene lists. Nucleic Acids Res.
37:1–13. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Habbe N, Koorstra JB, Mendell JT,
Offerhaus GJ, Ryu JK, Feldmann G, Mullendore ME, Goggins MG, Hong
SM and Maitra A: MicroRNA miR-155 is a biomarker of early
pancreatic neoplasia. Cancer Biol Ther. 8:340–346. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Goto T, Fujiya M, Konishi H, Sasajima J,
Fujibayashi S, Hayashi A, Utsumi T, Sato H, Iwama T, Ijiri M, et
al: An elevated expression of serum exosomal microRNA-191, −21,
−451a of pancreatic neoplasm is considered to be efficient
diagnostic marker. BMC Cancer. 18:1162018. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Pasqualini L, Bu H, Puhr M, Narisu N,
Rainer J, Schlick B, Schäfer G, Angelova M, Trajanoski Z, Börno ST,
et al: mR-22 and miR-29a are members of the androgen receptor
cistrome modulating LAMC1 and Mcl-1 in prostate cancer. Mol
Endocrinol. 29:1037–1054. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Wang G, Shen N, Cheng L, Lin J and Li K:
Downregulation of miR-22 acts as an unfavorable prognostic
biomarker in osteosarcoma. Tumour Biol. 36:7891–7895. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Bersani F, Lingua MF, Morena D, Foglizzo
V, Miretti S, Lanzetti L, Carrà G, Morotti A, Ala U, Provero P, et
al: Deep sequencing reveals a novel miR-Regulatory network with
therapeutic potential in rhabdomyosarcoma. Cancer Res.
76:6095–6106. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Koufaris C, Valbuena GN, Pomyen Y,
Tredwell GD, Nevedomskaya E, Lau CH, Yang T, Benito A, Ellis JK and
Keun HC: Systematic integration of molecular profiles identifies
miR-22 as a regulator of lipid and folate metabolism in breast
cancer cells. Oncogene. 35:2766–2776. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Jafarzadeh-Samani Z, Sohrabi S,
Shirmohammadi K, Effatpanah H, Yadegarazari R and Saidijam M:
Evaluation of miR-22 and miR-20a as diagnostic biomarkers for
gastric cancer. Chin Clin Oncol. 6:162017. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Fu Q, Liu CJ, Zhang X, Zhai ZS, Wang YZ,
Hu MX, Xu XL, Zhang HW and Qin T: Glucocorticoid receptor regulates
expression of microRNA-22 and downstream signaling pathway in
apoptosis of pancreatic acinar cells. World J Gastroenterol.
24:5120–5130. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Sui J, Liu Q, Zhang H and Kong Y: Deep
integrative analysis of microRNA-mRNA regulatory networks for
biomarker and target discovery in chondrosarcoma. J Cell Biochem.
120:9631–9638. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Wang D, Guo C, Kong T, Mi G, Li J and Sun
Y: Serum miR-22 may be a biomarker for papillary thyroid cancer.
Oncol Lett. 17:3355–3361. 2019.PubMed/NCBI
|
|
29
|
Pellatt DF, Stevens JR, Wolff RK, Mullany
LE, Herrick JS, Samowitz W and Slattery ML: Expression profiles of
miRNA subsets distinguish human colorectal carcinoma and normal
colonic mucosa. Clin Transl Gastroenterol. 7:e1522016. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Medarova Z, Pantazopoulos P and Yoo B:
Screening of potential miRNA therapeutics for the prevention of
multi-drug resistance in cancer cells. Sci Rep. 10:19702020.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Garaude J, Kent A, van Rooijen N and
Blander JM: Simultaneous targeting of toll- and nod-like receptors
induces effective tumor-specific immune responses. Sci Transl Med.
4:120ra1162012. View Article : Google Scholar
|