Introduction
Hepatocellular carcinoma (HCC) is an international
health problem that places a substantial burden on the healthcare
system (1). Low-cost treatment
options are recommended for economic reasons. Recent studies have
demonstrated that an increased preoperative neutrophil-lymphocyte
ratio (NLR) is an economical independent prognostic indicator in
several different types of malignancy, including HCC (2,3),
glioblastoma multiforme (4),
pancreatic neuroendocrine tumors (5), gastric (6), ovarian (7), renal (8)
and breast cancer (9).
Persistent inflammation promotes and accelerates the
progression of malignant tumors at different stages of tumor
development, including initiation, progression, malignant
conversion, invasion and metastasis (10). In recent years, certain studies have
focused on the effect of postoperative NLR on the prognosis of
patients with malignant tumors (11–21) and
have reported that an increased postoperative NLR was associated
with poorer survival outcomes in patients with solid tumors
(12,15,21).
Certain studies have begun to focus on the association between
preoperative NLR and postoperative NLR: Postoperative NLR changes
for advanced tumors (13,14); the preoperative plus the
postoperative NLR for gastric cancer (15); and the postoperative NLR minus
preoperative NLR for HCC (3,16), colorectal (17), non-small-cell lung (18) and gastric cancer (19,20).
Some of these studies were based on the hypothesis that the
postoperative NLR is higher than the preoperative NLR following
treatment, which may be due to a protumor inflammatory response,
and they found that patients with a postoperative NLR higher than
the preoperative NLR had a poorer prognosis (3,13,14,16–20).
However, the association between the preoperative NLR and
postoperative NLR remains controversial, and it may not be
appropriate to study the postoperative NLR in the context of the
preoperative NLR. Peng et al (16) reported that the balance between the
immune response and the inflammatory response may change following
the surgical removal of HCC lesions.
HCC is a typical example of an inflammation-related
tumor, as >90% of HCC cases arise in the context of hepatic
injury and inflammation (1,22). The prognostic utility of the
preoperative NLR and postoperative NLR for HCC requires further
study. Although preoperative NLR minus postoperative NLR was
identified as an independent prognostic factor for HCC in previous
studies, no significant differences were identified between the two
groups for commonly evaluated clinicopathological features
(3,16). Therefore, the application and
reliability of the postoperative NLR minus preoperative NLR and
other associated combinations for the prognosis of HCC require
further study.
Materials and methods
Patient selection
A total of 70 patients undergoing partial
hepatectomy for primary HCC admitted to Beijing Tsinghua Chang Gung
Hospital affiliated with Tsinghua University (Beijing, China)
between December 2014 and July 2019 were retrospectively analyzed.
The mean patient age was 56.97±10.06 years (range, 33–81 years).
The HCC cohort consisted of 54 males (77.1%) and 16 females
(22.9%). The study was approved by the Ethics Committee of Beijing
Tsinghua Chang Gung Hospital (Beijing, China). The inclusion
criteria were as follows: i) pathological diagnosis of primary HCC
with a planned treatment of curative resection; ii) no redness or
exudation from the incision when the patient was discharged from
the hospital and no infections or complications at the time of
discharge; iii) complete demographic data; iv) complete laboratory
and imaging examinations; and v) regular follow-up following the
operation.
Clinicopathological variables
All patient data (including laboratory indicators,
imaging data and pathology data) were obtained from the hospital's
electronic information system. The preoperative laboratory
indicators were taken from the first laboratory results after
admission. The postoperative laboratory examinations were performed
1–2 days before discharge after all complications had been
resolved. At that time, the surgical incisions had no redness or
exudations. The overall survival (OS) time was defined as the day
of surgery until the day the patient died or the last follow-up
day. All the deceased patients died as a result of their
tumors.
The study variables included the following:
(1) general information (age and
sex); (2) blood test results [white
blood cells, neutrophils, lymphocytes, hepatitis B surface antigen
(HBsAg), albumin, and alpha-fetoprotein (AFP)]; (3) pathological indicators (cirrhosis, tumor
number, tumor size and tumor differentiation); (4) prognostic information (patient survival
time); and (5) complications.
According to the World Health Organization standards, the degree of
differentiation of HCC was divided into poorly-, moderately- and
highly-differentiated (23).
The present study investigated the effect of the
preoperative NLR, postoperative NLR, postoperative NLR change,
preoperative NLR plus postoperative NLR and postoperative NLR minus
preoperative NLR on the prognosis of patients with HCC following
resection. The NLR was defined as the ratio of the absolute number
of neutrophils to the absolute number of lymphocytes (19). The postoperative change was defined
as the postoperative NLR divided by the preoperative NLR (13). The postoperative NLR minus
preoperative NLR was defined as the postoperative NLR value minus
the preoperative NLR value (3,18). The
preoperative NLR plus the postoperative NLR value was calculated
based on the preoperative NLR and postoperative NLR cut-off values
as follows: Patients with both an increased preoperative NLR and
postoperative NLR were assigned a score of 2, patients showing
either an increased preoperative NLR or an elevated postoperative
NLR were assigned a score of 1, and patients in whom neither the
preoperative NLR nor the postoperative NLR was increased were
assigned a score of 0.
Statistical analysis
Categorical data are reported as the number and
percentage of cases. The chi-square test or Fisher's exact test
were used to analyze the categorical data. Continuous variables are
reported as the mean ± standard deviation and were compared using
Student's t-test or analysis of variance (3,24). A Cox
proportional hazard model was used for the univariate and
multivariate analyses. The survival curve was drawn with the
‘Surv_fit’ function in the R software (25).
The optimal cut-off for continuous variables was
determined by using the maximally selected rank statistics by the
‘surv_cutpoint’ function of the ‘survminer’ R package (26,27). The
time-dependent receiver operating characteristic (td-ROC) curve was
estimated to assess the performance of the preoperative NLR,
postoperative NLR, postoperative NLR change, preoperative NLR plus
postoperative NLR, and postoperative NLR minus preoperative NLR.
The time-dependent area under the curve (td-AUC) was calculated by
the survival ROC function of the R software, and a larger td-AUC
indicated more accurate prognostic stratification (25). All data were analyzed using SPSS 26.0
software (IBM Corp.) and R version 3.6.1 (http://www.r-project.org/). Graphs were created using
R software. P<0.05 was considered to indicate a statistically
significant difference.
Results
Baseline characteristics
A total of 70 patients with HCC were included in the
present study. Hepatitis B was diagnosed in 59 patients. The mean
tumor size was 5.67±3.92 cm, and the number of patients with
solitary tumors was 57 (81.4%). The number of patients with
cirrhosis was 33 (47.1%). Complications included biliary leakage
(n=2, 2.86%), pleural effusion (n=56, 80%), pneumonia (n=3, 4.29%)
and perihepatic effusion (n=1, 1.43%). The mean preoperative white
blood cell, neutrophil and lymphocyte counts and the postoperative
white blood cell, neutrophil and lymphocyte counts were 5.41±1.91,
3.26±1.76, 1.55±0.56, 5.98±2.14 ng/ml, 3.82±1.61 and 1.39±0.65
mg/l, respectively.
Optimal cut-offs for continuous
variables
The optimal cut-offs of the preoperative NLR,
postoperative NLR, postoperative NLR change and postoperative NLR
minus preoperative NLR were 3.46, 4.33, −0.25 and 3.42,
respectively. The optimal cut-off for age and tumor size were also
calculated (47-years-old and 5 cm, respectively).
Clinical and pathological data for
preoperative NLR and postoperative NLR
An increased preoperative NLR was associated with a
higher preoperative white blood cell count (P<0.001), higher
preoperative neutrophil count (P=0.001), lower preoperative
lymphocyte count (P<0.003) and larger tumor size (P=0.001). An
increased postoperative NLR was associated with a higher
postoperative white blood cell count (P=0.010), higher
postoperative neutrophil count (P<0.001), and lower
postoperative lymphocyte count (P=0.005). There was no correlation
between an increased preoperative NLR and the occurrence of
complications. Similarly, there was no statistically significant
difference in complications between the low and high postoperative
NLR groups (Table I).
 | Table I.Comparison of baseline clinical
characteristics according to preoperative NLR and postoperative NLR
values. |
Table I.
Comparison of baseline clinical
characteristics according to preoperative NLR and postoperative NLR
values.
| Baseline
variable | Overall,
(n=70) | Preoperative
NLR≤3.46, (n=61) | Preoperative
NLR>3.4, (n=9) | P-value | Postoperative
NLR≤4.33, (n=58) | Postoperative
NLR>4.33, (n=12) | P-value |
|---|
| Age, years | 56.97±10.06 | 57.33±9.84 | 54.56±11.81 | 0.444 | 56.57±10.16 | 58.92±9.75 | 0.466 |
| Sex, male | 54 (77.1) | 45 (73.8) | 9 (100) | 0.082 | 42 (72.3) | 12 (100) | 0.055 |
| HBsAg (+) | 59 (84.3) | 51 (83.6) | 8 (88.9) | 1.000 | 49 (84.5) | 10 (83.3) | 1.000 |
| AFP (ng/ml) | 662.48±808.76 | 666.38±808.31 | 636.06±860.53 | 0.917 | 656.96±787.73 | 689.16±941.62 | 0.901 |
| Preoperative WBC
(109/l) | 5.41±1.91 | 5.02±1.20 | 8.10±3.40 | <0.001 | 5.33±1.84 | 5.84±2.28 | 0.407 |
| Preoperative
neutrophil (109/l) | 3.26±1.76 | 2.81±0.87 | 6.31±3.01 | 0.001 | 1.68±0.22 | 3.87±2.09 | 0.187 |
| Preoperative
lymphocyte (109/l) | 1.54±0.57 | 1.63±0.56 | 1.03±0.33 | <0.003 | 1.61±0.57 | 1.27±0.51 | 0.069 |
| Albumin (g/dl) | 42.53±8.53 | 43.25±8.84 | 37.68±3.30 | 0.067 | 43.15±9.14 | 39.55±3.41 | 0.185 |
| Postoperative WBC
(109/l) | 5.98±2.14 | 5.85±1.92 | 6.86±3.27 | 0.190 | 5.69±2.07 | 7.42±1.94 | 0.010 |
| Postoperative
neutrophil (109/l) | 3.83±1.61 | 3.70±1.50 | 4.70±2.12 | 0.080 | 3.47±1.39 | 5.56±1.56 | <0.001 |
| Postoperative
lymphocyte (109/l) | 1.39±0.65 | 1.41±0.56 | 1.29±1.13 | 0.627 | 1.49±0.66 | 0.92±0.31 | 0.005 |
| Cirrhosis, yes | 33 (47.1) | 28 (45.9) | 5 (55.6) | 0.854 | 27 (46.6) | 6 (50.0) | 0.828 |
| Tumor size, cm | 5.67±3.92 | 5.04±3.51 | 9.88±4.19 | 0.001 | 5.46±3.74 | 6.68±4.77 | 0.327 |
| Tumor number,
multiple | 13 (18.57) | 10 (16.39) | 2 (22.22) | 1.000 | 10 (17.24) | 2 (16.67) | 1.000 |
| Differentiation,
poor | 8 (11.43) | 6 (9.84) | 2 (22.22) | 0.597 | 5 (8.62) | 3 (25) | 0.261 |
| Biliary
leakage | 2 (2.86) | 2 (3.28) | 0 (0) | 1.000 | 2 (3.45) | 0 (0) | 1.000 |
| Pleural
effusion | 56 (70) | 49 (80.33) | 7 (77.78) | 1.000 | 45 (77.59) | 12 (91.67) | 0.267 |
| Pneumonia | 3 (4.28) | 3 (4.91) | 0 (0) | 0.858 | 3 (5.17) | 0 (0) | 0.982 |
| Perihepatic
effusion | 1 (1.43) | 1 (1.66) | 0 (0) | 1.000 | 1 (1.72) | 0 (0) | 1.000 |
Survival analysis
A total of 19 patients (27.14%) died during the
follow-up period. The mean survival duration was 12 months (range,
2–52 months). The 1-, 2-, 3- and 4-year OS rates were 87.1, 74.0,
72.8 and 72.8%, respectively.
The 70 patients with HCC were divided into 2 groups
according to their preoperative NLR values: preoperative NLR≤3.46
(n=61) and preoperative NLR>3.46 (n=9; Fig. 1A). Likewise, the patients with HCC
were divided into 2 groups according to their postoperative NLR
profiles: postoperative NLR≤4.33 (n=58) and postoperative
NLR>4.33 (n=12; Fig. 1B). Using
the Surv_fit function to analyze patient survival, high
preoperative NLR and high postoperative NLR were significantly
associated with OS (P=0.00068 and P=0.0044, respectively; Fig. 1A and B).
The 70 patients with HCC were divided into 2 groups
according to their postoperative NLR change and postoperative NLR
minus preoperative NLR values: postoperative NLR change>-0.25
(n=9) and postoperative NLR minus preoperative NLR≥3.42 (n=7). In
the Surv_fit function analysis, a high postoperative NLR change was
not a significant prognostic factor (P=0.27; Fig. 1C), but a high postoperative NLR minus
preoperative NLR of ≥3.42 was significantly associated with a
decreased OS (P=0.0048) (Fig.
1D).
Patients with preoperative NLR plus postoperative
NLR scores of 0 had the most favorable outcomes, and patients with
preoperative NLR plus postoperative NLR=2 had the poorest
prognosis. These findings indicated that an increased preoperative
NLR and an increased postoperative NLR were significantly
associated with poor survival compared with a low preoperative NLR
and/or postoperative NLR (P=0.00033; Fig. 1E).
Factors associated with prognosis
To identify the independent prognostic risk factors
in patients with primary HCC undergoing partial hepatectomy, Cox
univariate and multivariate analyses were performed. The results of
the univariate analysis are shown in Table II. The univariate analysis showed
that tumor size (HR, 2.795; 95% CI, 1.099–7.110; P=0.031),
preoperative NLR plus postoperative NLR (HR, 2.985; 95% CI,
1.648–5.407; P<0.001), preoperative NLR (HR, 4.618; 95% CI,
1.728–12.339; P=0.002), postoperative NLR (HR, 3.512; 95% CI,
1.728–12.339; P=0.008), and postoperative NLR minus preoperative
NLR (HR, 3.296; 95% CI, 1.181–9.199; P=0.023) were significantly
associated with a poor OS. Subsequently, the multivariate analysis
identified the preoperative NLR plus postoperative NLR (HR, 2.985;
95% CI, 1.648–5.407; P<0.001) as an independent prognostic risk
factor (Table II).
| Table II.Univariate and multivariate analyses
of prognostic factors of overall survival for patients with
hepatocellular carcinoma. |
Table II.
Univariate and multivariate analyses
of prognostic factors of overall survival for patients with
hepatocellular carcinoma.
|
| Univariate
analyses | Multivariate
analyses |
|---|
|
|
|
|
|---|
| Baseline
variable | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Age, >47
years | 0.696 | 0.250–1.936 | 0.488 |
|
|
|
| Sex, male | 3.010 | 0.694–13.045 | 0.141 |
|
|
|
| HBsAg (+) | 1.521 | 0.351–6.590 | 0.575 |
|
|
|
| AFP, >20
ng/ml | 2.340 | 0.681–8.047 | 0.177 |
|
|
|
| Preoperative WBC,
109/l | 1.030 | 0.830–1.297 | 0.786 |
|
|
|
| Preoperative
neutrophil, 109/l | 1.087 | 0.855–1.334 | 0.427 |
|
|
|
| Preoperative
lymphocyte, 109/l | 0.534 | 0.255–1.266 | 0.154 |
|
|
|
| Albumin, g/dl | 0.920 | 0.841–1.007 | 0.071 |
|
|
|
| Postoperative WBC,
109/l | 1.040 | 0.848–1.277 | 0.704 |
|
|
|
| Postoperative
neutrophil, 109/l | 1.224 | 0.939–1.596 | 0.135 |
|
|
|
| Postoperative
lymphocyte, 109/l | 0.682 | 0.291–1.599 | 0.379 |
|
|
|
| Cirrhosis, yes | 0.943 | 0.382–2.330 | 0.899 |
|
|
|
| Tumor size, >5
cm | 2.795 | 1.099–7.110 | 0.031 |
|
|
|
| Tumor number,
multiple | 1.549 | 0.513–4.681 | 0.438 |
|
|
|
| Differentiation,
poor | 3.079 | 1.001–9.473 | 0.050 |
|
|
|
| Biliary
leakage | 0.048 |
0.000–70634.465 | 0.675 |
|
|
|
| Pleural
effusion | 0.688 | 0.227–2.086 | 0.508 |
|
|
|
| Pneumonia | 0.941 | 0.126–7.060 | 0.953 |
|
|
|
| Perihepatic
effusion | 0.048 |
0.000–103525.973 | 0.683 |
|
|
|
| Preoperative
NLR | 4.618 | 1.728–12.339 | 0.002 |
|
|
|
| Postoperative
NLR | 3.512 | 1.381–8.934 | 0.008 |
|
|
|
| Preoperative NLR
plus Postoperative NLR | 2.985 | 1.648–5.407 | <0.001 | 2.985 | 1.648–5.407 | <0.001 |
| Postoperative NLR
change | 0.548 | 0.182–1.654 | 0.286 |
|
|
|
| Postoperative NLR
minus Preoperative NLR | 3.296 | 1.181–9.199 | 0.023 |
|
|
|
Preoperative NLR plus postoperative
NLR is superior to other factors in predicting prognosis
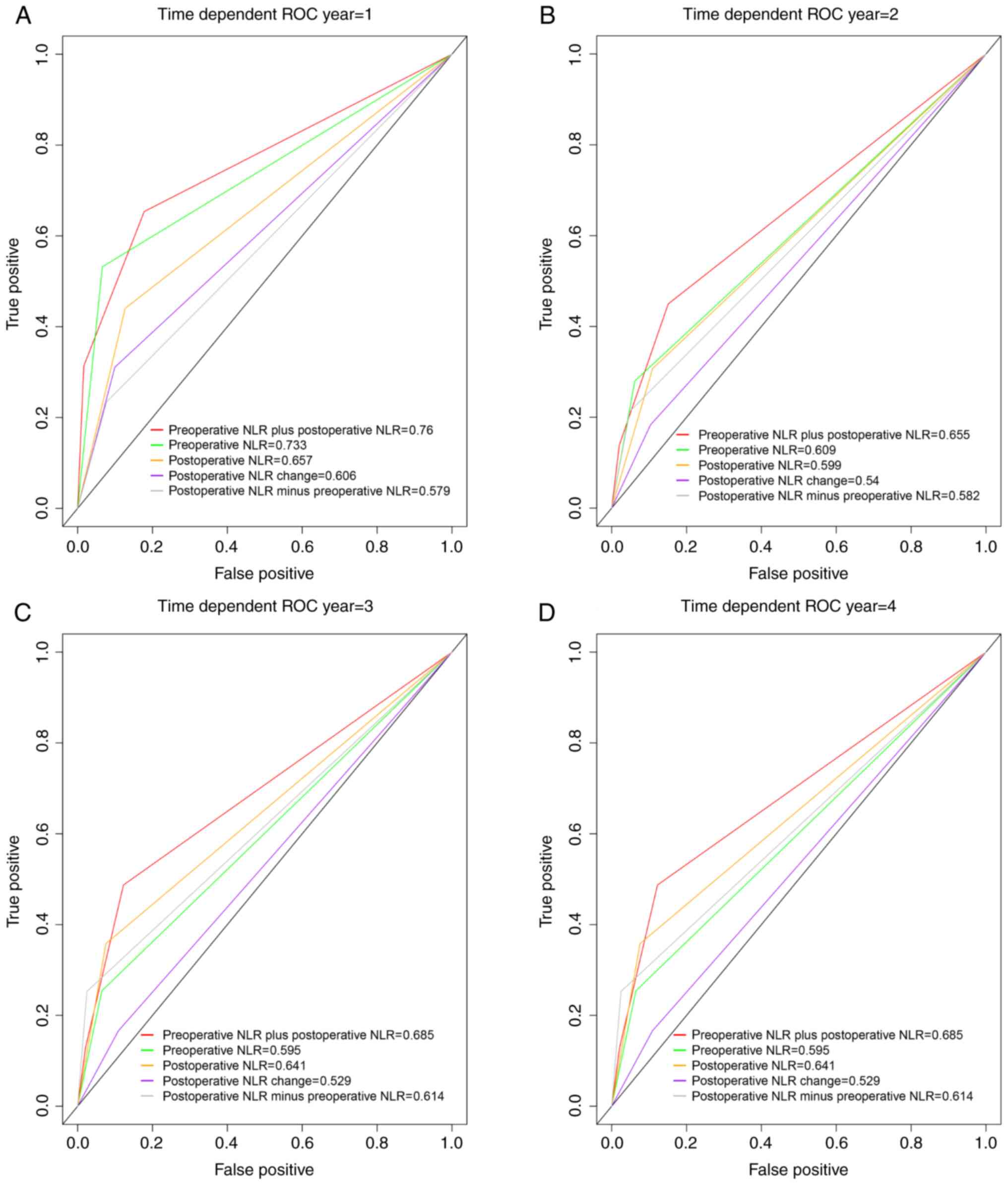
The td-ROC curves were used to assess the
discriminatory abilities of the preoperative NLR plus postoperative
NLR, preoperative NLR, postoperative NLR, postoperative NLR change,
and postoperative NLR minus preoperative NLR in terms of prognosis.
The preoperative NLR plus postoperative NLR had higher td-AUC
values at 1 year (0.76), 2 years (0.655), 3 years (0.685) and 4
years (0.685) than the preoperative NLR (1 year, td-AUC=0.733; 2
years, td-AUC=0.609; 3 years, td-AUC=0.595; and 4 years,
td-AUC=0.595; Fig. 2).
Compared with the postoperative NLR, the
preoperative NLR plus postoperative NLR had higher td-AUC values (1
year, 0.76 vs. 0.657; 2 years, 0.655 vs. 0.599; 3 years, 0.685 vs.
0.641; and 4 years, 0.685 vs. 0.641; Fig. 2).
The preoperative NLR plus postoperative NLR had
higher td-AUC values at 1 year (0.76), 2 years (0.655), 3 years
(0.685) and 4 years (0.685) than the CNLR (1 year, td-AUC=0.606; 2
years, td-AUC=0.54; 3 years, td-AUC=0.529; and 4 years,
td-AUC=0.529; Fig. 2). Similarly,
the preoperative NLR plus postoperative NLR had a higher td-AUC
than the postoperative NLR minus preoperative NLR in the first to
fourth years (Fig. 2).
Clinical and pathological data for
preoperative NLR plus postoperative NLR
Among the 70 patients, 53 (75.71%) were classified
as having a preoperative NLR plus postoperative NLR score of 0,
whereas 13 (15.87%) and 4 (0.06%) were classified as having a
preoperative NLR plus postoperative NLR score of 1 and 2,
respectively. Patients in the preoperative NLR plus postoperative
NLR=2 group had a relatively larger tumor size than those in the
preoperative NLR plus postoperative NLR=1/0 group (P=0.013).
Patients in the preoperative NLR plus postoperative NLR=0 group had
relatively lower preoperative white blood cell (P=0.004) and
postoperative neutrophil counts than those in the preoperative NLR
plus postoperative NLR=2 group (P<0.001). The preoperative
lymphocytes were significantly lower in patients in the
preoperative NLR plus postoperative NLR=2 group than in those in
the preoperative NLR plus postoperative NLR=0 group (P=0.012). An
increased preoperative NLR plus postoperative NLR score was
associated with multiple tumors and poor differentiation. The
demographic and clinicopathological features of the patients
according to the preoperative NLR plus postoperative NLR score are
shown in Table III.
| Table III.Comparison of clinical and
pathological data according to preoperative NLR plus postoperative
NLR values. |
Table III.
Comparison of clinical and
pathological data according to preoperative NLR plus postoperative
NLR values.
| Baseline
variable | Preoperative NLR
plus postoperative NLR=0, n=53 | Preoperative NLR
plus postoperative NLR=1, n=13 | Preoperative NLR
plus postoperative NLR=2, n=4 | P-value |
| Age, years | 59.19±9.837 | 55.08±11.507 | 60.25±9.467 | 0.641 |
| Sex, male | 37 (69.8) | 13 (100) | 4 (100) | 0.036 |
| HBsAg (+) | 44 (83) | 12 (92.3) | 3 (75) | 0.623 |
| AFP, ng/ml |
683.522±801.952 |
484.569±776.219 |
961.883±1105.531 | 0.552 |
| Preoperative WBC,
109/l | 5.018±1.195 | 6.046±3.040 | 7.458±3.154 | 0.004a |
| Preoperative
neutrophil, 109/l | 2.787±0.876 | 4.417±2.875 | 5.728±2.683 | <0.001 |
| Preoperative
lymphocyte, 109/l | 1.652±0.561 | 1.319±0.499 | 0.933±0.219 | 0.012b |
| Albumin, g/dl | 43.634±9.393 | 39.685±2.757 | 37.225±4.322 | 0.144 |
| Postoperative WBC,
109/l | 5.603±1.870 | 7.152±2.498 | 7.218±2.981 | 0.029c |
| Postoperative
neutrophil, 109/l | 3.427±1.354 | 4.882±1.621 | 5.695±2.300 |
<0.001a |
| Postoperative
lymphocyte, 109/l | 1.474±0.566 | 1.254±0.918 | 0.803±0.387 | 0.094 |
| Cirrhosis, yes | 24 (45.3) | 7 (53.8) | 2 (50) | 0.852 |
| Tumor size, cm | 5.111±3.622 | 6.331±3.618 | 10.850±5.555 | 0.013d |
| Tumor number,
multiple | 10 (18.86) | 0 (0) | 2 (50) | 0.027 |
| Differentiation,
poor | 5 (9.43) | 1 (7.69) | 2 (50) | 0.044 |
| Biliary
leakage | 2 (3.77) | 0 (0) | 0 (0) | 0.568 |
| Pleural
effusion | 42 (79.24) | 10 (76.9) | 4 (100) | 0.391 |
| Pneumonia | 3 (5.66) | 0 (0) | 0 (0) | 0.425 |
| Perihepatic
effusion | 1 (1.88) | 0 (0) | 0 (0) | 0.755 |
Discussion
A high NLR reflects a decreased lymphocyte count and
a relatively increased neutrophil count. Generally, neutrophils
promote HCC progression and drug resistance (28), while lymphocytes may delay HCC
progression (29). The mechanism by
which inflammation promotes the development, progression and
invasion of malignant tumors is complicated. The NLR may reflect
the preoperative and postoperative immune responses. Morizawa et
al (30) suggested that a high
NLR was correlated with increased IL-6 and IL-8 and regulatory T
cell expression. IL-6 prevents DNA-damage-induced hepatocyte
apoptosis and enhances tumor proliferation, and IL-6
trans-signaling directly induces endothelial cell proliferation to
promote tumor angiogenesis in a mouse HCC model (31). Cools-Lartigue et al (32) indicated that neutrophil extracellular
trap deposition resulted in increased tumor cell adhesion to the
hepatic microvasculature in vivo. Tumor cell trapping within
neutrophil extracellular traps was associated with increased
micrometastases (32).
Recently, numerous studies have indicated that an
increased preoperative NLR is a reliable and economical independent
prognostic indicator in different malignancies (2–8), and an
increasing amount of research has focused on the effect of the
postoperative inflammatory state on the prognosis of cancer
(3,13–20,33).
These studies have used traditional statistical methods, including
ROC curves, to obtain optimal cut-offs (2–8,13–20,33).
However, survival analysis is different from diagnostic
experiments. The ROC curve may not be optimal in assessing models
that stratify individuals into risk categories (34). Maximally selected rank statistics
have been proven to be more effective for determining the cut-offs
of continuous variables in survival analyses (26). Therefore, the present study used
maximally selected rank statistics instead of ROC curves to obtain
the best cut-offs. It is worth noting that certain studies have
defined the time to obtain postoperative NLR as 1 month after
surgery, but there were no infections and complications in the
exclusion criteria (11,20). However, complications and infections
may affect postoperative NLR (35).
Certain studies have obtained postoperative NLR at least 1 month or
3–6 months after surgery (18,19). The
time interval for obtaining postoperative NLR was long, and the
tumor may have progressed or recurred. Therefore, postoperative NLR
at discharge was used in the present study. There are differences
in the discharge standards for different hospitals. Patients are
discharged only after they recover well (no infections and no
unresolved complications) in our hospital. Therefore, the timing of
obtaining the indicators in the present study may be relatively
appropriate.
Although HCC has a different background to other
solid tumors, and HCC is often based on chronic inflammation of the
liver. To the best of our knowledge, no previous studies have
compared the preoperative NLR of HCC with that of other solid
tumors. However, consistent with HCC, the meta-analysis showed that
patients with solid tumors in the high-NLR group had a poorer
prognosis (36,37). Zhou et al (38) found that their colorectal cancer
group had a higher leukocyte count, neutrophil ratio and NLR than
their adenomatous polyp group and healthy control group. This
indicated that patients with a high tumor burden have a higher NLR.
Miyatani et al (15)
suggested that the preoperative NLR was significantly correlated
with tumor burden (tumor size, tumor depth, lymphatic invasion and
venous invasion), while there was no correlation between the
postoperative NLR and the various clinicopathological variables.
Shibutani et al (12) also
found that the postoperative NLR was not associated with
preoperative clinicopathological variables. The results of the
present study are consistent with those of previous studies; the
preoperative NLR was associated with tumor burden (tumor size) and
preoperative inflammatory markers (preoperative white blood cell,
neutrophil and lymphocyte counts), but there was no correlation
between the preoperative NLR and postoperative inflammatory
factors. Similarly, the postoperative NLR was associated with
postoperative inflammatory markers, and the postoperative NLR was
not associated with preoperative tumor burden or inflammatory
markers. A possible reason for this is that the preoperative NLR
represents the preoperative inflammatory status and high tumor
burden prior to surgery, and the postoperative NLR represents the
postoperative inflammatory status and potential tumor burden (for
example, micrometastases). Peng et al (16) reported that the balance between the
inflammatory response and the immune response may change following
the surgical removal of HCC tumors. It is certain that the tumor
burden following surgery is lower than that prior to surgery, but
the association between postoperative inflammatory status and
preoperative inflammatory status remains unclear. The immune status
prior to surgery differs from that following surgery, and the
optimal cut-offs for the preoperative NLR and the postoperative NLR
were different. The present study indicated that using the
postoperative NLR in the context of the preoperative NLR as a
baseline to predict prognosis may not be very accurate. The
prognostic effects of the preoperative NLR and postoperative NLR
should be considered separately.
Recent studies have combined the preoperative NLR
and postoperative NLR to study the prognostic impact on malignant
tumors. To the best of our knowledge, the present study was the
first to discuss the role of the preoperative NLR, postoperative
NLR, and their different combinations in determining the prognosis
of HCC. Similar to previous studies (2,3,11,12), an
increased preoperative NLR and an increased postoperative NLR were
prognostic factors in the study; the difference is that the results
of the present study suggested that an increased preoperative NLR
and an increased postoperative NLR were not independent prognostic
factors. However, the preoperative NLR plus postoperative NLR was
an independent prognostic factor for OS in patients with HCC.
Certain studies have divided the postoperative NLR by the
preoperative NLR or used the post NLR minus the preoperative NLR to
define novel prognostic factors (3,13,14,16–20).
Certain studies have hypothesized that an increase in the
postoperative NLR relative to the preoperative NLR following
treatment indicates that the balance has been tipped in favor of a
pro-tumor inflammatory response (3,16–20).
However, Lalani et al (13)
found that a relative NLR change of ≥25% from baseline to 6 weeks
after PD-1/PD-L1 immune checkpoint blockade therapy was an
independent prognostic factor for OS. Unlike previous studies
(13), the present study found that
the postoperative NLR cut-off was −0.25, instead of −0.25 and 0.25
as defined using traditional statistical methods. The present study
demonstrated a poor prognosis for a postoperative NLR change
reduction of <25%, but the prognostic difference between the two
groups was not statistically significant. The optimal cut-off for
the postoperative NLR minus preoperative NLR in this study was
3.42, rather than 0 (3,16,19,20),
0.037 (17) or 1.5 (18), as obtained using traditional
statistical methods. The results of the present study suggested
that the postoperative NLR change and postoperative NLR minus
preoperative NLR were not independent prognostic factors for OS.
Although the postoperative NLR minus preoperative NLR was an
independent prognostic factor for HCC in previous studies, no
significant differences were identified between the two groups in
terms of commonly used clinicopathological features (3,16).
Unfortunately, no clinical pathology data were compared in one
previous postoperative NLR change prognostic study (13). As the mechanisms causing a high NLR
prior to and following surgery are not consistent, the relative
changes (postoperative NLR change and postoperative NLR minus
preoperative NLR) in the postoperative NLR may not reflect the true
immune status following surgery. This may be the reason why there
was no significant difference in pathological parameters between
the postoperative NLR minus preoperative NLR groups (3,16).
In the present study, the postoperative NLR plus
preoperative NLR was first identified as an improved prognostic
factor for HCC following hepatectomy compared with the preoperative
NLR, postoperative NLR, postoperative NLR change, and postoperative
NLR minus preoperative NLR groups according to td-ROC curves. The
postoperative NLR plus preoperative NLR groups had the largest
td-AUC in the first to fourth years. This suggests that the
combination of the preoperative NLR and the postoperative NLR with
the postoperative NLR plus preoperative NLR is more effective than
the postoperative NLR change or the postoperative NLR minus
preoperative NLR in predicting the prognosis of patients with HCC.
The preoperative NLR plus postoperative NLR was also more useful
for predicting the prognosis of patients with HCC than either the
preoperative NLR or the postoperative NLR. Multivariate analysis
identified the preoperative NLR plus postoperative NLR as an
independent prognostic risk factor. Miyatani et al (15) also reported that a high preoperative
and a high postoperative NLR were independent prognostic indicators
for gastric cancer. In the present study, patients in the
preoperative NLR plus postoperative NLR=2 group had larger tumor
sizes than those in the preoperative NLR plus postoperative NLR=1/0
group. An increased preoperative NLR plus postoperative NLR score
was associated with multiple tumors and poor differentiation.
Several studies have indicated that multiple tumor numbers, larger
tumor sizes and poor differentiation are predictors of a poor
outcome (39–41). Similarly, the results of the present
study suggested that an increased preoperative NLR plus
postoperative NLR was associated with preoperative and
postoperative inflammatory indicators. Taken together, the results
of the present study suggested that the preoperative NLR plus
postoperative NLR more comprehensively reflects the preoperative
and postoperative tumor burden and inflammatory or immune status
than the other parameters; therefore, the preoperative NLR plus
postoperative NLR may be a more reliable prognostic factor. The
preoperative NLR plus postoperative NLR considers the two
preoperative and postoperative treatment phases, and thus, the
combined indicators may more accurately predict the prognosis,
compared with individual indicators. Lalani et al (13) found that a postoperative NLR decrease
≥25% from baseline to 6 weeks was associated with an improved OS,
but only a postoperative NLR increase by ≥25% was an independent
prognostic factor for OS following PD-1/PD-L1 immune checkpoint
blockade therapy. We hypothesized that the postoperative NLR may be
somewhat associated with the immunotherapy response.
The present study has certain limitations. To begin
with, the present study is a retrospective and single-center study
with possible unmeasurable selection biases. Furthermore, the small
sample size of this study may limit the assessment of the
prognostic value of different influencing factors. Additionally,
heterogeneity of the patient's liver disease background, including
patients with HBV or HCV-related HCC, may affect the NLR cut-off.
Finally, the preoperative NLR and postoperative NLR require further
investigation in immunotherapy studies, and it is necessary to
identify which neutrophil and lymphocyte subsets have prognostic
utility.
Compared with conventional prognostic factors,
including preoperative NLR, postoperative NLR, preoperative NLR
plus postoperative NLR, change in postoperative NLR, and
postoperative NLR minus preoperative NLR, the preoperative NLR plus
postoperative NLR, considering both the preoperative and
postoperative treatment phase, may be a more effective prognostic
factor for patients with HCC and requires further investigation in
the future.
Acknowledgements
The authors would like to thank Dr Zhaoyang Liu
(Statistical Consultant Center, Tsinghua University) for providing
statistical assistance.
Funding
The present study was supported by the National
Science & Technology Major Project (grant no. 2017ZX10203205),
National Natural Science Foundation of China (grant no. 81930119),
and the Medical-Engineering Project of Tsinghua University School
of Software (grant no. MESR201912-3).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
MW and SY are responsible for the study concept and
design, methodology, software, data collection and analyses,
writing the initial draft of the manuscript and critically revising
the manuscript. XF is responsible for the data analysis,
methodology and critically revising the manuscript. FY and XL are
responsible for the data collection. JD is responsible for the
study concept and design, methodology, critical revision of the
manuscript, and project administration and supervision. All authors
read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of Beijing Tsinghua Chang Gung Hospital (Beijing,
China).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Yang JD and Roberts LR: Hepatocellular
carcinoma: A global view. Nat Rev Gastroenterol Hepatol. 7:448–458.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Oh BS, Jang JW, Kwon JH, You CR, Chung KW,
Kay CS, Jung HS and Lee S: Prognostic value of C-reactive protein
and neutrophil-to-lymphocyte ratio in patients with hepatocellular
carcinoma. BMC Cancer. 13:782013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Dan J, Zhang Y, Peng Z, Huang J, Gao H, Xu
L and Chen M: Postoperative neutrophil-to-lymphocyte ratio change
predicts survival of patients with small hepatocellular carcinoma
undergoing radiofrequency ablation. PLoS One. 8:e581842013.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lopes M, Carvalho B, Vaz R and Linhares P:
Influence of neutrophil-lymphocyte ratio in prognosis of
glioblastoma multiforme. J Neurooncol. 136:173–180. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Luo G, Liu C, Cheng H, Jin K, Guo M, Lu Y,
Long J, Xu J, Ni Q, Chen J and Yu X: Neutrophil-lymphocyte ratio
predicts survival in pancreatic neuroendocrine tumors. Oncol Lett.
13:2454–2458. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Jin H, Sun J, Zhu K, Liu X, Zhang Q, Shen
Q, Gao Y and Yu J: The prognostic value of neutrophil-lymphocyte
ratio is superior to derived neutrophil-lymphocyte ratio in
advanced gastric cancer treated with preoperative chemotherapy and
sequential R0 resection: A 5-year follow-up. Onco Targets Ther.
10:2655–2664. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Komura N, Mabuchi S, Yokoi E, Kozasa K,
Kuroda H, Sasano T, Matsumoto Y and Kimura T: Comparison of
clinical utility between neutrophil count and neutrophil-lymphocyte
ratio in patients with ovarian cancer: A single institutional
experience and a literature review. Int J Clin Oncol. 23:104–113.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sun Z, Ju Y, Han F, Sun X and Wang F:
Clinical implications of pretreatment inflammatory biomarkers as
independent prognostic indicators in prostate cancer. J Clin Lab
Anal. 32:e222772018. View Article : Google Scholar
|
|
9
|
Ethier JL, Desautels D, Templeton A, Shah
PS and Amir E: Prognostic role of neutrophil-to-lymphocyte ratio in
breast cancer: A systematic review and meta-analysis. Breast Cancer
Res. 19:22017. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Grivennikov SI, Greten FR and Karin M:
Immunity, inflammation, and cancer. Cell. 140:883–899. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lee SK, Choi MY, Bae SY, Lee JH, Lee HC,
Kil WH, Lee JE, Kim SW and Nam SJ: Immediate postoperative
inflammation is an important prognostic factor in breast cancer.
Oncology. 88:337–344. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Shibutani M, Maeda K, Nagahara H, Ohtani
H, Iseki Y, Ikeya T, Sugano K and Hirakawa K: The prognostic
significance of a postoperative systemic inflammatory response in
patients with colorectal cancer. World J Surg Oncol. 13:1942015.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lalani AA, Xie W, Martini DJ, Steinharter
JA, Norton CK, Krajewski KM, Duquette A, Bossé D, Bellmunt J, Van
Allen EM, et al: Change in Neutrophil-to-lymphocyte ratio (NLR) in
response to immune checkpoint blockade for metastatic renal cell
carcinoma. J Immunother Cancer. 6:52018. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Li M, Spakowicz D, Burkart J, Patel S,
Husain M, He K, Bertino EM, Shields PG, Carbone DP, Verschraegen
CF, et al: Change in neutrophil to lymphocyte ratio during
immunotherapy treatment is a non-linear predictor of patient
outcomes in advanced cancers. J Cancer Res Clin Oncol.
145:2541–2546. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Miyatani K, Saito H, Kono Y, Murakami Y,
Kuroda H, Matsunaga T, Fukumoto Y, Osaki T, Ashida K and Fujiwara
Y: Combined analysis of the pre- and postoperative
neutrophil-lymphocyte ratio predicts the outcomes of patients with
gastric cancer. Surg Today. 48:300–307. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Peng W, Li C, Wen TF, Yan LN, Li B, Wang
WT, Yang JY and Xu MQ: Neutrophil to lymphocyte ratio changes
predict small hepatocellular carcinoma survival. J Surg Res.
192:402–408. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Guo D, Han A, Jing W, Chen D, Jin F, Li M,
Kong L and Yu J: Preoperative to postoperative change in
neutrophil-to-lymphocyte ratio predict survival in colorectal
cancer patients. Future Oncol. 14:1187–1196. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Jin F, Han A, Shi F, Kong L and Yu J: The
postoperative neutrophil-to-lymphocyte ratio and changes in this
ratio predict survival after the complete resection of stage I
non-small cell lung cancer. OncoTargets Ther. 9:6529–6537. 2016.
View Article : Google Scholar
|
|
19
|
Min KW, Kwon MJ, Kim DH, Son BK, Kim EK,
Oh YH and Wi YC: Persistent elevation of postoperative
neutrophil-to-lymphocyte ratio: A better predictor of survival in
gastric cancer than elevated preoperative neutrophil-to-lymphocyte
ratio. Sci Rep. 7:139672017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Zhou ZQ, Pang S, Yu XC, Xue Q, Jiang HY,
Liang XJ and Liu L: Predictive values of postoperative and dynamic
changes of inflammation indexes in survival of patients with
resected colorectal cancer. Curr Med Sci. 38:798–808. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Nishihara K, Suekane S, Ueda K, Nakiri M,
Matsuo M and Igawa T: High postoperative neutrophil-to-lymphocyte
ratio as a poorprognostic marker in patients with upper tract
urothelial carcinoma. Oncol Lett. 17:5241–5250. 2019.PubMed/NCBI
|
|
22
|
El-Serag HB and Rudolph KL: Hepatocellular
carcinoma: Epidemiology and molecular carcinogenesis.
Gastroenterology. 132:2557–2576. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Martins-Filho SN, Paiva C, Azevedo RS and
Alves VAF: Histological grading of hepatocellular carcinoma-a
systematic review of literature. Front Med (Lausanne). 4:1932017.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Huang SS, Xie DM, Cai YJ, Wu JM, Chen RC,
Wang XD, Song M, Zheng MH, Wang YQ, Lin Z and Shi KQ: C-reactive
protein-to-albumin ratio is a predictor of hepatitis B virus
related decompensated cirrhosis: Time-dependent receiver operating
characteristics and decision curve analysis. Eur J Gastroenterol
Hepatol. 29:472–480. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kamarudin AN, Cox T and Kolamunnage-Dona
R: Time- dependent ROC curve analysis in medical research: Current
methods and applications. BMC Med Res Methodol. 17:532017.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Hothorn T and Zeileis A: Generalized
maximally selected statistics. Biometrics. 64:1263–1269. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Martin D, Rodel F, Balermpas P, Winkelmann
R, Fokas E and Rodel C: C-reactive protein-to-albumin ratio as
prognostic marker for anal squamous cell carcinoma treated with
chemoradiotherapy. Front Oncol. 9:12002019. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Zhou SL, Zhou ZJ, Hu ZQ, Huang XW, Wang Z,
Chen EB, Fan J, Cao Y, Dai Z and Zhou J: Tumor-associated
neutrophils recruit macrophages and T-regulatory cells to promote
progression of hepatocellular carcinoma and resistance to
sorafenib. Gastroenterology. 150:1646–1658 e1617. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Nakagawa S, Umezaki N, Yamao T, Kaida T,
Okabe H, Mima K, Imai K, Hashimoto D, Yamashita YI, Ishiko T, et
al: Survival impact of lymphocyte infiltration into the tumor of
hepatocellular carcinoma in hepatitis B virus-positive or non-B
non-C patients who underwent curative resection. Hepatol Res.
48:E126–E132. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Morizawa Y, Miyake M, Shimada K, Hori S,
Tatsumi Y, Nakai Y, Onishi S, Tanaka N, Konishi N and Fujimoto K:
Correlation of immune cells and cytokines in the tumor
microenvironment with elevated neutrophil-to-lymphocyte ratio in
blood: An analysis of muscle-invasive bladder cancer. Cancer
Invest. 36:395–405. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Bergmann J, Muller M, Baumann N, Reichert
M, Heneweer C, Bolik J, Lücke K, Gruber S, Carambia A, Boretius S,
et al: IL-6 trans-signaling is essential for the development of
hepatocellular carcinoma in mice. Hepatology. 65:89–103. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Cools-Lartigue J, Spicer J, McDonald B,
Gowing S, Chow S, Giannias B, Bourdeau F, Kubes P and Ferri L:
Neutrophil extracellular traps sequester circulating tumor cells
and promote metastasis. J Clin Invest. 123:3446–3458. 2013.
View Article : Google Scholar
|
|
33
|
Li C, Wen TF, Yan LN, Li B, Wang WT, Yang
JY and Xu MQ: Postoperative neutrophil-to-lymphocyte ratio plus
platelet-to-lymphocyte ratio predicts the outcomes of
hepatocellular carcinoma. J Surg Res. 198:73–79. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Cook NR: Use and misuse of the receiver
operating characteristic curve in risk prediction. Circulation.
115:928–935. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Medina Fernandez FJ, Munoz-Casares FC,
Arjona-Sanchez A, Casado-Adam A, Gómez-Luque I, Garcilazo Arismendi
DJ, Thoelecke H, Rufián Peña S and Briceño Delgado J: Postoperative
time course and utility of inflammatory markers in patients with
ovarian peritoneal carcinomatosis treated with neoadjuvant
chemotherapy, cytoreductive surgery, and HIPEC. Ann Surg Oncol.
22:1332–1340. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Mei Z, Shi L, Wang B, Yang J, Xiao Z, Du
P, Wang Q and Yang W: Prognostic role of pretreatment blood
neutrophil-to-lymphocyte ratio in advanced cancer survivors: A
systematic review and meta-analysis of 66 cohort studies. Cancer
Treat Rev. 58:1–13. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Templeton AJ, McNamara MG, Seruga B,
Vera-Badillo FE, Aneja P, Ocaña A, Leibowitz-Amit R, Sonpavde G,
Knox JJ, Tran B, et al: Prognostic role of neutrophil-to-lymphocyte
ratio in solid tumors: A systematic review and meta-analysis. J
Natl Cancer Inst. 106:dju1242014. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Zhou WW, Chu YP and An GY: Significant
difference of neutrophil-lymphocyte ratio between colorectal
cancer, adenomatous polyp and healthy people. Eur Rev Med Pharmacol
Sci. 21:5386–5391. 2017.PubMed/NCBI
|
|
39
|
Hwang S, Lee YJ, Kim KH, Ahn CS, Moon DB,
Ha TY, Song GW, Jung DH and Lee SG: The impact of tumor size on
long-term survival outcomes after resection of solitary
hepatocellular carcinoma: Single-institution experience with 2558
patients. J Gastrointest Surg. 19:1281–1290. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Wang X, Wang Z and Wu L: Combined
measurements of tumor number and size helps estimate the outcome of
resection of Barcelona clinic liver cancer stage B hepatocellular
carcinoma. BMC Surg. 16:222016. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Zhang TT, Zhao XQ, Liu Z, Mao ZY and Bai
L: Factors affecting the recurrence and survival of hepatocellular
carcinoma after hepatectomy: A retrospective study of 601 Chinese
patients. Clin Transl Oncol. 18:831–840. 2016. View Article : Google Scholar : PubMed/NCBI
|