Introduction
Data from the recent GLOBOCAN report suggests that
cervical cancer is the fourth most common malignancy in females
worldwide and the second most common cancer type in low- and
middle-income countries (1).
Globally, a total of 569,847 new cases of cervical cancer were
reported in 2018 and an estimated 311,365 deaths (1). According to a recent systematic review
on cervical cancer, it is one of the leading causes of death
amongst females in developing countries (2).
According to the International Federation of
Gynecology and Obstetrics classification, stage IB2, IIA2, IIB,
IIIA, IIIB and IVA cervical cancer is defined as locally advanced
cervical cancer (LACC) (3). The
treatment of choice for patients with such a disease is definitive
concurrent chemoradiotherapy (CCRT), consisting of external beam
radiotherapy with concomitant platinum-based chemotherapy and with
or without further interstitial brachytherapy (4,5). Despite
the better survival it achieves compared to radiotherapy alone, the
5-year survival for patients remains ~70% (6). Completion or so-called ‘adjuvant’
hysterectomy has been used after CCRT in certain patients to
improve survival (7). However, no
consensus over the benefit of such adjuvant surgery in LACC has
been reached in the literature (8).
Advocates of additional surgery argue that early hysterectomy leads
to better disease control and avoidance of more extensive surgery,
such as pelvic exenteration, in the event of a future recurrence
(7,9). On the other hand, adjuvant hysterectomy
is not morbidity-free and the rate of grade-3 adverse events may be
as high as 26.5% (8).
So far, two meta-analyses have performed data
syntheses in an attempt to provide evidence on the benefit of
hysterectomy with CCRT for LACC. Shim et al (8) performed a meta-analysis of studies
published until April 2016 and compiled survival and recurrence
data from eight studies comparing CCRT with hysterectomy vs. CCRT
alone. However, they only pooled the odds ratio (OR) data in their
analysis. Shi et al (10)
provided another meta-analysis of studies published until August
2017, pooling eight studies that used both radiotherapy alone and
CCRT with or without hysterectomy. Their study only analyzed
survival data to obtain hazard ratios (HRs) without comparing
recurrence rates. The publication of new studies since then
(11,12) warrants a more comprehensive and
updated analysis to guide clinicians treating LACC. Therefore, the
purpose of the present study was to systematically search the
literature and conduct a comprehensive meta-analysis with
meta-regression to compare survival and recurrence between patients
undergoing CCRT with hysterectomy and those undergoing CCRT
alone.
Materials and methods
Inclusion criteria
The Preferred Reporting Items for Systematic Reviews
and Meta-analyses (PRISMA) (13)
guidelines were followed during the preparation of this review. The
protocol of the study was, however, not registered. All types of
peer-reviewed studies conducted on patients with LACC i.e., stages
IB2 to IVA, were included. The included studies compared groups of
patients undergoing CCRT with hysterectomy with those undergoing
CCRT alone and reported on overall survival (OS) and/or
disease-free survival (DFS) as outcome variables. Both groups of
patients included patients who underwent brachytherapy, who had
radical/simple hysterectomy and/or who had different histological
types of LACC. Studies including other cancer stages such as IB1 or
IVB were only considered if the overall percentage of patients with
these stages was <10% of the study sample. The criteria for
exclusion were as follows: i) Non-comparative single-arm studies;
ii) studies using only chemotherapy or radiotherapy and not
combined CCRT; iii) case series, case reports, letters to editors
and abstracts; iv) non-English language studies and articles with
unavailable full-text versions. In cases of studies with
overlapping data, only the study reporting the largest dataset was
included.
Search strategy
An electronic search of the PubMed, Scopus, Embase
and Google scholar databases was performed. The last search was
performed on the 20th of February, 2020. A total of two independent
reviewers (CL, ZY) performed the database search using the
following keywords in various combinations: ‘Cervical cancer’,
‘locally advanced cervical cancer’, ‘chemoradiotherapy’,
‘chemotherapy’, ‘radiotherapy’, ‘surgery’, ‘hysterectomy’ and
‘brachytherapy’. The exact search terms and the number of results
obtained are presented in Table SI.
After the selection of studies, the bibliography of all included
studies was manually checked to identify any studies missed during
the digital search. First, two different reviewers (CL, ZY)
screened the titles and abstracts of search records. After
screening of abstracts, the full texts of relevant articles were
extracted and assessed in detail based on the inclusion criteria.
Any disagreements during the study selection process were resolved
by discussion with the third reviewer (LG).
Data extraction and quality of
included studies
A data abstraction form was used to extract the
following details: Author name, publication year, study type,
sample size, demographic data, LACC stage, histological type, lymph
node metastasis, CCRT protocol, brachytherapy details, chemotherapy
regimen, hysterectomy type and timing, follow-up and study
outcomes. The primary outcomes of interest were the differences in
OS and DFS between patients with LACC undergoing CCRT with
hysterectomy and those undergoing CCRT alone using HRs. The
secondary outcomes of interest were differences in mortality and
recurrence (both local and distant) between the two groups by
comparing ORs.
The Cochrane Collaboration Risk Assessment Tool was
used to assess the risk of bias in randomized controlled trials
(RCTs) (14). For non-RCTs, the risk
of a bias assessment tool for non-randomized studies was used
(15). For each domain, studies were
graded as having low, high or unclear risk of bias.
Statistical analysis
The software Review Manager [version 5.3; Nordic
Cochrane Centre (Cochrane Collaboration)] was used for the
meta-analysis. HR values for OS and DFS, as well as data on the
absolute number of deaths and recurrences, were extracted from the
studies included. In cases in which HR values were unavailable,
they were extrapolated from Kaplan-Meier survival curves using the
Microsoft Excel sheet developed by Matthew Sydes and Jayne Tierney
(16). The study estimates were then
combined using inverse variance-weighted averages of logarithmic
HRs in a random-effects model. Categorical data of mortality and
any recurrences were summarized using the Mantel-Haenszel OR with
95% confidence intervals (CI) in a random-effects model.
Heterogeneity was calculated using the I2 statistic.
Based on I2 values, heterogeneity was classified as low
(25-50%) medium (50-75%) or substantial (>75%). Subgroup
analyses by study type and use of brachytherapy in the CCRT with
hysterectomy group were performed using a random effects model. A
sensitivity analysis was conducted to assess the influence of each
study on the overall estimate by excluding one study at a time.
Publication bias was assessed based on visual inspection of funnel
plots only if >10 studies had been included in the analysis. In
addition, a meta-regression analysis was performed using a
random-effects model with Open MetaAnalyst software (17). The influence on the pooled effect
size of the proportion of patients with stage IB2, stage II, stage
III and squamous cell carcinoma (SCC), as well as the proportion of
patients undergoing radical hysterectomy, were analyzed using a
univariate meta-regression analysis. Meta-regression coefficients
(Beta) with 95% CIs were calculated. Since logHR/logOR>0
corresponds to HR/OR>1 and log HR/OR<0 corresponds to
HR/OR<1, a negative meta-regression coefficient indicates that
HR/OR decreases as a given factor increases, and a positive
coefficient indicates that HR/OR increases as a given factor
increases.
Results
Study selection
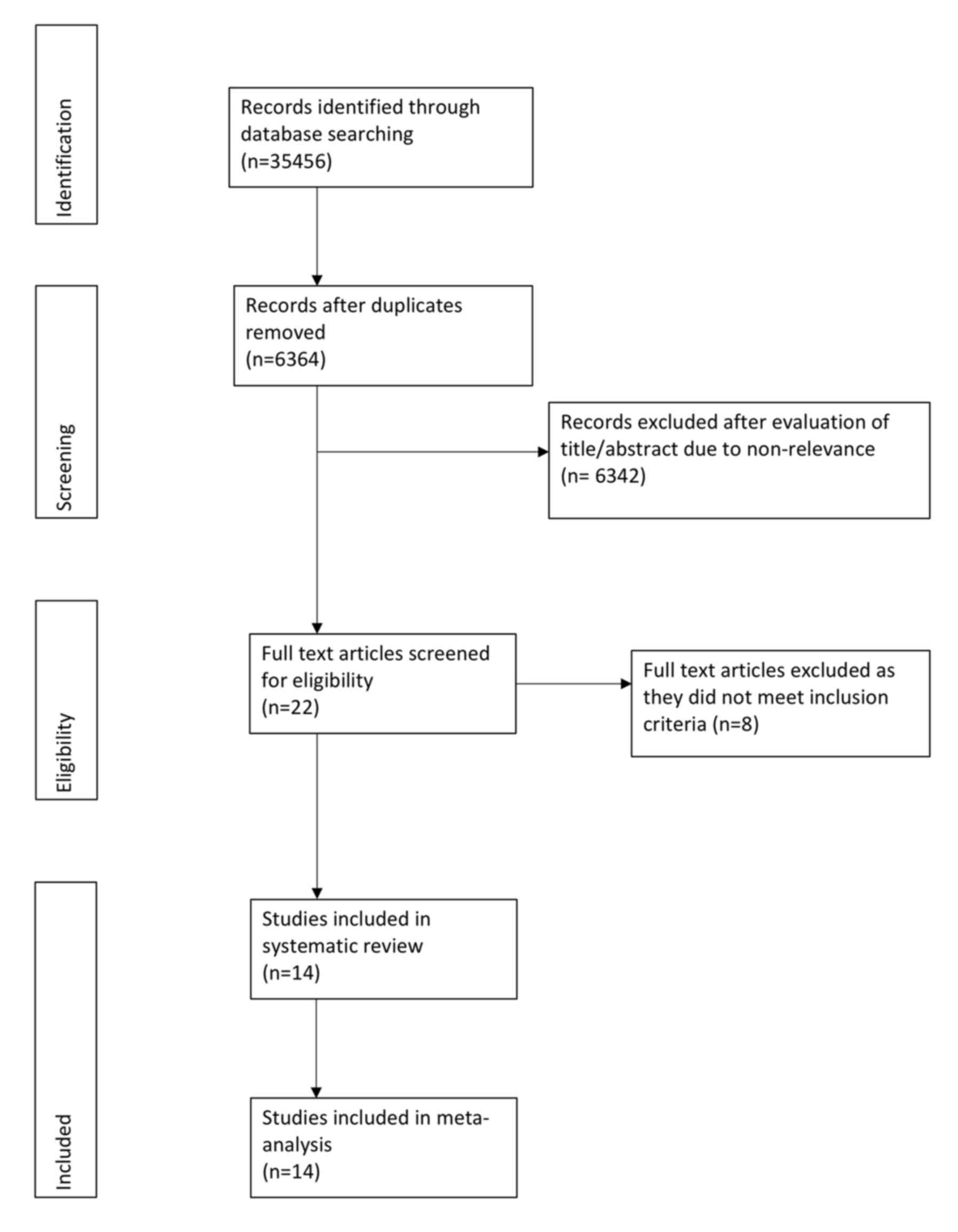
Fig. 1 presents the
PRISMA flow chart of the search and selection process. Of the
eligible records identified, 22 were subjected to full-text review,
eight of which (7,9,18–23) were
excluded for the following reasons: A total of two studies used
only radiotherapy (22,23), two were non-comparative studies
(7,19), one study included a large cohort of
patients with stage I cancer (21),
one study evaluated patients with stage IVB cervical cancer
(18), one study had duplicate data
(9) and the full-text of one study
was unavailable (20). Finally, data
from 14 studies were included in this systematic review and
meta-analysis (11,12,24–35).
Table I presents
details of the included studies. Except for 2 RCTs (31,32), all
were retrospective cohort studies. From these 14 studies, the data
of 1,224 patients undergoing CCRT and hysterectomy were compared
with those of 2,635 patients undergoing CCRT alone. The sample size
of the CCRT with hysterectomy groups ranged from 24 to 192
patients, while the sample size of the CCRT groups ranged from 30
to 1,407 patients. The median age of the patients was ≥45 years in
all studies. None of the studies reported any statistically
significant differences in the distribution of cancer stages
between the two groups. None of the studies reported any
statistically significant differences in tumor histology between
the two groups, except for one study (12). In addition, one study reported a
significant difference in lymph node metastasis between the two
groups at baseline (28).
Furthermore, four studies (25,27,29,31) did
not use brachytherapy in the CCRT with hysterectomy group and used
the procedure only in the CCRT group. The chemotherapy regimens
included mostly cisplatin (40 mg/m2 weekly) with certain
variations across studies. Of note, two studies (29,33)
carried out hysterectomies only in good responders, defined as
patients with a decrease in tumor volume of at least 50% according
to MRI on CCRT completion, while one RCT (32) conducted hysterectomies only in
complete responders (patients without residual disease). Most
studies did not report data on the percentage of patients with
residual disease after CCRT. Both simple and radical hysterectomies
were used across studies at varying proportions.
 | Table I.Characteristics of included
studies. |
Table I.
Characteristics of included
studies.
|
|
| Sample size
(n) | Median age
(years) | Stage (n) | Histology (n) | Lymph node
metastasis (n) |
|
|
|
|
|
| Residual disease
after CCRTa (percentage
of patients) |
|
|
|
|---|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|---|
| Author (year) | Study type | CCRT+AH | CCRT | CCRT+AH | CCRT | CCRT+AH | CCRT | CCRT+AH | CCRT | CCRT+AH | CCRT | Median dose of EBRT
(Gy) | Median dose of ICBT
(Gy) | Median duration of
CCRT (days) | ICBT for AH
group | Chemotherapy
regimen | Median time from
CCRT to AH (wk) | CCRT+AH | CCRT | AH type (n) | Median follow-up
(months) | (Refs.) |
|---|
| Darus | R | 24 | 30 | 41b | 41b | IB2: 24 | IB2: 30 | SCC: 16 | SCC: 23 | NR | NR | 47 | 45 | <56 | Yes | DDP weekly, |
|
|
|
|
|
|
| (2008) |
|
|
|
|
|
|
| Non-SCC: 8 | Non-SCC: 7 |
|
|
|
|
|
| 40
mg/m2 | 6 | NR | NR | SH: 24 | 47 | (35) |
| Cetina | R | 40 | 40 | 45 | 45 | IB2: 9 | IB2: 9 | SCC: 28 | SCC: 28 | NR | NR | 50 | 35 | 40 | Yes | DDP weekly, | <7 | NR | NR | RH: 40 | 22-26 | (34) |
| (2009) |
|
|
|
|
| IIA: 4 | IIA: 4 | Non-SCC: 12 | Non-SCC: 12 |
|
|
|
|
|
| 40
mg/m2 |
|
|
|
|
|
|
|
|
|
|
|
|
| IIB: 27 | IIB: 27 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Lèguevaque | R | 67 | 44 | 51b |
| IB2: 22 |
| SCC: 95 |
| 18 | 21 | 45 | 35 | NR | Yes | DDP weekly, | 5-7 | 28.3c | 56.8 | RH/SH: 67 | NR | (33) |
| (2011) |
|
|
|
|
| II: 71 |
| Non-SCC: 16 |
|
|
|
|
|
|
| 40
mg/m2 |
|
|
|
|
|
|
|
|
|
|
|
|
| III: 12 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| IVA: 3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Morice | RCT | 31 | 30 | 45 | 45 | IB2: 16 | IB2: 15 | SCC: 28 | SCC: 24 | 9 | 9 | 44-50 | 15 | 51 | Yes | DDP weekly, | 6-8 | 0 | 0 | RH/SH: 31 | 46 | (32) |
| (2012) |
|
|
|
|
| II: 15 | II: 15 | Non-SCC: 3 | Non-SCC: 6 |
|
|
|
|
|
| 40
mg/m2 |
|
|
|
|
|
|
| Cetina | RCT | 111 | 100 | 45 | 44 | IB2: 18 | IB2: 18 | SCC: 100 | SCC: 83 | NR | NR | 50.4 | 30-35 | 47 | No | DDP weekly, | 4-6 | NR | NR | RH: 86 | 36b | (31) |
| (2013) |
|
|
|
|
| IIA: 11 | IIA: 12 | Non-SCC: 11 | Non-SCC: 17 |
|
|
|
|
|
| 40 mg/m2
+ |
|
|
|
|
|
|
|
|
|
|
|
|
| IIB: 82 | IIB: 70 |
|
|
|
|
|
|
|
| gemcitabine, 125
mg/m2 |
|
|
|
|
|
|
| Wang | R | 119 | 121 | 45 | 52 | IIB: 119 | IIB: 121 | SCC: 112 | SCC: 116 | 13 | 14 | 40-50 | 28-35 | 60 | No | DDP weekly, | 2-3 | NR | NR | RH: 119 | 30-36 | (29) |
| (2014) |
|
|
|
|
|
|
| Non-SCC: 7 | Non-SCC: 5 |
|
|
|
|
|
| 40
mg/m2 |
|
|
|
|
|
|
| Chereau | R | 46 | 34 | 49b | 51b | IB2: 15 | IB2: 4 | SCC: 39 | SCC: 29 | 9c | 27 | 40-55 | 20 | NR | Yes | DDP 20–25
mg/m2 | 6 | NR | NR | SH: 31 | 31 | (28) |
| (2013) |
|
|
|
|
| IIA: 4 | IIA: 5 | Non-SCC: 7 | Non-SCC: 5 |
|
|
|
|
|
| days 1, 2, 4, 5
with |
|
|
| RH: 14 |
|
|
|
|
|
|
|
|
| IIB: 27 | IIB: 25 |
|
|
|
|
|
|
|
| triweekly 5-FU 750
mg/m2 |
|
|
|
|
|
|
| Sun (2014) | R | 192 | 186 | 48 | 48 | IIB: 90 | IIB: 84 | SCC: 149 | SCC: 140 | 18 | NR | 45-50 | 45-55 | NR | Yes | DDP weekly, | 10-12 | NR | NR | SH: 99 | 190b | (30) |
|
|
|
|
|
|
| III: 101 | III: 100 | Non-SCC: 43 | Non-SCC: 47 |
|
|
|
|
|
| 40 mg/m2
with |
|
|
| RH: 72 |
|
|
|
|
|
|
|
|
| IVA: 1 | IVA: 2 |
|
|
|
|
|
|
|
| 5-FU 500
mg/m2 |
|
|
|
|
|
|
| Fanfani | R | 73 | 77 | 52 | 56 | IIIA: 14 | IIIA: 19 | SCC: 68 | SCC: 68 | 26 | 32 | 45-50 | 30 | NR | No | DDP weekly, | 4-6 | 58.9 | 61.1 | RH: 73 | 39-41 | (27) |
| (2016) |
|
|
|
|
| IIIB: 59 | IIIB: 58 | Non-SCC: 5 | Non-SCC: 9 |
|
|
|
|
|
| 40
mg/m2 |
|
|
|
|
|
|
| Mazeron | R | 54 | 157 | 48.5b | 46.9b | IB1: 3 | IB1: 5 | SCC: 48 | SCC: 128 | 16 | 48 | 45-50 | 15 | NR | Yes | DDP weekly, | 8-12 | NR | NR | SH: 17 | 42-67 | (26) |
| (2016) |
|
|
|
|
| IB2: 18 | IB2: 50 | Non-SCC: 6 | Non-SCC: 29 |
|
|
|
|
|
| 40
mg/m2 |
|
|
| RH: 37 |
|
|
|
|
|
|
|
|
| IIA: 5 | IIA: 13 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| IIB: 28 | IIB: 89 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Hass (2017) | R | 87 | 161 | 50 | 63 | IB1: 4 | IIB: 3 | SCC: 77 | SCC: 136 | 32 | 37 | 50.4 | 28 | NR | No | DDP 20
mg/m2 | <6 | 54 | 52.2 | SH: 54 | 53 | (25) |
|
|
|
|
|
|
| IIA: 3 | IIIA: 25 | Non-SCC: 8 | Non-SCC: 19 |
|
|
|
|
|
| on days 1–5 in
the |
|
|
| RH: 33 |
|
|
|
|
|
|
|
|
| IIB: 15 | IIIB: 133 |
|
|
|
|
|
|
|
| 1st and 5th
week |
|
|
|
|
|
|
|
|
|
|
|
|
| IIIA: 4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| IIIB: 56 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| IVA: 5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Zheng | R | 163 | 151 | 51 | 55 | IB2: 35 | IB2: 28 | SCC: 136 | SCC: 121 | 60 | 41 | 46-50 | 25-30 | 42 | Yes | DDP weekly, | <8 | 41.1 | 40.4 | RH: 163 | NR | (24) |
| (2018) |
|
|
|
|
| IIA: 71 | IIA: 73 | Non-SCC: 27 | Non-SCC: 30 |
|
|
|
|
|
| 40
mg/m2 |
|
|
|
|
|
|
|
|
|
|
|
|
| IIB: 57 | IIB: 60 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Albert | R | 139 | 1,407 | 47 | 50 | IB2: 108 | IB2: 932 | SCC:
81c | SCC: 1113 | 11 | 235 | 60-80 | NR | NR | NR | NR | NR | NR | NR | NR | 33.3 | (12) |
| (2019) |
|
|
|
|
| IIA: 31 | IIA: 475 | Non-SCC: 58 | Non-SCC: 294 |
|
|
|
|
|
|
|
|
|
|
|
|
|
| Yang | R | 78 | 97 | 48 | 54 | IB2: 16 | IB2: 12 | Non-SCC: 78 | Non-SCC: 97 | 35 | 44 | 40-58 | 30-48 | 48 | Yes | DDP weekly, | 13 | 29.5 | 25.8 | SH: 76 | 23-28 | (11) |
| (2020) |
|
|
|
|
| IIA: 5 | IIA: 8 |
|
|
|
|
|
|
|
| 40 mg/m2
or |
|
|
| RH: 2 |
|
|
|
|
|
|
|
|
| IIB: 51 | IIB: 62 |
|
|
|
|
|
|
|
| Paclitaxel
weekly, |
|
|
|
|
|
|
|
|
|
|
|
|
| III: 6 | III: 15 |
|
|
|
|
|
|
|
| 75
mg/m2 |
|
|
|
|
|
|
Meta-analysis
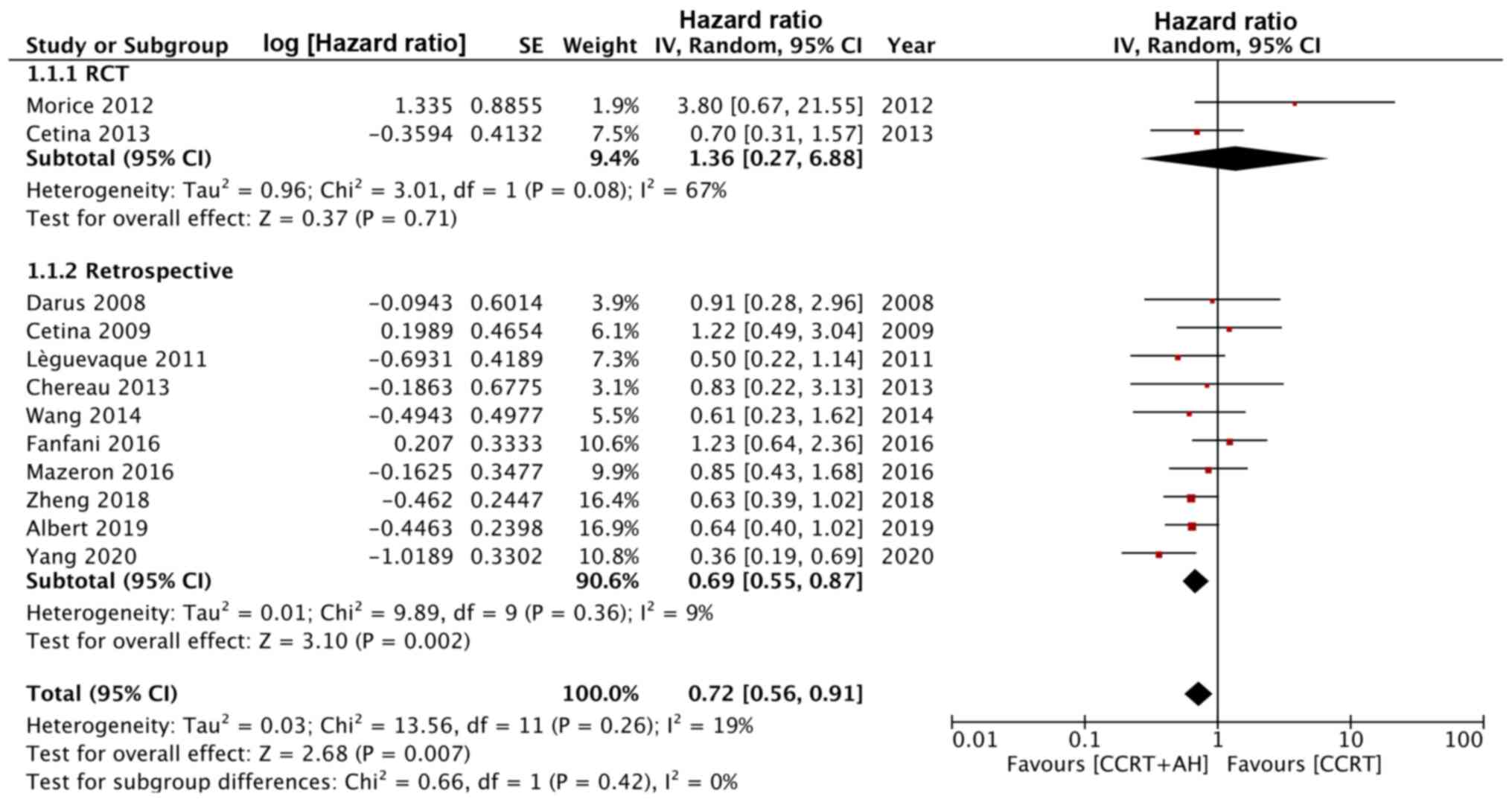
After pooling data from 12 studies, it was
determined that patients receiving CCRT with hysterectomy had
significantly better OS than those undergoing CCRT alone (HR, 0.72;
95% CI, 0.56 to 0.91; I2=19%; P=0.007; Fig. 2). The funnel plot did not indicate
any gross asymmetries (Fig. S1).
However, on subgroup analysis, the difference was significant only
for retrospective studies (HR, 0.69; 95% CI, 0.55-0.87;
I2=9%; P=0.002) but not for the two RCTs (HR, 1.36; 95%
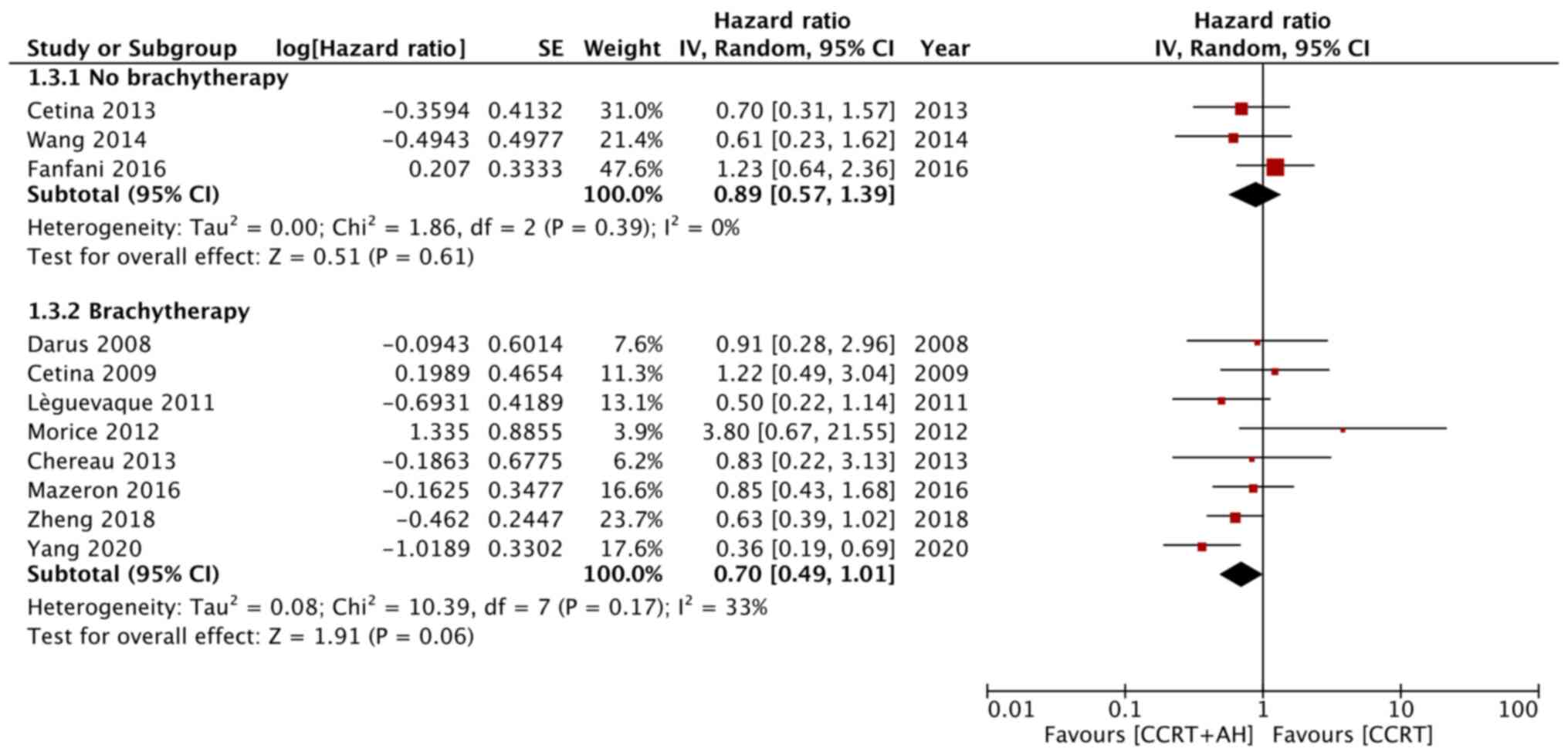
CI, 0.27-6.88; I2=67%; P=0.71; Fig. 2). Similarly, after dividing studies
based on the use of brachytherapy in the CCRT and hysterectomy
group, no statistically significant difference in OS was obtained
in any of the subgroups (without brachytherapy: HR, 0.89; 95% CI,
0.57-1.39; I2=0%; P=0.61; with brachytherapy: HR, 0.70;
95% CI, 0.49-1.01; I2=33%; P=0.06; Fig. 3).
A similar pattern was obtained after pooling data
from 10 studies in a meta-analysis for DFS. An overall significant
effect in favor of CCRT with hysterectomy was determined,
suggesting improved DFS with hysterectomy (HR, 0.72; 95% CI, 0.56
to 0.93; I2=27%; P=0.01; Fig.
4). However, on subgroup analysis, the significant effect was
restricted to retrospective studies only (HR, 0.68; 95% CI,
0.53-0.88, I2=12%; P=0.003) with no significant
differences in DFS in RCTs (HR, 1.10; 95% CI, 0.33-3.63;
I2=72%; P=0.88; Fig. 4).
No evidence of publication bias was observed in the funnel plot
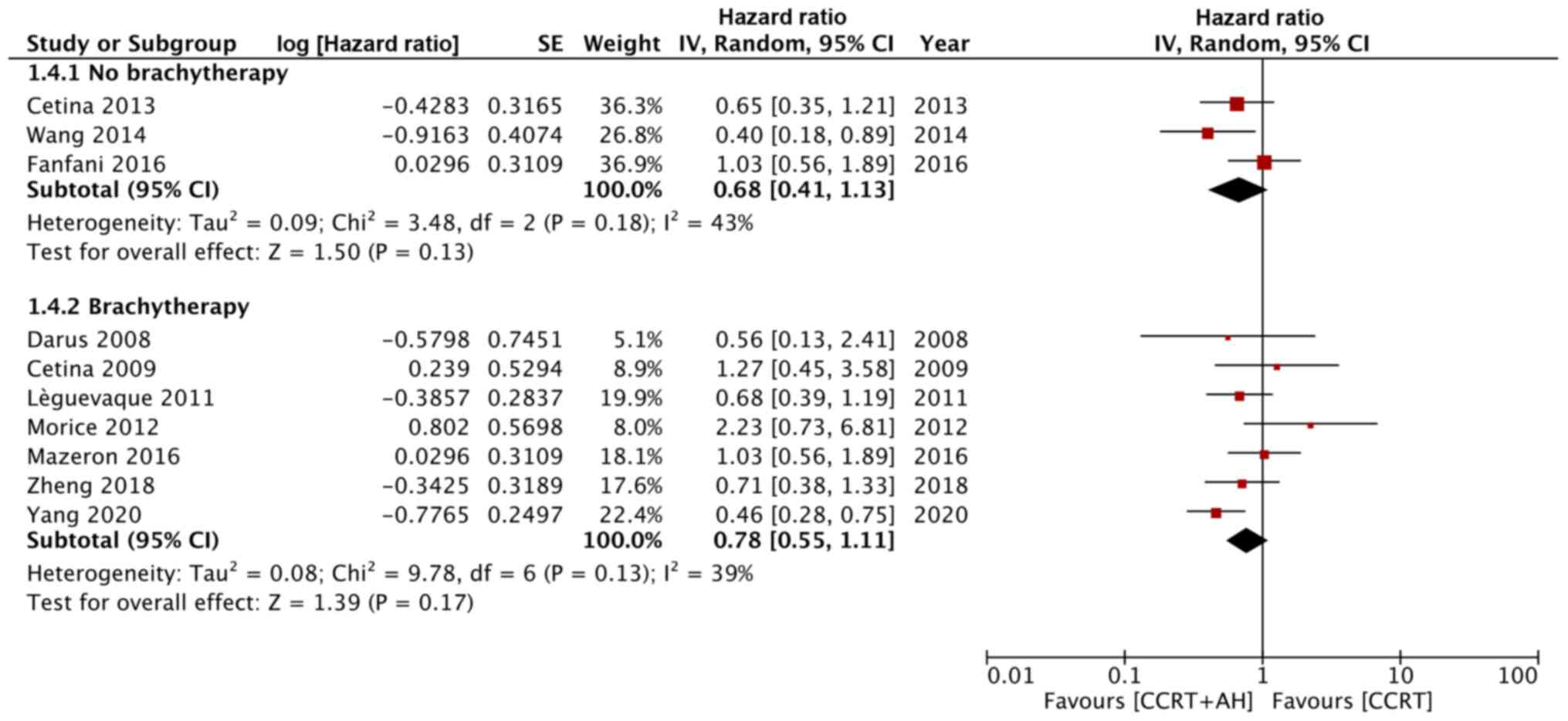
(Fig. S2). After further dividing
the studies based on the use of post-CCRT brachytherapy in the CCRT
with hysterectomy group, no differences in DFS were obtained
between the two groups with the use of brachytherapy (HR, 0.78; 95%
CI, 0.55-1.11; I2=39%; P=0.17) or without the use of
brachytherapy (HR, 0.68; 95% CI, 0.41-1.13; I2=43%;
P=0.13; Fig. 5).
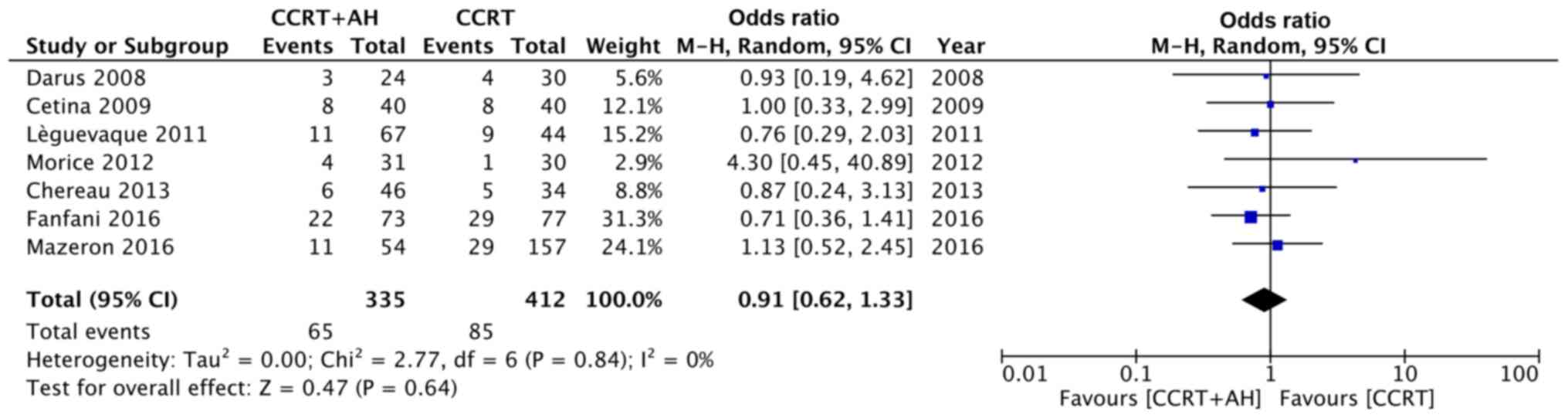
A total of seven studies reported data on the number
of deaths in their study population. The mortality was 19.4% in the
CCRT with hysterectomy group and 20.6% in the CCRT only group
without any statistically significant differences (OR, 0.91; 95%
CI, 0.62-1.33; I2=0%; P=0.64; Fig. 6). Data on recurrence were provided by
13 studies. Pooled analysis indicated a statistically significant
reduction in the incidence of recurrence in the CCRT with
hysterectomy group (17.14 vs. 26.96%; OR, 0.61; 95% CI, 0.47 to
0.79; I2=29%; P=0.0002; Fig.
7). Again, this result was significant only for retrospective
studies (OR, 0.56; 95% CI, 0.44-0.72; I2=19%;
P<0.0001) but not for RCTs (OR, 1.14; 95% CI, 0.40-3.26;
I2=49%; P=0.80; Fig. 7).
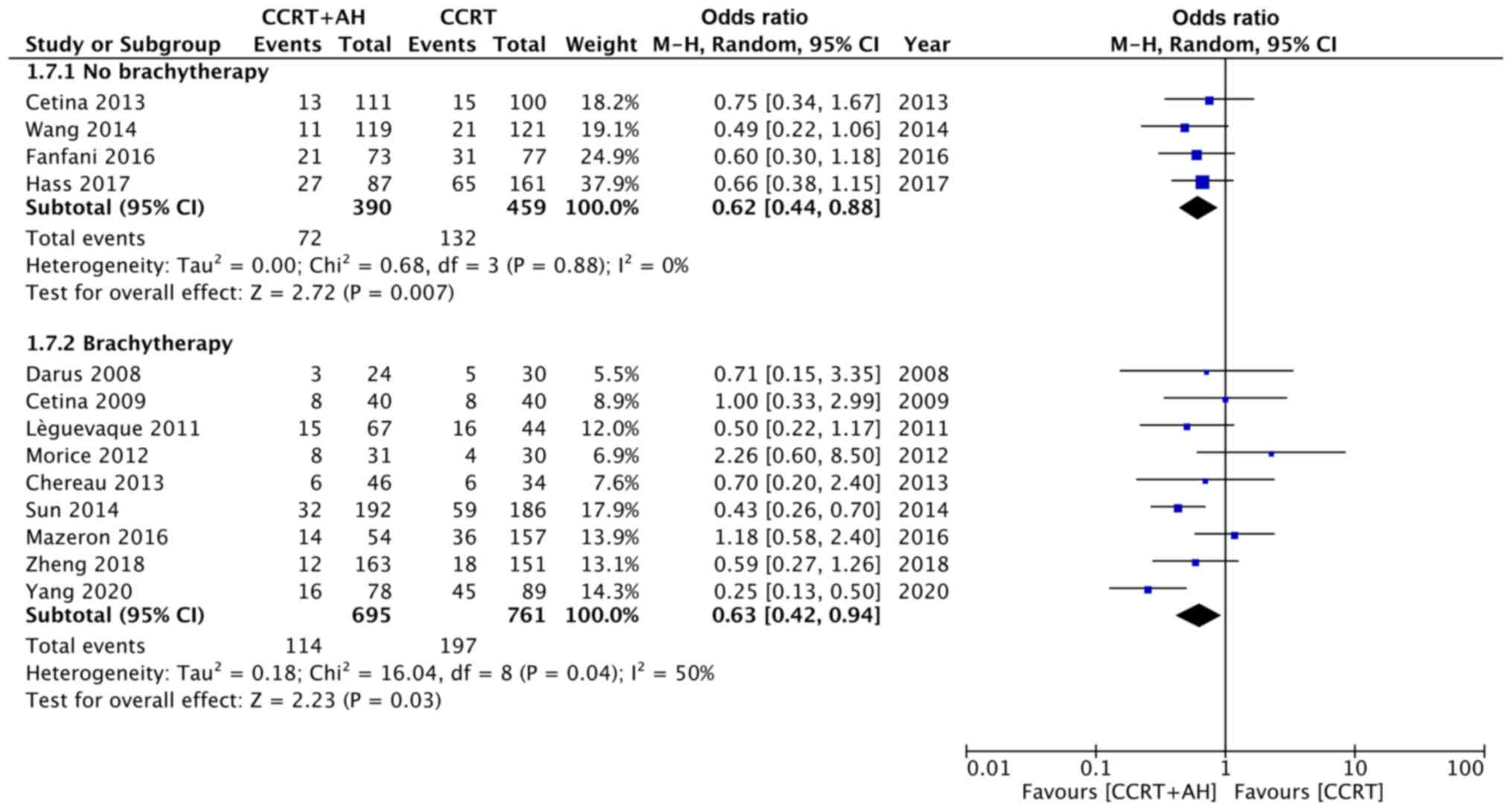
The funnel plot did not indicate any gross asymmetries (Fig. S3). On further subgroup analysis
based on the addition of brachytherapy in the CCRT with
hysterectomy group, recurrence rates were significantly lower in
the CCRT with hysterectomy group with brachytherapy (OR, 0.63; 95%
CI, 0.42-0.94; I2=50%; P=0.03) and in the CCRT with
hysterectomy group without brachytherapy (OR, 0.62; 95% CI,
0.44-0.88; I2=0%; P=0.007) than in the CCRT alone group
(Fig. 8).
Sensitivity and meta-regression
analysis
Both primary and secondary outcomes remained the
same after each one-at-a-time exclusion of singular studies. The
influence of the proportion of patients with stage IB2, stage II,
stage III, SCC and radical hysterectomy on the pooled effect size
was analyzed. The results are presented in Table II. The OS was significantly
influenced by the proportion of stage II patients. The log HR
decreased as the proportion of stage II patients increased,
indicating improved OS with CCRT and hysterectomy (Fig. 9).
| Table II.Meta-regression for proportion of
moderator on the pooled effect size. |
Table II.
Meta-regression for proportion of
moderator on the pooled effect size.
| A, Overall survival
(hazard ratio) |
|---|
|
|---|
| Moderator | β | Lower 95% CI | Upper 95% CI | SE | P-value |
|---|
| Stage IB2 | 0.000 | −0.008 | 0.009 | 0.004 | 0.974 |
| Stage II | −0.007 | −0.013 | −0.000 | 0.003 | 0.044 |
| Stage III | 0.005 | −0.000 | 0.011 | 0.003 | 0.069 |
| SCC | 0.007 | −0.001 | 0.015 | 0.004 | 0.069 |
| RH | 0.008 | −0.004 | 0.021 | 0.006 | 0.180 |
|
| B, Disease free
survival (hazard ratio) |
|
|
Moderator | β | Lower 95%
CI | Upper 95%
CI | SE | P-value |
|
| Stage IB2 | 0.008 | −0.005 | 0.020 | 0.007 | 0.246 |
| Stage II | −0.004 | −0.011 | 0.002 | 0.003 | 0.175 |
| Stage III | 0.002 | −0.004 | 0.007 | 0.003 | 0.525 |
| SCC | 0.005 | −0.001 | 0.011 | 0.003 | 0.121 |
| RH | 0.006 | −0.005 | 0.017 | 0.006 | 0.310 |
|
| C, Mortality
(odds ratio) |
|
|
Moderator | β | Lower 95%
CI | Upper 95%
CI | SE | P-value |
|
| Stage IB2 | 0.007 | −0.010 | 0.023 | 0.008 | 0.424 |
| Stage II | 0.004 | −0.009 | 0.017 | 0.007 | 0.507 |
| Stage III | −0.004 | −0.013 | 0.005 | 0.004 | 0.377 |
| SCC | −0.004 | −0.030 | 0.023 | 0.014 | 0.792 |
| RH | −0.005 | −0.023 | 0.012 | 0.009 | 0.548 |
|
| D, Recurrence
(odds ratio) |
|
|
Moderator | β | Lower 95%
CI | Upper 95%
CI | SE | P-value |
|
| Stage IB2 | 0.011 | −0.001 | 0.023 | 0.006 | 0.079 |
| Stage II | −0.004 | −0.011 | 0.003 | 0.004 | 0.270 |
| Stage III | 0.000 | −0.006 | 0.007 | 0.003 | 0.926 |
| SCC | −0.000 | −0.020 | 0.020 | 0.010 | 0.986 |
| RH | 0.007 | −0.007 | 0.020 | 0.007 | 0.334 |
Risk of bias analysis
Table SII presents
the results of the assessments of the risk of bias in the RCTs and
retrospective studies. The RCTs included failed to clearly describe
randomization, allocation concealment and blinding of outcome
assessment. The trial of Cetina et al (31) had high number of patients lost to
follow up Among the retrospective studies, the selection of
participants was from multiple hospital settings in four studies
(12,25–27);
only one study (34) performed
baseline matching of study cohorts, while two studies (11,12)
presented multivariate-adjusted HRs.
Discussion
The utility of additional surgery after CCRT for the
management of LACC has remained under considerable debate in the
gynecological literature for over two decades (7,18,22,23).
While adjuvant hysterectomy has fallen out of favor in the USA
(12), a French survey from 2016
reported that one-third of academic centers still perform the
procedure in patients with complete response to CCRT and negative
paraaortic nodes (26). To date, two
RCTs have been performed to compare outcomes for patients treated
with or without hysterectomy after CCRT. A trial by Morice et
al (32) in France conducted in
2003 included 61 patients but was closed early. The authors
reported that since a majority of the treating physicians favored
hysterectomies, they were reluctant to enroll patients for the
trial. In another study, Cetina et al (31) did not obtain any differences in OS or
DFS when comparing patients with patients stage IB2-IIB LACC
undergoing external beam radiotherapy (EBRT) with chemotherapy
followed by either hysterectomy or brachytherapy. Given the
limitations of both of these RCTs, numerous clinicians have
reported their experience regarding the role of adjuvant
hysterectomy, but by means of retrospective studies (11,12,24–30,33–35). The
present review was performed to provide comprehensive and updated
evidence on this subject.
The present analysis of all included studies points
to significantly better OS and DFS in patients undergoing
hysterectomy after CCRT. By contrast, a previous meta-analysis by
Shi et al (10) reported no
difference in OS between the two groups (HR, 1.13; 95% CI, 0.91 to
1.41). This discrepancy may be attributed to two major reasons:
First, the study by Shi et al (10) included only pooled data from eight
studies and furthermore, in two of those studies, patients were
only treated with radiotherapy without concurrent chemotherapy. The
results of the present study, however, require to be interpreted
with caution considering the instability of the subgroup analyses.
The pooled results of RCTs did not demonstrate any significant
differences in OS or DFS. However, the results may not be reliable
as only 2 RCTs were available for analysis both of small sample
size. There was high inter-study heterogeneity and low overall
quality. The pooled analysis of retrospective studies did indicate
a significantly improved OS and DFS in patients undergoing
hysterectomy.
Brachytherapy after EBRT is an important element of
CCRT. A combined dose of ≥80-85 Gy of brachytherapy and EBRT is
recommended for LACC (36). In the
present review, four studies compared hysterectomy as an
alternative to brachytherapy after EBRT and chemotherapy. In the
absence of brachytherapy, the total radiation dose in patients
undergoing CCRT with hysterectomy was lower than that in patients
receiving both EBRT and brachytherapy. This leads to baseline
differences among these studies that are absent from the
comparisons of studies utilizing brachytherapy for both study
groups. To eliminate such variation, a subgroup analysis was
performed. No significant differences in OS or DFS were identified,
irrespective of the use of brachytherapy in the CCRT and
hysterectomy group. The insignificant results in these subgroups
despite the significant results in the earlier total analysis may
be due to the small number of studies pooled. In addition, the
excluded data in the study by Albert et al (12) (which did not report data on
brachytherapy), with the upper end of the 95% CI above 1 (HR, 0.64;
95% CI, 0.40 to 1.01) may have contributed to the insignificant
results. It may be reasoned that the results of the present
meta-analysis with grouping based on the use of brachytherapy
provides better evidence than the overall analysis, as studies with
similar baseline treatment protocols were pooled in these
subgroups.
After pooling data on the absolute number of deaths
and recurrences, no significant difference in mortality was
observed between the two study groups, but a significantly higher
incidence of recurrence was determined in the CCRT only group. Shim
et al (8) obtained similar
results in their meta-analysis, which also reported no differences
in mortality (OR, 1.01; 95% CI, 0.58 to 1.78) but higher rates of
recurrence (OR, 0.59; 95% CI, 0.44 to 0.79) in patients undergoing
CCRT without hysterectomy than in those undergoing hysterectomy. On
further subgroup analyses, the recurrence rates did not differ for
the RCTs, probably due to the small sample size, and they remained
significant on subgroup analyses based on the use of brachytherapy.
Of note, the present analysis of DFS in the brachytherapy subgroup
indicated a lack of difference between the CCRT with hysterectomy
and CCRT alone groups. This variation may be due to the addition of
the study of Sun et al (30),
which reported a significant difference in recurrence rates [CCRT
with hysterectomy (16.6%) vs. CCRT alone (31.7%)] between the two
groups, in the latter analysis.
One of the biggest limitations when assessing the
benefit of adjuvant hysterectomy regarding clinical outcomes after
CCRT is the influence of confounding factors. The bias is further
amplified in the present results, as 12 of the 14 studies included
in the analysis were retrospective in nature. Several factors, such
as the presence of comorbidities, tumor size, tumor stage,
histology, residual disease after CCRT and lymph node involvement
may influence the decision to perform completion hysterectomy
(11,12,24,27).
Albert et al (12)
demonstrated that patients with stage IIA2 disease were less likely
to undergo hysterectomy, whereas patients with adenocarcinoma
(which is not as radiosensitive as SCC and has worse prognosis than
SCC) were more likely to undergo adjuvant surgery. Furthermore, the
use of radical vs. simple hysterectomy may also influence survival
and recurrence rates (37). In the
meta-regression analysis, a significant association between the
proportion of stage II disease and OS was determined. The OS
increased as the proportion of patients with stage II disease
increased. This may be attributed to the fact that adjuvant
hysterectomy after CCRT failure is easier to perform in patients
with stage II disease and may thereby account for the better
survival (10–12). In addition, it was not possible to
subdivide the present data according to the disease stage due to
the lack of adequate data from the included studies. No other
influence by the LACC stage, tumor histology or history of radical
hysterectomy on the pooled effect size was observed.
The presence of residual disease after CCRT is a
major concern and has been linked to local disease progression and
poor OS (38,39). According to certain clinicians,
adjuvant hysterectomy may remove residual tumor masses, thereby
improving local control (11,25).
Identification of patients with residual disease after CCRT is
generally based on clinical examination, MRI or cervical biopsy
results (40,41). However, these methods are less
accurate than surgical-pathology confirmation. Yang et al
(11) reported residual tumors in
27.4% of patients after CCRT based on imaging studies in their
cohort, but 64.1% of patients had residual tumor on the final
post-hysterectomy pathological examination. In the present study,
no meta-regression analysis was performed to assess the influence
of post-CCRT residual disease on pooled outcomes, as only six of
the included studies had reported these data.
Of note, the present meta-analysis had certain
limitations. First, as discussed earlier, the results are mostly
based on data from unmatched retrospective studies. The possibility
of selection bias having influenced the present results cannot be
ruled out. The HRs were only adjusted for confounding variables
using multivariate regression analysis in two of the studies
included (11,12). In addition, only two RCTs were
included (31,32), which was insufficient to determine
any significant differences. Furthermore, in most studies, HR
values were extrapolated from Kaplan-Meier survival curves and not
from the original data. The calculation of data from survival
curves is prone to errors (16). In
addition, variations amongst the included studies in patient
populations, and variables including CCRT doses, surgical
techniques and follow-up duration may have skewed the present.
Therefore, a random-effects model was used to account for such
inter-study variations. As another limitation, meta-regression was
not performed for all confounding factors, such as disease
sub-stages, lymph node metastasis or residual disease after CCRT
due to lack of data. Finally, the quality of the included studies
was not high, which limited our ability to draw strong
conclusions.
However, compared to previous studies (8,10), the
present review provides a significant update with the addition of
six new studies. Both HR and OR data were pooled with appropriate
subgroup and meta-regression analyses to provide a comprehensive
review. The stability of the results according to the sensitivity
analysis lends credibility to the present results.
To conclude, despite the overall analysis indicating
improved OS and DFS with the use of adjuvant hysterectomy after
CCRT, subgroup analyses of studies based on similar treatment
protocols failed to demonstrate any significant benefit of
hysterectomy post-CCRT for patients with LACC. However, it was
indicated that the recurrence rate may be higher in patients
undergoing CCRT without hysterectomy. In addition, analysis of
retrospective studies indicated significantly improved OS and DFS
in patients undergoing hysterectomy compared with patients not
undergoing the adjuvant surgery. The limited quality of studies and
selection bias from retrospective data restrict our ability to draw
conclusions. Further high-quality, homogenous RCTs are required to
derive stronger evidence. In addition, future studies should
provide detailed analyses regarding the use of adjuvant
hysterectomy based on different tumor histologies, tumor stages,
amounts of residual disease and different doses of total
radiotherapy to confirm or disprove the benefit of hysterectomy in
these patients.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
WL conceived and designed the study. CL, ZY and LG
collected the data and performed the literature search. WL was
involved in the writing of the manuscript. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Shrestha AD, Neupane D, Vedsted P and
Kallestrup P: Cervical cancer prevalence, incidence and mortality
in low and middle income countries: A systematic review. Asian Pac
J Cancer Prev. 19:319–324. 2018.PubMed/NCBI
|
|
3
|
Pecorelli S, Zigliani L and Odicino F:
Revised FIGO staging for carcinoma of the cervix. Int J Gynecol
Obstet. 105:107–108. 2009. View Article : Google Scholar
|
|
4
|
Haie-Meder C, Morice P and Castiglione M;
ESMO Guidelines Working Group, : Cervical cancer: ESMO clinical
recommendations for diagnosis, treatment and follow-up. Ann Oncol.
(20 Suppl 4):S27–S28. 2009. View Article : Google Scholar
|
|
5
|
Tanderup K, Lindegaard JC, Kirisits C,
Haie-Meder C, Kirchheiner K, de Leeuw A, Jürgenliemk-Schulz I, Van
Limbergen E and Pötter R: Image Guided Adaptive Brachytherapy in
cervix cancer: A new paradigm changing clinical practice and
outcome. Radiother Oncol. 120:365–369. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Fanfani F, Fagotti A, Ferrandina G,
Raspagliesi F, Ditto A, Cerrotta AM, Morganti A, Smaniotto D and
Scambia G: Neoadjuvant chemoradiation followed by radical
hysterectomy in FIGO Stage IIIB cervical cancer: Feasibility,
complications, and clinical outcome. Int J Gynecol Cancer.
19:1119–1124. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Platt SL, Patel A, Humphrey PJ, Al-Booz H
and Bailey J: Completion surgery after chemoradiotherapy for
cervical cancer -is there a role? UK Cancer Centre experience of
hysterectomy post chemo-radiotherapy treatment for cervical cancer.
J Obstet Gynaecol. 39:68–73. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Shim SH, Kim SN, Chae SH, Kim JE and Lee
SJ: Impact of adjuvant hysterectomy on prognosis in patients with
locally advanced cervical cancer treated with concurrent
chemoradiotherapy: A meta-analysis. J Gynecol Oncol. 29:e252018.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Yang J, Shen K, Wang J, Yang J and Cao D:
Extrafascial hysterectomy after concurrent chemoradiotherapy in
locally advanced cervical adenocarcinoma. J Gynecol Oncol.
27:e402016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Shi D, Liang Z, Zhang C, Zhang H and Liu
X: The effect of surgery on the survival status of patients with
locally advanced cervical cancer after
radiotherapy/chemoradiotherapy: A meta-analysis. BMC Cancer.
18:3082018. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Yang J, Yang J, Cao D, Shen K, Ma J and
Zhang F: Completion hysterectomy after chemoradiotherapy for
locally advanced adeno-type cervical carcinoma: Updated survival
outcomes and experience in post radiation surgery. J Gynecol Oncol.
31:e162020. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Albert A, Allbright R, Lee A and
Vijayakumar S: Preoperative chemoradiation followed by hysterectomy
for cervical cancer: Patterns of care and survival in a large,
hospital database. J Gynecol Oncol. 30:e412019. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Moher D, Liberati A, Tetzlaff J and Altman
DG; PRISMA Group, : Preferred reporting items for systematic
reviews and meta-analyses: The PRISMA statement. BMJ.
339:b25352009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Higgins JPT, Altman DG and Sterne JAC:
Chapter 8: Assessing risk of bias in included studies. Higgins JPT,
Churchill R, Chandler J and Cumpston MS: Cochrane Handbook for
Systematic Reviews of Interventions version 5.2.0. (updated June
2017), Cochrane, 2017. Available from. simplewww.training.cochrane.org/handbook
|
|
15
|
Kim SY, Park JE, Lee YJ, Seo HJ, Sheen SS,
Hahn S, Jang BH and Son HJ: Testing a tool for assessing the risk
of bias for nonrandomized studies showed moderate reliability and
promising validity. J Clin Epidemiol. 66:408–414. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Tierney JF, Stewart LA, Ghersi D, Burdett
S and Sydes MR: Practical methods for incorporating summary
time-to-event data into meta-analysis. Trials. 8:162007. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wallace BC, Schmid CH, Lau J and
Trikalinos TA: Meta-Analyst: Software for meta-analysis of binary,
continuous and diagnostic data. BMC Med Res Methodol. 9:802009.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Li H, Pang Y and Cheng X: Surgery of
primary sites for stage IVB cervical cancer patients receiving
chemoradiotherapy: A population-based study. J Gynecol Oncol.
31:e82020. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Gosset M, Chargari C, Bentivegna E, Leary
A, Genestie C, Maulard A, Morice P and Gouy S: Should we cease to
perform salvage hysterectomy after chemoradiation and brachytherapy
in locally advanced cervical cancer? Anticancer Res. 39:2919–2926.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Haque W, Verma V, Butler EB and Teh BS:
Utilization of hysterectomy following chemoradiation for IB2/IIA2
cervical cancer in the national cancer data base. Anticancer Res.
38:3175–3179. 2018.PubMed/NCBI
|
|
21
|
Huang XB, Zhang WW, Wu SG, Sun JY, He ZY
and Zhou J: Survival benefits with the addition of adjuvant
hysterectomy to radiochemotherapy for treatment of stage I–II
adenocarcinoma of the uterine cervix. J Surg Oncol. 118:574–580.
2018.PubMed/NCBI
|
|
22
|
Keys HM, Bundy BN, Stehman FB, Okagaki T,
Gallup DG, Burnett AF, Rotman MZ and Fowler WC Jr: Radiation
therapy with and without extrafascial hysterectomy for bulky stage
IB cervical carcinoma: A randomized trial of the Gynecologic
Oncology Group. Gynecol Oncol. 89:343–353. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Perez CA, Grigsby PW, Camel HM, Galakatos
AE, Mutch D and Lockett MA: Irradiation alone or combined with
surgery in stage IB, IIA and IIB carcinoma of uterine cervix:
Update of a nonrandomized comparison. Int J Radiat Oncol Biol Phys.
31:703–716. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Zheng D, Mou HP, Diao P, Li XM, Zhang CL,
Jiang J, Chen JL, Wang LS, Wang Q, Zhou GY, et al:
Chemoradiotherapy in combination with radical surgery is associated
with better outcome in cervical cancer patients. Oncotarget.
9:2866–2875. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Hass P, Eggemann H, Costa SD and Ignatov
A: Adjuvant hysterectomy after radiochemotherapy for locally
advanced cervical cancer. Strahlenther Onkol. 193:1048–1055. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Mazeron R, Gouy S, Chargari C, Rivin Del
Campo E, Dumas I, Mervoyer A, Genestie C, Bentivegna E, Balleyguier
C, Pautier P, et al: Post radiation hysterectomy in locally
advanced cervical cancer: Outcomes and dosimetric impact. Radiother
Oncol. 120:460–466. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Fanfani F, Vizza E, Landoni F, de Iaco P,
Ferrandina G, Corrado G, Gallotta V, Gambacorta MA, Fagotti A,
Monterossi G, et al: Radical hysterectomy after chemoradiation in
FIGO stage III cervical cancer patients versus chemoradiation and
brachytherapy: Complications and 3-years survival. Eur J Surg
Oncol. 42:1519–1525. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Chereau E, DE LA Hosseraye C, Ballester M,
Monnier L, Rouzier R, Touboul E and Daraï E: The role of completion
surgery after concurrent radiochemotherapy in locally advanced
stages IB2-IIB cervical cancer. Anticancer Res. 33:1661–1666.
2013.PubMed/NCBI
|
|
29
|
Wang N, Li WW, Li JP, Liu JY, Zhou YC,
Zhang Y, Hu J, Huang YH, Chen Y, Wei LC, et al: Comparison of
concurrent chemoradiotherapy followed by radical surgery and
high-dose-rate intracavitary brachytherapy: A retrospective study
of 240 patients with FIGO stage IIB cervical carcinoma. Onco
Targets Ther. 7:91–100. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Sun L, Sheng X, Jiang J, Li X, Liu N, Liu
Y, Zhang T, Li D, Zhang X and Wei P: Surgical morbidity and
oncologic results after concurrent chemoradiation therapy for
advanced cervical cancer. Int J Gynaecol Obstet. 125:111–115. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Cetina L, González-Enciso A, Cantú D,
Coronel J, Pérez-Montiel D, Hinojosa J, Serrano A, Rivera L,
Poitevin A, Mota A, et al: Brachytherapy versus radical
hysterectomy after external beam chemoradiation with gemcitabine
plus cisplatin: A randomized, phase III study in IB2-IIB cervical
cancer patients. Ann Oncol. 24:2043–2047. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Morice P, Rouanet P, Rey A, Romestaing P,
Houvenaeghel G, Boulanger JC, Leveque J, Cowen D, Mathevet P,
Malhaire JP, et al: Results of the GYNECO 02 study, an FNCLCC phase
III trial comparing hysterectomy with no hysterectomy in patients
with a (clinical and radiological) complete response after
chemoradiation therapy for stage IB2 or II cervical cancer.
Oncologist. 17:64–71. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Lèguevaque P, Motton S, Delannes M,
Querleu D, Soulé-Tholy M, Tap G and Houvenaeghel G: Completion
surgery or not after concurrent chemoradiotherapy for locally
advanced cervical cancer? Eur J Obstet Gynecol Reprod Biol.
155:188–192. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Cetina L, Garcia-Arias A, Candelaria M,
Cantú D, Rivera L, Coronel J, Bazan-Perkins B, Flores V, Gonzalez A
and Dueñas-González A: Brachytherapy versus radical hysterectomy
after external beam chemoradiation: A non-randomized matched
comparison in IB2-IIB cervical cancer patients. World J Surg Oncol.
7:192009. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Darus CJ, Callahan MB, Nguyen QN, Pastore
LM, Schneider BF, Rice LW and Jazaeri AA: Chemoradiation with and
without adjuvant extrafascial hysterectomy for IB2 cervical
carcinoma. Int J Gynecol Cancer. 18:730–735. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Gaffney DK, Erickson-Wittmann BA, Jhingran
A, Mayr NA, Puthawala AA, Moore D, Rao GG, Small W Jr, Varia MA,
Wolfson AH, et al: ACR Appropriateness Criteria® on
advanced cervical cancer expert panel on radiation
oncology-gynecology. Int J Radiat Oncol Biol Phys. 81:609–614.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Boers A, Arts HJG, Klip H, Nijhuis ER,
Pras E, Hollema H, Wisman GB, Nijman HW, Mourits MJ, Reyners AK, et
al: Radical surgery in patients with residual disease after
(chemo)radiation for cervical cancer. Int J Gynecol Cancer.
24:1276–1285. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Houvenaeghel G, Lelievre L, Buttarelli M,
Jacquemier J, Carcopino X, Viens P and Gonzague-Casabianca L:
Contribution of surgery in patients with bulky residual disease
after chemoradiation for advanced cervical carcinoma. Eur J Surg
Oncol. 33:498–503. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Azria E, Morice P, Haie-Meder C, Thoury A,
Pautier P, Lhomme C, Duvillard P and Castaigne D: Results of
hysterectomy in patients with bulky residual disease at the end of
chemoradiotherapy for stage IB2/II cervical carcinoma. Ann Surg
Oncol. 12:332–337. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Nijhuis ER, van der Zee AGJ, in't Hout BA,
Boomgaard JJ, de Hullu JA, Pras E, Hollema H, Aalders JG, Nijman
HW, Willemse PH and Mourits MJ: Gynecologic examination and
cervical biopsies after (chemo) radiation for cervical cancer to
identify patients eligible for salvage surgery. Int J Radiat Oncol
Biol Phys. 66:699–705. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Gui B, Valentini AL, Miccò M, D'Agostino
GR, Tagliaferri L, Zannoni GF, Fanfani F, Manfredi R and Bonomo L:
Cervical cancer response to neoadjuvant chemoradiotherapy: MRI
assessment compared with surgery. Acta radiol. 57:1123–1131. 2016.
View Article : Google Scholar : PubMed/NCBI
|