Introduction
Bile duct carcinoma (BDC) consists of heterogenous
groups of neoplasia according to their location. Extrahepatic BDC
has been divided into perihilar and distal BDC (1). The two subtypes are regarded as
separate entities because of differences in their epidemiology,
clinical management, and prognosis (2–5).
However, the histopathological differences have not been
clarified.
Mesothelin (MSLN) is a 40-kDa cell surface
glycoprotein, which is expressed in normal mesothelial cells that
line the surface of the pleura, pericardium, and peritoneum
(6,7). Overexpression of MSLN in various types
of malignant tumors, including malignant mesothelioma, ovarian
cancer, and pancreatic cancer has been reported (8–11). The
full-length human MSLN gene encodes primarily a 71-kDa precursor
protein. It can be physiologically cleaved by several furin-like
proteases into a membrane-bound 40-kDa C-terminal fragment and a
31-kDa N-terminal fragment, and the latter is secreted into the
blood. The former fragment is MSLN, which is attached to the cell
membrane through a glycosyl-phosphatidylinositol anchor (7,12).
MSLN is one of the binding partners of cancer
antigen 125 (CA125) (13–15). Previous studies showed that
heterotypic adhesion through the high affinity interaction between
MSLN and CA125 could facilitate peritoneal metastases of ovarian
cancer (13,15). Other studies (16,17)
showed that expression of MSLN in patients with extrahepatic BDC
and intrahepatic cholangiocellular carcinoma was associated with
poor prognosis. However, no studies have evaluated the incidence of
MSLN and CA125 co-expression in patients with extrahepatic BDC. The
aim of this study was to evaluate the differences in the incidence
of co-expression between perihilar and distal BDC patients and the
impact of CA125 and MSLN expression on prognosis.
Materials and methods
Ethics approval and consent to
participate
This study was performed in accordance with the
Declaration of Helsinki and was approved by the institutional
review board of the National Defense Medical College (approval no.
4115). All patients agreed to participate in this study, and
written informed consent was obtained from all patients.
Tumor specimens
Tissue samples taken from patients who underwent
surgical resection for perihilar or distal BDC from January 2007 to
December 2015 were immunohistochemically examined. Pathological T
and N factors and Stage were recorded according to the 8th edition
of the Union for International Cancer Control (UICC) staging
(1).
Immunohistochemistry
Formalin-fixed paraffin-embedded tissue blocks were
collected. Immunohistochemistry (IHC) was performed on tumor
samples using monoclonal antibodies against MSLN (clone 5B2 diluted
1:50; Leica Biosystems Newcastle Ltd.) and CA125 (clone M11
Ready-to-Use; Agilent Technologies Inc.) at room temperature for 60
min. Next, samples were incubated with Histofine (Simple Stain MAX
PO (MULTI); Nichirei Biosciences Inc.) at room temperature for 30
min. Specific antigen-antibody reactions were visualized with
diaminobenzidine tetrahydrochloride and hydrogen peroxide (Liquid
DAB+ Substrate Chromogen System; Agilent Technologies Inc.). Slides
were counterstained with hematoxylin for 1.5 min, then rinsed
gently in reagent quality water for 10 min.
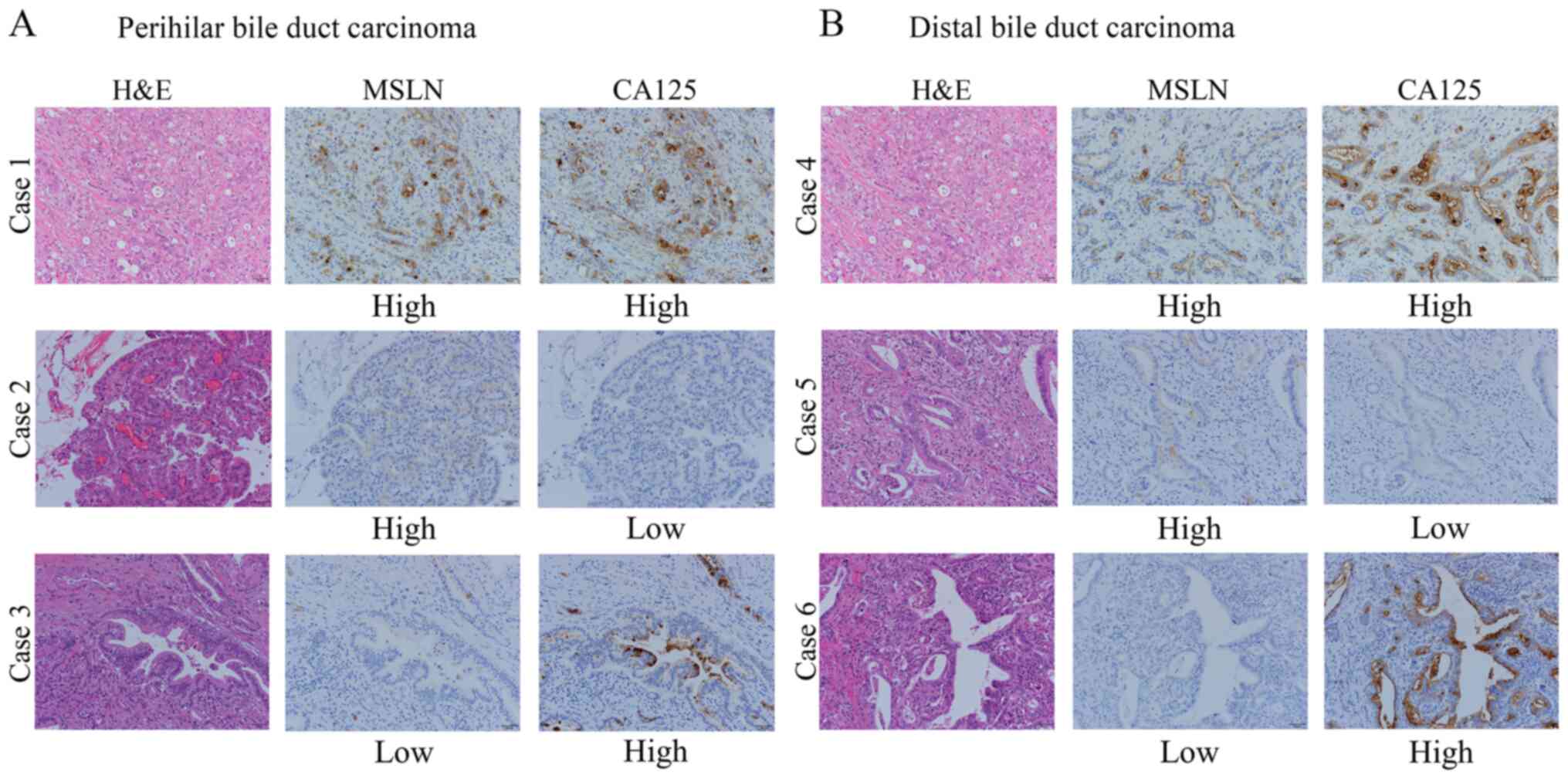
Immunohistochemical evaluation
All histological assessments were performed on the
tumor region of the specimen with magnification, ×200. Each slide
was independently evaluated by three observers (Y.T., Y.Y. and
T.E.) who were blinded to the clinical outcomes. Discrepancies
among the investigators were resolved by consensus using a
multiheaded microscope. Immunostaining for MSLN and CA125 was
evaluated for the proportion of tumor cells stained in each case.
The levels of MSLN and CA125 expression were assessed as the number
of stained tumor cells divided by the total number of tumor cells
on the largest cross-sectioned slice of the tumor and were
classified as follows: 0% to <50% and ≥50% (Fig. 1). The proportional expression levels
in the tumor, <50% and ≥50%, were defined as low- and high-level
expression, respectively. We defined the positive co-expression as
the expression of both MSLN and CA125 in ≥50% of the tumor
cells.
Statistical analysis
We used the Chi-squared (χ2) test or
Fisher's exact test to determine the association of MSLN and CA125
co-expression with clinicopathological data. All numerical data
were compared by independent samples t-test. Survival curves of
patients were drawn using the Kaplan-Meier method. Differences in
survival curves were analyzed by the log-rank test. Statistical
significance was defined as P<0.05 for all analyses. Excel
Statistics 2012® software package (SSRI) was used for
statistical analyses.
Results
Specimen selection
Tissue samples were obtained from 31 patients with
perihilar BDC and 43 patients with distal BDC. The patients'
clinicopathological characteristics are summarized in Table I. There were no significant
differences in the distribution of age, sex, incidence of lymph
node metastases, and proportion of patients who received adjuvant
chemotherapy between the two groups. Conversely, the distribution
of T category and stage, types of surgical procedure, and R status
differed significantly.
 | Table I.Clinicopathological characteristics of
74 patients with perihilar (n=31) or distal (n=43) BDC. |
Table I.
Clinicopathological characteristics of
74 patients with perihilar (n=31) or distal (n=43) BDC.
| Parameter | Total, n | Perihilar BDC | Distal BDC | P-value |
|---|
| Median age (range),
years |
| 72 (38–86) | 70 (42–88) | 0.654 |
| Sex, n (%) |
|
|
|
|
| Male | 54 | 20 (37) | 34 (63) | 0.164 |
|
Female | 20 | 11 (55) | 9 (45) |
|
| pT stage UICC, n
(%) |
|
|
|
|
|
pT1-2 | 51 | 16 (31) | 35 (69) |
0.006 |
| pT3-4 | 23 | 15 (65) | 8 (35) |
|
| pN stage UICC, n
(%) |
|
|
|
|
| pN0 | 27 | 11 (41) | 16 (59) |
0.879 |
| pN1-2 | 47 | 20 (43) | 27 (57) |
|
| Pathological stage
UICC, n (%) |
|
|
|
|
|
I–II | 41 | 8 (20) | 33 (80) | <0.001 |
|
III–IV | 33 | 23 (70) | 10 (30) |
|
| Surgical procedure,
n (%) |
|
|
|
|
|
Extended right or left
hepatectomya with bile
duct resection | 25 | 25 (100) | 0 (0) | NC |
|
Extrahepatic bile duct
resection | 1 | 1 (100) | 0 (0) |
|
|
Subtotal stomach-preserving
pancreaticoduodenectomy | 37 | 1 (2) | 36 (98) |
|
|
Hepatectomy and
pancreaticoduodenectomy | 11 | 4 (36) | 7 (64) |
|
| Residual tumor, n
(%) |
|
|
|
|
| R0 | 40 | 12 (30) | 28 (70) |
0.025 |
| R1 | 34 | 19 (56) | 15 (44) |
|
| Recurrence, n
(%) |
|
|
|
|
|
Yes | 40 | 20 (50) | 20 (50) |
0.125 |
| No | 34 | 11 (32) | 23 (68) |
|
| Adjuvant
chemotherapy, n (%) |
|
|
|
|
|
Yes | 11 | 4 (36) | 7 (64) |
0.477 |
| No | 63 | 27 (43) | 36 (57) |
|
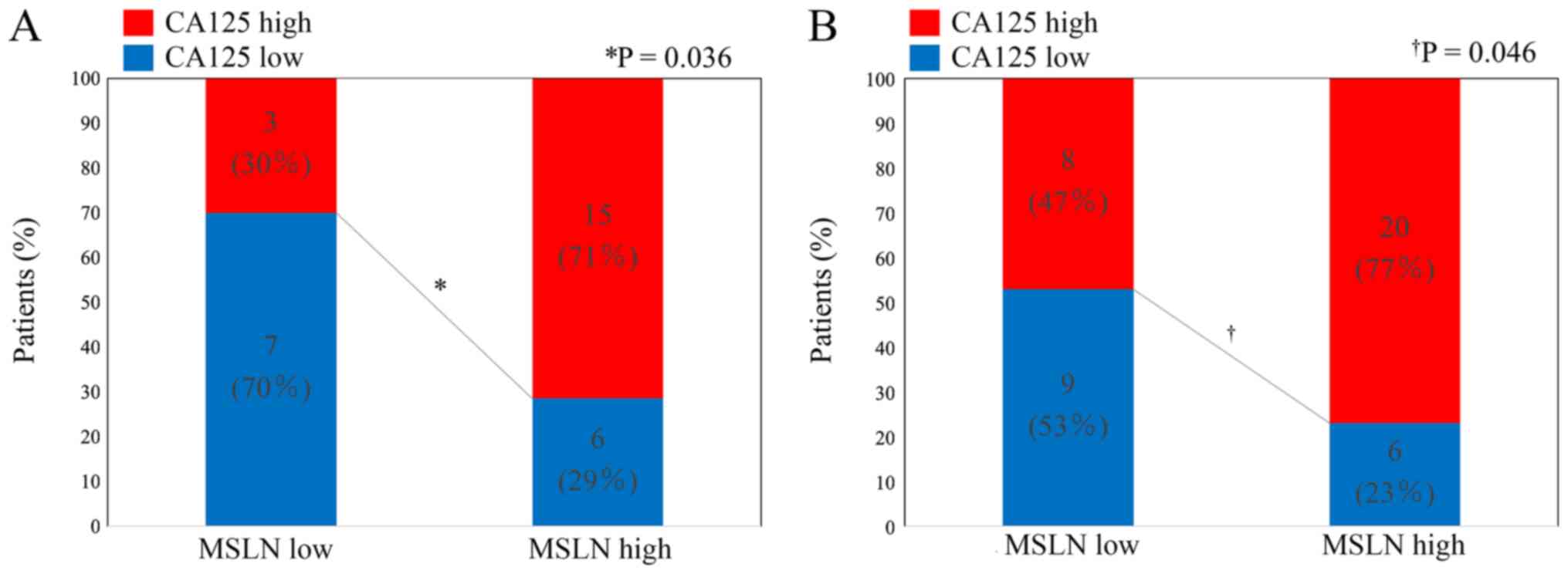
MSLN and CA125 expression in perihilar
or distal BDC
High-level expression of MSLN and CA125 was detected
in 21 specimens (68%) and 18 specimens (58%), respectively, from
perihilar BDC, and in 26 specimens (60%) and 28 specimens (65%),
respectively, from distal BDC. Fisher's exact test indicated the
association between these two expressions in perihilar BDC
(P=0.036) and in distal BDC (P=0.046) (Fig. 2).
Tables II and
III show the comparison of
pathological features according to the expression of MSLN and CA125
in patients with perihilar and distal BDC, respectively. In the
perihilar BDC group, lymph node metastases were more frequently
observed in patients with MSLN high-level expression (P=0.060),
CA125 high-level expression (P=0.014), and co-expression (P=0.002).
Blood vessel permeation (P=0.064) and neural invasion (P=0.064)
were more frequently observed in patients with high-level CA125
expression. In the distal BDC group, neural invasion was more
frequently observed in patients with MSLN high-level expression
(P=0.055) and CA125 high-level expression (P=0.037). However,
co-expression of MSLN and CA125 was not associated with any of the
evaluated clinicopathological factors.
| Table II.Clinicopathological features of
patients with perihilar bile duct carcinoma according to the
expression levels of MSLN and CA125. |
Table II.
Clinicopathological features of
patients with perihilar bile duct carcinoma according to the
expression levels of MSLN and CA125.
|
| MSLN
expression | CA125
expression | Co-expression |
|---|
|
|
|
|
|
|---|
| Parameter | High level
(n=21) | Low level
(n=10) | P-value | High level
(n=18) | Low level
(n=13) | P-value | Positive
(n=15) | Negative
(n=16) | P-value |
|---|
| Histological
classification |
|
|
|
|
|
|
|
|
|
| Grade
1/2 | 15 | 10 | 0.074 | 13 | 12 | 0.176 | 10 | 15 | 0.072 |
| Grade
3 | 6 | 0 |
| 5 | 1 |
| 5 | 1 |
|
| Type |
|
|
|
|
|
|
|
|
|
|
Papillary-expanding | 1 | 1 | NC | 0 | 2 | NC | 0 | 2 | NC |
|
Papillary-infiltrating | 5 | 3 |
| 6 | 2 |
| 4 | 4 |
|
|
Nodular-expanding | 0 | 0 |
| 0 | 0 |
| 0 | 0 |
|
|
Nodular-infiltrating | 9 | 4 |
| 7 | 6 |
| 7 | 6 |
|
|
Flat-expanding | 0 | 0 |
| 0 | 0 |
| 0 | 0 |
|
|
Flat-infiltrating | 6 | 2 |
| 5 | 3 |
| 4 | 4 |
|
| pT stage UICC |
|
|
|
|
|
|
|
|
|
|
pT1-2 | 9 | 7 | 0.152 | 8 | 8 | 0.347 | 6 | 10 | 0.210 |
|
pT3-4 | 12 | 3 |
| 10 | 5 |
| 9 | 6 |
|
| pN stage UICC |
|
|
|
|
|
|
|
|
|
|
pN0 | 5 | 6 | 0.060 | 3 | 8 | 0.014 | 1 | 10 | 0.002 |
|
pN1-2 | 16 | 4 |
| 15 | 5 |
| 14 | 6 |
|
| pStage UICC |
|
|
|
|
|
|
|
|
|
|
pI–II | 3 | 5 | 0.048 | 2 | 6 | 0.037 | 0 | 8 | 0.002 |
|
pIII–IV | 18 | 5 |
| 16 | 7 |
| 15 | 8 |
|
| Lymphatic
permeation |
|
|
|
|
|
|
|
|
|
|
Positive | 20 | 9 | 0.548 | 18 | 11 | 0.168 | 15 | 14 | 0.258 |
|
Negative | 1 | 1 |
| 0 | 2 |
| 0 | 2 |
|
| Blood vessel
permeation |
|
|
|
|
|
|
|
|
|
|
Positive | 19 | 9 | 0.704 | 18 | 10 | 0.064 | 15 | 13 | 0.125 |
|
Negative | 2 | 1 |
| 0 | 3 |
| 0 | 3 |
|
| Neural
invasion |
|
|
|
|
|
|
|
|
|
|
Positive | 19 | 9 | 0.704 | 18 | 10 | 0.064 | 15 | 13 | 0.125 |
|
Negative | 2 | 1 |
| 0 | 3 |
| 0 | 3 |
|
| Residual tumor |
|
|
|
|
|
|
|
|
|
| R0 | 9 | 3 | 0.390 | 6 | 6 | 0.470 | 6 | 6 | 0.886 |
| R1 | 12 | 7 |
| 12 | 7 |
| 9 | 10 |
|
| Recurrence |
|
|
|
|
|
|
|
|
|
|
Yes | 6 | 5 | 0.221 | 14 | 6 | 0.076 | 11 | 9 | 0.269 |
| No | 15 | 5 |
| 4 | 7 |
| 4 | 7 |
|
| Table III.Clinicopathological features of
patients with distal bile duct carcinoma according to the
expression levels of MSLN and CA125. |
Table III.
Clinicopathological features of
patients with distal bile duct carcinoma according to the
expression levels of MSLN and CA125.
|
| MSLN
expression | CA125
expression | Co-expression |
|---|
|
|
|
|
|
|---|
| Parameter | High level
(n=26) | Low level
(n=17) | P-value | High level
(n=28) | Low level
(n=15) | P-value | Positive
(n=20) | Negative
(n=23) | P-value |
|---|
| Histological
classification |
|
|
|
|
|
|
|
|
|
| Grade
1/2 | 20 | 14 | 0.489 | 21 | 13 | 0.315 | 15 | 19 | 0.405 |
| Grade
3 | 6 | 3 |
| 7 | 2 |
| 5 | 4 |
|
| Type |
|
|
|
|
|
|
|
|
|
|
Papillary-expanding | 2 | 2 | NC | 1 | 3 | NC | 1 | 3 | NC |
|
Papillary-infiltrating | 14 | 2 |
| 12 | 4 |
| 11 | 5 |
|
|
Nodular-expanding | 0 | 1 |
| 0 | 1 |
| 0 | 1 |
|
|
Nodular-infiltrating | 7 | 7 |
| 10 | 4 |
| 5 | 9 |
|
|
Flat-expanding | 0 | 0 |
| 0 | 0 |
| 0 | 0 |
|
|
Flat-infiltrating | 3 | 5 |
| 5 | 3 |
| 3 | 5 |
|
| pT stage UICC |
|
|
|
|
|
|
|
|
|
|
pT1-2 | 20 | 15 | 0.304 | 28 | 11 | 0.212 | 16 | 19 | 0.566 |
|
pT3-4 | 6 | 2 |
| 4 | 4 |
| 4 | 4 |
|
| pN stage UICC |
|
|
|
|
|
|
|
|
|
|
pN0 | 8 | 8 | 0.280 | 8 | 8 | 0.109 | 6 | 10 | 0.362 |
|
pN1-2 | 18 | 9 |
| 20 | 7 |
| 14 | 13 |
|
| pStage UICC |
|
|
|
|
|
|
|
|
|
|
pI–II | 21 | 12 | 0.440 | 22 | 11 | 0.488 | 16 | 17 | 0.459 |
|
pIII–IV | 5 | 5 |
| 6 | 4 |
| 4 | 6 |
|
| Lymphatic
permeation |
|
|
|
|
|
|
|
|
|
|
Positive | 24 | 13 | 0.155 | 26 | 11 | 0.099 | 18 | 19 | 0.403 |
|
Negative | 2 | 4 |
| 2 | 4 |
| 2 | 4 |
|
| Blood vessel
permeation |
|
|
|
|
|
|
|
|
|
|
Positive | 25 | 14 | 0.163 | 27 | 12 | 0.114 | 19 | 20 | 0.359 |
|
Negative | 1 | 3 |
| 1 | 3 |
| 1 | 3 |
|
| Neural
invasion |
|
|
|
|
|
|
|
|
|
|
Positive | 26 | 14 | 0.055 | 28 | 12 | 0.037 | 20 | 20 | 0.144 |
|
Negative | 0 | 3 |
| 0 | 3 |
| 0 | 3 |
|
| Residual tumor |
|
|
|
|
|
|
|
|
|
| R0 | 17 | 11 | 0.964 | 18 | 10 | 0.876 | 13 | 15 | 0.988 |
| R1 | 9 | 6 |
| 10 | 5 |
| 7 | 8 |
|
| Recurrence |
|
|
|
|
|
|
|
|
|
|
Yes | 11 | 9 | 0.494 | 12 | 8 | 0.512 | 8 | 12 | 0.425 |
| No | 15 | 8 |
| 16 | 7 |
| 12 | 11 |
|
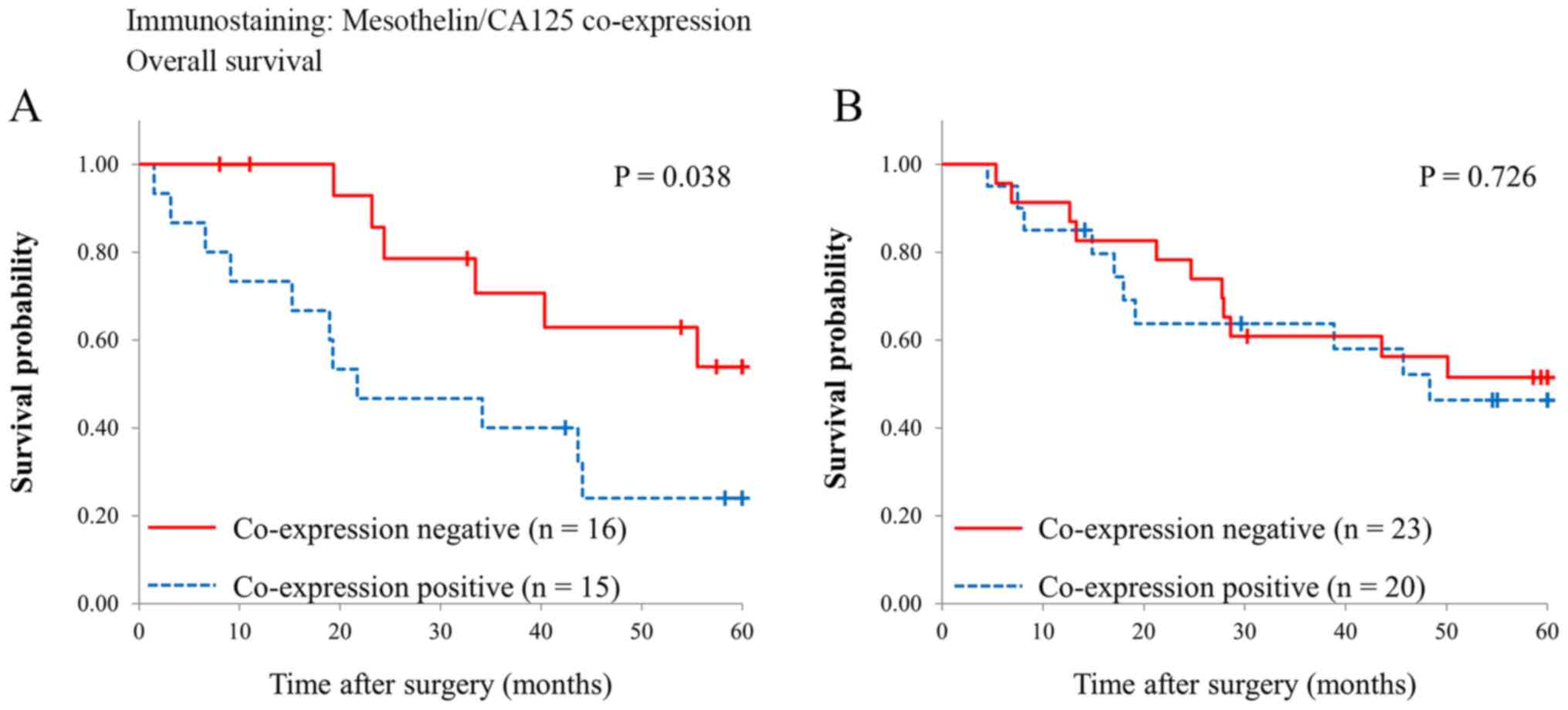
Survival analyses
Fig. 3 shows survival
curves of the patients with and without MSLN and CA125
co-expression. Overall survival was significantly different in the
patients with perihilar BDC (5-year survival rate, co-expression
negative vs. positive, 63 vs. 24%, P=0.038), while it was
comparable in the patients with distal BDC (5-year survival rate,
co-expression negative vs. co-expression positive, 56 vs. 46%,
P=0.726).
Discussion
In this study, we demonstrated that high-level
co-expression of MSLN and CA125 was observed in nearly half of the
patients either with perihilar (48%) or distal BDC (47%). However,
our results showed that co-expression was associated with lymph
node metastases and worse prognosis only in the patients with
perihilar BDC.
MSLN expression has been shown to promote
tumorigenesis and metastasis via lymphatic invasion of cancer both
in vitro and in vivo (18). Clinicopathologically, MSLN expression
was associated with lymph node metastases in patients with gastric
cancer (19) and colorectal cancer
(20). To date, few studies have
addressed MSLN expression in extrahepatic BDC. Kawamata et
al (16) showed that MSLN
high-level expression in extrahepatic BDC was associated with a
high incidence of liver metastases and worse survival rates, while
there was no association between MSLN expression and lymph node
metastases. However, their study included BDC from various
locations as follows: hilar, 16 cases; upper, 17 cases; middle, 20
cases; lower, 8 cases. We evaluated perihilar and distal BDC
separately because they were different in the types of surgical
procedure used or peritumor environment. In fact, our study showed
that there is a difference in the association of MSLN or CA125
expression with clinicopathological features between perihilar and
distal BDC. Our results suggested that biological features of BDC
might differ between the two subgroups.
Some papers indicated the differences for lymph node
metastasis between perihilar and distal BDC. Wang et al
(21) reported that distant lymph
node metastasis was commonly seen in perihilar BDC, not in distal
BDC. Hasebe et al (22)
reported that nodal tumors with more than 4 mitotic figures
significantly increased the hazard ratios of tumor recurrence and
initial distant organ metastasis in the perihilar portion.
Moreover, Noji et al (23)
showed that incidence of extra capsular lymph node involvement in
perihilar BDC was significantly lower than in the distal BDC. These
findings supported that lymph node metastasis showed different
pathological features between the perihilar and distal BDC. In this
study, co-expression of MSLN and CA125 was associated with lymph
node metastasis in perihilar BDC, not in distal BDC. These results
suggested that the mechanism of lymph node metastasis might be
different in perihilar and distal BDC.
A previous study showed that MSLN and CA125
co-expression was an independent predictor of poor survival in
patients with pancreatic ductal adenocarcinoma (PDAC) (11). Shimizu et al (24) showed that there is an interaction
between MSLN and CA125 by immunoprecipitation assay and revealed
that they were observed only in infiltrating components of PDAC and
increased at the invasion front by immunohistochemical analysis.
Chen et al (25) demonstrated
that the interaction of MSLN and CA125 markedly enhanced motility
and invasion of pancreatic cancer cells via selective induction of
matrix metalloproteinase (MMP)-7. Further, they reported that the
MSLN-CA125 interaction might induce pancreatic cancer cell motility
and invasion via a p38 MAPK-dependent pathway. These results
suggest that co-expression of MSLN and CA125 plays a significant
role in the acquisition of cell motility and invasive properties
(13). The relation between MSLN
expression and neural invasion in extrahepatic BDC was evaluated by
previous study (16). They reported
that MSLN expression did not associate with neural invasion. In
this study, CA125 expression was more associated with the neural
invasion than MSLN expression in perihilar and distal BDC. These
findings imply that CA125 promotes neural invasion in perihilar and
distal BDC, although it remains necessary to clarify the biological
function of CA125 expression in vitro and in vivo
studies.
A recent study by Ishida et al (26) reported that low expression of MUC5AC
and MUC6 predicts poor prognosis in patients with perihilar BDC but
not in those with distal BDC. Their results suggest that the role
of MUC5AC expression might differ between perihilar and distal BDC.
Our results similarly suggest that the role of MSLN and CA125
co-expression differs according to the location of BDC. The
embryological origin of perihilar and distal bile duct is the same,
but the environment is different. Most of the distal bile duct is
located in the pancreatic parenchyma, whereas the perihilar bile
duct is partially surrounded by the liver, hepatic artery, and
portal vein. The differences in tumor environment might influence
the invasion process and biological function of the MSLN and CA125
co-expression. Furthermore, the genomic spectra of BDC differs
according to the anatomical location, such as intrahepatic bile
duct, extrahepatic bile duct, or gallbladder (27). Genomic changes in the tumor might
influence the signaling pathway controlled by the co-expression of
MSLN and CA125. Genomic analysis of perihilar or distal BDC may
reveal the factors affecting the signaling pathway induced by MSLN
and CA125 co-expression.
Limitations of this study include its retrospective
nature and that it was conducted in a single facility with a
relatively small number of patients. However, to the best of our
knowledge, this was the first study evaluating the association of
MSLN and CA125 expression with clinicopathological features of
extrahepatic BDC by focusing on the differences in tumor location.
Our data should contribute to a better understanding of the
clinicopathological role of MSLN-CA125 co-expression in perihilar
or distal BDC. Another prospective multicenter trial is needed to
confirm the effectiveness of MSLN and CA125 expression in the
prediction of patient survival in perihilar and distal BDC.
In conclusion, MSLN and CA125 co-expression was
associated with advanced tumor stage and poor prognosis in patients
with perihilar BDC but not in those with distal BDC, which suggests
that the role of co-expression in BDC differs depending on the
location of the tumor.
Acknowledgements
The authors would like to thank Dr Nicole Clarke for
editing a draft of this manuscript.
Funding
The present study was supported in part by the Japan
Society for the Promotion of Science KAKENHI (grant no. JP
18K15295).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
YT, TE, KK, TS, NY, IF, TT, YY, TI, YM, ES, HT, HU
and YK analyzed and interpreted the patient data regarding the bile
duct carcinoma, the surgical procedure and the prognosis. YT, YY,
TE and SO performed the histological examination of the BDC
tissues. YT was a major contributor in writing the manuscript. TE,
HU and YK confirmed the authenticity of all the raw data. All
authors read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was performed in accordance with
the Declaration of Helsinki and was approved by the institutional
review board of the National Defense Medical College (Tokorozawa,
Japan; approval no. 4115). All patients agreed to participate in
this study, and written informed consent was obtained from all
patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
BDC
|
bile duct carcinoma
|
|
MSLN
|
mesothelin
|
|
CA125
|
cancer antigen 125
|
References
|
1
|
Brierley JD, Gospodarowicz MK and
Wittekind C: Digestive system tumours. TNM Classification of
Malignant Tumours. 8th edition. Wiley-Blackwell; Oxford: pp. 83–90.
2017
|
|
2
|
Rizvi S and Gores GJ: Pathogenesis,
diagnosis, and management of cholangiocarcinoma. Gastroenterology.
145:1215–1229. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hoyos S, Navas MC, Restrepo JC and Botero
RC: Current controversies in cholangiocarcinoma. Biochim Biophys
Acta Mol Basis Dis. 1864:1461–1467. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Khan SA, Tavolari S and Brandi G:
Cholangiocarcinoma: Epidemiology and risk factors. Liver Int. 39
(Suppl 1):19–31. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Matsukuma S, Tokumitsu Y, Shindo Y, Matsui
H and Nagano H: Essential updates to the surgical treatment of
biliary tract cancer. Ann Gastroenterol Surg. 3:378–389. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Chang K, Pai LH, Pass H, Pogrebniak HW,
Tsao MS, Pastan I and Willingham MC: Monoclonal antibody K1 reacts
with epithelial mesothelioma but not with lung adenocarcinoma. Am J
Surg Pathol. 16:259–268. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Chang K and Pastan I: Molecular cloning of
mesothelin, a differentiation antigen present on mesothelium,
mesotheliomas, and ovarian cancers. Proc Natl Acad Sci USA.
93:136–140. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Argani P, Iacobuzio-Donahue C, Ryu B,
Rosty C, Goggins M, Wilentz RE, Murugesan SR, Leach SD, Jaffee E,
Yeo CJ, et al: Mesothelin is overexpressed in the vast majority of
ductal adenocarcinomas of the pancreas: Identification of a new
pancreatic cancer marker by serial analysis of gene expression
(SAGE). Clin Cancer Res. 7:3862–3868. 2001.PubMed/NCBI
|
|
9
|
Ordóñez NG: Application of mesothelin
immunostaining in tumor diagnosis. Am J Surg Pathol. 27:1418–1428.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ho M, Hassan R, Zhang J, Wang QC, Onda M,
Bera T and Pastan I: Humoral immune response to mesothelin in
mesothelioma and ovarian cancer patients. Clin Cancer Res.
11:3814–3820. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Einama T, Kamachi H, Nishihara H, Homma S,
Kanno H, Takahashi K, Sasaki A, Tahara M, Okada K, Muraoka S, et
al: Co-expression of mesothelin and CA125 correlates with
unfavorable patient outcome in pancreatic ductal adenocarcinoma.
Pancreas. 40:1276–1282. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hassan R, Bera T and Pastan I: Mesothelin:
A new target for immunotherapy. Clin Cancer Res. 10:3937–3942.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Rump A, Morikawa Y, Tanaka M, Minami S,
Umesaki N, Takeuchi M and Miyajima A: Binding of ovarian cancer
antigen CA125/MUC16 to mesothelin mediates cell adhesion. J Biol
Chem. 279:9190–9198. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kaneko O, Gong L, Zhang J, Hansen JK,
Hassan R, Lee B and Ho M: A binding domain on mesothelin for
CA125/MUC16. J Biol Chem. 284:3739–3749. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gubbels JAA, Belisle J, Onda M, Rancourt
C, Migneault M, Ho M, Bera TK, Connor J, Sathyanarayana BK, Lee B,
et al: Mesothelin-MUC16 binding is a high affinity, N-glycan
dependent interaction that facilitates peritoneal metastasis of
ovarian tumors. Mol Cancer. 5:502006. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kawamata F, Kamachi H, Einama T, Homma S,
Tahara M, Miyazaki M, Tanaka S, Kamiyama T, Nishihara H, Taketomi
A, et al: Intracellular localization of mesothelin predicts patient
prognosis of extrahepatic bile duct cancer. Int J Oncol.
41:2109–2118. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Nomura R, Fujii H, Abe M, Sugo H, Ishizaki
Y, Kawasaki S and Hino O: Mesothelin expression is a prognostic
factor in cholangiocellular carcinoma. Int Surg. 98:164–169. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
He X, Wang L, Riedel H, Wang K, Yang Y,
Dinu CZ and Rojanasakul Y: Mesothelin promotes
epithelial-to-mesenchymal transition and tumorigenicity of human
lung cancer and mesothelioma cells. Mol Cancer. 16:632017.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Einama T, Homma S, Kamachi H, Kawamata F,
Takahashi K, Takahashi N, Taniguchi M, Kamiyama T, Furukawa H,
Matsuno Y, et al: Luminal membrane expression of mesothelin is a
prominent poor prognostic factor for gastric cancer. Br J Cancer.
107:137–142. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kawamata F, Homma S, Kamachi H, Einama T,
Kato Y, Tsuda M, Tanaka S, Maeda M, Kajino K, Hino O, et al:
C-ERC/mesothelin provokes lymphatic invasion of colorectal
adenocarcinoma. J Gastroenterol. 49:81–92. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Wang J, Bo X, Nan L, Wang CC, Gao Z, Suo
T, Ni X, Liu H, Lu P, Wang Y, et al: Landscape of distant
metastasis mode and current chemotherapy efficacy of the advanced
biliary tract cancer in the United States, 2010–2016. Cancer Med.
9:1335–1348. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Hasebe T, Konishi M, Iwasaki M, Endoh Y,
Nakagohri T, Takahashi S, Kinoshita T and Ochiai A: Histological
characteristics of tumor cells and stromal cells in vessels and
lymph nodes are important prognostic parameters of extrahepatic
bile duct carcinoma: A prospective study. Hum Pathol. 36:655–664.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Noji T, Miyamoto M, Kubota KC, Shinohara
T, Ambo Y, Matsuno Y, Kashimura N and Hirano S: Evaluation of extra
capsular lymph node involvement in patients with extra-hepatic bile
duct cancer. World J Surg Oncol. 10:1062012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Shimizu A, Hirono S, Tani M, Kawai M,
Okada K, Miyazawa M, Kitahata Y, Nakamura Y, Noda T, Yokoyama S, et
al: Coexpression of MUC16 and mesothelin is related to the invasion
process in pancreatic ductal adenocarcinoma. Cancer Sci.
103:739–746. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Chen SH, Hung WC, Wang P, Paul C and
Konstantopoulos K: Mesothelin binding to CA125/MUC16 promotes
pancreatic cancer cell motility and invasion via MMP-7 activation.
Sci Rep. 3:18702013. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ishida K, Osakabe M, Eizuka M, Tai S,
Sugimoto R, Fujita Y, Katagiri H, Takahara T, Uesugi N, Nitta H, et
al: The expression of gastrointestinal differentiation markers in
extrahepatic cholangiocarcinoma: Clinicopathological significance
based on tumor location. Hum Pathol. 92:91–100. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Nakamura H, Arai Y, Totoki Y, Shirota T,
Elzawahry A, Kato M, Hama N, Hosoda F, Urushidate T, Ohashi S, et
al: Genomic spectra of biliary tract cancer. Nat Genet.
47:1003–1010. 2015. View
Article : Google Scholar : PubMed/NCBI
|