Introduction
A major obstacle to cancer treatment is the adaptive
resistance of tumor cells, and alterations in the regulation of
gene expression caused by therapeutic stress may lead to treatment
failure (1). Several mechanisms,
including upregulation of gene expression and activation of signal
transducers, defend cancer cells against radiation to confer a
survival advantage. These events induce the expression of genes
encoding molecules that promote survival, repair DNA damage, induce
inflammation and inhibit apoptosis (2,3).
The expression of genes that encode components of
the urokinase system is associated with the diagnosis and prognosis
of cancer of the breast, gastrointestinal tract, colon and rectum,
esophagus, kidneys, endometrium and ovaries (4,5). The
urokinase system comprises of urokinase-type plasminogen activator
(uPA), tissue plasminogen activator (tPA), urokinase plasminogen
activator receptor (uPAR) and the plasminogen activator inhibitors
(PAI)-1 and −2 (6). Similar to
matrix metalloproteinases, urokinase principally induces lysis of
the basement membrane and the extracellular matrix during tissue
remodeling, which confers upon urokinase multifunctional roles in
neoplastic and malignant transformation, tumor angiogenesis, tumor
progression and metastasis (7).
The transcription of the gene encoding uPA, which
mediates metastasis, is activated by transcription factors such as
AP1, erythroblast transformation specific-1 (Ets-1) and Ets-2
(8). Furthermore, uPA is involved in
tissue remodeling (9). The
expression of its receptor uPAR (also known as CD87), a glycosyl
phosphatidylinositol-anchor protein, is regulated by transcription
factors such as Sp1, NF-κB, TCF, hypoxia-inducible factor-1α and
forkhead box protein (Fox)M1 (6,10). The
main functions of uPAR involve the regulation of extracellular
proteolysis and cell-extracellular matrix interactions (11). Upregulation of the expression of uPAR
and uPA enhances tumor progression as well as the aggressiveness of
numerous cancer cell types such as lung, breast and stomach cancer
(12). Furthermore, uPAs serve as
biomarkers and targets for treatment of human malignancies such as
breast and pancreatic cancer (13).
For example, the expression levels of uPA and PAI-1 are recommended
by the American Society of Clinical Oncology as markers for
selecting a regimen to treat patients with node-negative breast
cancer and to predict metastasis (14).
Cervical cancer remains a major public health
problem for women in developing countries, where it has caused
~270,000 deaths annually worldwide as of 2018 (15). In total, ~5% of all human cancer
cases are caused by infection with human papillomavirus (HPV), and
most are cancer cases are of the cervix (16). Despite the development and
availability of HPV vaccines, oncogenic HPVs are detected by
cervical cancer screening programs (17). Expression of uPA and PAI-1 correlates
with the prognosis of patients with cervical cancer, and HPV16 E6
induces cancer cells to migrate following the activation of uPA
(18,19). Furthermore, uPA serves as a
prognostic marker for the metastatic potential of cervical cancer
(20).
The present study therefore reasoned that
investigation of the components of the uPA system and their
relationship with resistance to therapy may improve the outcomes of
patients with cervical cancer. To provide support for this
hypothesis, whether irradiation enhanced the expression of uPA and
uPAR in patient tissue samples and cell lines and whether such
changes predicted patients' clinical outcomes were
investigated.
Materials and methods
Antibodies and reagents
Antibodies against uPAR, Ets-1 and FoxM1 (cat. nos.
12863, 14069 and 5436, respectively) were purchased from Cell
Signaling Technology, Inc., anti-GAPDH (cat. no. MA5-15738) was
purchased from Thermo Fisher Scientific, Inc. and anti-uPA (cat.
no. MAB7776) was purchased from EMD Millipore. Secondary
antibodies, goat anti-mouse IgG peroxidase conjugated (cat. no.
AP124P) and goat anti-rabbit IgG peroxidase conjugated (cat. no.
AP132P), were purchased from EMD Millipore. RIPA cell lysis buffer
and ECL solution were purchased from Merck KGaA. The working
dilution for uPAR, Ets-1 and FoxM1 antibodies was 1:1,000, 1:500
for uPA antibody and 1:15,000 for GAPDH antibody. The dilution used
for both secondary antibodies was 1:15,000.
Cell lines and irradiation
The human cervical carcinoma cell lines SiHa
(HPV16-positive), HeLa (HPV18-positive) and C33A (HPV-negative)
were purchased from the American Type Culture Collection and
maintained in DMEM medium supplemented with 10% fetal bovine serum
(Thermo Fisher Scientific, Inc.), 100 U/ml penicillin, and 100
mg/ml streptomycin in a humidified incubator at 37°C (5%
CO2). When exponentially proliferating cells in culture
dishes reached 70–80% confluence, they were exposed at room
temperature to 5 Gray ionizing radiation (6 MV) generated using a
linear accelerator (Varian Medical Systems, Inc.);
source-to-surface distance, 100 cm; field size=25×25
cm2. The sham-irradiated cell lysates in Fig. 1 were collected at 24 h after
irradiation. Irradiated cell lysates were collected at 4, 8, 16, 24
and 48 h after irradiation and subjected to immunoblotting.
Immunoblotting
Whole cell lysates from sham and irradiated cell
lines were prepared using RIPA cell lysis buffer were briefly
sonicated, at 20 kHz on ice for 30 sec, using an ultrasonic
sonicator (Thermo Fisher Scientific, Inc.). Protein concentrations
were quantified using the bicinchoninic acid (BCA) method. Next,
the proteins in the lysates were separated using 10% gel SDS-PAGE
electrophoresis and then electrophoretically transferred onto
nitrocellulose membranes, which were probed with the aforementioned
antibodies listed above at 4°C overnight. GAPDH served as a loading
control. Immunocomplexes were detected using secondary antibodies
conjugated to horseradish peroxidase for 1 h at room temperature,
and a western blot imaging system (Synoptics Ltd) that employs ECL
(Immobilon Forte Western HRP substrate; Merck KGaA) was used to
visualize the bands. Densitometry was determined using ImageJ
version 1.53 g (National Institutes of Health). Immunoblotting was
performed in triplicate.
Patients and sample preparation
Patients diagnosed with cervical cancer (n=153) who
underwent initial external beam radiation therapy (EBRT) between
April 2014 and August 2017 at the Department of Radiation Oncology,
Chulabhorn Hospital (Bangkok, Thailand), were considered for
inclusion in the present study. The inclusion criteria were as
follows: i) Patients pathologically diagnosed with cervical cancer
[stages IB-IVA according to the International Federation of
Gynecology and Obstetrics (FIGO) 2009] (21), ii) tissue specimens collected at
baseline (before treatment with EBRT) and during radiotherapy
(before 1st brachytherapy), and iii) clinical data available at
initial diagnosis. The exclusion criteria were incomplete sample
collection and inadequate amount of tissue sample. The inclusion
criteria were met by 72 patients who were included in the data
analyses. The primary outcomes of the study were 5-year
disease-free survival rate (DFS) and 5-year overall survival rate
(OS), defined as the date of radiation therapy until April 2020.
DFS refers to patients who survived without signs or recurrence of
cervical cancer, and OS refers to those who survived until April
2020. The follow-up was performed at the Department of Radiation
Oncology, Chulabhorn Hospital. The patients were followed-up every
3 months after the completion of treatment in the first 2 years,
every 4 months in year 3–4 and every 6 months thereafter.
Tumor samples and ELISAs
Cervical tumor biopsies were obtained from patients
with their informed consent before their first radiation treatment
and during the 16th to 22nd fractions of EBRT at the conventional
dose of 2 Gy per fraction, before the first brachytherapy session.
Tumor tissue samples were stored at −80°C and then lysed with RIPA
lysis buffer and sonicated on ice at 40 kHz for one minute each.
ELISAs of uPA and uPAR levels were performed using human uPA and
uPAR kits (cat. nos. ab119611 and ab119612, respectively) in
accordance with the manufacturer's instructions (Abcam). Color
intensity at 450 nm was determined using an EnSight multimode plate
reader (PerkinElmer, Inc.). Each ELISA reaction included 40 µg of
tissue lysate. The concentrations of uPA and uPAR were calculated
according to standard curves. An increase of uPA and uPAR ≥1.0 ng
per 40 µg of total protein of irradiated vs pretreatment tissues
was defined as increased expression, and a reduction of uPA and
uPAR by ≥1.0 ng per 40 µg of total protein was defined as decreased
expression. ELISAs were performed in duplicate. The median levels
for uPA and uPAR pretreatment before and after completion of EBRT
were used as cut-off values for survival analysis. For uPA, the
median values were 2.64 ng and 1.79 ng/40 µg of tissue sample
protein for pretreatment and after EBRT, respectively. For uPAR,
the median values were 1.04 ng and 1.36 ng/40 µg of tissue sample
protein for pretreatment and after EBRT, respectively.
Statistical analysis
Continuous variables are presented the median and
range, and categorical variables are shown as frequencies and
percentages (unless otherwise shown). Statistical comparisons
between continuous variables were undertaken using one-way ANOVA
with Tukey's post hoc test. A paired t-test was used to compare
protein expression levels. DFS and OS were evaluated using the
Kaplan-Meier method with a log-rank test. The Cox proportional
hazards model was used for univariate analysis of covariates as
well as for multivariate analysis. P<0.05 was considered to
indicate a statistically significant difference. All statistical
analyses were performed using STATA version 12.1 software
(StataCorp LLC).
Results
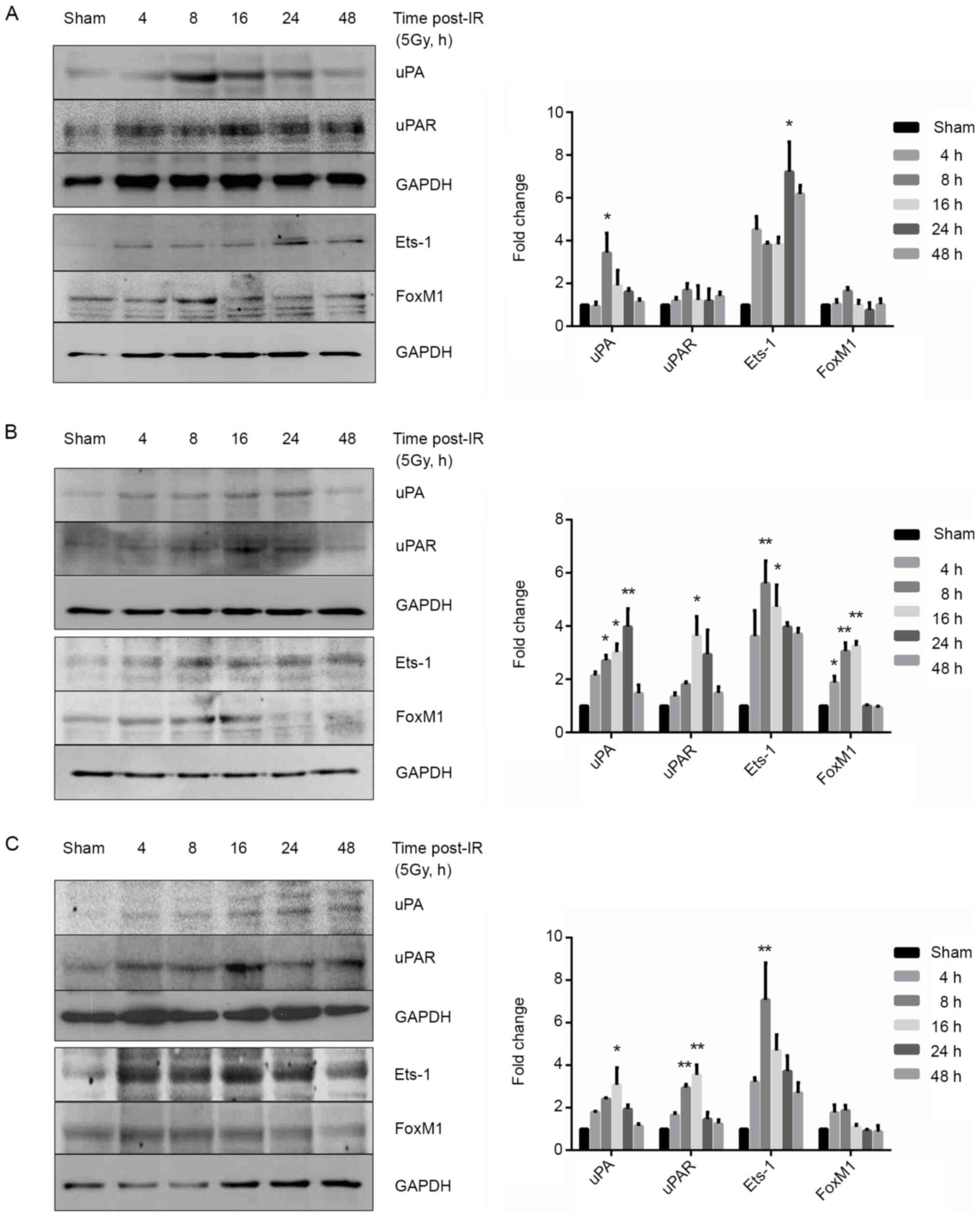
Exposure to ionizing radiation
upregulates uPA expression in cervical cancer cell lines
To determine whether the expression of uPA and its
receptor uPAR were regulated by ionizing radiation, the human
cervical cancer cell lines were irradiated (5 Gy) as follows: SiHa
(HPV16-Positive), HeLa (HPV18-positive) and C33A (HPV-negative). As
shown in Fig. 1, immunoblotting
analysis revealed that the expression of uPA and uPAR was increased
in irradiated cells after 8–24 h. uPA was significantly increased
at 8 h, 8–24 h and 16 h post-irradiation for SiHa, HeLa and C33A
cells, respectively. uPAR expression levels were significantly
upregulated at 8 h and 8–16 h after irradiation in HeLa and C33A
cells but not in SiHa cells. Radiation exposure also generally
increased the expression level of uPA-regulated transcription
factor Ets-1 in all three cell lines after 4–48 h, but only
significantly upregulated the protein after 24 h, 8–16 h and 8 h
for SiHa, HeLa and C33A cells, respectively. Furthermore, the
uPAR-regulated transcription factor FoxM1 was significantly
upregulated by ionizing radiation in HeLa cells after 8–16 h, but
not in the other cell lines.
Patient characteristics and responses
to treatment
It was next determined whether the expression of uPA
and uPAR was upregulated in patients receiving radiotherapy.
Patient demographic data are shown in Table I. Their mean age was 53.5 years
(range, 25–85 years), 73.61% had squamous cell carcinoma (38.89%
with FIGO Stage IIB). In total, ~67% of patients were HPV-positive,
76.39% received concurrent chemoradiotherapy followed by
intracavitary radiotherapy, 65.28% were administered
cisplatin-based chemotherapy and 16.67% were administered
carboplatin. The patients received a median dose of 89.45 Gy
(equivalent dose2) with median radiation treatment for
43 days.
 | Table I.Characteristics of 72 patients with
cervical cancer. |
Table I.
Characteristics of 72 patients with
cervical cancer.
| Variables | Value |
|---|
| Age at diagnosis,
median (range) years | 53.5 (25–85) |
| Histological type,
n (%) |
|
|
Squamous cell carcinoma | 53 (73.61) |
|
Neuroendocrine carcinoma | 4 (5.55) |
|
Adenosquamous carcinoma | 12 (16.67) |
|
Adenocarcinoma | 3 (4.17) |
| FIGO staging, n
(%) |
|
| IB2-
IIA | 17 (23.61) |
|
IIB | 28 (38.89) |
|
IIIA-IIIB | 25 (34.72) |
|
IVA | 2 (2.78) |
| HPV status, n
(%) |
|
|
Negative | 8 (11.11) |
|
Positive | 48 (66.67) |
| Not
available | 16 (22.22) |
| Treatment, n
(%) |
|
| CCRT +
ICRT | 55 (76.39) |
| CCRT +
ICRT + Adjuvant treatment | 13 (18.06) |
| EBRT +
ICRT | 3 (4.17) |
| EBRT +
ICRT + Adjuvant treatment | 1 (1.39) |
| Chemotherapy
regimen, n (%) |
|
| No
chemotherapy | 4 (5.56) |
|
Cisplatin | 47 (65.28) |
|
Carboplatin | 12 (16.67) |
|
Combination | 9 (12.50) |
| Number of days for
radiation treatments, median (range) days | 43 (12–87) |
| EBRT +
Brachytherapy, median (range), Gy | 89.45
(56–99.6) |
| ICRT course
fractions, range, days | 3–5 |
| Cycle of
chemotherapy, range, cycles | 0–7 |
| Technique of EBRT,
n (%) |
|
|
AP/PA | 21 (29.17) |
| 4-field
box | 44 (61.11) |
|
VMAT | 2 (2.78) |
|
Combination | 5 (6.94) |
All patients were treated and regularly underwent
follow-up examinations. As shown in Table II, ~70.8% experienced a complete
response (undetectable tumors) and the median survival time was 35
months (range, 2–60 months). Cervical tumor biopsies were performed
during their 16th to 22nd fractions of pelvic irradiation at the
conventional dose of 2 Gy per fraction, before the first
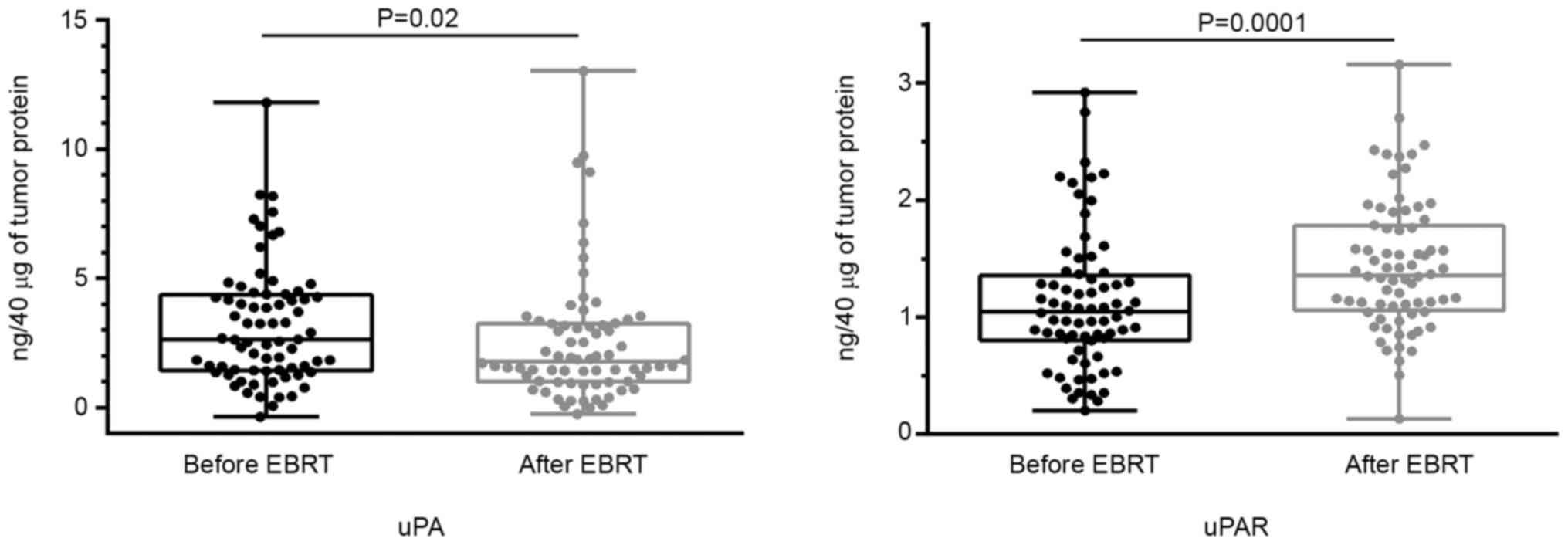
brachytherapy session. The uPA and uPAR levels remained largely
unchanged (47.22 and 79.17% of the patients, respectively), whereas
radiotherapy led to an increase in uPA and uPAR levels in 16.67 and
18.06% of patients, respectively. Furthermore, uPA and uPAR levels
in 36.11 and 2.78% decreased, respectively. For uPA, 34 patients
had no change in expression, 26 patients had decreased expression
and 12 patients had increased expression. For uPAR, 57 patients had
no change in expression, two patients had decreased expression and
13 patients had increased expression. These results showed that uPA
expression generally decreased after EBRT (P=0.02), although uPAR
expression increased (P=0.001) (Fig.
2). Notably, the changes in uPA and uPAR expression in
HPV-positive patients followed a similar trend (Fig. S1), suggesting that HPV plays a role
in the regulation of the expression of uPA and uPAR.
| Table II.Responses to treatment of 72 patients
with cervical cancer who underwent radiation therapy. |
Table II.
Responses to treatment of 72 patients
with cervical cancer who underwent radiation therapy.
| Variables | Value |
|---|
| Patient treatment
outcome, n (%) |
|
|
Survived | 59 (81.94) |
|
Deceased | 13 (18.06) |
|
Experienced recurrence | 4 (5.56) |
| Treatment response,
n (%) |
|
|
Complete response | 51 (70.83) |
| Partial
response | 8 (11.11) |
|
Progressive disease | 6 (8.33) |
|
N/A | 7 (9.72) |
| uPA levels, n
(%) |
|
| No
change | 34 (47.22) |
|
Decreased | 26 (36.11) |
|
Increased | 12 (16.67) |
| uPAR levels, n
(%) |
|
| No
change | 57 (79.17) |
|
Decreased | 2 (2.78) |
|
Increased | 13 (18.06) |
| Overall survival
time, median (range) months | 35 (2–60) |
Factors influencing therapeutic
outcome
The results shown in Table III indicated that treatment
response was a major predictive factor of outcomes. Among the 72
patients, 13 died, 59 survived and four experienced recurrence
(Table II). The DFS of patients
with progressive disease was significantly shorter (HR, 56.59; 95%
CI, 13.45–238.09) as well as their OS [HR, 13.41; 95% CI,
1.17–153.07 (univariate analysis); and HR, 47.16; 95% CI,
3.11–714.63 (multivariate analysis)]. The patients with a partial
response to therapy experienced shorter OS (HR, 7.22; 95% CI,
1.17–44.73).
| Table III.Univariate and multivariate Cox
proportional hazard regression analyses of DFS and OS. |
Table III.
Univariate and multivariate Cox
proportional hazard regression analyses of DFS and OS.
|
| DFS | OS |
|---|
|
|
|
|
|---|
|
| Univariate
analysis | Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|
|---|
| Variable | HR (95% CI) | P-value | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age, years |
|
|
|
|
|
|
|
≤50 | Ref. | – | Ref. | – |
|
|
|
>50 | 0.58
(0.22–1.49) | 0.256 | 0.81
(0.27–2.42) | 0.707 |
|
|
| FIGO stage |
|
|
|
|
|
|
| IB2-
IIA | Ref. | – | Ref. | – |
|
|
|
IIB | 2.25
(0.47–10.83) | 0.312 | 1.48
(0.29–7.66) | 0.637 |
|
|
|
IIIA-IIIB | 3.25
(0.67–15.70) | 0.142 | 2.93
(0.59–14.62) | 0.190 |
|
|
|
IVA | 6.37
(0.58–70.55) | 0.131 | 0.00 | >0.999 |
|
|
| Histological
type |
|
|
|
|
|
|
|
Squamous cell carcinoma | Ref. | – | Ref. |
|
|
|
|
Neuroendocrine carcinoma | 1.23
(0.16–9.59) | 0.840 | 0.00 | >0.999 |
|
|
|
Other | 1.66
(0.57–4.78) | 0.351 | 1.70
(0.52–5.55) | 0.379 |
|
|
| Treatment
response |
|
|
|
| Ref. | – |
|
Complete | Ref. | – | Ref. | – | 6.07
(0.90–41.10) | 0.064 |
|
Partial | 2.41
(0.50–11.66) | 0.273 | 7.22
(1.17–44.73) | 0.034 | 47.16
(3.11–714.63) | 0.005 |
|
Progressive disease | 56.59
(13.45–238.09) | <0.001 | 13.41
(1.17–153.07) | 0.037 | 58.58
(11.47–299.34 | <0.001 |
|
N/A | 3.68
(0.76–17.92) | 0.107 | 40.97
(9.27–181.04) | <0.001 |
|
|
| uPA levels |
|
|
|
|
|
|
| No
change | Ref. | – | Ref. | – |
|
|
|
Decreased | 0.54
(0.16–1.74) | 0.299 | 0.93
(0.25–3.48) | 0.918 |
|
|
|
Increased | 1.39
(0.43–4.53) | 0.585 | 2.68
(0.71–10.06) | 0.145 |
|
|
| uPAR levels |
|
|
|
|
|
|
| No
change | Ref. | – | Ref. | – | Ref. | – |
|
Decreased | 2.32
(0.30–17.76) | 0.419 | 0.00 | >0.999 | 0.00 | >0.999 |
|
Increased | 1.12
(0.32–3.96) | 0.855 | 3.65
(1.18–11.30) | 0.025 | 6.72
(1.71–26.37) | 0.006 |
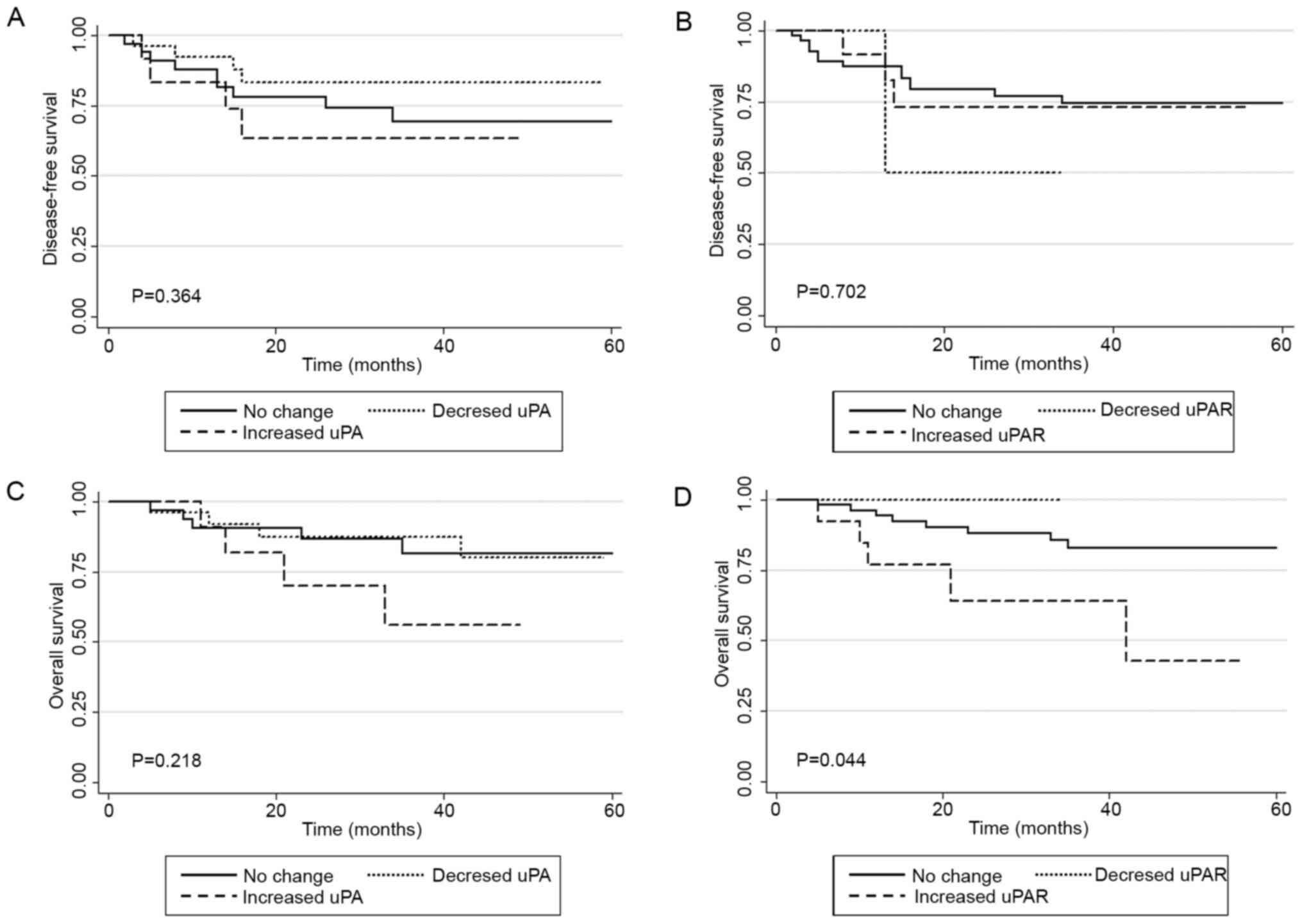
Although the level of uPA expression was not
significantly associated with OS (HR, 2.68; 95% CI, 0.71–10.06),
increased uPAR expression was predictive. Univariate and
multivariate analyses indicated that the upregulation of uPAR
levels in cervical tumor tissue may serve as a prognostic factor
for predicting OS [HR, 3.65; 95% CI, 1.18–11.30 (univariate
analysis); and HR, 6.72; 95% CI, 1.71–26.37 (multivariate
analysis)]. The data shown in Fig. 3
support the conclusion that increased uPAR expression may serve as
a prognostic factor for OS but not DFS. Neither the absolute levels
of expression nor the differences of either protein were a
significant predictor of DFS. Together, these findings supported
the conclusion that the levels of uPA and uPAR before and after
EBRT were not significantly associated with DFS or OS (Figs. S2–5).
Discussion
Irradiation of tumor cells activates numerous genes
encoding products that contribute to tumor invasion and metastasis,
which frequently shortens survival time (22). For example, irradiation activates uPA
and uPAR expression and causes meningiomas to grow in vivo
(23). Consistent with these
findings, the present in vitro data showed that uPA and uPAR
expression was upregulated by radiation, which may be explained by
their transcriptional activation by Ets-1 and FoxM1, respectively
(10,24). Radiation-induced activation of NF-ĸB
activation may account for upregulation of uPA and uPAR as well
(25,26). In contrast to this, the current data
acquired using tumor samples differed from these results regarding
uPA expression, particularly because the protocol mimicked that
employed in the clinic (five fractions per week). This may be
attributed to the presence of HPV, which confers radiosensitivity
(27), and patients who were
HPV-positive appeared to have reduced uPA levels but enhanced uPAR
levels after receiving radiotherapy. The HPV E6 oncoprotein targets
and reduces the expression of microRNA (miR)- (miR-23b) and
miR-34a, which negatively regulates uPA expression (18,28,29).
These miRs are induced in irradiated tumor tissue samples (30,31).
Thus, fractionated irradiation may enhance miR-23b and miR-34a
expression and subsequently downregulate uPA expression.
HPV status and genotypes may affect the outcome of
treatment because the prognosis of patients who are HPV-negative
with cervical cancer is worse compared with those with HPV
infection (32). Furthermore, HPV
titers may predict the radiation response of cervical tumors
(33). Similarly, HPV-positive head
and neck tumors are more sensitive to conventional radiation or
chemo- therapies (34,35). Higher radiosensitivity is caused by
defective DNA damage repair, particularly due to double-stand
breaks (36). An improved
understanding of the interactions between HPV and therapeutics will
hopefully contribute to the development of optimal individualized
treatments. Another plausible reason for the downregulation of uPA
after EBRT is activation of c-Myc by radiation (37,38).
Although the expression of uPA and PAI-1 in cervical
tumor tissue was previously suggested to serve as a prognostic
marker for stage II cervical cancer (19), the induced expression of uPA in
response to radiotherapy was not significantly related to a patient
DFS or OS in the present study. Furthermore, the level of uPA in
cervical tumor tissue has little prognostic value (39). Nevertheless, evidence indicates that
the urokinase system is closely associated with stem cell-like
properties of numerous types of cancer cell, such as activated
STAT3 in lung cancer and CD24−/CD44+ breast
cancer (40). Accumulating evidence
also indicates an association between the urokinase system and EMT,
involving tumor cell depolarization into a mesenchymal phenotype
characterized by high motility and enhanced resistance to cell
death (41). Inhibition or
downregulation of uPA, uPAR or both, inhibits hypoxia-mediated EMT
(42). Additionally, uPA is known
for its functions in tumor cell invasion, its involvement in TGF-β
activation as well as its participation in EMT (43). Thus, uPA may contribute to the
formation of distant metastasis and the characteristics of the
tumor microenvironment, which further studies should be looking
into.
The present study demonstrated that uPAR expression
may serve to predict prognosis because of its contributions to
metastasis and cell survival through expression of mesenchymal
genes (44). Furthermore, uPAR
affects DNA damage repair through activation of Chk1 and Rad51 and
contributes to multidrug resistance mechanisms through its
interaction with proteins such as vitronectin, integrins and EGFR
(45,46). The current study further highlights
that increased expression of uPAR in cervical tumor tissue,
particularly during treatment, may serve as a prognostic factor
that predicts survival. In accordance with the present findings,
circulating soluble uPAR serves as a marker for diagnosis and
prognosis of cervical cancer (47).
Thus, uPAR should be considered a marker for predicting the
prognosis of patients with cervical cancer as serum levels of uPAR
are associated with treatment outcomes of patients with breast,
colon, rectal and ovarian cancer (48,49).
Acquiring post-EBRT tissue biopsies is relatively invasive, and
future studies should focus on determining whether less invasive
assays, such as those that measure serum uPAR, are as sensitive and
specific as those that measure tissue uPAR. The lack of serum uPA
and uPAR level measurements is a potential limitation of the
current study. In the meantime, for those patients who poorly
respond to radiotherapy, the authors hypothesize that post-EBRT
biopsies can be used to determine the levels of uPAR as well as
those of other prognostic markers. uPAR should therefore be
considered to select the most effective treatment strategy.
The current study reported that the expression of
uPA and uPAR was unsuitable as a prognostic marker for patients
with cervical cancer, which may be explained by the proteolytic
activities of uPA and uPAR that are often associated with tumor
cell migration and metastasis, which then contributed to a
radioresistant phenotype (50). In
contrast to this, uPAR expression may reflect the induction of the
epithelial mesenchymal transition (EMT) upon activation of the
ERK1/2 signaling pathway (51).
Nevertheless, the results were based on the limited availability of
number of patients (n=72) who underwent EBRT and were voluntary to
participate in the study. Several other factors should be
considered when comparing the results from different studies, such
as genotype and HPV status. A larger number of subjects will
therefore be required to validate the present findings.
With the emergence of high-throughput sequencing and
advances in bioinformatics, computational methods are used to
analyze genotypes, transcriptomes, proteomes and metabolomes to
identify specific diagnostic and prognostic markers of cancer
(52). For example, a mutation
profiling study found that mutations in the gene encoding
fibroblast growth factor receptor are associated with poor
progression-free survival rate in patients with cervical cancer
(53). System biology approaches may
therefore prove useful and provide new directions in the pursuit of
identifying new markers for cancer diagnosis and therapy.
In summary, although the expression levels of uPA
and uPAR were altered by irradiation, only the upregulation in uPAR
expression in tissue samples predicted the OS of patients with
cervical cancer. Targeting uPAR expressed in cervical tumors may
therefore contribute to more effective therapeutic strategies.
Supplementary Material
Supporting Data
Acknowledgments
The authors would like to thank Mr Chirasak
Khamfongkhruea, Mr Saengutid Thongsawad, Mr Kittipol Dachaworakul
and Dr Nuttavut Kantathavorn (all Faculty of Medicine and Public
Health, Chulabhorn Royal Academy) for assistance in conducting the
study, Dr Kamonwan Soonklang (Department of Research Innovation and
International Relations, HRH Princess Chulabhorn College of Medical
Science) for assistance in conducting the statistical analyses and
Dr Steven Tronick (Edanz Group) for editing a draft of this
manuscript.
Funding
This study was supported by Chulabhorn Royal Academy
granted to KL.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author upon reasonable
request.
Authors' contributions
DN conceptualized the study and wrote the
manuscript. DN, SC and KL designed the study. DN and PC performed
the in vitro experiments and collected the data. PC, SB and
SC collected and evaluated the clinical data and conducted the
statistical analyses. DN and SC confirmed the authenticity of the
raw data. SC and KL supervised the study and revised the
manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The Committee on Human Rights Related to Research
Involving Human Subjects, Chulabhorn Research Institute, (Bangkok,
Thailand) approved the study (approval no. 04/2557). Written
informed consent was provided by each patient.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Gatenby RA, Silva AS, Gillies RJ and
Frieden BR: Adaptive therapy. Cancer Res. 69:4894–4903. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ahmed KM and Li JJ: NF-kappa B-mediated
adaptive resistance to ionizing radiation. Free Radic Biol Med.
44:1–13. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Roos WP, Thomas AD and Kaina B: DNA damage
and the balance between survival and death in cancer biology. Nat
Rev Cancer. 16:20–33. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Duffy MJ, Maguire TM, McDermott EW and
O'Higgins N: Urokinase plasminogen activator: A prognostic marker
in multiple types of cancer. J Surg Oncol. 71:130–135. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Gonias SL and Hu J: Urokinase receptor and
resistance to targeted anticancer agents. Front Pharmacol.
6:1542015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Mahmood N, Mihalcioiu C and Rabbani SA:
Multifaceted role of the urokinase-type plasminogen activator (uPA)
and its receptor (uPAR): Diagnostic, prognostic, and therapeutic
applications. Front Oncol. 8:242018. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ulisse S, Baldini E, Sorrenti S and
D'Armiento M: The urokinase plasminogen activator system: A target
for anti-cancer therapy. Curr Cancer Drug Targets. 9:32–71. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Watabe T, Yoshida K, Shindoh M, Kaya M,
Fujikawa K, Sato H, Seiki M, Ishii S and Fujinaga K: The Ets-1 and
Ets-2 transcription factors activate the promoters for
invasion-associated urokinase and collagenase genes in response to
epidermal growth factor. Int J Cancer. 77:128–137. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lund IK, Nielsen BS, Almholt K, Rono B,
Hald A, Illemann M, Green KA, Christensen IJ, Romer J and Lund LR:
Concomitant lack of MMP9 and uPA disturbs physiological tissue
remodeling. Dev Biol. 358:56–67. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Li D, Wei P, Peng Z, Huang C, Tang H, Jia
Z, Cui J, Le X, Huang S and Xie K: The critical role of
dysregulated FOXM1-PLAUR signaling in human colon cancer
progression and metastasis. Clin Cancer Res. 19:62–72. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Blasi F and Sidenius N: The urokinase
receptor: Focused cell surface proteolysis, cell adhesion and
signaling. FEBS Lett. 584:1923–1930. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kugaevskaya EV, Gureeva TA, Timoshenko OS
and Solovyeva NI: The urokinase-type plasminogen activator system
and its role in tumor progression. Biomed Khim. 64:472–486. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Su SC, Lin CW, Yang WE, Fan WL and Yang
SF: The urokinase-type plasminogen activator (uPA) system as a
biomarker and therapeutic target in human malignancies. Expert Opin
Ther Targets. 20:551–566. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Harbeck N, Schmitt M, Meisner C, Friedel
C, Untch M, Schmidt M, Sweep CG, Lisboa BW, Lux MP, Beck T, et al:
Ten-year analysis of the prospective multicentre Chemo-N0 trial
validates American society of clinical oncology (ASCO)-recommended
biomarkers uPA and PAI-1 for therapy decision making in
node-negative breast cancer patients. Eur J Cancer. 49:1825–1835.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Small W Jr, Bacon MA, Bajaj A, Chuang LT,
Fisher BJ, Harkenrider MM, Jhingran A, Kitchener HC, Mileshkin LR,
Viswanathan AN and Gaffney DK: Cervical cancer: A global health
crisis. Cancer. 123:2404–2412. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
de Sanjose S, Quint WG, Alemany L, Geraets
DT, Klaustermeier JE, Lloveras B, Tous S, Felix A, Bravo LE, Shin
HR, et al: Human papillomavirus genotype attribution in invasive
cervical cancer: A retrospective cross-sectional worldwide study.
Lancet Oncol. 11:1048–1056. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Machalek DA, Roberts JM, Garland SM,
Thurloe J, Richards A, Chambers I, Sivertsen T and Farnsworth A:
Routine cervical screening by primary HPV testing: Early findings
in the renewed National cervical screening program. Med J Aust.
211:113–119. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Au Yeung CL, Tsang TY, Yau PL and Kwok TT:
Human papillomavirus type 16 E6 induces cervical cancer cell
migration through the p53/microRNA-23b/urokinase-type plasminogen
activator pathway. Oncogene. 30:2401–2410. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kobayashi H, Fujishiro S and Terao T:
Impact of urokinase-type plasminogen activator and its inhibitor
type 1 on prognosis in cervical cancer of the uterus. Cancer Res.
54:6539–6548. 1994.PubMed/NCBI
|
|
20
|
Sugimura M, Kobayashi H, Kanayama N and
Terao T: Clinical significance of urokinase-type plasminogen
activator (uPA) in invasive cervical cancer of the uterus. Gynecol
Oncol. 46:330–336. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Pecorelli S: Revised FIGO staging for
carcinoma of the vulva, cervix, and endometrium. Int J Gynaecol
Obstet. 105:103–104. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Lee SY, Jeong EK, Ju MK, Jeon HM, Kim MY,
Kim CH, Park HG, Han SI and Kang HS: Induction of metastasis,
cancer stem cell phenotype, and oncogenic metabolism in cancer
cells by ionizing radiation. Mol Cancer. 16:102017. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kargiotis O, Chetty C, Gogineni V, Gondi
CS, Pulukuri SM, Kyritsis AP, Gujrati M, Klopfenstein JD, Dinh DH
and Rao JS: uPA/uPAR downregulation inhibits radiation-induced
migration, invasion and angiogenesis in IOMM-Lee meningioma cells
and decreases tumor growth in vivo. Int J Oncol. 33:937–947.
2008.PubMed/NCBI
|
|
24
|
Nakada M, Yamashita J, Okada Y and Sato H:
Ets-1 positively regulates expression of urokinase-type plasminogen
activator (uPA) and invasiveness of astrocytic tumors. J
Neuropathol Exp Neurol. 58:329–334. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Qu M, Yu J, Liu H, Ren Y, Ma C, Bu X and
Lan Q: The candidate tumor suppressor gene SLC8A2 inhibits
invasion, angiogenesis and growth of glioblastoma. Mol Cells.
40:761–772. 2017.PubMed/NCBI
|
|
26
|
Reuning U, Wilhelm O, Nishiguchi T,
Guerrini L, Blasi F, Graeff H and Schmitt M: Inhibition of NF-kappa
B-Rel A expression by antisense oligodeoxynucleotides suppresses
synthesis of urokinase-type plasminogen activator (uPA) but not its
inhibitor PAI-1. Nucleic Acids Res. 23:3887–3893. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Mesher D, Cuschieri K, Hibbitts S, Jamison
J, Sargent A, Pollock KG, Powell N, Wilson R, McCall F, Fiander A
and Soldan K: Type-specific HPV prevalence in invasive cervical
cancer in the UK prior to national HPV immunisation programme:
Baseline for monitoring the effects of immunisation. J Clin Pathol.
68:135–140. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Pang RT, Leung CO, Ye TM, Liu W, Chiu PC,
Lam KK, Lee KF and Yeung WS: MicroRNA-34a suppresses invasion
through downregulation of Notch1 and Jagged1 in cervical carcinoma
and choriocarcinoma cells. Carcinogenesis. 31:1037–1044. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Wang X, Wang HK, McCoy JP, Banerjee NS,
Rader JS, Broker TR, Meyers C, Chow LT and Zheng ZM: Oncogenic HPV
infection interrupts the expression of tumor-suppressive miR-34a
through viral oncoprotein E6. RNA. 15:637–647. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Lacombe J and Zenhausern F: Emergence of
miR-34a in radiation therapy. Crit Rev Oncol Hematol. 109:69–78.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Li B, Sun M, Gao F, Liu W, Yang Y, Liu H,
Cheng Y, Liu C and Cai J: Up-regulated expression of miR-23a/b
targeted the pro-apoptotic Fas in radiation-induced thymic
lymphoma. Cell Physiol Biochem. 32:1729–1740. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Harima Y, Sawada S, Nagata K, Sougawa M
and Ohnishi T: Human papilloma virus (HPV) DNA associated with
prognosis of cervical cancer after radiotherapy. Int J Radiat Oncol
Biol Phys. 52:1345–1351. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Datta NR, Kumar P, Singh S, Gupta D,
Srivastava A and Dhole TN: Does pretreatment human papillomavirus
(HPV) titers predict radiation response and survival outcomes in
cancer cervix?-A pilot study. Gynecol Oncol. 103:100–105. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Gottgens EL, Ostheimer C, Span PN, Bussink
J and Hammond EM: HPV, hypoxia and radiation response in head and
neck cancer. Br J Radiol. 92:201800472019.PubMed/NCBI
|
|
35
|
Nagel R, Martens-de Kemp SR, Buijze M,
Jacobs G, Braakhuis BJ and Brakenhoff RH: Treatment response of
HPV-positive and HPV-negative head and neck squamous cell carcinoma
cell lines. Oral Oncol. 49:560–566. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Rieckmann T, Tribius S, Grob TJ, Meyer F,
Busch CJ, Petersen C, Dikomey E and Kriegs M: HNSCC cell lines
positive for HPV and p16 possess higher cellular radiosensitivity
due to an impaired DSB repair capacity. Radiother Oncol.
107:242–246. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Alfano D, Votta G, Schulze A, Downward J,
Caputi M, Stoppelli MP and Iaccarino I: Modulation of cellular
migration and survival by c-Myc through the downregulation of
urokinase (uPA) and uPA receptor. Mol Cell Biol. 30:1838–1851.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Sawey MJ, Hood AT, Burns FJ and Garte SJ:
Activation of c-myc and c-K-ras oncogenes in primary rat tumors
induced by ionizing radiation. Mol Cell Biol. 7:932–935. 1987.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Horn LC, Pippig S, Raptis G, Fischer U,
Kohler U, Hentschel B and Martin R: Clinical relevance of
urokinase-type plasminogen activator and its inhibitor type 1
(PAI-1) in squamous cell carcinoma of the uterine cervix. Aust N Z
J Obstet Gynaecol. 42:383–386. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Jo M, Eastman BM, Webb DL, Stoletov K,
Klemke R and Gonias SL: Cell signaling by urokinase-type
plasminogen activator receptor induces stem cell-like properties in
breast cancer cells. Cancer Res. 70:8948–8958. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Madunic J: The urokinase plasminogen
activator system in human cancers: An overview of its prognostic
and predictive role. Thromb Haemost. 118:2020–2036. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Gupta R, Chetty C, Bhoopathi P, Lakka S,
Mohanam S, Rao JS and Dinh DE: Downregulation of uPA/uPAR inhibits
intermittent hypoxia-induced epithelial-mesenchymal transition
(EMT) in DAOY and D283 medulloblastoma cells. Int J Oncol.
38:733–744. 2011.PubMed/NCBI
|
|
43
|
Santibanez JF, Obradovic H, Kukolj T and
Krstic J: Transforming growth factor-β, matrix metalloproteinases,
and urokinase-type plasminogen activator interaction in the cancer
epithelial to mesenchymal transition. Dev Dyn. 247:382–395. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Gilder AS, Natali L, Van Dyk DM, Zalfa C,
Banki MA, Pizzo DP, Wang H, Klemke RL, Mantuano E and Gonias SL:
The urokinase receptor induces a mesenchymal gene expression
signature in glioblastoma cells and promotes tumor cell survival in
Neurospheres. Sci Rep. 8:29822018. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Narayanaswamy PB, Tkachuk S, Haller H,
Dumler I and Kiyan Y: CHK1 and RAD51 activation after DNA damage is
regulated via urokinase receptor/TLR4 signaling. Cell Death Dis.
7:e23832016. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Wang K, Xing ZH, Jiang QW, Yang Y, Huang
JR, Yuan ML, Wei MN, Li Y, Wang ST, Liu K and Shi Z: Targeting uPAR
by CRISPR/Cas9 system attenuates cancer malignancy and multidrug
resistance. Front Oncol. 9:802019. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Jing J, Zheng S, Han C, Du L, Guo Y and
Wang P: Evaluating the value of uPAR of serum and tissue on
patients with cervical cancer. J Clin Lab Anal. 26:16–21. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Duffy MJ and Duggan C: The urokinase
plasminogen activator system: A rich source of tumour markers for
the individualised management of patients with cancer. Clin
Biochem. 37:541–548. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Wang L, Yang R, Zhao L, Zhang X, Xu T and
Cui M: Basing on uPAR-binding fragment to design chimeric antigen
receptors triggers antitumor efficacy against uPAR expressing
ovarian cancer cells. Biomed Pharmacother. 117:1091732019.
View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Pavon MA, Arroyo-Solera I, Cespedes MV,
Casanova I, Leon X and Mangues R: uPA/uPAR and SERPINE1 in head and
neck cancer: Role in tumor resistance, metastasis, prognosis and
therapy. Oncotarget. 7:57351–57366. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Wang P, Ma M and Zhang S: EGF-induced
urokinase plasminogen activator receptor promotes epithelial to
mesenchymal transition in human gastric cancer cells. Oncol Rep.
38:2325–2334. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Manzoni C, Kia DA, Vandrovcova J, Hardy J,
Wood NW, Lewis PA and Ferrari R: Genome, transcriptome and
proteome: The rise of omics data and their integration in
biomedical sciences. Brief Bioinform. 19:286–302. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Yoshimoto Y, Sasaki Y, Murata K, Noda SE,
Miyasaka Y, Hamamoto J, Furuya M, Hirato J, Suzuki Y, Ohno T, et
al: Mutation profiling of uterine cervical cancer patients treated
with definitive radiotherapy. Gynecol Oncol. 159:546–553. 2020.
View Article : Google Scholar : PubMed/NCBI
|