Introduction
Malignant tumors of the breast generally occur in
the ductal or acinar epithelium. Because of its high morbidity and
high mortality, breast cancer is a major disease that seriously
impacts on the lives and health of men and women worldwide
(1). Surgery is one of the most
important treatment options for breast cancer since it is
frequently used for breast cancer therapy (2). Although this method can cause
deformity or even loss of the breasts of the patient, which can
have a great impact on their physical and mental health.
Chemotherapy is a reliable method for the treatment of breast
malignant tumors. However, multi-drug resistance and metastasis of
tumor cells has narrowed the scope of clinical application of
chemotherapy drugs to a certain extent (3). Therefore, finding drugs with good
curative and anti-metastatic effects in breast cancer has become
the focus of breast cancer research.
With the rapid development of life science research,
the basic processes of tumor cell signal transduction, cell cycle
regulation, apoptosis induction and angiogenesis are gradually
being elucidated. Vascular endothelial growth factor receptor
(VEGFR) signaling has been identified to play a pivotal role in the
regulation of neo-angiogenesis, the process that leads to the
formation of new blood vessels from the existing vasculature and
that is crucial for tumor growth, invasion and metastasis (4). Therefore, VEGFR has become an
important candidate in anti-tumor drug research and a potential
target in drug research and development. Drugs directed against the
VEGF/VEGFR system can be mainly categorized into two classes,
monoclonal antibodies and small-molecule tyrosine kinase inhibitors
(TKIs). Since 2018, >20 TKIs have been approved by the Food and
Drug Administration (5). These
drugs are characterized by high selectivity, high efficacy and low
side effects. They are superior to traditional cytotoxicity
anti-tumor drugs in the treatment of various cancer types, and some
have become first-line drugs for cancer treatment (6).
Anlotinib is a novel multi-kinase inhibitor that has
exhibited efficacy against various types of malignancies in
preclinical models, including medullary thyroid cancer, renal cell
cancer, gastric cancer and esophageal squamous cell carcinoma
(7). It is designed to primarily
inhibit VEGFR, platelet-derived growth factor receptors α and β,
fibroblast growth factor receptors, c-Kit and RET (8). Anlotinib is currently undergoing
phase-II and/or -III clinical development in China, the USA and
Italy for soft tissue sarcomas and various cancer types, such as
lung cancer, gastric cancer and thyroid cancer (9,10).
Another small-molecule TKI that selectively blocks VEGFR-2,
Vandetanib, has been approved for use in 2012 for advanced thyroid
cancer and was reported to inhibit cell growth and angiogenesis in
breast cancer cells (11).
Moreover, the effect of Vandetanib on the proliferation and tumor
growth response of breast cancer cells was dependent on
transcription factor AP-2γ (TFAP2C) expression (12). A recent study has demonstrated that
Anlotinib has good efficacy and low toxicity in a phase-II study
evaluating Anlotinib in pre-treated HER-2 negative metastatic
breast cancer (13). Additionally,
Zhang et al (14) suggested
that Anlotinib combined with neoadjuvant chemotherapy had good
efficacy and safety in the treatment of occult breast cancer and
may represent a potential therapeutic option. TFAP2C is a member of
the AP-2 transcription factor family, which has been shown to play
a critical role in multiple subtypes of breast cancer (15). In breast cancer, data mining of
microarray expression studies has shown an association between high
levels of TFAP2C mRNA and higher clinical grade and shorter
survival times (16,17). However, the effects of Anlotinib on
TFAP2C on the progression of breast cancer remain to be elucidated.
The aim of the present study was to explore the antitumor effect
and mechanism of action of Anlotinib in the human breast cancer
cell line MCF-7. Whether Anlotinib could inhibit MCF-7 cell
proliferation and migration by regulating TFAP2C expression was
also explored.
Materials and methods
Cell culture and treatment
The human breast cancer cell line MCF-7 was
purchased from the American Type Culture Collection and cultured in
RPMI-1640 medium supplemented with 10% FBS and 1% penicillin and
streptomycin at 37°C with 5% CO2 (all from Gibco; Thermo
Fisher Scientific, Inc.).
Cell transfection
The full length of the TFAP2C sequence was cloned
into the pcDNA3.1 vector by Gene Script Biotech Co., Ltd. to
construct 2 µg TFAP2C overexpression vector (Ov-TFAP2C). The empty
vector pcDNA3.1 (2 µg) was used as a negative control (Ov-NC).
Cells were cultured overnight to reach 60–70% confluence before
transfection. The plasmid transfection was performed using
Lipofectamine® 2000 (Invitrogen; Thermo Fisher
Scientific, Inc.) according to the manufacturer's instructions.
Cells were incubated with 5% CO2 at 37°C and were used
in subsequent experiments 48 h post-transfection.
Cell viability measurement
Cell viability was measured using Cell Counting
Kit-8 (CCK-8; Beyotime Institute of Biotechnology) assays. Control
or transfected MCF-7 cells were seeded in 96-well plates at
5×103 cells/well and incubated at 37°C for 24 h. The
cells were the treated with different concentrations of Anlotinib
(0, 2, 4 and 6 µM; >99%; Selleck Chemicals) at 37°C for 24 h. A
total of 10 µl CCK-8 solution was added to each well for 2 h of
culture at 37°C. Cell viability was detected using a microplate
reader (Bio-Rad Laboratories, Inc.) at the absorbance of 450
nm.
Colony formation assay
For colony formation assays, control or transfected
MCF-7 cells (1×103 cells) were resuspended in 1 ml
medium, then cultured in 24-well plates overnight. The attached
cells were treated with Anlotinib (0, 2, 4 and 6 µM) at 37°C for 24
h, then cultured in complete RPMI-1640 medium for an additional 2
weeks. After fixation with 20% methanol for 30 min at room
temperature, 0.5% crystal violet was used to stain cells for 5 min
at room temperature and the number of colonies with >50 cells
was counted manually using a light microscope (magnification,
×100).
Wound healing assay
Control or transfected MCF-7 cells were seeded onto
6-well plates (4×105 cells/well) and cultured in normal
conditions to 70–80% confluence. The cell surface was scratched
with a 100-µl pipette tip to create an artificial wound, and the
medium was replaced with serum-free RPMI-1640 containing Anlotinib
(0, 2, 4 and 6 µM) and culturing for 24 h at 37°C. The cell
migration was observed with images captured in each group at 0 and
24 h using a light microscope (magnification, ×100; Olympus
Corporation). The cell migration rate was calculated using the
following equation: (Initial width at 0 h - final width at 24
h)/Initial width at 0 h. The relative migration rate was obtained
by normalizing to the control group.
Transwell assay
For Transwell analysis, an 8-µm Transwell chamber
(Corning, Inc.) was coated with 250 mg/ml Matrigel™ (BD
Biosciences) at room temperature for 24 h (18–20),
then placed into a 24-well plate. The upper chambers were seeded
with control or transfected MCF-7 cells suspended in 200 µl
serum-free DMEM at a density of 1×105 following
Anlotinib treatment. RPMI-1640 medium containing 10% FBS was added
to the lower chamber for 24 h of incubation at 37°C. Finally, the
invading cells into the bottom of chamber were fixed with 4%
methanol at 37°C for 10 min, then stained with 0.1% crystal violet
solution at 37°C for 15 min. The number of invasive cells in five
random fields were counted using a light microscope (magnification,
×100).
TUNEL staining
Cell apoptosis was detected using the TUNEL assay
kit (Abcam) following the manufacturer's instructions. The control
or transfected MCF-7 cells were fixed with 1% paraformaldehyde at
room temperature for 15 min after Anlotinib treatment, and then
treated with 70% ethanol on ice. After being exposed to the TUNEL
detection reagent for 1 h at 37°C, cells were treated with 10 µg/ml
DAPI (Shanghai Haoyang Bio Technology Co., Ltd.) to stain the
nucleus at 37°C for 2–3 min and mounted in an anti-fade reagent
(Beijing Solarbio Science & Technology Co., Ltd.). In total,
three fields of view were selected at random, each with ~300–500
cells and the images were captured using a fluorescence microscope
(magnification, ×100; Olympus Corporation) and analyzed using the
ImageJ software (version 1.48v; National Institutes of Health).
Western blot analysis
Cells were lysed with RIPA buffer (Beyotime
Institute of Biotechnology) containing protease inhibitors (Roche
Diagnostics), and protein concentration was quantified using a
bicinchoninic-acid assay kit (Thermo Fisher Scientific, Inc.).
Equal amount of protein samples (20 µg) were separated 12% SDS-PAGE
on 12% gels, then transferred onto PVDF membranes (EMD Millipore).
After being blocked with 5% non-fat milk for 2 h at room
temperature (diluted with PBS-0.1% Tween-20), membranes were
incubated overnight at 4°C with the primary antibodies against
proliferating cell nuclear antigen (PCNA; 1:5,000, cat. no. ab29;
Abcam), Ki-67 (1:1,000, cat. no. ab92742; Abcam), matrix
metalloproteinase (MMP)2 (1:1,000, cat. no. ab92536; Abcam), MMP9
(1:1,000, cat. no. ab76003; Abcam), tissue inhibitor of
metalloproteinase-1 (TIMP-1; 1:1,000, cat. no. ab211926; Abcam),
Bcl-2 (1:2,000, cat. no. ab32124; Abcam), Bax (1:5,000, cat. no.
ab32503; Abcam), cleaved caspase-3 (1:500 cat. no. ab32042; Abcam),
caspase-3 (1:5,000, cat. no. ab32351; Abcam), TFAP2C (1:1,000, cat.
no. ab218107; Abcam), GAPDH (1:5,000, cat. no. ab8245; Abcam) and
the corresponding secondary HRP-conjugated goat anti-rabbit IgG
(1:5,000, cat. no. 7074; Cell signaling technology) at room
temperature for 2 h, followed by visualization with the Pierce™
enhanced chemiluminescence western blotting substrate (Thermo
Fisher Scientific, Inc.) and quantitative analysis with the ImageJ
software (version 1.48v; National Institutes of Health).
Reverse transcription-quantitative PCR
(RT-qPCR)
Total RNA was extracted from cells using
TRIzol® (Invitrogen; Thermo Fisher Scientific, Inc.)
according to the manufacturers protocol. A total of 5 µg RNA was
then reverse transcribed into cDNA using PrimerScript™ RT Master
Mix (cat. no. RR036A; Takara Bio, Inc.). The temperature protocol
was 37°C for 15 min and reaction at 85°C for 5 sec. The qPCR
reactions were performed using TB Green® Premix Ex Taq™
(cat. no. RR420A; Takara Bio, Inc.) on an ABI Prism 7500 sequence
detector (Applied Biosystems, Inc.; Thermo Fisher Scientific,
Inc.). The thermocycling conditions: Pre-denaturation at 95°C for
30 sec, followed by denaturation at 95°C for 10 sec and annealing
at 55°C for 30 sec for 40 cycles. The specific primers used were as
follows: TFAP2C forward, 5′-ATCGAAAAATGGAGGCCGGT-3′ and reverse,
5′-CGGCTTCACAGACATAGGCA-3′; PCNA forward,
5′-GTTACTGAGGGCGAGAAGCG-3′ and reverse, 5′-AAGTCTAGCTGGTTTCGGCT-3′;
Ki-67 forward, 5′-CTGACCCTGATGAGAGTGAGGGA-3′ and reverse,
5′-GGACAGGTGGAGTGTGCATTA-3′ and GAPDH forward,
5′-GCAACCGGGAAGGAAATGAATG-3′ and reverse,
5′-CCCAATACGACCAAATCAGAGA-3′. Results were normalized to GAPDH
expression, and the comparative Cq method (2−ΔΔCq) was
used to calculate the relative gene expression levels (21).
Statistical analysis
GraphPad Prism 8 (GraphPad Software, Inc.) was used
for data analysis. Data were generated from three independent
experimental repeats. The results are presented as the mean ±
standard deviation. Data analysis was carried out using one-way
analysis of variance followed by Tukey's post hoc test. P<0.05
was considered to indicate a statistically significant
difference.
Results
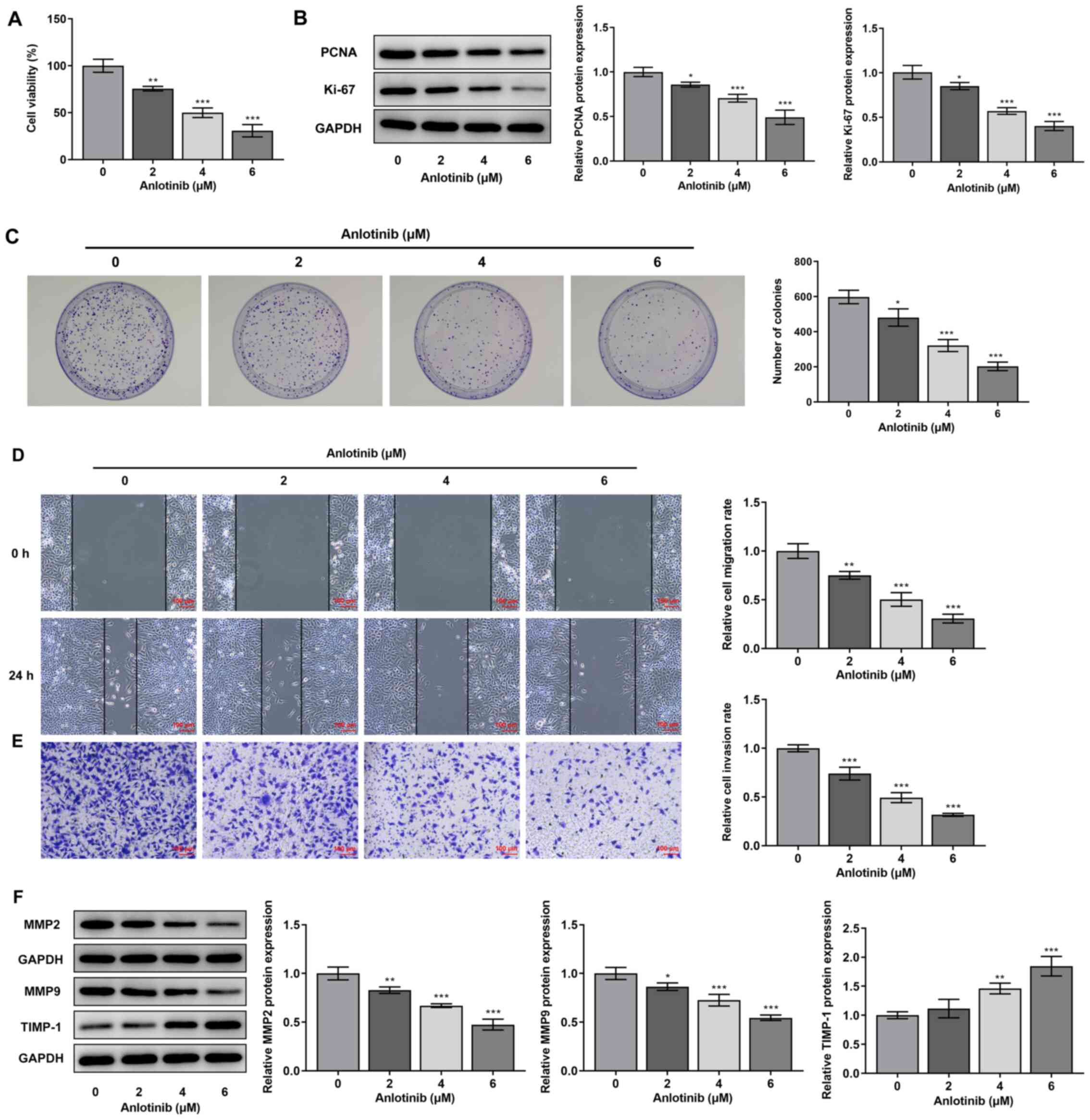
Anlotinib inhibits the proliferation,
migration and invasion of breast cancer cell line MCF-7 in a
concentration-dependent manner
Different concentrations of Anlotinib (0, 2, 4 and 6
µM) were used to treat MCF-7 cells, and cell viability, colony
formation and PCNA and Ki-67 protein expression were assessed. As
shown in Fig. 1A, cell viability
was significantly reduced following 2, 4 and 6 µM Anlotinib
treatment. Moreover, the protein expression of PCNA and Ki-67 was
significantly reduced by Anlotinib (Fig. 1B). Anlotinib also significantly
reduced the number of colonies in MCF-7 cells (Fig. 1C). Furthermore, wound healing and
Transwell assays were used to evaluate the effect of Anlotinib on
cell migration and invasion, respectively. As demonstrated in
Fig. 1D and E, both the cell
migration and invasion rate were significantly inhibited by
Anlotinib. Moreover, Anlotinib resulted in a significant decrease
in MMP2 and MMP9 expression levels and a significant increase in
TIMP-1 expression, further indicating an inhibitory effect on cell
migration (Fig. 1F). Thus,
Anlotinib exerted a concentration-dependent inhibitory effect on
MCF-7 cell proliferation, migration and invasion.
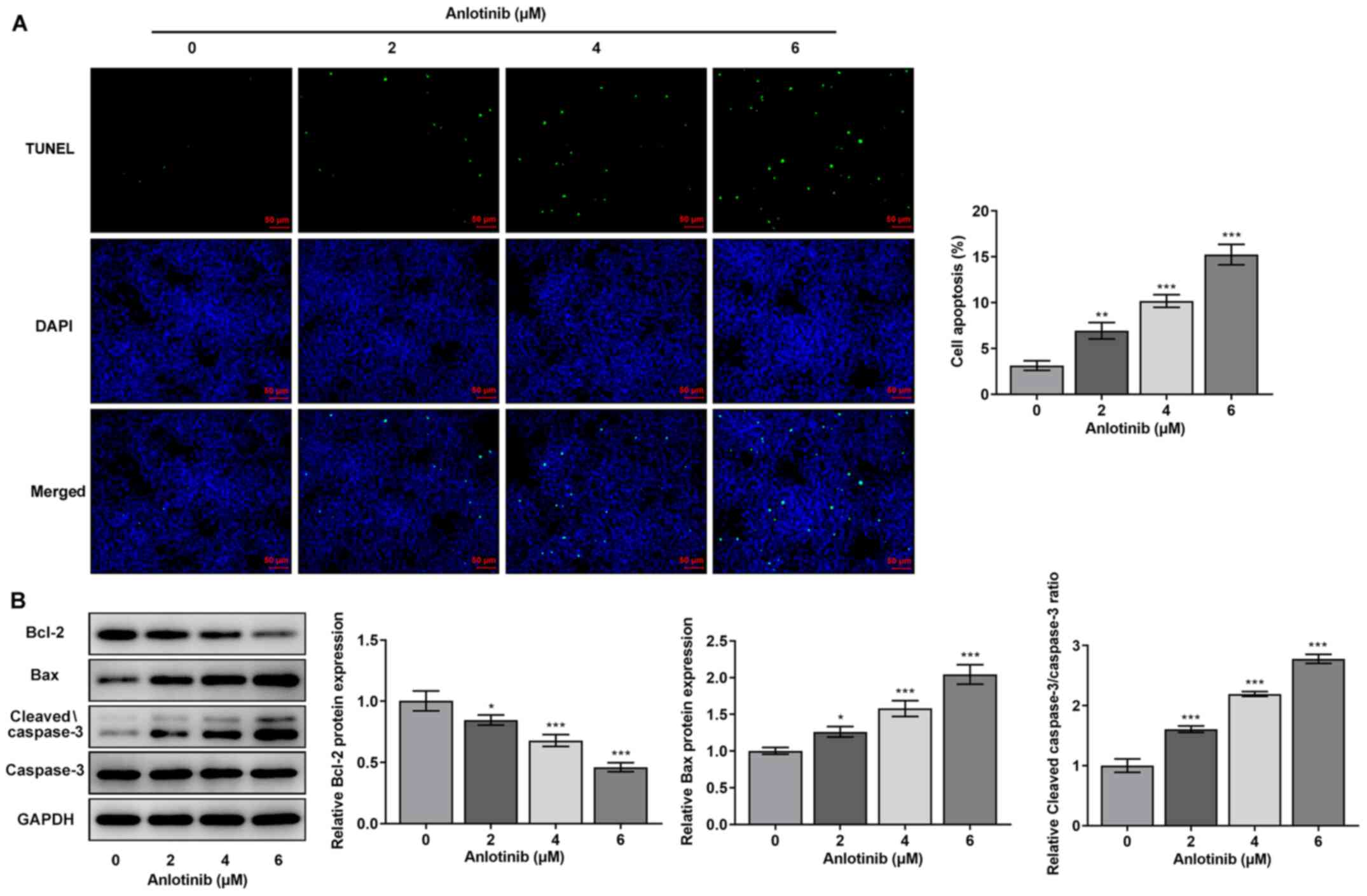
Anlotinib promotes the apoptosis of
MCF-7 breast cancer cells
Subsequently, the effect of Anlotinib on MCF-7 cells
apoptosis was evaluated using TUNEL staining and western blot
assays. As shown in Fig. 2A, cells
exposed to 2, 4 and 6 µM Anlotinib exhibited a higher frequency of
TUNEL-positive (apoptotic) cells compared with control (0 µM)
cells, indicating that Anlotinib could promote apoptosis. This was
further evidenced by the decrease in Bcl-2 expression, as well as
the increase in Bax expression and cleaved-caspase-3/caspase-3
ratio following treatment with 2, 4 and 6 µM Anlotinib (Fig. 2B).
TFAP2C overexpression partially blocks
the effect of Anlotinib on MCF-7 cell proliferation, migration and
apoptosis
Next, the effect of Anlotinib on TFAP2C expression
was determined. As shown in Fig. 3A
and B, both the mRNA and protein expression levels of TFAPC2
were reduced in response to Anlotinib treatment, and the effect was
concentration-dependent.
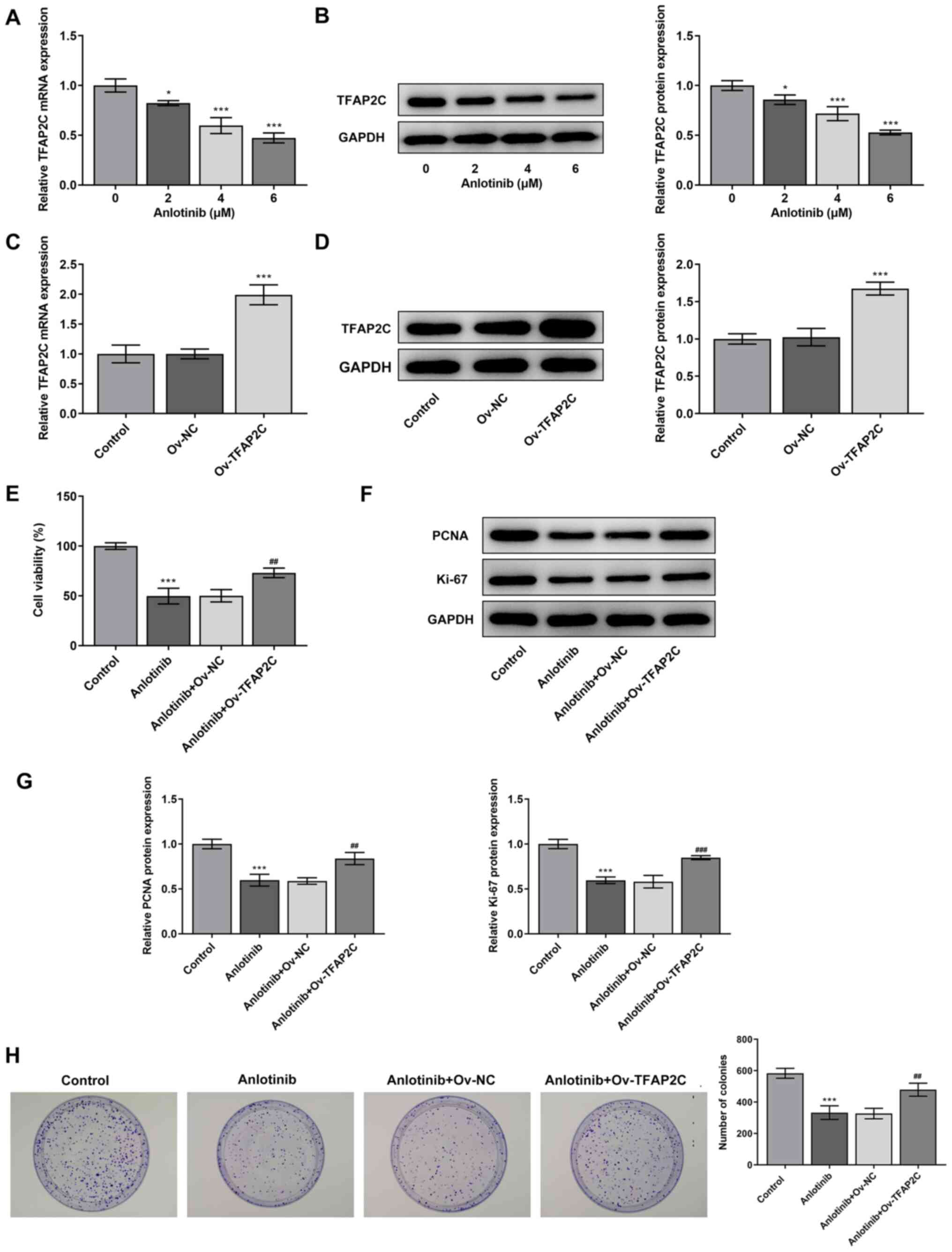 | Figure 3.TFAP2C overexpression blocks the
inhibitory effect of Anlotinib on MCF-7 cell proliferation. MCF-7
cells were cultured in medium containing 0, 2, 4 or 6 µM Anlotinib
for 24 h, then (A) TFAP2C mRNA and (B) protein expression levels
were measured by RT-qPCR and western blotting, respectively. Data
were obtained from three independent repeated experiments.
*P<0.05 and ***P<0.001 vs. 0 µM Anlotinib. MCF-7 cells were
transfected with Ov-TFAP2C or Ov-NC, then (C) TFAP2C mRNA and (D)
protein expression levels were measured by RT-qPCR and western
blotting, respectively. All experiments were independently
performed for three times. ***P<0.001 vs. Ov-NC. (E-H) MCF-7
cells transfected with Ov-TFAP2C or Ov-NC were exposed to 4 µM
Anlotinib for 24 h, then (E) cell viability was tested using Cell
Counting Kit-8 assays, (F and G) the expression of PCNA and Ki-67
was measured by western blotting and (H) cell proliferation was
evaluated using colony formation assays. Data were obtained from
three independent experiments. ***P<0.001 vs. control;
##P<0.01 and ###P<0.001 vs. Anlotinib +
Ov-NC. RT-qPCR, reverse transcription-quantitative PCR; TFAP2C,
transcription factor AP-2γ; Ov, overexpression; NC, negative
control; PCNA, proliferating cell nuclear antigen. |
TFAP2C was overexpressed in MCF-7 cells (Fig. 3C and D) to explore the changes in
the effect of Anlotinib on MCF-7 cells proliferation, migration and
apoptosis. Cell viability was higher in Anlotinib + Ov-TFAPC2 group
compared with that in the Anlotinib + Ov-NC group (Fig. 3E). In addition, Anlotinib inhibited
the expression of PCNA and Ki-67, whereas TFAP2C overexpression
partially rescued PCNA and Ki-67 expression (Fig. 3F and G). Similarly, the decreased
number of colony-forming units caused by Anlotinib was also
significantly increased by TFAP2C overexpression (Fig. 3H). These data revealed the
protective effects of TFAP2C overexpression against
Anlotinib-induced reduction in MCF-7 cell viability. Finally,
TFAP2C-overexpressing MCF-7 cells were exposed to 4 µM Anlotinib,
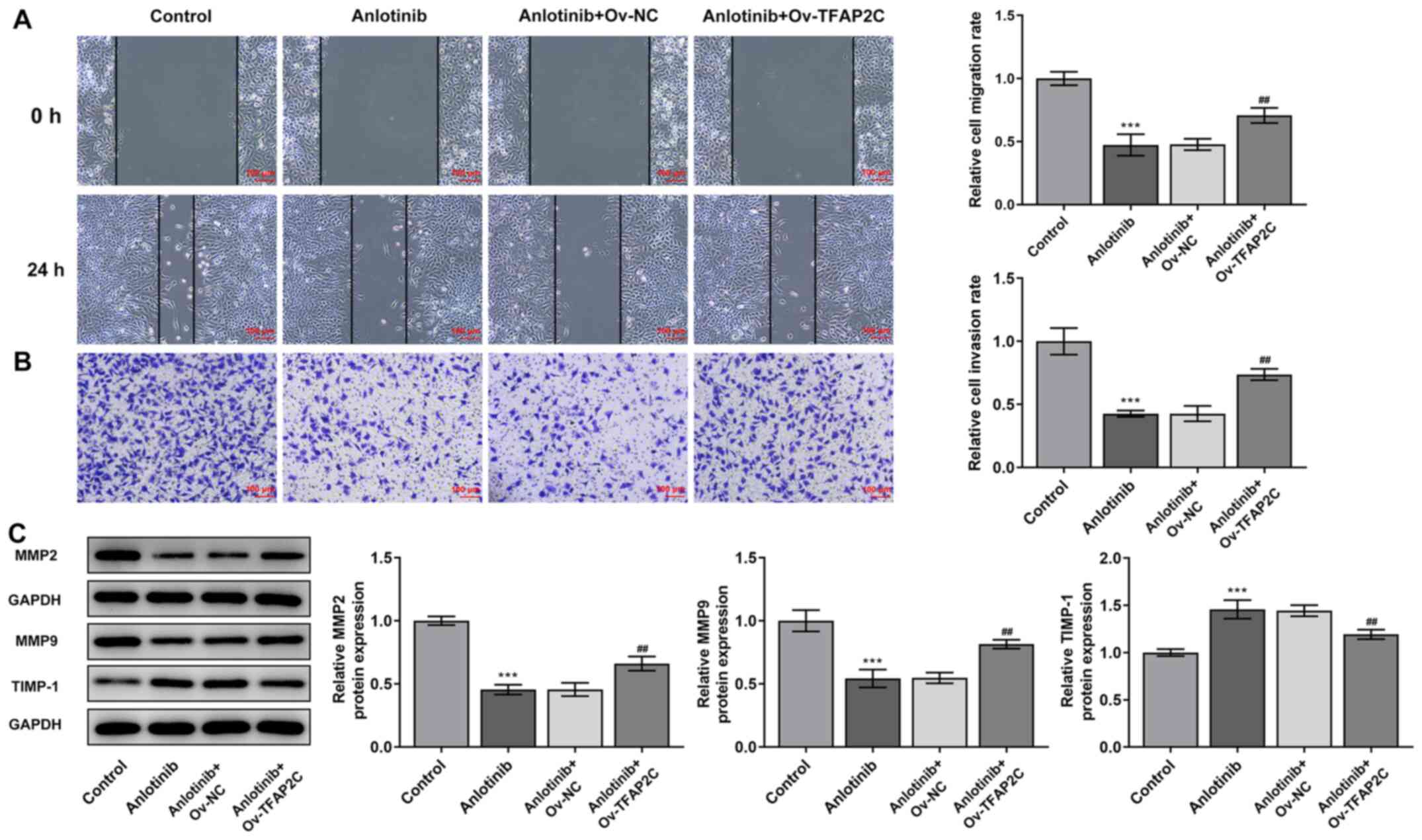
then cell migration, invasion and apoptosis were assessed. As shown
in Fig. 4A and B, the reduced
ability of migration and invasion caused by Anlotinib was reversed
following TFAP2C overexpression. Consistently, TFAP2C
overexpression also blocked the effect of Anlotinib on MMP2, MMP9
and TIMP-1 expression (Fig. 4C).
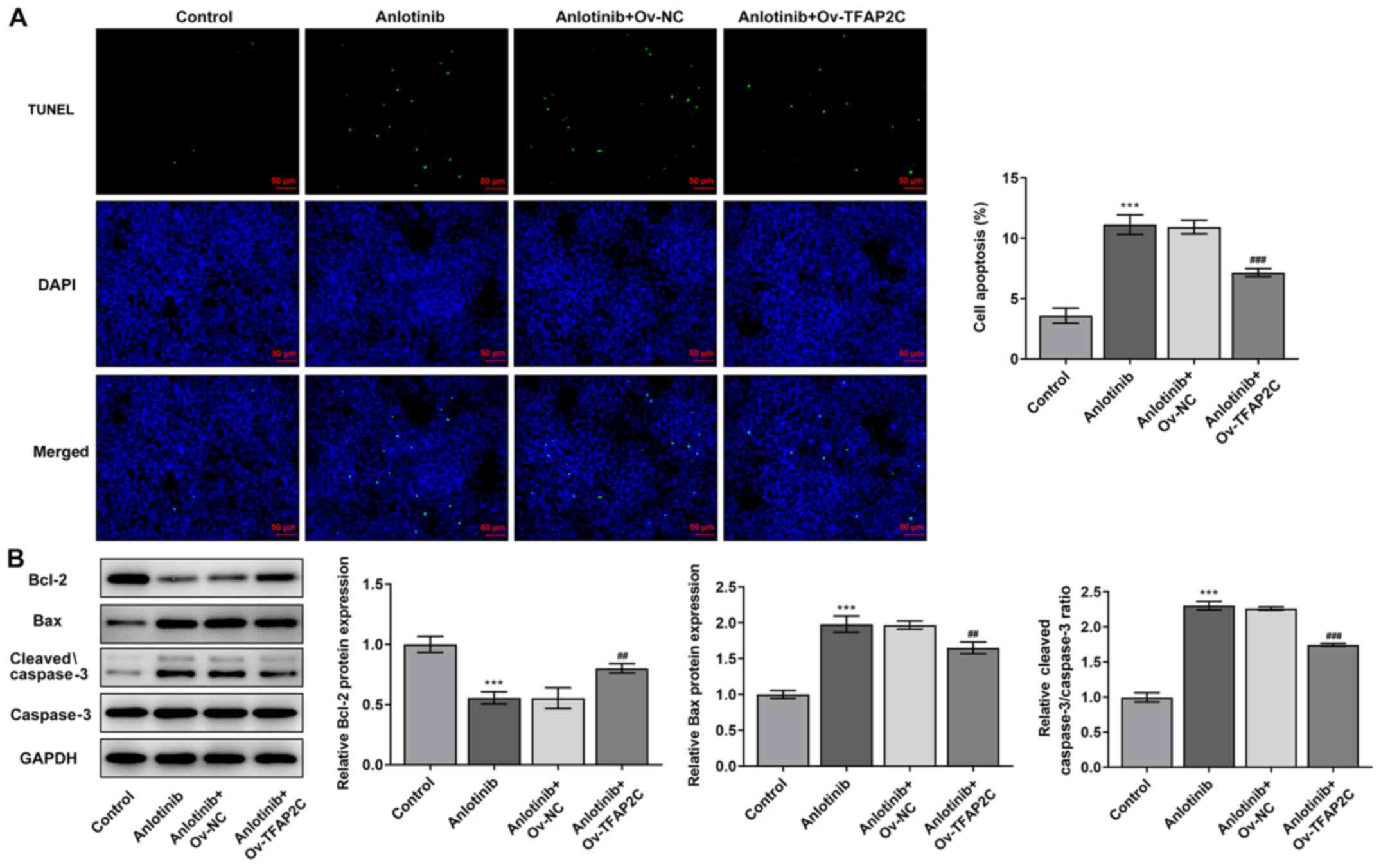
Furthermore, TFAP2C overexpression significantly reversed the
effect of Anlotinib on the frequency of apoptotic cells, as well as
on the protein expression of Bcl-2, Bax and the
cleaved-caspase-3/caspase-3 ratio (Fig. 5A and B).
Discussion
In 2018, the latest data released by the
International Agency for Research on Cancer showed that among all
cancer types, the incidence and mortality of breast cancer ranked
second (22). Breast cancer is
also one of the most important causes of death in women over 45
years of age with malignant tumors (23). In most breast cancer cases,
patients have excellent prognosis, whereas ~40% of breast cancer
patients undergoing treatment experience recurrence and metastasis
(24). The 5-year survival rate of
patients with metastatic breast cancer is not higher than 60%, and
most patients die due to locoregional recurrence and distant
metastasis (25). Therefore, the
development of novel effective therapeutic agents for breast cancer
remains an urgent medical requirement. In the present study, the
potential therapeutic effect of the novel multi-kinase inhibitor
Anlotinib was evaluated in breast cancer cells. The results
suggested that Anlotinib had an antitumor effect on breast cancer
cells by inhibiting their proliferation, migration, invasion and
inducing their apoptosis in vitro.
TFAP2C regulates the expression of estrogen receptor
α (ERα), which is transcriptionally regulated in breast cancer
(26). Thus, the involvement of
TFAP2C in breast cancer has been extensively studied (12,26,27).
For example, higher TFAP2C expression has been shown to correlate
with poor overall survival after 10 years of diagnosis in
ERα+ and endocrine therapy-treated subgroups of breast
cancer (28). TFAP2C also predicts
the outcome in HER2+ breast cancer (29). In the present study, Anlotinib
inhibited the expression of TFAP2C in a concentration-dependent
manner. In luminal breast cancer, the response of cancer cells to
Vandetanib is mediated by the TFAP2C target genes epidermal growth
factor receptor (EGFR) and RET (12). Similarly, Anlotinib can inhibit the
expression of RET, which is a downstream target of TFAP2C in breast
cancer (30). Thus, it was
hypothesized that Anlotinib may exert its antitumor effect on
breast cancer cells by downregulating TFAP2C expression. TFAP2C was
overexpressed in MCF-7 cells, which were then subjected cells to
Anlotinib treatment. In accordance with our hypothesis, the data
revealed that TFAP2C overexpression markedly blocked the antitumor
effect of Anlotinib on MCF-7 breast cancer cells. However, the
specific signaling pathways downstream of Anlotinib/TFAP2C have not
been investigated in this study. TFAP2C is the key regulator of
hormone responsiveness in breast cancer cells through the control
of multiple pathways of estrogen signaling (25,30,31).
Whether these pathways are involved in the effect of Anlotinib on
breast cancer via TFAP2C remains to be elucidated. In addition, the
conclusion of this study only came from in vitro
experiments, lacking the validation of in vivo animal
models. The effects of knockdown by using small interfering RNA
targeting TFAP2C or overexpression of TFAP2C in MCF-7 cells
(without Anlotinib treatment) on cell growth, cell migration,
invasion, and cell apoptosis will be investigated in future
experiments. Moreover, the use of only a TUNEL assay to detect
apoptotic cells is another limitation of this study. Future
research should aim to strengthen the conclusions of this study
using comprehensive analysis and uncover the underlying mechanisms.
For instance, whether signaling pathways is associated with
Anlotinib in breast cancer should be analyzed.
In conclusion the present study demonstrated that
Anlotinib exerts antitumor effects on breast cancer cells through
inhibition of cell growth, induction of apoptosis and suppression
of cell migration and invasion. Importantly, the effect Anlotinib
against breast cancer might be partially dependent on inhibiting
TFAP2C expression. Thus, the finding that Anlotinib may be used as
an effective antitumor agent for breast cancer treatment was
further confirmed.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
FF and QY designed the experimental study and
analyzed the experiment data. FF performed the experiments. FF and
QY confirmed the authenticity of all the raw data. All authors have
read and approved the final manuscript for submission.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
DeSantis C, Siegel R, Bandi P and Jemal A:
Breast cancer statistics, 2011. CA Cancer J Clin. 61:409–418. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Tajima T, Tokuda T and Kubota M: Treatment
of advanced breast cancer: current issues. Cancer and Chemotherapy.
25:1832–1840. 1998.(In Japanese). PubMed/NCBI
|
|
3
|
Maughan KL, Lutterbie MA and Ham PS:
Treatment of breast cancer. Am Fam Physician. 81:1339–1346.
2010.PubMed/NCBI
|
|
4
|
Yang J, Yan J and Liu B: Targeting
VEGF/VEGFR to modulate antitumor immunity. Front Immunol.
9:9782018. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Jiao Q, Bi L, Ren Y, Song S, Wang Q and
Wang YS: Advances in studies of tyrosine kinase inhibitors and
their acquired resistance. Mol Cancer. 17:362018. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kerbel RS: Strategies for improving the
clinical benefit of antiangiogenic drug based therapies for breast
cancer. J Mammary Gland Biol Neoplasia. 17:229–239. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Gao Y, Liu P and Shi R: Anlotinib as a
molecular targeted therapy for tumors. Oncol Lett. 20:1001–1014.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sun Y, Niu W, Du F, Du C, Li S, Wang J, Li
L, Wang F, Hao Y, Li C, et al: Safety, pharmacokinetics, and
antitumor properties of anlotinib, an oral multi-target tyrosine
kinase inhibitor, in patients with advanced refractory solid
tumors. J Hematol Oncol. 9:1052016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Syed YY: Anlotinib: First global approval.
Drugs. 78:1057–1062. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Han B, Li K, Wang Q, Zhang L, Shi J, Wang
Z, Cheng Y, He J, Shi Y, Zhao Y, et al: Effect of anlotinib as a
third-line or further treatment on overall survival of patients
with advanced non-small cell lung cancer: The ALTER 0303 Phase 3
Randomized Clinical Trial. JAMA Oncol. 4:1569–1575. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Li L, Yu J, Jiao S, Wang W, Zhang F and
Sun S: Vandetanib (ZD6474) induces antiangiogenesis through
mTOR-HIF-1 alpha-VEGF signaling axis in breast cancer cells.
OncoTargets Ther. 11:8543–8553. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
De Andrade JP, Park JM, Gu VW, Woodfield
GW, Kulak MV, Lorenzen AW, Wu VT, Van Dorin SE, Spanheimer PM and
Weigel RJ: EGFR is regulated by TFAP2C in luminal breast cancer and
is a target for vandetanib. Mol Cancer Ther. 15:503–511. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hu N, Si Y, Yue J, Sun T, Wang X, Jia Z,
Gao S, Li Q, Shao Y, Wang J, et al: Anlotinib has good efficacy and
low toxicity: A phase II study of anlotinib in pre-treated HER-2
negative metastatic breast cancer. Cancer Biol Med. 18:849–859.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zhang Y, Wu D, Zhao B, Tian XL, Yao TC, Li
F, Liu WF and Shi AP: Application of neoadjuvant chemotherapy
combined with anlotinib in occult breast cancer: A case report and
review of literature. World J Clin Cases. 9:919–926. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Bogachek MV, Chen Y, Kulak MV, Woodfield
GW, Cyr AR, Park JM, Spanheimer PM, Li Y, Li T and Weigel RJ:
Sumoylation pathway is required to maintain the basal breast cancer
subtype. Cancer Cell. 25:748–761. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Sotiriou C, Wirapati P, Loi S, Harris A,
Fox S, Smeds J, Nordgren H, Farmer P, Praz V, Haibe-Kains B, et al:
Gene expression profiling in breast cancer: Understanding the
molecular basis of histologic grade to improve prognosis. J Natl
Cancer Inst. 98:262–272. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sørlie T, Perou CM, Tibshirani R, Aas T,
Geisler S, Johnsen H, Hastie T, Eisen MB, van de Rijn M, Jeffrey
SS, et al: Gene expression patterns of breast carcinomas
distinguish tumor subclasses with clinical implications. Proc Natl
Acad Sci USA. 98:10869–10874. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Gu C, Zou S, He C, Zhou J, Qu R, Wang Q,
Qi J, Zhou M, Yan S and Ye Z: Long non-coding RNA CCAT1 promotes
colorectal cancer cell migration, invasiveness and viability by
upregulating VEGF via negative modulation of microRNA-218. Exp Ther
Med. 19:2543–2550. 2020.PubMed/NCBI
|
|
19
|
Sui C, Liu D, Hu Y and Zhang L:
MicroRNA-708-5p affects proliferation and invasion of osteosarcoma
cells by targeting URGCP. Exp Ther Med. 17:2235–2241.
2019.PubMed/NCBI
|
|
20
|
Wang Y, Liu M, Chen S and Wu Q:
Plantamajoside represses the growth and metastasis of malignant
melanoma. Exp Ther Med. 19:2296–2302. 2020.PubMed/NCBI
|
|
21
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(−Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Plichta JK, Thomas SM, Vernon R, Fayanju
OM, Rosenberger LH, Hyslop T, Hwang ES and Greenup RA: Breast
cancer tumor histopathology, stage at presentation, and treatment
in the extremes of age. Breast Cancer Res Treat. 180:227–235. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Gouri A, Benarba B, Dekaken A, Aoures H
and Benharkat S: Prediction of late recurrence and distant
metastasis in early-stage breast cancer: Overview of current and
emerging biomarkers. Curr Drug Targets. 21:1008–1025. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Woolston C: Breast cancer. Nature.
527:S1012015. View
Article : Google Scholar : PubMed/NCBI
|
|
26
|
Franke CM, Gu VW, Grimm BG, Cassady VC,
White JR, Weigel RJ and Kulak MV: TFAP2C regulates carbonic
anhydrase XII in human breast cancer. Oncogene. 39:1290–1301. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Woodfield GW, Horan AD, Chen Y and Weigel
RJ: TFAP2C controls hormone response in breast cancer cells through
multiple pathways of estrogen signaling. Cancer Res. 67:8439–8443.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Perkins SM, Bales C, Vladislav T, Althouse
S, Miller KD, Sandusky G, Badve S and Nakshatri H: TFAP2C
expression in breast cancer: Correlation with overall survival
beyond 10 years of initial diagnosis. Breast Cancer Res Treat.
152:519–531. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Wu VT, Kiriazov B, Koch KE, Gu VW, Beck
AC, Borcherding N, Li T, Addo P, Wehrspan ZJ, Zhang W, et al: A
TFAP2C gene signature is predictive of outcome in HER2-positive
breast cancer. Mol Cancer Res. 18:46–56. 2020.PubMed/NCBI
|
|
30
|
Spanheimer PM, Woodfield GW, Cyr AR, Kulak
MV, White-Baer LS, Bair TB and Weigel RJ: Expression of the RET
proto-oncogene is regulated by TFAP2C in breast cancer independent
of the estrogen receptor. Ann Surg Oncol. 20:2204–2212. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Kulak MV, Cyr AR, Woodfield GW, Bogachek
M, Spanheimer PM, Li T, Price DH, Domann FE and Weigel RJ:
Transcriptional regulation of the GPX1 gene by TFAP2C and aberrant
CpG methylation in human breast cancer. Oncogene. 32:4043–4051.
2013. View Article : Google Scholar : PubMed/NCBI
|