Introduction
Lymph node (LN) status is a key prognostic factor in
colon cancer (1). Staging accuracy
and prognosis improve with increased numbers of dissected and
examined LNs, both in stage II and III colon cancer (2). At present, the most widely used LN
staging system is number of metastatic LNs in pathological
assessment (pN) from the 8th edition of the TNM American Joint
Committee on Cancer/Union for International Cancer Control
(AJCC/UICC) staging system, which takes into account the number of
metastatic LNs (3). To evaluate LN
status, the AJCC/UICC guidelines recommend resection and assessment
of ≥12 LNs. Nevertheless, as reported by numerous studies, the LN
yield from a colectomy varies and may not be sufficient to meet
these recommendations (4,5); this is because LN yield depends on
various factors, such as surgical technique and differences in
pathological procedure for obtaining LNs from the specimen
(5,6).
Evaluation of LN status based only on the number of
metastatic LNs and omitting the total number of dissected LNs (as
in pN) may be insufficient and lead to understaging. For that
reason, two novel systems analysing not only the number of positive
LNs, but also number of dissected LNs (NDLNs) were developed: LN
ratio (LNR) (7) and log odds of
positive LNs (LODDS) (8). LNR is
the ratio of positive LNs divided by the total number of dissected
LNs, which reflects the probability of metastatic LNs in the LN
yield. LNR has been reported to be a strong independent prognostic
factor in rectal and colon cancer (9,10),
as well as multiple types of solid malignant tumors, such as
breast, pancreatic, gastric, lung and bladder cancer (11–14).
LODDS is another LN staging system that has been proved to be a
strong prognostic factor in colon and rectal cancer (8,15–17).
This staging system is particularly useful for patients without
metastases to regional LNs. In patients with node-negative cancer,
LNR is zero and does not provide any additional information in
comparison with pN0 from TNM classification, whereas LODDS may
stratify patients according to prognosis in this group (15–17).
The aim of the present study was to compare three LN
staging systems in patients with colon cancer who underwent
elective tumour resection.
Materials and methods
Patients
The present study recruited 298 patients who were
operated on between September 2006 and May 2014 in the Department
of Oncological Surgery, Gdynia Centre of Oncology, Pomeranian
Hospitals, Poland. The inclusion criteria were as follows: Patients
aged >18 years; histologically proven adenocarcinoma of the
colon; curative surgical tumor resection and minimal follow-up
period of 65 months or until death. Patients with in situ
disease, other malignancy, lack of complete information about LN
status or follow-up and neoadjuvant treatment were excluded. The
present study was approved by the Independent Ethics Committee of
the Regional Medical Chamber in Gdańsk (approval no. KB-2/20).
Because of the retrospective design of the study based on data
analysis, the requirement for informed consent was waived. The
patient data included age at diagnosis, sex, primary tumor site,
details of surgical procedure, pathological grade (G),
postoperative tumor staging (pT stage), presence of distant
metastasis (M stage), number of retrieved LNs, number of metastatic
LNs (pN stage) and follow-up. The follow-up of all investigated
cases proceeded until death or October 2019. The caecum, ascending
colon, hepatic flexure and proximal two-thirds of the transverse
colon were defined as the right colon. The distal one-third of the
transverse colon, splenic flexure, descending colon, sigmoid and
rectosigmoid junction were defined as the left colon. In some
cases, groups were combined due to minor abundance (e.g., pT1 +
pT2, pT3 + pT4, G1 + G2 and G3 + G4). The clinical and
histopathological characteristics of the study population are
presented in Table I.
 | Table I.Univariate survival analysis. |
Table I.
Univariate survival analysis.
| Parameter | n | 5-year OS
probability | P-value |
|---|
| Age, years (median,
71 years) |
|
| 0.0005 |
| ≤71 | 156 | 0.75 |
|
|
>71 | 142 | 0.57 |
|
| Sex |
|
|
|
|
Female | 143 | 0.69 | 0.5000 |
| Male | 155 | 0.65 |
|
| Location |
|
| 0.4000 |
| Right
colon | 138 | 0.68 |
|
| Left
colon | 160 | 0.65 |
|
| Depth of invasion,
pT |
|
| 0.0200 |
| 1 +
2 | 50 | 0.80 |
|
| 3 + 4a +
4b | 248 | 0.64 |
|
| pN |
|
| <0.0001 |
| pN0 | 181 | 0.80 |
|
| pN1a | 27 | 0.66 |
|
| pN1b | 49 | 0.46 |
|
| pN2a | 17 | 0.35 |
|
| pN2b | 24 | 0.29 |
|
| LNR |
|
| <0.0001 |
| LNR0 | 182 | 0.80 |
|
|
LNR1 | 51 | 0.62 |
|
|
LNR2 | 32 | 0.43 |
|
|
LNR3 | 21 | 0.33 |
|
|
LNR4 | 12 | 0.08 |
|
| LODDS |
|
| <0.0001 |
|
LODDS1 | 190 | 0.79 |
|
|
LODDS2 | 78 | 0.55 |
|
|
LODDS3 | 30 | 0.23 |
|
| Distant
metastasis |
|
| <0.0001 |
| M0 | 274 | 0.71 |
|
| M1a +
1b + 1c | 24 | 0.20 |
|
| Number of nodes
retrieved by lymphadenectomy |
|
| 0.1000 |
|
<12 | 123 | 0.62 |
|
|
≥12 | 175 | 0.70 |
|
| World Health
Organization histological grade |
|
| 0.0200 |
| G1 +
G2 | 264 | 0.69 |
|
| G3 +
G4 | 34 | 0.50 |
|
Definition of LN classifications
LN status according to pN from TNM staging system is
defined by the number of metastatic LNs (Table II) (3).
| Table II.Classification of LN staging
systems. |
Table II.
Classification of LN staging
systems.
| A, pN |
|
|---|
|
|---|
| Stage | Value (number of
metastatic LN) |
|---|
| pN0 | 0 |
| pN1a | 1 |
| pN1b | 2-3 |
| pN1c | No metastatic LN
but there are tumor deposits |
| pN2a | 4-6 |
| pN2b | ≥7 |
|
| B, LNR |
|
| Stage | Values |
|
| LNR0 | 0.00 |
| LNR1 | 0.01-0.17 |
| LNR2 | 0.18-0.41 |
| LNR3 | 0.42-0.69 |
| LNR4 | ≥0.70 |
|
| C,
LODDS |
|
| Stage | Values |
|
| LODDS1 | <-2.18 |
| LODDS2 | -(2.18-0.23) |
| LODDS3 | >-0.23 |
LNR is defined as the ratio of metastatic to
examined LNs. Previous studies used distinct methods to determine
LNR cut-off values to discriminate patients by their prognosis,
with only a few studies using statistical methods (9,16,18).
The majority of previous studies used quartiles, mean values or
arbitrary classification. The present study used cut-off values
developed by Rosenberg et al (9), which were established using
statistical methods (classification and regression trees technique)
and evaluated using a large population of patients with colorectal
cancer (n=17,309) (19). This
classification divides patients into five subgroups according to
LNR (Table II).
LODDS is the log of the ratio between the numbers of
positive and negative LNs: loge [(pN + 0.5)/(nN + 0.5)],
where pN is the number of positive LNs and nN is the number of
negative LNs and 0.5 is added to both the numerator and denominator
to avoid an infinite value. In the present study, cut-off values
determined statistically by Zhang et al (20) using a large group of patients
(n=240,898) were used to stratify the patients. The prognostic
cut-off values were determined as −2.18 and −0.23 and subgroups are
presented in Table II.
Statistical analysis
Statistical analysis was performed using Statistica
(version 13; TIBCO Software, Inc.). Pearson's χ2 test
was performed to evaluate the association between clinical and
histopathological parameters and investigate the LN staging
systems. Univariate analysis of survival was performed using the
Kaplan-Meier method and differences in survival rates between
subgroups were compared using log-rank test. The end point of the
present study was 5-year overall survival (OS). A multivariate
analysis was conducted using the Cox proportional hazard model. The
three-step multivariate analysis was applied to assess the
prognostic discriminating power of different LN staging systems. In
step one, all relevant factors from the univariate analysis were
encompassed, including pN, but excluding LNR and LODDS. In step 2,
LODDS was added, but not LNR. In step 3, all three LN
classifications were included. Additionally, Akaike Information
Criterion (AIC) was used to assess which model fit best.
Principally, the predictive model with the lowest AIC displayed the
best fit. The correlation between different LN classifications was
analysed using Pearson correlation coefficient. P<0.05 was
considered to indicate a statistically significant difference.
Results
The results of the univariate analysis of survival
and 5-year OS rates are presented in Table I. Age (>71 years), pT, M stage
and pathological grade were significantly negatively associated
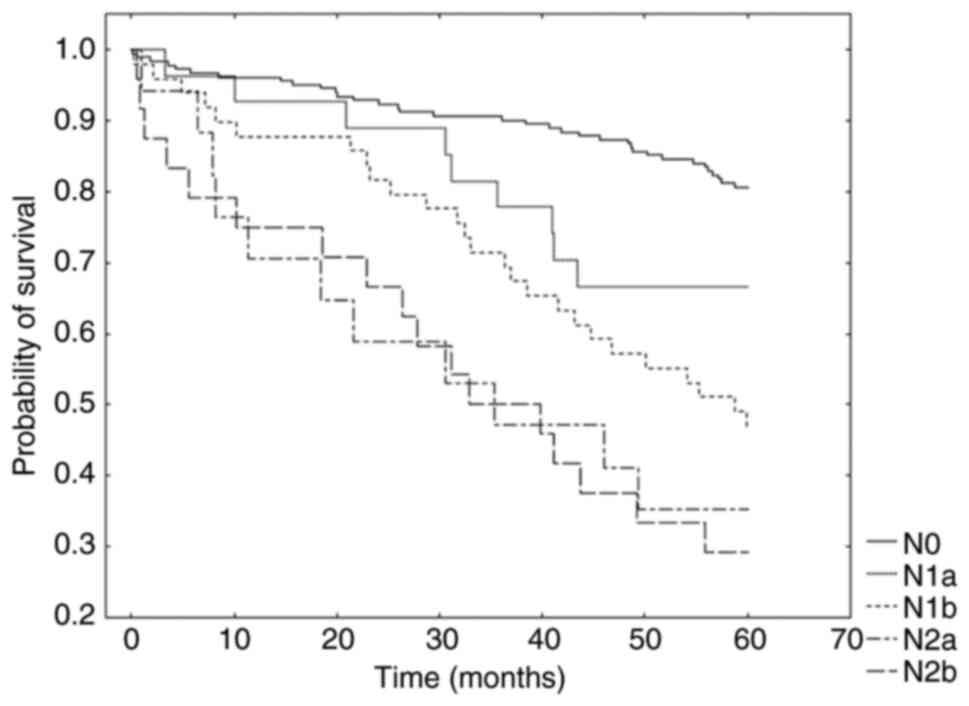
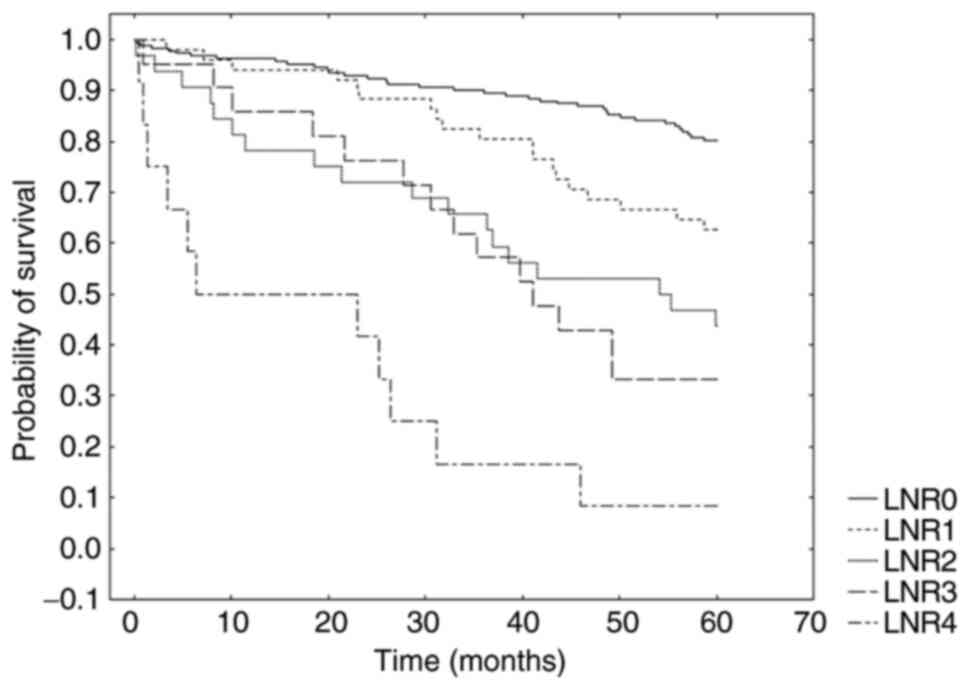
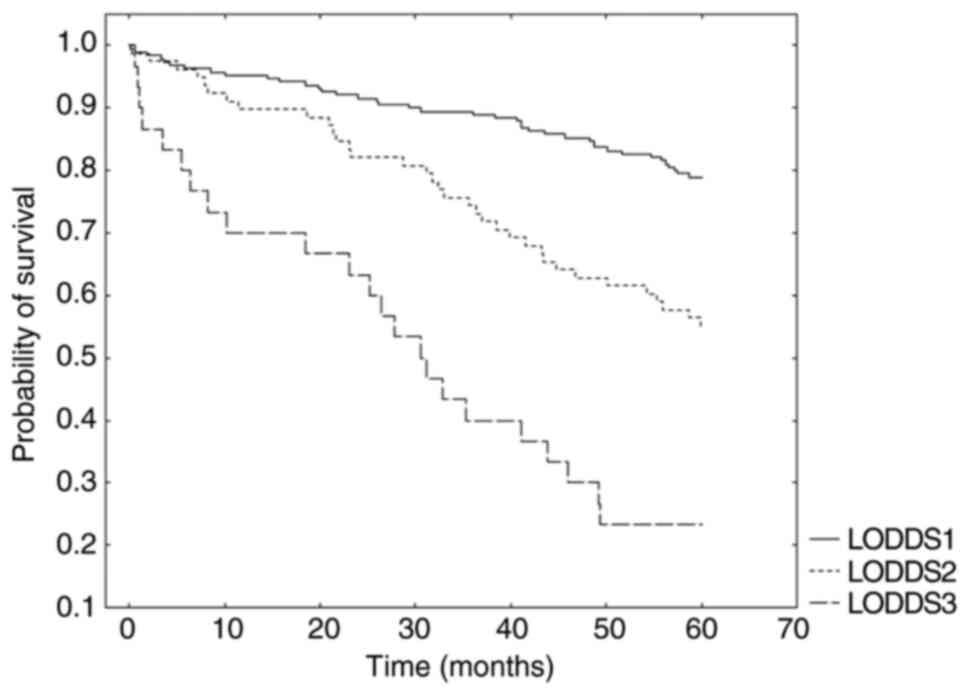
with patient prognosis. Furthermore, the analysis demonstrated a
significant association between increasing number of metastatic LN
and worse prognosis (Fig. 1); this
was also observed for increasing LNR (Fig. 2) and increasing LODDS (Fig. 3). Multivariate analysis was
performed in three steps. In step 1 (Model 1), pN was identified as
an independent prognostic factor. In step 2 (Model 2), when LODDS
was added, pN was displaced by LODDS, which became a significant
independent prognostic factor in relation to prognosis. In step 3
(Model 3), when all three classifications were included, pN and
LODDS were replaced by LNR. The results of the multivariate
analysis are shown in Table III.
Additionally, the AIC confirmed that the LNR staging system
displayed the best performance in relation to prognosis among all
three classifications (AIC for Model 1, 2 and 3, 1012.022, 1010.827
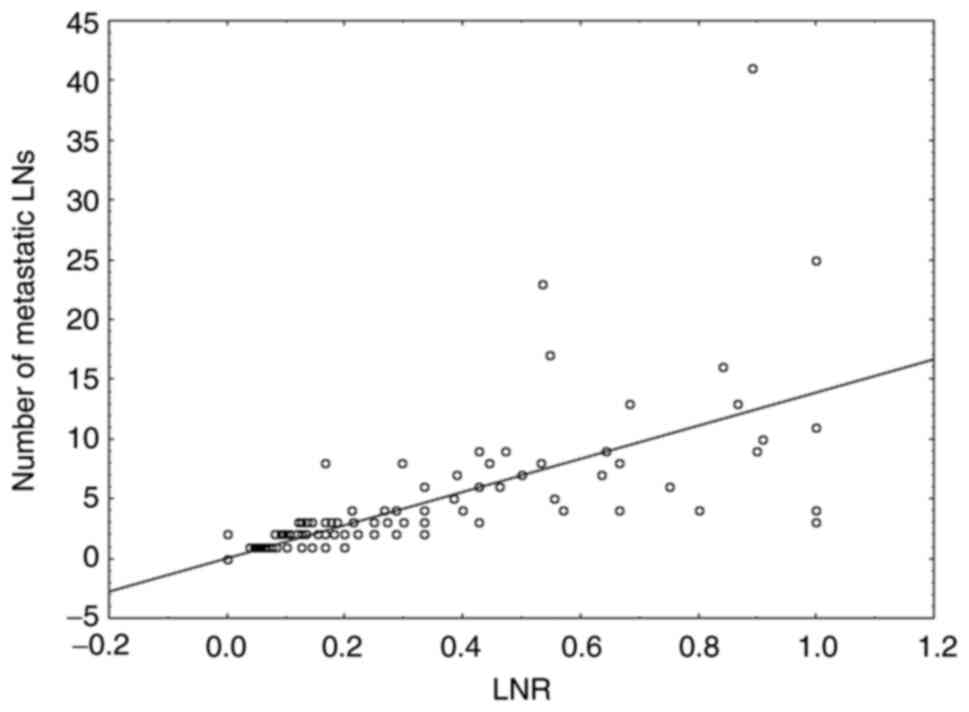
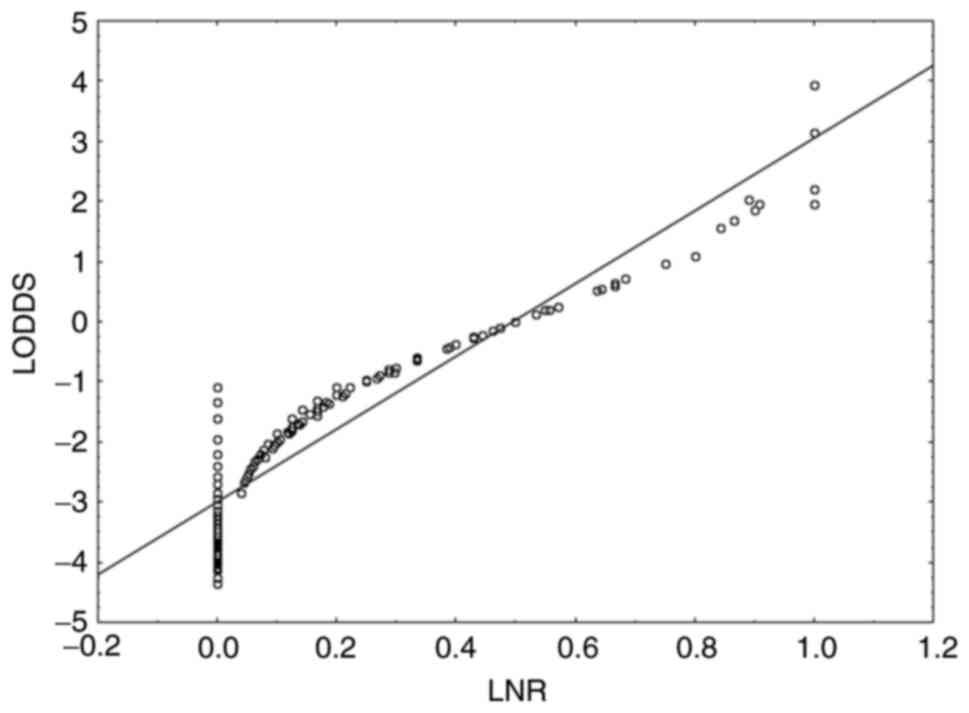
and 1004.578, respectively). The scatter plots of the correlation
between different LN classifications are presented in Figs. 4 and 5. Patients with the same number of
metastatic LNs can be assigned to different LNR values (r=0.77,
P<0.001) (Fig. 4). LODDS and
LNR were closely correlated (r=0.9, P<0.001), despite the
situation when LNR is close to 0 or 1. In this case the value of
LODDS is still heterogeneous (Fig.
5).
| Table III.Three-step multivariate analysis (Cox
proportional hazards model). |
Table III.
Three-step multivariate analysis (Cox
proportional hazards model).
|
| Model 1 | Model 2 | Model 3 |
|---|
|
|
|
|
|
|---|
| Parameter | HR | 95% CI | P-value | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Median age,
years | 0.45 | −1.220–0.380 | 0.0001 | 0.40 | −1.330–0.480 | <0.0001 | 0.37 | −1.410–0.550 | <0.0001 |
| World Health | 1.57 | −0.080-0.980 | 0.0900 | 1.55 | −0.090-0.970 | 0.1000 | 1.67 | −0.010-1.050 | 0.0500 |
| Organization
histological grade |
|
|
|
|
|
|
|
|
|
| Depth of invasion,
pT | 1.28 | −0.420-0.920 | 0.4600 | 1.52 | −0.260-1.100 | 0.2000 | 1.52 | −0.250-1.100 | 0.2000 |
| Distant metastasis,
M | 4.54 | 0.960-2.060 | <0.0001 | 3.84 | 0.770-1.910 | <0.0001 | 3.41 | 0.660-1.800 | <0.0001 |
| pN from
pTNM | 1.01 | 0.005-0.010 | <0.0001 | 1.00 | −0.002-0.009 | 0.3000 | 0.99 | −0.007-0.006 | 0.8000 |
| LODDS | - | - | - | 1.87 | 0.200-1.040 | 0.0030 | 0.89 | −0.740-0.530 | 0.7000 |
| LNR | - | - | - | - | - | - | 1.88 | 0.200-1.050 | 0.0030 |
Further analysis was performed in subpopulations of
patients with NDLN ≥12 and <12. In univariate analysis in both
subpopulations, all three LN classifications were significant
prognostic factors. In the multivariate analysis of patients with
NDLN≥12, the best LN staging system was LNR. In the multivariate
analysis of patients with NDLN<12, when all three LN
classifications were included, none of them displayed significant
differences between levels of staging. However, when 5-year OS
(according to pN) was directly compared in subgroups pN1b and pN2a,
the prognosis was significantly worse in patients with inadequate
lymphadenectomy (NDLN<12) compared with that in patients with
adequate lymphadenectomy (NDLN≥12; Table IV). By contrast, when comparing
LNR and LODDS subgroups, prognosis was similar in patients with
inadequate and adequate lymph node dissection (Table IV).
| Table IV.Univariate analysis of 5-year OS
depending on extent of lymphadenectomy. |
Table IV.
Univariate analysis of 5-year OS
depending on extent of lymphadenectomy.
| A, pN |
|---|
|
|---|
|
| 5-year OS
probability |
|
|---|
| Parameter | NDLN<12 | NDLN≥12 | P-value |
|---|
| pN0 | 0.77 | 0.83 | 0.40 |
| pN1a | 0.62 | 0.68 | 0.80 |
| pN1b | 0.30 | 0.60 | 0.02 |
| pN2a | 0.11 | 0.62 | 0.02 |
| pN2b | 0.40 | 0.26 | 0.70 |
|
| B, LNR |
|
|
| 5-year OS
probability |
|
|
|
|
|
|
Parameter |
NDLN<12 | NDLN≥12 | P-value |
|
| LNR0 | 0.76 | 0.83 | 0.30 |
| LNR1 | 0.57 | 0.63 | 0.70 |
| LNR2 | 0.31 | 0.61 | 0.10 |
| LNR3 | 0.42 | 0.28 | 0.80 |
| LNR4 | 0.12 | <0.001 | 0.10 |
|
| C,
LODDS |
|
|
| 5-year OS
probability |
|
|
|
|
|
|
Parameter |
NDLN<12 | NDLN≥12 | P-value |
|
| LODDS1 | 0.75 | 0.81 | 0.4 |
| LODDS2 | 0.51 | 0.58 | 0.5 |
| LODDS3 | 0.21 | 0.25 | 0.6 |
Discussion
The prognostic value of LNR and LODDS have been
investigated and proven by numerous researchers (7–10,15–21).
pN from TNM is still the most widely used classification despite
only considering the number of metastatic LNs. A potential
limitation of this classification is that its prognostic power is
highly affected by the number of examined LNs. Dissection of ≥12
LNs is enough to evaluate LN status (3). However, inadequate lymphadenectomy
during colon cancer surgery is commonly observed (4,5).
Here, LNR and LODDS were shown to be more accurate LN staging
systems compared with pN, potentially due to decreased dependence
on the number of dissected LNs.
Numerous studies have investigated the prognostic
value of each LN staging system assessed in the present study, but
few surveys that have directly compared the three staging systems
(16,18,21).
As their results have not reached a consensus, the differences may
be an outcome of different statistical methods, cut-off values and
populations of patients. Song et al (18) (n=1,297) concluded that among all
three LN staging systems, LNR was superior to the other two
classifications. Moreover, for patients in each LNR subgroup,
prognosis was highly homologous between those in different pN or
LODDS subgroups. However, for patients in particular pN and LODDS
subgroups, significant differences in survival were identified
between patients in different LNR subgroups.
Fang et al (16) performed multivariate analysis in a
smaller sample of patients (n=192), which showed that LODDS was a
better prognostic factor compared with LNR and pN and that LODDS
was more efficient in differentiating patients with different
outcomes, particularly when the ratio of metastatic LNs was close
to 0 or 1.
Pei et al (21) compared all three LN staging systems
using a large group of patients with colorectal cancer (n=56,747),
analysing pN, LNR and LODDS as both continuous and categorical
variables. When investigated as a categorical variable, cut-off
values from Berger et al (7) and Rosenberg et al (9) were used for the LNR staging system,
whereas cut-off values from Wang et al (8) and Persiani et al (15) were implemented for the LODDS
staging system. The analysis showed that, when considered as a
categorical variable, LNR using Rosenberg's cut-off values
exhibited the best prognostic performance in the whole population
of patients. This was also true for the subpopulation with
NDLN<12, whereas for the subpopulation with NDLN≥12, pN was the
best prognostic model. When investigated as a continuous variable,
the LODDS staging system was superior to the others. However,
according to Pei et al (21) LODDS as a continuous variable would
be impractical to apply in clinical practice; thus, it should be
changed into a categorical variable by calculating the optimal
cut-off values to make it applicable for clinical use.
As aforementioned, the most suitable cut-off values
for LNR and LODDS are still under discussion. In the present study,
cut-off values developed by Rosenberg et al (9) were used for LNR, whereas cut-off
points determined by Zhang et al (20) were used for LODDS. These cut-off
values were selected because they were established statistically
using large populations of patients with colorectal cancer. The
results of the present study confirmed the usefulness of these
cut-off values and, in our opinion, they should be tested in
consecutive studies and then considered for use in wide clinical
practice. In the present study, LNR was identified as the best LN
staging system, both for the whole population of patients and for
the subpopulation with NDLN≥12. In multivariate analysis of the
subpopulation with NDLN <12, none of three LN classifications
provided significantly different prognostic results in the context
of 5-year OS. This may be due to the small number of patients in
subgroups. However, there were significant differences between pN1b
and pN2a subgroups in 5-year OS for patients with adequate and
inadequate lymphadenectomy. These differences were not observed for
LNR and LODDS, which suggested that LNR and LODDS were more
independent of number of dissected LNs, as previously hypothesized
(15,22).
A scatter plot demonstrated an association between
LODDS and LNR. LODDS value was heterogeneous only when LNR was
close to 0 or 1. This indicated that LODDS was particularly
valuable in patients without metastatic LNs because when LNR and pN
for all patients was 0, LODDS classification still divided patients
into subgroups with different prognoses.
The present study has certain limitations because it
was single centre retrospective study that included a relatively
limited number of patients. Therefore, multicentre studies on
larger populations of patients should be performed to verify the
present conclusions. Patients without metastatic LNs could not be
used for full analysis of prognosis according to LODDS due to small
sample size of LODDS subgroups. Therefore, further studies on
larger populations of patients are required to test the prognostic
value of LOODS in pN0 patients operated on for colon
adenocarcinoma.
In conclusion, the present study indicated that LNR
is the most accurate LN staging system for predicting prognosis for
patients with colon cancer who have undergone surgical resection,
especially those with metastatic LNs subjected to adequate
lymphadenectomy. Due to the limitations of LNR in pN0 patients and
the promising prognostic results for LODDS, further studies are
required in this group. Subsequent studies should also be performed
to investigate patients with NDLN <12, as LNR or LODDS might be
more suitable in estimating prognosis in this group than LN staging
using pN from TNM.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analysed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
AMM conceptualized and designed the present study,
collected and interpreted data and drafted the manuscript. MS
analysed the data, generated figures and tables and drafted the
manuscript. WJK conceived the study and revised the manuscript. AMM
and MS confirm the authenticity of all the raw data. All authors
have read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Independent
Ethics Committee of the Regional Medical Chamber in Gdańsk
(approval no. KB-2/20). Due to the retrospective design of the
study based on data analysis, the requirement for informed consent
was waived.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
LN
|
lymph node
|
|
LNR
|
lymph node ratio
|
|
LODDS
|
log odds of positive lymph nodes
|
|
AJCC/UICC
|
American Joint Committee on
Cancer/Union for International Cancer Control
|
|
AIC
|
Akaike Information Criterion
|
|
NDLN
|
number of dissected lymph nodes
|
References
|
1
|
Compton CC, Fielding LP, Burgart LJ,
Conley B, Cooper HS, Hamilton SR, Hammond ME, Henson DE, Hutter RV,
Nagle RB, et al: Prognostic factors in colorectal cancer. College
of American Pathologists Consensus Statement 1999. Arch Pathol Lab
Med. 124:979–994. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chang GJ, Rodriguez-Bigas MA, Skibber JM
and Moyer VA: Lymph node evaluation and survival after curative
resection of colon cancer: Systematic review. J Natl Cancer Inst.
99:433–441. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Weiser MR: (AJCC 8th Edition). Colorectal
Cancer. Ann Surg Oncol. 25:1454–1455. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ostadi MA, Harnish JL, Stegienko S and
Urbach DR: Factors affecting the number of lymph nodes retrieved in
colorectal cancer specimens. Surg Endosc. 21:2142–2146. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Leung AM, Scharf AW and Vu HN: Factors
affecting number of lymph nodes harvested in colorectal cancer. J
Surg Res. 168:224–230. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Jestin P, Påhlman L, Glimelius B and
Gunnarsson U: Cancer staging and survival in colon cancer is
dependent on the quality of the pathologists' specimen examination.
Eur J Cancer. 41:2071–2078. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Berger AC, Sigurdson ER, LeVoyer T, Hanlon
A, Mayer RJ, Macdonald JS, Catalano PJ and Haller DG: Colon cancer
survival is associated with decreasing ratio of metastatic to
examined lymph nodes. J Clin Oncol. 23:8706–8712. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Wang J, Hassett JM, Dayton MT and Kulaylat
MN: The prognostic superiority of log odds of positive lymph nodes
in stage III colon cancer. J Gastrointest Surg. 12:1790–1796. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Rosenberg R, Friederichs J, Schuster T,
Gertler R, Maak M, Becker K, Grebner A, Ulm K, Höfler H, Nekarda H
and Siewert JR: Prognosis of patients with colorectal cancer is
associated with lymph node ratio: A single-center analysis of 3,026
patients over a 25-year time period. Ann Surg. 248:968–978. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Zhang CH, Li YY, Zhang QW, Biondi A, Fico
V, Persiani R, Ni XC and Luo M: The prognostic impact of the
metastatic lymph nodes ratio in colorectal cancer. Front Oncol.
8:6282018. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ataseven B, Kümmel S, Weikel W, Heitz F,
Holtschmidt J, Lorenz-Salehi F, Kümmel A, Traut A, Blohmer J,
Harter P and du Bois A: Additional prognostic value of lymph node
ratio over pN staging in different breast cancer subtypes based on
the results of 1,656 patients. Arch Gynecol Obstet. 291:1153–1166.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Smith DD, Nelson RA and Schwarz RE: A
comparison of five competing lymph node staging schemes in a cohort
of resectable gastric cancer patients. Ann Surg Oncol. 21:875–882.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Tamura M, Matsumoto I, Saito D, Yoshida S,
Takata M and Takemura H: Lymph node ratio as a prognostic factor in
patients with pathological N2 non-small cell lung cancer. World J
Surg Oncol. 14:2952016. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Herr HW: Superiority of ratio based lymph
node staging for bladder cancer. J Urol. 169:943–945. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Persiani R, Cananzi FC, Biondi A, Paliani
G, Tufo A, Ferrara F, Vigorita V and D'Ugo D: Log odds of positive
lymph nodes in colon cancer: A meaningful ratio-based lymph node
classification system. World J Surg. 36:667–674. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Fang HY, Yang H, He ZS, Zhao H, Fu ZM,
Zhou FX and Zhou YF: Log odds of positive lymph nodes is superior
to the number- and ratio-based lymph node classification systems
for colorectal cancer patients undergoing curative (R0) resection.
Mol Clin Oncol. 6:782–788. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Arslan NC, Sokmen S, Canda AE, Terzi C and
Sarioglu S: The prognostic impact of the log odds of positive lymph
nodes in colon cancer. Colorectal Dis. 16:O386–O392. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Song YX, Gao P, Wang ZN, Tong LL, Xu YY,
Sun Z, Xing CZ and Xu HM: Which is the most suitable classification
for colorectal cancer, log odds, the number or the ratio of
positive lymph nodes? PLoS One. 6:e289372011. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Rosenberg R, Engel J, Bruns C, Heitland W,
Hermes N, Jauch KW, Kopp R, Pütterich E, Ruppert R, Schuster T, et
al: The prognostic value of lymph node ratio in a population-based
collective of colorectal cancer patients. Ann Surg. 251:1070–1078.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Zhang QW, Zhang CH, Pan YB, Biondi A, Fico
V, Persiani R, Wu S, Gao YJ, Chen HM, Shi OM, et al: Prognosis of
colorectal cancer patients is associated with the novel log odds of
positive lymph nodes scheme: Derivation and external validation. J
Cancer. 11:1702–1711. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Pei JP, Zhang CD, Fan YC and Dai DQ:
Comparison of different lymph node staging systems in patients with
resectable colorectal cancer. Front Oncol. 8:6712019. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Rausei S, Iovino D, Tenconi S, Mangano A,
Inversini D, Boni L, Rovera F, Dionigi G and Dionigi R: Impact of
lymph node ratio on survival of colorectal cancer patients. Int J
Surg. 11 (Suppl 1):S95–S99. 2013. View Article : Google Scholar : PubMed/NCBI
|