With the recent development of molecular targeted
therapies and immune checkpoint inhibitors (ICIs), the management
of metastatic brain tumors is undergoing major changes with respect
to the systemic treatment of cancer. Cytotoxic chemotherapy is
ineffective in treating intracranial lesions due to the blood-brain
barrier (BBB) (9). Therefore,
whole-brain radiotherapy (WBRT) has been the primary treatment for
metastatic brain tumors, especially in cases with multiple lesions
(10).
Since the development of irradiation techniques, an
emphasis has been placed on treatment strategies focusing on
long-term outcomes without severe clinical adverse effects
(11,12). A linear accelerator, which is
widely used in cancer treatment, is a device that speeds up
electrons with a small linear accelerator and collides them with a
metal target to produce X-rays of 4–10 MV. Recent progress in
image-guided radiation therapy and intensity-modulated radiation
therapy (IMRT) has made it possible to treat several brain
metastases at once in a non-invasive manner (13). The combination of
high-dose-delivery mode and volumetric modulated arc therapy, which
is an advanced type of IMRT, has made it possible to deliver a high
dose of radiation suitable for stereotactic radiosurgery in a short
period (14,15).
In recent years, the advent of immunotherapy has
revolutionized the systemic treatment of cancer, which has led to
the reconsideration of treatment strategies for brain metastasis.
We consider that it is necessary to review the management of brain
metastasis while factoring in the use of the novel therapeutic
agents. The present study reviews the general management of brain
metastasis and how it has been impacted by the recent advances in
systemic therapy and radiation therapy.
Although WBRT has been the standard treatment for
multiple brain metastases, cognitive dysfunction after WBRT is a
major clinical problem (16).
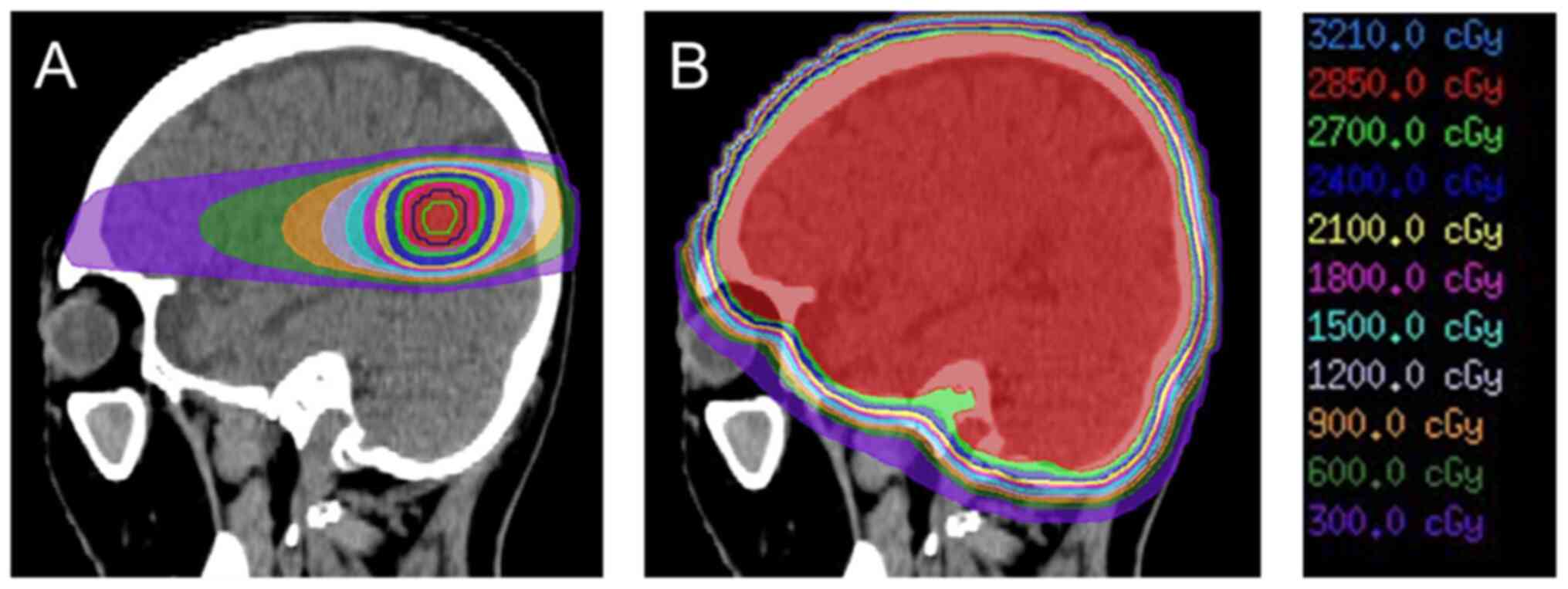
Recently, the stereotactic irradiation (STI) technique, involving a
linear accelerator, Gamma Knife or CyberKnife, was developed.
Fig. 1 represents the difference
in dose distribution for WBRT and STI in a metastatic brain tumor.
The role of STI has become more important, as it makes it possible
to focus the radiation on the lesion from multiple directions,
while minimizing the dose to the surrounding normal tissue.
Radiation necrosis (RN) after STI is one of the most frequent
adverse events. The incidence rate of RN after stereotactic
radiotherapy is reported to be 6–25% (17–20).
Minniti et al (21)
analyzed 310 metastatic brain tumors treated by STI and reported 75
cases of RN (24%), consisting of symptomatic 31 cases and
asymptomatic 44 cases. The incidence rate of RN is associated with
the maximum size of the treatment target tumor (22). According to Radiation Therapy
Oncology Group protocol 90–05, the maximum tolerated dose is
considered to be 24 Gy when the maximum diameter of the tumor is ≤2
cm (23). Recently, more detailed
radiation parameters, such as the normal brain volume receiving a
specific dose of 10 Gy or 12 Gy, have been widely used as
sophisticated predictors of RN (24). Putz et al (25) revealed that fractionated
stereotactic radiotherapy leads to a reduction in both RN risk
[hazard ratio (HR), 0.18; P=0.045] and local progression rate (HR,
0.47; P=0.015) compared with single-session radiosurgery.
In patients with SCLC, STI is considered
inappropriate for managing brain metastasis. According to the
American Society of Clinical Oncology-Society for
Neuro-Oncology-American Society for Radiation Oncology
collaborative guidelines for the treatment of brain metastases, STI
alone, without WBRT, should be offered to patients with 1–4 small
brain metastases, excluding cases of SCLC (34). A prospective randomized phase III
study is currently comparing STI with hippocampal-avoidance whole
brain radiotherapy in patients with 5–20 brain metastases
(ClinicalTrials.gov Identifier:
NCT03075072). WBRT is the primary method of managing brain
metastases in patients with SCLC. However, in a recent multicenter
retrospective cohort study, the median OS time after STI did not
significantly differ from that after WBRT in propensity
score-matched analyses (6.5 vs. 5.2 months, respectively; P=0.003)
(35).
Prophylactic cranial irradiation (PCI) has been used
for intracranial progression control and OS benefits in patients
with limited-stage SCLC (36,37).
According to a recent meta-analysis, patients treated with PCI
exhibited decreased brain metastasis (HR, 0.45; P<0.001) and
prolonged OS times (HR, 0.81; P<0.001) compared with those
without PCI treatment (38).
However, with the widespread use of diagnostic imaging techniques,
such as magnetic resonance imaging (MRI) and high-precision
radiotherapy techniques, the use of PCI has become controversial.
Pezzi et al (39) reported
that PCI did not prolong OS time and increase intracranial control
compared with MRI, as assessed using a propensity score-matching
analysis. Identification of appropriate patient groups for the use
of PCI will be necessary in the future.
A new generation of molecular targeted therapies is
expected to have notable therapeutic efficacy in intracranial
lesions (40). Osimertinib, a
third-generation EGFR-tyrosine kinase inhibitor (TKI), is highly
effective in controlling intracranial lesions, as shown by a subset
analysis of the FLAURA trial (41). In this study, 20 out of 22 patients
with EGFR mutation-positive advanced NSCLC, who had evaluable
intracranial lesions, achieved an intracranial response. Lorlatinib
is a third-generation anaplastic lymphoma kinase (ALK)-TKI that was
developed to improve the central nervous system (CNS) distribution
of alectinib and is expected to have a high suppressive effect on
CNS lesions (42). In the recently
reported CROWN trial, lorlatinib had an intracranial response
efficiency of 82% in patients with advanced ALK-positive NSCLC
without prior systemic therapy and with evaluable brain metastases
(43). A clinical randomized phase
III trial is currently evaluating the clinical advantage of upfront
radiotherapy before systemic therapy in patients with
driver-mutated NSCLC and asymptomatic brain metastases (ClinicalTrials.gov Identifier: NCT05236946).
Tiramurtinib, a second-generation Bruton's tyrosine
kinase inhibitor, has shown a good intracranial response in
patients with relapsed and refractory CNS lymphoma (44). Tucatinib, a HER2 inhibitor,
improves intracranial response efficiency when included in a
regimen consisting of trastuzumab and capecitabine for patients
with HER2-positive breast cancer and brain metastasis (45).
In recent years, cancer treatment has advanced
significantly, and prognostic techniques and systemic therapy,
especially in advanced-stage cancer, have changed markedly. For
example, the development of ICIs was given the Nobel Prize in
Physiology or Medicine in 2018 (46). Table
I represents frequently used ICIs in cancer therapy. Initially,
it was hypothesized that monoclonal antibodies, including ICIs,
could not pass through the BBB due to their large molecular size.
ICIs were considered to be ineffective against intracranial lesions
as they are antibody therapies and do not directly pass through the
BBB. However, ICIs have exhibited good results when used for the
treatment of brain metastasis, as they not only directly penetrate
the brain, but also stimulate a systemic immune response against
malignant cells (47). Goldberg
et al (48) evaluated the
efficacy of pembrolizumab, an anti-programmed cell death-1
antibody, for brain metastases in a phase II trial and reported
that 29.7% of patients with programmed cell death-ligand 1
(PD-L1)-positive NSCLC brain metastases responded to the treatment.
The CheckMate 204 study reported a response rate of 57% for
intracranial lesions in patients with brain metastases from
malignant melanoma treated with the anti-PD-L1 antibody nivolumab
in combination with the anti-cytotoxic T-lymphocyte-associated
protein 4 antibody ipilimumab (49). This result is similar to the
response rate of extracranial lesions in the same study. Further
studies are needed to identify whether ICIs or STIs should be
administered first. An ongoing clinical trial is currently
evaluating the timing of STI with respect to ICI (ClinicalTrials.gov Identifier: NCT04650490).
When deciding a treatment strategy for a single
patient, one of the principal components to be considered is
patient prognosis. In the 1990s, the Radiation Therapy Oncology
Group designated patient groups based on clinical trial data and
reported on the recursive partitioning analysis (RPA) score
(50), which was calculated from
Karnofsky Performance Status (51), age and extracranial disease status.
The median survival time was 7.1 months for RPA class I, 4.2 months
for class II and 2.3 months for class III. Due to its simplicity,
the RPA classification has been widely used for the assessment of
patient prognosis in a clinical setting. However, its disadvantage
is that it does not include the differences in prognosis due to the
number of brain lesions and primary cancer sites. Moreover, in the
era of its first use, brain metastasis was mainly treated with
WBRT.
For the treatment of brain metastases, it is
necessary to carefully consider the merits and drawbacks of various
treatments based on patient prognosis, primary pathology, size and
number of tumors, general patient condition, systemic therapy
options and performance status. According to the results of the
QUARTZ trial, additional WBRT for steroid administration provides
little benefit to patients, with a poor prognosis (56).
FLASH radiotherapy, applying irradiation at an
extremely high dose rate that is >1,000 times higher than the
conventional dose rate, is a potentially powerful therapeutic
modality for cancer treatment; it reduces associated side effects
and delivers safer radiation therapy (57). Montay-Gruel et al (58) reported that FLASH radiotherapy has
neuroprotective effects and suppresses neurocognitive deficits
after radiation therapy.
Treatment strategy for brain metastasis should be
discussed by a multidisciplinary cancer board, where physicians,
neurosurgeons, pathologists, radiologists and radiation oncologists
work together. Combination treatment, such as a combination of ICIs
and STI, augments the potential clinical efficacy in patients with
advanced cancer and brain metastasis (59). An ongoing prospective cohort trial
is evaluating the synergetic efficacy of the treatment response to
STI and ICI in patients with NSCLC and malignant melanoma
(ClinicalTrials.gov Identifier:
NCT03458455). In conclusion, since brain metastasis has a
significant impact on the quality of life of patients with
advanced-stage cancer, appropriate management is critical.
Not applicable.
Funding: No funding was received.
Not applicable.
AK wrote the manuscript and performed the literature
search. HY conceived this study and participated in its design and
coordination. HY and AK revised this report critically for
important intellectual content. Both authors have read and approved
the final manuscript. Data authentication is not applicable.
Written informed consent was obtained from the
patient for publication of the data in Fig. 1.
Not applicable.
The authors declare that they have no competing
interests.
|
1
|
Nayak L, Lee EQ and Wen PY: Epidemiology
of brain metastases. Curr Oncol Rep. 14:48–54. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Lin X and DeAngelis LM: Treatment of brain
metastases. J Clin Oncol. 33:3475–3484. 2015. View Article : Google Scholar
|
|
3
|
Sacks P and Rahman M: Epidemiology of
brain metastases. Neurosurg Clin N Am. 31:481–488. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Bhambhvani HP, Granucci M, Rodrigues A,
Kakusa BW and Hayden Gephart M: The primary sites leading to brain
metastases: Shifting trends at a tertiary care center. J Clin
Neurosci. 80:121–124. 2020. View Article : Google Scholar
|
|
5
|
Ostrom QT, Wright CH and Barnholtz-Sloan
JS: Brain metastases: Epidemiology. Handb Clin Neurol. 149:27–42.
2018. View Article : Google Scholar
|
|
6
|
Tabouret E, Chinot O, Metellus P, Tallet
A, Viens P and Gonçalves A: Recent trends in epidemiology of brain
metastases: An overview. Anticancer Res. 32:4655–4662.
2012.PubMed/NCBI
|
|
7
|
Hsu F, De Caluwe A, Anderson D, Nichol A,
Toriumi T and Ho C: Patterns of spread and prognostic implications
of lung cancer metastasis in an era of driver mutations. Curr
Oncol. 24:228–233. 2017. View Article : Google Scholar
|
|
8
|
Pestalozzi BC, Zahrieh D, Price KN,
Holmberg SB, Lindtner J, Collins J, Crivellari D, Fey MF, Murray E,
Pagani O, et al: Identifying breast cancer patients at risk for
Central Nervous System (CNS) metastases in trials of the
International Breast Cancer Study Group (IBCSG). Ann Oncol.
17:935–944. 2006. View Article : Google Scholar
|
|
9
|
Arvanitis CD, Ferraro GB and Jain RK: The
blood-brain barrier and blood-tumour barrier in brain tumours and
metastases. Nat Rev Cancer. 20:26–41. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
McTyre E, Scott J and Chinnaiyan P: Whole
brain radiotherapy for brain metastasis. Surg Neurol Int. 4 (Suppl
4):S236–S244. 2013. View Article : Google Scholar
|
|
11
|
Mehta SR, Suhag V, Semwal M and Sharma N:
Radiotherapy: Basic concepts and recent advances. Med J Armed
Forces India. 66:158–162. 2010. View Article : Google Scholar
|
|
12
|
Gelband H, Jha P, Sankaranarayanan R and
Horton S: Cancer: Disease Control Priorities. Third Edition.
(Volume 3). The International Bank for Reconstruction and
Development/The World Bank; Washington, D.C.: 2015
|
|
13
|
Xing L, Thorndyke B, Schreibmann E, Yang
Y, Li TF, Kim GY, Luxton G and Koong A: Overview of image-guided
radiation therapy. Med Dosim. 31:91–112. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Otto K: Volumetric modulated arc therapy:
IMRT in a single gantry arc. Med Phys. 35:310–317. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sapkaroski D, Osborne C and Knight KA: A
review of stereotactic body radiotherapy-is volumetric modulated
arc therapy the answer? J Med Radiat Sci. 62:142–151. 2015.
View Article : Google Scholar
|
|
16
|
DeAngelis LM, Delattre JY and Posner JB:
Radiation-induced dementia in patients cured of brain metastases.
Neurology. 39:789–796. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Ali FS, Arevalo O, Zorofchian S, Patrizz
A, Riascos R, Tandon N, Blanco A, Ballester LY and Esquenazi Y:
Cerebral radiation necrosis: Incidence, pathogenesis, diagnostic
challenges, and future opportunities. Curr Oncol Rep. 21:662019.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kim JM, Miller JA, Kotecha R, Xiao R,
Juloori A, Ward MC, Ahluwalia MS, Mohammadi AM, Peereboom DM,
Murphy ES, et al: The risk of radiation necrosis following
stereotactic radiosurgery with concurrent systemic therapies. J
Neurooncol. 133:357–368. 2017. View Article : Google Scholar
|
|
19
|
Donovan EK, Parpia S and Greenspoon JN:
Incidence of radionecrosis in single-fraction radiosurgery compared
with fractionated radiotherapy in the treatment of brain
metastasis. Curr Oncol. 26:e328–e333. 2019. View Article : Google Scholar
|
|
20
|
Vellayappan BA, McGranahan T, Graber J,
Taylor L, Venur V, Ellenbogen R, Sloan AE, Redmond KJ, Foote M,
Chao ST, et al: Radiation necrosis from stereotactic
radiosurgery-how do we mitigate? Curr Treat Options Oncol.
22:572021. View Article : Google Scholar
|
|
21
|
Minniti G, Clarke E, Lanzetta G, Osti MF,
Trasimeni G, Bozzao A, Romano A and Enrici RM: Stereotactic
radiosurgery for brain metastases: Analysis of outcome and risk of
brain radionecrosis. Radiat Oncol. 6:482011. View Article : Google Scholar
|
|
22
|
Kohutek ZA, Yamada Y, Chan TA, Brennan CW,
Tabar V, Gutin PH, Yang TJ, Rosenblum MK, Ballangrud Å, Young RJ,
et al: Long-term risk of radionecrosis and imaging changes after
stereotactic radiosurgery for brain metastases. J Neurooncol.
125:149–156. 2015. View Article : Google Scholar
|
|
23
|
Shaw E, Scott C, Souhami L, Dinapoli R,
Kline R, Loeffler J and Farnan N: Single dose radiosurgical
treatment of recurrent previously irradiated primary brain tumors
and brain metastases: Final report of RTOG protocol 90-05. Int J
Radiat Oncol Biol Phys. 47:291–298. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Loo M, Clavier JB, Attal Khalifa J, Moyal
E and Khalifa J: Dose-Response effect and dose-toxicity in
stereotactic radiotherapy for brain metastases: A review. Cancers
(Basel). 13:60862021. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Putz F, Weissmann T, Oft D, Schmidt MA,
Roesch J, Siavooshhaghighi H, Filimonova I, Schmitter C, Mengling
V, Bert C, et al: FSRT vs. SRS in brain metastases-differences in
local control and radiation Necrosis-A volumetric study. Front
Oncol. 10:5591932020. View Article : Google Scholar
|
|
26
|
Brown PD, Jaeckle K, Ballman KV, Farace E,
Cerhan JH, Anderson SK, Carrero XW, Barker FG II, Deming R, Burri
SH, et al: Effect of radiosurgery alone vs. radiosurgery with whole
brain radiation therapy on cognitive function in patients with 1 to
3 brain metastases: A randomized clinical trial. JAMA. 316:401–409.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Yamamoto M, Serizawa T, Shuto T, Akabane
A, Higuchi Y, Kawagishi J, Yamanaka K, Sato Y, Jokura H, Yomo S, et
al: Stereotactic radiosurgery for patients with multiple brain
metastases (JLGK0901): A multi-institutional prospective
observational study. Lancet Oncol. 15:387–395. 2014. View Article : Google Scholar
|
|
28
|
Patchell RA, Tibbs PA, Regine WF, Dempsey
RJ, Mohiuddin M, Kryscio RJ, Markesbery WR, Foon KA and Young B:
Postoperative radiotherapy in the treatment of single metastases to
the brain: A randomized trial. JAMA. 280:1485–1489. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Patchell RA, Tibbs PA, Walsh JW, Dempsey
RJ, Maruyama Y, Kryscio RJ, Markesbery WR, Macdonald JS and Young
B: A randomized trial of surgery in the treatment of single
metastases to the brain. N Engl J Med. 322:494–500. 1990.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Kayama T, Sato S, Sakurada K, Mizusawa J,
Nishikawa R, Narita Y, Sumi M, Miyakita Y, Kumabe T, Sonoda Y, et
al: Effects of surgery with salvage stereotactic radiosurgery
versus surgery with whole-brain radiation therapy in patients with
one to four brain metastases (JCOG0504): A phase III,
noninferiority, randomized controlled trial. J Clin Oncol.
JCO20187861862018.
|
|
31
|
Brown PD, Ballman KV, Cerhan JH, Anderson
SK, Carrero XW, Whitton AC, Greenspoon J, Parney IF, Laack NNI,
Ashman JB, et al: Postoperative stereotactic radiosurgery compared
with whole brain radiotherapy for resected metastatic brain disease
(NCCTG N107C/CEC·3): A multicentre, randomised, controlled, phase 3
trial. Lancet Oncol. 18:1049–1060. 2017. View Article : Google Scholar
|
|
32
|
Kępka L, Tyc-Szczepaniak D, Bujko K,
Olszyna-Serementa M, Michalski W, Sprawka A, Trąbska-Kluch B,
Komosińska K, Wasilewska-Teśluk E and Czeremszyńska B: Stereotactic
radiotherapy of the tumor bed compared to whole brain radiotherapy
after surgery of single brain metastasis: Results from a randomized
trial. Radiother Oncol. 121:217–224. 2016. View Article : Google Scholar
|
|
33
|
Randall Patrinely J Jr, Funck-Brentano E,
Nguyen K, Rapisuwon S, Salem JE, Gibney GT, Carlino M and Johnson
DB: A multicenter analysis of immune checkpoint inhibitors as
adjuvant therapy following treatment of isolated brain metastasis.
Oncologist. 26:e505–e507. 2021. View Article : Google Scholar
|
|
34
|
Vogelbaum MA, Brown PD, Messersmith H,
Brastianos PK, Burri S, Cahill D, Dunn IF, Gaspar LE, Gatson NTN,
Gondi V, et al: Treatment for brain metastases: ASCO-SNO-ASTRO
guideline. J Clin Oncol. 40:492–516. 2022. View Article : Google Scholar
|
|
35
|
Rusthoven CG, Yamamoto M, Bernhardt D,
Smith DE, Gao D, Serizawa T, Yomo S, Aiyama H, Higuchi Y, Shuto T,
et al: Evaluation of first-line radiosurgery vs. whole-brain
radiotherapy for small cell lung cancer brain metastases: The
FIRE-SCLC Cohort Study. JAMA Oncol. 6:1028–1037. 2020. View Article : Google Scholar
|
|
36
|
Aupérin A, Arriagada R, Pignon JP, Le
Péchoux C, Gregor A, Stephens RJ, Kristjansen PE, Johnson BE, Ueoka
H, Wagner H and Aisner J: Prophylactic cranial irradiation for
patients with small-cell lung cancer in complete remission.
Prophylactic Cranial Irradiation Overview Collaborative Group. N
Engl J Med. 341:476–484. 1999. View Article : Google Scholar
|
|
37
|
Arriagada R, Le Chevalier T, Borie F,
Rivière A, Chomy P, Monnet I, Tardivon A, Viader F, Tarayre M and
Benhamou S: Prophylactic cranial irradiation for patients with
small-cell lung cancer in complete remission. J Natl Cancer Inst.
87:183–190. 1995. View Article : Google Scholar
|
|
38
|
Yin X, Yan D, Qiu M, Huang L and Yan SX:
Prophylactic cranial irradiation in small cell lung cancer: A
systematic review and meta-analysis. BMC Cancer. 19:952019.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Pezzi TA, Fang P, Gjyshi O, Feng L, Liu S,
Komaki R and Lin SH: Rates of overall survival and intracranial
control in the magnetic resonance imaging Era for patients with
limited-stage small cell lung cancer with and without prophylactic
cranial irradiation. JAMA Netw Open. 3:e2019292020. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Zhong L, Li Y, Xiong L, Wang W, Wu M, Yuan
T, Yang W, Tian C, Miao Z, Wang T and Yang S: Small molecules in
targeted cancer therapy: Advances, challenges, and future
perspectives. Signal Transduct Target Ther. 6:2012021. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Ramalingam SS, Vansteenkiste J, Planchard
D, Cho BC, Gray JE, Ohe Y, Zhou C, Reungwetwattana T, Cheng Y,
Chewaskulyong B, et al: Overall Survival with Osimertinib in
Untreated, EGFR-Mutated Advanced NSCLC. N Engl J Med. 382:41–50.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Ando K, Manabe R, Kishino Y, Kusumoto S,
Yamaoka T, Tanaka A, Ohmori T and Sagara H: Comparative efficacy
and safety of lorlatinib and alectinib for ALK-Rearrangement
positive advanced non-small cell lung cancer in asian and non-asian
patients: A systematic review and network meta-analysis. Cancers
(Basel). 13:37042021. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Shaw AT, Bauer TM, de Marinis F, Felip E,
Goto Y, Liu G, Mazieres J, Kim DW, Mok T, Polli A, et al:
First-Line lorlatinib or crizotinib in advanced ALK-positive lung
cancer. N Engl J Med. 383:2018–2029. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Narita Y, Nagane M, Mishima K, Terui Y,
Arakawa Y, Yonezawa H, Asai K, Fukuhara N, Sugiyama K, Shinojima N,
et al: Phase I/II study of tirabrutinib, a second-generation
Bruton's tyrosine kinase inhibitor, in relapsed/refractory primary
central nervous system lymphoma. Neuro Oncol. 23:122–133. 2021.
View Article : Google Scholar
|
|
45
|
Murthy RK, Loi S, Okines A, Paplomata E,
Hamilton E, Hurvitz SA, Lin NU, Borges V, Abramson V, Anders C, et
al: Tucatinib, trastuzumab, and capecitabine for HER2-Positive
metastatic breast cancer. N Engl J Med. 382:597–609. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Huang PW and Chang JW: Immune checkpoint
inhibitors win the 2018 Nobel Prize. Biomed J. 42:299–306. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Corroyer-Dulmont A, Jaudet C, Frelin AM,
Fantin J, Weyts K, Vallis KA, Falzone N, Sibson NR, Chérel M,
Kraeber-Bodéré F, et al: Radioimmunotherapy for brain metastases:
The potential for inflammation as a target of choice. Front Oncol.
11:7145142021. View Article : Google Scholar
|
|
48
|
Goldberg SB, Gettinger SN, Mahajan A,
Chiang AC, Herbst RS, Sznol M, Tsiouris AJ, Cohen J, Vortmeyer A,
Jilaveanu L, et al: Pembrolizumab for patients with melanoma or
non-small-cell lung cancer and untreated brain metastases: Early
analysis of a non-randomised, open-label, phase 2 trial. Lancet
Oncol. 17:976–983. 2016. View Article : Google Scholar
|
|
49
|
Tawbi HA, Forsyth PA, Hodi FS, Algazi AP,
Hamid O, Lao CD, Moschos SJ, Atkins MB, Lewis K, Postow MA, et al:
Long-term outcomes of patients with active melanoma brain
metastases treated with combination nivolumab plus ipilimumab
(CheckMate 204): Final results of an open-label, multicentre, phase
2 study. Lancet Oncol. 22:1692–1704. 2021. View Article : Google Scholar
|
|
50
|
Gaspar L, Scott C, Rotman M, Asbell S,
Phillips T, Wasserman T, McKenna WG and Byhardt R: Recursive
partitioning analysis (RPA) of prognostic factors in three
Radiation Therapy Oncology Group (RTOG) brain metastases trials.
Int J Radiat Oncol Biol Phys. 37:745–751. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Schag CC, Heinrich RL and Ganz PA:
Karnofsky performance status revisited: Reliability, validity, and
guidelines. J Clin Oncol. 2:187–193. 1984. View Article : Google Scholar
|
|
52
|
Sperduto PW, Berkey B, Gaspar LE, Mehta M
and Curran W: A new prognostic index and comparison to three other
indices for patients with brain metastases: An analysis of 1,960
patients in the RTOG database. Int J Radiat Oncol Biol Phys.
70:510–514. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Sperduto PW, Kased N, Roberge D, Xu Z,
Shanley R, Luo X, Sneed PK, Chao ST, Weil RJ, Suh J, et al: Summary
report on the graded prognostic assessment: An accurate and facile
diagnosis-specific tool to estimate survival for patients with
brain metastases. J Clin Oncol. 30:419–425. 2012. View Article : Google Scholar
|
|
54
|
Sperduto PW, Yang TJ, Beal K, Pan H, Brown
PD, Bangdiwala A, Shanley R, Yeh N, Gaspar LE, Braunstein S, et al:
Estimating survival in patients with lung cancer and brain
metastases: An update of the graded prognostic assessment for lung
cancer using molecular markers (Lung-molGPA). JAMA Oncol.
3:827–831. 2017. View Article : Google Scholar
|
|
55
|
Sperduto PW, Mesko S, Li J, Cagney D,
Aizer A, Lin NU, Nesbit E, Kruser TJ, Chan J, Braunstein S, et al:
Beyond an updated graded prognostic assessment (Breast GPA): A
prognostic index and trends in treatment and survival in breast
cancer brain metastases from 1985 to today. Int J Radiat Oncol Biol
Phys. 107:334–343. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Mulvenna P, Nankivell M, Barton R,
Faivre-Finn C, Wilson P, McColl E, Moore B, Brisbane I, Ardron D,
Holt T, et al: Dexamethasone and supportive care with or without
whole brain radiotherapy in treating patients with non-small cell
lung cancer with brain metastases unsuitable for resection or
stereotactic radiotherapy (QUARTZ): Results from a phase 3,
non-inferiority, randomised trial. Lancet. 388:2004–2014. 2016.
View Article : Google Scholar
|
|
57
|
Lin B, Gao F, Yang Y, Wu D, Zhang Y, Feng
G, Dai T and Du X: FLASH radiotherapy: History and future. Front
Oncol. 11:6444002021. View Article : Google Scholar
|
|
58
|
Montay-Gruel P, Acharya MM, Petersson K,
Alikhani L, Yakkala C, Allen BD, Ollivier J, Petit B, Jorge PG,
Syage AR, et al: Long-term neurocognitive benefits of FLASH
radiotherapy driven by reduced reactive oxygen species. Proc Natl
Acad Sci USA. 116:10943–10951. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Shepard MJ, Xu Z, Donahue J, Eluvathingal
Muttikkal TJ, Cordeiro D, Hansen L, Mohammed N, Gentzler RD, Larner
J, Fadul CE and Sheehan JP: Stereotactic radiosurgery with and
without checkpoint inhibition for patients with metastatic
non-small cell lung cancer to the brain: A matched cohort study. J
Neurosurg. 133:685–692. 2019. View Article : Google Scholar
|