Introduction
Breast cancer, one of the most common malignant
tumor types in females, is the leading cause of death in women
worldwide (1). According to global
cancer statistics, in 2020, 2.26 million new cases of female breast
cancer were diagnosed, accounting for about a quarter of female
malignancies, and the death toll from breast cancer was 680,000,
ranking first among female malignancies (2). Although early detection, early
diagnosis and early treatment have contributed to a gradual decline
in breast cancer mortality over the past few decades, the prognosis
of patients remains poor (3). New
prognostic biomarkers are still needed to develop targeted
therapies and improve patient survival.
Recently, several studies have demonstrated the
importance of the tumor immune microenvironment in cancer
progression (4). Among them, the
interaction between tumor cells and immune cells has become the
focus of current attention (5).
Tumor-infiltrating lymphocytes (TILs) are important components of
the tumor immune microenvironment and have a key role in the local
immune response of cancer (6). The
appearance of TILs is a sign of the immune response of the host's
immune system to tumor antigens and reflects the local immune
response of the tumor. The level of TILs in the primary tumor
reflects the body's anti-tumor potential and their quantity also
indicates the therapeutic effect against the tumor (7,8). In
the adaptive immune system, cytotoxic (CD8+) T cells are
the primary immune cells involved in recognizing and killing tumors
(9,10). In breast cancer, the relationship
between the expression of CD8+ TILs and prognosis has
remained to be fully elucidated. Most previous studies on
CD8+ T lymphocytes in breast cancer reported that
CD8+ T cells were associated with improved prognosis
(11–13). However, other studies were in
disagreement with this (14). In
addition to their association with survival, certain studies have
also found a link between the presence of immune cells and the
effect of chemotherapy (15,16).
Therefore, analyzing the prognostic value of CD8+ T
cells in breast cancer may improve prognosis and enhance the
application of individualized and customized therapy.
The objective of the present systematic review and
meta-analysis was to investigate the prognostic value of
CD8+ T cells in breast cancer and to explore the
association between CD8+ T cells and the pathological
characteristics of patients with breast cancer in order to provide
new prognostic biomarkers for the clinical treatment of breast
cancer.
Materials and methods
Protocol and registration
The present systematic review and meta-analysis were
performed based on the requirements of the Preferred Reporting
Items for Systematic Reviews and Meta-Analyses statement (17). The protocol was registered at
PROSPERO with the following ID: CRD42022313171.
Literature inclusion and exclusion
criteria
The inclusion criteria were as follows: Prospective
or retrospective studies were included in this meta-analysis;
patients with breast cancer were the subject of the research; the
language was limited to English. The following exclusion criteria
were applied: Duplicate publications; research without full text,
incomplete information or inability to conduct data extraction;
animal experiments; reviews and systematic reviews.
Search strategy
For the present meta-analysis, the Pubmed
(https://pubmed.ncbi.nlm.nih.gov/),
Embase (https://www.embase.com) and Cochrane
Library (https://www.cochranelibrary.com/) databases were
searched from the establishment of the database up until to
November 2021. The search terms were mainly as follows: ‘Breast
neoplasm’, ‘breast tumor’, ‘breast cancer’, ‘breast carcinoma’ AND
‘CD8-positive T-lymphocytes’, ‘CD8-positive lymphocyte’, ‘CD8+T’
AND ‘prognosis’, ‘prognostic’, ‘overall survival’, ‘disease-free
survival’ and ‘progression-free survival’. As the analysis was
based on published studies, neither ethical approval nor patient
consent was required.
Literature screening and data
extraction
The literature search, screening and information
extraction were all independently completed by two researchers (YPS
and YLK). In case of any doubts or disagreements, the decision was
made after discussion or consultation with the third researcher
(XL). The data extracted included the author, year of publication,
country, study design, sample size, median age, median follow-up
time, location of CD8+ TILs and the indicators for
evaluating outcome, including hazard ratio (HR) for overall
survival (OS) and disease-free survival (DFS).
Literature quality assessment
The quality of evidence for each study was assessed
by two independent researchers (YPS and YLK) using the
Newcastle-Ottawa Scale (NOS) (18). The NOS includes 4 items (4 points)
for ‘Research Subject Selection’, 1 item (2 points) for
‘Comparability between Groups’ and 3 items (3 points) for ‘Result
Measurement’, with a full score of 9 points and studies with ≥7 are
regarded as high-quality literature, while those with <7 are
classified as lower-quality literature. When the ratings were
inconsistent, the score was decided through discussion or
consultation with the third researcher (XL). Publication bias was
assessed by two independent researchers (YPS and YLK) using funnel
plots and Egger's test. The sensitivity analysis was performed by
two independent researchers (YPS and YLK) if necessary. In case of
any doubts or disagreements, the decision was made after discussion
or consultation with the third researcher (XL).
Data synthesis and statistical
analysis
STATA 15.1 (Stata Corporation) was used to analyze
the data, with P<0.05 suggesting a statistical significance. The
HR (95% CI) was used to evaluate the OS and DFS. Cochran's Q-test
and I2 statistics were used to evaluate the
heterogeneity among the included studies. If the heterogeneity test
result was P≥0.1 or I2≤50%, it indicated that there was
no significant heterogeneity among studies. Subsequently, the
fixed-effects Mantel-Haenszel model (19) was used for combined OR analysis and
the fixed-effects Inverse-Variance model was used for pooled HR
evaluation. Otherwise, if P<0.1 or I2>50%, it
indicated that there was statistically significant heterogeneity
and the random-effects model (REM) according to DerSimonian and
Laird (20) was used to analyze
the pooled results. Sensitivity analysis and subgroup analysis were
used to identify the source of heterogeneity. A funnel plot and
Egger's test were jointly used to assess the publication bias.
In a fixed-effects model (FEM) (21), it is assumed that all included
studies share a common true effect size. The sampling error is the
only one source of variation, which is equal to the within-study
error variance. The weight assigned to each study is based on the
inverse of the within-study error variance, which is related to the
precision of the estimation of each study. In general, studies with
a larger sample yield a more precise estimate of the population
mean and thus will be assigned more weight compared to those with a
smaller sample. Therefore, studies with a small sample will be
neglected more easily. By contrast, in an REM (22,23),
the true effect size changes according to different included
studies. There are two levels of sampling, and therefore two
sources of variance. The overall study error variance in a
random-effects meta-analysis contains two components: One is the
within-study error variance due to sampling error (same as in the
FEM) and the other is the inter-study variance resulting from the
difference in effect size distribution. Therefore, the weight
assigned to each study is based on the inverse of the sum of the
within-study error variance and the inter-study variance. Different
from the FEM, studies with a small sample may also be assigned more
weight if the inter-study variance is small. If there is no
significant heterogeneity between studies, the inter-study variance
is zero. The result estimated from the REM would then be identical
to that of the FEM. The challenge in the REM is how to estimate the
inter-study variance. The DerSimonian and Laird estimate is easy to
compute and is qualitatively consistent with the heterogeneity test
based on the Q statistic.
Results
Results of the literature search
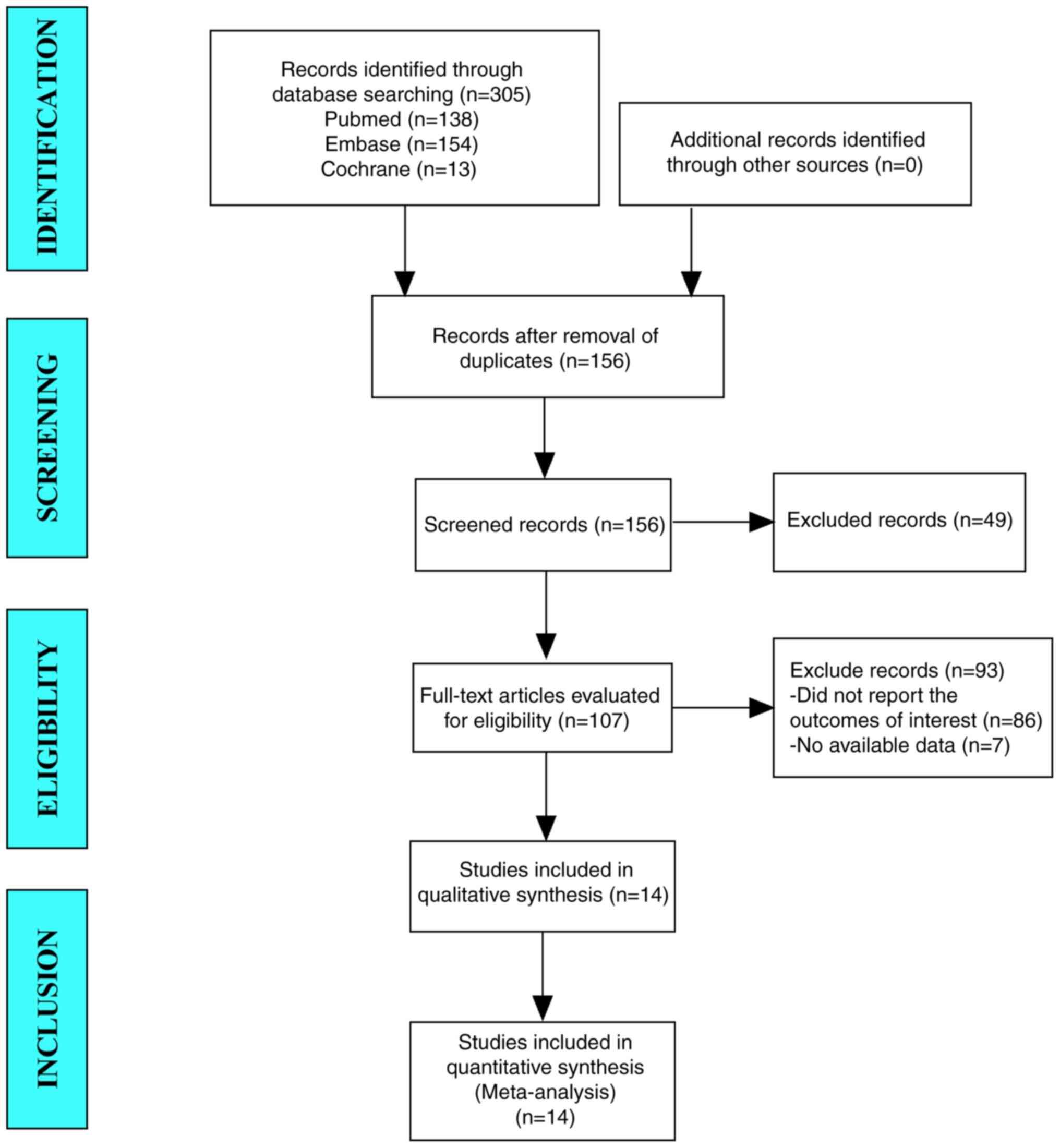
A total of 305 studies were retrieved from the
Pubmed, Embase and Cochrane Library databases via a literature
search. After the removal of duplicates, 156 studies were
preliminarily screened by browsing the titles and abstracts with 49
studies excluded, retaining 107 studies for further full-text
screening. After browsing through the full text, 14 studies were
retained as eligible for inclusion. Finally, 14 studies were
included in the meta-analysis. Fig.
1 illustrates the flowchart of the selection process with
reasons for exclusions. Baseline characteristics and quality
assessment of the included studies. A total of 14 retrospective
studies (11,12,14,24–34)
were included in the present meta-analysis. The sample size of
patients was 22,222 in total. The patients from 8 articles were
from Asia, while the patients from 5 articles were from Europe.
Furthermore, the patients from Ali et al (29) were from several countries. All of
the studies were published between 2011 and 2019. Locations of
CD8+ TILs included Intratumoral, Peritumoral and
Intratumoral & Peritumoral. The NOS scores used for quality
assessment were all >7. The baseline characteristics of all
included studies are listed in Table
I. The CD8+ T-cell infiltration level was derived from the
original studies. The CD8+ T-cell infiltration was assessed via
immunohistochemistry staining and evaluated manually by the number
of positive cells or the density of positive cells. Since the
evaluation methods and cutoff points to separate high and low
infiltration levels vary between studies as indicated in Table I, it is hard to use the same
criterion to evaluate the CD8+ T-cell infiltration level for all
the included studies. Therefore, the cutoff value for defining
high-level CD8+ T-cell infiltration or positive CD8+ T-cells was
determined according to each included study separately, as
indicated in Table I.
 | Table I.Baseline characteristics and quality
assessment of the included studies. |
Table I.
Baseline characteristics and quality
assessment of the included studies.
| First author,
year | Country | Sample size | Median age,
years | Median follow-up
time, months | Location of
CD8+ TILs | Evaluation
method | Cutoff
(positive/high level) | Outcome | NOS score | (Refs.) |
|---|
| Mahmoud, 2011 | UK | 1902 | 55 | 127 | P | Number of positive
cells | ≥2 | OS | 7 | (12) |
| Liu, 2011 | China | 1270 | 52 | 66 | I/P | Infiltrating
density | Median | OS/DFS | 7 | (14) |
| Liu, 2012 | China | 3992 | 58.9 | 151.2 | I | Count of positive
cells | ≥1 | OS | 7 | (11) |
| Ma, 2012 | China | 81 | / | / | I&P | Positive cell
number | Median | OS | 8 | (24) |
| Mohammed, 2013 | UK | 338 | / | 164 | I&P | Number of
lymphocytes | ≥40 | OS | 7 | (25) |
| Kim, 2013 | Korea | 72 | 49 | 33.7 | I&P | Number of CD8+ T
cells | >60 | DFS | 7 | (26) |
| Sun, 2014 | China | 218 | 57.6 | 72 | I&P | Infiltrating
density | Median | OS/DFS | 8 | (27) |
| Chen, 2014 | China | 332 | / | 152 | I&P | Intensity of
infiltrate | Infiltrate score
>0 | OS/DFS | 8 | (28) |
| Ali, 2014 | Several
countries | 12439 | / | 114.8 | I | Absolute count | >0 | OS | 7 | (29) |
| Chung, 2017 | Korea | 377 | 51 | 69 | I&P | Number of TIL
subsets | Median | DFS | 7 | (30) |
| Liu, 2017 | China | 647 | 55 | 21.5 | I/P | CD8+ TIL count | sTIL ≥3, iTIL
≥1 | OS | 7 | (31) |
| Papaioannou,
2019 | Greece | 207 | 60 | 70 | P | Absolute
number | Median | OS/DFS | 8 | (32) |
| Groot, 2019 | Netherlands | 196 | / | 55.2 | I | Number of CD8+ | Median | DFS | 8 | (33) |
| Catacchio,
2019 | Italy | 151 | 57 | 63 | I&P/I/P | Number of TILs | Median | DFS | 8 | (34) |
Results of the meta-analysis
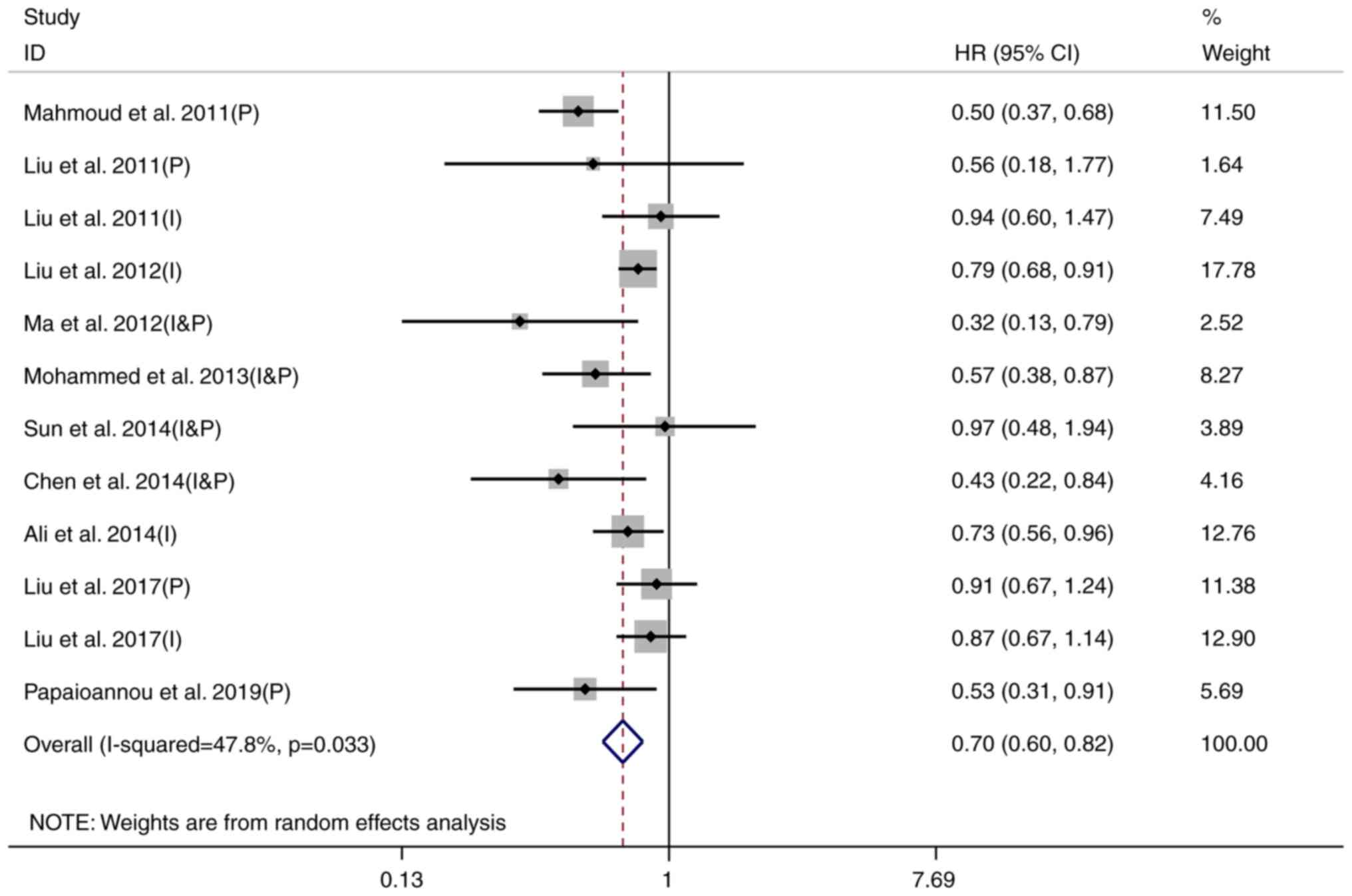
CD8+ T-cell infiltration and OS
The results of the heterogeneity test indicated
significant heterogeneity among the studies (I2=47.8%,
P=0.033). Since the sensitivity analysis did not find any
individual study that had a significant impact on the results of
the meta-analysis, the REM was used to pool the results. The pooled
results indicated that a high CD8+ T-cell infiltration
level was significantly related to better OS of patients with
breast cancer (HR=0.70, 95% CI: 0.60-0.82, P<0.001), as
indicated in Fig. 2.
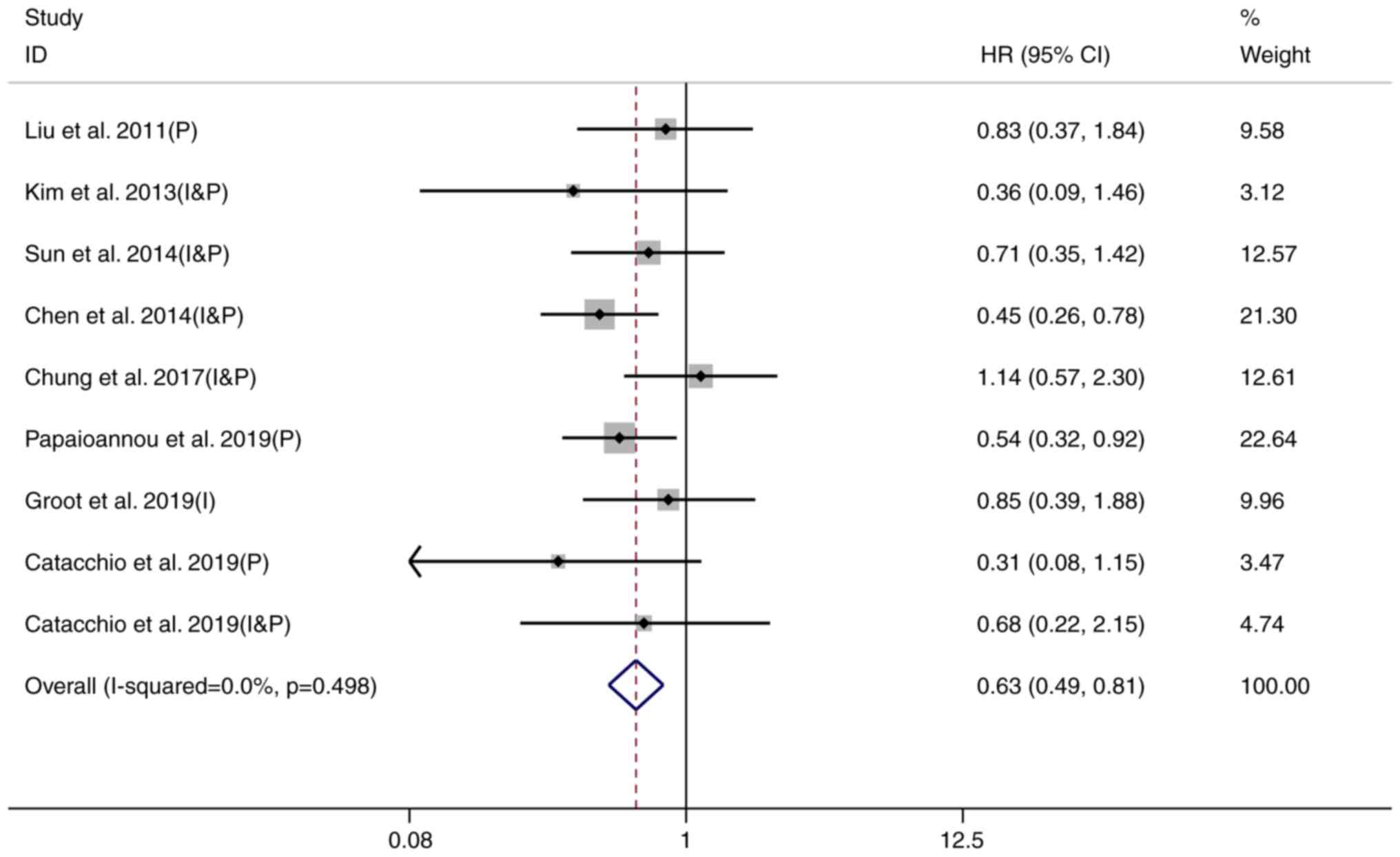
CD8+ T-cell infiltration
and DFS
In addition, the relationship between
CD8+ T-cell infiltration and DFS in patients with breast
cancer was explored. By excluding each included study one by one
and analyzing the pooled results of the remaining studies (HR and
95% CI), the sensitivity analysis indicated that the study on the
CD8+ T-cell infiltration within the tumor (intratumoral TILs) and
DFS by Catacchio et al (34) had an excessive impact on the
results, as indicated in Fig. 3
and Fig. S1, Fig. S2, Fig. S3. The results of the I2
heterogeneity test were reduced from 33.7 to 0.0% when the study of
Catacchio et al (34)
(intratumoral TILs) was excluded. Therefore, in the subsequent
analysis of the relationship between CD8+ T-cell infiltration and
DFS, the study by Catacchio et al (34) (intratumoral TILs) was excluded. The
results of the heterogeneity test revealed no significant
heterogeneity among the studies (I2=0.0%, P=0.498), and
thus, an FEM was used. The pooled results suggested that a high
CD8+ T-cell infiltration level was significantly related
to better DFS of patients with breast cancer (HR=0.63, 95% CI:
0.49-0.81, P<0.001), as presented in Fig. 3.
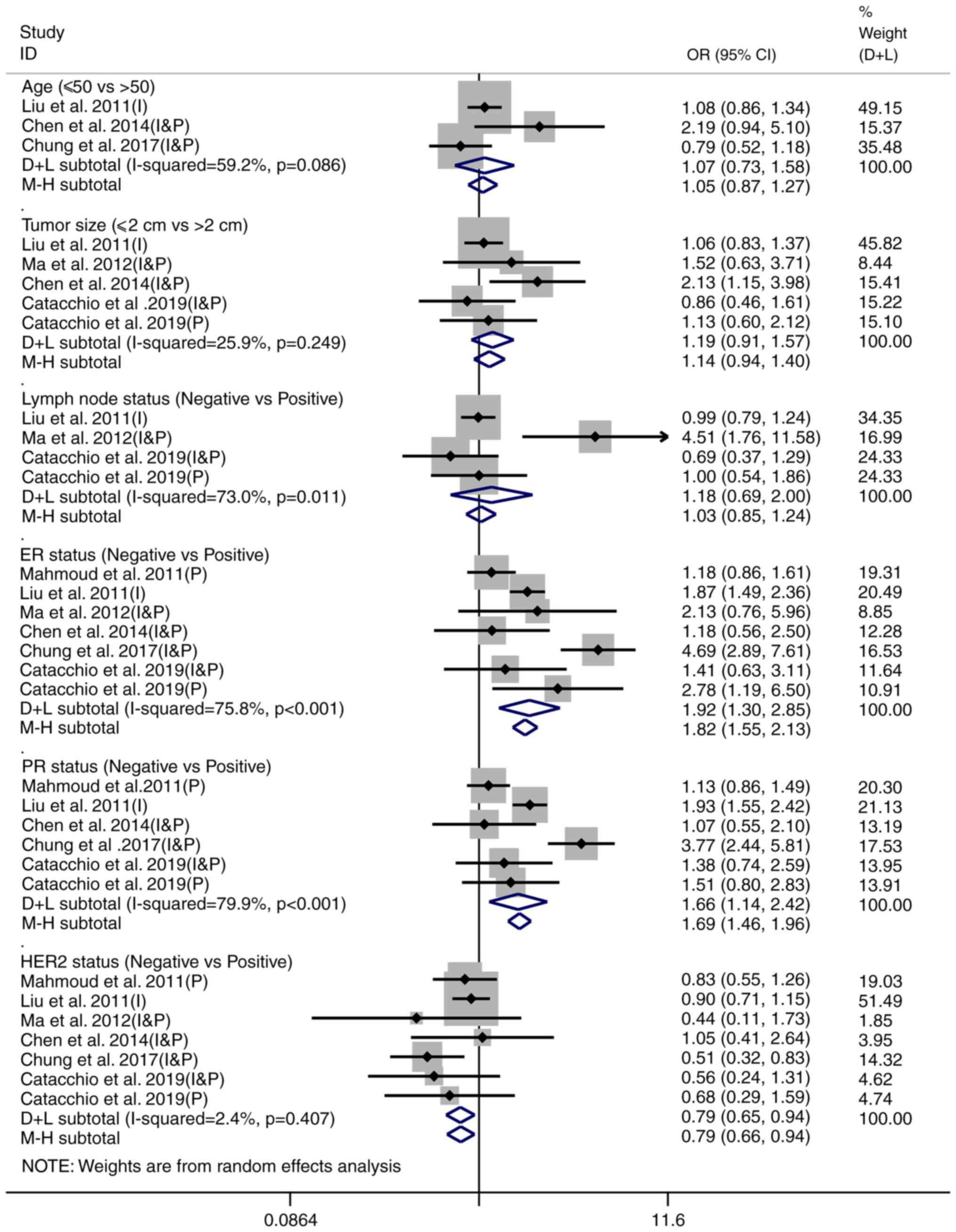
CD8+ T-cell infiltration
and clinicopathological characteristics of breast cancer
Furthermore, the relationship between
CD8+ T-cell infiltration and clinicopathological
characteristics, including clinical stage, N stage and performance
status, was analyzed (Fig. 4).
Both random-effects (D+L) and fixed-effects (M-H) models were used
to analyze the pooled OR value. It was indicated that the
estimation from the REM was different from the FEM when there was
significant heterogeneity between studies, and the difference
vanished when no heterogeneity existed (i.e. for HER2 status).
These results agree with the above discussion regarding the REM and
FEM. The result yielded from the REM (D+L) was adopted when there
was significant heterogeneity among studies (I2>50%);
otherwise, the estimation from the FEM (M-H) was used.
A high CD8+ T-cell infiltration level was
significantly associated with decreased expression of ER (OR=1.92,
95% CI: 1.30-2.85, P=0.001; I2=75.8%, P<0.001) and PR
(OR=1.66, 95% CI: 1.14-2.42, P=0.008; I2=79.9%,
P<0.001) and increased HER2 expression (OR=0.79, 95% CI:
0.66-0.94, P=0.010; I2=2.4%, P=0.407) in patients with
breast cancer, while there was no significant association between
CD8+ T-cell infiltration and age, tumor size and lymph
node status of patients with breast cancer (P>0.05), as
indicated in Table II.
| Table II.Relationship between CD8+
T-cell infiltration and clinicopathological characteristics of
patients with breast cancer. |
Table II.
Relationship between CD8+
T-cell infiltration and clinicopathological characteristics of
patients with breast cancer.
|
|
| Test for
relationship |
|---|
| Characteristic | Number of
studies |
|
|---|
| OR | 95% CI | P-value |
|---|
| Age, years (≤50 vs.
>50) | 3 | 1.07 | 0.73-1.58 | 0.717 |
| Tumor size, cm (≤2
vs. >2) | 5 | 1.14 | 0.94-1.40 | 0.211 |
| Lymph node status
(negative vs. positive) | 4 | 1.18 | 0.69-2.00 | 0.549 |
| ER status (negative
vs. positive) | 7 | 1.92 | 1.30-2.85 | 0.001 |
| PR status (negative
vs. positive) | 6 | 1.66 | 1.14-2.42 | 0.008 |
| HER2 status
(negative vs. positive) | 7 | 0.79 | 0.66-0.94 | 0.010 |
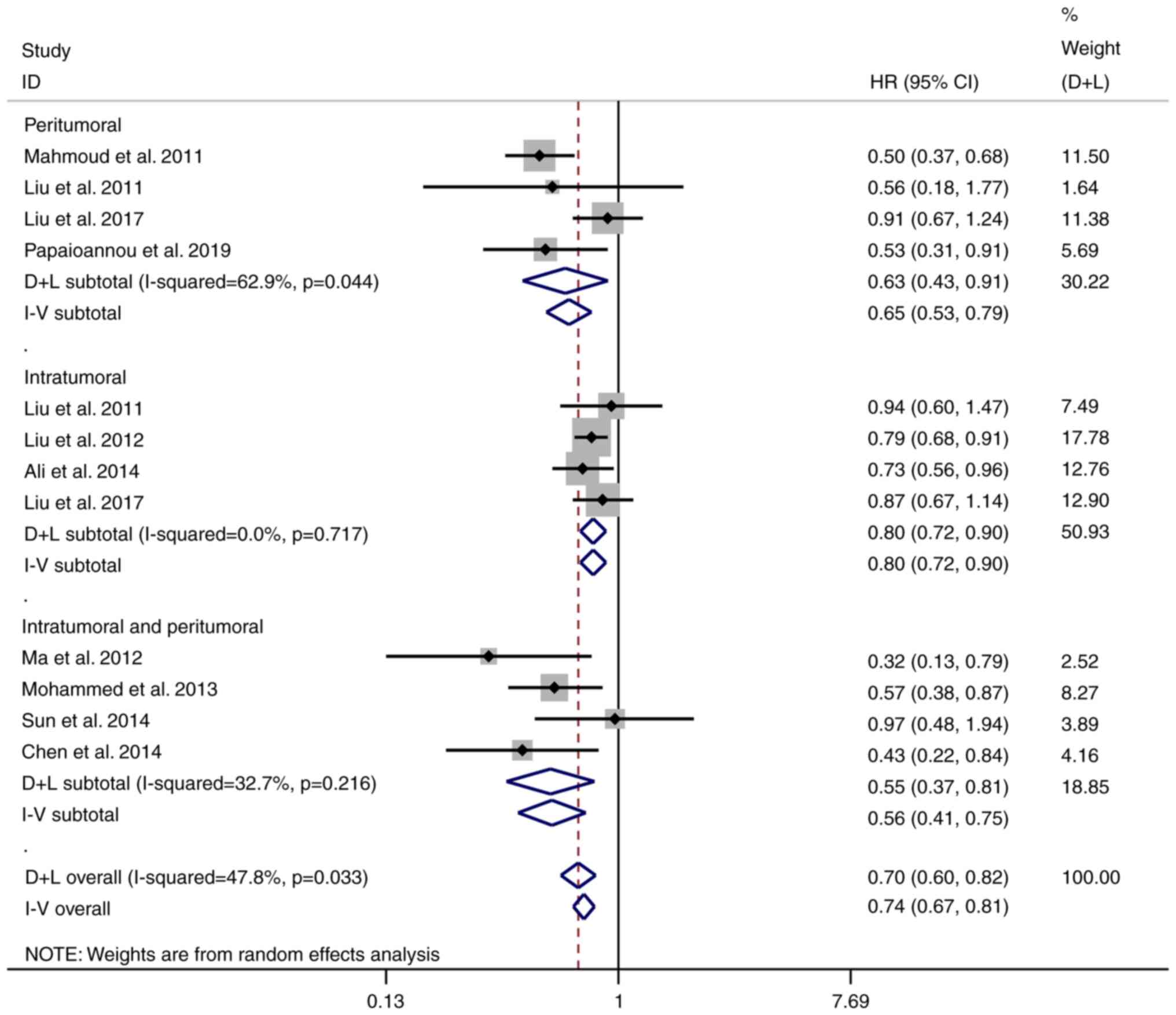
Subgroup analysis
In order to explore whether the location of
CD8+ TILs affects the relationship between
CD8+ T-cell infiltration and the prognosis of patients
with breast cancer, a subgroup analysis was further carried out.
The pooled results are listed in Table III. The result yielded from the
REM (D+L) was adopted when there was significant heterogeneity
among studies (I2>50%); otherwise, the estimation
from the FEM (I–V) was used. It was indicated that a high
infiltration level of CD8+ T cells in the peritumoral
group (HR=0.63, 95% CI: 0.43-0.91, P=0.015), intratumoral group
(HR=0.80, 95% CI: 0.72-0.90, P<0.001) and intratumoral and
peritumoral group (HR=0.56, 95% CI: 0.41-0.75, P=0.002) were all
significantly related to better OS of patients with breast cancer,
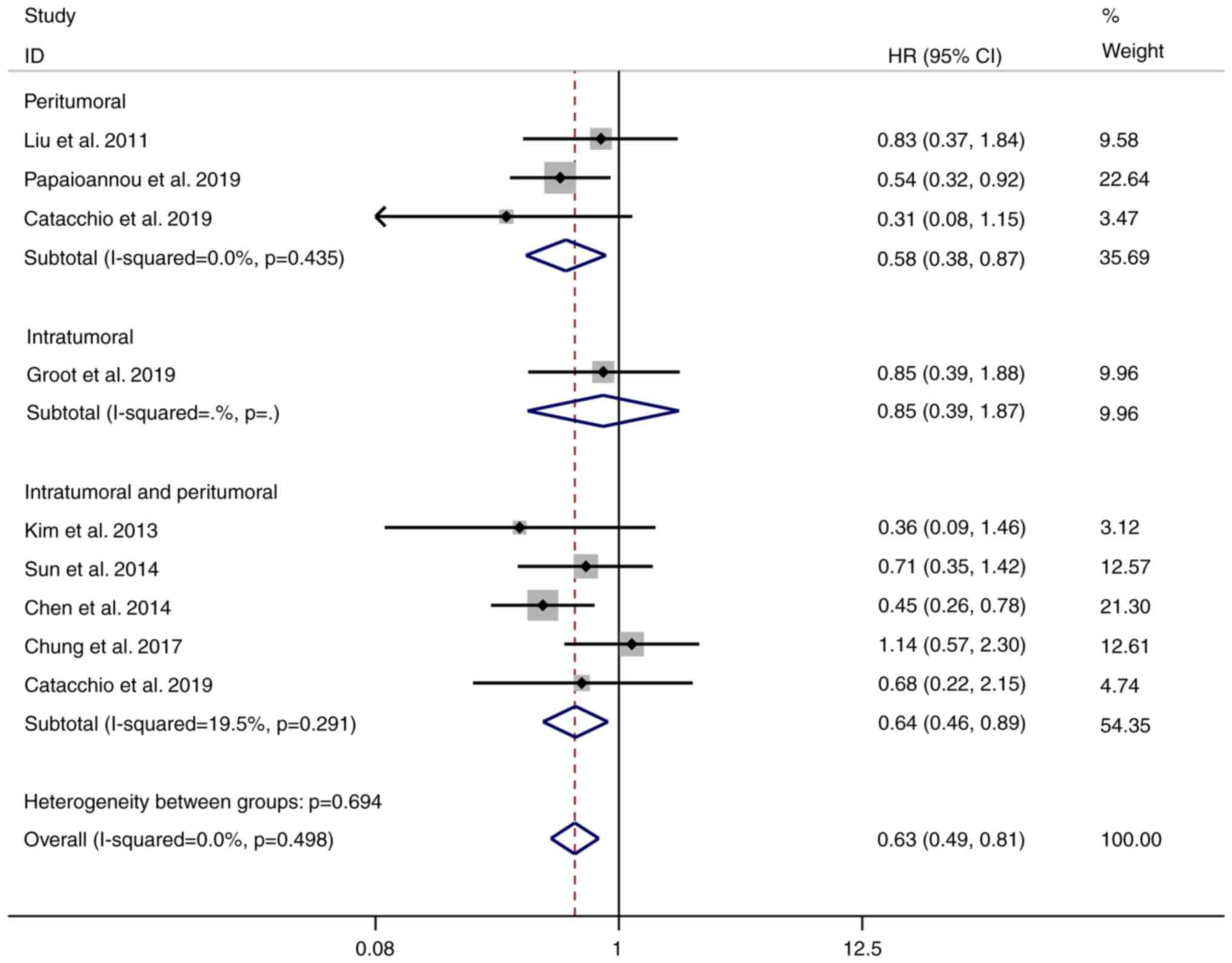
as presented in Fig. 5. In
addition, the pooled results illustrated that a high infiltration
level of CD8+ T cells in the peritumoral (HR=0.58, 95%
CI: 0.38-0.87, P=0.010) and intratumoral and peritumoral group
(HR=0.64, 95% CI: 0.46-0.89, P=0.009) was significantly related to
better DFS of patients with breast cancer, but not in the
intratumoral group (HR=0.85, 95% CI: 0.39-1.87, P=0.685), as
indicated in Fig. 6.
| Table III.Pooled HRs for OS and DFS according
to subgroup analyses. |
Table III.
Pooled HRs for OS and DFS according
to subgroup analyses.
| A, OS |
|---|
|
|---|
| Subgroup | Number of
studies | HR (95% CI) | P-value |
|---|
| P | 4 | 0.63
(0.43-0.91) | 0.015 |
| I | 4 | 0.80
(0.72-0.90) | <0.001 |
| I&P | 4 | 0.56
(0.41-0.75) | 0.002 |
|
| B, DFS |
|
|
Subgroup | Number of
studies | HR (95%
CI) | P-value |
|
| P | 3 | 0.58
(0.38-0.87) | 0.010 |
| I | 1 | 0.85
(0.39-1.87) | 0.685 |
| I&P | 5 | 0.64
(0.46-0.89) | 0.009 |
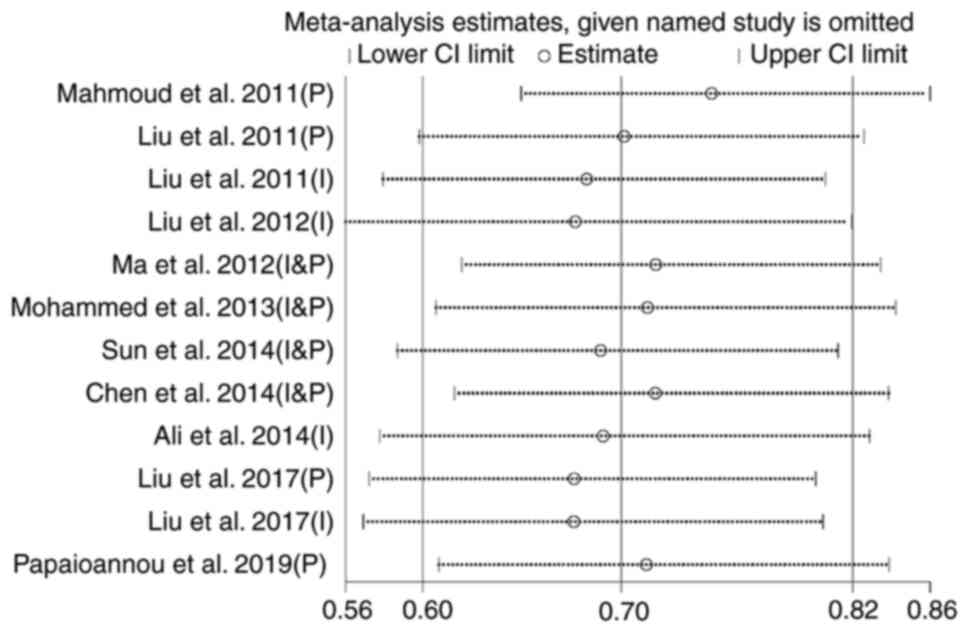
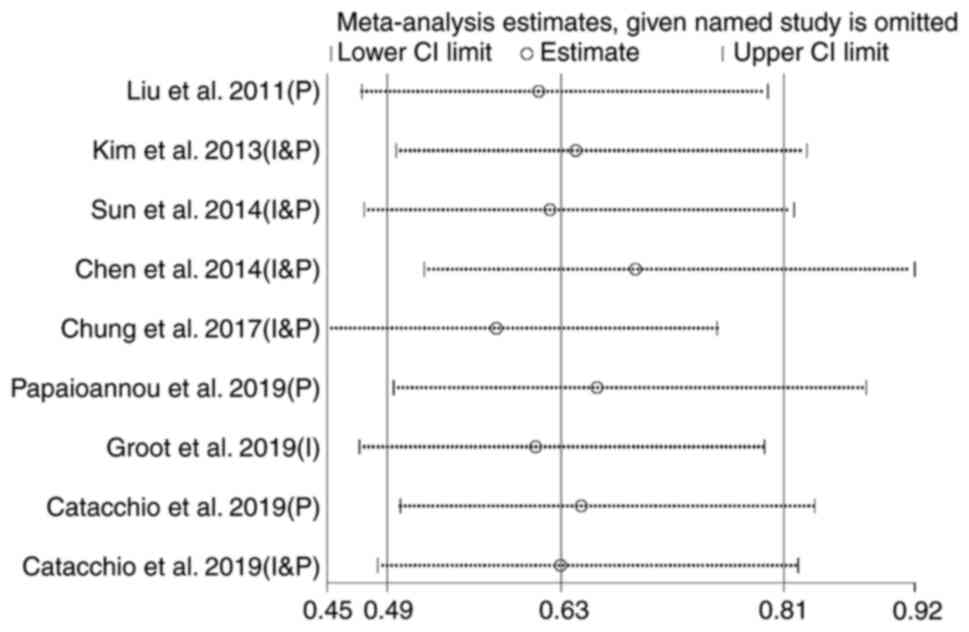
Sensitivity analysis
By excluding each included study one by one and
analyzing the impact on the results of the remaining studies (OS
and DFS), a sensitivity analysis was performed. The analysis did
not indicate any study that had any excessive impact on the OS
(Fig. 7) and DFS (Fig. 8). This means that the results of
the present meta-analysis are stable and reliable.
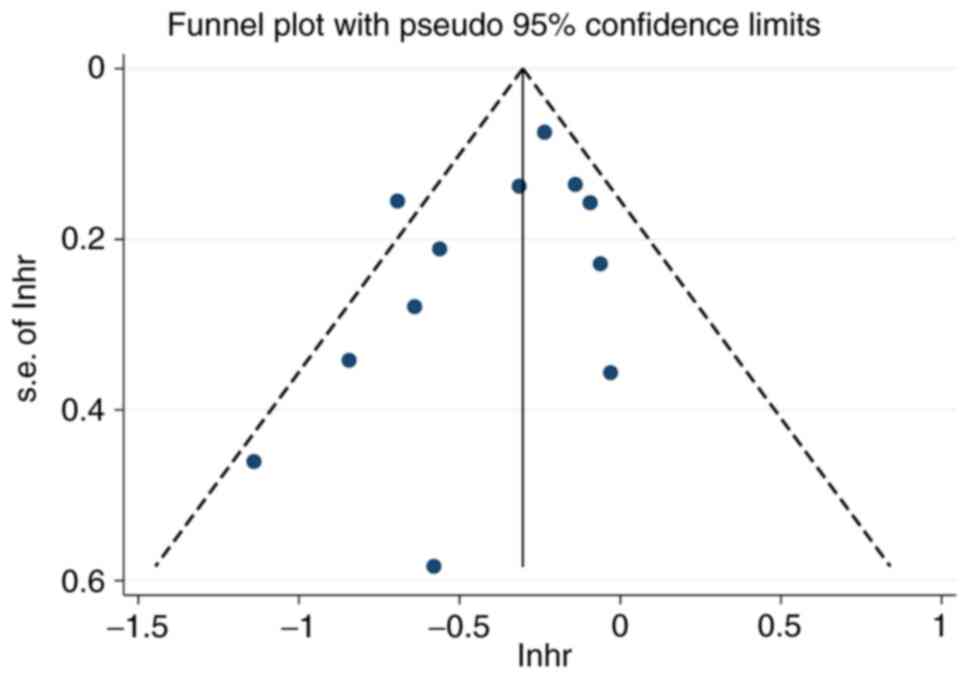
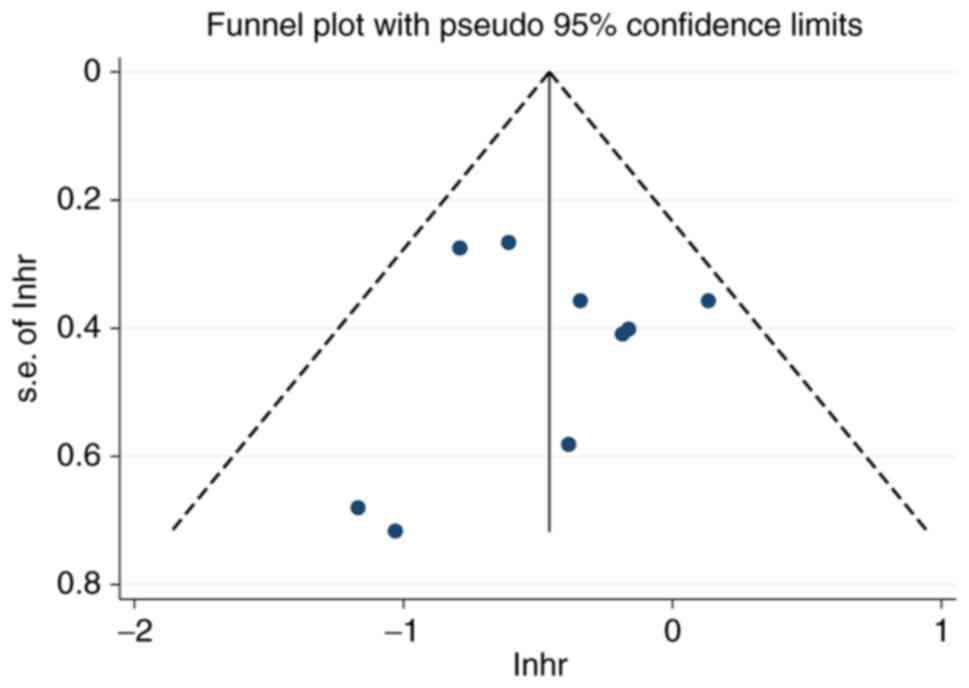
Publication bias
The funnel plots for publication bias are provided
in Figs. 9 and 10. It may be observed that the funnel
plots are near-symmetrical. The P-values of Egger's test were
P=0.141 for the studies regarding OS and P=0.897 for the studies
regarding DFS, indicating that there is no obvious publication bias
in the present study. No small-study effects were indicated, since
all the P-values were >0.05.
Discussion
TILs, as an important component of the tumor
microenvironment, predict prognosis and therapeutic response to
immunotherapy (35,36). High levels of tumor-infiltrating
CD8+ T-lymphocytes are characteristic of immunogenic hot
tumors, which respond significantly better to immunotherapy
(35,36). In the present review and
meta-analysis, 14 studies including 22,222 patients were pooled in
order to investigate the prognostic value of CD8+ T
cells in breast cancer, and to explore the association between
CD8+ T cells and the pathological characteristics of
patients with breast cancer, with the aim of providing new
prognostic biomarkers for the clinical treatment of breast
cancer.
The pooled results of the present study suggested
that the high CD8+ T-cell infiltration level was
significantly associated with better OS and DFS of patients with
breast cancer. Cytotoxic T cells are marked by CD8. Cells
presenting foreign antigens associated with major
histocompatibility complex class I molecules are recognized by
CD8+ T cells through specific interactions between the
presented antigens and T-cell receptors (37). CD8+ T cells represent a
marker of immune response against tumor, directly triggering
apoptosis of the target cell via the perforin/granzyme A/B system
or through FAS ligand expression (37). Enhancing tumor infiltration by
cytotoxic T cells appears to be an important therapeutic strategy,
which may convert immunogenic cold tumors to hot tumors, thereby
increasing the response rate to immunotherapy. In order to explore
whether the location of CD8+ TILs affects the
relationship between CD8+ T-cell infiltration and the
prognosis of patients with breast cancer, a subgroup analysis was
further performed. The pooled results indicated that a high
infiltration level of CD8+ T cells was significantly
related to better OS of patients with breast cancer regardless of
the location. This suggests that the location of CD8+ T
cells in breast cancer does not affect the relationship between
CD8+ T cells and OS. However, the pooled results
illustrated that a high infiltration level of CD8+ T
cells in the peritumoral, and intratumoral and peritumoral, but not
in the intratumoral region, was significantly related to better DFS
of patients with breast cancer. This suggests that peritumoral
CD8+ T cells are more helpful in predicting DFS in
patients with breast cancer. Regarding the differences in the
prediction results of the two locations, future studies are
required in order to reveal the mechanisms in detail.
In addition, the present results suggested that a
high CD8+ T-cell infiltration level was significantly
associated with decreased expression of ER and PR, as well as
increased HER2 expression, in patients with breast cancer. The
above results indicate that drugs targeting ER and PR are not
suitable for patients with breast cancer with a high
CD8+ T-cell infiltration level, while drugs targeting
HER2 are more suitable for patients with breast cancer with a high
CD8+ T-cell infiltration level. Furthermore, patients
with HER2-positive breast cancer may have a better prognosis.
The present review and meta-analysis also has
certain limitations. First, since all patients with breast cancer
were included in the present study, the heterogeneity of patients
with breast cancer itself was not excluded in this study, resulting
in mild to moderate heterogeneity of the study results. However, as
the included studies did not specify the type of breast cancer, it
was not possible to perform any further subgroup analysis.
Furthermore, the small number of studies included in the present
subgroup analysis of CD8+ T-cell location may challenge
the objectivity of the results. Finally, since the evaluation
method and cutoff point to separate high and low infiltration
levels vary among the studies, it is difficult to use the same
criteria to evaluate the CD8+ T-cell infiltration level for all of
the studies. These differences may have led to heterogeneity among
the included studies.
In conclusion, CD8+ T cells are of value
in predicting the prognosis of patients with breast cancer. A high
level of CD8+ T-cell infiltration was related to
improved prognosis, including OS and DFS, in patients with breast
cancer. In addition, a high CD8+ T-cell infiltration
level was significantly associated with decreased expression of ER
and PR, and increased HER2 expression.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author upon reasonable
request.
Authors' contributions
YPS and XL contributed to the conception, design and
modification of the study. YPS and YLK screened articles for
inclusion and extracted the data. YPS performed the statistical
analysis. YPS and YLK contributed to the interpretation of the
results. YPS and XL drafted the manuscript. YPS and XL confirm the
authenticity of all the raw data. All authors contributed to
manuscript revision, and read and approved the final manuscript.
All authors agreed to be accountable for all aspects of the
work.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ghoncheh M, Pournamdar Z and Salehiniya H:
Incidence and mortality and epidemiology of breast cancer in the
world. Asian Pac J Cancer Prev. 17:43–46. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sung H, Ferlay J, Siegel RL, Laversanne M,
Soerjomataram I, Jemal A and Bray F: Global cancer statistics 2020:
GLOBOCAN estimates of incidence and mortality worldwide for 36
cancers in 185 countries. CA Cancer J Clin. 71:209–249. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Emens LA: Breast cancer immunotherapy:
Facts and hopes. Clin Cancer Res. 24:511–520. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Saponaro C, Vagheggini A, Scarpi E,
Centonze M, Catacchio I, Popescu O, Pastena MI, Giotta F,
Silvestris N and Mangia A: NHERF1 and tumor microenvironment: A new
scene in invasive breast carcinoma. J Exp Clin Cancer Res.
37:962018. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Shiao SL, Ganesan AP, Rugo HS and Coussens
LM: Immune microenvironments in solid tumors: New targets for
therapy. Genes Dev. 25:2559–2572. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Naito Y, Saito K, Shiiba K, Ohuchi A,
Saigenji K, Nagura H and Ohtani H: CD8+ T cells infiltrated within
cancer cell nests as a prognostic factor in human colorectal
cancer. Cancer Res. 58:3491–3494. 1998.PubMed/NCBI
|
|
7
|
Paijens ST, Vledder A, de Bruyn M and
Nijman HW: Tumor-infiltrating lymphocytes in the immunotherapy era.
Cell Mol Immunol. 18:842–859. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Lotfinejad P, Asghari Jafarabadi M, Abdoli
Shadbad M, Kazemi T, Pashazadeh F, Sandoghchian Shotorbani S,
Jadidi Niaragh F, Baghbanzadeh A, Vahed N, Silvestris NJ and
Baradaran B: Prognostic role and clinical significance of
tumor-infiltrating lymphocyte (TIL) and programmed death ligand 1
(PD-L1) expression in triple-negative breast cancer (TNBC): A
systematic review and meta-analysis study. Diagnostics (Basel).
10:7042020. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Farhood B, Najafi M and Mortezaee K:
CD8(+) cytotoxic T lymphocytes in cancer immunotherapy: A review. J
Cell Physiol. 234:8509–8521. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Li F, Li C, Cai X, Xie Z, Zhou L, Cheng B,
Zhong R, Xiong S, Li J, Chen Z, et al: The association between CD8+
tumor-infiltrating lymphocytes and the clinical outcome of cancer
immunotherapy: A systematic review and meta-analysis.
EClinicalMedicine. 41:1011342021. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Liu S, Lachapelle J, Leung S, Gao D,
Foulkes WD and Nielsen TO: CD8+ lymphocyte infiltration is an
independent favorable prognostic indicator in basal-like breast
cancer. Breast Cancer Res. 14:R482012. View
Article : Google Scholar : PubMed/NCBI
|
|
12
|
Mahmoud SM, Paish EC, Powe DG, Macmillan
RD, Grainge MJ, Lee AH, Ellis IO and Green AR: Tumor-infiltrating
CD8+ lymphocytes predict clinical outcome in breast cancer. J Clin
Oncol. 29:1949–1955. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Baker K, Lachapelle J, Zlobec I, Bismar
TA, Terracciano L and Foulkes WD: Prognostic significance of CD8+ T
lymphocytes in breast cancer depends upon both oestrogen receptor
status and histological grade. Histopathology. 58:1107–1116.
2011.PubMed/NCBI
|
|
14
|
Liu F, Lang R, Zhao J, Zhang X, Pringle
GA, Fan Y, Yin D, Gu F, Yao Z and Fu L: CD8(+) cytotoxic T cell and
FOXP3(+) regulatory T cell infiltration in relation to breast
cancer survival and molecular subtypes. Breast Cancer Res Treat.
130:645–655. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Denkert C, Loibl S, Noske A, Roller M,
Muller BM, Komor M, Budczies J, Darb-Esfahani S, Kronenwett R,
Hanusch C, et al: Tumor-associated lymphocytes as an independent
predictor of response to neoadjuvant chemotherapy in breast cancer.
J Clin Oncol. 28:105–113. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Loi S, Sirtaine N, Piette F, Salgado R,
Viale G, Van Eenoo F, Rouas G, Francis P, Crown JP, Hitre E, et al:
Prognostic and predictive value of tumor-infiltrating lymphocytes
in a phase III randomized adjuvant breast cancer trial in
node-positive breast cancer comparing the addition of docetaxel to
doxorubicin with doxorubicin-based chemotherapy: BIG 02-98. J Clin
Oncol. 31:860–867. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Moher D, Liberati A, Tetzlaff J and Altman
DG; PRISMA Group, : Preferred reporting items for systematic
reviews and meta-analyses: The PRISMA statement. Ann Intern Med.
151:264–269. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Margulis AV, Pladevall M, Riera-Guardia N,
Varas-Lorenzo C, Hazell L, Berkman ND, Viswanathan M and
Perez-Gutthann S: Quality assessment of observational studies in a
drug-safety systematic review, comparison of two tools: The
newcastle-ottawa scale and the RTI item bank. Clin Epidemiol.
6:359–368. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Mantel N and Haenszel W: Statistical
aspects of the analysis of data from retrospective studies of
disease. J Natl Cancer Inst. 22:719–748. 1959.PubMed/NCBI
|
|
20
|
DerSimonian R and Laird N: Meta-analysis
in clinical trials revisited. Contemp Clin Trials. 45:139–145.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Borenstein M, Hedges LV, Higgins JP and
Rothstein HR: A basic introduction to fixed-effect and
random-effects models for meta-analysis. Res Synth Methods.
1:97–111. 2010. View
Article : Google Scholar : PubMed/NCBI
|
|
22
|
DerSimonian R and Kacker R: Random-effects
model for meta-analysis of clinical trials: An update. Contemp Clin
Trials. 28:105–114. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Riley RD, Higgins JP and Deeks JJ:
Interpretation of random effects meta-analyses. BMJ. 342:d5492011.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Ma C, Zhang Q, Ye J, Wang F, Zhang Y,
Wevers E, Schwartz T, Hunborg P, Varvares MA, Hoft DF, et al:
Tumor-infiltrating γδ T lymphocytes predict clinical outcome in
human breast cancer. J Immunol. 189:5029–5036. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Mohammed ZM, Going JJ, Edwards J,
Elsberger B and McMillan DC: The relationship between lymphocyte
subsets and clinico-pathological determinants of survival in
patients with primary operable invasive ductal breast cancer. Br J
Cancer. 109:1676–1684. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kim ST, Jeong H, Woo OH, Seo JH, Kim A,
Lee ES, Shin SW, Kim YH, Kim JS and Park KH: Tumor-infiltrating
lymphocytes, tumor characteristics, and recurrence in patients with
early breast cancer. Am J Clin Oncol. 36:224–231. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Sun S, Fei X, Mao Y, Wang X, Garfield DH,
Huang O, Wang J, Yuan F, Sun L, Yu Q, et al: PD-1(+) immune cell
infiltration inversely correlates with survival of operable breast
cancer patients. Cancer Immunol Immunother. 63:395–406. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Chen Z, Chen X, Zhou E, Chen G, Qian K, Wu
X, Miao X and Tang Z: Intratumoral CD8(+) cytotoxic lymphocyte is a
favorable prognostic marker in node-negative breast cancer. PLoS
One. 9:e954752014. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Ali HR, Provenzano E, Dawson SJ, Blows FM,
Liu B, Shah M, Earl HM, Poole CJ, Hiller L, Dunn JA, et al:
Association between CD8+ T-cell infiltration and breast cancer
survival in 12,439 patients. Ann Oncol. 25:1536–1543. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Chung YR, Kim HJ, Jang MH and Park SY:
Prognostic value of tumor infiltrating lymphocyte subsets in breast
cancer depends on hormone receptor status. Breast Cancer Res Treat.
161:409–420. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Liu S, Chen B, Burugu S, Leung S, Gao D,
Virk S, Kos Z, Parulekar WR, Shepherd L, Gelmon KA and Nielsen TO:
Role of cytotoxic tumor-infiltrating lymphocytes in predicting
outcomes in metastatic HER2-positive breast cancer: A secondary
analysis of a randomized clinical trial. JAMA Oncol. 3:e1720852017.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Papaioannou E, Sakellakis M, Melachrinou
M, Tzoracoleftherakis E, Kalofonos H and Kourea E: A Standardized
evaluation method for FOXP3+ tregs and CD8+ T-cells in breast
carcinoma: Association with breast carcinoma subtypes, stage and
prognosis. Anticancer Res. 39:1217–1232. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
de Groot AF, Blok EJ, Charehbili A, Engels
CC, Smit V, Dekker-Ensink NG, Putter H, Meershoek-Klein Kranenbarg
E, van de Velde CJ, Liefers GJ, et al: Strong CD8+ lymphocyte
infiltration in combination with expression of HLA class I is
associated with better tumor control in breast cancer patients
treated with neoadjuvant chemotherapy. Breast Cancer Res Treat.
175:605–615. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Catacchio I, Silvestris N, Scarpi E,
Schirosi L, Scattone A and Mangia A: Intratumoral, rather than
stromal, CD8+ T cells could be a potential negative prognostic
marker in invasive breast cancer patients. Transl Oncol.
12:585–595. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Galon J and Bruni D: Approaches to treat
immune hot, altered and cold tumours with combination
immunotherapies. Nat Rev Drug Discov. 18:197–218. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
van der Woude LL, Gorris MA, Halilovic A,
Figdor CG and de Vries IJ: Migrating into the tumor: A roadmap for
T cells. Trends Cancer. 3:797–808. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Berke G: The binding and lysis of target
cells by cytotoxic lymphocytes: Molecular and cellular aspects.
Annu Rev Immunol. 12:735–773. 1994. View Article : Google Scholar : PubMed/NCBI
|