Introduction
Uterine corpus cancer is the sixth most commonly
diagnosed malignancy among women, with 417,000 new cases and 97,000
cases of mortality reported worldwide in 2020 (1). A total of 81,964 new cases and 16,607
cases of associated mortality were reported in China in 2020
(2). Endometrial endometrioid
carcinoma (EEC) is the most prevalent subtype of uterine corpus
cancer, accounting for ~75% of all cases (3). The incidence of EEC has been
gradually increasing over the past decade worldwide (4). Atypical hyperplasia (AH) and
endometrioid intraepithelial neoplasia (EIN) refer to the precursor
lesions that occur prior to EEC. This terminology is used in the
World Health Organization (WHO) Classification (2014) of Tumors of
Female Reproductive Organs (3). In
total, ~25% of all AH cases will typically progress into EEC
(5). Furthermore, both AH and EIN
have similar morphological features, the occurrence of which has
been reported to be largely associated with long-term
non-antagonistic estrogen. In total, ~14% of patients with EEC are
women of child-bearing age (6). At
present, a large proportion of fertile women will delay bearing
children, which has been reported to have caused an increase in the
number of nulliparous women diagnosed with EEC (7). In 1997, Kim et al (8) first reported that patients with EEC
could conceive successfully after progestin treatment. Hormonal
treatment with progesterone may also be a viable option in women
with well-differentiated EEC or AH who wish to preserve their
fertility. Fertility-sparing treatment is becoming more popular and
is increasingly being used for young women diagnosed with
International Federation of Gynecology and Obstetrics (FIGO) stage
IA, grade 1 EEC of the uterus who wish to have children in the
future (7,9).
Excessive exposure of the endometrium to estrogen
has been reported to be one of the most important risk factors for
EEC (10). Pathologically
well-differentiated EEC typically presents with positive estrogen
receptor (ER) and progesterone receptor (PR) expression, and is
also associated with a good prognosis (11). Protein biomarkers, such as PTEN and
paired box 2 (PAX2), have been reported to be useful for the
differential diagnosis of EEC and AH (12).
Therefore, the present study assessed the prognostic
value of certain clinicopathological features and their protein
marker expression profiles, specifically in women of childbearing
age with EEC/AH. The ultimate aim was to evaluate if these protein
markers were able to predict prognosis and provide guidance on the
management of young women with EEC/AH. Furthermore, the present
study evaluated these markers potential association with
histological classification and prognosis following repeated
conservative fertility-preserving treatments against EEC/AH.
Materials and methods
Case selection
In total, the cases of 83 patients, of whom 37 were
initially diagnosed with AH and 46 were diagnosed with EEC, who
were treated between August 2013 and September 2021 at Peking
University People's Hospital (Beijing, China) were retrospectively
analyzed. Endometrial biopsies had been collected from these
patients, who were followed up ≥2 times. All patients had been
treated using progestin and had undergone follow-up clinical
examination using ultrasound every month. Furthermore, patients had
undergone endometrial sampling using hysteroscopy or curettage to
assess the endometrial response every 3 months. The follow-up
duration was defined as the period from the initial treatment to
the time of last observation. All pathological slides were
carefully, independently, reviewed by two experienced gynecological
pathologists. Before treatment, the absence of muscular
infiltration, cervical invasion or extrauterine diffusion had been
confirmed through inspection. The present study was approved by the
Ethics Committee of Peking University People's Hospital (approval
number 2016PHB054-01).
Pathological response evaluation
Pre-treatment biopsies evaluation
According to the criteria stated by the WHO
Classification of Tumors of Female Reproductive Organs (3), EEC can be graded as grade 1, 2 or 3
using the FIGO grading criteria, exhibiting ≤5, 6–50 and >50%
solid area (non-glandular and non-squamous growth area),
respectively. AH is defined as a simultaneous change in epithelial
cells (including enlarged nucleus and visible nucleoli) and
increase in the number of endometrial glands (crowded gland
architecture) within a morphologically defined region that is
distinct from the surrounding endometrium of entrapped normal
glands. AH size must be ≥1 mm.
Post-treatment evaluation
The patients underwent follow-up using endometrial
sampling by hysteroscopy or curettage to assess endometrial changes
every 3 months. According to Wheeler et al (13) and Chen et al (14), response to treatment based on the
latest biopsy can be classified as follows: i) Complete response
(CR), defined as a proliferative, secretory, inactive or atrophic
endometrium without hyperplasia or atypia; ii) partial response
(PR), defined as histological regression with decidual endometrial
change; iii) stable disease (SD), defined as the persistence of EEC
or AH/EIN in both the original and final specimens; iv) progressive
disease (PD), defined as progression to lesions if the
pre-treatment specimen showed AH whereas the latest specimen showed
EEC, or if the original specimen showed grade 1 EEC whereas the
latest specimen showed EEC grade 2 or 3; and v) recurrent disease
(RD), defined as a CR to progestin treatment once or more according
to a follow-up biopsy, but in which EEC/AH recurrence was
subsequently identified. All pre-treatment and post-treatment
evaluations were independently performed by two experienced
gynecological pathologists. A consensus was considered to be
reached if both observers agreed and a third pathologist would
review it if both observers disagreed.
Histological and immunohistochemical
analysis
All pathological specimens were fixed using 4%
neutral formaldehyde (room temperature; 120 min), before the sample
was conventionally dehydrated (graded alcohol series) and soaked,
embedded in paraffin and sectioned (5 µm) for hematoxylin and eosin
staining (room temperature; 10 min).
All immunohistochemical staining was performed
according to the manufacturers' protocols. Formalin-fixed
paraffin-embedded blocks were sectioned at 4 µm each and incubated
with antibodies (37°C; 20–30 min) against p53 (1:100; cat. no.
ZM-0408; clone D0-7), ER (1:100; cat. no. ZM-0104; clone 6F11), PR
(1:100; cat. no. ZM-0215; clone 16), PTEN (1:50; cat. no. ZM-0116;
clone 6H2.1) and PAX2 (1:100; cat. no. ZM-0467; clone EP235) (all
ZSGB-BIO Technology Co, Ltd.). Secondary antibody (HRP; cat. no.
ZLI-9013; ZSGB-BIO Technology Co, Ltd.) incubation was 20–30 min at
37°C. The presence of brown/yellow staining under a light
microscope indicated positivity. PAX2, p53, ER, PR and PTEN
positivity was present in the nucleus. ER and PR protein expression
levels were assessed based on the intensity and the proportion of
nuclear staining according to the area of positively stained
nuclei, and were divided into two groups: >50 and ≤50% as
estimated by a pathologist. p53 expression levels were used to
divide cells into wild-type (sporadic or few cells positive) and
mutant-type (>70% cells positive) (3). Positive PAX2 and PTEN expression was
defined as >90% of EEC/AH having retained PTEN and PAX2
staining. Adjacent stromal cells or normal endometrial glands
served as positive internal controls.
Statistical analysis
Statistical analysis was performed using SPSS 25
(IBM Corp.). The measurement data are presented as the count and
percentage [n (%)]. The association between the clinicopathological
features and patient outcome was assessed using the χ2
test. All statistical tests were two-sided and P<0.05 was
considered to indicate a statistically significant difference.
Results
Clinicopathological
characteristics
Clinicopathological and outcome data were collected
from 46 women with EEC and 37 women with AH. Patient age at
diagnosis ranged from 19 to 44 years, with a median age of 32.6
years. The duration of clinical follow-up ranged from 4 to 98
months, with a median follow-up time of 37 months. In total, 5
patients abandoned progestin treatment, as a CR was not achieved
within a given period of time (15–24 months), and instead opted for
a hysterectomy. All patients received multiple cycles of high-dose
progestin treatment (number of treatment cycles, 2–8). All but 5
patients were receiving progestin treatment continuously during the
follow-up period. The detailed clinicopathological features of the
EEC and AH groups are presented in Table I.
 | Table I.Relationship between
clinicopathological features and prognosis of patients after
treatment. |
Table I.
Relationship between
clinicopathological features and prognosis of patients after
treatment.
| Clinicopathological
feature | Total, n | CR, n | No CR, n | P-value |
|---|
| Age, years |
|
|
| 0.342 |
| ≤35 | 45 | 36 | 9 |
|
|
>35 | 38 | 27 | 11 |
|
| BMI |
|
|
| 0.883 |
|
<25 | 26 | 20 | 6 |
|
|
≥25 | 57 | 43 | 14 |
|
| Pathological
type |
|
|
| 0.043 |
|
EEC | 46 | 31 | 15 |
|
| AH | 37 | 32 | 5 |
|
| CR duration (<6
Months) |
|
|
|
|
| EEC | 46 | 16 | 30 | <0.001 |
| AH | 37 | 28 | 9 |
|
Comparison of outcomes between
patients with EEC and patients with AH after repeated
fertility-preserving treatments
According to the aforementioned definition of
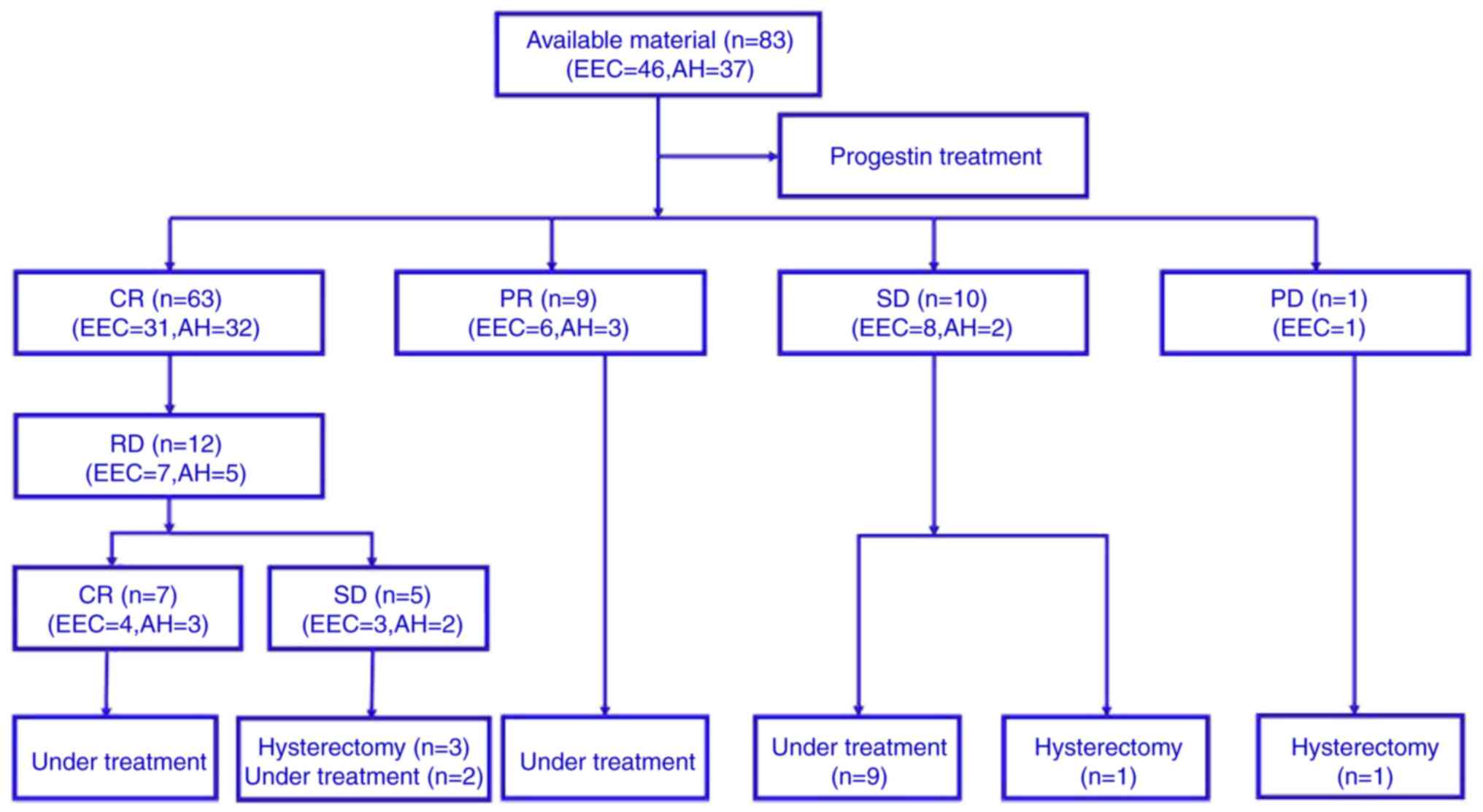
post-treatment evaluation, the overall CR rate in the EEC group was
67.39% (31/46). In total, 16 patients reached CR in <6 months
and 30 patients reached CR in >6 months. Furthermore, 6 patients
achieved PR and 8 patients demonstrated SD. Moreover, one patient
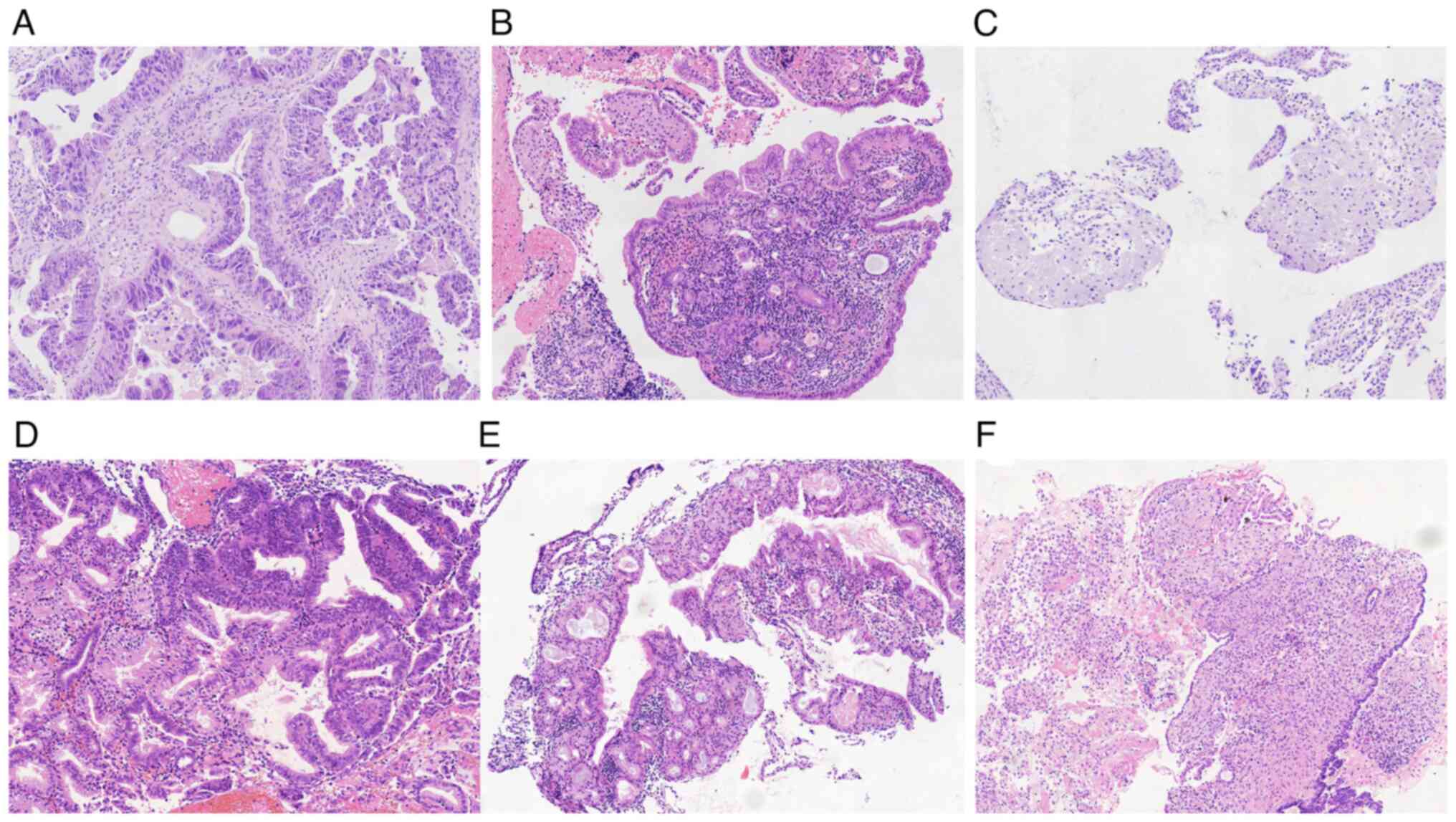
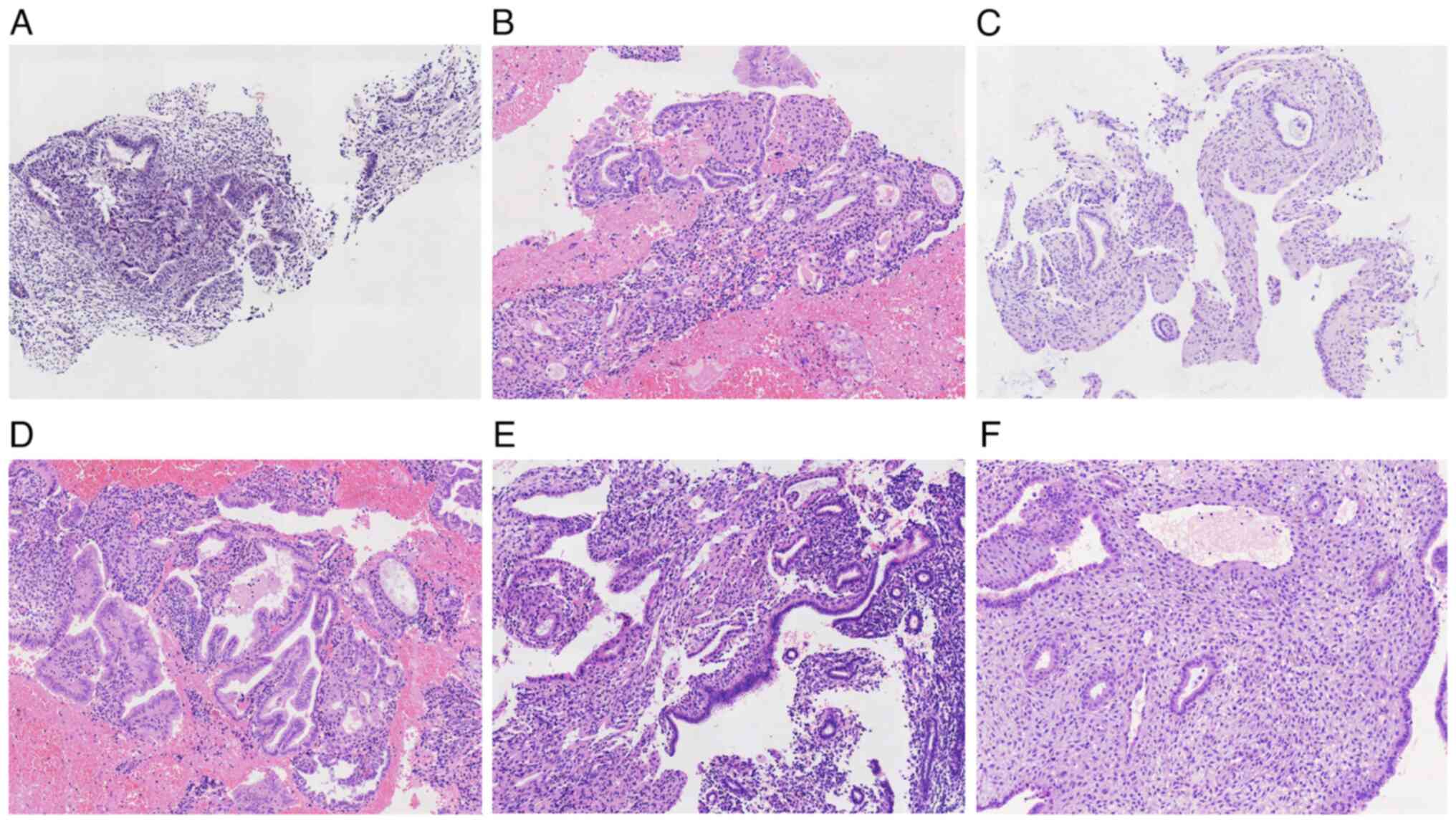
experienced PD. Among the 31 patients who achieved CR, 7 patients
experienced RD. In terms of patients with RD, 4 patients achieved
CR, whereas 3 patients gave up fertility preservation treatment and
underwent a hysterectomy. Figs. 1
and 2 show representative
hematoxylin and eosin staining images of EEC and AH sections after
fertility-preserving treatment.
The overall CR rate in the AH group was 86.49%
(32/37), where 28 cases reached CR in <6 months and nine cases
required >6 months. There were 3 cases of PR and 2 patients
demonstrated SD. Among the 32 patients who achieved CR, 5 patients
(15.63%) experienced RD. In the RD group, 3 cases reached CR and 2
cases reached SD. PD cases were not observed (Table I).
The CR rate of patients with EEC (67.39%) was
significantly lower compared with that in AH patients (86.49%)
(P=0.043; Table I). Furthermore,
the CR rate in the EEC and AH groups at 6 months was statistically
significant (P=0.000) and the CR rate in the AH was higher. The
time required by the AH group to reach CR was significantly shorter
compared with that in EEC group (Table
I). Among the 46 cases of EEC, 36 cases were grade 1 and 10
cases were grade 2 (Table II). In
the grade 1 EEC group, 26 cases achieved CR, 4 cases were PR and 6
cases were SD. In the grade 2 EEC group, 5 cases were CR, 2 cases
were PR and 1 case was PD. SD was demonstrated in 2 cases. The CR
rate of patients with grade 2 EEC (50.0%) was markedly lower
compared with that of patients with grade 1 EEC (72.22%) (Table II). All patients were alive at the
last follow-up (Fig. 3).
| Table II.Association between pathological
subtype/expression of biomarkers and prognosis of patients after
treatment. |
Table II.
Association between pathological
subtype/expression of biomarkers and prognosis of patients after
treatment.
| A, EEC pathological
grade |
|---|
|
|---|
| Parameter | Total, n | CR, n | No CR, n | P-value |
|---|
| Pathological
grade |
|
|
| 0.185 |
| I | 36 | 26 | 10 |
|
| II | 10 | 5 | 5 |
|
|
| B, EEC
biomarkers |
|
|
Parameter | Total,
n | CR, n | No CR,
n | P-value |
|
| ER |
|
|
| >0.999 |
|
≤50% | 9 | 6 | 3 |
|
|
>50% | 37 | 25 | 12 |
|
| PR |
|
|
| 0.010 |
|
≤50% | 6 | 1 | 5 |
|
|
>50% | 40 | 30 | 10 |
|
| PAX2 |
|
|
| 0.070 |
|
Negative | 34 | 20 | 14 |
|
|
Positive | 12 | 11 | 1 |
|
| PTEN |
|
|
| 0.603 |
|
Negative | 24 | 17 | 7 |
|
|
Positive | 22 | 14 | 8 |
|
| p53 |
|
|
| 0.326 |
|
Mutant | 1 | 0 | 1 |
|
|
Wild-type | 45 | 31 | 14 |
|
|
| C, AH
biomarkers |
|
|
Parameter | Total,
n | CR, n | No CR,
n | P-value |
|
| ER |
|
|
| 0.110 |
|
≤50% | 10 | 7 | 3 |
|
|
>50% | 27 | 25 | 2 |
|
| PR |
|
|
| 0.012 |
|
≤50% | 5 | 2 | 3 |
|
|
>50% | 32 | 30 | 2 |
|
| PAX2 |
|
|
| >0.999 |
|
Negative | 23 | 20 | 3 |
|
|
Positive | 14 | 12 | 2 |
|
| PTEN |
|
|
| >0.999 |
|
Negative | 27 | 23 | 4 |
|
|
Positive | 10 | 9 | 1 |
|
Relationship between pre-treatment
biomarker expression and prognosis in the different groups
All patients with EEC and AH demonstrated positive
PR and ER expression in 10–100% of the tumor cells before treatment
and were divided into the following two groups: ≤50 and >50%. In
EEC, there were 9 cases with ≤50% ER expression and 37 cases with
>50% ER expression (Table II).
For PR expression in EEC, 6 cases demonstrated ≤50% expression and
40 cases demonstrated >50% expression. In patients with AH, 10
cases presented with ≤50% ER expression and 27 cases presented with
>50% ER expression. There were 5 cases with ≤50% PR expression
and 32 cases with >50% PR expression. In EEC, 34 cases
demonstrated PAX2-negative staining, whereas 12 cases demonstrated
PAX2-positive staining. There were also 24 PTEN-negative cases and
22 PTEN-positive cases. The p53-mutant type was found in 1 case and
the p53 wild-type was found in 45 cases (P=0.326) in EEC group. In
the grade 2 EEC group, 2 cases demonstrated ≤50% PR expression and
8 cases demonstrated >50% PR expression. A total of 3 cases
demonstrated PAX2-negative staining, whereas 7 cases demonstrated
PAX2-positive staining.
In patients with AH, 10 cases presented with ≤50% ER
expression whilst 27 cases showed >50% ER expression (Table II). There were 5 cases showing
≤50% PR expression and 32 cases showing >50% PR expression.
Patients with either EEC or AH showing >50% positive PR
expression had higher CR rates compared with the ≤50% positive PR
groups. The relationship between prognosis after treatment and PR
expression in the initially untreated AH/EEC groups was
significantly different (P=0.012; P=0.010; Table II). A total of 23 PAX2-negative
cases were demonstrated whereas 14 PAX2-positive cases were
demonstrated (Table II). There
were 27 PTEN-negative cases and 10 PTEN-positive cases. The p53
mutant type was found in one case, whereas 37 cases had the p53
wild-type in the EEC groups. The relationships between prognosis
after treatment and ER, PTEN and PAX2 expression in the
pretreatment AH/EEC groups were not significantly different. The
relationship between prognosis and p53 expression in the EEC groups
were not significantly different. In the AH groups, p53 IHC test
was not performed. Representative immunohistochemical results for
the EEC and AH cases before treatment are presented in Fig. 4.
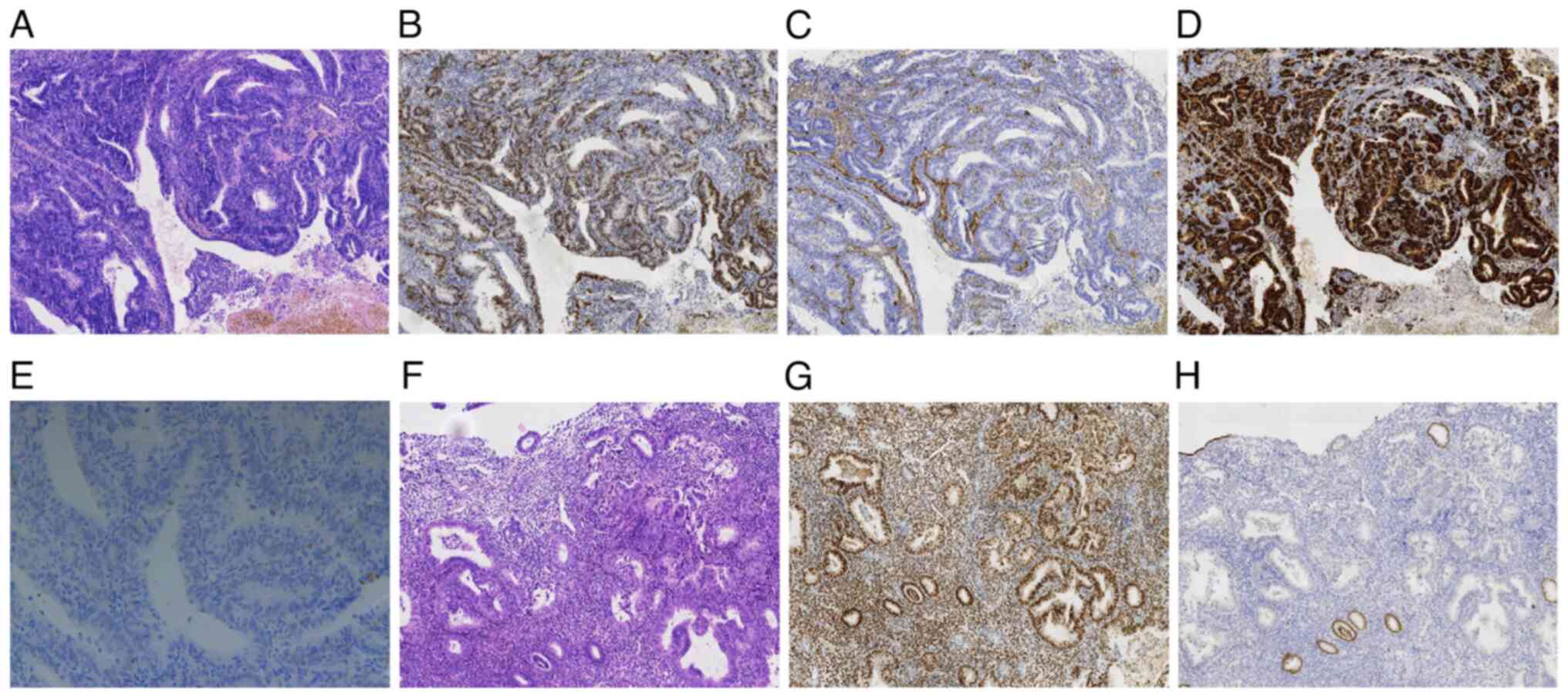 | Figure 4.Differential immunohistochemical
staining profiles before treatment for EEC and AH. (A)
Representative image of grade 1 EEC (hematoxylin and eosin;
magnification, ×100). (B) Representative image of positive ER
expression in an EEC biopsy before treatment (magnification, ×100).
(C) Representative EEC biopsy image of negative PTEN expression
before treatment, but with positive PTEN expression in stroma cells
(magnification, ×100). (D) Representative image showing strongly
positive PR expression in an EEC biopsy before treatment
(magnification, ×100). (E) Representative image showing p53
scattered (wild-type) expression in an EEC biopsy before treatment
(magnification, ×200). (F) Representative AH biopsy image
(hematoxylin and eosin; magnification, ×100). (G) Representative
image showing positive ER expression in a pre-treatment biopsy
(magnification, ×100). (H) Representative AH biopsy image showing
negative PAX2 expression before treatment, but positive PAX2
expression could be observed seen in the adjacent normal epithelium
(magnification, ×100). EEC, endometrial endometrioid carcinoma; AH,
atypical hyperplasia; ER, estrogen receptor; PAX2, paired box
2. |
Discussion
In 1983, endometrial carcinoma was divided into type
I and type II by Bokhman, according to the relationship between
endometrial carcinoma and estrogen, and histopathological and
epidemiological characteristics (15). Type I cancer was EEC and defined as
being hormone-associated tumors, which responded well to progestin
therapy and were associated with a good prognosis, with a 5-year
survival rate of 81%. Type II cancer was serous carcinoma, which
was not considered in the present study. However, the 5-year
survival rate was reported to be 96% for patients with EEC with
FIGO stage I (16). The National
Comprehensive Cancer Network (NCCN) previously recommended
(17) that patients should be
included for repeated fertility-preserving treatments if they met
the following conditions: i) Diagnosed with well-differentiated
EEC; ii) lesions confined to the endometrium, assessed using
ultrasound or MRI, with no suspicious metastatic lesions; iii) no
contraindications for medications; and iv) have been informed that
the fertility preservation option is not the standard treatment for
endometrial cancer. If these conditions are met, a proportion of
women of childbearing age can receive fertility-preserving
treatment. With the rapid development of assisted reproductive
technology, an increasing number of patients with EEC, especially
those in the younger population, have the opportunity to achieve
pregnancy and childbirth despite an EEC diagnosis.
Fertility-sparing management is being increasingly
adopted for younger patients with EEC who wish to preserve their
fertility. However, the CR rate of fertility-sparing therapy can
vary significantly. Qin et al (18) performed a systematic review and
meta-analysis to evaluate the efficacy of progestin treatment for
endometrial cancer. The study identified 25 studies reporting a
total of 445 cases. The CR rate of patients with EEC was 82.4%.
However, Wang et al (19)
reported that the CR rates of patients with EEC and AH were 66.7
and 92.9%, respectively. These CR rates were slightly higher
compared with the above reports demonstrated in the present study.
The present study demonstrated that the CR rates of patients with
EEC and AH were 67.39 and 86.49%, respectively. This may be due to
the short duration of follow-up, in the present study, 10 patients
were only treated for ~4 months and so the follow-up times were
shorter.
In the present study, 16 patients in the EEC group
demonstrated CR ≤6 months after treatment, whereas 28 cases in the
AH group achieved CR ≤6 months. There was a statistically
significant difference between the CR rates of the EEC and AH
groups. The AH group demonstrated a higher CR rate and the time
required for CR was also shorter compared with that in the EEC
group. Therefore, it could be hypothesized that AH may be more
receptive to progestin treatment compared with EEC, with superior
curative effects and a shorter remission time. From the perspective
of histopathology, AH is a precancerous lesion of EEC, where ~25%
of AH cases progress to EEC (5).
The lesion severity and size range (lesions <2 mm) of AH were
weaker and smaller compared with those of EEC, which rendered the
therapeutic effect and time required for CR shorter, which was
consistent with their histological characteristics. Among the 46
cases of EEC in the present study, there were 36 cases with grade 1
and 10 cases with grade 2 EEC. The CR rate of patients with grade 2
EEC (5/10; 50.0%) was markedly lower compared with that of patients
with grade 1 EEC (26/36; 72.22%); however, no significant
difference was demonstrated between the two groups. These results
indicated that there was no difference in the effect of treatment
between these two groups and that progestin treatment was equally
effective against EEC and AH. These results were consistent with
those reported in previous studies (19,20)
but were lower compared with the CR rate of 76.5% reported in the
multicenter retrospective study by Park et al (21), which consisted of patients with
stage Ia, grade G2-G3 EEC without muscular invasion. This suggested
that fertility-preserving treatment could also be attempted in
patients with grade 2 EEC. For patients who desire to preserve
their fertility and meet all other conditions of progestin
treatment, this may be a viable choice. However, the small sample
size in the present study is a limitation. Larger sample sizes are
required to validate the findings of the present study.
The 2018 NCCN guidelines recommended that if
patients suffered from adverse events as a result of
fertility-preserving treatment for 9–12 months and the disease was
not in CR, then surgical treatment was indicated (17). However, at present, there is no
absolute limit for the duration of use of fertility-preserving
treatment. Previous studies have reported that the cumulative
response rate gradually increases as the treatment time increases,
where 10–13% patients require >12 months to achieve CR whilst
not causing recurrence and/or affecting pregnancy outcome (22,23).
The time to reach CR in the present study was a little longer
compared with that reported in the aforementioned studies (21,24),
which was especially the case in the EEC group, where 15 patients
achieved CR in >6 months. The RD rates in the EEC and AH groups
were 22.28% (7/31) and 15.63% (5/32), respectively. There was no
significant difference between these two groups in this regard.
Therefore, the treatment time was longer; however, the RD rate was
not different, which suggested that the treatment was efficacious.
Therefore, if patients wish to preserve their fertility and there
are no contraindications to progestin treatment or severe lesions,
such as muscular infiltration and metastasis, and they have been
explicitly informed that this form of treatment may cause adverse
effects, then fertility-preserving treatment time may be extended
appropriately. In such cases, this therapy could continue, but the
option to terminate treatment at any time should remain open in
cases of emergency.
Numerous immunohistochemical markers have been used
for the diagnosis of EEC and AH. In particular, PR and ER are
reported to be commonly used markers for this disease (25). However, a previous study reported
that as the normal endometrium progressed to the cancerous
endometrium and the pathological grade and clinical stage
increased, ER and PR expression decreased (3). ER and PR have been reported as
potential targets, as progestins primarily mediate their effects
through PR, but an imbalance between estrogen and progestin has
been reported to be involved in the pathogenesis of EEC (26). Previous studies have reported that
PR-positive patients with EEC have superior outcomes following
fertility-preserving treatment (21,27).
Raffone et al (27)
reported that the CR rate of fertility-sparing therapy was 60% in
PR-positive patients with EEC, whereas it was only 18.8% in
PR-negative patients. A retrospective study previously performed by
Travaglino et al (28)
suggested that PR expression was a highly sensitive predictive
marker for conservative EEC and AH treatment. These results were
similar to those of the present study. In the present study,
>50% ER positivity was not demonstrated to confer higher a CR
rate compared with the CR rate demonstrated by the ≤50% ER
positivity group in the EEC and AH groups. However, >50% PR
positivity was found to confer a higher CR rate compared with a
≤50% PR positivity rate in the EEC and AH groups. This suggested
that the expression of PR might have a prognostic implication.
However, reports regarding the utility of hormone receptor
expression for the prediction of the response to progestin therapy
have been controversial, suggesting that there was no significant
difference in the outcome between PR-positive and PR-negative
patients (28). Therefore, a study
using a larger sample is required for verification.
PAX2 is involved in the carcinogenesis of numerous
cancer types through the regulation of cell proliferation and
apoptosis. Loss of PAX2 protein expression has been frequently
reported in EEC and AH (12).
However, PTEN is a tumor suppressor, the expression of which can be
lost through numerous mechanisms, including point mutations in EEC
and AH (29). In the present
study, PAX2 positivity was not demonstrated to confer higher CR
rates compared with PAX2-negative findings among patients with EEC
and AH. PAX2 protein expression was not significantly associated
with prognosis in the EEC group. Similarly, an association between
PTEN protein expression and prognosis was not demonstrated in the
EEC and AH groups before treatment. This was not consistent with
the data previously reported by Chen et al (14). In a previous meta-analysis or
systematic review of fertility-sparing treatment of EEC or AH in
young women, no clear predictive biomarkers which were associated
with remission, recurrence or progression could be identified
following multivariate analysis (30). However, the present study has
certain limitations that should be discussed. The present study was
a single-center retrospective study. Therefore, it remains
difficult to compare the effects of different interventions
directly. Furthermore, the relatively small sample size reduced the
scientific power of the conclusions. A larger sample, prospective
study is required to verify the preliminary findings from the
present study. Moreover, certain patients were under treatment
until the last follow-up, which may have influenced the results of
the present study. Therefore, longer term monitoring and increasing
the frequency of evaluation would be of value in future
studies.
In 2013, The Cancer Genome Atlas divided endometrial
carcinoma into DNA polymerase epsilon mutations, microsatellite
instability high mutant, low copy number and high copy number types
based on the gene mutation spectrum ε mutant (31). Molecular typing can be used to more
accurately estimate patient prognosis and guide treatment design;
its introduction may contribute to the further selection of
patients who are eligible for fertility-sparing treatment (32). The NCCN 2018 guidelines recommended
the molecular typing of EEC for the first time (17). Integration of clinical pathology
and molecular features is expected to be completed for early EEC
risk stratification in patients and for guiding clinical decision
making, which could deepen our understanding into the effects of
fertility-sparing treatment for EEC and AH. Additional studies
based on molecular classification will contribute to more accurate
and individualized treatment strategies.
In summary, fertility-sparing treatment is
relatively effective for patients with EEC and AH who wish to
preserve their fertility. In the AH group, a higher proportion of
patients achieved a CR whilst also achieving this more rapidly
compared with those in the EEC groups PR may also have prognostic
implications as it is a useful marker for the evaluation of EEC and
AH.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
All data generated or analyzed during the present
study are included in this published article.
Authors' contributions
XBZ contributed to data acquisition and drafted and
wrote the manuscript. XYZ, CW, SSL prepared the materials and aided
in the analysis. YQW and YJH contributed to collection of clinical
information. JLW and DHS designed and supervised the study. XBZ,
JLW and DHS confim the authenticity of all the raw data. All
authors have read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of The Peking University People's Hospital (approval no.
2016PHB054-01).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Sung H, Ferlay J, Siegel RL, Laversanne M,
Soerjomataram I, Jemal A and Bray F: Global cancer statistics 2020:
GLOBOCAN estimates of incidence and mortality worldwide for 36
cancers in 185 countries. CA Cancer J Clin. 71:209–249. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sun P, Shen Y, Wang T, He Y, Zhang Y, Tian
W, Yang B and Hu Y: Distinct clinical and genetic mutation
characteristics in sporadic and Lynch syndrome-associated
endometrial cancer in a Chinese population. Cancer Epidemiol.
73:1019342021. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kurman RJ, Carcangiu ML, Herrington CS and
Young RH: WHO Classification of Tumous of Female Reproductive
Organs. IARC Press; Lyon: 2014
|
|
4
|
Chen W, Zheng R, Baade PD, Zhang S, Zeng
H, Bray F, Jemal A, Yu XQ and He J: Cancer statistics in China,
2015. CA Cancer J Clin. 66:115–132. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sanderson PA, Critchley H, Williams A,
Arends MJ and Saunders P: New Concepts for an Old Problem: The
Diagnosis of Endometrial Hyperplasia. Oxford University Press;
2016, View Article : Google Scholar
|
|
6
|
Coakley K, Wolford J and Tewari KS:
Fertility preserving treatment for gynecologic malignancies: A
review of recent literature. Curr Opin Obstet Gynecol. 32:51–56.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Corzo C, Barrientos Santillan N, Westin SN
and Ramirez PT: Updates on conservative management of endometrial
cancer. Obstet Gynecol Surv. 72:715–716. 2017. View Article : Google Scholar
|
|
8
|
Kim YB, Holschneider CH, Ghosh K, Nieberg
RK and Montz FJ: Progestin alone as primary treatment of
endometrial carcinoma in premenopausal women: Report of seven cases
and review of the literature. Cancer. 79:320–327. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Aristizabal P, Graesslin O, Barranger E,
Clavel-Chapelon F, Haddad B, Luton D, Darai E, Rouzier R and Koskas
M: A suggested modification to FIGO stage I endometrial cancer.
Gynecol Oncol. 133:192–196. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Moir-Meyer GL, Pearson JF and Lose F;
Australian National Endometrial Cancer Study Group, ; Scott RJ,
McEvoy M, Attia J, Holliday EG; Hunter Community Study; Studies of
Epidemiology and Risk Factors in Cancer Heredity, ; et al: Rare
germline copy number deletions of likely functional importance are
implicated in endometrial cancer predisposition. Hum Genet.
134:269–278. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Jerzak KJ, Duska L and Mackay HJ:
Endocrine therapy in endometrial cancer: An old dog with new
tricks. Gynecol Oncol. 153:175–183. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Quick CM, Laury AR, Monte NM and Mutter
GL: Utility of PAX2 as a marker for diagnosis of endometrial
intraepithelial neoplasia. Am J Clin Pathol. 138:678–684. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Wheeler DT, Bristow RE and Kurman RJ:
Histologic alterations in endometrial hyperplasia and
well-differentiated carcinoma treated with progestins. Am J Surg
Pathol. 31:988–998. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Chen H, Lucas E, Strickland AL, Carrick K,
Gwin K, Castrillon DH, Rivera-Colon G, Niu S, Molberg KH and Zheng
W: Specific biomarker expression patterns in the diagnosis of
residual and recurrent endometrial precancers after progestin
treatment: A longitudinal study. Am J Surg Pathol. 44:1429–1439.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Bokhman JV: Two pathogenetic types of
endometrial carcinoma. Gynecol Oncol. 15:10–17. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Miller KD, Nogueira L, Mariotto AB,
Rowland JH, Yabroff KR, Alfano CM, Jemal A, Kramer JL and Siegel
RL: Cancer treatment and survivorship statistics, 2019. CA Cancer J
Clin. 69:363–385. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Koh WJ, Abu-Rustum NR, Bean S, Bradley K,
Campos SM, Cho KR, Chon HS, Chu C, Cohn D, Crispens MA, et al:
Uterine neoplasms, version 1.2018, NCCN clinical practice
guidelines in oncology. J Natl Compr Canc Netw. 16:170–199. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Qin Y, Yu Z, Yang J, Cao D, Yu M, Wang Y
and Shen K: Oral Progestin Treatment for early-stage endometrial
cancer: A systematic review and meta-analysis. Int J Gynecol
Cancer. 26:1081–1091. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Wang Y, Yu M, Yang JX, Cao DY, Yuan Z,
Zhou HM, Zhang Y, Li L, Shen K and Wu H: Prolonged conservative
treatment in patients with recurrent endometrial cancer after
primary fertility-sparing therapy: 15-Year experience. Int J Clin
Oncol. 24:712–720. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Hwang JY, Kim DH, Bae HS, Kim ML, Jung YW,
Yun BS, Seong SJ, Shin E and Kim MK: Combined oral
medroxyprogesterone/levonorgestrel-intrauterine system treatment
for women with grade 2 stage IA endometrial cancer. Int J Gynecol
Cancer. 27:738–742. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Park JY, Kim DY, Kim TJ, Kim JW, Kim JH,
Kim YM, Kim YT, Bae DS and Nam JH: Hormonal therapy for women with
stage IA endometrial cancer of all grades. Obstet Gynecol.
122:7–14. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Fan Z, Li H, Hu R, Liu Y, Liu X and Gu L:
Fertility-preserving treatment in young women with grade 1 presumed
stage IA endometrial adenocarcinoma: A meta-analysis. Int J Gynecol
Cancer. 28:385–393. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Chen M, Jin Y, Li Y, Bi Y, Shan Y and Pan
L: Oncologic and reproductive outcomes after fertility-sparing
management with oral progestin for women with complex endometrial
hyperplasia and endometrial cancer. Int J Gynaecol Obstet.
132:34–38. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Rodolakis A, Biliatis I, Morice P, Reed N,
Mangler M, Kesic V and Denschlag D: European society of
gynecological oncology task force for fertility preservation:
Clinical recommendations for fertility-sparing management in young
endometrial cancer patients. Int J Gynecol Cancer. 25:1258–1265.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Srijaipracharoen S, Tangjitgamol S,
Tanvanich S, Manusirivithaya S, Khunnarong J, Thavaramara T,
Leelahakorn S and Pataradool K: Expression of ER, PR, and Her-2/neu
in endometrial cancer: A clinicopathological study. Asian Pac J
Cancer Prev. 11:215–220. 2010.PubMed/NCBI
|
|
26
|
Sherman ME: Theories of endometrial
carcinogenesis: A multidisciplinary approach. Mod Pathol.
13:295–308. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Raffone A, Travaglino A, Saccone G, Mollo
A, De Placido G, Insabato L and Zullo F: Should progesterone and
estrogen receptors be assessed for predicting the response to
conservative treatment of endometrial hyperplasia and cancer? A
systematic review and meta-analysis. Acta Obstet Gynecol Scand.
98:976–987. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Travaglino A, Raffone A, Saccone G,
Insabato L, Mollo A, De Placido G and Zullo F: Immunohistochemical
predictive markers of response to conservative treatment of
endometrial hyperplasia and early endometrial cancer: A systematic
review. Acta Obstet Gynecol Scand. 98:1086–1099. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Monte NM, Webster KA, Neuberg D, Dressler
GR and Mutter GL: Joint loss of PAX2 and PTEN expression in
endometrial precancers and cancer. Cancer Res. 70:6225–6232. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Jing W, Zhang W, Feng L and Gao W:
Comparison of fertility-sparing treatments in patients with early
endometrial cancer and atypical complex hyperplasia: A
meta-analysis and systematic review. Medicine (Baltimore).
96:e80342017. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Cancer Genome Atlas Research Network, .
Kandoth C, Schultz N, Cherniack AD, Akbani R, Liu Y, Shen H,
Robertson AG, Pashtan I, Shen R, et al: Integrated genomic
characterization of endometrial carcinoma. Nature. 497:67–73. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Horak P: Gene signature profiling of
gynaecological malignancies. Memo-Mag Eur Med Oncol. 7:252–255.
2014.
|