Introduction
As a major cause of cancer-related death in the
world, gastric cancer (GC) remains the third most frequent cause of
cancer-related death worldwide, resulting in 782,685 deaths
annually, with a 5-year survival rate of only 20–30% after curative
resection (1). Radical surgical
resection is the preferred treatment for GC, supplemented by
combined perioperative radiotherapy, chemotherapy and biotherapy.
It is worth mentioning that numerous factors affect the prognosis
and treatment strategies of patients with GC (1,2), such
as Lauren classification, degree of differentiation and TNM
staging, and the clinical and pathological features of GC are an
important consideration. Accurate preoperative evaluation of the
clinical and pathological features of GC is conducive to treatment
plan formulation and prognosis evaluation (2). At present, as a common screening
method for clinically suspicious gastric space-occupying lesions,
upper gastrointestinal barium X-ray examination is especially
suitable for patients who have suspicious gastric mucosa and
morphological changes (3). There
have been few clinical studies based on upper gastrointestinal
barium X-ray examination, and to the best of our knowledge, the
associations between the gastric morphological types and
clinicopathological features of GC have not been reported in the
literature. Given this, the present study analyzed the association
between gastric morphological type, and the clinical and
pathological features of GC in order to provide a clinical
reference.
Patients and methods
Patients and study design
The study was approved by the Institutional Review
Board of The First Hospital of Zhengzhou University (Zhengzhou,
China; approval no. 2021-KY-1070-002). The requirement for written
informed consent was waived by the Institutional Review Board due
to the retrospective nature of the study. A total of 329 patients
with GC who had undergone radical surgical resection in the First
Affiliated Hospital of Zhengzhou University between January 2020
and April 2021 were retrospectively selected following application
of inclusion and exclusion criteria. There were 245 males and 84
females, with a male-to-female ratio of ~3:1. The mean age (±SD)
was 65±14 years (age range, 28–86 years). The medical history of
all patients in this study included the following: Hypertension
(n=42), diabetes (n=16), cholecystectomy for cholecystolithiasis
(n=6), hepatitis B (n=3), chronic gastritis (n=8), herpes zoster
(n=1), polypectomy of the colon (n=1), lymphoma of the bile duct
(n=1), rheumatoid arthritis (n=1), hysteromyoma surgery (n=6),
coronary heart disease (n=7), appendicectomy for appendicitis
(n=2), parotid adenoma surgery (n=1), thyroid cancer resection
(n=1), pneumoconiosis (n=1), ovarian tumor removal (n=1), pulmonary
tuberculosis (n=1), pulmonary heart disease (n=1), prostate surgery
(n=1), rectal cancer resection (n=1) and lipoma resection (n=1).
The ICD-10 classification codes of the cancer types included in
this study were C15-C26 (4).
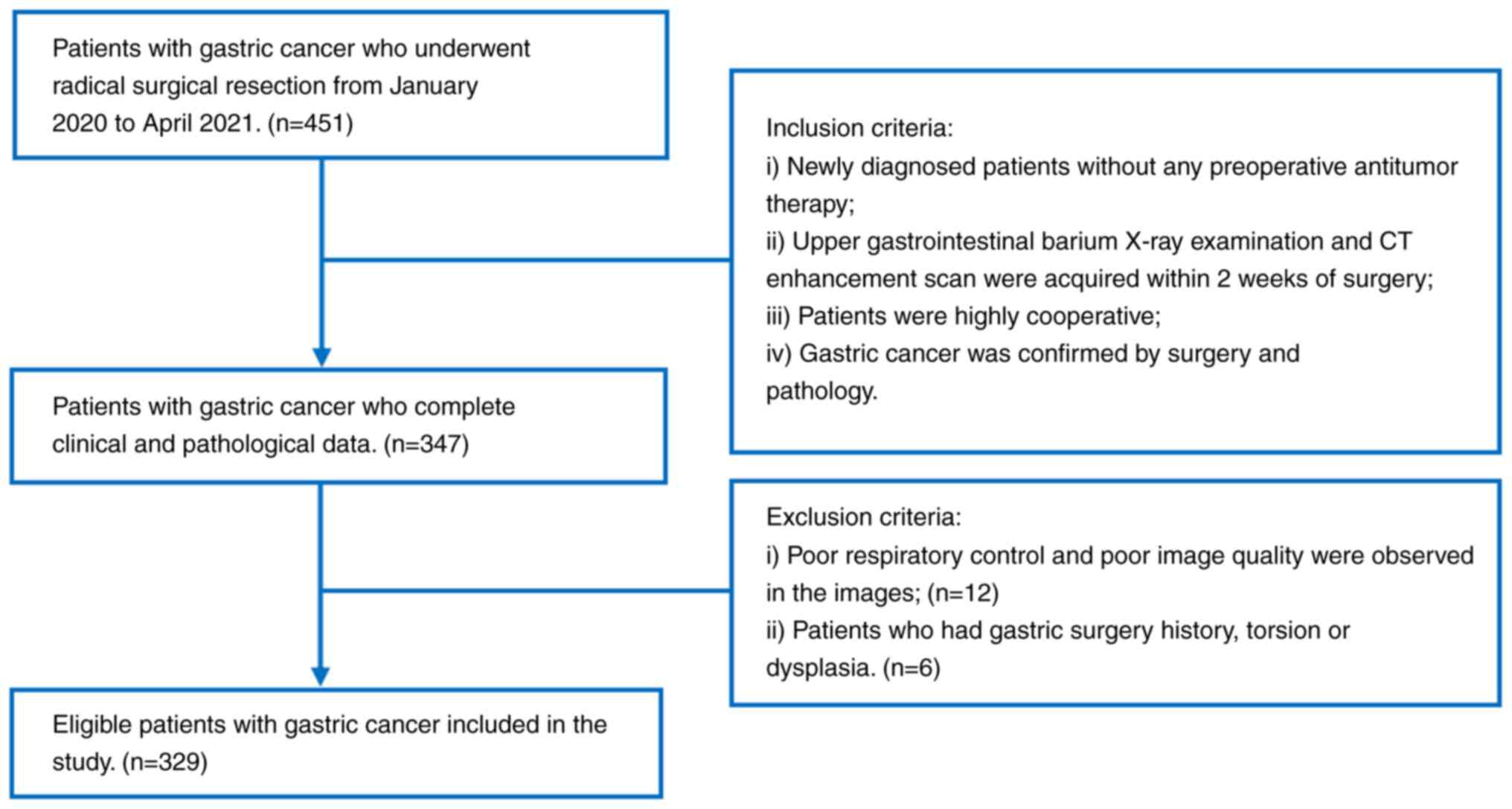
The inclusion criteria were as follows: i) Newly
diagnosed patients without any preoperative antitumor therapy; ii)
upper gastrointestinal barium X-ray examination acquired within 2
weeks of surgery; iii) patients were highly cooperative in order to
complete the examination; and iv) gastric adenocarcinoma confirmed
by surgery and pathology data. The exclusion criteria were as
follows: i) Poor respiratory control and poor image quality
observed in the images; and ii) patients who had gastric surgery
history, torsion or dysplasia. The flow chart for the study
population recruitment is shown in Fig.
1.
Upper gastrointestinal barium X-ray
examination
The upper gastrointestinal barium X-ray examination
was performed using the Shimadzu digital gastrointestinal machine
(Social Vision SafireII; Shimadzu Corporation). The ‘automatic’
option was selected for gastrointestinal fluoroscopy. Before the
examination, the patients fasted for 10–12 h, and oral doses of
barium were administered at 150–250 ml immediately before
examination. The mucosa, filling and pressure phases were observed.
The shape, outline, position, size, peristalsis and pylorus opening
of the stomach were observed in different body positions and
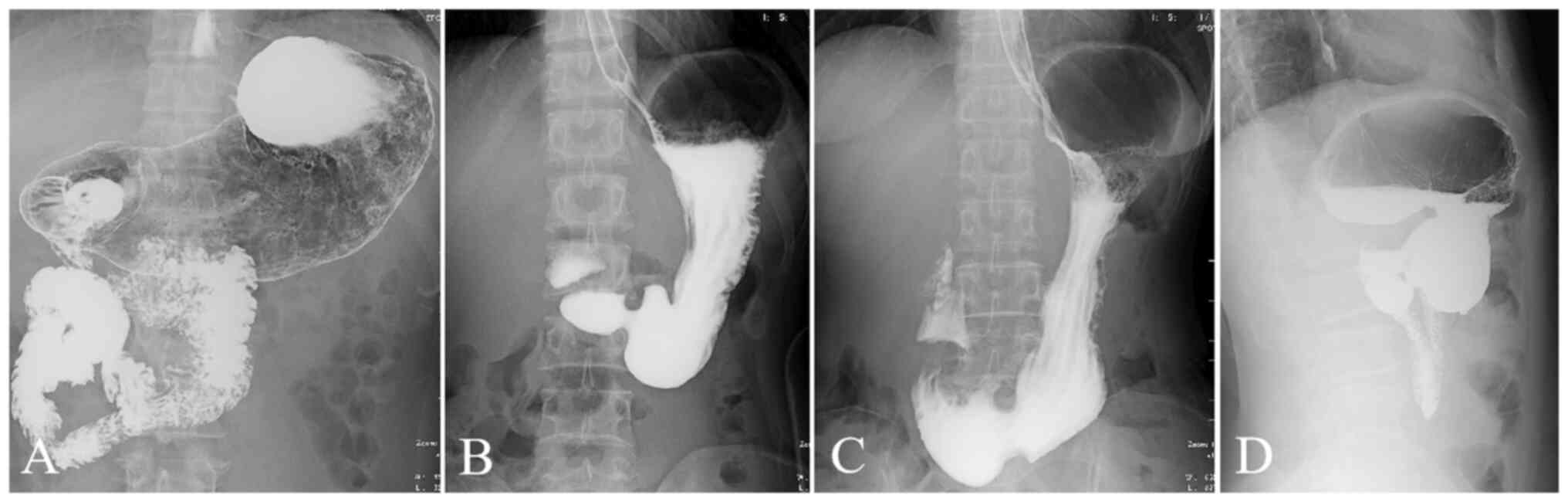
filling states, and X-ray films were taken. According to the
different morphological features, the gastric morphology was
divided into four types (Fig. 2):
The horn-type, hook-type, weak-type and waterfall-type stomach. The
horn-shaped stomach has a high position and tension, is horizontal,
wide in the upper part and narrow in the lower part, and the
stomach angle is not obvious. This type of gastric morphology is
commonly seen in obese people. The hook-shaped stomach has a
moderate position and tension, an obvious gastric angle and the
lower gastric pole is roughly at the level of the iliac crest. The
weak-type stomach has a low position and tension. The upper stomach
cavity is narrow and wide like a water bag, while the lower part of
the stomach is often below the level of the iliac crest. This type
of gastric morphology is commonly seen in slender people. In the
waterfall-type stomach, the fundus of the stomach is in the shape
of a sac, the stomach is large, the body of the stomach is small
and the tension is high. The gastric morphological type was
analyzed by two senior physicians, with 4 and 10 years of
experience in abdominal radiology, respectively, who were blinded
to the clinical information and pathological results.
Statistical analysis
Statistical analyses were performed using SPSS
software version 23.0 (IBM Corp.). The categorical variables are
presented as frequencies and percentages. The χ2 test or
Fisher's exact test were used to assess categorical variables
(gastric types of GC and age, sex, site, differentiation degree,
Lauren classification and T staging). Two-sided P<0.05 was
considered to indicate a statistically significant difference.
Results
In this study of 329 patients with GC, 160 cases
(48.63%) were of the hook-type stomach, 12 cases (3.65%) were of
the horn-type stomach, 91 cases (27.66%) were of the weak-type
stomach and 66 cases (20.06%) were of the waterfall-type stomach.
Among the 245 male patients, there were 10 cases of the horn-type
stomach, 123 cases of the hook-type stomach, 45 cases of the
weak-type stomach and 67 cases of the waterfall-type stomach. Among
the 84 female cases, there were 2 cases of the horn-type stomach,
37 cases of the hook-type stomach, 21 cases of the weak-type
stomach and 24 cases of the waterfall-type stomach. The
classification and distribution in patients with GC of different
sexes were similar, and the most common type was the hook-type
stomach, followed by the waterfall-type stomach. A total of 134
cases (40.73%) of GC were located in the upper stomach, 74 cases
(22.49%) in the middle stomach and 121 cases (36.78%) in the lower
stomach, with the hook-type and horn-type GC being more common in
the lower stomach, and the waterfall-type GC being mainly located
in the upper stomach. There were 156 cases of poorly differentiated
GC (47.42%) and 173 cases of non-poorly differentiated GC (52.58%),
among which the incidence of non-poorly differentiated GC in the
waterfall-type stomach was higher than that in other gastric types
and the incidence of poorly differentiated GC in the horn-type
stomach was more common. There were 73 cases of diffuse-type GC
(22.19%), 131 cases of intestinal-type GC (39.82%), and 125 cases
of mixed-type GC (37.99%), among which the incidence of
intestinal-type GC in the waterfall-type stomach was higher than
that in the other gastric types and the incidence of mixed-type GC
in the horn-type stomach was more common. There were 76 cases of T1
+ T2 GC (23.10%), 163 cases of T3 GC (49.54%) and 90 cases of T4 GC
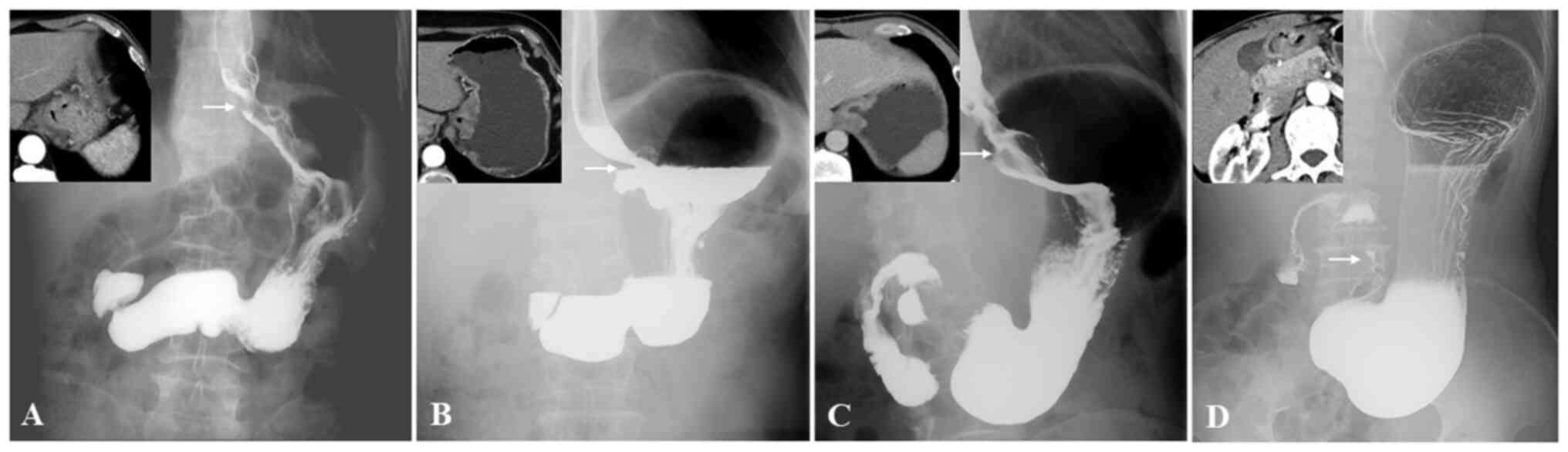
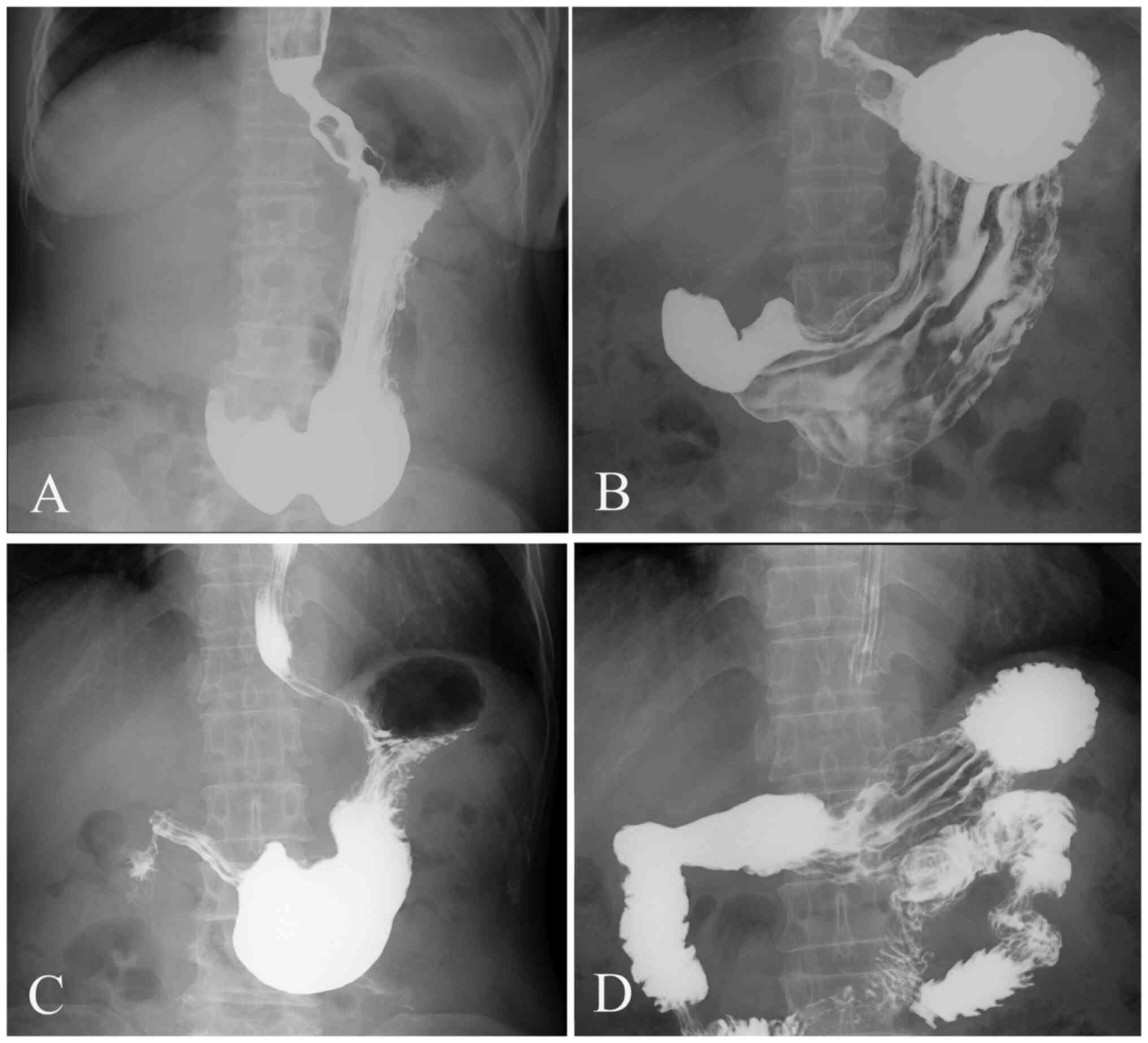
(27.36%). There was a statistically significant difference in the
T-staging of GC between different gastric morphological types. The
incidence of T1 + T2 GC in the hook-type stomach was higher than
that in other gastric morphological types and T3 GC was present at
the highest proportion among the four gastric morphological types.
Overall, there were statistically significant differences in the
site and T stage of GC classified by different gastric
morphological types (Figs. 3 and
4), as shown in Table I.
 | Table I.Comparison of clinicopathological
features of patients with gastric cancer and different gastric
morphological types. |
Table I.
Comparison of clinicopathological
features of patients with gastric cancer and different gastric
morphological types.
| Variables | Hook-type stomach,
n | Horn-type stomach,
n | Waterfall-type
stomach, n | Weak-type stomach,
n | χ2 | P-value |
|---|
| Age, years |
|
|
|
| 3.40 | 0.334 |
| ≤60 | 76 | 3 | 45 | 27 |
|
|
|
>60 | 84 | 9 | 46 | 39 |
|
|
| Sex |
|
|
|
| 2.39 | 0.496 |
| Male | 123 | 10 | 67 | 45 |
|
|
|
Female | 37 | 2 | 24 | 21 |
|
|
| Site |
|
|
|
| 14.72 | 0.023 |
|
Upper | 54 | 8 | 46 | 26 |
|
|
|
Middle | 37 | 2 | 23 | 12 |
|
|
|
Lower | 69 | 2 | 22 | 28 |
|
|
| Differentiation |
|
|
|
| 3.93 | 0.267 |
| Poorly
differentiated | 77 | 8 | 37 | 34 |
|
|
|
Non-poorly differentiated | 83 | 4 | 54 | 32 |
|
|
| Lauren
classification |
|
|
|
| 7.44 | 0.282 |
| Diffuse
type | 36 | 4 | 18 | 15 |
|
|
|
Intestinal type | 63 | 1 | 43 | 24 |
|
|
| Mixed
type | 61 | 7 | 30 | 27 |
|
|
| T staging |
|
|
|
| 16.87 | 0.010 |
| T1 +
T2 | 52 | 1 | 12 | 11 |
|
|
| T3 | 68 | 7 | 54 | 34 |
|
|
| T4 | 40 | 4 | 25 | 21 |
|
|
Discussion
Compared with electronic gastroscopy, ultrasound
endoscopy and CT gastric reconstruction, upper gastrointestinal
barium X-ray examination in clinical application is less commonly
used. However, upper gastrointestinal barium X-ray examination is
still a necessary examination before the surgery for gastric
space-occupying lesions, as it can provide images of gastric
motility that other examination techniques cannot show, in addition
to the morphological changes; it is a simple, easy, non-invasive
and less painful technique, and the interpretation and judgment of
the results is intuitive (5). Upper
gastrointestinal barium X-ray examination can show the location,
shape, depth and size of GC, as well as the relationship between
adjacent organs and tissues (5). At
the same time, the peristalsis and softness of the gastric wall at
the site of the lesion can be observed to determine whether there
are functional abnormalities (5).
The value of upper gastrointestinal barium X-ray
examination in the diagnosis of disease has always been a knowledge
point that must be mastered during the training period in higher
medical education. Therefore, the importance and particularity of
upper gastrointestinal barium X-ray examination in clinical work
and personnel training can be seen. Given this, we consider that
upper gastrointestinal barium X-ray examination in gastric disease
should be fully explored in terms of its clinical value, so that
the clinical application of this technology can be awarded greater
value. The clinical application value of upper gastrointestinal
barium X-ray examination has been reported in the literature, such
as its ability to differentially diagnose the waterfall-type
stomach and gastric torsion (6),
and the weak-type stomach and mild gastroptosis (7). It is worth mentioning that, in the
past, upper gastrointestinal barium X-ray examination studies
concentrated on lesion detection, and a study did analyze the
invasion depth of the tumor based on upper gastrointestinal barium
X-ray examination (8); however,
previous studies were limited to the morphological features of
pathological changes. There has been little literature about the
associations between gastric morphological type and the
clinicopathological features of patients with GC based on
double-contrast barium X-ray imaging.
The gastric morphological type is a descriptive term
based on anatomical features, which were related to the body shape,
gastric cavity position and tension (3). The morphological assessment in the
present study was not of the morphological changes of the GC
itself, but rather the upper gastrointestinal barium X-ray
examination showed the gastric morphological type, that is, the
horn-type, hook-type, weak-type and waterfall-type stomach. The
purpose of the present study was to expand the application value of
upper gastrointestinal barium X-ray examination in patients with
GC, that is, in addition to the conventional display of mucosal
changes, ulcers and peripheral mucosal lesions, the purpose of this
study was to demonstrate the biological behavior of GC. Upper
gastrointestinal barium X-ray examination has played a very
important role in clinic. For medical institutions without CT
equipment or contrast-enhanced ultrasound examination, the more
popular upper gastrointestinal barium X-ray examination can be
applied, and the detection, diagnosis, and preliminary analysis of
biological behavior of gastric space-occupying lesions can be
performed to improve clinical treatment. As an upper
gastrointestinal barium X-ray examination is a necessary
examination before surgery in The First Affiliated Hospital of
Zhengzhou University, if the value of this technique is expanded,
the biological behavior of gastric space-occupying lesions can be
investigated preliminarily, which can be confirmed by CT equipment
or contrast-enhanced ultrasonography at a later stage, and has
great clinical application value.
Among the gastric morphological types, the hook-type
stomach is the most common, followed by the horn-type stomach. The
present study showed that there were 160 cases of hook-type
stomach, accounting for 48.63% of all cases (160/329), which was
higher than the number of the other three types. TO the best of our
knowledge, a study on the relationship between gastric
morphological type and sex in patients with GC has not been
reported. In the present study, it was found that the
classification and the distribution of the gastric morphological
type among the different sexes were similar, with the hook-type
stomach being the most common, followed by the waterfall-type
stomach.
In a previous study, the site of GC was recorded as
an independent risk factor for the prognosis of patients with GC,
and the prognosis of GC at different sites varied (9). Therefore, it is of great clinical
importance to compare the clinicopathological characteristics of GC
at different sites. With the change of lifestyle and the influence
of natural environmental factors, epidemiological studies on the
occurrence site of GC have shown that compared with that of distal
GC, the incidence of proximal GC is on the rise, and the incidence
of the cancer in the cardia and gastric body is common (10). In the present study, the occurrence
site of GC was the upper stomach in 134 cases (40.73%), the middle
stomach in 74 cases (22.49%) and the lower stomach in 121 cases
(36.78%). The study further analyzed the association between
gastric morphological types and the site of GC. The results showed
that there were differences in terms of the site of GC in patients
with different gastric morphological types, with the hook-type and
horn-type being most common in the lower stomach, while the upper
stomach mainly contained waterfall-type GC.
Accurate preoperative assessment of GC
differentiation is of great importance for the selection of
individualized treatment and prognosis evaluation (11). Studies have pointed out that the
enhancement mode of GC is closely related to the pathological basis
and microvascular structure (12–14).
GC with a low differentiation degree has dense and regular surface
blood vessels and more deep fibrous connective tissue, which is
more likely to show continuous enhancement (12). Therefore, it is difficult to
evaluate the differentiation degree of GC by gastric barium X-ray
radiography. In more recent years, relevant imaging literature
reports have mostly been based on CT enhanced examination, such as
three-stage CT enhanced imaging (12), CT perfusion imaging (13) and CT energy imaging (14). The present study showed that the
incidence of non-poorly differentiated GC in the waterfall-type
stomach was higher than that in other gastric types, and the
incidence of poorly differentiated GC in the horn-type stomach was
common.
In the past, it was considered that an upper
gastrointestinal barium X-ray examination could not diagnose the
depth of invasion and the metastasis of the surrounding lymph nodes
and distant organs, so it could not be used for the evaluation of
GC staging. However, the deeper the degree of invasion of GC, the
more significant the degree of gastric wall stiffness in the upper
gastrointestinal barium X-ray examination (15). Given this, the stiffness of the
gastric wall can provide a preliminary reference for the clinical
evaluation of surgical indications. It is worth mentioning that, to
the best of our knowledge, there has been no correlation study
between gastric morphological types and T staging. The present
study showed that there were statistically significant differences
in the T-stage distribution of GC according to the gastric
morphological types. The incidence of stage T1+T2 GC in the
hook-type stomach was higher than that in other gastric types, and
the proportion of stage T3 GC was the highest among the gastric
morphological types.
The 2010 World Health Organization classification
recognizes four major histological patterns of GC (16,17):
Tubular, papillary, mucinous and poorly cohesive (including signet
ring cell carcinoma), plus an uncommon histological variant. As the
pathological examination of The First Affiliated Hospital of
Zhengzhou University did not distinguish between tubular and
papillary adenocarcinoma, all cases were reported as just
adenocarcinoma. In this retrospective study, the distribution
characteristics of the samples were carefully checked, and of the
329 patients, 256 were pathologically reported as cases of
adenocarcinoma, 20 as cases of mucinous adenocarcinoma and 53 as
cases of signet ring cell carcinoma. Further analysis of the
association between the four major histological patterns of GC and
the gastric morphological types may be helpful to further expand
the scope of application and the clinical value of examination,
which will be analyzed in future research.
There are a number of limitations to the present
study. As a preliminary screening method, the upper
gastrointestinal barium X-ray examination lacks quantitative
parameters, which makes it difficult to conduct an in-depth
comparative analysis with pathology data. There are also certain
differences in the number of samples among gastric morphological
types, which need to be further assessed using large sample data.
Furthermore, T1 and T2 stage GC were not separately discussed. The
reasons for combining the T1 and T2 stages are as follows: i) T1
stage GC is rare, which can be confirmed from the previously
published studies on early GC and clinical work; and ii) in
clinical work, most of the patients with T1 and T2 stage GC can be
treated by radical resection. In order to be closer to the
situation in the clinic, these two groups of patients with GC
should be combined to improve the value of upper gastrointestinal
barium X-ray examination. Furthermore, prognostic information was
not available for the patients in the study. The follow-up
observations have been made for the patients included in this
study, but it should be noted that the lack of contact information
in some patients affected the observations in this study. In
addition, the focus of this study was to observe the relationship
between the gastric morphological type on upper gastrointestinal
barium X-ray examination and its biological behavior. In the
follow-up study, focus will be placed on the patient's prognostic
information.
In conclusion, the present study found an
association between gastric morphological type, and the clinical
and pathological features of patients with GC on upper
gastrointestinal X-ray imaging. There were differences with regard
to incidence site and T-stage distribution of gastric morphological
types, which may be used as a supplementary factor for making a
diagnosis.
Acknowledgements
Not applicable.
Funding
This study was supported by the Outstanding Youth Project in
Henan Province for Young and Middle-aged Health and Health
Technology Innovation (grant no. YXKC2020053).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
PL is the primary author. PL and JBG designed the
study. JBG critically reviewed the paper and revised it. PL, BZ,
XCR, DL and MC performed the database search and literary review.
BZ performed the statistical analysis. PL, BZ, XCR, DL and MC
analysed the data. PL and JBG confirm the authenticity of all the
raw data. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Institutional Review
Board of The First Affiliated Hospital of Zhengzhou University
(approval no. 2021-KY-1070-002). The requirement for written
informed consent was waived by the Institutional Review Board due
to the retrospective nature of the study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Sun KY, Hu HT, Chen SL, Ye JN, Li GH, Chen
LD, Peng JJ, Feng ST, Yuan YJ, Hou X, et al: CT-based radiomics
scores predict response to neoadjuvant chemotherapy and survival in
patients with gastric cancer. BMC Cancer. 20:4682020. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Wang K, Jiang X, Ren Y, Ma Z, Cheng X, Li
F, Xiao J, Yu Z and Jiao Z: The significance of preoperative serum
carcinoembryonic antigen levels in the prediction of lymph node
metastasis and prognosis in locally advanced gastric cancer: A
retrospective analysis. BMC Gastroenterol. 20:1002020. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Yamamichi N, Shimamoto T, Hirano C,
Takahashi Y, Minatsuki C, Takeuchi C, Takahashi M, Sakaguchi Y,
Tsuji Y, Niimi K, et al: Clinicopathological features and prognosis
of developed gastric cancer based on the diagnosis of mucosal
atrophy and enlarged folds of stomach by double-contrast upper
gastrointestinal barium X-ray radiography. Clin J Gastroenterol.
14:947–954. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Roderburg C, Loosen SH, Jördens MS, Konrad
M, Luedde T, Kostev K and Luedde M: Heart failure and dementia: A
comparative analysis with different types of cancer. Eur Heart J
Open. 1:oeab0032021. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Yamamichi N, Hirano C, Shimamoto T,
Minatsuki C, Takahashi Y, Nakayama C, Matsuda R, Fujishiro M,
Konno-Shimizu M, Kato J, et al: Associated factors of atrophic
gastritis diagnosed by double-contrast upper gastrointestinal
barium X-ray radiography: A cross-sectional study analyzing 6,901
healthy subjects in Japan. PLoS One. 9:e1113592014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Patoulias D, Rafailidis V, Kalogirou M,
Farmakis K, Rafailidis D and Patoulias I: Acute primary
mesenteroaxial gastric volvulus in a 6 years old child; the
contribution of ultrasonographic findings to the prompt diagnosis
(a case report and review of the literature). Folia Med Cracov.
57:47–55. 2017.PubMed/NCBI
|
|
7
|
Wang YJ, Hung KL, Yang JN, Yang JN, Wang
TC and Chin CH: Gastric anatomic type is associated with obesity
and gender. Obes Facts. 9:221–229. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yang ZH, Gao JB, Yue SW, Guo H and Yang
XH: X-ray diagnosis of synchronous multiple primary carcinoma in
the upper gastrointestinal tract. World J Gastroenterol.
17:1817–1824. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Zhao L, Huang H, Zhao D, Wang C, Tian Y,
Yuan X, Ma F, Ren H, Zhao Y, Aimaiti S, et al: Clinicopathological
characteristics and prognosis of proximal and distal gastric cancer
during 1997–2017 in china National cancer center. J Oncol.
2019:97840392019. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kim DH, Park CH, Park SY, Cho E, Kim HS
and Choi SK: Diagnostic yields of endoscopic ultrasound-guided
fine-needle tissue acquisition according to the gastric location.
Medicine (Baltimore). 100:e264772021. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Zeydanli T and Kilic HK: Performance of
quantitative CT texture analysis in differentiation of gastric
tumors. Jpn J Radiol. 40:56–65. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lee JS, Kim YS, Kim EY and Jin W:
Prognostic significance of CT-determined sarcopenia in patients
with advanced gastric cancer. PLoS One. 13:e02027002018. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Zongqiong S, Xiaohong L, Wei C, Jiangfeng
Z, Yuxi G, Zhihui X, Linfang J, Yong P and Gen Y: CT perfusion
imaging of the stomach: A quantitative analysis according to
different degrees of adenocarcinoma cell differentiation. Clin
Imaging. 40:558–562. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Xu JJ, Taudorf M, Ulriksen PS, Achiam MP,
Resch TA, Nielsen MB, Lönn LB and Hansen KL: Gastrointestinal
applications of iodine quantification using Dual-Energy CT: A
systematic review. Diagnostics (Basel). 10:8142020. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gotoda T, Ishikawa H, Ohnishi H, Sugano K,
Kusano C, Yokoi C, Matsuyama Y and Moriyasu F: Randomized
controlled trial comparing gastric cancer screening by
gastrointestinal X-ray with serology for Helicobacter pylori and
pepsinogens followed by gastrointestinal endoscopy. Gastric Cancer.
18:605–611. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kim YH, Kim JH, Kim H, Kim H, Lee YC, Lee
SK, Shin SK, Park JC, Chung HS, Park JJ, et al: Is the recent WHO
histological classification for gastric cancer helpful for
application to endoscopic resection? Gastric Cancer. 19:869–875.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hu B, El Hajj N, Sittler S, Lammert N,
Barnes R and Meloni-Ehrig A: Gastric cancer: Classification,
histology and application of molecular pathology. J Gastrointest
Oncol. 3:251–261. 2012.PubMed/NCBI
|