Introduction
Synovial sarcoma (SS) is the fourth most common type
of soft tissue sarcoma (STS) and accounts for 5–10% of all STS
cases (1–3). SS most commonly arises in the deep
soft tissue of the lower extremities, and ~7% of SS cases originate
in the head and neck region, predominantly in the hypopharynx and
parapharyngeal spaces (4,5). The term ‘synovial sarcoma’ was first
proposed by Knox in 1936 because the tumor histologically resembled
normal synovial tissue (6);
however, this was a misnomer because SS does not originate from
synovium. The widespread distribution of SS and the uncertain
differentiation make the precise origin of SS still controversial;
however, the prevalent onset in proximity of joints, bones, and
skeletal muscles suggested a multipotent mesenchymal stem cell
origin (7). STS occurring primarily
within the bone is very rare (1,8,9), and
only nine cases of SS in the mandible have been reported thus far
(10–18).
As SS lacks characteristic symptoms and imaging
findings, the clinical diagnosis of SS is often difficult. The
present study presented an extremely rare case of monophasic SS
arising from the mandibular bone marrow and described its clinical,
imaging, histological, and immunohistochemical features.
Case report
A 54-year-old woman was referred to our hospital
with complaints of numbness and touch-evoked pain in the area
innervated by left mental nerve area. The patient was otherwise
healthy. She developed pain on mastication four months prior to the
initial visit to Kyushu University Hospital (Fukuoka, Japan) and
was diagnosed with temporomandibular joint disorder at a dental
clinic and treated with an occlusal splint. However, the symptoms
worsened with numbness appearing in the left chin. The patient was
referred to an otolaryngologist, orthopedic surgeon, and
neurosurgeon, but no abnormalities were noted. Therefore, she was
referred to Kyushu University Hospital by the dental clinic for
examination and treatment.
On initial examination, there was a slightly hard
mass measuring 23×13 mm with spontaneous pain posterior to the left
second molar. The mucosa overlying the mass was normal and
non-adherent. Limited mouth opening limitation and enlargement of
the regional lymph nodes were not observed. Neuropathy, such as
allodynia and hypoesthesia, was observed objectively in the left
mental nerve area. There was no medical history of induced
neuropathy; therefore, radiological examinations were planned to
determine the origin of the disease.
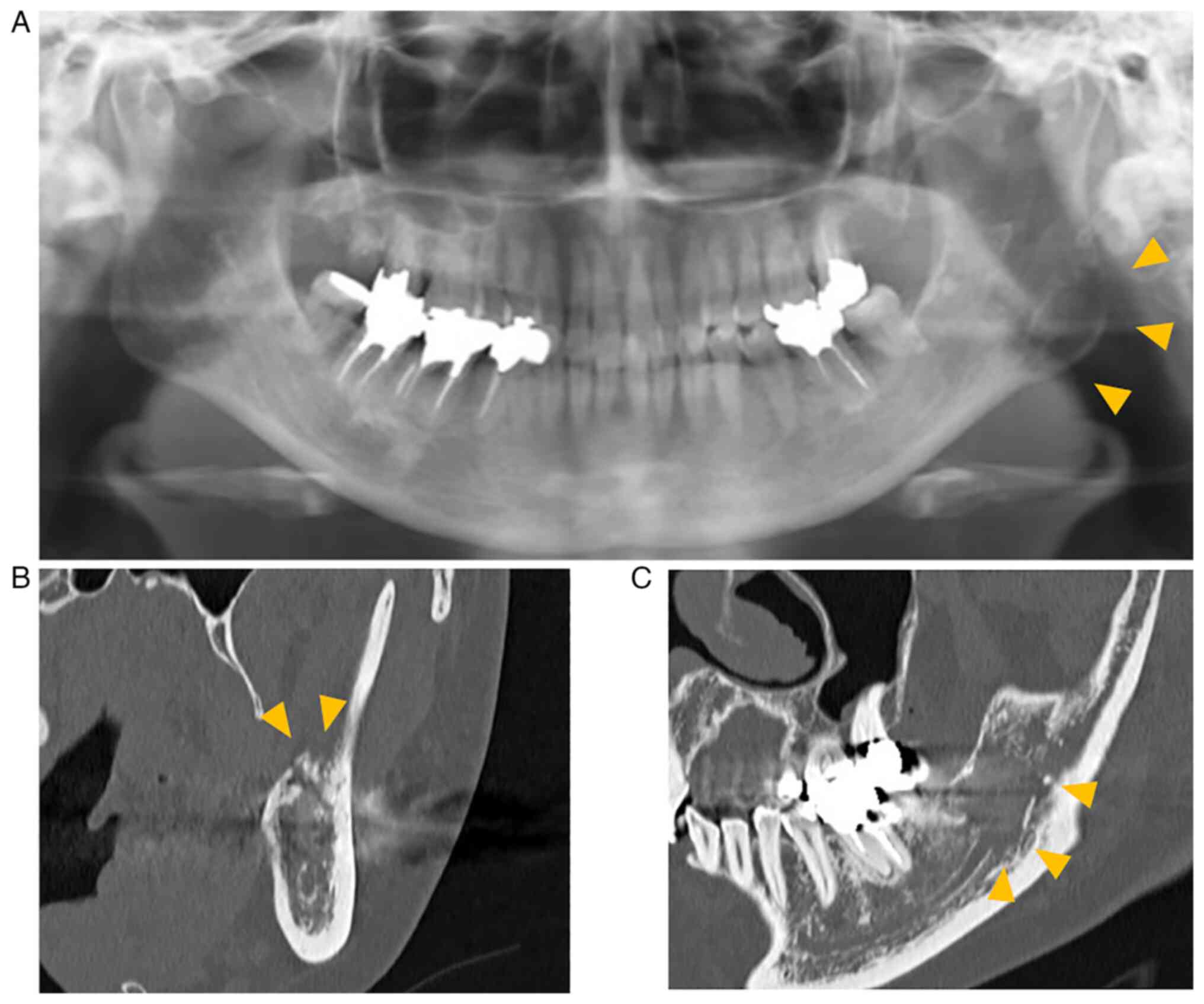
Panoramic radiography showed a poorly marginated
radiolucent area in the left mandibular angle and ramus (Fig. 1A). Computed tomography (CT) revealed
changes from marrow to soft tissue in the left mandible, small
perforations in the cortical bone under the mass, and destruction
of the left mandibular canal (Fig. 2B
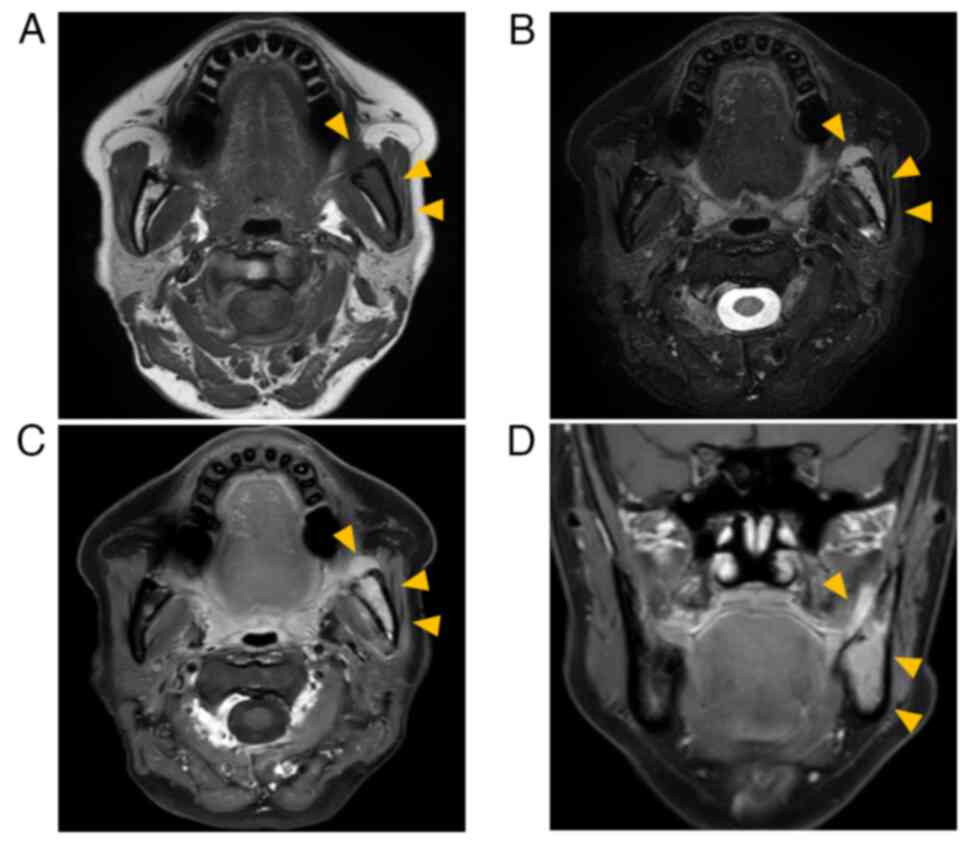
and C). Magnetic resonance imaging (MRI) revealed an isointense
mass on T1-weighted images (T1-WI) and hyperintensity on
T2-weighted images (T2-WI) in the bone marrow between the left
lower molar region and the left mandibular notch. The mass had an
extraosseous extension, and its maximum width and length were 55
and 25 mm, respectively. The tumor was homogeneously enhanced by
gadobutrol (Gd-BTDO3A) (Fig. 2A-D).
Positron emission tomography-CT showed mild fluorodeoxyglucose
uptake in the extraosseous mass but no other lesions in distant
organs. Blood biochemical test results did not reveal any
abnormalities. The patient was clinically diagnosed with malignant
lymphoma.
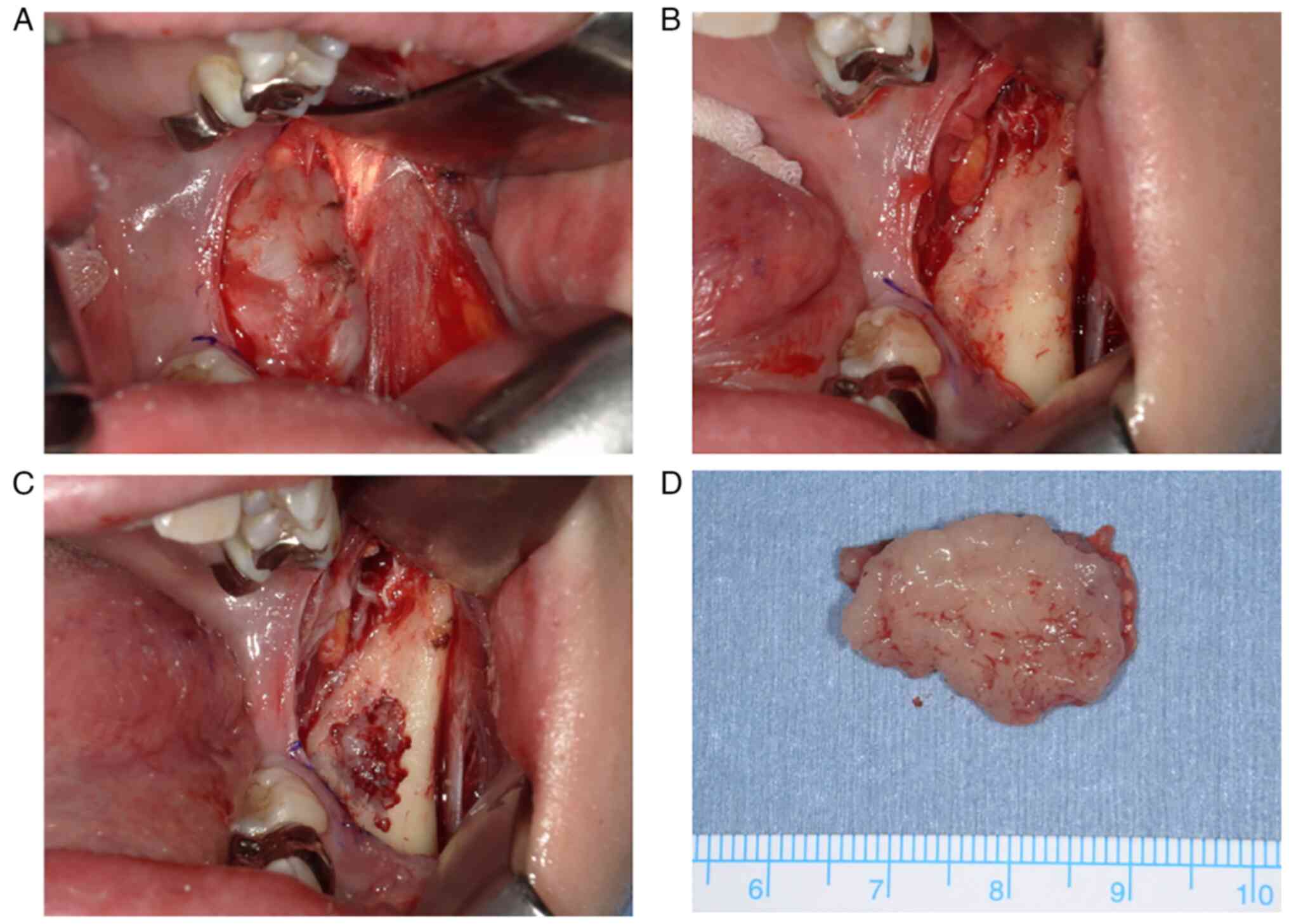
Biopsies were performed under general anesthesia.
The possibility of solid tumors could not be completely ruled out,
and tissue detachment was minimized to prevent dissemination. The
extraosseous tumor lay under the periosteum; therefore, the tumor
was removed along with the periosteum. The extraosseous tumor was
easily detached from the mandible, and there were small holes in
the cortical bone in contact with it. The mass was fragile and
yellowish white. Intraosseous tissue was also collected from the
bone marrow with small cortical bone removal because it could
represent a different disease. Gross findings of the extraosseous
and intraosseous tumors were the same (Fig. 3). The specimens were then subjected
to histopathological examination. Imprint cytology was performed
immediately, but malignant lymphoma was ruled out. Remaining
specimens were fixed with 10% formalin neutral buffer solution for
24 h at room temperature. Fixed sections were embedded in paraffin
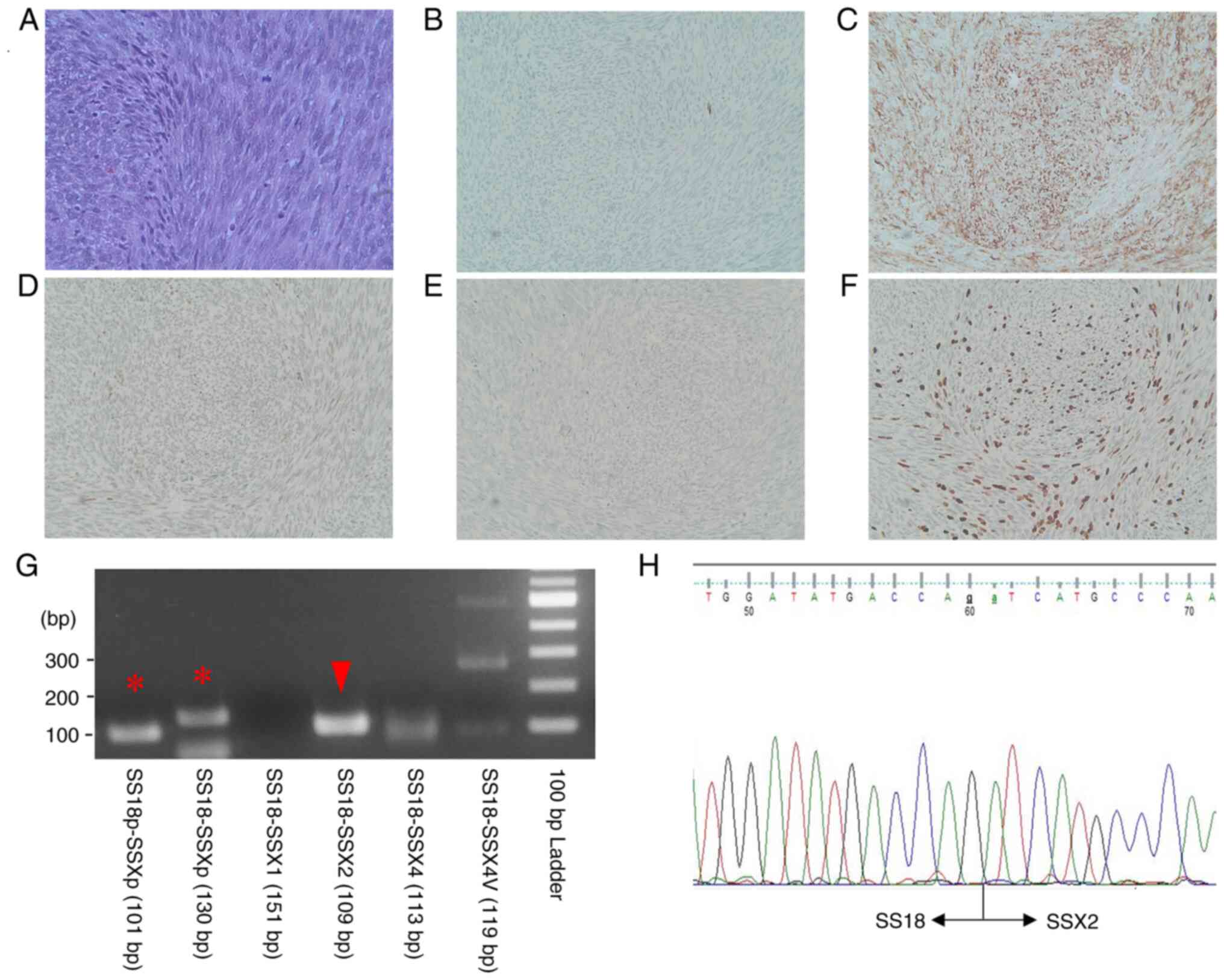
and 4-µm-thick tissue sections were stained. Routine hematoxylin
and eosin (H&E)-stained sections showed a dense proliferation
of oval to spindle-shaped cells with hyperchromatic nuclei arranged
in a fascicular pattern (Fig. 4A).
Mitotic figures were frequently seen (15 mitoses in 10 high-power
fields). Immunohistochemical staining except for SWI/SNF related
matrix associated actin dependent regulator of chromatin subfamily
b/integrase interactor 1 (SMARCB/INI1) were performed using a fully
automated system [Leica Bond-III (Leica Microsystems GmbH) or
VENTANA BenchMark ULTRA (Roche Applied Science)] and the following
primary antibodies: Pan-cytokeratin (AE1/AE3; IS053; Dako; Agilent
Technologies, Inc.), smooth muscle actin (SMA; cat. no. M0851;
Dako; Agilent Technologies, Inc.), SMARCB/INI1 (cat. no. 612110; BD
Biosciences), p16 (cat. no. 705-4713; Roche Diagnostics), CD34
(cat. no. NCL-L-END; Leica Microsystems GmbH), S-100 (cat. no.
IR504; Dako; Agilent Technologies, Inc.) and Ki-67 (cat. no. M7240;
Dako; Agilent Technologies, Inc.). The reaction of secondary
antibody and following 3,3′-diaminobenzidine reaction were
performed using EnVision+ System HRP Labelled Polymer kit (Dako;
Agilent Technologies, Inc.). Appropriate positive control sections
were mounted on the same slide glasses. Immunohistochemically, the
tumor cells were positive for AE1/AE3 (focally; Fig. 4B) and SMA (Fig. 4C). The expression of SMARCB/INI1 was
reduced compared with that in the normal region (Fig. 4D). The tumor was also positive for
p16 but negative for CD34 and S-100 protein (Fig. 4E). The Ki-67 labeling index was 30%
(Fig. 4F). The SS18-SSX2
fusion gene was confirmed using PCR and sequencing analysis
(Fig. 4G and H). RNA was extracted
from formalin-fixed paraffin-embedded tissue using the RNAstorm kit
(Cell Data Sciences). The reverse transcription was performed using
RverTra Ace (Toyobo Life Science). PCR was performed using a KOD
One (Toyobo Life Science) with SS18p-foward
(5′-CCAGCAGAGGCCTTATGGATA-3′), SS18-foward
(5′-GACCAACACAGCCTGGACCAC-3′), SSXp-reverse
(5′-CGTTTTGTGGGCCAGATGCTTC-3′), SSX1-reverse
(5′-GGTGCAGTTGTTTCCCATCG-3′), SSX2-reverse
(5′-GCACTTCCTCCGAATCATTTC-3′), SSX4-reverse
(5′-GCCTCTGGCACTTCCTTCAAAC-3′), SSX4V-reverse
(5′-CGCTGATCTCTTCATAAACCAC-3′) primers. PCR conditions were initial
denaturation at 95°C for 2 min, 45 cycles of 98°C for 10 sec,
annealing at 64°C for 30 sec, 68°C for 20 sec, and a final
extension 68°C for 5 min. PCR products were electrophoresed on 2.0%
agarose gel and visualized using Midori Green Direct (NE-MG06;
NIPPON Genetics). Sequencing was outsourced to another facility
within the university. Sanger sequencing was performed using 3500×L
Genetic Analyzer (Applied Biosystems; Thermo Fisher Scientific,
Inc.). The tumor was diagnosed as SS, monophasic fibrous SS.
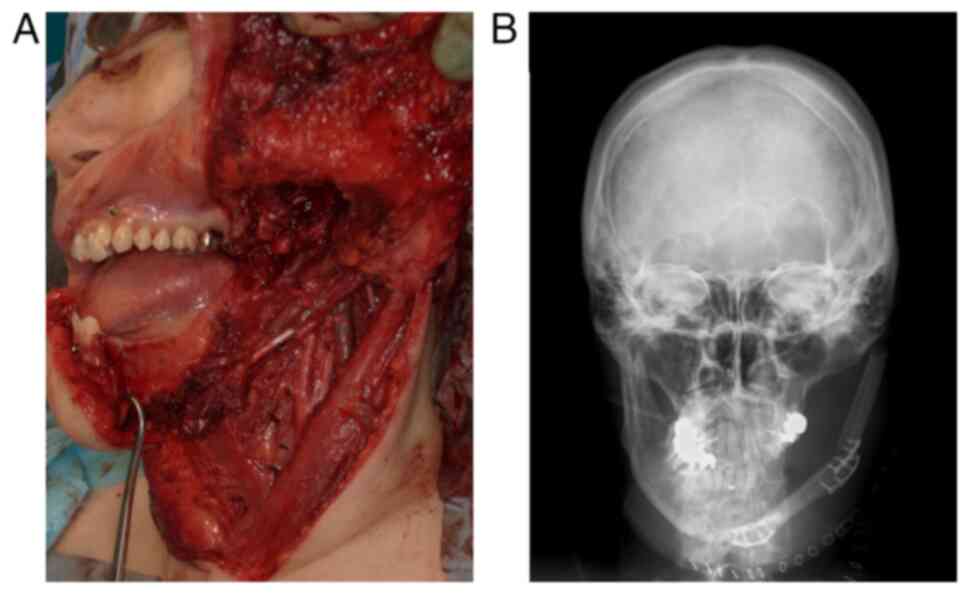
Multidisciplinary treatment was discussed with a
medical oncologist, orthopedist, otorhinolaryngologist, and plastic
surgeon. On imaging findings, the tumor seemed resectable, with a
potential acceptable functional outcome after reconstruction;
therefore, surgical treatment was decided upon. The patient
underwent tracheotomy, left supraomohyoid neck dissection, left
hemimandibulectomy, and immediate reconstruction using a fibular
myocutaneous flap (Fig. 5).
Histopathological examination revealed no cervical lymph node
metastasis. Adjuvant chemotherapy with doxorubicin and ifosfamide
was administered one month after surgery since SS arising in the
head and neck has a high risk of distant metastases. After
demineralization of the resected specimen, histopathological
examination was performed. The SS penetrated the cortical bone and
formed an extraosseous mass that invaded to the inferior alveolar
nerve. Radiotherapy was not performed because the safety margins of
the resected specimen were sufficient. At the 27-month follow-up,
the patient was free of recurrence and metastasis.
Discussion
SS occurring primarily within the mandible is very
rare and only nine cases have been reported (10–18),
the details of which are summarized in Table I. Variants of SS are classified into
the monophasic, biphasic and poorly differentiated types (2,3). The
monophasic type is subdivided into epithelial and fibrous type
(11,14). Monophasic SS comprises spindle cells
that are fairly uniform and relatively small, with sparse cytoplasm
and ovoid, hyperchromatic nuclei with granular chromatin and
inconspicuous nucleoli. Biphasic SS has epithelial and spindle cell
components in varying proportions. The epithelial cells are
arranged in solid nests or cords, or in glands with a tubular or
occasionally alveolar or papillary architecture. The spindle cells
in biphasic SS resemble the spindle sells found in monophasic SS.
In otherwise monophasic or biphasic SS, poorly differentiated areas
with increased cellularity, greater nuclear atypia, and high
mitotic activity may be found (5).
SS is characterized by a specific chromosomal translocation
t(X;18)(p11;q11) (5). This
translocation leads to the formation of a SS18-SSX fusion protein,
which drive sarcomagenesis (2,7,19). The
fusion protein integrates, by means of the SS18 component, into
barrier-to-autointegration factor (BAF; also known as mammalian
SWI/SNF) family complexes, which have crucial roles in chromatin
organization (7). The SS18-SSX
fusion protein, by inducing imbalance in BAF family complexes, can
alter chromatin remodeling and activate aberrant gene transcription
(7). The SSX component mediates
interaction with polycomb chromatin repressor complexes involved in
gene transcription inhibition. By inducing broad transcriptional
dysregulation, the SS18-SSX fusion oncogene represents a
major driver of transformation and malignancy (7). The SS18-SSX fusion gene has
subtypes, including SS18-SSX1, SS18-SSX2 and
SS18-SSX4 (2,5,7). The
subtype of fusion gene correlates with the tumor phenotype; almost
all biphasic SS has been shown to harbor the SS18-SSX1
fusion gene, and almost all of the SS18-SSX2 tumor are
monophasic SS (2,3,7,19).
 | Table I.Summary of clinical features of nine
previously reported cases and present case of SS arising from the
mandible. |
Table I.
Summary of clinical features of nine
previously reported cases and present case of SS arising from the
mandible.
| First author,
year | Age, years | Sex | Site | Symptoms | Subtype | Treatment | Outcome | (Refs.) |
|---|
| Torsiglieri,
1991 | 28 | Male | Body | Swelling | UK | S, C, R | Dead (3 y 8 m) | (10) |
| Koga, 2005 | 42 | Male | Body | Swelling | UK | S | Alive (7 y) | (11) |
| Granowetter,
2006 | 11 | Male | UK | Pain, trismus | UK | C, R, S | Alive | (12) |
| Tilakaratne,
2006 | 29 | Female | Condyle | Swelling | UK | S, R | Alive (2 y) | (13) |
| Wang, 2008 | 32 | Male | Condyle | Swelling,
trismus | B | S | UK | (14) |
| Tao, 2011 | 20 | Female | Body | Swelling | M | S, R | Alive (1 y) | (15) |
| Wadhwan, 2011 | 28 | Male | Body | Swelling, pus
discharge, pain | B | S | Alive (1 y) | (16) |
| Khalili, 2012 | 76 | Male | Body | Swelling, pain,
paresthesia | M | S | Dead (2 m) | (17) |
| Teixeira, 2021 | 22 | Male | Body | Pain, swelling | M | UK | Alive (2 y) | (18) |
| Imajo, 2023 | 54 | Female | Body | Pain,
paresthesia | M | S, C | Alive (27 m) | Present case |
The clinical appearance and symptoms of head and
neck SS vary among the reported cases and are usually determined by
the tumor site (3,4). SS arising from the oral cavity mainly
presents as a slowly enlarging, painless, non-tender, spherical,
and deeply seated mass (4,11,14).
Patients become symptomatic when the size of the SS grows enough to
cause pressure symptoms on adjacent structures (4). In the present patient, the cause of
the pain was thought to be inferior alveolar nerve compression by
the tumor because the pain decreased soon after cortical bone
opening by incisional biopsy. However, the hypoesthesia of the left
chin did not improve. Therefore, the cause of the hypoesthesia was
thought to be invasion of SS into the inferior alveolar nerve.
On CT, SS presents as a uniform and well-defined
lesion (4,8,9). On
MRI, SS displays an image that has been described as a triple
signal pattern, which reflects a combination of calcification,
cystic changes due to necrosis and hemorrhage and air-fluid levels
(2,8,9,20). In
the case of intraosseous SS, lesions appear osteolytic on plain
radiography, low- or iso-intense on T1-WI MRI, of variable
intensity on T2-WI MRI, and heterogeneously enhanced using
diethylenetriaminepentaacetic acid-gadolinium (8). There are no characteristic imaging
findings for SS; therefore, it is difficult to diagnose it using
only imaging modalities. SS originating from the bone forms an
extraosseous mass via the Haversian system, similar to that seen in
the current case (8,9,20). The
formation of an extraosseous mass without bone destruction is a
rare feature of other solid tumors; therefore, it may be a
characteristic finding of intraosseous SS.
Biopsy is essential for proper treatment planning.
Options for biopsy include incisional biopsies, core needle
biopsies (CNB) and fine needle aspirations (FNA). CNB and FNA
guided by imaging are useful for deep-seated tumors, but they tend
to have lower diagnostic accuracy than do open incisional biopsy
because they cannot provide large tissue samples (2). CNB and FNA are also associated with
the risk of dissemination owing to needle tract seeding. Biopsy
should be performed properly according to the location and size of
the tumor. Since the tumor in the present case was under the oral
mucosa and not deep, an open incisional biopsy was performed. The
incision was designed to be included on the resection side and
tissue detachment was minimized to prevent dissemination, and large
tissue samples were taken from both extraosseous and intraosseous
tumor to make a definitive diagnosis. As the extra- and
intraosseous tumors were the same, biopsy of intraosseous tumors
was unnecessary. In cases of SS, it is harder to microscopically
diagnose monophasic types than biphasic types, particularly in
unusual locations because of the resemblance to fibrosarcoma or
other spindle cell tumors (14,17,18).
In the jaws, additional consideration to other odontogenic spindle
cell tumors is required (17).
Therefore, in addition to routine H&E staining,
immunohistochemical staining is also available to facilitate
diagnosis. SMARCB/INI1 expression is downregulated in SS and the
same finding was noted in the present case (21). SMARCB/INI1 is also known as BAF47.
The SS18-SSX fusion proteins competitively replace the wild-type
SS18 in canonical BAF complex, thus resulting in ejection of
SMARCB/INI1 (22). The presence of
the SS18-SSX fusion gene confirms the diagnosis in difficult
cases with unusual histological features or unusual locations
(4,13,15,16,20,23).
Owing to the paucity of SS cases in the oral and
maxillofacial areas, information regarding appropriate therapy is
limited. Surgical resection is the mainstay of therapy for
localized STS, and the adequate margin size depends on several
factors (24). For STS, a margin of
≥1 cm or an intact anatomic barrier is recommended, and the same is
true for SS (24). Radical excision
with negative margins is most important for local control and
overall survival of SS patients (2). However, radical excision with negative
margins is not always possible in the head and neck region because
of the complicated anatomy, and radiation therapy is often
recommended (4). Adjuvant radiation
therapy improves local control of head and neck SS (4). Preoperative radiation is associated
with an increase in wound complication rate, while post-operative
radiation can cause fibrous and joint stiffness, which may lead to
long term dysfunction (2). Unlike
the majority of STS, SS appears to be more chemosensitive (2,7).
However, adjuvant chemotherapy remains controversial since the
results of randomized trials are non-conclusive (2,7). In
general, chemotherapy including anthracyclines and ifosfamide is
administered for high-risk or advanced patients (2,3,7,24).
Treatment options should be decided by a multidisciplinary team
based on the patient's age, performance status, comorbidities,
tumor location, and histological subtype. In the present case,
neoadjuvant radiation therapy was considered ineffective because
the SS was mostly surrounded by thick cortical bone, and the safety
margin was sufficient for histopathological examination; therefore,
adjuvant radiation therapy was not performed. Considering the high
rate of distant metastasis in patients with SS, systemic
chemotherapy with doxorubicin and ifosfamide was administered.
Neoadjuvant chemotherapy effect can be assessed by determining the
changes in tumor size; however, if it is not effective and
progresses to the skull base, the tumor becomes unresectable. So,
chemotherapy was administered post-operatively in the present
case.
The prognosis of SS is affected by tumor size,
location, patient age, extent, histological subtype, mitotic
activity, fusion type, margin of resection and adjuvant
radiotherapy (1–4,12–15,20,23).
The 5-year survival rate of patients with SS originating in the jaw
is 69.1% (1). Late local
recurrences and pulmonary metastasis >5 years after the initial
diagnosis are more typical of SS than other sarcomas (2–4,7,16,20).
Long-term follow-up is necessary because the prognosis is often
poor, and a number of patients develop lung metastasis.
The present study was a report of a rare case of SS
arising in the left mandible. Intraosseous SS penetrated via the
Haversian system and spread outside the bone. There are no
characteristic imaging findings for SS, but the formation of an
extraosseous mass without bone destruction may be a characteristic
finding of intraosseous SS.
Acknowledgements
Not applicable.
Funding
The present study was supported by JSPS KAKENHI (grant no.
JP19K19164).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
II was responsible for collecting clinical, imaging
and pathological data of the patient and responsible for the
conception, design, content and writing of the manuscript. TY, TC,
TK, and ES contributed to the conception and revisions of the
manuscript. TC and TY made analysis and interpretation of imaging
data. TK, KK, YO made analysis and interpretation of
histopathological data. ES made analysis and interpretation of
neurological data. MI made analysis and interpretation of data
related to chemotherapy. II and TY confirmed the authenticity of
the raw data. All authors agreed on the journal to which the
article has been submitted and agreed to be accountable for all
aspects of the work. All authors have read and approved the final
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient for publication of this case report and the accompanying
images.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
SS
|
synovial sarcoma
|
|
STS
|
soft tissue sarcoma
|
|
CT
|
computed tomography
|
|
MRI
|
magnetic resonance imaging
|
|
T1-WI
|
T1-weighted images
|
|
T2-WI
|
T2-weighted images
|
|
H&E
|
hematoxylin and eosin
|
|
SMA
|
smooth muscle actin
|
|
CNB
|
core needle biopsy
|
|
FNA
|
fine needle aspiration
|
|
SMARCB/INI1
|
SWI/SNF related matrix associated
actin dependent regulator of chromatin subfamily b/Integrase
interactor 1
|
References
|
1
|
Liu Z, Jin S, Fu S, Hu Y and He Y:
Management of the primary intraosseous synovial sarcoma of the
jaws: Be careful of the surgical margin. J Oral Maxillofac Surg.
73:550–563. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Gazendam AM, Popovic S, Munir S, Parasu N,
Wilson D and Ghert M: Synovial sarcoma: A clinical review. Curr
Oncol. 28:1909–1920. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Fiore M, Sambri A, Spinnato P, Zucchini R,
Giannini C, Caldari E, Pirini MG and De Paolis M: The biology of
synovial sarcoma: State-of-the-art and future perspectives. Curr
Treat Options Oncol. 22:1092021. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Doubi A, Doubi M, Alzaher N and Tulbah A:
Synovial sarcoma of the hard palate: The third case in the medical
literature. Hematol Oncol Stem Cell Ther. 12:60–63. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
WHO Classification of Tumours Editorial
Board, . WHO classification of tumours of soft tissue and bone. 5th
edition. IARC Press; Lyon, France: pp. 290–293. 2020
|
|
6
|
Knox LC: Synovial sarcoma. Am J Cancer
Res. 28:461–480. 1936.
|
|
7
|
Landuzzi L, Ruzzi F, Lollini PL and
Scotlandi K: Synovial sarcoma preclinical modeling: Integrating
transgenic mouse models and patient-derived models for
translational research. Cancers (Basel). 15:5882023. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Fujibuchi T, Miyawaki J, Kidani T, Imai H,
Kiyomatsu H, Kitazawa R and Miura H: Intraosseous synovial sarcoma
of the distal ulna: A case report and review of the literature. BMC
Cancer. 19:1162019. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Caracciolo JT, Henderson-Jackson E and
Binitie O: Synovial sarcoma of bone: Sarcoma typically of soft
tissues presenting as a primary bone tumor. Radiol Case Rep.
14:204–207. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Torsiglieri AJ Jr, Hendrix RA and Quinn
PS: Synovial sarcoma of the jaw. Ear Nose Throat J. 70:396–398.
1991.PubMed/NCBI
|
|
11
|
Koga C, Harada H, Kusukawa J and Kameyama
T: Synovial sarcoma arising in the mandibular bone. Oral Oncol
Extra. 41:45–48. 2005. View Article : Google Scholar
|
|
12
|
Granowetter L, Ladas E, Taromina K, Rooney
D and Kelly KM; Integrative Tumor Board, : Integrative tumor board:
Pediatric synovial sarcoma. Integr Cancer Ther. 5:48–55. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Tilakaratne WM: Synovial sarcoma of the
mandible. J Oral Pathol Med. 35:61–63. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wang H, Zhang J, He X and Niu Y: Synovial
sarcoma in the oral and maxillofacial region: Report of 4 cases and
review of the literature. J Oral Maxillofac Surg. 66:161–167. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Tao Q, Qiao B, Wang Y and Hu F: Diagnosis
and treatment of primary synovial cell sarcoma that occurred in the
left mandible body: A case report and literature review. Oral Surg
Oral Med Oral Pathol Oral Radiol Endod. 111:e12–e20. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Wadhwan V, Malik S, Bhola N and Chaudhary
M: Biphasic synovial sarcoma in mandibular region. J Oral
Maxillofac Pathol. 15:239–243. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Khalili M, Eshghyar N, Ensani F and Shakib
PA: Synovial sarcoma of the mandible. J Res Med Sci. 17:1082–1085.
2012.PubMed/NCBI
|
|
18
|
Teixeira LN, da Cruz EZ, Rosa ACG,
Rodrigues AA, Passador-Santos F, de Araújo VC and Soares AB:
Primary intraosseous synovial sarcoma in the mandible. Case Rep
Oncol Med. 2021:99455912021.PubMed/NCBI
|
|
19
|
Saito T: The SYT-SSX fusion protein and
histological epithelial differentiation in synovial sarcoma:
Relationship with extracellular matrix remodeling. Int J Clin Exp
Pathol. 6:2272–2279. 2013.PubMed/NCBI
|
|
20
|
Beck SE, Nielsen GP, Raskin KA and Schwab
JH: Intraosseous synovial sarcoma of the proximal tibia. Int J Surg
Oncol. 2011:1848912011.PubMed/NCBI
|
|
21
|
Kohashi K, Oda Y, Yamamoto H, Tamiya S,
Matono H, Iwamoto Y, Taguchi T and Tsuneyoshi M: Reduced expression
of SMARCB1/INI1 protein in synovial sarcoma. Mod Pathol.
23:981–990. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kadoch C and Crabtree GR: Reversible
disruption of mSWI/SNF (BAF) complexes by the SS18-SSX oncogenic
fusion in synovial sarcoma. Cell. 153:71–85. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Salcedo-Hernández RA, Lino-Silva LS and
Luna-Ortiz K: Synovial sarcomas of the head and neck: Comparative
analysis with synovial sarcoma of the extremities. Auris Nasus
Larynx. 40:476–480. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
López-Pousa A, Martin Broto J, Martinez
Trufero J, Sevilla I, Valverde C, Alvarez R, Carrasco Alvarez JA,
Cruz Jurado J, Hindi N and Garcia Del Muro X: SEOM clinical
guideline of management of soft-tissue sarcoma (2016). Clin Transl
Oncol. 18:1213–1220. 2016. View Article : Google Scholar : PubMed/NCBI
|