Introduction
Cervical cancer is the fourth most common type of
cancer in women globally accounting for 604,127 new cases and
341,831 new deaths in 2020 (1).
Surgical treatment with radical hysterectomy and pelvic lymph node
dissection is one of the options for the primary treatment of stage
IB-IIB [2008 Federation of Gynecology and Obstetrics (FIGO) staging
system] cervical cancer according to the National Comprehensive
Cancer Network guidelines (2) and
the Japan Society of Gynecologic Oncology guidelines (3). After surgical treatment, adjuvant
therapy such as whole-pelvic irradiation or chemoradiation is
recommended depending on risk factors for recurrence, which is
evaluated using pathological factors of specimens from resected
tissues (2,3). However, the combination of radical
hysterectomy and whole-pelvic irradiation or chemoradiation is
linked with an increased occurrence of complications such as
lower-limb lymphedema, urinary disturbance, bowel obstruction,
sexual dysfunction, and mental issues related to those lasting
issues (4–6). Chemotherapy has been reported as an
effective post-surgical adjuvant therapy for patients with
intermediate- and high-risk stage IB-IIB cervical cancer (7–9). For
these reasons, chemotherapy has been increasingly chosen as
post-surgical adjuvant therapy in clinical practice (10,11).
As adjuvant chemotherapy is not a standard treatment yet, if the
recurrence after adjuvant chemotherapy can be predicted, (that is
patients who will not benefit from adjuvant chemotherapy), it would
assist gynecological oncologists in deciding which adjuvant therapy
(chemotherapy or radiation therapy) would be suitable.
Cleft lip and palate transmembrane protein 1-like
protein [CLPTM1L, also known as cisplatin resistance-related
protein 9 (CRR9)] has been identified as an overexpressed protein
in human ovarian tumor cells resistant to cisplatin (12). CLPTM1L is a protein that is highly
expressed in several types of tumor cells, including lung cancer,
pancreatic cancer, prostate cancer, bladder cancer, glioma,
melanoma, basal cell carcinoma, and cervical cancer (13–22).
The expression of CLPTM1L is associated with the apoptosis
mechanism and related to the growth of the tumor cells and
resistance against chemotherapy (12,23).
In the present study, the relationship between
CLPTM1L expression in patients with intermediate- and high-risk
stage IB-IIB cervical cancer undergoing radical hysterectomy
followed by treatment with cisplatin and paclitaxel (TP) as
adjuvant chemotherapy and recurrence were determined. Additionally,
the effect of knockdown of CLPTM1L on the sensitivity to
chemotherapy agents using a cervical cancer cell line. The results
showed that the expression of CLPTM1L in patients with
intermediate- and high-risk stage IB-IIB cervical cancer undergoing
radical hysterectomy followed by TP was associated with recurrence
in those patients and suppression of expression of CLPTM1L on
cervical cancer cell line can enhance the sensitivity to
cisplatin.
Materials and methods
Patients
The present study was a retrospective study in which
a total of 91 patients were enrolled. The inclusion criteria were
as follows: i) Patients diagnosed with FIGO 2008 stage IB-IIB
cervical cancer; ii) patients who received radical hysterectomy at
Osaka City University Hospital (Osaka, Japan) between January 1st,
2014 and December 31st, 2019; iii) patients who underwent TP
chemotherapy [paclitaxel (135 mg/m2) plus cisplatin (50
mg/m2) every 3 weeks for 3–6 cycles) after surgery as
adjuvant chemotherapy; and iv) the medical records were available
to analyze. Information on the clinical factors such as FIGO stage,
age, histology, pathological findings of the specimens from
resected organs, laboratory data of blood samples, date of
recurrence, and date of death was collected. Overall survival was
defined as the duration between the date of primary surgery and
death from any cause. Data of patients who were still alive were
censored at the date when the patient's survival was last
confirmed.
To investigate the relationship between CLPTM1L
expression and cancer recurrence, the patients were divided into
two groups; one in which cancer recurred within 2 years after
primary surgery, and the other in which cancer did not recur within
2 years. Recurrence was evaluated by radiological assessments using
computed tomography (CT) or Magnetic resonance imaging (MRI) after
every three cycles of adjuvant chemotherapy, whilst a physical
examination was performed after every cycle. After completion of
adjuvant chemotherapy, a physical examination was conducted every 3
months and radiological assessments were conducted every year since
the primary surgery was performed for 2 years. Radiological
assessments were also conducted when physical examination detected
any abnormal findings.
This study was performed at Osaka City University
and Osaka Metropolitan University. All the patients enrolled in
this study provided written informed consent for the treatment and
the use of their samples in future research including the present
study. The Institutional Review Board of Osaka City University
Hospital approved this study (approval no. 2021-150).
Immunohistochemical staining and
scoring
For immunohistochemistry, 4 µm sections from
paraffin-embedded tissue blocks of cervical cancer which were
dissected during the surgery were obtained. Following routine
deparaffinization and dehydration, antigen retrieval was performed
by immersing in Target Retrieval Solution, pH 9.0 (cat. no. S2367;
Agilent Technologies, Inc.) and heating in an autoclave at 121°C
for 20 min. For the primary antibody, a rabbit monoclonal
anti-CLPTM1L antibody (cat. no. HPA014791; MilliporeSigma; 1:400
dilution) was used and slides were incubated at 4°C overnight. For
the secondary antibody, a biotinylated goat immunoglobulin G
antibody (cat. no. K0675; Agilent Technologies, Inc.) was used, and
samples were incubated at room temperature for 10 min. To stabilize
staining, the slides were immersed in DAB solution at room
temperature for 10 min. Finally, the tissue sections were
counterstained with hematoxylin at room temperature for 1 min.
CLPTM1L expression was quantified by weighted
scoring, as described previously (24). This score is calculated by
multiplying the score of the percentage of stained tumor cells by
the score of staining intensity of each slide. The percentage
stained was scored as follows: 0, <5%; 1, 5–25%; 2, 25–50%; 3,
50–75%; and 4, >75%. The intensity was scored as follows: 1,
weak; 2, moderate; and 3, intense.
Cell culture
CaSki cells (cat. no. IFO50007; Japanese Collection
of Research Biosources Cell Bank) were cultured in RPMI medium
(Gibco; Thermo Fisher Scientific, Inc.) supplemented with 10% FBS
and 1% penicillin. Cells were incubated in a humidified incubator
at 37°C supplied with 5% CO2.
CLPTM1L knockdown and cell survival
assays
For CLPTM1L siRNA transfections,
Lipofectamine® RNAiMAX (Invitrogen; Thermo Fisher
Science, Inc.) was used. CLPTM1L-specific siRNA (CLPTM1L siRNA;
cat. no. 4392420; Invitrogen; Thermo Fisher Scientific, Inc.) or
control siRNA (control siRNA-A; cat. no. 4390843; Invitrogen;
Thermo Fisher Scientific, Inc.) were used. The sequence of the
CLPTM1L siRNA was 5′-GAAUUUUUGUAGAUACCA Att; the sequence of the
control siRNA was confidential according to the company's policy.
CaSki cells were seeded at a density of 2×103 cells/well
in 96-well tissue culture plates. Cells were incubated with medium
containing CLPTM1L siRNA or control siRNA at 37°C for 24 h, after
which they were incubated with media containing 1.5, 3.1, 6.2, or
12.5 µM cisplatin at 37°C for 48 h. Next, 10 µl Cell Counting Kit-8
solution (Dojindo Molecular Technologies, Inc.) was added per well,
and cells were further incubated at 37°C for 2 h, and subsequently,
the absorbance at 450 nm was measured using a microplate reader
(Corona Electric, Co., Ltd.).
Reverse transcription-quantitative PCR
(RT-qPCR)
After CLPTM1L siRNA transfection, RT-qPCR was used
to confirm the knock down of CLPTM1L mRNA expression. TaqMan primer
and probes for CLPTM1L (cat. no. Hs00363947_m1) and hypoxanthine
phosphoribosyl-transferase 1 (cat. no. Hs02800695_ml; both from
Thermo Fisher Scientific, Inc.) were used according to the
manufacturer's protocol. Total RNA from CaSki cells was obtained
using a RNeasy Mini Kit (Qiagen GmbH). Then total RNA (1 µg) was
reverse transcribed into cDNA using a High-Capacity cDNA Reverse
Transcription Kit according to the manufacturer's protocol (Thermo
Fisher Scientific, Inc.). Finally, qPCR was performed using TaqMan
Fast Universal PCR MasterMix (Thermo Fisher Scientific, Inc.). The
following thermocycling conditions were used: Initial denaturation
at 95°C for 20 sec; followed by 40 cycles of 95°C for 3 sec and
60°C for 30 sec. To calculate the relative changes in gene
expression, the 2−ΔΔCq method was used (25).
Statistical analysis
GraphPad Prism version 9 (GraphPad Software, Inc.)
was used to analyze the data. Data are presented as the median and
the range. Significant differences between two groups were
determined using a Fisher's exact test and a Mann-Whitney U-test. A
receiver operating characteristic (ROC) curve was used to determine
the cut-off value of Weighted scores of CLPTM1L expression. For
prognostic analysis, the Kaplan-Meier method and log-rank tests
were used. For risk factors for recurrence, which were detected in
univariate analysis with Fisher's exact test, multivariate analysis
was performed to detect independent risk factors using logistic
regression analysis. P<0.05 was considered to indicate a
statistically significant difference. Five replicates were
performed for RT-qPCR, and ten replicates were performed for the
cell survival assays.
Results
Patient characteristics
There were 76 patients included in the no-recurrence
group and 15 patients in the recurrence group. Regarding age and
FIGO stage, there were no significant differences between the two
groups. In the recurrence group, the proportion of cases of
non-squamous cell carcinoma (non-SCC), positive lymph node
metastasis, and positive parametrium invasion were significantly
higher (P=0.013, P=0.023, and P=0.011, respectively; Table I). This suggests that non-SCC,
positive lymph node metastasis, and positive parametrium invasion
were risk factors for recurrence in the univariate analysis.
Non-SCC histology includes five usual type endocervical
adenocarcinomas and two large cell neuroendocrine carcinomas in the
non-recurrence group and eight usual type endocervical
adenocarcinomas, two endometrioid carcinomas, one clear cell
carcinoma and one adenosquamous carcinoma in the recurrence
group.
 | Table I.Patient characteristics. |
Table I.
Patient characteristics.
|
Characteristics | Non-recurrence
group | Recurrence
group | P-value |
|---|
| No. of
patients | 76 | 15 |
|
| Median age, years
(range) | 55 (27–78) | 55 (39–76) | 0.974a |
| FIGO stage, n |
|
| 0.163b |
| I | 46 | 6 |
|
| II | 30 | 9 |
|
| Histology, n |
|
| 0.013b,c |
|
SCC | 64 | 8 |
|
|
Non-SCC | 12 | 7 |
|
| Lymph node
metastasis, n |
|
| 0.023b,c |
|
Negative | 46 | 4 |
|
|
Positive | 30 | 11 |
|
| Parametrium
invasion, n |
|
| 0.011b,c |
|
Negative | 58 | 6 |
|
|
Positive | 18 | 9 |
|
CLPTM1L weighted score and cutoff
value to predict recurrence
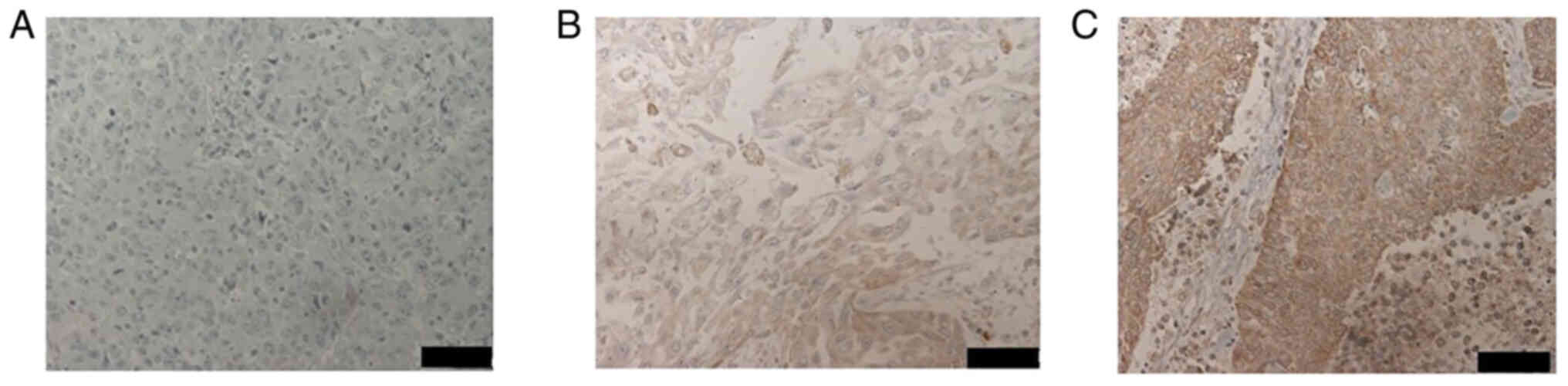
The expression of CLPTM1L was compared between the
two groups using immunohistochemical staining. CLPTM1L protein
expression was observed in the cytoplasm of cervical cancer cells
macroscopically which was identical to previous reports describing
the localization of CLPTM1L in the mitochondria, endoplasmic
reticulum and the plasma membrane (26–28).
The representative images of weighted scores 0, 6, and 12 are shown
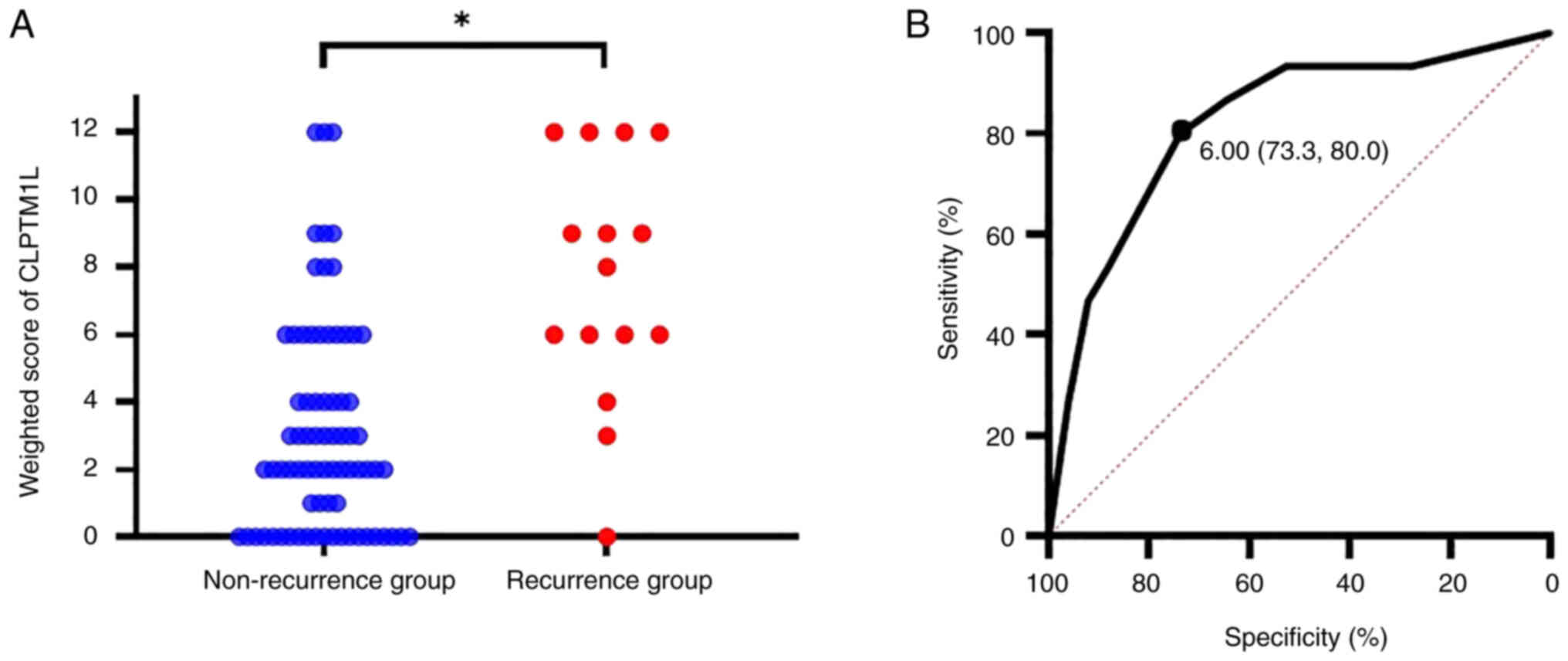
in Fig. 1. The expression of
CLPTM1L which was evaluated using a weighted score was
significantly higher in the recurrence group (P<0.05, Fig. 2A). To identify the optimal cut-off
weighted score value of CLPTM1L to predict recurrence, ROC curves
were drawn. They showed that a cut-off weighted score value of 6
predicted recurrence with a sensitivity of 73.3% and specificity of
80.0%, with an area under the curve of 0.82 and a 95% confidence
interval of 0.698–0.942 (Fig.
2B).
CLPTM1L expression for predicting
recurrence and overall survival
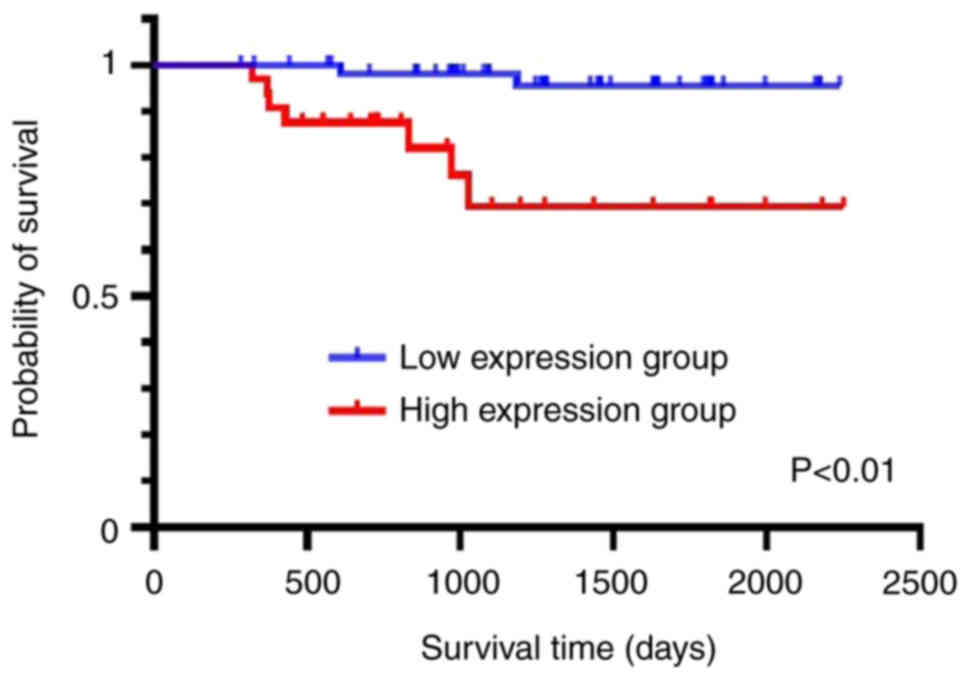
Based on the cut-off weighted score value of 6,
patients were divided into two groups: low expression group (score
≤4; 59 patients) and high expression group (score ≥6; 32 patients).
Regarding age, FIGO stage (2008), histology, lymph node metastasis,
and parametrium invasion, there were no significant differences
between the two groups (Table II).
In the low-expression group, 56 patients (94.9%) did not exhibit
recurrence and only 3 patients (5.1%) exhibited a recurrence. In
the high expression group, 20 patients (62.5%) did not exhibit a
recurrence and 12 patients (37.5%) exhibited recurrence, showing
that patients in the high expression group were more likely to
exhibit a recurrence than in the low expression group (P<0.010;
Table III). Regarding overall
survival, patients in the low expression group had a better
prognosis (P<0.01; Fig. 3),
suggesting that CLPTM1L expression could be used to predict overall
survival.
| Table II.Characteristics of the patients
stratified by cleft lip and palate transmembrane protein 1-like
protein expression. |
Table II.
Characteristics of the patients
stratified by cleft lip and palate transmembrane protein 1-like
protein expression.
|
Characteristics | Low expression
group | High expression
group | P-value |
|---|
| No. of
patients | 59 | 32 |
|
| Median age, years
(range) | 54 (29–76) | 56 (27–78) | 0.930a |
| FIGO stage, n |
|
| 0.659b |
| I | 35 | 17 |
|
| II | 24 | 15 |
|
| Histology, n |
|
| 0.281b |
|
SCC | 49 | 23 |
|
|
Non-SCC | 10 | 9 |
|
| Lymph node
metastasis, n |
|
| 0.051b |
|
Positive | 37 | 13 |
|
|
Negative | 22 | 19 |
|
| Parametrium
invasion, n |
|
| 0.100b |
|
Positive | 45 | 19 |
|
|
Negative | 14 | 13 |
|
| Table III.Association between CLPTM1L
expression and recurrence. |
Table III.
Association between CLPTM1L
expression and recurrence.
| CLPTM1L
expression | No recurrence, n
(%) | Recurrence, n
(%) | P-value |
|---|
| Low expression,
score ≤4 | 56 (94.9) | 3 (5.1) |
<0.010a,b |
| High expression,
score ≥6 | 20 (62.5) | 12 (37.5) |
|
Multivariate analysis for detecting
independent risk factors of recurrence
To identify independent risk factors for recurrence,
multivariate analysis using logistic regression was performed.
Multivariate analysis revealed high CLPTM1L expression and
histology of non-SCC were significantly associated with recurrence
(P<0.010 and 0.042, respectively; Table IV). The odds ratio for recurrence
of high CLPTM1L and histology of non-SCC were 7.990 and 4.660,
respectively. This suggests that high CLPTM1L expression and
histology of non-SCC are independent risk factors for recurrence of
intermediate- and high-risk stage IB-IIB cervical cancer undergoing
radical hysterectomy followed by TP as adjuvant chemotherapy.
| Table IV.Multivariate analysis to detect
independent risk factors for recurrence. |
Table IV.
Multivariate analysis to detect
independent risk factors for recurrence.
|
|
| 95% confidence
interval |
|
|---|
|
|
|
|
|
|---|
| Variables | Odds ratio | Lower | Upper | P-value |
|---|
| CLPTM1L expression
(high vs. low) | 7.990 | 1.850 | 34.400 |
<0.010a |
| Lymph node
metastasis (positive vs. negative) | 2.940 | 0.679 | 12.700 | 0.149 |
| Histology (SCC vs.
non-SCC) | 4.660 | 1.060 | 20.500 | 0.042b |
| Parametrium
invasion (positive vs. negative) | 3.100 | 0.791 | 12.100 | 0.105 |
Contribution of CLPTM1L knockdown to
the sensitivity of cervical cancer cells to cisplatin
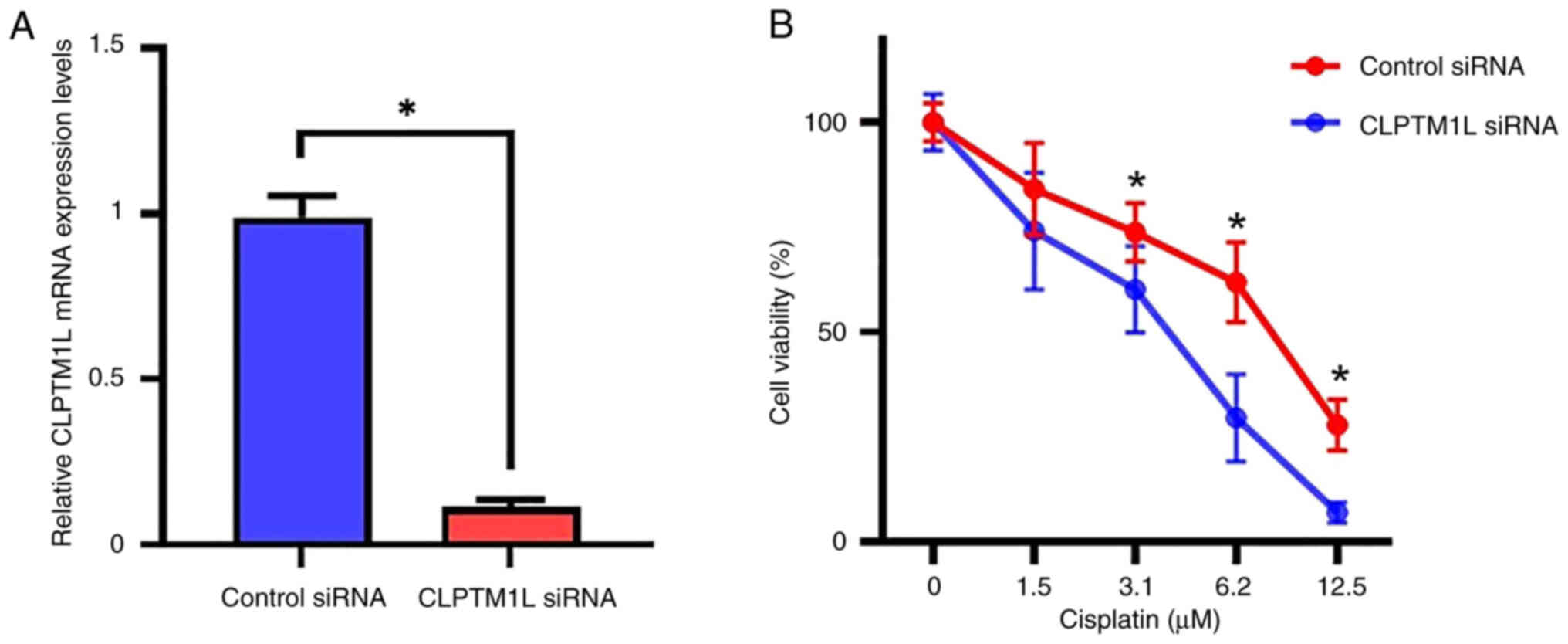
To determine the effect of CLPTM1L knockdown on the
sensitivity to chemotherapy, human cervical cells were used in
vitro. CLPTM1L expression was knocked down by transfection of
si-CLPTM1L. Knockdown of CLPTM1L mRNA was confirmed by RT-qPCR.
CLPTM1L mRNA expression was significantly suppressed compared with
cells transfected with the control siRNA (P<0.05; Fig. 4A). After confirmation of successful
knockdown of CLPTM1L with siRNA, the viability of cervical cancer
cells with CLPTM1L expression knocked down was compared with the
control transfected cells. In cells treated with ≥3.1 µM cisplatin,
the viability of tumor cells in which CLPTM1L was knocked down was
significantly lower than the respective control cells (P<0.05;
Fig. 4B). These results indicate
that knockdown of CLPTM1L enhances sensitivity to cisplatin.
Discussion
Even though radiation therapy, including
whole-pelvic irradiation, or chemoradiation is recommended as
adjuvant therapy for patients with intermediate- and high-risk
stage IB-IIB cervical cancer undergoing radical hysterectomy,
chemotherapy has been increasingly chosen as adjuvant therapy
(10). This is due to the adverse
events associated with radiation therapy following radical surgery
such as lower-limb lymphedema, urinary disturbance, bowel
obstruction, sexual dysfunction, and mental health issues caused by
the lasting issues of other adverse events, and these are
frequently more severe than the extent of adverse events associated
with chemotherapy (10).
Additionally, the efficacy of adjuvant chemotherapy has been
increasingly reported (6,10,29).
Additionally, one of the advantages of using chemotherapy as
adjuvant therapy is that if radiation therapy is not performed as
adjuvant therapy during the primary treatment, it can be used if
loco-regional recurrence occurs (4,10,30).
However, adjuvant chemotherapy following radical hysterectomy is
not a standard treatment yet; if the probability of recurrence
following adjuvant chemotherapy could be predicted, this may assist
gynecological oncologists in deciding which adjuvant therapy
(chemotherapy or radiation therapy) to use.
CLPTM1L was first identified in cisplatin resistance
ovarian tumor cells, and recent reports noted that genome-wide
association studies revealed a correlation between CLPTM1L
expression and lung cancer, pancreatic cancer, prostate cancer,
bladder cancer, glioma, melanoma, basal cell carcinoma, and
cervical cancer (13–22). Understanding the function of CLPTM1L
in healthy organs or tissues requires further study; however,
CLPTM1L has been reported to play a crucial role in fetal
development and neonatal survival but is not essential in adult
animals (27). The function of
CLPTM1L in cancer is well understood, where it exerts an
anti-apoptotic effect (21,23,31–33).
CLPTM1L has been reported to play a crucial role in the activation
of the PI3K/AKT pathway by Akt phosphorylation, which regulates
proliferative and survival signals in cancer cells including
apoptotic signals, and also upregulates the expression of Bcl-xL
(21,32), an anti-apoptotic Bcl-2 family member
(21,34). Therefore, over-expression of CLPTM1L
demonstrate tumor-specific cytoprotective and chemoresistive
function by suppressing apoptosis, which is induced by genotoxic
agents in cancers (21,31–33).
Knockdown of CLPTM1L using siRNA has been reported to decrease Akt
phosphorylation and reduce Bcl-xL expression leading to increased
chemosensitivity to cisplatin in the cancer cells (31–33).
In the present study, high expression of CLPTM1L was
associated with recurrence and a poor prognosis of cervical cancer.
There were other factors other than the levels of expression of
CLPTM1L, which contribute to recurrence in the univariate analysis
in the current study including non-SCC histology, lymph node
metastasis, and parametrium invasion. In multivariate analysis, the
levels of expression of CLPTM1L were still an independent risk
factor for the recurrence along with non-SCC histology. Non-SCC
histology has been reported to be one of risk factors for poor
prognosis of patients with cervical cancer (35). The results of this study are
comparable to the report. In this research, three cases experienced
cancer recurrence despite low expression of CLPTM1L. Two cases of
them had non-SCC histology of mucinous carcinoma and the other one
case had parametrium invasion, which may contribute to the
recurrence. Following knockdown of CLPTM1L, the viability of
cervical cancer cells treated with cisplatin for 48 h was
significantly decreased compared to the control group, which
indicated that knockdown of CLPTM1L enhanced the sensitivity of
cervical cancer cells to cisplatin. It indicates that CLPTM1L might
be one of useful biomarkers to predict the recurrence and also one
of candidates of therapeutic target which can enhance the efficacy
of chemotherapy in patients with intermediate- and high-risk stage
IB-IIB cervical cancer undergoing radical hysterectomy followed by
TP as adjuvant chemotherapy.
The present study has some limitations. First, this
was a retrospective study with a relatively small number of cases
from a single institute. Additionally, the expression levels of
CLPTM1L did not predict recurrence with 100% accuracy, highlighting
the likely involvement of several other factors in recurrence.
Thus, larger prospective studies including patients from several
institutions are required to confirm the results of this study.
Additionally, studies that explore other factors that may be
combined with CLPTM1L expression levels are required to enhance the
sensitivity and specificity of predicting recurrence.
To the best of our knowledge, this study is the
first study to show the association between CLPTM1L expression and
the recurrence of patients with cervical cancer who underwent TP as
adjuvant chemotherapy. CLPTM1L may serve as a valuable clinical
biomarker for predicting the recurrence of cervical cancer treated
by radical hysterectomy followed by TP. Adjuvant chemotherapy is
increasing in popularity due to the increase in the body of
literature highlighting its clinical efficacy as adjuvant
chemotherapy; however, there remain cases that are not sensitive to
this regimen. Thus, it is of significant importance to explore
reliable indicators that gynecological oncologists can use to
assess the sensitivity to adjuvant chemotherapy. The present study
may contribute to achieving the goal of identifying the optimal
candidate for adjuvant chemotherapy in patients with cervical
cancer.
In conclusion, this study revealed that CLPTM1L
expression may be a predictive biomarker of recurrence in patients
with intermediate- and high-risk stage IB-IIB cervical cancer
undergoing radical hysterectomy followed by TP as adjuvant
chemotherapy.
Acknowledgements
The authors would like to thank Dr Yukimi Kira
(Research Support Platform of Osaka Metropolitan University
Graduate School of Medicine, Osaka, Japan) for their technical
support.
Funding
The present study was funded by a grant from JSPS KAKENHI (grant
no. 19K09808).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
YA, TF and TS designed the study. YA, TN, EU, SN, KI
and MY performed the experiments and collected the data. YA, TF, TY
and TS analyzed the data. YA and TF wrote the manuscript. YA and TF
confirm the authenticity of all the raw data. All authors have read
and approved the final manuscript.
Ethics approval and consent to
participate
The present study protocol was approved by the
Institutional Review Board of Osaka City University Hospital
(approval no. 2021-150; Osaka, Japan). Written informed consent for
participation in the current study was obtained from all
patients.
Patient consent for publication
Written informed consent for publication was
obtained from all patients.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Sung H, Ferlay J, Siegel RL, Laversanne M,
Soerjomataram I, Jemal A and Bray F: Global Cancer Statistics 2020:
GLOBOCAN estimates of incidence and mortality worldwide for 36
cancers in 185 countries. CA Cancer J Clin. 71:209–249. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Abu-Rustum NR, Yashar CM, Bean S, Bradley
K, Campos SM, Chon HS, Chu C, Cohn D, Crispens MA, Damast S, et al:
NCCN guidelines insights: Cervical cancer, version 1.2020. J Natl
Compr Canc Netw. 18:660–666. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ebina Y, Mikami M, Nagase S, Tabata T,
Kaneuchi M, Tashiro H, Mandai M, Enomoto T, Kobayashi Y, Katabuchi
H, et al: Japan Society of Gynecologic Oncology guidelines 2017 for
the treatment of uterine cervical cancer. Int J Clin Oncol.
24:1–19. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Matoda M, Takeshima N, Michimae H, Iwata
T, Yokota H, Torii Y, Yamamoto Y, Takehara K, Nishio S, Takano H,
et al: Postoperative chemotherapy for node-positive cervical
cancer: Results of a multicenter phase II trial (JGOG1067). Gynecol
Oncol. 149:513–519. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Li S, Hu T, Chen Y, Zhou H, Li X, Cheng X,
Yang R, Wang S, Xie X and Ma D: Adjuvant chemotherapy, a valuable
alternative option in selected patients with cervical cancer. PLoS
One. 8:e738372013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hosaka M, Watari H, Takeda M, Moriwaki M,
Hara Y, Todo Y, Ebina Y and Sakuragi N: Treatment of cervical
cancer with adjuvant chemotherapy versus adjuvant radiotherapy
after radical hysterectomy and systematic lymphadenectomy. J Obstet
Gynaecol Res. 34:552–556. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zhang H, Yu R, Zhang L, Wang R and Xiao L:
Chemotherapy versus chemoradiotherapy for FIGO stages IB1 and IIA1
cervical squamous cancer patients with lymphovascular space
invasion: A retrospective study. BMC Cancer. 22:2022022. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Weng D, Xiong H, Zhu C, Wan X, Chen Y,
Wang X, Zhang Y, Jiang J, Zhang X, Gao Q, et al: Adjuvant
chemotherapy versus adjuvant concurrent chemoradiotherapy after
radical surgery for early-stage cervical cancer: A randomized,
non-inferiority, multicenter trial. Front Med. 17:93–104. 2023.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Zhang YF, Fan Y, Zhang P, Ruan JY, Mu Y
and Li JK: Cervical cancer recurrence and patient survival after
radical hysterectomy followed by either adjuvant chemotherapy or
adjuvant radiotherapy with optional concurrent chemotherapy: A
systematic review and meta-analysis. Front Oncol. 12:8230642022.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ikeda M, Shida M, Shigeta S, Nagase S,
Takahashi F, Yamagami W, Katabuchi H, Yaegashi N, Aoki D and Mikami
M: The trend and outcome of postsurgical therapy for high-risk
early-stage cervical cancer with lymph node metastasis in Japan: A
report from the Japan Society of Gynecologic Oncology (JSGO)
guidelines evaluation committee. J Gynecol Oncol. 32:e442021.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Matsuo K, Nusbaum DJ, Matsuzaki S, Klar M,
Shimada M, Takekuma M and Roman LD: Utilization and outcomes of
adjuvant systemic chemotherapy alone in high risk, early stage
cervical cancer in the United States. Int J Gynecol Cancer.
31:991–1000. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yamamoto K, Okamoto A, Isonishi S, Ochiai
K and Ohtake Y: A novel gene, CRR9, which was up-regulated in
CDDP-resistant ovarian tumor cell line, was associated with
apoptosis. Biochem Biophys Res Commun. 280:1148–1154. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Chen XF, Cai S, Chen QG, Ni ZH, Tang JH,
Xu DW and Wang XB: Multiple variants of TERT and CLPTM1L constitute
risk factors for lung adenocarcinoma. Genet Mol Res. 11:370–378.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Pande M, Spitz MR, Wu X, Gorlov IP, Chen
WV and Amos CI: Novel genetic variants in the chromosome 5p15.33
region associate with lung cancer risk. Carcinogenesis.
32:1493–1499. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wang S, Wu J, Hu L, Ding C, Kan Y, Shen Y,
Chen X, Shen H, Guo X and Hu Z: Common genetic variants in TERT
contribute to risk of cervical cancer in a Chinese population. Mol
Carcinog. 51 (Suppl 1):E118–E122. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Petersen GM, Amundadottir L, Fuchs CS,
Kraft P, Stolzenberg-Solomon RZ, Jacobs KB, Arslan AA,
Bueno-de-Mesquita HB, Gallinger S, Gross M, et al: A genome-wide
association study identifies pancreatic cancer susceptibility loci
on chromosomes 13q22.1, 1q32.1 and 5p15.33. Nat Genet. 42:224–228.
2010. View
Article : Google Scholar : PubMed/NCBI
|
|
17
|
Rothman N, Garcia-Closas M, Chatterjee N,
Malats N, Wu X, Figueroa JD, Real FX, Van Den Berg D, Matullo G,
Baris D, et al: A multi-stage genome-wide association study of
bladder cancer identifies multiple susceptibility loci. Nat Genet.
42:978–984. 2010. View
Article : Google Scholar : PubMed/NCBI
|
|
18
|
Zhao Y, Chen G, Zhao Y, Song X, Chen H,
Mao Y and Lu D: Fine-mapping of a region of chromosome 5p15.33
(TERT-CLPTM1L) suggests a novel locus in TERT and a CLPTM1L
haplotype are associated with glioma susceptibility in a Chinese
population. Int J Cancer. 131:1569–1576. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Mandour I, Hussein SAM, Essam R and
El-Hossainy MA: Study of genetic variants in chromosome 5p15.33
region in non-smoker lung cancer patients. Adv Respir Med.
88:485–494. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Thomsen H, Chattopadhyay S, Hoffmann P,
Nöthen MM, Kalirai H, Coupland SE, Jonas JB, Hemminki K and Försti
A: Genome-wide study on uveal melanoma patients finds association
to DNA repair gene TDP1. Melanoma Res. 30:166–172. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Clarke WR, Amundadottir L and James MA:
CLPTM1L/CRR9 ectodomain interaction with GRP78 at the cell surface
signals for survival and chemoresistance upon ER stress in
pancreatic adenocarcinoma cells. Int J Cancer. 144:1367–1378. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Karami S, Han Y, Pande M, Cheng I, Rudd J,
Pierce BL, Nutter EL, Schumacher FR, Kote-Jarai Z, Lindstrom S, et
al: Telomere structure and maintenance gene variants and risk of
five cancer types. Int J Cancer. 139:2655–2670. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Parashar D, Geethadevi A, McAllister D,
Ebben J, Peterson FC, Jensen DR, Bishop E, Pradeep S, Volkman BF,
Dwinell MB, et al: Targeted biologic inhibition of both tumor
cell-intrinsic and intercellular CLPTM1L/CRR9-mediated
chemotherapeutic drug resistance. NPJ Precis Oncol. 5:162021.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Sinicrope FA, Ruan SB, Cleary KR, Stephens
LC, Lee JJ and Levin B: bcl-2 and p53 oncoprotein expression during
colorectal tumorigenesis. Cancer Res. 55:237–241. 1995.PubMed/NCBI
|
|
25
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(−Delta Delta C(T)) Method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ni Z, Chen Q, Lai Y, Wang Z, Sun L, Luo X
and Wang X: Prognostic significance of CLPTM1L expression and its
effects on migration and invasion of human lung cancer cells.
Cancer Biomark. 16:445–452. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Trezise S, Karnowski A, Fedele PL,
Mithraprabhu S, Liao Y, D'Costa K, Kueh AJ, Hardy MP, Owczarek CM,
Herold MJ, et al: Mining the plasma cell transcriptome for novel
cell surface proteins. Int J Mol Sci. 19:21612018. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Jia J, Bosley AD, Thompson A, Hoskins JW,
Cheuk A, Collins I, Parikh H, Xiao Z, Ylaya K, Dzyadyk M, et al:
CLPTM1L promotes growth and enhances aneuploidy in pancreatic
cancer cells. Cancer Res. 74:2785–2795. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Ye Y, Li Z, Kang S, Zhan X, Zhang Y, Xu Y,
Li W, Lang J, Liu P and Chen C: Impact of different postoperative
adjuvant therapies on the survival of early-stage cervical cancer
patients with one intermediate-risk factor: A multicenter study of
14 years. J Obstet Gynaecol Res. 49:1579–1591. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Curtin JP, Hoskins WJ, Venkatraman ES,
Almadrones L, Podratz KC, Long H, Teneriello M, Averette HA and
Sevin BU: Adjuvant chemotherapy versus chemotherapy plus pelvic
irradiation for high-risk cervical cancer patients after radical
hysterectomy and pelvic lymphadenectomy (RH-PLND): A randomized
phase III trial. Gynecol Oncol. 61:3–10. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
James MA, Vikis HG, Tate E, Rymaszewski AL
and You M: CRR9/CLPTM1L regulates cell survival signaling and is
required for Ras transformation and lung tumorigenesis. Cancer Res.
74:1116–1127. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
James MA, Wen W, Wang Y, Byers LA, Heymach
JV, Coombes KR, Girard L, Minna J and You M: Functional
characterization of CLPTM1L as a lung cancer risk candidate gene in
the 5p15.33 locus. PLoS One. 7:e361162012. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Puskás LG, Mán I, Szebeni G, Tiszlavicz L,
Tsai S and James MA: Novel Anti-CRR9/CLPTM1L antibodies with
antitumorigenic activity inhibit cell surface accumulation, PI3K
interaction, and survival signaling. Mol Cancer Ther. 15:985–997.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Grad JM, Zeng XR and Boise LH: Regulation
of Bcl-xL: A little bit of this and a little bit of STAT. Curr Opin
Oncol. 12:543–549. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Shimada M, Nishimura R, Nogawa T, Hatae M,
Takehara K, Yamada H, Kurachi H, Yokoyama Y, Sugiyama T and Kigawa
J: Comparison of the outcome between cervical adenocarcinoma and
squamous cell carcinoma patients with adjuvant radiotherapy
following radical surgery: SGSG/TGCU Intergroup Surveillance. Mol
Clin Oncol. 1:780–784. 2013. View Article : Google Scholar : PubMed/NCBI
|