Introduction
Hypoxia and the simultaneous activation of
antioxidative enzymes are well-known causes of tumor
radio-resistance (1–3). A novel radiosensitizer, Kochi Oxydol
Radiation Therapy for Unresectable Carcinoma (KORTUC), was
developed by Dr Yasuhiro Ogawa at Kochi University (Japan) in 2006,
for the treatment of malignant solid tumors containing numerous
hypoxic cancer cells and/or large quantities of antioxidative
enzymes (4–6). Hydrogen peroxide
(H2O2) is the only agent capable of
simultaneously inactivating antioxidant enzymes and producing
oxygen when applied to tumor tissues (7,8).
KORTUC is an injectable radiosensitizing drug solution consisting
of 0.5% H2O2 and 0.83% sodium hyaluronate
(HA). H2O2 is the active ingredient in this
radiosensitizer, whereas HA sustains H2O2 in
the tumor and delays the decomposition of
H2O2, which results in the maintenance of a
high concentration of oxygen in the tumor. Injecting these two
components at a particular ratio is a key feature of this product.
Ogawa et al (6) reported
that HA was the most effective supporting agent for
H2O2 in maintaining the oxygen concentration
in tumor tissues following intratumoral injection of the
H2O2 agent and for pain relief at the
intratumoral injection site.
A phase 2 clinical trial for locally
advanced/recurrent breast cancer is ongoing in the UK and India
(NCT03946202). In addition, several clinical studies on various
solid tumors are ongoing in Japan (6–11).
Clinical research on KORTUC at our institution has been conducted
since May 2010; as of April 2023, ~250 patients with various solid
cancers received this treatment, including >40 patients with
gynecological cancers treated with brachytherapy (BT) and
KORTUC.
The present study aimed to report the experience of
the present authors with the use of KORTUC, in combination with
interstitial BT (ISBT), in patients with locally recurrent cervical
cancer (LRCC), who are likely to have a high risk of poor
prognosis. Limited studies have evaluated BT for sensitizing
gynecological cancers (12,13). Moreover, the present authors have
previously reported a case of KORTUC for cervical cancer (14), in which radiotherapy (RT) combined
with KORTUC was performed for postoperative pelvic wall recurrence
of giant uterine cancer, and long-term control and survival were
achieved. Therefore, the present report summarized 15 cases in
which ISBT was performed in combination with KORTUC for long-term
control and life extension in patients with LRCC localized to the
pelvis.
Patients and methods
Ethical considerations
At our institution, KORTUC treatment was performed
after written informed consent was obtained from patients who were
expected to survive ≥1 year and met the following additional
criteria: i) Local control by conventional RT alone was presumed to
be difficult; ii) the dosage of additional irradiation they could
receive was limited; and iii) patients refused surgery as a
treatment option.
Patients with LRCC scheduled to undergo ISBT were
enrolled. The present clinical research was approved by the ethics
committee of Osaka Medical and Pharmaceutical University [Osaka
Medical and Pharmaceutical University; Clinical Trials Registry,
trial no. 1973 (May 10, 2010); UMIN Clinical Trials Registry, trial
no. UMIN000003734 (June 10, 2010)].
Method for dosing the KORTUC
sensitizer
KORTUC is an injectable solution consisting of 0.83%
HA and 0.5% H2O2 (also known as ‘OXYDOL’
antimicrobial antiseptic in Japan). It is prepared aseptically
before each use by mixing 2.5 ml HA (Adant® Dispo; Meiji
Saka Pharma) and 1.0 ml xylocaine 1% with 0.5 ml of OXYDOL to be
dispensed as a total volume of 4 ml from a single vial. The dosing
volume of KORTUC was 4–12 ml based on the tumor size. When used in
combination with external beam RT (EBRT), intratumoral injection of
KORTUC was performed either under direct vision via colposcopy or
through transrectal ultrasound (TRUS) guidance within 2 h before
EBRT. When used in combination with ISBT, KORTUC was administered
immediately after the interstitial bapplicator placement. If the
treatment was performed for 3 consecutive days or more, KORTUC was
additionally injected on the third day of treatment. Applicator
implantation was performed under TRUS guidance. The ambulatory
implantation technique was used. Flexible needle applicators were
cut down shortly to allow the patients to stand up and walk during
treatment. Three-dimensional-image CT-based treatment planning with
MRI assistance was also performed.
ISBT
For patients with no previous history of
irradiation, ISBT was combined with EBRT at 24 or 25 Gy in four or
five fractions. For patients with a previous irradiation history,
ISBT was administered as monotherapy at 45.5 Gy in seven fractions.
For palliative BT, the prescribed dose varies depending on the
patient. Local response was assessed by CT/MRI or gynecological
examination. The applicators were implanted under TRUS
guidance.
Outcomes
Survival periods were measured from the day after
the end of treatment. The treatment efficacy was evaluated through
gynecological examination, CT and MRI according to RECIST criteria
(15).
Statistical analysis
The tumor volume was measured using the Eclipse™
treatment planning system v11.0 (Varian Medical Systems, Inc.).
Continuous variables are presented as mean ± standard deviation.
Categorical variables are presented as numbers (percentages). The
Kaplan-Meier method was used to perform survival analysis and
differences were compared using the Wilcoxon rank-sum test.
Comparisons between the two groups and differences in the
parameters depending on the irradiation dose were performed using
the Wilcoxon rank-sum test. All experiments were performed in
duplicates. EZR v1.54 (Saitama Medical Center, Jichi Medical
University) and Excel 2016 (Microsoft Office Professional Plus
2016; Microsoft Corporation) were used for statistical analyses.
P<0.05 was considered to indicate a statistically significant
difference.
Results
Patient baseline characteristics
From April 2012 to January 2020, 14 female patients
with 15 lesions, with a mean age of 55 years (range, 34–80 years)
and primary FIGO stage IIB to IVB with LRCC, received KORTUC in
combination with ISBT (Table
I).
 | Table I.Patients characteristics. |
Table I.
Patients characteristics.
| Variable | Total) |
|---|
| Mean age (range),
years | 55 (34–80) |
| Histology, n (%) |
|
| Squamous
cell carcinoma | 11 (73.3) |
|
Adenocarcinoma | 4 (26.7) |
| Primary FIGO stage, n
(%) |
|
| IIB | 2 (13.3) |
| IIIA | 2 (13.3) |
| IIIB | 9 (60.0) |
| IVA | 2 (13.3) |
| IVB | 2 (13.3) |
| Prior therapy, n
(%) |
|
| RT | 8 (53.3) |
|
Surgery | 4 (26.7) |
| Surgery +
RT | 3 (20.0) |
Tumor site and treatment plans
The previous treatments for the 15 lesions with
recurrence were surgery (n=4), radiation therapy (RT; n=8) and
surgery + RT (n=3) (Table II).
Target lesions included the vaginal stump (n=5), pelvic wall (n=3),
cervix (n=3), vaginal wall (n=2) and lymph nodes (n=2). The median
tumor volume was 36 ml (range, 5–116 ml). Of the 15 target lesions,
four were treated with EBRT and cisplatin-based chemotherapy
(weekly cisplatin 40 mg/m2) before ISBT. The median
total BED (EBRT + ISBT) was 75 Gy (range, 54–98 Gy).
| Table II.Patient details regarding RT. |
Table II.
Patient details regarding RT.
| Patient no. | Target lesion | Tumor volume, ml | Post-surgery | Re-RT | External beam
radiation therapy, Gy × Fr. | Interstitial
brachytherapy, Gy × Fr. | Biological effective
dose, α/β10 |
|---|
| 1 | Vaginal stump | 69 | Yes | No | 50/25 | 24/4 | 98 |
| 2 | Vaginal stump | 92 | No | Yes | ND | 45.5/7 | 75 |
| 3 | Pelvic wall | 116 | Yes | No | 50/25 | 25/5 | 98 |
| 4 | Ln | 5 | Yes | No | 50/25 | 21/3 | 97 |
|
5a | Vaginal stump | 12 | Yes | Yes | ND | 45.5/7 | 75 |
| 6 | Cervix | 45 | No | Yes | ND | 45.5/7 | 75 |
| 7 | Ln | 11 | Yes | No | 50/25 | 18/3 | 89 |
| 8 | Pelvic wall | 30 | No | Yes | ND | 45.5/7 | 75 |
| 9 | Vaginal wall | 7 | No | Yes | ND | 32.5/5 | 54 |
| 10 | Cervix | 49 | No | Yes | ND | 45.5/7 | 75 |
| 11 | Vaginal wall | 42 | No | Yes | ND | 40/5 | 72 |
| 12 | Pelvic wall | 29 | No | Yes | ND | 25/2 | 56 |
| 13a | Vaginal stump | 13 | Yes | Yes | ND | 45.5/7 | 75 |
| 14 | Vaginal stump | 27 | Yes | Yes | ND | 45.5/7 | 75 |
| 15 | Cervix | 83 | No | Yes | ND | 45.5/7 | 75 |
Before RT, KORTUC was injected intratumorally under
the direct vision of colposcopy. For patients who received ISBT,
KORTUC was administered before or after insertion of the
applicator, before irradiation. The intratumoral injection of
KORTUC was completed without any technical or safety issues for any
of the 15 patients. KORTUC was well tolerated and no adverse events
related to the KORTUC injection were observed, except for transient
local pain (grade 1) in three patients at the injection site. In
any of these cases, local pain disappeared within 10 min after
injection. No late adverse events such as increased tissue fibrosis
associated with the addition of sensitizers were observed. However,
in cases where KORTUC was injected before implantation, the
transrectal echo image acquired high brightness owing to the
influence of oxygen and insertion became difficult because the
cross-sectional information was not accessible. Subsequently, in
all cases, the injection was performed after implantation and the
problem disappeared.
Therapeutic effects
Table III shows
that patients were followed up for 6–116 months (median follow-up,
24 months). Of the 14 patients, eight died due to cancer
exacerbation within 8–30 months after treatment. A total of five
(33%) patients experienced disease recurrence after treatment. A
complete response (CR) was observed in 86.7% (13/15) of patients
and the overall response rate (partial response + CR) was 100.0%
(15/15).
| Table III.Patients' outcomes. |
Table III.
Patients' outcomes.
| Patient no. | Local response | Recurrence | Follow-up,
months |
|---|
| 1 | CR | No | 116 |
| 2 | CR | No | 11 |
| 3 | CR | No | 61 |
| 4 | CR | No | 59 |
|
5a | CR | Yes | 53 |
| 6 | PR | Yes | 9 |
| 7 | CR | No | 42 |
| 8 | CR | Yes | 24 (TD) |
| 9 | CR | Yes | 30 (TD) |
| 10 | CR | No | 6 |
| 11 | PR | No | 8 |
| 12 | CR | No | 8 (TD) |
| 13a | CR | No | 32 |
| 14 | CR | No | 8 |
| 15 | CR | N0 | 6 |
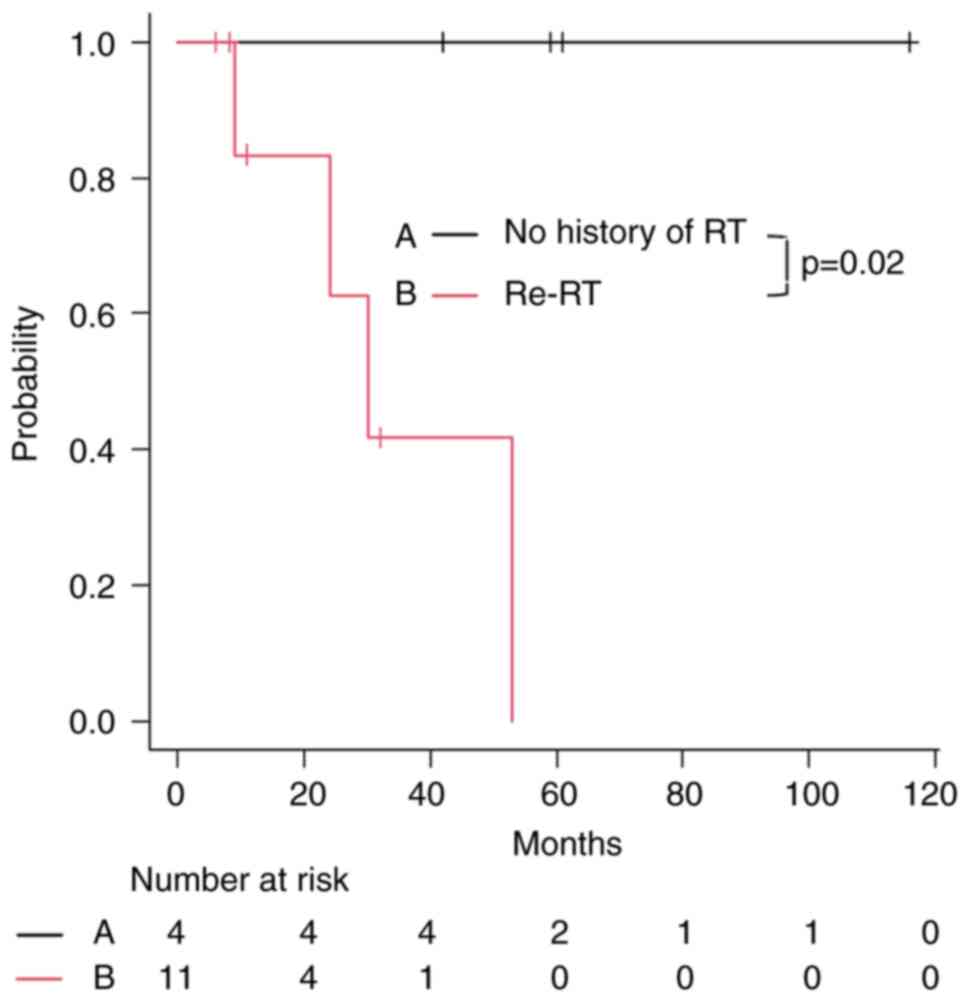
The 2-year local control rate (LCR) in patients who
received ISBT + KORTUC was 79% (Fig.
1). The 2-year LCR was significantly lower (P=0.02) in the
re-irradiation group (63%) than that in the non-irradiation group
(100%), as shown in Fig. 2.
Discussion
Radical treatment of LRCC is difficult in most cases
because several organs located near the tumor site are at risk,
such as the rectum, sigmoid colon, small intestine, bladder and
urethra. The indications for curative organ-sparing salvage surgery
or pelvic exenteration are limited (16). EBRT with or without chemotherapy is
well tolerated; however, its treatment outcomes are not
satisfactory and its indication is limited to patients with a
history of RT (17). RT has become
the treatment of choice for unresectable gynecological cancers
(18–20); however, EBRT is almost inapplicable
in patients with a history of RT (21).
Therefore, we hypothesize that ISBT may act as a
salvage treatment for such patients. However, even in the present
case, ISBT (without KORTUC) achieved a 3-year LCR rate of 75% in 56
patients with LRCC (14). The
3-year LCR was 85% in patients with no history of RT after radical
surgery, whereas the recurrence rate after radical irradiation was
significantly lower (46%) (14). In
the present study, the 2-year LCR was 79%, of which 100% was in
patients with no history of RT, whereas it was 63% in patients with
recurrence and history of RT.
Previous reports indicated that the LCR of ISBT for
recurrence after radical irradiation ranges from 45–100% (19–26).
This is because, even in the same recurrence cases, there is a
mixture of patients with various prognostic factors, such as size,
location and previous treatment history; therefore, it is difficult
to make a comparison with the present study. The current study did
not recruit patients with small tumors close to the vaginal stump
that could be controlled with RT alone. For this reason, it was
speculated that the results would be lower than those of other
studies; nevertheless, good results were obtained in this
study.
In agreement with previous studies, KORTUC had
almost no adverse events associated with intratumor injection
(9–11,27).
However, when KORTUC was injected before
implantation, it became difficult to accurately understand the
positional information of the tumor; therefore, this point requires
further attention. In this case, the problem can be solved by
injection after implantation; however, it becomes somewhat
difficult to distinguish between the echo image of the applicator
that has already been inserted and the KORTUC injection needle. In
CT-guided implantation, the location of the tumor is somewhat
obscured; however, information on the position of the injection
needle is easy to obtain. MRI-guided implantation has the potential
to solve all these problems (tumor and injection needle location
information) and the present authors are considering introducing it
in the future. At present, it is unclear whether the presence or
absence of KORTUC can improve the outcome of RT; however, the
current evidence is promising. The present study presents some
drawbacks that limit its ability in discussing the efficacy of
KORTUC. For example, this study was conducted at a single
institution and included a small number of cases. Future studies
may evaluate the efficacy of KORTUC by conducting prospective
clinical trials at other institutions.
To the best of our knowledge, only one phase I
clinical trial has been completed at the time of writing and it
showed no significant adverse effects in patients with locally
advanced breast cancer (28). A
phase II study for breast cancer is ongoing at five sites in the UK
and India, which is the only phase II trial to date (NCT03946202).
In the future, more clinical trials are needed to promote the
widespread use of KORTUC and to include it within insurance
coverage. To further evaluate the effects of KORTUC, a Phase I/II
study of locally advanced cervical cancer is planned to start in
2023. In that study, KORTUC will be administered in combination
with EBRT for newly diagnosed patients with locally advanced
cervical cancer.
The present study confirmed that KORTUC
intra-tumoral injection is safe, well-tolerated and effective for
the ISBT-sensitizing treatment of LRCC. KORTUC also showed efficacy
in local control in patients with recurrence. Based on these
findings, the present authors would like to confirm in a future
study the efficacy of KORTUC combined with EBRT, as well as ISBT,
for newly diagnosed unresectable locally advanced cervical cancer,
with high-risk factors of poor prognosis. KORTUC may be an
effective radiation response enhancer in multiple cancer types, in
which locoregional control after RT alone remains poor.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
TS, KN and KY designed the study and wrote the
manuscript. TS, MN and HY analyzed and interpreted the patient's
clinical data. TS, KK, TO, AK, CS, AH and ST performed the KORTUC
treatment and statistical analysis. HA contributed to collecting
the relevant literature and performing the data analysis. TS and KY
confirm the authenticity of all the raw data. All authors have read
and approved the final version of the manuscript.
Ethics approval and consent to
participate
Written informed consent was obtained from all
patients. Approval was obtained from the Ethics Committee of Osaka
Medical and Pharmaceutical University [Osaka Medical and
Pharmaceutical University Clinical Trials Registry, trial no. 1973,
(May 10, 2010); UMIN Clinical Trials Registry, trial no.
UMIN000003734, (June 10, 2010)].
Patient consent for publication
The patients provided written informed consent for
the publication.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Moeller BJ and Dewhirst MW: HIF-1 and
tumour radiosensitivity. Br J Cancer. 95:1–5. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ogawa Y, Nishioka A, Hamada N, Terashima
M, Inomata T, Yoshida S, Seguchi H and Kishimoto S:
Immunohistochemical study of c-fos-positive lymphocytes infiltrated
into human squamous cell carcinomas of the head and neck during
radiation therapy and its clinical significance. Clin Cancer Res.
3((12 Pt 1)): 2301–2307. 1997.PubMed/NCBI
|
|
3
|
Ogawa Y, Nishioka A, Hamada N, Terashima
M, Inomata T, Yoshida S, Seguchi H and Kishimoto S: Expression of
Fas (CDcd95/APO-1) antigen induced by radiation therapy for diffuse
B-cell lymphoma: Immunohistochemical study. Clin Cancer Res. 3((12
Pt 1)): 2211–2216. 1997.PubMed/NCBI
|
|
4
|
Ogawa Y, Kubota K, Ue H and Nishioka A:
Development and clinical application of a new radiosensitizer
containing hydrogen peroxide and hyaluronic acid sodium for topical
tumor injection-A new enzyme-targeting radiosensitization
treatment, KORTUC II (Kochi Oxydol-Radiation Therapy for
Unresectable Carcinomas, Type II). Procedings of the 8th
International Meeting on Progress in Radio-Oncology (ICRO/OGRO 8).
ICRO/OGRO 8. 183:100–101. 2007.PubMed/NCBI
|
|
5
|
Ogawa Y, Ue H, Tsuzuki K, Tadokoro M,
Miyatake K, Sasaki T, Yokota N, Hamada N, Kariya S, Hitomi J, et
al: New radiosensitization treatment (KORTUC I) using hydrogen
peroxide solution soaked gauze bolus for unresectable and
superficially exposed neoplasms. Oncol Rep. 19:1389–1394.
2008.PubMed/NCBI
|
|
6
|
Ogawa Y, Kubota K, Ue H, Kataoka Y,
Tadokoro M, Miyatake K, Tsuzuki K, Yamanishi T, Itoh S, Hitomi J,
et al: Phase I study of a new radiosensitizer containing hydrogen
peroxide and sodium hyaluronate for topical tumor injection: A new
enzyme targeting radiosensitization treatment, Kochi Oxydol
Radiation Therapy for Unresectable Carcinomas, type II (KORTUC II).
Int J Oncol. 34:609–618. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ogawa Y, Kubota K, Aoyama N, Yamanishi T,
Kariya S, Hamada N, Nogami M, Nishioka A, Onogawa M and Miyamura M:
Non-surgical breast-conserving treatment (KORTUC-BCT) using a new
radio-sensitization method (KORTUC II) for patients with stage I or
II breast cancer. Cancers (Basel). 7:2277–2289. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Takaoka T, Shibamoto Y, Matsuo M, Sugie C,
Murai T, Ogawa Y, Miyakawa A, Manabe Y, Kondo T, Nakajima K, et al:
Biological effects of hydrogen peroxide administered intratumorally
with or without irradiation in murine tumors. Cancer Sci.
108:1787–1792. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Shimbo T, Nakata M, Yoshioka H, Sato C,
Hori A, Kimura K, Iwamoto M, Yoshida K, Uesugi Y, Akiyama H and
Nihei K: New enzyme-targeting radiosensitizer (KORTUC II) treatment
for locally advanced or recurrent breast cancer. Mol Clin Oncol.
15:2412021. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Obata S, Ishimaru Y, Miyagi S, Nakatake M,
Kuroiwa A, Ohta Y, Kan T, Kanegae S, Inoue Y, Nishizato R and
Miyazaki K: Actual practice of Kochi oxydol radiation therapy for
unresectable carcinomas by intra-tumoral administration of hydrogen
peroxide as a radiosensitizer. Mol Clin Oncol. 16:682022.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Nishioka A, Ogawa Y, Miyatake K, Tadokoro
M, Nogami M, Hamada N, Kubota K, Kariya S, Kohsaki T, Saibara T, et
al: Safety and efficacy of image-guided enzyme-targeting
radiosensitization and intraoperative radiotherapy for locally
advanced unresectable pancreatic cancer. Oncol Lett. 8:404–408.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Tseng M, Ngoi NY, Tan DS and Tong PS:
Combined modality management of advanced cervical cancer including
novel sensitizers. Int J Gynecol Cancer. 32:246–259. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Zhou Y, Espenel S, Achkar S, Leary A, Gouy
S and Chargari C: Combined modality including novel sensitizers in
gynecological cancers. Int J Gynecol Cancer. 32:389–401. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Nakata M, Yoshida K, Shimbo T, Yoshikawa
N, Yoshioka H, Hori A, Sato C, Uesugi Y, Kogata Y, Masui K, et al:
High-dose-rate interstitial brachytherapy with hypoxic
radiosensitizer KORTUC II for unresectable pelvic sidewall
recurrence of uterine cervical cancer: A case report. J Contemp
Brachytherapy. 12:606–611. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Miller B, Morris M, Rutledge F, Mitchell
MF, Atkinson EN, Burke TW and Wharton JT: Aborted exenterative
procedures in recurrent cervical cancer. Gynecol Oncol. 50:94–99.
1993. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Maneo A, Landoni F, Cormio G, Colombo A,
Placa F, Pellegrino A and Mangioni C: Concurrent
carboplatin/5-fluorouracil and radiotherapy for recurrent cervical
carcinoma. Ann Oncol. 10:803–807. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Stock RG, Chan K, Terk M, Dewyngaert JK,
Stone NN and Dottino P: A new technique for performing Syed-Neblett
template interstitial implants for gynecologic malignancies using
transrectal-ultrasound guidance. Int J Radiat Oncol Biol Phys.
37:819–825. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Mabuchi S, Takahashi R, Isohashi F, Yokoi
T, Okazawa M, Sasano T, Maruoka S, Anzai M, Yoshioka Y, Ogawa K and
Kimura T: Reirradiation using highdose-rate interstitial
brachytherapy for locally recurrent cervical cancer. Int J Gynecol
Cancer. 24:141–148. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Nag S, Yacoub S, Copeland LJ and Fowler
JM: Interstitial brachytherapy for salvage treatment of vaginal
recurrences in previously unirradiated endometrial cancer patients.
Int J Radiat Oncol Biol Phys. 54:1153–1159. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Hedman M, Bjork-Eriksson T, Mercke C, West
C, Hesselius P and Brodin O: Comparison of predicted and clinical
response to radiotherapy: A radiobiology modelling study. Acta
Oncol. 48:584–590. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Yoshida K, Yamazaki H, Kotsuma T, Takenaka
T, Masui K, Yoshioka Y, Uesugi Y, Shimbo T, Yoshikawa N, Yoshioka
H, et al: Treatment results of image-guided high-dose-rate
interstitial brachytherapy for pelvic recurrence of uterine cancer.
Brachytherapy. 14:440–448. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Viswanathan AN, Cormack R, Holloway CL,
Tanaka C, O'Farrell D, Devlin PM and Tempany C: Magnetic
resonance-guided interstitial therapy for vaginal recurrence of
endometrial cancer. Int J Radiat Oncol Biol Phys. 66:91–99. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Beriwal S, Rwigema JC, Higgins E, Kim H,
Houser C, Sukumvanich P, Olawaiye A, Richard S, Kelley JL, Edwards
RP and Krivak TC: Three-dimensional imagebased high-dose-rate
interstitial brachytherapy for vaginal cancer. Brachytherapy.
11:176–180. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Popowski Y, Hiltbrand E, Joliat D and
Rouzaud M: Open magnetic resonance imaging using titanium-zirconium
needles: Improved accuracy for interstitial brachytherapy implants?
Int J Radiat Oncol Biol Phys. 47:759–765. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Tewari K, Cappuccini F, Brewster WR,
DiSaia PJ, Berman ML, Manetta A, Puthawala A, Nisar Syed AM and
Kohler MF: Interstitial brachytherapy for vaginal recurrences of
endometrial carcinoma. Gynecol Oncol. 74:416–422. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Ogawa Y, Kubota K, Ue H, Tadokoro M,
Matsui R, Yamanishi T, Hamada N, Kariya S, Nishioka A, Nakajima H,
et al: Safety and effectiveness of a new enzyme-targeting
radio-sensitization treatment (KORTUC II) for intratumoral
injection for low-LET radio-resistant tumors. Int J Oncol.
39:553–560. 2011.PubMed/NCBI
|
|
28
|
Nimalasena S, Gothard L, Anbalagan S,
Allen S, Sinnett V, Mohammed K, Kothari G, Musallam A, Lucy C, Yu
S, et al: Intratumoral hydrogen peroxide with radiation therapy in
locally advanced breast cancer: Results from a phase 1 clinical
trial. Int J Rad Oncol Biol Phys. 108:1019–1029. 2020. View Article : Google Scholar : PubMed/NCBI
|