Introduction
Triple-negative breast cancer (TNBC) cases account
for 15–20% of total breast cancer incidence, but patients with TNBC
face a worse prognosis in due to the fact that these tumor cells do
not express traditional therapeutic targets, including hormone
receptors and human epidermal growth factor receptor-2 (1). In addition, TNBC cases tend to be more
aggressive and associated with a higher risk or recurrence,
contributing to a higher overall mortality risk (2,3). As
endocrine and targeted therapy strategies fail to effectively treat
TNBC, patients primarily undergo chemotherapeutic and surgical
treatment. No differences in survival rates have been observed
between patients with TNBC who undergo adjuvant chemotherapy and
those that undergo neoadjuvant chemotherapy (NAC), such that the
latter has emerged as the preferred systemic treatment regimen for
this cancer type (4). NAC enables
the direct assessment of tumor responses to chemotherapeutic drug
administration, allowing clinicians to gauge patient prognosis and
to opt for further adjuvant chemotherapy as appropriate (5). Given that TNBC tumors are generally
more sensitive to cytotoxic drugs, higher pathological complete
response (pCR) rates tend to be observed following NAC, which is
noteworthy given that those patients who achieve pCR after NAC
exhibit a better prognosis compared with those who do not (6). When residual tumor (RT) tissue is
evident after NAC, patients face higher recurrence rates and
shorter overall survival (OS) (7).
The CREATE-X trial determined that those patients with TNBC and RT
who postoperatively undergo intensified adjuvant capecitabine
therapy experience improved outcomes (5). However, the administration of further
cytotoxic drugs can also contribute to a higher risk of toxic side
effects with the potential to impact patient quality of life,
including persistent peripheral neuropathy and an elevated risk of
cardiac events (8). Moreover, a
subset of these patients with RT fail to relapse, suggesting that
some of these individuals exhibit a good prognosis (9). Thus, there is a pressing need to
identify novel biomarkers capable of reliably predicting patients
with RT outcomes in order to guide the identification of high-risk
patients that are most likely to benefit from the administration of
further adjuvant chemotherapy. Such biomarkers would provide an
effective approach to the individualized treatment of patients with
TNBC by minimizing the risk of unnecessary treatment-related
toxicity while maximizing the odds of better therapeutic
outcomes.
Malignant tumor development is strongly influenced
by the composition of the tumor microenvironment (TME), which
consists of extracellular matrix components and a range of cell
types. Tumor-infiltrating lymphocytes (TILs) within the TME are
particularly relevant, given that they comprise the majority of
this niche and are also vital to the effective control of
tumorigenesis (10,11). TILs include a range of mononuclear
immune cell populations including natural killer cells, dendritic
cells, CD4+ T cells and CD8+ T cells
(12,13). TIL infiltration has been reported in
up to 75% of TNBC tumors, of which ~20% exhibit particularly high
levels of such infiltration (14).
In one recent meta-analysis focused on patients with TNBC
undergoing NAC, a higher level of total TIL or TIL subtype
(CD4+ or CD8+) infiltration prior to
treatment was associated with higher pCR rates and improved
post-treatment OS and recurrence-free survival (RFS) (15). Cytotoxic drug treatment can
contribute to the mobilization and activation of TILs within the
TME, thus reflecting TME responses to chemotherapy. Accordingly,
analyses of TILs present in RT tissue can potentially offer
additional prognostic information beyond that provided by analyses
of pre-treatment TILs (16). The
evaluation of RT TILs is also currently recommended by both the
International Immuno-Tumor Biomarkers Working Group (14) and the International Immuno-Tumor
Biomarkers Working Group.
There have been relatively few studies focused on
the clinical relevance of TIL infiltration in RT tissue following
NAC in patients with TNBC, and the prognostic value of such
infiltration is still subject to controversy. As such, the present
meta-analysis focused on those patients with TNBC that failed to
achieve pCR after NAC in order to assess the prognostic value of
TILs in RT tissue.
Materials and methods
Search strategy
Relevant studies published as of March 2023 were
identified by searching the Pubmed (https://pubmed.ncbi.nlm.nih.gov/), Embase (www.embase.com/), The Cochrane Library (https://www.cochranelibrary.com/), and Web of
Science (https://www.webofknowledge.com/) databases using the
following search terms: ‘Triple negative breast cancer’,
‘tumor-infiltrating lymphocytes’, ‘neoadjuvant chemotherapy’ and
‘residual tumors’. Subject headings combined with free words were
used for study retrieval.
Inclusion and exclusion criteria
Studies eligible for inclusion were: i) Published in
English; ii) studies enrolling patients with TNBC that did not
achieve pCR following NAC; iii) studies assessing the association
between RT TILs and TIL subtypes (CD8+ or
CD4+) in RT tissue and patient prognosis; iv) original
research studies of any design; and v) studies in which
prognosis-related hazard ratios (HRs) and 95% confidence intervals
(CIs) were provided or could be calculated indirectly. Studies were
excluded if they were: i) Case reports, systematic reviews or
literature reviews; ii) articles enrolling patients that achieved
pCR following NAC; iii) studies lacking outcome indicators; or iv)
studies for which HRs and 95% CIs could not be established.
Data extraction and quality
analyses
Study screening was independently performed by two
investigators, who initially conducted title, abstract and
full-text review based on the established inclusion and exclusion
criteria. Discrepancies were resolved by discussion and consensus.
Relevant data were extracted from eligible studies, including:
First author, publication year, country, sample size, TILs subtype,
high infiltration threshold, detection method, outcome indicators,
HRs and 95% CIs.
Literature quality evaluation
Included study quality was assessed using the
Newcastle-Ottawa Quality Assessment Scale (NOS) (17). Possible NOS scores were between 0
and 9, and high-quality studies were those with scores of ≥6.
Statistical analysis
Stata 14.0 (version 12.0; StataCorp LP) and Rev Man
5.3 (RevMan 5.3; Cochrane) were used to conduct this meta-analysis
as per the Cochrane International Collaboration Network Systematic
Review Guidelines. Pooled effect sizes for survival data were
calculated using HRs and 95% CIs, and P<0.05 was selected as the
cut-off for statistical significance. The I2 statistic
and Cochrane's Q test were used to assess the heterogeneity of
included studies, with P<0.10 or I2>50% being
considered indicative of significant heterogeneity. Random and
fixed effect models were used when significant heterogeneity was
and was not detected, respectively (18). Additional analyses of heterogeneity
were performed by specifically analyzing results pertaining to TILs
and TILs subtypes (CD8+ or CD4+). Egger's
test and funnel plots were used to gauge publication bias, with
P<0.05 as the cut-off for publication bias detection. P<0.05
was considered to indicate a statistically significant
difference.
Results
Study selection and
characteristics
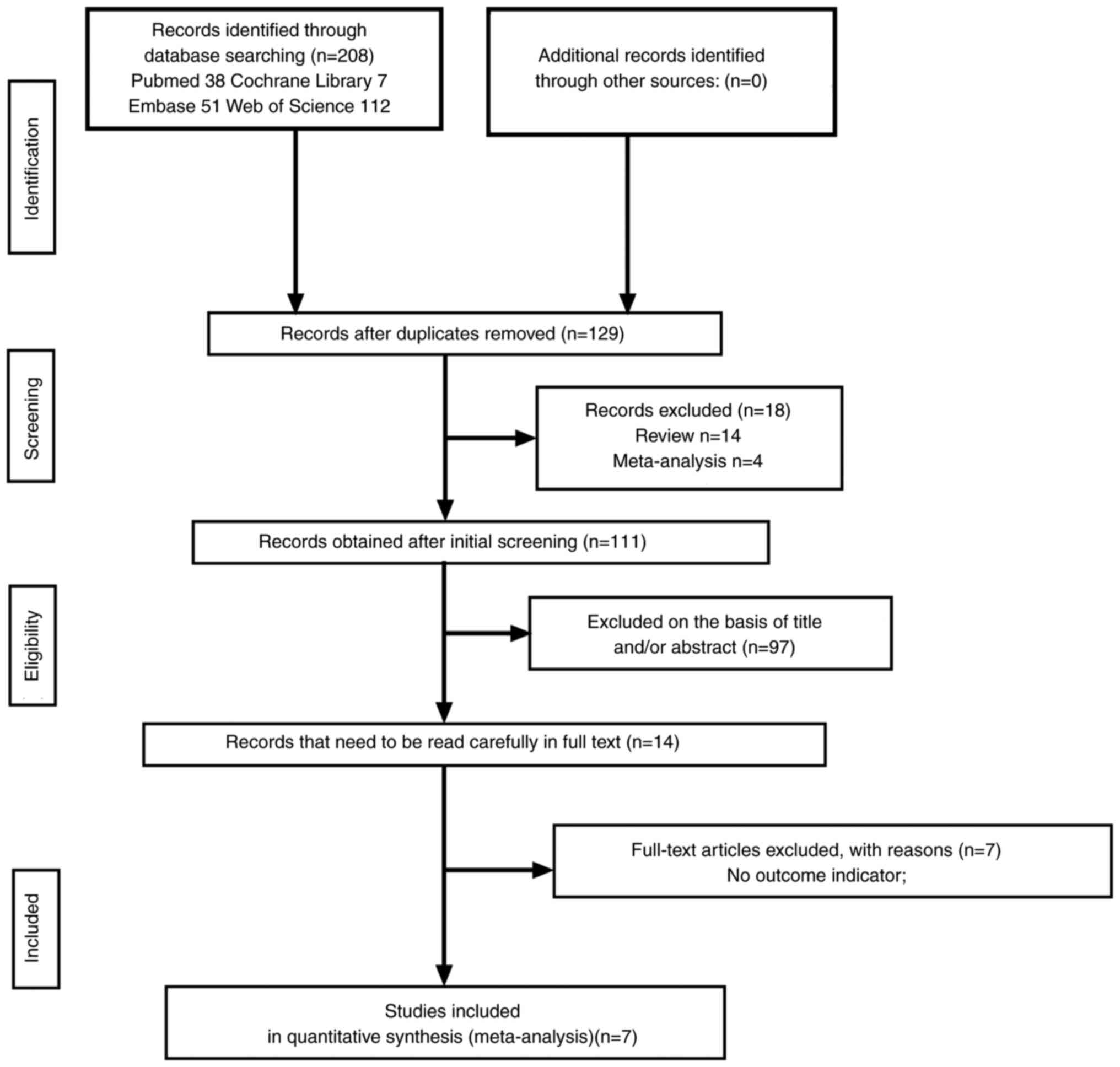
The initial study search yielded 208 potentially
relevant studies, of which seven enrolling 1,202 patients with TNBC
were ultimately included in this analysis (Fig. 1).
All studies eligible for inclusion in the present
meta-analysis were retrospective cohort studies. TILs were
classified into intratumoral TILs (iTILs) and stromal TILs (sTILs)
based on their distributions. CD4+ and CD8+ T
cells were the primary TIL subtypes, as distinguished through
immunohistochemical staining, and the thresholds used to define
high TIL or TIL subtype (CD4+ or CD8+)
infiltration varied across studies (Table I).
 | Table I.Baseline characteristics of included
studies. |
Table I.
Baseline characteristics of included
studies.
| First author | Year | Country | Sample size | Type of TILs | Threshold | TILs evaluation
method | Outcome | (Refs.) |
|---|
| Dieci et
al | 2014 | France | 278 | iTILs and/or
sTILs | 60% | H&E | MFS/OS | (27) |
| Miyashita et
al | 2015 | Japan | 101 |
CD8+ | Not specified |
IHC | RFS/BCSS | (36) |
| Luen et
al | 2019 | Australia | 375 | sTILs | 20% | H&E | RFS/OS | (19) |
| Pinard et
al | 2019 | France | 109 |
CD8+ | 0.164 |
IHC | DRFI | (32) |
|
| 2019 | France | 109 |
CD4+ | 0.066 |
IHC | DRFI | (32) |
| Wang et
al | 2021 | China | 109 | sTILs | 30% | H&E | RFS/OS | (29) |
| Da Silva et
al | 2022 | Brazilian | 134 |
CD8+ | Not specified |
IHC | EFS | (31) |
|
| 2022 | Brazilian | 134 |
CD4+ | Not specified |
IHC | EFS/OS | (31) |
| Lejeune et
al | 2023 | Spain | 96 |
CD4+ | Not specified |
IHC | RFS/OS | (28) |
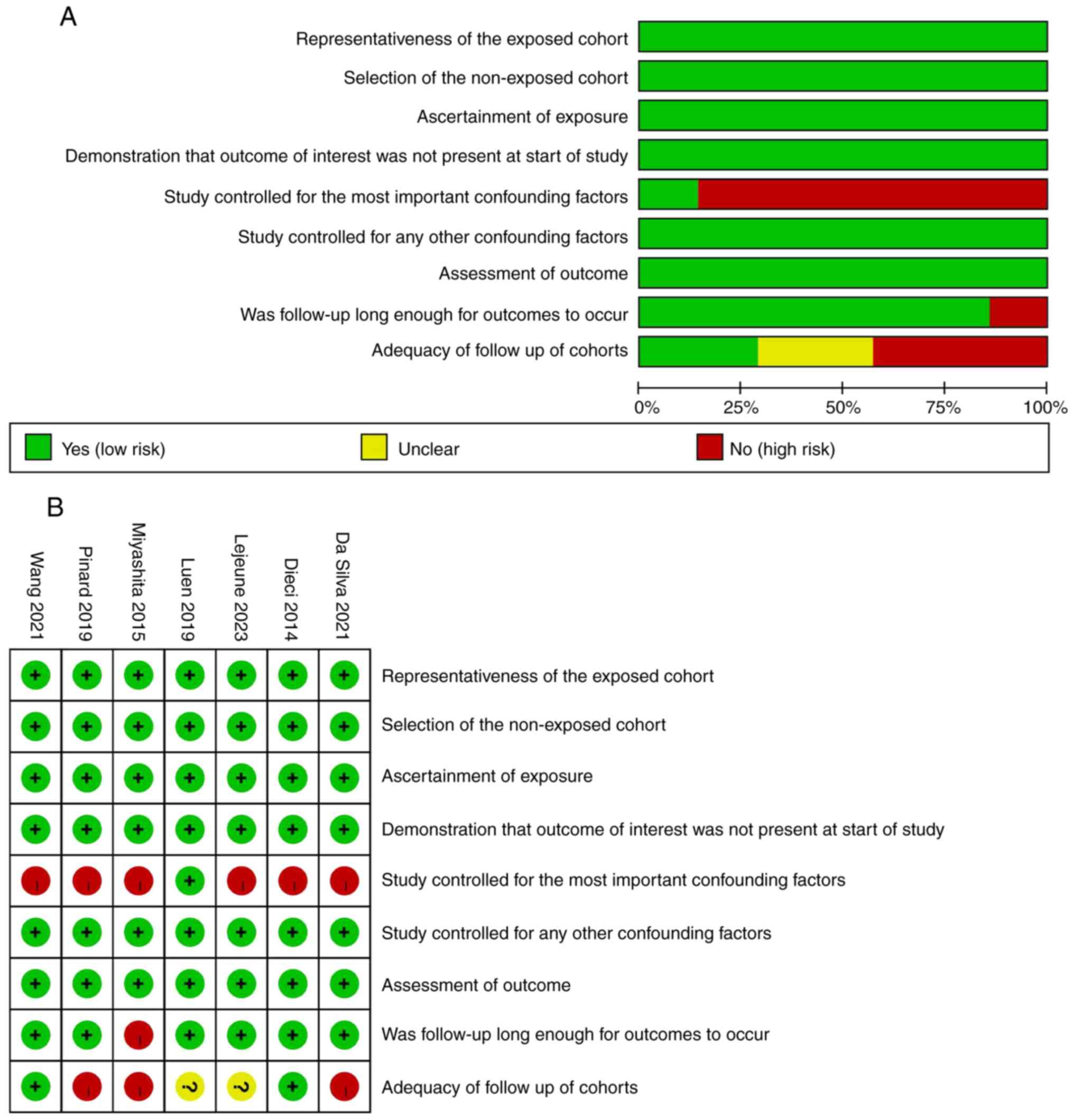
Analyses of study quality
All seven of the included studies exhibited NOS
scores >7, and were thus classified as high-quality studies
(Fig. 2).
Association between RT TIL
infiltration and RFS/MFS/EFS/DRFI
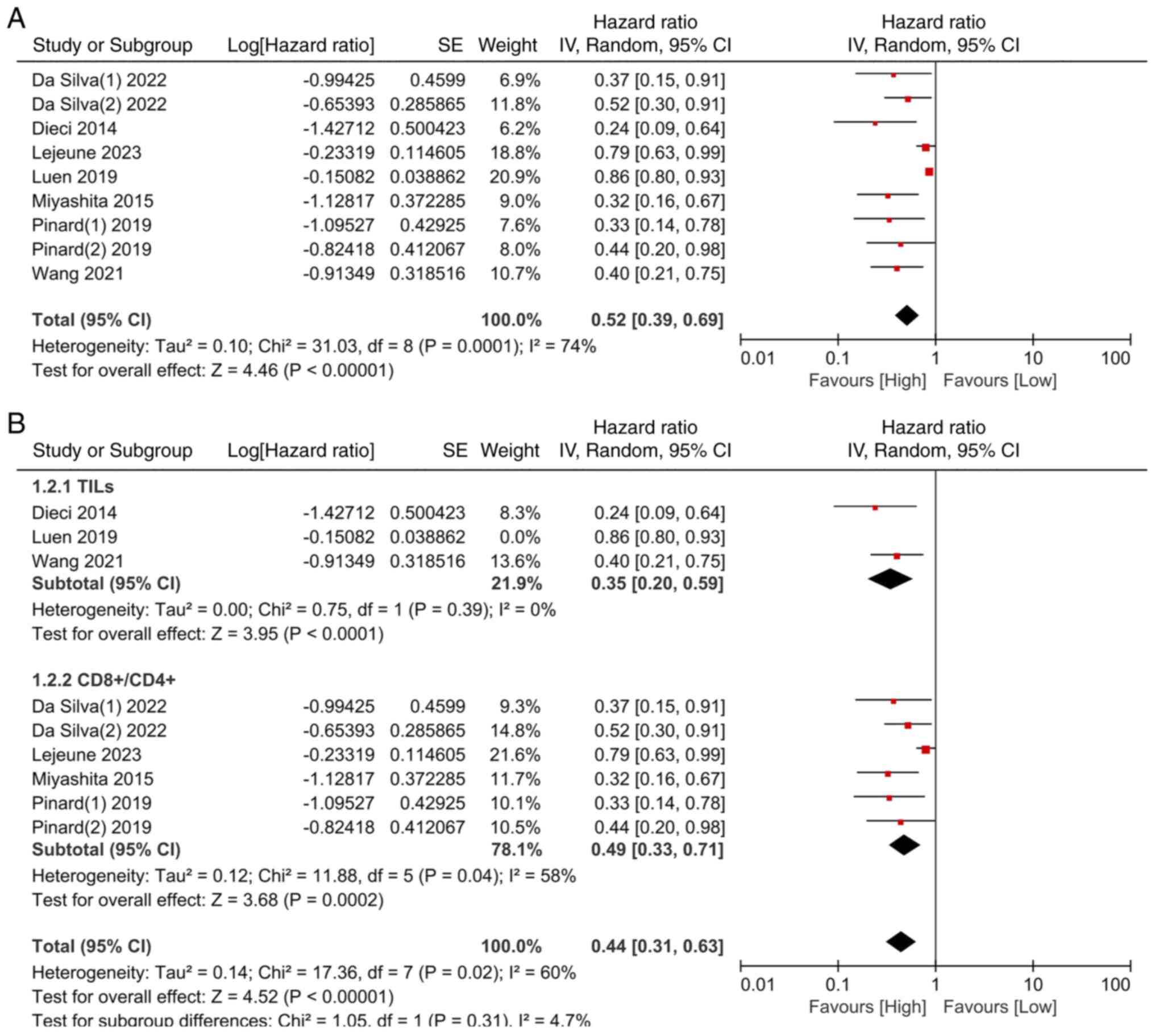
In total, the seven included studies enrolled 1,202
patients. A high degree of heterogeneity was detected among these
studies (I2=74.2%; P=0.0001), and results were thus
analyzed with a random effects model. In sensitivity analyses, the
iterative omission of individual studies from pooled analyses did
not impact the overall results, indicating that this selected
random effects model yielded stable and reliable results. Pooled
analyses revealed that those patients with high levels of total TIL
or TIL subtype (CD4+ or CD8+) infiltration in
RT tissue following NAC exhibited significantly improved
recurrence-free survival (RFS)/metastasis-free survival
(MFS)/event-free survival (EFS)/distant recurrence-free interval
(DRFI) as compared with patients with lower infiltration levels
(HR=0.52; 95% CI=0.39–0.69; P<0.00001) (Fig. 3A).
When subgroup analyses for this endpoint were
conducted for studies analyzing total TILs and TIL subtypes
(CD4+ or CD8+), a total of three studies were
included that provided results for overall TIL infiltration. Pooled
analyses of these studies were conducted with a random effects
model owing to a high degree of heterogeneity (I2=83%;
P=0.002), and the exclusion of the study by Luen et al
(2019) (19) eliminated this
heterogeneity (I2=0%; P=0.39). When results were
analyzed with a fixed effects model for this subgroup, patients
with high levels of TIL infiltration exhibited improved
RFS/MFS/EFS/DFRI compared with patients with low TIL infiltration
(HR=0.35; 95% CI=0.20–0.59; P<0.0001) (Fig. 3B). In addition, four studies
reported results for the TIL subtype (CD4+ or
CD8+) subgroup, and a random effects model was used
owing to moderate heterogeneity (I2=58%; P=0.04). Pooled
analyses for this subgroup similarly confirmed that patients with
high levels of TIL infiltration exhibited improved RFS/MFS/EFS/DRFI
compared with patients with low levels of TIL infiltration
(HR=0.49; 95% CI=0.33–0.71; P=0.0002) (Fig. 3B). Sensitivity analyses revealed no
changes in the combined effect size when alternating between fixed
and random effects models, confirming that these results are
robust.
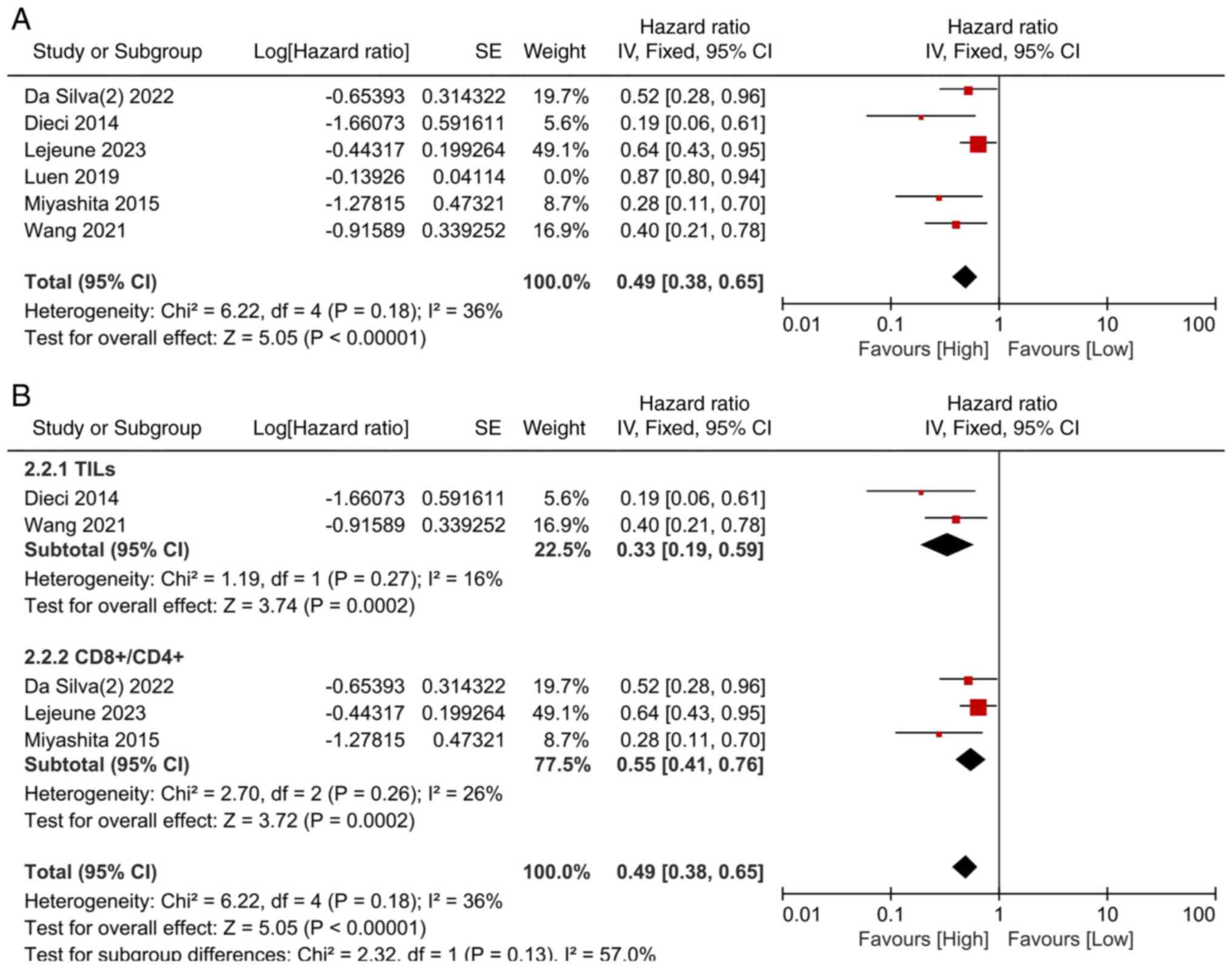
Association between RT TIL
infiltration and OS/BCSS
In total, six of the included studies incorporating
1,093 patients reported on OS/BCSS outcomes. As a high degree of
heterogeneity was detected (I2=77%; P=0.0007), a random
effects model was selected. Sensitivity analyses indicated that the
study conducted by Luen et al (19) had the greatest effect on this
heterogeneity, which was reduced following the exclusion of this
study (I2=36%; P=0.18). A fixed effects model was thus
selected for pooled analyses based on this reduction in
heterogeneity. This approach revealed that patients with high
levels of total TIL or TIL subtype (CD4+ or
CD8+) infiltration exhibited significantly improved
OS/BCSS relative to patients with lower levels of such infiltration
(HR=0.49; 95% CI=0.38–0.65; P<0.00001) (Fig. 4A).
Subgroup analyses of studies assessing TILs and TIL
subtypes (CD4+ or CD8+) were additionally
conducted for this endpoint. Just two studies were included in the
TILs subgroup, and pooled analyses of these studies were performed
with a fixed effects model owing to an absence of heterogeneity
(I2=16%; P=0.27). The present analysis demonstrated that
patients with higher levels of RT TIL infiltration following NAC
exhibited better OS/BCSS as compared with patients with low levels
of infiltration (HR=0.33; 95% CI=0.19–0.59; P=0.0002) (Fig. 4B). In addition, three studies
reported results for TIL subtypes (CD4+ or
CD8+), and these pooled analyses were also performed
with a fixed effects model owing to the absence of significant
heterogeneity (I2=26%; P=0.26). As aforementioned, those
patients with higher levels of TIL (CD4+ or
CD8+) infiltration exhibited significantly better
OS/BCSS as compared with patients with lower levels of such
infiltration (HR=0.55; 95% CI=0.41–0.76; P=0.0002) (Fig. 4B). Sensitivity analyses revealed no
changes in the combined effect size when alternating between fixed
and random effects models, confirming that these results are
robust.
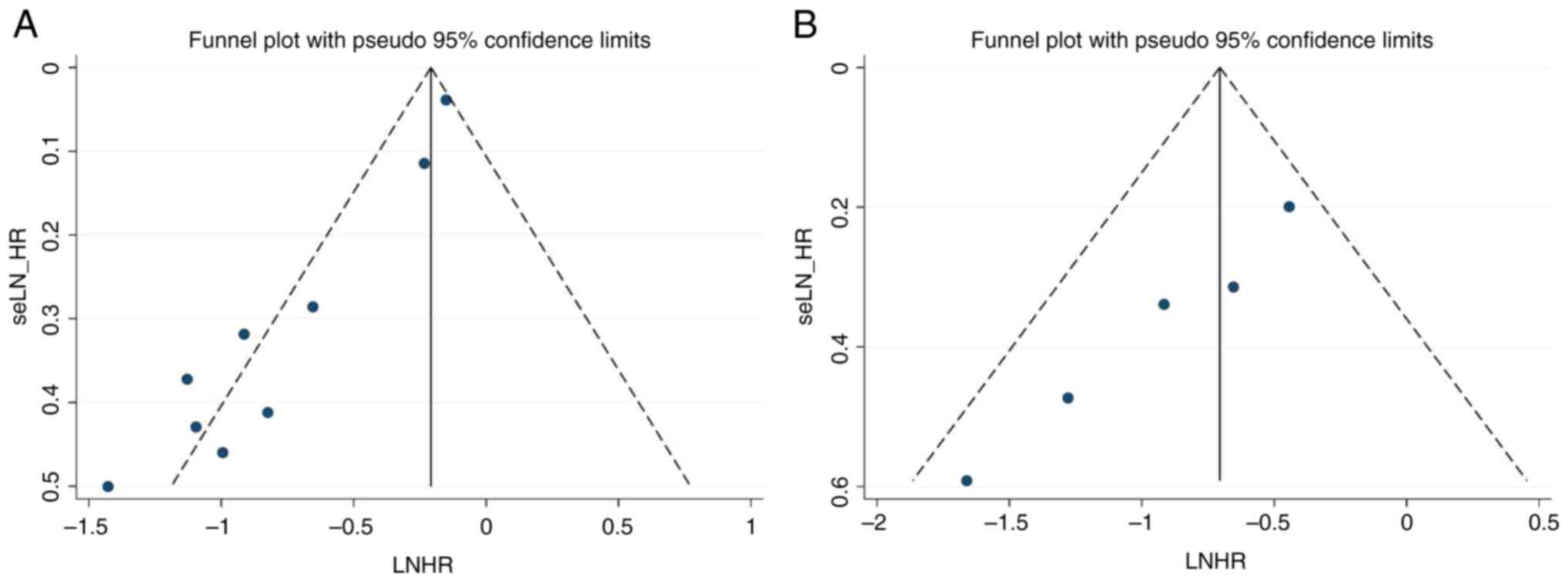
Publication bias
Generated funnel plots were asymmetrical, and
Egger's test yielded evidence of significant publication bias
(P<0.0001 and P=0.002) (Fig. 5).
This suggests that these results are subject to some degree of
publication bias. This may be attributable to the choice to only
include English language studies, contributing to language bias. In
addition, negative research results often go unpublished,
contributing to further bias in the literature. These findings
suggest that the present meta-analysis results are not stable,
underscoring the need for further research focused on this
experimental topic.
Discussion
NAC has emerged as the standard approach to TNBC
management, with most patients receiving a combination of
anthracyclines, alkylates and taxanes while undergoing NAC
treatment (20). The administration
of these cytotoxic drugs can modulate lymphocyte infiltration of
the TME in a manner that induces a robust antitumor immune response
(21,22). Adaptive immunity can also be
triggered in response to tumor-specific antigens, promoting the
infiltration of lymphocytes engaged in immune surveillance
whereupon they can destroy target tumor cells (23). TIL infiltration can impact the
effects of cytotoxic drugs on tumor cells, while also offering
value as a biomarker associated with treatment outcomes and the
overall prognosis of patients with cancer, providing guidance for
treatment planning efforts. A number of studies to date have
confirmed that TIL infiltration is significantly correlated with
TNBC patient prognostic outcomes and treatment responses (24–26).
While numerous studies have explored the association between TIL
infiltration and pCR following NAC, there is also some evidence
that a subset of patients who fail to achieve pCR can also achieve
better outcomes (19,27).
Several recent studies have documented an
association between TILs present in RT tissue following the
prognosis of patients with NAC and TNBC (28,29).
While this suggests the existence of a relationship between TILs
and patient survival, systematic high-quality studies focused on
this topic are lacking at present. As such, a meta-analysis was
conducted in the present study as a means of systematically
reviewing published studies to explore the prognostic implications
of RT TIL infiltration levels. Owing to limitations with respect to
the outcome indicators used in different studies, RFS/MFS/EFS/DRFI
were utilized as short-term endpoints. Pooled analyses indicated
that patients exhibiting higher levels of TIL infiltration
experienced better postoperative RFS/MFS/EFS/DRFI compared with
patients with lower levels of such infiltration (HR=0.52; 95%
CI=0.39–0.69). OS/BCSS were additionally analyzed as long-term
outcomes, revealing that those patients with TNBC with higher RT
TIL infiltration levels following NAC exhibited a significantly
lower risk of death compared with patients with lower levels of TIL
infiltration (HR=0.49; 95% CI=0.38–0.65).
Different TIL subtypes play specific roles in the
context of antitumor immunity, engaging in cross-regulatory
interactions that can shape immune response induction (30). The presence of specific TIL subtypes
in RT tissue can contribute to a better or worse patient prognosis,
and high levels of infiltration for certain TILs may thus provide a
robust means of detecting patients in particular prognostic
subgroups (31,32). CD4+ and CD8+ T
cells are the primary TIL subtypes (31). CD4+ T cells primarily act
as helper T cells that are reliant on antigen-presenting cells to
support the activation of other immune cell types following the
recognition of soluble tumor-derived antigens, ultimately exerting
antitumor roles (33). Through this
activity, CD4+ T cells have the potential to increase
the numbers of other TILs in the TME or to enhance their
functionality (33). Cytolytic
CD8+ T cells can directly destroy target tumor cells,
making them particularly important mediators of antitumor immunity
(34). Greater levels of
CD4+ and CD8+ T cell infiltration in the TME
have been linked to higher pCR rates and better prognostic outcomes
in patients with TNBC (33,35,36).
Accordingly, subgroup analyses were conducted in the present study
based on the TIL subtypes included in the analyzed studies. With
respect to short-term outcomes, high levels of TIL or TIL subtype
(CD4+ or CD8+) infiltration were associated
with a better prognosis (HR=0.35, 95% CI=0.20–0.59; HR=0.49, 95%
CI=0.33–0.71), suggesting a higher risk of metastasis and disease
recurrence in individuals with low levels of TIL infiltration.
Similar findings were also observed with respect to long-term
outcome indicators (HR=0.33, 95% CI=0.19–0.59; HR=0.55, 95% CI,
0.41–0.76).
These meta-analysis results highlight a clear
relationship between RT TIL infiltration following prognosis of
patients with NAC and TNBC. Residual cancer burden (RCB) has also
been used to predict the outcomes of patients with TNBC based on RT
levels following NAC (37),
suggesting that combining analyses of RCB and RT TIL infiltration
profiles may improve prognostic assessment efforts. Indeed, Luen
et al (19) observed a
significant interactive effect of TIL infiltration and RCB on
prognosis, while Asano et al (38) determined that the combined
assessment of TILs and RCB can predict post-NAC breast cancer
recurrence more sensitively compared with TILs alone. Given that
TNBC tumors exhibit unique immunological characteristics that can
better sensitize these tumors to immunotherapeutic treatment, there
is growing interest in the post-NAC immunotherapy-based management
of this cancer type (39). As a
result, TIL profiles represent increasingly important targets that
can be used to stratify patients in post-NAC immunotherapy clinical
trials. For example, results from the KEYNOTE-086 study highlighted
the fact that sTILs can predict pembrolizumab efficacy when used as
a first-line treatment for metastatic TNBC (40). The KEYNOTE-173 study revealed that
there was a significant association between high levels of TILs and
improved pathological complete response or objective response rate
in patients with TNBC who underwent treatment with pembrolizumab
(41). These findings were similar
to the results of the KEYNOTE-086 study. TIL immune checkpoint
receptor expression has been linked to better immunotherapy
responses (42,43). Low levels of TIL infiltration may be
indicative of the need for chemotherapeutic treatment using
cytotoxic drugs and of the potential for the addition of PD-1/PD-L1
therapy. Higher TIL infiltration and lower disease burden, by
contrast, may suggest that single-agent immunotherapy represents a
viable treatment strategy (44).
The present study is subject to certain limitations.
For one, the included studies employed different methods when
detecting TILs/TIL subtypes and when selecting the threshold values
used to define high levels of TIL infiltration. This, coupled with
the inconsistent outcome indicators across studies, is likely to
have impacted the overall accuracy of these results. In addition,
the pre-NAC TIL infiltration profiles in the patients included in
these studies were not evaluated, and the prognostic relevance of
dynamic changes in TIL infiltration was thus not assessed,
highlighting a promising avenue for future research. Lastly, owing
to the limited number of relevant studies published to date, the
overall sample size in this meta-analysis was somewhat small,
potentially contributing to some degree of bias that may have
impacted study results. Additional large-scale studies will be
essential to explore the correlation between post-NAC TILs in RT
tissue and TNBC patient prognostic outcomes in order to provide a
comprehensive and evidence-based approach that can better guide
clinical decision-making.
The present meta-analysis results suggest that TIL
infiltration in RT tissue following NAC is a valuable prognostic
indicator associated with TNBC patient outcomes. Specifically,
higher levels of TIL infiltration were found to be associated with
a lower risk of disease recurrence, metastasis and death such that
patients exhibiting higher levels of RT TIL infiltration tended to
exhibit a better prognosis compared with patients with lower levels
of RT TIL infiltration. Analyzing levels of total TIL or TIL
subtype (CD4+ or CD8+) infiltration in RT
tissue following NAC can thus improve the ability of clinicians to
predict the efficacy of further adjuvant chemotherapy
administration and the prognosis of patients with TNBC.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
BC and ZZ contributed to the conception and design
of the study. CW and XL prepared the materials, collected the data
and performed the analysis. ZZ drafted the manuscript. BC and ZZ
confirm the authenticity of all the raw data. All authors revised
the manuscript. All authors have read and approved the final
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Authors' information
ORCID: Dr Ziran Zhang,
orcid.org/0000-0002-7835-8788.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Garrido-Castro AC, Lin NU and Polyak K:
Insights into molecular classifications of triple-negative breast
cancer: Improving patient selection for treatment. Cancer Discov.
9:176–198. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Diana A, Carlino F, Franzese E,
Oikonomidou O, Criscitiello C, De Vita F, Ciardiello F and Orditura
M: Early triple negative breast cancer: Conventional treatment and
emerging therapeutic landscapes. Cancers (Basel). 12:8192020.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Won KA and Spruck C: Triple-negative
breast cancer therapy: Current and future perspectives (Review).
Int J Oncol. 57:1245–1261. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Gupta GK, Collier AL, Lee D, Hoefer RA,
Zheleva V, Siewertsz van Reesema LL, Tang-Tan AM, Guye ML, Chang
DZ, Winston JS, et al: Perspectives on triple-negative breast
cancer: Current treatment strategies, unmet needs, and potential
targets for future therapies. Cancers (Basel). 12:23922020.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Masuda N, Lee SJ, Ohtani S, Im YH, Lee ES,
Yokota I, Kuroi K, Im SA, Park BW, Kim SB, et al: Adjuvant
capecitabine for breast cancer after preoperative chemotherapy. N
Engl J Med. 376:2147–2159. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Cortazar P, Zhang L, Untch M, Mehta K,
Costantino JP, Wolmark N, Bonnefoi H, Cameron D, Gianni L,
Valagussa P, et al: Pathological complete response and long-term
clinical benefit in breast cancer: The CTNeoBC pooled analysis.
Lancet. 384:164–172. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Liedtke C, Mazouni C, Hess KR, André F,
Tordai A, Mejia JA, Symmans WF, Gonzalez-Angulo AM, Hennessy B,
Green M, et al: Response to neoadjuvant therapy and long-term
survival in patients with triple-negative breast cancer. J Clin
Oncol. 26:1275–1281. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Isakoff SJ: Triple-negative breast cancer:
Role of specific chemotherapy agents. Cancer J. 16:53–61. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Symmans WF, Wei C, Gould R, Yu X, Zhang Y,
Liu M, Walls A, Bousamra A, Ramineni M, Sinn B, et al: Long-Term
prognostic risk after neoadjuvant chemotherapy associated with
residual cancer burden and breast cancer subtype. J Clin Oncol.
35:1049–1060. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Apetoh L, Ghiringhelli F, Tesniere A,
Criollo A, Ortiz C, Lidereau R, Mariette C, Chaput N, Mira JP,
Delaloge S, et al: The interaction between HMGB1 and TLR4 dictates
the outcome of anticancer chemotherapy and radiotherapy. Immunol
Rev. 220:47–59. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Zitvogel L and Kroemer G: The immune
response against dying tumor cells: Avoid disaster, achieve cure.
Cell Death Differ. 15:1–2. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
García-Teijido P, Cabal ML, Fernández IP
and Pérez YF: Tumor-Infiltrating lymphocytes in triple negative
breast cancer: The future of immune targeting. Clin Med Insights
Oncol. 10 (Suppl 1):S31–S39. 2016.PubMed/NCBI
|
|
13
|
Ravelli A, Roviello G, Cretella D,
Cavazzoni A, Biondi A, Cappelletti MR, Zanotti L, Ferrero G, Ungari
M, Zanconati F, et al: Tumor-infiltrating lymphocytes and breast
cancer: Beyond the prognostic and predictive utility. Tumour Biol.
39:10104283176950232017. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Dieci MV, Radosevic-Robin N, Fineberg S,
van den Eynden G, Ternes N, Penault-Llorca F, Pruneri G, D'Alfonso
TM, Demaria S, Castaneda C, et al: Update on tumor-infiltrating
lymphocytes (TILs) in breast cancer, including recommendations to
assess TILs in residual disease after neoadjuvant therapy and in
carcinoma in situ: A report of the International Immuno-Oncology
Biomarker Working Group on breast cancer. Semin Cancer Biol. 52((Pt
2)): 16–25. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gao G, Wang Z, Qu X and Zhang Z:
Prognostic value of tumor-infiltrating lymphocytes in patients with
triple-negative breast cancer: A systematic review and
meta-analysis. BMC Cancer. 20:1792020. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Demaria S, Volm MD, Shapiro RL, Yee HT,
Oratz R, Formenti SC, Muggia F and Symmans WF: Development of
tumor-infiltrating lymphocytes in breast cancer after neoadjuvant
paclitaxel chemotherapy. Clin Cancer Res. 7:3025–3030.
2001.PubMed/NCBI
|
|
17
|
Wells GA, Shea B, O'Connell D, Peterson J,
Welch V, Losos M and Tugwell P: The Newcastle-Ottawa Scale (NOS)
for Assessing the Quality of Non-Randomised Studies in
Meta-Analyses. Symposium on Systematic Reviews: Beyond the Basics.
2014.
|
|
18
|
DerSimonian R and Laird N: Meta-analysis
in clinical trials revisited. Contemp Clin Trials. 45((Pt A)):
139–145. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Luen SJ, Salgado R, Dieci MV, Vingiani A,
Curigliano G, Gould RE, Castaneda C, D'Alfonso T, Sanchez J, Cheng
E, et al: Prognostic implications of residual disease
tumor-infiltrating lymphocytes and residual cancer burden in
triple-negative breast cancer patients after neoadjuvant
chemotherapy. Ann Oncol. 30:236–242. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Park JH, Ahn JH and Kim SB: How shall we
treat early triple-negative breast cancer (TNBC): From the current
standard to upcoming immuno-molecular strategies. ESMO Open. 3
(Suppl 1):e0003572018. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Andre F, Dieci MV, Dubsky P, Sotiriou C,
Curigliano G, Denkert C and Loi S: Molecular pathways: Involvement
of immune pathways in the therapeutic response and outcome in
breast cancer. Clin Cancer Res. 19:28–33. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ladoire S, Mignot G, Dabakuyo S, Arnould
L, Apetoh L, Rébé C, Coudert B, Martin F, Bizollon MH, Vanoli A, et
al: In situ immune response after neoadjuvant chemotherapy for
breast cancer predicts survival. J Pathol. 224:389–400. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Lee H, Lee M, Seo JH, Gong G and Lee HJ:
Changes in tumor-infiltrating lymphocytes after neoadjuvant
chemotherapy and clinical significance in triple negative breast
cancer. Anticancer Res. 40:1883–1890. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Denkert C, von Minckwitz G, Darb-Esfahani
S, Lederer B, Heppner BI, Weber KE, Budczies J, Huober J, Klauschen
F, Furlanetto J, et al: Tumour-infiltrating lymphocytes and
prognosis in different subtypes of breast cancer: A pooled analysis
of 3771 patients treated with neoadjuvant therapy. Lancet Oncol.
19:40–50. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Pruneri G, Gray KP, Vingiani A, Viale G,
Curigliano G, Criscitiello C, Láng I, Ruhstaller T, Gianni L,
Goldhirsch A, et al: Tumor-infiltrating lymphocytes (TILs) are a
powerful prognostic marker in patients with triple-negative breast
cancer enrolled in the IBCSG phase III randomized clinical trial
22–00. Breast Cancer Res Treat. 158:323–331. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Pruneri G, Vingiani A, Bagnardi V,
Rotmensz N, De Rose A, Palazzo A, Colleoni AM, Goldhirsch A and
Viale G: Clinical validity of tumor-infiltrating lymphocytes
analysis in patients with triple-negative breast cancer. Ann Oncol.
27:249–256. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Dieci MV, Criscitiello C, Goubar A, Viale
G, Conte P, Guarneri V, Ficarra G, Mathieu MC, Delaloge S,
Curigliano G and Andre F: Prognostic value of tumor-infiltrating
lymphocytes on residual disease after primary chemotherapy for
triple-negative breast cancer: A retrospective multicenter study.
Ann Oncol. 25:611–618. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Lejeune M, Reverté L, Sauras E, Gallardo
N, Bosch R, Roso A, Petit A, Peg V, Riu F, García-Fontgivell J, et
al: Prognostic implications of the residual tumor microenvironment
after neoadjuvant chemotherapy in triple-negative breast cancer
patients without pathological complete response. Cancers (Basel).
15:5972023. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Wang Y, Zong B, Yu Y, Wang Y, Tang Z, Chen
R, Huang M and Liu S: Ki67 index changes and tumor-infiltrating
lymphocyte levels impact the prognosis of triple-negative breast
cancer patients with residual disease after neoadjuvant
chemotherapy. Front Oncol. 11:6686102021. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Ghajar CM: On leukocytes in mammary
development and cancer. Cold Spring Harb Perspect Biol.
4:a0132762012. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
da Silva JL, de Albuquerque LZ, Rodrigues
FR, de Mesquita GG, Fernandes PV, Thuler LCS and de Melo AC:
Prognostic influence of residual tumor-infiltrating lymphocyte
subtype after neoadjuvant chemotherapy in triple-negative breast
cancer. Front Oncol. 11:6367162021. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Pinard C, Debled M, Ben Rejeb H, Velasco
V, Tunon de Lara C, Hoppe S, Richard E, Brouste V, Bonnefoi H and
MacGrogan G: Residual cancer burden index and tumor-infiltrating
lymphocyte subtypes in triple-negative breast cancer after
neoadjuvant chemotherapy. Breast Cancer Res Treat. 179:11–23. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Gu-Trantien C, Loi S, Garaud S, Equeter C,
Libin M, de Wind A, Ravoet M, Le Buanec H, Sibille C,
Manfouo-Foutsop G, et al: CD4+ follicular helper T cell
infiltration predicts breast cancer survival. J Clin Invest.
123:2873–2892. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Lin KR, Pang DM, Jin YB, Hu Q, Pan YM, Cui
JH, Chen XP, Lin YX, Mao XF, Duan HB and Luo W: Circulating
CD8+ T-cell repertoires reveal the biological
characteristics of tumors and clinical responses to chemotherapy in
breast cancer patients. Cancer Immunol Immunother. 67:1743–1752.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Matsumoto H, Thike AA, Li H, Yeong J, Koo
SL, Dent RA, Tan PH and Iqbal J: Increased CD4 and CD8-positive T
cell infiltrate signifies good prognosis in a subset of
triple-negative breast cancer. Breast Cancer Res Treat.
156:237–247. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Miyashita M, Sasano H, Tamaki K, Hirakawa
H, Takahashi Y, Nakagawa S, Watanabe G, Tada H, Suzuki A, Ohuchi N
and Ishida T: Prognostic significance of tumor-infiltrating CD8+
and FOXP3+ lymphocytes in residual tumors and alterations in these
parameters after neoadjuvant chemotherapy in triple-negative breast
cancer: A retrospective multicenter study. Breast Cancer Res.
17:1242015. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Sheri A, Smith IE, Johnston SR, A'Hern R,
Nerurkar A, Jones RL, Hills M, Detre S, Pinder SE, Symmans WF and
Dowsett M: Residual proliferative cancer burden to predict
long-term outcome following neoadjuvant chemotherapy. Ann Oncol.
26:75–80. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Asano Y, Kashiwagi S, Goto W, Takada K,
Takahashi K, Hatano T, Noda S, Takashima T, Onoda N, Tomita S, et
al: Prediction of survival after neoadjuvant chemotherapy for
breast cancer by evaluation of tumor-infiltrating lymphocytes and
residual cancer burden. BMC Cancer. 17:8882017. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Cortes J, Cescon DW, Rugo HS, Nowecki Z,
Im SA, Yusof MM, Gallardo C, Lipatov O, Barrios CH, Holgado E, et
al: Pembrolizumab plus chemotherapy versus placebo plus
chemotherapy for previously untreated locally recurrent inoperable
or metastatic triple-negative breast cancer (KEYNOTE-355): A
randomised, placebo-controlled, double-blind, phase 3 clinical
trial. Lancet. 396:1817–1828. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Loi S, Adams S, Schmid P, Cortés J, Cescon
DW, Winer EP, Toppmeyer DL, Rugo HS, De Laurentiis M, Nanda R, et
al: Relationship between tumor infiltrating lymphocyte (TIL) levels
and response to pembrolizumab (pembro) in metastatic
triple-negative breast cancer (mTNBC): Results from KEYNOTE-086.
Ann Oncol. 28:V6082017. View Article : Google Scholar
|
|
41
|
Schmid P, Salgado R, Park YH,
Muñoz-Couselo E, Kim SB, Sohn J, Im SA, Foukakis T, Kuemmel S, Dent
R, et al: Pembrolizumab plus chemotherapy as neoadjuvant treatment
of high-risk, early-stage triple-negative breast cancer: Results
from the phase 1b open-label, multicohort KEYNOTE-173 study. Ann
Oncol. 31:569–581. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Ellis PM, Vella ET and Ung YC: Immune
checkpoint inhibitors for patients with advanced non-small-cell
lung cancer: A systematic review. Clin Lung Cancer. 18:444–459.e1.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Kluger HM, Zito CR, Turcu G, Baine MK,
Zhang H, Adeniran A, Sznol M, Rimm DL, Kluger Y, Chen L, et al:
PD-L1 studies across tumor types, its differential expression and
predictive value in patients treated with immune checkpoint
inhibitors. Clin Cancer Res. 23:4270–4279. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Blackley EF and Loi S: Targeting immune
pathways in breast cancer: Review of the prognostic utility of TILs
in early stage triple negative breast cancer (TNBC). Breast. 48
(Suppl 1):S44–S48. 2019. View Article : Google Scholar : PubMed/NCBI
|