Introduction
Intrahepatic cholangiocarcinoma (iCCA) is an
adenocarcinoma arising from cholangiocytes in bile ducts proximal
to second-order branches within the liver parenchyma, with poor
outcomes owing to its generally aggressive nature, late-stage
diagnosis and lack of treatment options for advanced disease
(1,2). iCCA can be hidden and misclassified as
carcinoma of unknown primary (CUP) due to difficulty in
distinguishing it pathologically from metastatic adenocarcinoma
arising from extrahepatic primary tumors. This is especially the
case for tumors originating in the foregut, such as the pancreas,
esophagus and stomach due to the lack of iCCA-specific
immunohistochemical biomarkers (3,4).
Numerous cancers previously classified as adenocarcinomas of
unknown primary may be iCCA (5).
Novel diagnostic modalities, such as CT, MRI imaging and
immunohistochemistry, have improved clinical distinction between
iCCA and CUP (6). These factors may
have contributed to the increasing incidence of iCCA worldwide over
the past three decades. iCCA is the second most common primary
liver cancer after hepatocellular carcinoma, accounting for 10–15%
of cases of primary liver cancer (5,7).
However, the diagnosis of iCCA remains challenging, and a
multidisciplinary approach may be required. CUP is only considered
if localized lymph node metastases are detected (8). To the best of our knowledge, iCCA,
which initially presents as CUP with localized lymph node
metastases, has rarely been reported (9). The present study reports a patient
diagnosed with iCCA as CUP and the clinical course from the time of
radical lymphadenectomy in the hepatoduodenal ligament and
diagnosis of CUP to the detection of iCCA after long-term
surveillance.
Case report
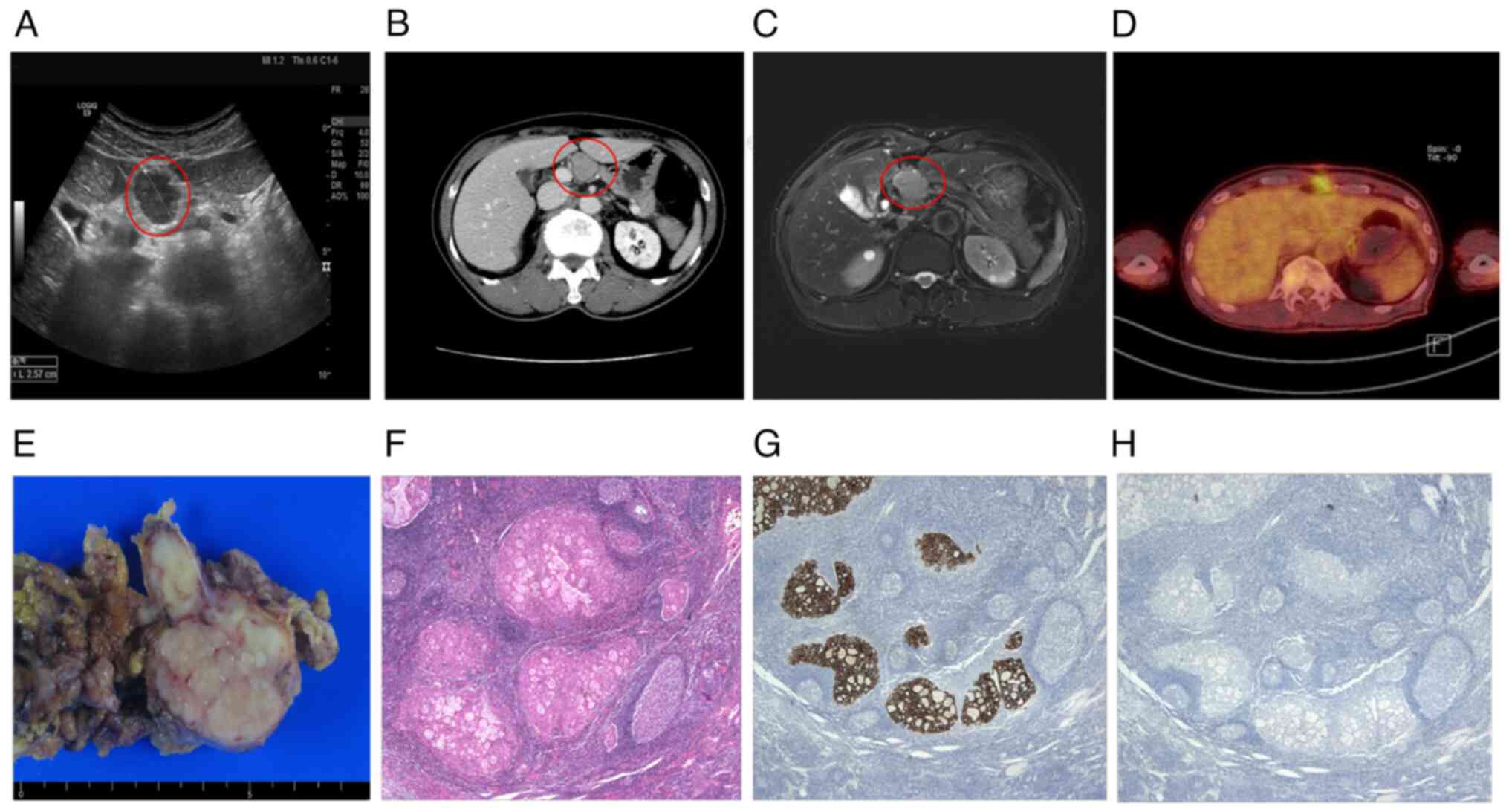
A 69-year-old male patient with a history of
hypertension presented with an incidentally discovered lymph node
measuring 2.7 cm within the hepatoduodenal ligament, suggesting a
pathological lymph node, upon serial abdominal ultrasonography (US;
Fig. 1A) evaluation due to chronic
kidney disease at Veterans Health Service Medical Center (Seoul,
Korea) in September 2018. Tumor marker tests were performed; cancer
antigen 19–9 (CA 19-9) was elevated to 1,199 U/ml (normal range,
0.0–37.0 U/ml), whereas carcinoembryonic antigen (CEA, 3.6 ng/ml;
normal range, 0.0–5.0 ng/ml), prostate-specific antigen (PSA, 2.8
mg/ml; normal range, 0.0–4.0 mg/ml), α-fetoprotein (AFP, 4.2 ng/ml;
normal range, 0.0–7.0 ng/ml) and β-human chorionic gonadotropin
(0.2 mIU/ml; normal range, <1.0 mIU/ml) were within normal
ranges. Abdominal contrast-enhanced computed tomography (CT;
Fig. 1B) and magnetic resonance
imaging (MRI; Fig. 1C) revealed
enlarged hepatoduodenal ligament lymph nodes ~2.7 and 1.5 cm in
diameter, respectively, with no detectable liver mass. In October
2018, the patient underwent an exploratory laparotomy and
lymphadenectomy for diagnostic and therapeutic purposes,
respectively. Intraoperatively, no liver mass was identified,
except for enlarged lymph nodes visible to the naked eye. The cut
surfaces of the excised pathological lymph nodes had a pale yellow
and granular appearance (Fig. 1E).
Four-micrometer thick sections were obtained from the
formalin-fixed and paraffin-embedded (FFPE) tissue block and
stained with hematoxylin and eosin. Under the light microscope,
histological evaluation was performed. Histopathological
examination revealed poorly differentiated metastatic
adenocarcinoma in two of the 22 lymph nodes (Fig. 1F). Immunohistochemical staining for
cytokeratin (CK) 7, CK20, thyroid transcription factor-1 (TTF-1),
CDX-2, p53, alpha-methylacyl-CoA racemase (AMACR), prostate
specific antigen (PSA), and S100 protein were performed on the
4-micrometer FFPE tissue block of the fresh specimen. The slides
were stained on the Ventana BenchMark XT platform (Ventana Medical
Systems, Tucson, AZ) and on a Leica Bond Max instrument (Leica
Biosystems, Chicago, IL) according to the standard protocol
(Table I). All slides were
evaluated under the light microscope. Immunohistochemistry (IHC)
results showed cytokeratin (CK) 7(+; Fig. 1G), CK20 (−; Fig. 1H), thyroid transcription factor 1
(TTF-1) (−), CDX-2 (−), periodic acid-Schiff (PAS) (+),
diastase-PAS (−), p53 (+), SMAD-3 (+), α-methylacyl-CoA racemase
(−), PSA (−) and S100 protein (−; data not shown). These results
suggested a potential origin from the upper gastrointestinal tract
and pancreaticobiliary system. Postoperatively, positron emission
tomography/CT (PET/CT) was performed; however, the primary site,
particularly a hepatopancreatobiliary origin, could not be
identified (Fig. 1D). A diagnosis
of poorly differentiated CUP was confirmed based on clinical,
radiological and histopathological characteristics following tumor
board discussion. Following an in-depth discussion with the
patient, regular investigations of the tumor marker CA 19-9 and
follow-up CT scans were performed without further anticancer
therapy, considering patient age and underlying chronic kidney
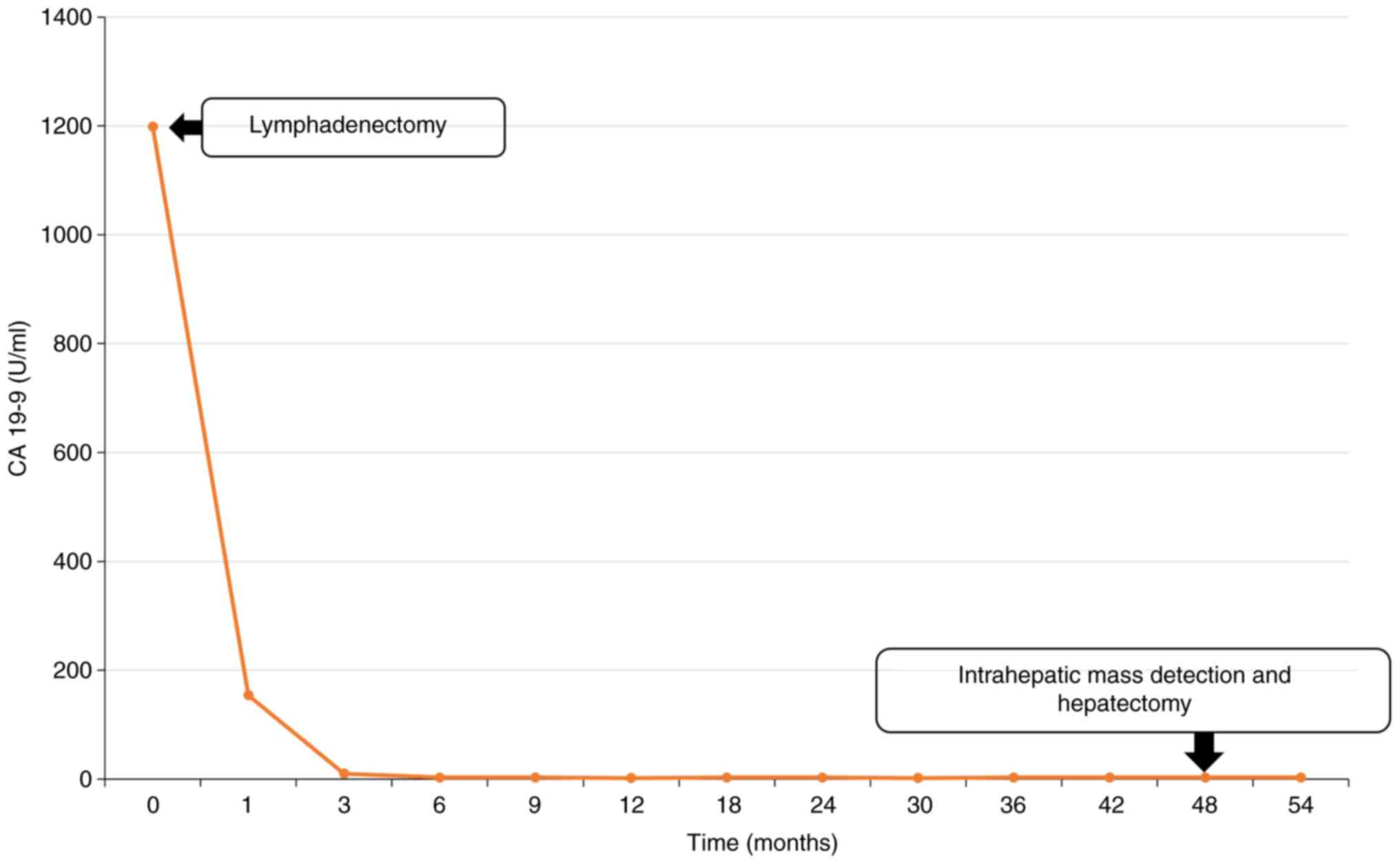
disease. One month after the lymphadenectomy, the CA 19-9 levels
decreased to 154.04 U/ml and returned to normal range after 3
months (Fig. 2). During
surveillance every 6 months, the CA 19-9 levels remained within the
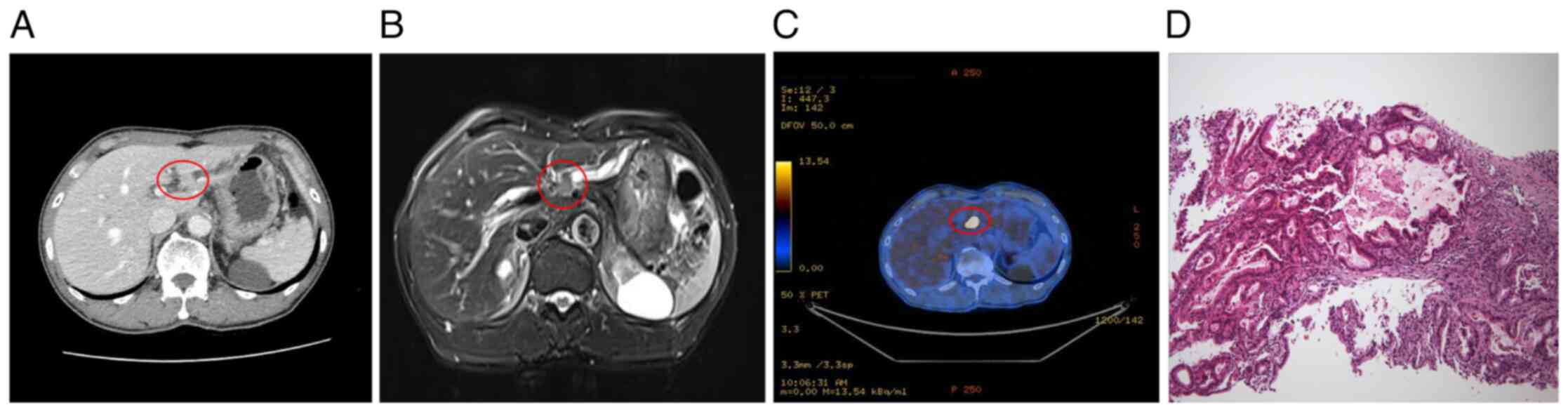
normal range. In October 2022, a CT scan displayed a faintly
enhancing intraductal polypoid mass ~1.1 cm in diameter with
localized ductal dilatation in liver segment 3 (Fig. 3A), which was also confirmed in the
same area on MRI (Fig. 3B) and
PET/CT (Fig. 3C). US-guided
percutaneous needle biopsy was performed for pathological diagnosis
and moderately differentiated adenocarcinoma was confirmed
(Fig. 3D). The patient refused a
second surgical treatment because of general weakness caused by
Coronavirus disease 2019 infection. As an alternative treatment,
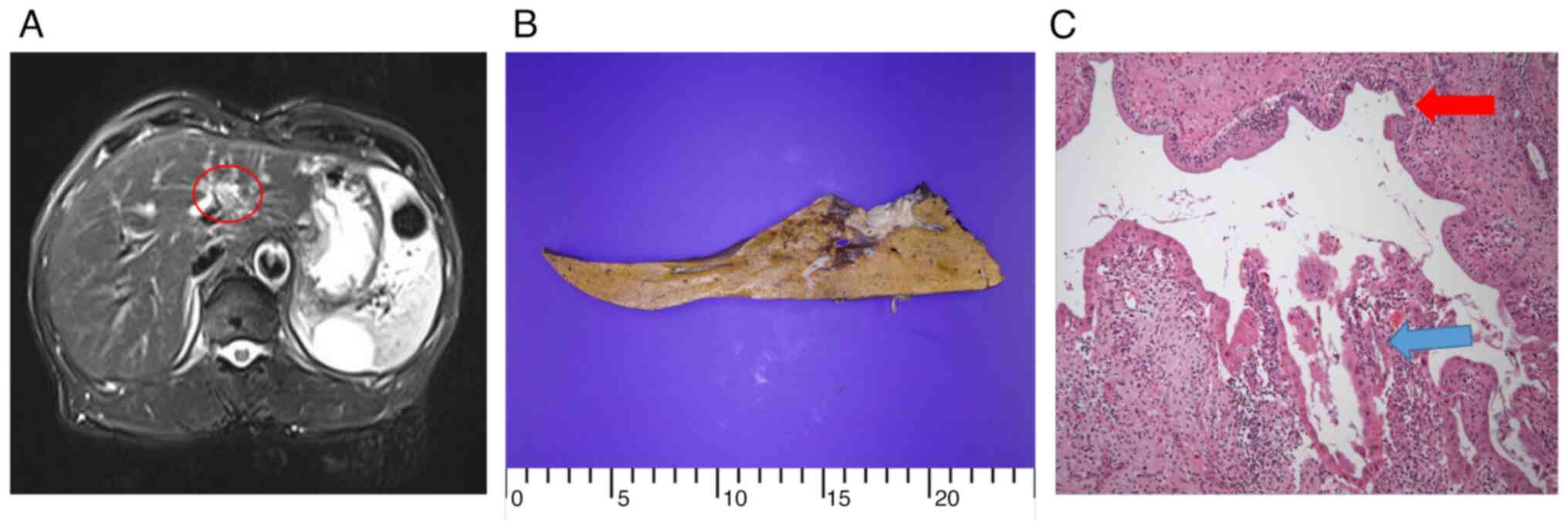
stereotactic body radiation therapy (60 Gy in four fractions) was
initiated, which showed a partial response (Fig. 4A). Gradually, performance status
improved and the patient consented to surgical treatment and
underwent a left lobectomy of the liver in February 2023. The
resected liver specimen revealed a cavitary mass and periductal
fibrosis with multifocal hemorrhage (Fig. 4B). Histopathological examination of
the surgical specimen demonstrated that fibrosis and mucin
accumulation were prevalent and scattered cancer cells were found
focally in the resected liver specimen because of the effect of
radiotherapy (Fig. 4C) and were too
small for further assessment of immunohistochemical markers. Based
on these clinical, radiological and histopathological findings, the
patient was diagnosed with iCCA, which was accompanied by regional
lymph node metastases. As of October 2023, the patient is still
alive and undergoing regular surveillance every 3 months without
any evidence of local recurrence or metastasis following
hepatectomy.
 | Table I.Antibodies for immunohistochemical
staining. |
Table I.
Antibodies for immunohistochemical
staining.
| Antibody | Clone | Dilution | Result | Supplier | Catalogue number |
|---|
| CK7 | OV-TL 12/30 | 1:600 | Positive | Novocastra | M7018 |
| CK20 | KS20-8 | 1:200 | Negative | Novocastra | M7019 |
| TTF-1 | 8G7G3/1 | 1:400 | Negative | Labvision | M3575 |
| CDX-2 | EPR2764Y | RTU | Negative | Ventana | 760-4380 |
| p53 | DO-7 | 1:400 | Positive | Cellmarque | 800-2912 |
| AMACR | 13H4 | 1:200 | Negative | Dako | M3616 |
| PSA | Polyclonal | RTU | Negative | Ventana | 760-2506 |
| S100 protein | Polyclonal | RTU | Negative | Ventana | 760-2523 |
Discussion
The present patient was initially diagnosed with CUP
with hepatoduodenal ligament lymph node metastases. During 48-month
follow-up after radical lymphadenectomy, a delineated intrahepatic
mass was discovered and iCCA was confirmed histopathologically
following hepatectomy. The present case report presents a latent
diagnosis of iCCA with a clear pathology, initially diagnosed as
CUP, and a long-term clinical course without additional anticancer
therapy.
iCCA initially diagnosed as CUP has been diagnosed
by autopsy: Oda et al (9)
reported a 57-year-old male with systemic lymph node metastases.
Imaging revealed no primary cancer. Autopsy indicated occult
intrahepatic cholangiocarcinoma after death from a liver abscess.
It was suggested that heartbeat can interfere with diagnostic
imaging and that it may be difficult to detect a solid tumor in the
subphrenic area of the lateral segment of the liver. There are two
patterns of lymph node metastases from the left lobe: Metastasis to
lymph nodes in the hepatoduodenal ligament (regional lymph nodes)
and around the cardiac portion of the stomach or along the common
hepatic artery (distant lymph nodes), termed skip metastasis
(10). Conway et al
(4) reported iCCA in 24 (10.5%) of
228 CUP cases. The majority of these cases had radiographic
satellite liver nodules and half of the patients showed vascular
encasement. Cases of liver capsular retraction and intrahepatic
bile duct dilatation have also been reported (4,11).
CUPs have the potential to be diagnosed as iCCA; however, the lack
of specific immunohistochemical biomarkers for iCCA diagnosis and
rarity of CUP contribute to its misdiagnosis.
The most common sites of lymph node metastases in
iCCA are pericholedochal, periportal and common hepatic artery
lymph nodes (12). Regional lymph
node metastases involving the hilar, periduodenal and
peripancreatic nodes are considered N1 diseases with a IIIB TNM
stage according to the American Joint Committee on Cancer eighth
edition (13). The present patient
was a representative case of iCCA of the left hemiliver with
regional hepatoduodenal lymph node metastasis. In Japan, a study of
70 patients with iCCA reported that a hepatoduodenal lymph node may
be a sentinel lymph node of iCCA (14). Lymph node metastasis is a key
prognostic factor of iCCA. This occurs in up to 33% of early-stage
tumors and typically precludes surgery (15). Lymph node metastases following iCCA
resection are associated with a median overall survival (OS) of
15–22 months, which is less than half that of patients with
node-negative disease (16–18). Martin et al (12) reviewed the National Cancer Database
and evaluated patients with clinically node-positive iCCA treated
with either resection- or chemotherapy-alone, or a combination of
resection and chemotherapy; combined resection and chemotherapy is
the optimal therapeutic approach with a median OS of 22.5 months
vs. 11.9 months for chemotherapy-alone and 12.4 months for
resection-alone. In addition, Jolissaint et al (19) reported that resection or hepatic
arterial infusion chemotherapy significantly increases OS compared
with systemic chemotherapy-alone in lymph node-positive disease.
Therefore, resection is the first treatment option for patients
with iCCA with lymph node metastasis.
Intrahepatic cholangiocarcinoma has three main
growth patterns: Mass-forming, periductal-infiltrating and
intraductal-growing. The mass-forming type is the most common and
is characterized by intraparenchymal mass with distinct borders.
The periductal-infiltrating type is characterized by tumor
infiltration along the bile duct, often causing dilatation of the
peripheral bile duct. Certain studies have shown worse survival
after resection of the periductal-infiltrating type than the
mass-forming type, whereas other reports have shown no difference
in survival (20–22). The intraductal growth type is a
slow-growing papillary tumor with a favorable prognosis compared
with the other two types (11,23).
Although the present patient was expected to have a poor prognosis
due to early lymph node metastases and did not receive systemic
chemotherapy, it was hypothesized that he had a relatively good
prognosis with no distant metastases due to having the slow-growing
intraductal growth type of the iCCA. iCCA is further classified
into two main histological subtypes based on the level or size of
the affected duct. Small bile duct iCCAs present as small tubular
or acinar adenocarcinomas with nodular growth invading liver
parenchyma, with no or minimal mucin production. Large bile duct
iCCAs arise in large intrahepatic bile ducts and comprise
mucin-producing columnar tumor cells arranged in a large duct or
papillary architecture (1). In the
present case, fibrosis and mucin accumulation were prevalent and
scattered cancer cells were found focally in the resected liver
specimen following radiotherapy. Owing to the effect of radiation,
it was difficult to distinguish the three types of growth in the
resected liver specimens. However, based on the US-guided liver
biopsy specimen, the present case was considered to be of the
intraductal growth type iCCA of the large duct. Serum CA 19-9 and
CEA levels have been suggested to be independent risk factors for
prognosis of cholangiocarcinomas, including iCCA (23).
The positivity rates for CA 19-9 (>37 U/ml) and
CEA (>5 ng/ml) are 54.1 and 33.6%, respectively, in Japanese
patients with iCCA (24). According
to the clinical practice guidelines for iCCA of the Liver Cancer
Study Group of Japan (LCSGJ), CA 19-9 and CEA are recommended as
tumor markers for early detection and diagnosis of iCCA (25). In the present case, CA 19-9 was
elevated at the time of the initial detection of lymphadenopathy
and within the normal range at the time of the latent detection of
the intrahepatic mass. Therefore, monitoring may be possible using
imaging modalities, such as abdominal US, CT, and MRI, as well as
tumor markers. Although tumor mutation profiling for treatment
decisions for iCCA has not yet been established, patients with
lymph node-positive iCCA with TP53 or KRAS mutation or
cyclin-dependent kinase inhibitor 2A/B deletion have a worse
prognosis than wild-type. Conversely, patients with isocitrate
dehydrogenase 1/2 mutations exhibit no difference in survival
compared with wild-type patients (19). Further analysis of tumor genetic
alterations will provide information for assessing prognosis and
selecting treatment options.
In conclusion, the present study reports a rare case
of a definitively confirmed iCCA after a long-term follow-up of a
patient who underwent resection for an incidentally detected
lymphadenopathy in the hepatoduodenal ligament. Furthermore, it was
suggested that surgical resection be performed when regional
intra-abdominal lymphadenopathy is detected in the perihepatic
region. iCCA of the left hemiliver should be considered as a
differential diagnosis of primary tumors and monitoring should be
performed. The present study may contribute to a better
understanding of the pathophysiology and clinical course of ICCA,
particularly of the intraductal growth type.
Acknowledgements
Not applicable.
Funding
The present study was supported by a Veterans Health Service
Medical Center Research Grant from the Republic of Korea (grant no.
VHSMC 22058).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
TL and SN conceptualized and designed the study. JRG
and AH collected and analyzed radiological images. SN performed
surgery and tissue collection. ML performed histopathological
diagnosis. TL and AH interpreted the data and wrote the manuscript.
TL and AH confirm the authenticity of all the raw data. All authors
reviewed and edited the manuscript. All authors have read and
approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Veterans
Health Service Medical Center review board (Seoul, Korea; approval
no. 2022-12-006). Written informed consent was obtained from the
patient.
Patient consent for publication
Written informed consent was obtained from the
patient for the publication of details of their medical case and
accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Sigel CS, Drill E, Zhou Y, Basturk O,
Askan G, Pak LM, Vakiani E, Wang T, Boerner T, Do RKG, et al:
Intrahepatic cholangiocarcinomas have histologically and
immunophenotypically distinct small and large duct patterns. Am J
Surg Pathol. 42:1334–1345. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Banales JM, Marin JJG, Lamarca A,
Rodrigues PM, Khan SA, Roberts LR, Cardinale V, Carpino G, Andersen
JB, Braconi C, et al: Cholangiocarcinoma 2020: The next horizon in
mechanisms and management. Nat Rev Gastroenterol Hepatol.
17:557–588. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bridgewater J, Galle PR, Khan SA, Llovet
JM, Park JW, Patel T, Pawlik TM and Gores GJ: Guidelines for the
diagnosis and management of intrahepatic cholangiocarcinoma. J
Hepatol. 60:1268–1289. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Conway AM, Morris GC, Smith S, Vekeria M,
Manoharan P, Mitchell C, Backen A, Oliveira P, Hubner RA, Lamarca
A, et al: Intrahepatic cholangiocarcinoma hidden within cancer of
unknown primary. Br J Cancer. 127:531–540. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sirica AE, Gores GJ, Groopman JD, Selaru
FM, Strazzabosco M, Wei Wang X and Zhu AX: Intrahepatic
cholangiocarcinoma: Continuing challenges and translational
advances. Hepatology. 69:1803–1815. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Raoof M and Singh G: Rising trends in
intrahepatic cholangiocarcinoma incidence and mortality: Getting at
the root cause. Hepatobiliary Surg Nutr. 8:301–303. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Florio AA, Ferlay J, Znaor A, Ruggieri D,
Alvarez CS, Laversanne M, Bray F, McGlynn KA and Petrick JL: Global
trends in intrahepatic and extrahepatic cholangiocarcinoma
incidence from 1993 to 2012. Cancer. 126:2666–2678. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Varadhachary GR: Carcinoma of unknown
primary origin. Gastrointest Cancer Res. 1:229–235. 2007.PubMed/NCBI
|
|
9
|
Oda E, Hashimoto D, Shiomi Y, Ohnishi K,
Hayashi H, Chikamoto A, Takeya M and Baba H: A case of occult
intrahepatic cholangiocarcinoma diagnosed by autopsy. Surg Case
Rep. 1:1012015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Nozaki Y, Yamamoto M, Ikai I, Yamamoto Y,
Ozaki N, Fujii H, Nagahori K, Matsumoto Y and Yamaoka Y:
Reconsideration of the lymph node metastasis pattern (N factor)
from intrahepatic cholangiocarcinoma using the International Union
Against Cancer TNM staging system for primary liver carcinoma.
Cancer. 83:1923–1929. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Chung YE, Kim MJ, Park YN, Choi JY, Pyo
JY, Kim YC, Cho HJ, Kim KA and Choi SY: Varying appearances of
cholangiocarcinoma: Radiologic-pathologic correlation.
RadioGraphics. 29:683–700. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Martin SP, Drake J, Wach MM, Ruff SM,
Diggs LP, Wan JY, Good ML, Dominguez DA, Ayabe RI, Glazer ES, et
al: Resection and chemotherapy is the optimal treatment approach
for patients with clinically node positive intrahepatic
cholangiocarcinoma. HPB (Oxford). 22:129–135. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Amin MB, Greene FL, Edge SB, Compton CC,
Gershenwald JE, Brookland RK, Meyer L, Gress DM, Byrd DR and
Winchester DP: American Joint Committee on Cancer, American Cancer
Society: AJCC cancer staging manual. 8th edition. American Joint
Committee on Cancer; Chicago, IL: 2017
|
|
14
|
Yamamoto M, Takasaki K and Yoshikawa T:
Lymph node metastasis in intrahepatic cholangiocarcinoma. Jpn J
Clin Oncol. 29:147–150. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Martin SP, Ruff S, Diggs LP, Drake J,
Ayabe RI, Brown ZJ, Wach MM, Steinberg SM, Davis JL and Hernandez
JM: Tumor grade and sex should influence the utilization of portal
lymphadenectomy for early stage intrahepatic cholangiocarcinoma.
HPB (Oxford). 21:419–424. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
de Jong MC, Nathan H, Sotiropoulos GC,
Paul A, Alexandrescu S, Marques H, Pulitano C, Barroso E, Clary BM,
Aldrighetti L, et al: Intrahepatic cholangiocarcinoma: An
international multi-institutional analysis of prognostic factors
and lymph node assessment. J Clin Oncol. 29:3140–3145. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Jutric Z, Johnston WC, Hoen HM, Newell PH,
Cassera MA, Hammill CW, Wolf RF and Hansen PD: Impact of lymph node
status in patients with intrahepatic cholangiocarcinoma treated by
major hepatectomy: A review of the National Cancer Database. HPB
(Oxford). 18:79–87. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Zhang XF, Xue F, Dong DH, Weiss M, Popescu
I, Marques HP, Aldrighetti L, Maithel SK, Pulitano C, Bauer TW, et
al: Number and station of lymph node metastasis after
curative-intent resection of intrahepatic cholangiocarcinoma impact
prognosis. Ann Surg. 274:e1187–e1195. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Jolissaint JS, Soares KC, Seier KP, Kundra
R, Gönen M, Shin PJ, Boerner T, Sigel C, Madupuri R, Vakiani E, et
al: Intrahepatic cholangiocarcinoma with lymph node metastasis:
Treatment-Related outcomes and the role of tumor genomics in
patient selection. Clin Cancer Res. 27:4101–4108. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Yamamoto M, Takasaki K, Yoshikawa T, Ueno
K and Nakano M: Does gross appearance indicate prognosis in
intrahepatic cholangiocarcinoma? J Surg Oncol. 69:162–167. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ohtsuka M, Ito H, Kimura F, Shimizu H,
Togawa A, Yoshidome H and Miyazaki M: Results of surgical treatment
for intrahepatic cholangiocarcinoma and clinicopathological factors
influencing survival. Br J Surg. 89:1525–1531. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Shimada K, Sano T, Sakamoto Y, Esaki M,
Kosuge T and Ojima H: Surgical outcomes of the mass-forming plus
periductal infiltrating types of intrahepatic cholangiocarcinoma: A
comparative study with the typical mass-forming type of
intrahepatic cholangiocarcinoma. World J Surg. 31:2016–2022. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Wang Y, Li J, Xia Y, Gong R, Wang K, Yan
Z, Wan X, Liu G, Wu D, Shi L, et al: Prognostic nomogram for
intrahepatic cholangiocarcinoma after partial hepatectomy. J Clin
Oncol. 31:1188–1195. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Utada M, Ohno Y, Tamaki T, Sobue T and
Endo G: Long-term trends in incidence and mortality of intrahepatic
and extrahepatic bile duct cancer in Japan. J Epidemiol.
24:193–199. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kubo S, Shinkawa H, Asaoka Y, Ioka T,
Igaki H, Izumi N, Itoi T, Unno M, Ohtsuka M, Okusaka T, et al:
Liver Cancer Study Group of Japan Clinical Practice Guidelines for
Intrahepatic Cholangiocarcinoma. Liver Cancer. 11:290–314. 2022.
View Article : Google Scholar : PubMed/NCBI
|