Introduction
The cancers of unknown primary (commonly named CUPs)
are a heterogeneous group of tumors characterized by a difficult
diagnosis, because the primary site remains occult after extensive
work-up (1). The CUPs represent
about 3–5% of all cancer diagnosis and the most common
manifestations are metastases in the lymph nodes, lung, liver, or
bone (2). In 75–85% of the cases,
the metastases are disseminated (3). Considering its enigmatic features, it
was discussed about the validity of CUP as a distinct cancer entity
supporting the hypothesis that the diagnosis of CUP could be
erroneous because the work-up may be incomplete or the syndrome may
be correlated to relapses of precedent cancers (4).
Therefore, International Guidelines tried to clarify
the diagnostic management (5),
highlighting the importance of patients' clinical and familiar
history, and on risk factors such as cancer predisposition and
occupational activity. A complete physical examination should be
performed with accuracy for respiratory and abdominal systems which
are the most common sites of primary cancers, according to the data
reported in the follow-up and autopsy of CUPs' patients, without
neglecting the clinical presentation that could drive the primary
tumor research (6). The initial
diagnostic work-up should include basic blood analyses and relevant
tumor markers. A computerized tomography (CT) of chest, abdomen and
pelvis is recommended by ESMO guidelines (7) and Positron emission tomography (PET)
imaging is frequently additionally employed in CUP to identify
unrecognized malignant lesions (8).
Only after that an extensive work-up has been performed without the
detection of a primitive cancer, the possibility of CUP syndrome
should be considered. The pathogenesis is controversial, but CUP
condition may be created by an early metastatic dissemination,
whereas the primary tumor has receded or is too small to be
detected (9). The CUPs of possible
breast origin represent a complex topic. ESMO Clinical Practice
Guidelines recommended mammography and eventual magnetic resonance
image (MRI) of the breast only for the women suspected of CUP,
considering the wide spreading of breast cancer in the female sex.
Breast investigation is not required routinely for men because male
breast cancer (BC) is rare, representing approximately 1% of
cancers that occur in males (10).
Therefore, CUPs of male BC origin are rarely considered for the
diagnosis and very few cases are reported in literature. Their
management represents an unclear topic, characterized by an extreme
variety of treatments and prognosis.
Case report
A 64 year-old male patient was admitted at the
General Surgery Division of a Teaching Hospital (Luigi Vanvitelli
University of Campania, Naples, Italy) for an axillary swelling
with severe pain to the arm and forearm. His past medical history
excluded other co-morbidities or cancer anamnesis. He was regular
smoker (15 cigarettes a day for 40 years). His familiar medical
history included breast cancer of one sister and ovarian cancer of
the other sister. Physical examination revealed a left swelling in
axilla, by the size of 2 cm, with irritated and reddened skin
above. Swelling was painful and without mobility along surface and
deep planes. No other signs in other districts were showed during
the physical examination.
He was admitted in November 2020 and during the
hospitalization (he was submitted to an axillary ultrasound (US)
that revealed increased volume and thickness of many axillary lymph
nodes, one of these with 2 cm of diameter and tender aspect.
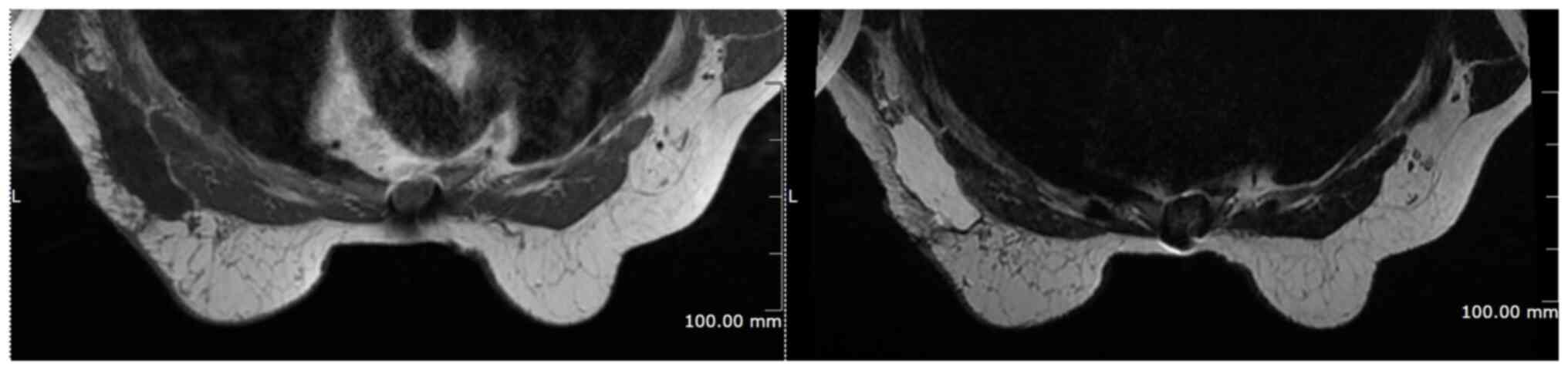
Magnetic Resonance Imaging (MRI) confirmed the presence of
multiples oval and round homogeneous shape nodules, similar to
lymph nodes, with low signal on T1 and T2. No breast lesion was
identified (Fig. 1). Ultrasound
guided fine needle aspiration biopsy (FNAB) was performed on the
largest lymph node. Definitive pathology showed malignant cells
with atypical elements like epithelioma, with clear cytoplasm,
chromatin clearing nucleus and evident nucleolus. In the attempt to
recognize the primary localization, a screening Total Body CT was
performed and showed repetitive lung nodes and confirmed the
presence of multiples axillary nodes. The largest was estimated of
4×2.3 cm in diameter. Positron emission tomography with
computerized tomography (PET-CT) exam was performed in an external
diagnostic center because it was not available in the hospital. The
examination completed the diagnostic process, confirming the
presence of numerous axillary and lung lymph nodes with elevated
metabolic activity and evidencing already left thorax subcutaneous
thickening and two bone lesions on D6.
The patient underwent a lymphadenectomy of the first
and second axillary levels. A drain was placed. The post-operative
course was regular, and no complications occurred. A total of 3
days after admission he was discharged from the hospital with no
symptoms or pain and the drain was removed the fifth postoperative
day. Histological exam showed adenocarcinoma with multiples nodes,
oxyphilic and apocrine aspect, sclerosis stromal and multifocal
coagulative and colliquative areas into the tumor. It was described
local perineural neoplastic infiltration without neoplastic
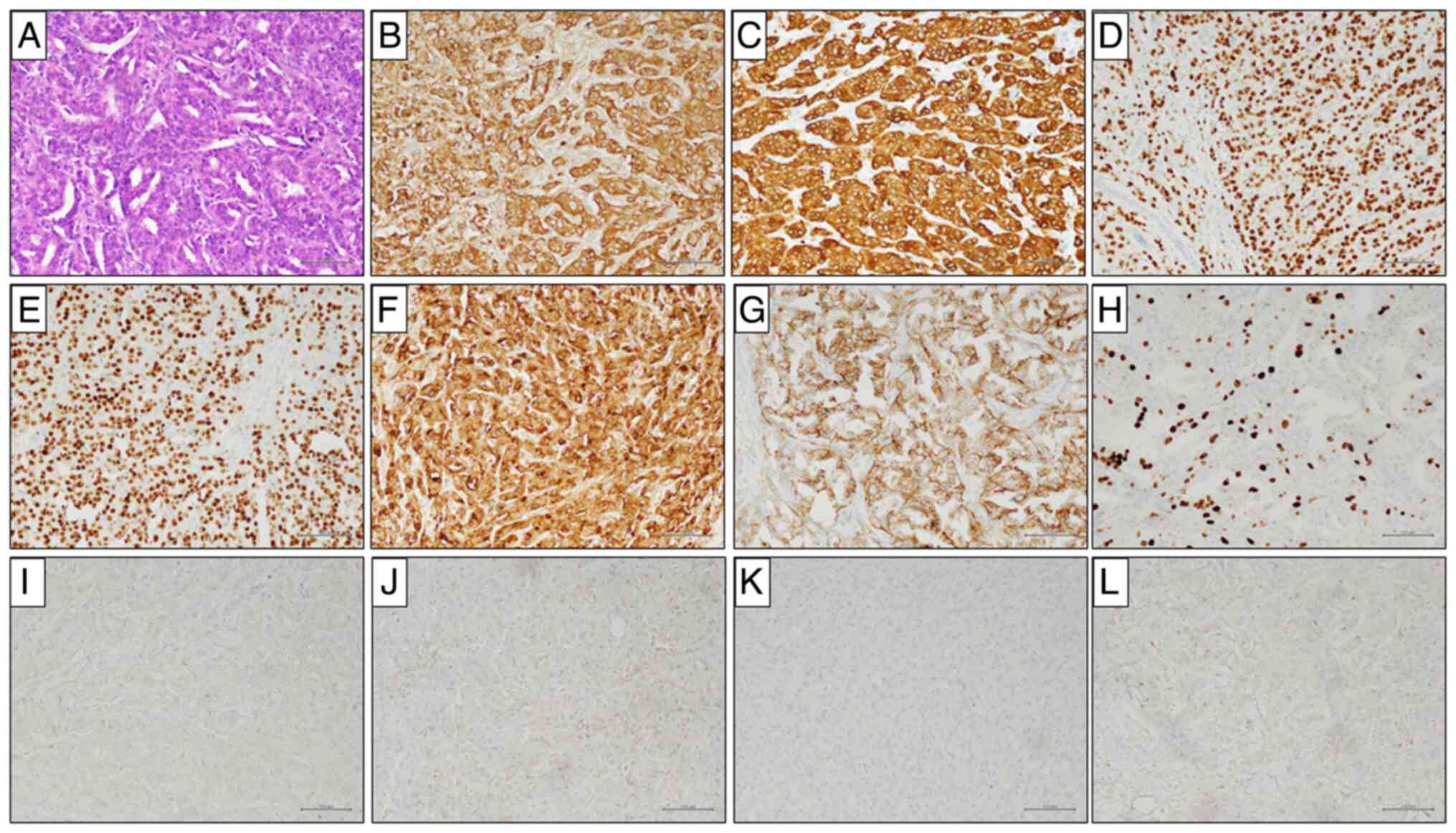
embolus. Immunohistochemistry was performed automatically on
BenchMark Ultra platform (Ventana Medical Systems), according to
the manufacturer's instructions, as previously described (11). Immunohistochemistry (IHC) (Fig. 2) analysis was positive for
cytokeratin (CK) AE1/AE3, CK7, GATA3, Gross cystic disease fluid
protein (GCDFP)-15, androgen receptor (AR), human epidermal growth
factor receptor 2 (HER 2), low and focal positive for mammaglobin.
The lesion did not show CK20, transcriptional thyroid factor (TTF)
1, Napsin A, Estrogen Receptor (ER), Progesterone Receptor (PgR).
The expression rate of proliferation marker Ki67 was 40%. The final
diagnosis was moderate differentiation grade 2 (G2) apocrine
carcinoma, inter-medial differentiation sec. Elston-Ellis score 7:
tubules formation, nuclear pleomorphism score 2, mitosis score 3.
The histological findings correlated with IHC were no sufficient to
make a differential diagnosis between cutaneous annexes
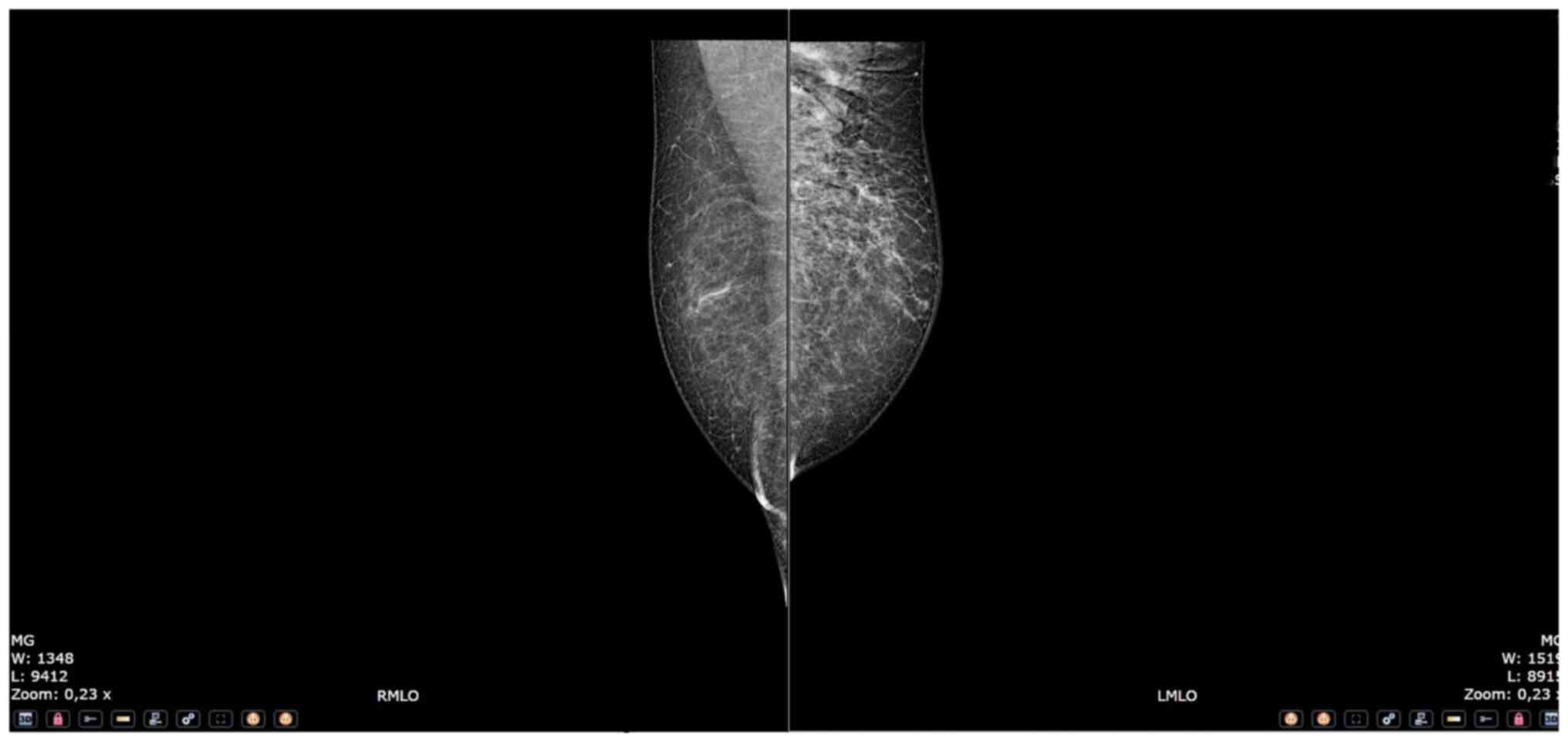
histogenesis and breast origin. Considering ER and mammaglobin
expression, we performed Mammography and breast US searching a rare
male BC, without identifying any breast lesions (Fig. 3). MRI revealed presence of focal
areas on D5 and D10 (maximum diameter was 11 mm), micro nodular
areas on D2, D12 and L1 and Multiples Bone lesions on pelvic region
(diameter maximum of 15 mm). Dermatology visit excluded cutaneous
histogenesis and the case was treated like man CUP syndrome of
possible breast origin. The patients signed a written consensus and
agreed the publication of his clinical case.
Discussion
CUPs are a group of neoplasms characterized by the
diagnosis of metastasis in the absence of a detectable primitivity,
after a complete clinical work-up (12,13).
The CUPs represent about 3–5% of all cancer diagnosis with an
overall age-standardized incidence ranges between 4 and 9 cases per
100.000 people annually worldwide (3). It is recognized as the fifth most
common cause of cancer death (14).
CUPs accounts for up to 1% of all breast cancers and the
involvement of axillary is the most common presentation in these
cases. It is known, in fact, that in over 50% of the cases of
axillary lymphadenopathy, the primary originates from the breast
(15–17). Therefore, mammography and
axillary-breast US should be included in the instrumental work-up
in all CUPs with axillary repetitions (18–20).
Breast Magnetic Resonance Imaging (MRI) is also recommended by
international guidelines because it can improve the detection of an
occult primary breast cancer in a wide range of cases (from 35 to
100%) (21–23).
BC is common in women and innovative technologies
for very accurate diagnosis and treatments were established
(24–26) while male breast cancer is rare, and
CUP of male breast origin is anecdotal. Moreover, there is no
consensus in literature about a specific panel of IHC due to their
rarity (27).
Using the PubMed database, a systematic review of
the current literature was carried out, up to March 2023. The final
article was realized in accordance with the Preferred Reporting
Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines
(28). The MeSH (Medical Subject
Headings) search terms used were ‘breast’, ‘cancer of unknown
primary’, ‘occult breast cancer’. The Authors observed that male
breast cancer of unknown primary was an extremely rare neoplasm.
The keywords ‘male breast cancer’, ‘occult male breast cancer’,
‘male breast cancer of unknown primary’ were used for the research.
Several combinations of the keywords and MeSH terms were utilized,
and the various terms were substituted during the search.
References of the more relevant articles were manually searched.
The last research was concluded on March 21, 2022.
Twelve articles published from 2008 to 2020 and
reporting cases of CUP of breast cancer origin were identified
(27,29–39)
(Table I). The mean age of the
patients was 59,23 years (range 29 to 83). Three men were smokers
(35,38,39)
and two of them (35,38) referred a familiarity for gastric
cancer: in a case the father, and in the other the mother was
affected. In 12 cases reported the first presentation was an
axillary mass; in one case the tumor was located on the anterior
chest wall (29) while in another
case, a vertebral painful lesion was diagnosed in the same moment
of the axillary nodule (39). Seven
men was affected by comorbidities: four of them showed dermatologic
disease such as eczema, reddish skin, dermatomyositis, and erythema
(27,29,34–35). A
patient had a benign thyroid nodule (35), one presented gynecomastia (37), and another found out a renal cystic
(39).
 | Table I.Reported cases of occult male breast
cancers. |
Table I.
Reported cases of occult male breast
cancers.
| First author,
year | Age, years | Risk factors | Clinical
presentation | Examinations | H&E
histopathological examination | Immunohistochemical
staining | Surgery | Neoadjuvant
therapy | Adjuvant CT | RT | Follow up | (Refs.) |
|---|
| Gu, 2008 | 72 | N/A | Painless and | MX, breast and | Breast | ER (−), PgR
(−), | ALNB, | No | No | No | After 18
months: | (36) |
|
|
|
| enlarged | axillary US | infiltrating | P53 (+), PCNA
(+), | mastectomy, |
|
|
| The lesion |
|
|
|
|
| lymph node |
| ductal | BCL 2
oncoprotein | ALND |
|
|
| disappeared |
|
|
|
|
|
|
| carcinoma | (+), Nm 23 (+),
HER2 |
|
|
|
|
|
|
|
|
|
|
|
|
| score 3+, MPR
(+) |
|
|
|
|
|
|
| Gu, 2009 | 72 | No | Painless | MX, breast and | Infiltrating | ER (−), PgR
(−), | ALNB, | No | No | No | After 24
months: | (31) |
|
|
|
| enlarged | axillary US | breast ductal | P53 (+), PCNA
(+), | mastectomy |
|
|
| The lesion |
|
|
|
|
| axillary |
| carcinoma | BCL 2
oncoprotein |
|
|
|
| disappeared |
|
|
|
|
| lymph node |
|
| (+), Nm 23 (+),
HER2 |
|
|
|
|
|
|
|
|
|
|
|
|
| score 3+, MPR
(+) |
|
|
|
|
|
|
| Takeyama, | 58 | N/A | 1 cm right, | Chest CT, MX, | Metastatic | ER 40%, PgR
30%, | ALNB, | Cisplatin, | Anthracycline, | No | N/A | (27) |
| 2010 |
|
| non-mobile, | breast and
axillary | adenocarcinoma | mammaglobulin | resection, | paclitaxel | taxane, |
|
|
|
|
|
|
| hard axillary | US, breast
MRI, | from an
unknown | 70–80%, HER2
(−), | ALND |
| tamoxifen |
|
|
|
|
|
|
| mass | head, lung,
upper | primary | P53 (−) |
|
|
|
|
|
|
|
|
|
|
| and lower |
|
|
|
|
|
|
|
|
|
|
|
|
|
gastrointestinal |
|
|
|
|
|
|
|
|
|
|
|
|
| system
endoscopy |
|
|
|
|
|
|
|
|
| Hur, 2012 | 59 | Smoking; | Palpable | MX, breast and | Metastatic
poor | ER (+), PgR
(+), | ALNB, | No | Doxorubicin, |
| After 10
years: | (35) |
|
|
| gastric | mass in | axillary US,
breast | differentiated | HER2 (score
1+), | skin sparing |
| cyclophospha- |
| The lesion |
|
|
|
| cancer | right axilla | MRI, chest CT, | adenocarcinoma | BRST-2 (+), S-100
(−) | mastectomy, |
| mide,
docetaxel, |
| disappeared |
|
|
|
| familiarity |
| abdominal US, | likely of
breast |
| ALND |
| tamoxifen |
|
|
|
|
|
| (father) |
| EGDS, | origin |
|
|
|
|
|
|
|
|
|
|
|
| colonoscopy |
|
|
|
|
|
|
|
|
|
|
|
|
| AFP, CEA, PSA, |
|
|
|
|
|
|
|
|
|
|
|
|
| CA 19-9, CA
15-3 |
|
|
|
|
|
|
|
|
| Hur, 2012 | 45 | No | Palpable | MX, breast and | Adenocarcinoma | TTF-1 (−), CK 20
(−), | ALND | No | Doxorubicin, | Yes | After 24
months: | (35) |
|
|
|
| mass in |
| axillary US,
breast | CEA (+), ER
(+), |
|
| cyclophospha- |
| The lesion |
|
|
|
|
| left axilla |
| MRI, PET,
chest | PgR (+), HER2
(−), |
|
| mide,
docetaxel, |
| disappeared |
|
|
|
|
|
|
| CT, abdominal | Ki-67 (+), EGFR
(−), |
|
| tamoxifen |
|
|
|
|
|
|
|
|
| CT, EGDS; CEA, | BRST-2 (+) |
|
|
|
|
|
|
|
|
|
|
|
| PSA, CA 19-9, |
|
|
|
|
|
|
|
|
|
|
|
|
| CA 15-3, |
|
|
|
|
|
|
|
|
|
|
|
|
| Calcitonin
blood |
|
|
|
|
|
|
|
|
|
|
|
|
| test |
|
|
|
|
|
|
|
| Wang, | 58 | N/A | Left armpit | Breast and
axillary | Glandular
cancer | After neoadjuvant
CT: | ALNB, | Paclitaxel, | Doxorubicin | Yes | After 12
months: | (32) |
| 2014 |
|
| painful | US, MX,
PET-CT; | with high | E-cadherin
(+), | mastectomy | oxaliplatin |
|
| The lesion |
|
|
|
|
| 0.8×0.6 cm | CA-125, CEA | possibility of | P120 (+), CK7
(+), |
| with partial |
|
| disappeared |
|
|
|
|
| mass | blood test | primary
mammary | ER 90%, PgR
85% |
| response; |
|
|
|
|
|
|
|
|
|
| tumor |
|
| docetaxel, |
|
|
|
|
|
|
|
|
|
|
|
|
| lobaplatin |
|
|
|
|
|
|
|
|
|
|
|
|
| with no |
|
|
|
|
|
|
|
|
|
|
|
|
| response |
|
|
|
|
| He, 2015 | 40 | No | Left axillary | Breast and
axillary | Moderately | CK 20 (−), | ALNB, | No | Trastuzumab, | No | After 9
months: | (37) |
|
|
|
| palpable | US, total body | differentiated | mammaglobin
(−), | mastectomy, |
| paclitaxel, |
| Newly
increased |
|
|
|
|
| 2.2 cm | CT, abdominal | adenocarcinoma | TTF-1 (−), ER
(−), | ALND |
| carboplatin |
| uptake on left |
|
|
|
|
| nodule | US, thyroid
US, | with solid
nests | GCDPF 15 (−), |
|
|
|
|
supraclavicular |
|
|
|
|
|
| genitourinary
US, | and cord-like | PgR (+), HER2 |
|
|
|
| region
detected |
|
|
|
|
|
| breast MRI,
PET; | arrangements
of | (score 2+) |
|
|
|
| on PET/CT; |
|
|
|
|
|
| CEA, PSA, CA | cancer cells |
|
|
|
|
| after 3 years |
|
|
|
|
|
| 19-9, CA 15-3, |
|
|
|
|
|
| Stable disease |
|
|
|
|
|
| Calcitonin,
AFP |
|
|
|
|
|
|
|
|
|
|
|
|
| blood test |
|
|
|
|
|
|
|
|
| Rigakos, | 54 | Smoking | Painful | Lumbar spinal | Metastatic low | CK AE1/3 (+), | ALNB, | | Capecitabine, |
| After 33
months: | (39) |
| 2016 |
|
| vertebral | MRI, PSA,
total | grade
carcinoma | CAM 5.2 (+), | ALND |
| trastuzumab, |
| Stable bone |
|
|
|
|
| mass, right | body CT,
PET-CT | of epithelial
origin | epithelial
membrane |
|
| vinorelbine, |
| disease |
|
|
|
|
| axillary |
| origin | antigen (+), |
|
| tamoxifen, |
|
|
|
|
|
|
| mass, bone |
|
| E-cadherin
(+), |
|
| letrozole |
|
|
|
|
|
|
| lesions |
|
| melan A (+), |
|
|
|
|
|
|
|
|
|
|
|
|
| synaptophysin
(+), |
|
|
|
|
|
|
|
|
|
|
|
|
| placental
alkaline |
|
|
|
|
|
|
|
|
|
|
|
|
| phosphatase
(+), |
|
|
|
|
|
|
|
|
|
|
|
|
| NSE (+), CD
(1), |
|
|
|
|
|
|
|
|
|
|
|
|
| human melanoma |
|
|
|
|
|
|
|
|
|
|
|
|
| black 45 (+),
renal |
|
|
|
|
|
|
|
|
|
|
|
|
| cell (−), inhibin
(−), |
|
|
|
|
|
|
|
|
|
|
|
|
| TTF-1 (−), CK5/6
(−), |
|
|
|
|
|
|
|
|
|
|
|
|
| GCDPF 15 (−), |
|
|
|
|
|
|
|
|
|
|
|
|
| vimentin (−), |
|
|
|
|
|
|
|
|
|
|
|
|
| CD 117 (−), PSA
(−); |
|
|
|
|
|
|
|
|
|
|
|
|
| after
Micro-RNA: |
|
|
|
|
|
|
|
|
|
|
|
|
| ER (+), PgR
(+), |
|
|
|
|
|
|
|
|
|
|
|
|
| HER2 (+) |
|
|
|
|
|
|
| Zhang, | 84 | No | Palpable | Total body CT | Metastatic
poor | ER (−), PgR
(−), | Core needle | No | Paclitaxel, | No | After 24
months: | (34) |
| 2017 |
|
| 3.9 cm |
| differentiated | PSA (−), GCDPF
15 | biopsy, |
| cyclophospha- |
| The lesion |
|
|
|
|
| nodule |
| adenocarcinoma | (+), AE1/AE3
(+), | ALND |
| mide |
| disappeared |
|
|
|
|
| in right |
| likely of
breast | CK 7 (+), CK 20
(+), |
|
|
|
|
|
|
|
|
|
| axilla |
| origin | HER2 (−) |
|
|
|
|
|
|
| Kuninaka, | 67 | N/A | 3 cm left | CT | Metastatic | ER (+), PgR
(<1%), | ALNB | No | Trastuzumab | No | After 18
months: | (29) |
| 2017 |
|
| anterior |
| adenocarcinoma | HER2 score 3+, |
|
|
|
| The lesion |
|
|
|
|
| chest wall |
| from an
unknown | CK 7 (+), CK 20
(−), |
|
|
|
| disappeared |
|
|
|
|
| tumor |
| primary | GCDPF 15 (+) |
|
|
|
|
|
|
| Xu, 2017 | 29 | Smoking, | Left axillary | Chest CT,
PET-CT, | Infiltrating
ductal | CK 5/6 (+), CK 7
(+), | ALND | No | Adriamycin, | Yes | After 9
months: | (38) |
|
|
| gastric | palpable | breast and
axillary | carcinoma | CDX-2 (+), P63
(+), |
|
| docetaxel |
| The lesion |
|
|
|
| cancer | 4.3×2.3 cm | US, MX
(rejected); |
| TTF-1 (+), |
|
|
|
| disappeared |
|
|
|
| familiarity | nodule | CEA, PSA, CA |
| synaptophysin
(+), |
|
|
|
|
|
|
|
|
| (mother) |
| 19-9, CA 15-3, |
| chromogranin A
(+), |
|
|
|
|
|
|
|
|
|
|
| CA 72-4, NSE, |
| S 100 (+),
GCDPF |
|
|
|
|
|
|
|
|
|
|
| Cyfra 21-1, |
| 15 (−), HER2 |
|
|
|
|
|
|
|
|
|
|
| Calcitonin,
AFP |
| (score 2+), FISH
(−), |
|
|
|
|
|
|
|
|
|
|
| blood test |
| ER (−), PgR
(−), |
|
|
|
|
|
|
|
|
|
|
|
|
| EMA (+), GATA-3
(−), |
|
|
|
|
|
|
|
|
|
|
|
|
| CK 20 (−), |
|
|
|
|
|
|
|
|
|
|
|
|
| mammaglobin
(−) |
|
|
|
|
|
|
| Wang, | 49 | N/A | Painless | US PET-TC, | Metastatic | ER (+), PgR
(+), | ALNB, | No | Paclitaxel, | Yes | After 4 years: | (33) |
| 2018 |
|
| 4×3 cm side | MX (rejected) | adenocarcinoma | GCDPF 15 (+), | mastectomy |
| phosphamide, |
| The lesion |
|
|
|
|
| mass in left |
| from an
unknown | HER2 (−), CK 7
(−), | (rejected), |
| pharmorubicin, |
| disappeared |
|
|
|
|
| axilla |
| primary | CK 20 (−), TTF-1
(+) | ALNB |
| tamoxifen |
|
|
|
| Sood, | 83 | N/A | 10×6 cm | Mammography | Metastatic | ER (+), PgR
(+), | ALNB, | No | Yes | No | N/A | (30) |
| 2020 |
|
| right |
| adenocarcinoma | GCDPF 15 (+), | ALND |
|
|
|
|
|
|
|
|
| axillary |
| from an
unknown | androgen receptor
(+), |
|
|
|
|
|
|
|
|
|
| mass |
| primary | E-cadherin
(+), |
|
|
|
|
|
|
|
|
|
|
|
|
| calponin (−), P53
(−), |
|
|
|
|
|
|
|
|
|
|
|
|
| HER2 (−), NSE
(+), |
|
|
|
|
|
|
|
|
|
|
|
|
| synaptophysin
(+) |
|
|
|
|
|
|
Despite mammography is considered the gold standard
for the breast cancer diagnosis, in four cases it was not
recommended by the surgeons (29,34,37,39)
and in another two studies the patient rejected it (32,38).
US was performed in 9 out of 13 cases (27,31–33,35–38),
while breast MRI was planned for only 4 patients (27,35,37). A
complete work-up with the association of US, mammography and breast
MRI has been realized in only three case reports (27–35).
Therefore, it is possible to assume that more accurate and
diagnostic process would be desirable to define a diagnosis of CUP.
In fact, a patient underwent to an incomplete diagnostic work-up is
not suitable to receive this kind of diagnosis. In the present
case, despite the complete preoperative diagnostic work-up with
mammography, US, MRI, Total Body CT and 18 FDG PET-CT was not
possible to clearly identify a primary origin conuring a ‘real’
CUP. The clinical suspicious was driven only by the familiarity for
breast and ovarian cancers of the sisters, and for the IHC on the
resected specimen. Moreover, the diagnostic trouble appears even
more relevant considering that even after the definitive pathology
was not possible to certainly distinguish between the breast and
the cutaneous annexes histogenesis. Only the dermatological
counselling, after an accurate clinical examination was able to
exclude the cutaneous annexes origin.
The most important method for the individuation and
characterization of the breast origin of a CUP was the
immunochemistry (IHC) performed on the biopsied specimen, pointing
out the preeminence of the surgical approach. Only Zhang et
al (34) obtained the diagnosis
performing an IHC analysis on a core needle biopsy. Noteworthy, the
necessity of the surgery in the diagnostic process reduces the
opportunities for the neoadjuvant approach and this fact could
negatively influence the prognosis. The conventional histological
diagnosis with eosin and hematoxylin (H&E) staining was able to
reach the diagnosis only in 5 cases on 13 (38,5%) (31,32,34–36);
three patients was affected by infiltrating ductal carcinoma
(31,32,36),
while for the other two case the diagnosis was less accurate
(34–35). Considering the c-erbB-2 mutation,
three tumors were Her2 positive with score 3+ (29,31,36);
some authors reported a positive determination for Her2 with lower
score while He et al (37),
referred about a Her2 positivity with score 2+ but the florescent
in situ hybridization (FISH) test was not reported. Wang
et al (33) had not
mentioned Her2 verify and Rigakos et al (39) had not detailed the Her2 positivity.
Lack of the FISH analysis and Her2 determination has precluded any
possible adjuvant treatment with Trastuzumab. Luminal forms were
the most diagnosed (6 out of 13 cases, 46.2%) (27,29,33,35,37,39).
Only one patient was candidate to neoadjuvant treatment (27), after an incisional biopsy. Taxane
drugs were indicated for 7 patients on 13 (27,33–35,37,38).
Only four patients underwent to irradiation during the neoadjuvant
phase (32,33,35,38).
Two studies did not reported data about the follow up (27,30).
The other papers referred that the patients were alive until the
last follow up. The mean period of observation was 22,4 months
(range 9–48).
Rigakos et al (39) performed the microRNA Rosetta Cancer
Origin test to find out the primitivity after the failure of
PET-TC, Total body CT and MRI. Many studies have demonstrated that
microRNA profiling may be useful for the CUPs' work up, with
agreement to final diagnosis for microRNA testing ranging from 84
to 92% (40–42). MicroRNAs are small, non-coding RNAs
of 17–25 nucleotides involved in a regulatory function in protein
translation and expression. Since their discovery, they are
becoming important as cancer biomarker. However, it is not clear if
this technique was necessary in the diagnostic process, because it
was performed before the axillary surgery and the HIC test.
Despite CUP of male BC origin is very rare, this
review highlighted the heterogeneity of the diagnostic methods and
the therapeutic strategies. In any suspicious cases of CUP, a
strict and accurate diagnostic work-up appears mandatory to exclude
any possible primary origin of the tumor. This aspect seems even
more important since the scarce experience with this pathology and
the absence of guidelines could influence the treatment and the
prognosis of the CUP patients. Larger comparative studies about the
diagnostic methods and therapeutic approach are needed to address
this issue.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
SP was responsible for collecting clinical, imaging
and pathological data of the patient, and was responsible for the
conception, design, content and writing of the manuscript. FF, FI,
MLV, GC, FMM and LB collected data. CG, RR, ST, LD and FSL
contributed to the conception and revisions of the manuscript. RA
contributed to the writing of the manuscript, the conception of the
study and the collection of pathological images. All authors agreed
on the journal to which the article has been submitted and agreed
to be accountable for all aspects of the work. All authors read and
approved the final manuscript. SP and CG confirm the authenticity
of the raw data.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient for publication of this case report and the accompanying
images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bochtler T, Löffler H and Krämer A:
Diagnosis and management of metastatic neoplasms with unknown
primary. Semin Diagn Pathol. 35:199–206. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Abbruzzese JL, Abbruzzese MC, Hess KR,
Raber MN, Lenzi R and Frost P: Unknown primary carcinoma: Natural
history and prognostic factors in 657 consecutive patients. J Clin
Oncol. 12:1272–1280. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Pavlidis N and Pentheroudakis G: Cancer of
unknown primary site. Lancet. 379:1428–1435. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Bochtler T and Krämer A: Does cancer of
unknown primary (CUP) truly exist as a distinct cancer entity?
Front Oncol. 9:4022019. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Pauli C, Bochtler T, Mileshkin L,
Baciarello G, Losa F, Ross JS, Pentheroudakis G, Zarkavelis G,
Yalcin S, Özgüroğlu M, et al: A challenging task: Identifying
patients with cancer of unknown primary (CUP) according to ESMO
guidelines: The CUPISCO trial experience. Oncologist. 26:e769–e779.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tay J and Dewdney A: Cancers of unknown
primary. Br J Hosp Med (Lond). 80:C70–C74. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Piga A, Gesuita R, Catalano V, Nortilli R,
Cetto G, Cardillo F, Giorgi F, Riva N, Porfiri E, Montironi R, et
al: Identification of clinical prognostic factors in patients with
unknown primary tumors treated with a platinum-based combination.
Oncology. 69:135–144. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Keller F, Psychogios G, Linke R, Lell M,
Kuwert T, Iro H and Zenk J: Carcinoma of unknown primary in the
head and neck: Comparison between positron emission tomography
(PET) and PET/CT. Head Neck. 33:1569–1575. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Fizazi K, Greco FA, Pavlidis N and
Pentheroudakis G; ESMO Guidelines Working Group, : Cancers of
unknown primary site: ESMO clinical practice guidelines for
diagnosis, treatment and follow-up. Ann Oncol. 26:S133–S138. 2015.
View Article : Google Scholar
|
|
10
|
Gucalp A, Traina TA, Eisner JR, Parker JS,
Selitsky SR, Park BH, Elias AD, Baskin-Bey ES and Cardoso F: Male
breast cancer: A disease distinct from female breast cancer. Breast
Cancer Res Treat. 173:37–48. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ronchi A, Pagliuca F, Marino FZ, Accardo
M, Cozzolino I and Franco R: Current and potential
immunohistochemical biomarkers for prognosis and therapeutic
stratification of breast carcinoma. Semin Cancer Biol. 72:114–122.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Conner JR and Hornick JL: Metastatic
carcinoma of unknown primary: Diagnostic approach using
immunohistochemistry. Adv Anat Pathol. 22:149–167. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Krämer A, Hübner G, Schneeweiss A,
Folprecht G and Neben K: Carcinoma of unknown primary-an orphan
disease? Breast Care (Basel). 3:164–170. 2008.PubMed/NCBI
|
|
14
|
National Cancer Registration and Analysis
Service, . Routes to Diagnosis. Cancer of Unknown Primary.
2010.Available from:. http://ncin.org.uk/publications/data_briefings/routes_to_diagnosis_cancer_of_unknown_primary12–December.
2018
|
|
15
|
De Andrade JM, Marana HR, Filho JM, Murta
EF, Velludo MA and Bighetti S: Differential diagnosis of axillary
masses. Tumori. 82:596–599. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Gupta RK, Naran S, Lallu S and Fauck R:
Diagnostic value of needle aspiration cytology in the assessment of
palpable axillary lymph nodes. A study of 336 cases. Acta Cytol.
47:550–554. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Blanchard DK and Farley DR: Retrospective
study of women presenting with axillary metastases from occult
breast carcinoma. World J Surg. 28:535–539. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Baron PL, Moore MP, Kinne DW, Candela FC,
Osborne MP and Petrek JA: Occult breast cancer presenting with
axillary metastases. Updated management. Arch Surg. 125:210–214.
1990. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Galimberti V, Bassani G, Monti S, Simsek
S, Villa G, Renne G and Luini A: Clinical experience with axillary
presentation breast cancer. Breast Cancer Res Treat. 88:43–47.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Walker GV, Smith GL, Perkins GH, Oh JL,
Woodward W, Yu TK, Hunt KK, Hoffman K, Strom EA and Buchholz TA:
Population-based analysis of occult primary breast cancer with
axillary lymph node metastasis. Cancer. 116:4000–4006. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Mann RM, Balleyguier C, Baltzer PA, Bick
U, Colin C, Cornford E, Evans A, Fallenberg E, Forrai G, Fuchsjäger
MH, et al: European society of breast imaging (EUSOBI), with
language review by Europa Donna-The European breast cancer
coalition. Breast MRI: EUSOBI recommendations for women's
information. Eur Radiol. 25:3669–3678. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Stella GM, Senetta R, Cassenti A, Ronco M
and Cassoni P: Cancers of unknown primary origin: Current
perspectives and future therapeutic strategies. J Transl Med.
10:122012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Sardanelli F, Boetes C, Borisch B, Decker
T, Federico M, Gilbert FJ, Helbich T, Heywang-Köbrunner SH, Kaiser
WA, Kerin MJ, et al: Magnetic resonance imaging of the breast:
Recommendations from the EUSOMA working group. Eur J Cancer.
46:1296–1316. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Parisi S, Ruggiero R, Gualtieri G, Volpe
ML, Rinaldi S, Nesta G, Bogdanovich L, Lucido FS, Tolone S,
Parmeggiani D, et al: Combined LOCalizer™ and intraoperative
ultrasound localization: First experience in localization of
non-palpable breast cancer. In Vivo. 35:1669–1676. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Parisi S, Gambardella C, Ruggiero R,
Tolone S, Lucido FS and Docimo L: Radiofrequency
identification-RFID using LOCalizer-tag in non-palpable breast
lump. Indian J Surg. 85:934–938. 2023. View Article : Google Scholar
|
|
26
|
Iovino F, Diana A, Carlino F, Ferraraccio
F, Antoniol G, Fisone F, Perrone A, Marino FZ, Panarese I, Tathode
MS, et al: Expression of c-MET in estrogen receptor positive and
HER2 negative resected breast cancer correlated with a poor
prognosis. J Clin Med. 11:69872022. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Takeyama H, Takahashi H, Tabei I, Fukuchi
O, Nogi H, Kinoshita S, Uchida K and Morikawa T: Malignant neoplasm
in the axilla of a male: Suspected primary carcinoma of an
accessory mammary gland. Breast Cancer. 17:151–154. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Liberati A, Altman DG, Tetzlaff J, Mulrow
C, Gøtzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J
and Moher D: The PRISMA statement for reporting systematic reviews
and meta-analyses of studies that evaluate healthcare
interventions: Explanation and elaboration. BMJ. 339:b27002009.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Kuninaka K, Takahashi R, Nakagawa Y and
Nishimaki T: A case of HER2-positive male occult breast carcinoma
with skin and lymph node metastases that exhibited complete
response to trastuzumab monotherapy. Clin Case Rep. 5:591–593.
2017. View
Article : Google Scholar : PubMed/NCBI
|
|
30
|
Sood N, Gupta R and Gupta S: Invasive
solid papillary carcinoma: Report of the first case presenting as
an occult breast carcinoma in a male. Indian J Pathol Microbiol.
63:S141–S142. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Gu GL, Wang SL, Wei XM, Ren L and Zou FX:
Axillary metastasis as the first manifestation of occult breast
cancer in a male patient. Breast Care (Basel). 4:43–45. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Wang WW, Chen L and Ouyang XN:
Misdiagnosed male breast cancer with an unknown primary tumor: A
case report. Oncol Lett. 8:190–192. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Wang X, Fan L, Yan W, Zhang Q, Bao S, Wang
Y, Bao X and Liu L: Axillary lymph node metastasis as the first
manifestation of male occult breast cancer: A case report. Medicine
(Baltimore). 97:e137062018. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Zhang L, Zhang C, Yang Z, He M, Zhang L,
Ezzat S and Liang X: Male occult triple-negative breast cancer with
dermatomyositis: A case report and review of the literature. Onco
Targets Ther. 10:5459–5462. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Hur SM, Cho DH, Lee SK, Choi MY, Bae SY,
Koo MY, Kim S, Nam SJ, Lee JE and Yang JH: Occult breast cancers
manifesting as axillary lymph node metastasis in men: A two-case
report. J Breast Cancer. 15:359–563. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Gu GL, Wang SL, Wei XM, Ren L and Zou FX:
Axillary metastasis as the first manifestation of male breast
cancer: A case report. Cases J. 30:2852008. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
He M, Liu H and Jiang Y: A case report of
male occult breast cancer first manifesting as axillary lymph node
metastasis with part of metastatic mucinous carcinoma. Medicine
(Baltimore). 94:e10382015. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Xu R, Li J, Zhang Y, Jing H and Zhu Y:
Male occult breast cancer with axillary lymph node metastasis as
the first manifestation: A case report and literature review.
Medicine (Baltimore). 96:e93122017. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Rigakos G, Vakos A, Papadopoulos S,
Vernadou A, Tsimpidakis A, Papachristou D and Razis E: Cancer of
unknown primary ultimately diagnosed as male breast cancer: A rare
case report. Mol Clin Oncol. 5:263–266. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Varadhachary GR, Spector Y, Abbruzzese JL,
Rosenwald S, Wang H, Aharonov R, Carlson HR, Cohen D, Karanth S,
Macinskas J, et al: Prospective gene signature study using microRNA
to identify the tissue of origin in patients with carcinoma of
unknown primary. Clin Cancer Res. 17:4063–4070. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Pentheroudakis G, Pavlidis N, Fountzilas
G, Krikelis D, Goussia A, Stoyianni A, Sanden M, St Cyr B,
Yerushalmi N, Benjamin H, et al: Novel microRNA-based assay
demonstrates 92% agreement with diagnosis based on
clinicopathologic and management data in a cohort of patients with
carcinoma of unknown primary. Mol Cancer. 12:572013. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Rosenwald S, Gilad S, Benjamin S, Lebanony
D, Dromi N, Faerman A, Benjamin H, Tamir R, Ezagouri M, Goren E, et
al: Validation of a microRNA-based qRT-PCR test for accurate
identification of tumor tissue origin. Mod Pathol. 23:814–823.
2010. View Article : Google Scholar : PubMed/NCBI
|