Introduction
Sarcomatoid carcinoma is a rare neoplasm with
distinct cellular differentiation (1–8). It is
considered as a more aggressive variant of squamous cell carcinoma
in the head and neck region (1–8). Due
to limited literature, there are currently no clear and unified
diagnostic and treatment guidelines for laryngeal sarcomatoid
carcinoma (9). This malignancy can
occur in various anatomical sites, including the upper respiratory
tract, lungs, breast, skin, gastrointestinal tract and the
urogenital system (10). However,
it most commonly affects the lungs (11–15).
Laryngeal sarcomatoid carcinoma is rare (1,2,16),
accounting for 2–3% of all laryngeal cancers (3), with glottis being the most common site
affected, with an incidence of ~1.5% of all laryngeal-related
cancers (4). Although lymph node
metastasis and distant spread are relatively uncommon in laryngeal
sarcomatoid carcinoma, the recurrence rates remain high (5–7).
Squamous cell carcinoma originates from the
epithelium, whereas sarcoma arises from the mesenchyme.
Carcinosarcoma is a biphasic tumor comprising either in situ
or invasive squamous cell carcinoma and a malignant spindle cell
component of epithelial origin, showing mesenchymal characteristics
(1–8). It is considered as an aggressive
variant of squamous cell carcinoma (1–8). Due
to their morphological and immunohistochemical similarities,
pathologists face significant challenges in differentiating
carcinosarcoma from spindle cell sarcoma (17,18).
Therefore, the rate of misdiagnosis is high and this type of tumor
is often mistaken with vocal cord polyps or laryngeal squamous cell
carcinomas (9,10).
In the present study, the case of a patient who
underwent two vocal cord tumor resection surgeries in another
hospital, followed by partial resection of the larynx combined with
laryngeal functional reconstruction surgery in the Second
Affiliated Hospital of the Army Military Medical University
(Chongqing, China) was reported. Shortly after each surgery, signs
of recurrence at the surgical site were suspected.
Histopathological and immunohistochemical examinations on tumor
specimens verified sarcomatoid carcinoma of the larynx and,
therefore, a third surgery on the larynx was performed. After
surgery, the patient was followed up for an additional 6 months and
no signs of recurrence were observed.
The analysis of the present case study could assist
clinical practitioners in drawing from relevant experiences,
reducing misdiagnosis rates for laryngeal sarcomatoid carcinoma and
achieving early detection and diagnosis.
Case report
The present study reports the case of a 69-year-old
male patient. Approximately 18 months prior admission to the Second
Affiliated Hospital of the Army Military Medical University
(Chongqing, China), the voice of the patient remained hoarse after
contracting a cold, while the medication treatment was not
satisfactory. At 16 months prior admission, the patient sought
medical attention in the People's Hospital of Hechuan Chongqing
(Chongqing, China) and underwent surgical resection of vocal cord
lesions under laryngoscopy. Postoperative pathological diagnosis
revealed inflammatory granulation tissue and a small amount of
fibrinous exudate in the vocal cords. However, no further
immunohistochemical examinations were performed. At 14 months prior
admission, although the patient reported improved postoperative
hoarseness, the patient subsequently experienced a recurrence of
persistent hoarseness and morning voice loss. Laryngoscopy revealed
the regrowth of the mass in the surgical area. Therefore, at 11
months prior admission, the patient was subjected to an endoscopic
excision procedure to support the removal of the vocal cord mass.
The postoperative pathological diagnosis still indicated
inflammatory granulation tissue with multinucleated giant cell
reaction in the left vocal cord mass. However, no additional
immunohistochemical examination was conducted. At 1 month after the
second surgery, the patient experienced a recurrence of hoarseness
in his voice. However, no further medical intervention was applied.
Furthermore, at 1 month prior to admission, the patient suddenly
developed symptoms of grade III laryngeal obstruction, which
required immediate medical attention. To alleviate respiratory
distress, the patient underwent tracheostomy. Subsequently, the
patient sought further treatment by our medical team at the Second
Affiliated Hospital of the Army Military Medical University in
November 2023.
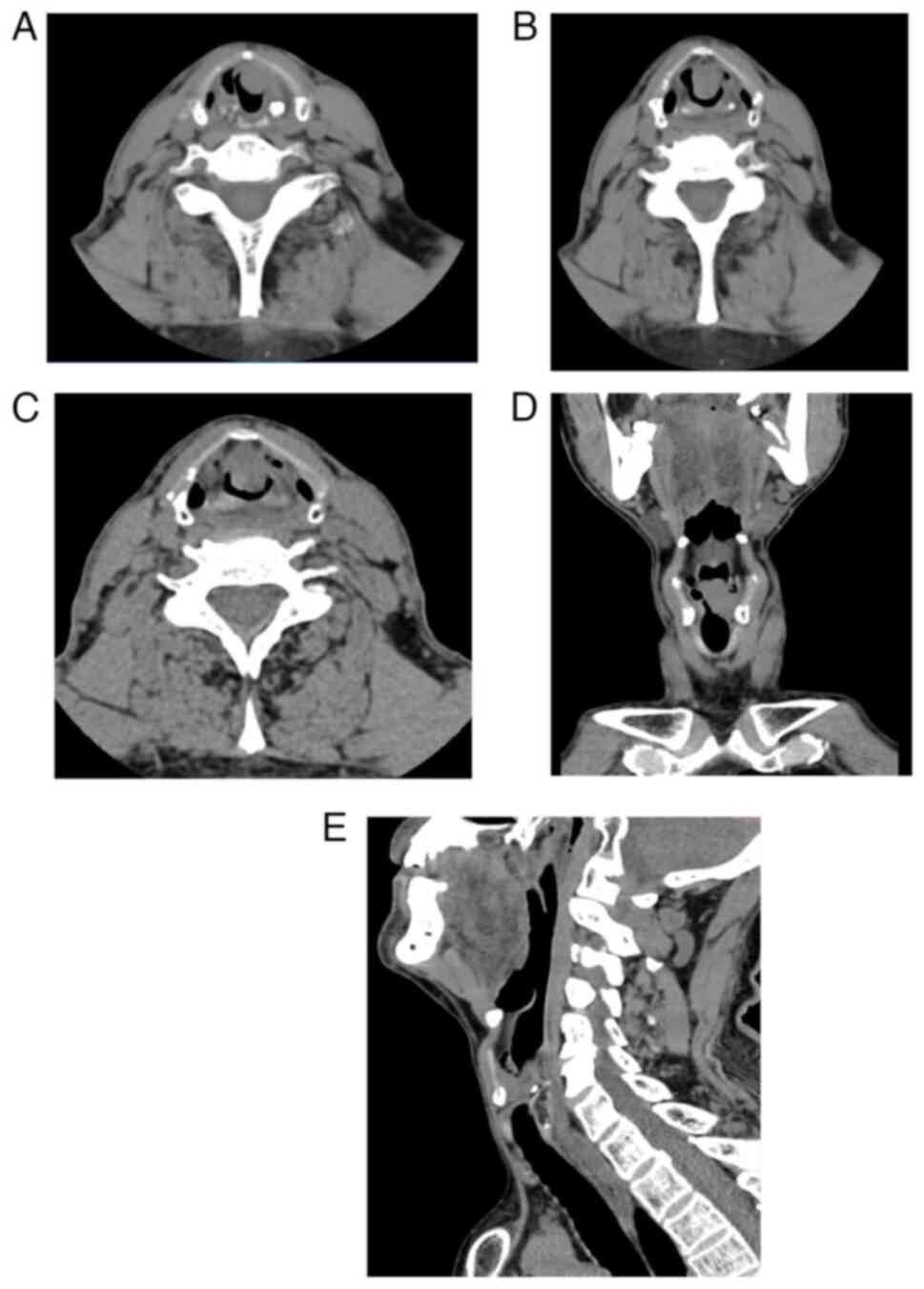
Therefore, the patient was first subjected to throat
spiral computed tomography. The results revealed a tumor mass of
~1.9×1.7 cm2 in size (Fig.
1A-E). Additionally, as shown in Fig. 1D and E, complete obstruction at the
glottis level in the larynx was observed, which directly resulted
in the patient's sudden onset of upper airway obstruction prior to
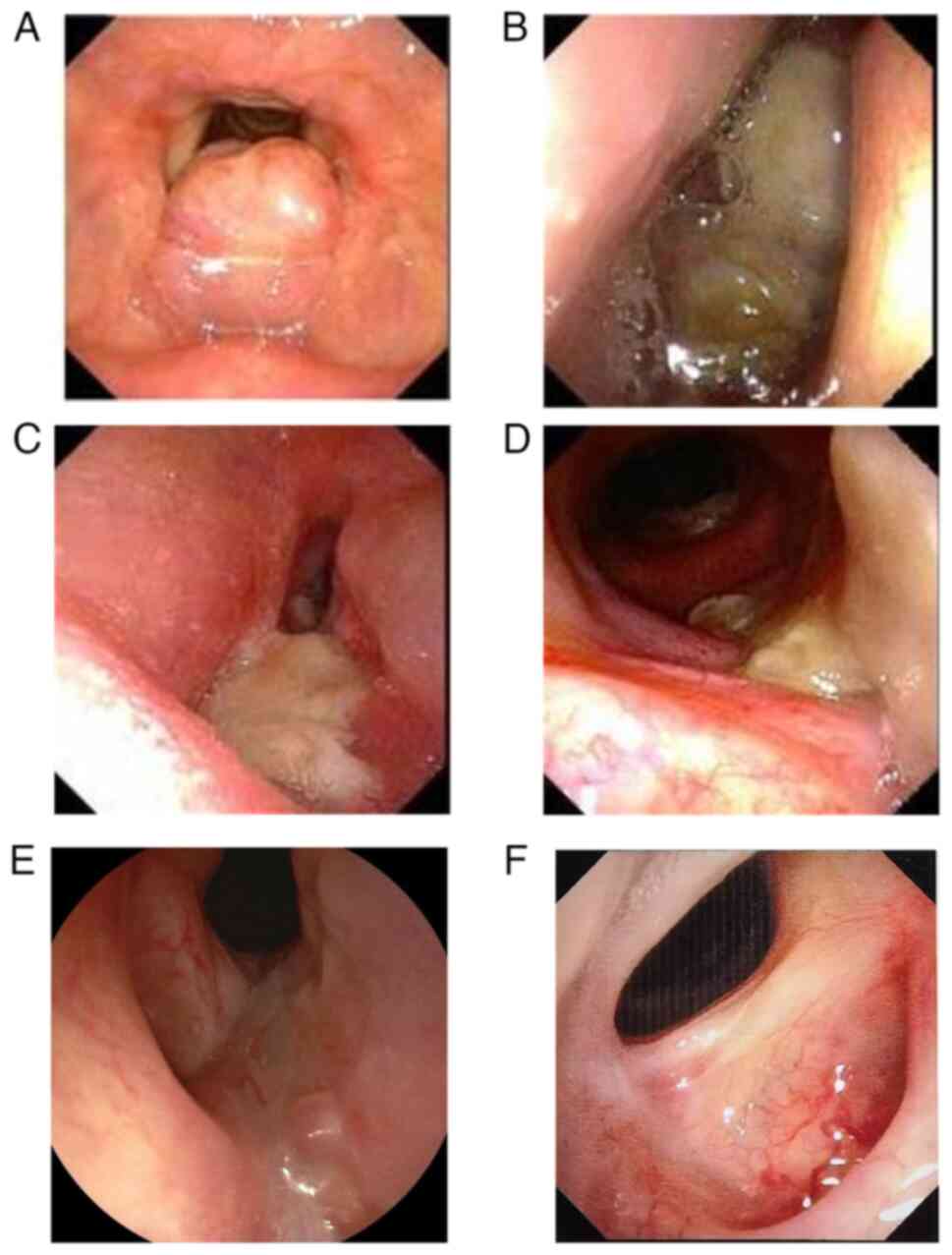
hospital admission. In addition, laryngoscopy followed by biopsy
was performed at the tumor site. Laryngoscopic images were captured
at 1 month and 1 day prior to surgery. The tumor displayed a
polypoid growth pattern, occupying a substantial portion of the
glottis with localized expansion, smooth surface and absence of
evident ulceration or secretion (Fig.
2A and B).
The significant increase in tumor size within <1
month between both laryngoscopic examinations aligned with the
findings from previous imaging studies and further underscored the
characteristic features of sarcomatoid carcinoma of the larynx,
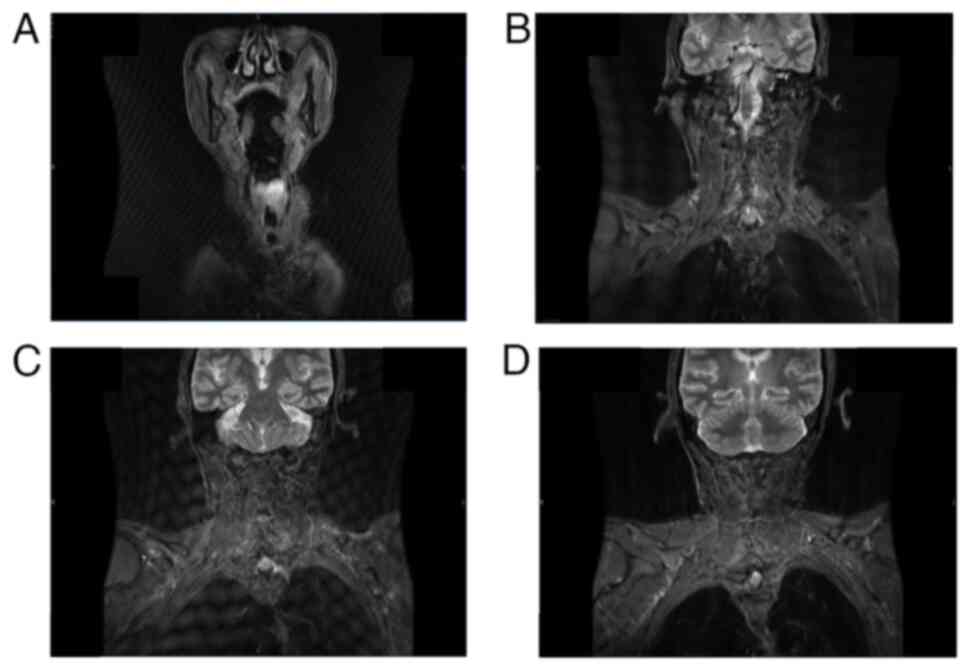
namely high malignancy and rapid progression. Then, at 5 days prior
surgery the patient was subjected to neck magnetic resonance
imaging scan with both plain and enhanced scans. The results showed
that the tumor size was ~2.8×1.9 cm2 (Fig. 3A-D), which signified a significant
increase compared with the spiral CT results obtained 1 month
prior, thereby highlighting the rapid tumor progression rate. In
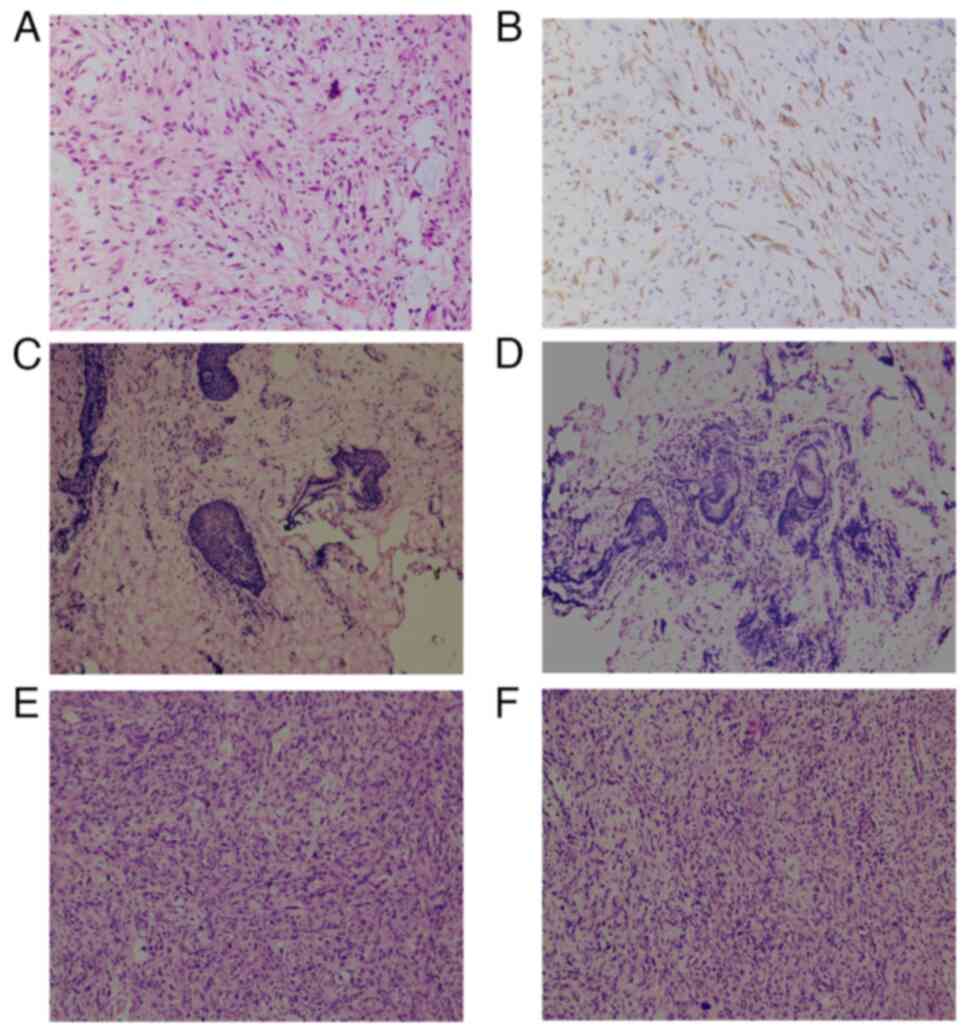
addition, immunohistochemical pathological analysis of preoperative
outpatient tumor biopsy sections taken 1 month prior to surgery
under local anesthesia was performed using rapid paraffin-embedded
tissue sections [Fig. 4A, Image 1
of the preoperative biopsy paraffin section indicating nuclear
atypia and typical spindle-shaped cells; Fig. 4B, Image 2 of the preoperative biopsy
immunohistochemistry showing positivity for cytokeratin (CK) and
vimentin]. Eventually, based on its morphology and
immunophenotyping, the patient was diagnosed with laryngeal
sarcomatoid carcinoma. The laryngeal tumor was classified as
T2N0M0, according to the established criteria of the TNM staging
system (19).
Based on the aforementioned findings, the patient
underwent partial laryngectomy and left neck lymph node dissection
with concurrent functional reconstruction of the larynx under
general anesthesia. The surgical procedure was carried out as
follows: A transverse incision in the shape of a ‘T’ was created
using a tungsten needle, thus gradually dissecting through the
layers of the skin, subcutaneous tissue and platysma myoides. The
left sternocleidomastoid muscle was then carefully separated to
access and examine the lymph nodes adjacent to the carotid sheath
for clearance purposes. No significantly enlarged lymph nodes were
identified during this process. To expose the thyrohyoid membrane,
an incision was made on the thyroid cartilage, cutting along the
midline. From there, the incision was continued downwards to reach
the cricoid membrane. Subsequently, a vertical incision at the
posterior part of the thyroid cartilage on the side of the tumor
was created, while preserving a narrow strip of cartilage, 3–5 mm
in width, connecting its upper and lower angles. The laryngeal
ventricle was accessed from the contralateral side through a
cartilage incision, thus revealing an extensive neoplasm involving
the left laryngeal ventricle, the vestibular fold and the vocal
cord. The tumor was excised at a vertical angle and specimens of
the left upper, left lower, right and posterior margins were
collected for intraoperative frozen section analysis. The analysis
results were all negative for malignancy. The vocal fold function
was ultimately restored through the use of absorbable thread to
suture the thyroid cartilage membrane, reconstruction of the
laryngeal cavity with a strap muscle flap and subsequent alignment
suturing of the anterior strap muscles.
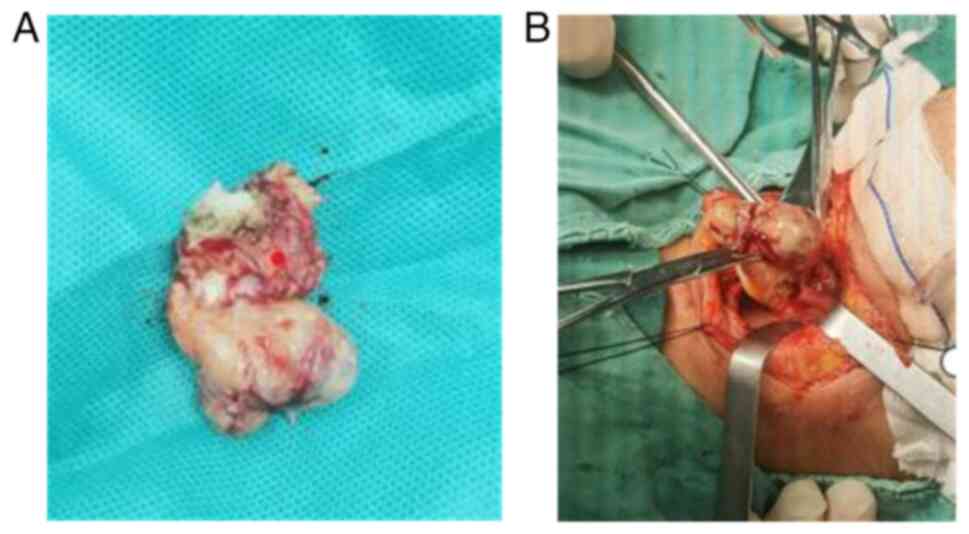
The tumor images captured intraoperatively revealed
that the tumor was spherical in shape with distinct sarcoma-like
characteristics, completely occupying the laryngeal space (Fig. 5A and B). In addition, frozen section
pathology examinations of the tumor margin tissue revealed that
there were no cancer cells, thus indicating that complete resection
was achieved. The results of the intraoperative frozen section
biopsy of the upper left, lower left, right and posterior margins
of the tumor are depicted in Fig. 4C
and D.
Postoperatively, histopathological analysis of
paraffin sections verified the diagnosis as laryngeal sarcomatoid
carcinoma without any evidence of cancer cells in the lymph nodes
[paraffin embedding of tissues (10% neutral formalin; temperature,
25°C; duration, 24 h), immunohistochemical sections were prepared
with a thickness of 3 µm and routine HE staining with a thickness
of 4 µm; blocking reagent, 3% H2O2;
temperature, 37°C; duration, 4 min (BenchMark ULTRA IHC/ISH
Staining Module, Ventana Medical Systems, Inc., used according to
the manufacturer's instructions); microscope, Leica DM1000LED
(Leica Microsystems GmbH].
More specifically, the postoperative pathological
and immunohistochemical analyses were performed using monoclonal
antibodies, special staining [Gomori's silver ammonium hydroxide
staining method; Henan Sainuote Biotechnology Co.; Yu Zheng Food
and Drug Administration Equipment Production Record no. 20140010
(updated)] and enzyme histochemistry (Fig. 4E and F). The tumor tissue was
positive for the epithelial immunohistochemical marker CK and the
sarcomatoid tissue-related marker vimentin, thus verifying the
diagnosis of laryngeal carcinosarcoma. No tumor cells were found in
the neck lymph node biopsy, thus suggesting that metastasis did not
occur in the neck lymph nodes. The immunohistochemical protocol
referred to the study by De Stefani et al (6) and Heidarian and Wenig (17) and experimental and antibody details
are provided in Fig. S1.
The reticulin staining was positive (temperature,
25°C; duration, potassium permanganate solution oxidized for 5 min;
oxalic acid solution bleached for 1–3 min; ammonium iron sulfate
solution stained for 3–5 min; silver ammonia solution stained for
3–5 min; formaldehyde solution restored for 2–3 min; gold chloride
solution reacted for 30 sec; sodium thiosulfate solution reacted
for 2 min).
The patient received symptomatic supportive therapy
after surgery and recovered well. The patient was discharged on the
10th day after surgery. Laryngoscopic follow-up examinations were
performed on days 7 and 20, and on the 3rd and 6th months after
surgery (Fig. 2C-F). The results
showed good healing of the surgical site, with no signs of tumor
recurrence. Therefore, after 20 days of surgery, the follow-up
laryngoscopy showed good postoperative recovery. Consequently,
radiotherapy was deemed unnecessary. Subsequent follow-up
examinations in June 2024, the 6th month after surgery, indicated
significant improvement in the patient's condition. Currently,
there is no evidence of tumor recurrence or metastasis.
Discussion
The nature of sarcomatoid carcinoma has long been a
subject of controversy. Several hypotheses have been proposed
regarding its histogenesis, including the theories of metaplasia,
collision, embryonic remnants and pluripotent stem cells. As a
result, there are multiple terms used to describe sarcomatoid
carcinoma, including carcinosarcoma, pleomorphic carcinoma, spindle
cell carcinoma, carcinoma in a sarcomatoid stroma and sarcomatoid
carcinoma (20,21). Currently, there is a growing
consensus on the transformation of squamous epithelial cancer into
sarcomatoid components. Therefore, sarcomatoid carcinoma is now
widely accepted as the preferred terminology.
In a previous retrospective study of 103 patients
with sarcomatoid carcinoma in the head and neck region, the
proportion of laryngeal cancer was the second highest (17.5%),
behind only to that of oral cavity cancer (63.1%) (16). Between 2004 and 2007, a total of 171
spindle cell tumors were reported at the pathology department of
this hospital (Tata Memorial Hospital, Parel, Mumbai, India), with
103 cases diagnosed as sarcomatoid carcinoma, accounting for ~70%
(16). Among them, 95% of patients
had symptoms lasting <1 year. Follow-up data from 39 patients
confirmed eight cases of recurrence, two cases of distant
metastasis and three deaths. The most common sites of metastasis
were the lungs (4), followed by the
lymph nodes (16). The metastatic
components included conventional squamous cell carcinoma,
sarcomatoid carcinoma or a combination of both (17). Sarcomatoid carcinoma predominantly
affects the glottis within the larynx, accounting for ~72% of all
cases (4). Hoarseness of voice is
the most common initial symptom of sarcomatoid carcinoma. However,
coughing and breathing difficulties can also occur in the later
stages (18). Another study also
reported a mortality rate ranging from 18 to 32% for this disease
(16). In the present study, the
follow-up period was still short and therefore further monitoring
of prognosis is needed. Sarcomatoid tumors often present as
polypoid growths or ulcerative lesions, which is consistent with
the findings of the large polypoid protrusions within the airway
observed in the present case. Sarcomatoid carcinoma usually occurs
between the ages of 20–90 years, mainly affecting men, while the
highest incidence is observed in individuals aged 50–60 years
(16). Consistently, in the present
study the case of male patient aged between 50 and 60 years was
reported.
There are several risk factors associated with the
development of sarcomatoid carcinoma, including tobacco use (both
smoking and chewing), alcohol consumption, exposure to radioactive
substances and contact with toxic chemicals. Among these risk
factors, chewing tobacco is the most significant, followed by
smoking (16). In this particular
case, the patient had a prolonged history of smoking, which aligns
with previous findings.
Sarcomatoid carcinoma typically presents as a large
polypoid neoplasm, with or without the presence of ulceration
(22). Fibrinogen deposits can be
also present on the surface (4). A
case study documented a massive tumor-like carcinoma lesion in the
throat, with a volume of 6×5×3 cm3 (3). In the present study, the tumor size
was 2.8×1.9 cm2. Under microscopic examination,
sarcomatoid carcinoma displays prominent atypical spindle-shaped
and polygonal cells, with a diffuse distribution pattern. In
particular areas with transitional zones, nest-like structures
could occasionally be observed.
In cases where conventional squamous cell carcinoma
components cannot be identified histologically, the diagnosis of
the disease primarily relies on rapid paraffin sectioning combined
with immunohistochemistry (17).
However, in a previous study, sarcomatoid carcinoma was
misdiagnosed as vocal cord polyps or other tumors based solely on
rapid paraffin sections (9). The
monoclonal nature of carcinosarcoma cells has been well
established, thus supporting their origin from the transformation
of squamous cell carcinoma into sarcomatoid differentiation. It has
been reported that these cells exhibit positive expression of
several epithelial-related immunohistochemical markers, including
CK(AE1/AE3), epithelial membrane antigen, keratin (K)I and K18
(5–7). Additionally, carcinosarcoma cells can
display positivity for the sarcomatoid tissue-related
immunohistochemical markers, vimentin and K (1,2).
However, the occasional aberrant expression of mesenchymal markers
can also lead to misdiagnosis. Furthermore, emerging evidence has
suggested that sarcomatoid carcinoma cells can carry intricate
genetic alterations. Therefore, Choi et al (1) reported a consistent phenomenon of
heterozygous deletion or retention in 80% of sarcomatoid carcinoma
cases. Furthermore, the study (1)
supported the notion that sarcomatoid carcinoma could be evolved
from conventional squamous cell carcinoma, thus verifying the
malignant nature of the sarcomatoid component, eventually
supporting the sarcomatoid transformation-related molecular
progression. Ki67 serves as an indicator of cellular proliferation.
Therefore, a higher Ki67 rate is associated with poorer tissue
differentiation, accelerated cell growth and enhanced tumor
development (9). In the current
case, the Ki67 expression rate was 70%, accompanied by rapid tumor
growth over a short period of time. The aforementioned findings
clearly verified the rapid growth of the sarcomatoid tumor.
Therefore, an extended follow-up period is necessary.
As widely acknowledged, early tumor diagnosis plays
a pivotal role in distinguishing sarcomatoid tumors from other
benign and malignant tumors, such as leiomyosarcoma, malignant
fibrous histiocytoma, reactive or benign spindle cell
proliferation, malignant peripheral nerve sheath tumor and synovial
sarcoma (monophasic type) (23).
Therefore, the early diagnosis directly affects the extent of
surgical intervention and treatment approach. The diagnostic
criteria for distinguishing sarcoma from other types of cancer can
be as follows (23): i) Malignant
fibrous histiocytoma exhibits a complex cellular composition with
pleomorphism, primarily consisting of fibroblasts and histiocytes
arranged in a ‘spoke-wheel’ pattern. These tumor cells do not
commonly express CK. ii) Leiomyosarcoma is characterized by larger
and tightly arranged cells, with frequent mitotic figures.
Immunohistochemical staining shows positivity for
diethylstilbestrol and actin expression, but not for CK. iii)
Malignant peripheral nerve sheath tumor presents spindle-shaped
tumor cells with wavy or dot-like nuclei, without significant
atypia. Immunohistochemical testing commonly displays positive
expression of S100, Leu-7 and myelin basic protein (23). Pathologists should also be aware of
reported cases of laryngeal carcinosarcoma with heterologous of
striated muscle cells components (3), as this information is significant in
the field.
Currently, there are no particular treatment
guidelines or expert consensus available for laryngeal
carcinosarcoma. However, surgical resection is considered the
primary treatment approach, with radiotherapy being recommended as
an adjunctive treatment option based on staging (24,25).
It has been proposed that postoperative radiotherapy can be
beneficial for patients with positive surgical margins, since their
survival outcomes are comparable with those with negative ones
(26). However, a previous study
reported rapid systemic metastasis in patients with laryngeal
sarcomatoid carcinoma following radiotherapy (27). By contrast, a retrospective analysis
compared the data of 187 patients with laryngeal sarcomatoid
carcinoma treated solely by surgery with those of patients who
underwent surgery combined with postoperative radiotherapy, with a
follow-up period of 7.7 and 6.7 years, respectively. The analysis
revealed that the former had an improved prognosis (4). Several proponents advocate primary
local radiotherapy for patients with stage T1 and T2 glottic
carcinoma, aiming to optimize vocal function preservation. For
patients with stage T3 and T4 glottic carcinoma, partial or total
laryngectomy is recommended as the primary treatment modality,
accompanied by postoperative radiotherapy (4). A study by the Mayo Clinic indicated
that surgical treatment alone for advanced laryngeal sarcomatoid
carcinoma had a higher recurrence rate, reaching 39% (8). According to previous reports, the
5-year survival rate of patients with laryngeal sarcomatoid
carcinoma after surgery can exceed 70% (3,4,28).
The reasons for the previous two pathological
diagnosis errors can be as follows: i) According to the theory
supported by the majority of studies (1–8),
laryngeal sarcomatoid carcinoma can evolve from squamous cell
carcinoma. The first two events can occur during the process of
epithelial hyperplasia prior its differentiation into cancer.
Therefore, only inflammatory granulomatous lesions can be observed
on the pathological examination. ii) During the early stage of the
disease, the tumors are characterized by a small volume. Therefore,
it is difficult to obtain tissue samples. The pathological tissue
sampling is relatively superficial, resulting in failure to obtain
truly cancerous tissues or obtaining very few ones. The specimens
mainly consist of inflammatory tissues of the surface of the tumor,
leading to misdiagnosis. In addition, early throat tumors exhibit
well-defined boundaries, a smooth surface and small dimensions, and
they can be therefore misdiagnosed as benign tumors. And iii) the
main factor leading to misdiagnosis is the lack of
immunohistochemical analysis, which is required to identify rapidly
progressing vocal cord lesions.
In the present study, the patient underwent three
consecutive vocal cord tumor resections within a short period of
time. However, it was unacceptable that immunohistochemical
examination was not performed in the first two surgeries. Without
these tests, establishing a definitive diagnosis and determining
whether the subsequent development of sarcomatoid carcinoma in the
surgical area was due to missed diagnoses in the previous
pathologies or simply due to disease progression could be
challenging. Therefore, due to the lack of evidence, the cause of
sarcomatoid carcinoma cannot be determined. The literature review
highlighted that there can be a significant misdiagnosis rate in
cases where laryngeal sarcomatoid carcinoma is misdiagnosed as
vocal cord polyps or other types of tumors, followed by surgical
resection (10). Therefore,
clinicians should pay close attention to the management of
recurrent vocal cord polyps or masses, particularly in patients
without habitual voice use and with a prolonged history of smoking.
Special consideration should be given in cases where rapid growth
of vocal cord masses is observed. The tissue should be excised
intact for paraffin section examinations, followed by
immunohistochemistry, to rule out conditions, such as sarcomatoid
carcinoma. Further surgical resection should be considered based on
the results of postoperative pathology. Clarifying the nature of
the tumor necessitates the utilization of intraoperative frozen
section pathological tests for guidance, while ensuring that the
tumor margin tissue is sent for pathological examination to further
ensure complete tumor resection.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
This study was funded by The Key Project of the Youth Doctoral
Program at the Second Affiliated Hospital of the Army Military
Medical University: Screening and Validation of Urinary Protein
Biomarkers for Obstructive Sleep Apnea-Hypopnea Syndrome (grant no.
2023YQB031).
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
AD and XZ conceived and designed the work. DJ, XL
and LZ acquired the data. JY, BL and XZ analyzed and interpreted
the data. DJ and XL drafted the manuscript. All authors read and
approved the final manuscript. DJ and XL confirm the authenticity
of all the raw data.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written consent from the patient has been obtained
for all quoted information and associated patient images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Choi HR, Sturgis EM, Rosenthal DI, Luna
MA, Batsakis JG and El-Naggar AK: Sarcomatoid carcinoma of the head
and neck: Molecular evidence for evolution and progression from
conventional squamous cell carcinomas. Am J Surg Pathol.
27:1216–1220. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Barnes L: Surgical pathology of the head
and neck. vol. 1. 3rd ed. CRC Press; 2008, pp. 174–181
|
|
3
|
Singh RK, Sinha R, Singh A, Suman S and
Priya M: Huge carcinosarcoma of the endolarynx: A rare tumour with
unusual presentation. Indian J Surg Oncol. 8:227–230. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Thompson LD, Wieneke JA, Miettinen M and
Heffner DK: Spindle cell (sarcomatoid) carcinomas of the larynx: A
clinicopathologic study of 187 cases. Am J Surg Pathol. 26:153–170.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lewis JE, Olsen KD and Sebo TJ: Spindle
cell carcinoma of the larynx: Review of 26 cases including DNA
content and immunohistochemistry. Hum Pathol. 28:664–673. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
De Stefani A, Boffano P and Bongioannini
G: Review of histologic and immunohistochemical features of spindle
cell carcinomas (Carcinosarcomas) of the larynx. J Craniofac Surg.
5:e430–e433. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Boamah H and Ballard B: A case report of
spindle cell (sarcomatoid) carcinoma of the larynx. Case Rep Med.
2012:3702042012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Gamez ME, Jeans E, Hinni ML, Moore E,
Young G, Ma D, McGee L, Buras MR and Patel SH: Outcomes and
patterns of failure of sarcomatoid carcinoma of the larynx: The
mayo clinic experience. Laryngoscope. 128:373–377. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wu Y, Zhang F, Liu Y, Wang X and Huang D:
Clinical analysis of 6 cases of laryngeal carcinosarcoma and
sarcomatoid carcinoma. Chinese Journal of Otolaryngology and
Cranial Base Surgery,. 29:19–25. 2023.(In Chinese).
|
|
10
|
Tian Y, Su K, Wang S, Tong W, Zhang X, Wei
M and Feng Q: Sarcoma like carcinoma of the throat: a report of 5
cases and literature review(J). J Jilin Univ (Medical Edition).
3:697–700. 2019.
|
|
11
|
Ma Y, Li W, Li Z, Chen J, Wang H, Jiang T
and Zhu J: Immunophenotyping of pulmonary sarcomatoid carcinoma.
Front Immunol. 20:9767392022. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Zombori-Tóth N, Kiss S, Oštarijaš E,
Alizadeh H and Zombori T: Adjuvant chemotherapy could improve the
survival of pulmonary sarcomatoid carcinoma: A systematic review
and meta-analysis. Surg Oncol. 44:1018242022. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Wang L, Zhang J, Chen X, Liang M, Li S,
Zhou W and Cao J: Pulmonary sarcomatoid carcinoma mimicking pleural
mesothelioma: A case report. Medicine (Baltimore). 100:e278132021.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Terra S, Roden AC, Yi ES, Aubry MC and
Boland JM: Loss of methylthioadenosine phosphorylase by
immunohistochemistry is common in pulmonary sarcomatoid carcinoma
and sarcomatoid mesotheliomap. Am J Clin Pathol. 157:33–39. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wu S, Wu S, Liao X, Zhou C, Qiu F, Wang C
and Zhong W: Pembrolizumab combined with anlotinib improves
therapeutic efficacy in pulmonary sarcomatoid carcinoma with TMB-H
and PD-L1 expression: A case report and literature review. Front
Immunol. 14:12749372023. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Viswanathan S, Rahman K, Pallavi S, Sachin
J, Patil A, Chaturvedi P, D'Cruz A, Agarwal J and Kane SV:
Sarcomatoid (Spindle Cell) carcinoma of the head and neck mucosal
region: A clinicopathologic review of 103 case from a tertiary
referral cancer centre. Head Neck Pathol. 4:265–275. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Heidarian A and Wenig BM: The most common
mistake in laryngeal pathology and how to avoid it. Head Neck
Pathol. 15:130–137. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Roy S, Purgina B and Seethala RR: Spindle
cell carcinoma of the larynx with rhabdomyoblastic heterologous
element: A rare form of divergent differentiation. Head Neck
Pathol. 7:263–267. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Caudell JJ, Gillison ML, Maghami E,
Spencer S, Pfister DG, Adkins D, Birkeland AC, Brizel DM, Busse PM,
Cmelak AJ, et al: NCCN Guidelines® Insights: Head and
Neck Cancers, Version 1.2022. J Natl Compr Canc Netw. 20((3)):
224–234. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ouyang Y, Wang B, Wang C, Chen Q and Liu
L: One case of early infiltrating squamous cell carcinoma of the
larynx with sarcomatoid stromal response. Journal of Clinical
Otolaryngology Head and Neck Surgery. 4:188–189. 2011.(In
Chinese).
|
|
21
|
Katase N, Tamamura R, Gunduz M, Murakami
J, Asaumi J, Tsukamoto G, Sasaki A and Nagatsuka H: A spindle cell
carcinoma presenting with osseous metaplasia in the gingiva: A case
report with immunohistochemical analysis. Head Face Med. 4:282008.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Cardesa A and Zidar N: Pathology and
genetics of head and neck tumours. 3rd Edition. Volume 9. Barnes L,
Eveson JW, Reichart P and Sidransky D: IARC press; Lyon: 2005, pp.
127
|
|
23
|
Osorio-Velásquez A, Chiesa-Estomba CM,
Betances-Reinoso FA, Miguel-Fraile MP and Ortiz-Rey JA: Sarcomatoid
carcinoma of larynx. A histological challenge. Rev Esp Patol.
51:30–33. 2018.PubMed/NCBI
|
|
24
|
Ballo MT, Garden AS, El-Naggar AK,
Gillenwater AM, Morrison WH, Goepfert H and Ang KK: Radiation
therapy for early stage (T1-T2) sarcomatoid carcinoma of true vocal
cords: Outcomes and patterns of failure. Laryngoscope. 108:760–763.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kelly MD, Hahn SS, Spaulding CA, Kersh CR,
Constable WC and Cantrell RW: Definitive radiotherapy in the
management of stage I and II carcinomas of the glottis. Ann Otol
Rhinol Laryngol. 98:235–239. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Su HH, Chu ST, Hou YY, Chang KP and Chen
CJ: Spindle cell carcinoma of the oral cavity and oropharynx:
Factors affecting outcome. J Chin Med Assoc. 69:478–483. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Onishi H, Kuriyama K, Komiyama T,
Yamaguchi M, Tanaka S, Marino K, Sano N, Araki T and Miyata K: T1N0
laryngeal sarcomatoid carcinoma that showed rapid systemic
metastases after radical radiotherapy: A case report and review of
literature. Am J Otolaryngol. 26:400–402. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Sun RX, Zhao Y, Yu TP and Huang S:
Sarcomatoid carcinoma of larynx: one case report. J Clin
Otorhinolaryngol Head Neck Surg. 28:1444–1445. 2014.(In
Chinese).
|