Introduction
Glioblastoma (GBM) is the most common malignant
primary brain tumor, with a poor prognosis and a median survival
time of 12–16 months (1–3). The majority of patients with this
cancer experience local progression during the disease course.
Extracranial metastasis (ECM) is a rare occurrence in GBM, with an
estimated incidence of 0.4–2.0%. Common metastatic sites include
the lungs, lymph nodes, liver and spine (4,5).
Despite its rarity, ECM has been reported in several case studies;
however, its underlying mechanism is not fully understood (3–6). The
prognosis for patients with ECM is poor due to limited treatment
options. Current standard treatment methods include maximal safe
surgical resection followed by adjuvant radiotherapy and
chemotherapy, the latter of which typically consists of the oral
alkylating agent temozolomide (Stupp regimen) (6,7). The
present report documents a case of GBM with spinal metastasis after
surgery in a patient who was treated with the standard therapeutic
regiment, including tumor treating fields (TTF), achieving an
overall survival time of 28 months. The present study describes a
rare occurrence of extracranial metastasis, highlighting the need
for further investigation into potential mechanisms and novel
therapeutic strategies.
Case report
A 31-year-old female patient presented with a
1-month history of recurrent headaches and dizziness. In November
2020, the patient began experiencing headaches and dizziness,
characterized by a sensation of fullness in the head accompanied by
lightheadedness, gradually worsening over time. Therefore, in
December 2020, the patient visited the Department of Neurosurgery,
Fuzong Clinical Medical College of Fujian Medical University
(Fuzhou, China). The patient had no history of immunosuppressive
drug use, intravenous drug abuse, organ transplantation or
high-risk sexual behavior. Additionally, there were no other
sensory or motor deficits. Routine laboratory tests revealed that
all parameters were within normal ranges, with serological tests
for human immunodeficiency virus, hepatitis B virus and hepatitis C
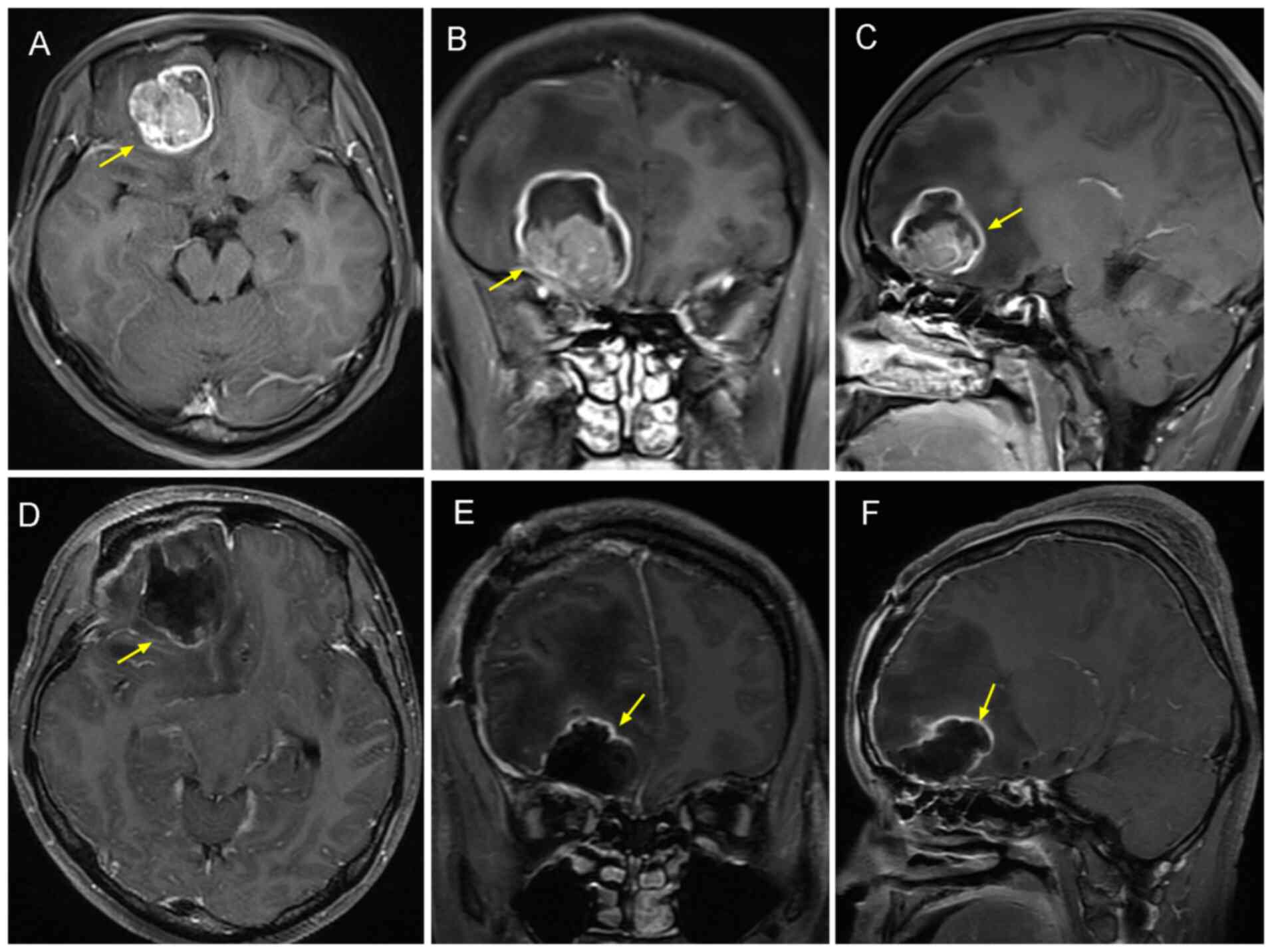
virus being negative. Brain MRI with contrast revealed a right
frontal lobe mass measuring 3.8×3.4 cm (Fig. 1). In addition, high-signal intensity
on T2-weighted imaging (T2WI), a slightly low signal on T1-weighted
imaging (T1WI) and a slightly high signal on diffusion-weighted
imaging, with a surrounding area of patchy edema, were observed.
Chest CT and abdominal ultrasound did not yield abnormalities, and
no other space-occupying lesions were found in other organs.
A craniotomy was subsequently performed and the
lesion was completely resected. Formalin-fixed, paraffin-embedded
tissue sections (4 µm thick) were stained with hematoxylin and
eosin (H&E) using standard protocols. Briefly, tissues were
fixed in 10% neutral buffered formalin at room temperature for 24
h, followed by routine processing. Sections were stained with
hematoxylin at room temperature for 5 min, rinsed, and
counterstained with eosin for 1 min. Slides were examined under a
bright-field microscope) revealed extensive necrosis with scattered
pleomorphic cells, consistent with GBM, specifically giant cell
GBM. Molecular pathological report results of the right frontal
lobe (Table I) showed isocitrate
dehydrogenase 1 (IDH1) wild-type and O6-methylguanine-DNA
methyltransferase (MGMT)-positive methylation, confirming the
diagnosis of GBM (World Health Organization grade IV) (8). The final diagnosis was therefore GBM
(IDH wild-type and MGMT methylation-positive).
 | Table I.Immunohistochemistry results of the
right frontal lobe mass provided by the Department of
Pathology. |
Table I.
Immunohistochemistry results of the
right frontal lobe mass provided by the Department of
Pathology.
| Antibody type | Staining
location | Staining
intensity | Description |
|---|
| H3K27Me3 | Nucleus | +++ |
|
| Ki-67 | Nucleus | 60% |
|
| Vimentin | Cytoplasm | ++++ |
|
| Glial fibrillary
acidic protein | Cytoplasm | +++ |
|
| Oligodendrocyte
transcription factor 2 | Nucleus | ++ |
|
| p53 | Nucleus | 90% |
|
| CD34 | Membrane | Small foci+ |
|
| ATRX | Nucleus | + | Mutation |
| PTEN | Cytoplasm | +++ |
|
| S-100 |
Cytoplasm/nucleus | ++ |
|
| Synaptophysin | Cytoplasm | + |
|
The postoperative chemoradiotherapy regimen was as
follows: i) Radiation therapy, 2 Gy/session 5 days per week for 6
weeks, with a total dose of 60 Gy; and ii) temozolomide, 75
mg/m2 per day 7 days per week, followed by maintenance
temozolomide at 150 mg/m2 for 5 days every 28 days for a
total of 6 cycles. During the chemoradiotherapy, the patient
experienced grade III chemotherapy-induced myelosuppression, which
improved after symptomatic treatment, such as white blood cell
stimulating therapy . In total, ~4 months after diagnosis, the
treating physician decided to add TTF to the standard Stupp
regimen, given the patient's tolerance to the treatment. In
addition, ~15 months after diagnosis, after a multidisciplinary
team consultation, bevacizumab 10 mg/kg was added to the treatment
plan, administered every 21 days for 13 cycles. Follow-up brain MRI
scans every 2–3 months showed no recurrence of the tumor.
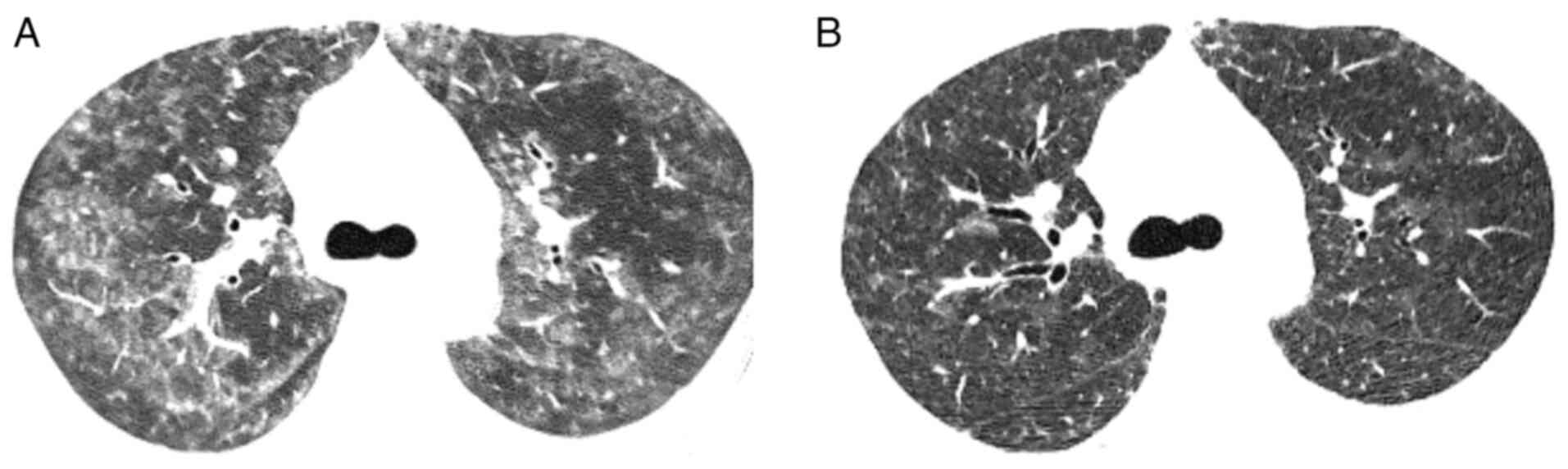
At 23 months post-surgery, the patient contracted
coronavirus disease 2019 (COVID-19) and developed severe bilateral
pneumonia. After receiving a 10-day course of corticosteroid
therapy (5 mg dexamethasone) for COVID-19 at the First Affiliated
Hospital of Fujian Medical University, the patient recovered and
was transferred to the 900th Hospital of the PLA for further
treatment of GBM (Fig. 2). At 25
months post-surgery, the patient developed facial swelling and
bilateral lower limb edema with pain. Although the patient had
received dexamethasone treatment, the potential adverse impact of
corticosteroids on GBM progression could not be excluded, and
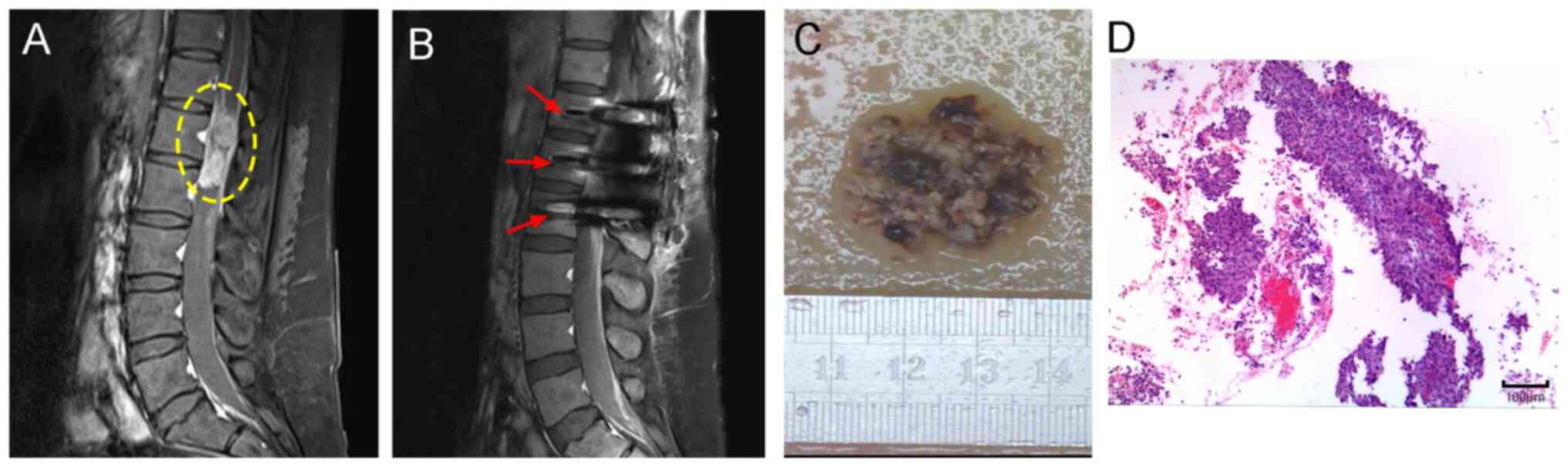
recurrence or metastasis was suspected. Therefore, an MRI scan of
the lumbar spine (Fig. 3C) was
performed, revealing an abnormal oval-shaped signal at the L1-L2
vertebral level with dimensions of 1.6×2.4×4.3 cm. The lesion
showed isointensity on T1WI, a slightly high signal on T2WI and a
number of low signals at the edges. No metastasis was observed in
other locations. The suspicion was that the patient was suffering
from a malignant GBM with ECM, as the patient exhibited symptoms
indicative of spinal metastasis, such as persistent lower back
pain, recurrent flatulence and ultimately, quadriplegia. Despite
the severity of the condition, the patient opted to continue
treatment. At 26 months after the initial diagnosis of GBM, the
patient underwent further surgery for resection of the L1-L2
vertebral canal tumor. The strong vimentin expression, high Ki-67
proliferation index, ATRX loss, p53 mutation, and retained H3K27Me3
are all consistent with glioblastoma. These features, alongside the
overall pattern of marker expression, strongly suggest that the
lumbar spinal metastasis is derived from a primary glioblastoma
(Table II), confirming the
diagnosis of ECM (Fig. 3D).
| Table II.Molecular pathological report results
of lumbar spinal tumor. |
Table II.
Molecular pathological report results
of lumbar spinal tumor.
| Antibody type | Staining
location | Antibody staining
intensity | Description |
|---|
| Vimentin | Cytoplasm | ++++ |
|
| Glial fibrillary
acidic protein | Cytoplasm | + | Focally scattered
positive |
| Somatostatin
receptor-2 | Cytoplasm | + |
|
| ATRX | Cytoplasm | + |
|
| Ki-67 | Nucleus | 80% |
|
| Integrase
interactor 1 | Nucleus | ++++ |
|
| S-100 | Nucleus | Few + |
|
| p53 |
Cytoplasm/nucleus | 80% | Mutant type |
| Epithelial membrane
antigen | Nucleus | Few + |
|
| H3K27Me3 | Cytoplasm | ++++ |
|
Postoperatively, the patient continued to experience
severe pain, with a Numerical Rating Scale (9,10)
score of 9. Despite receiving an intrathecal pain pump from the
Department of Anesthesiology, the pain persisted, with a Critical
Care Pain Observation Tool (11)
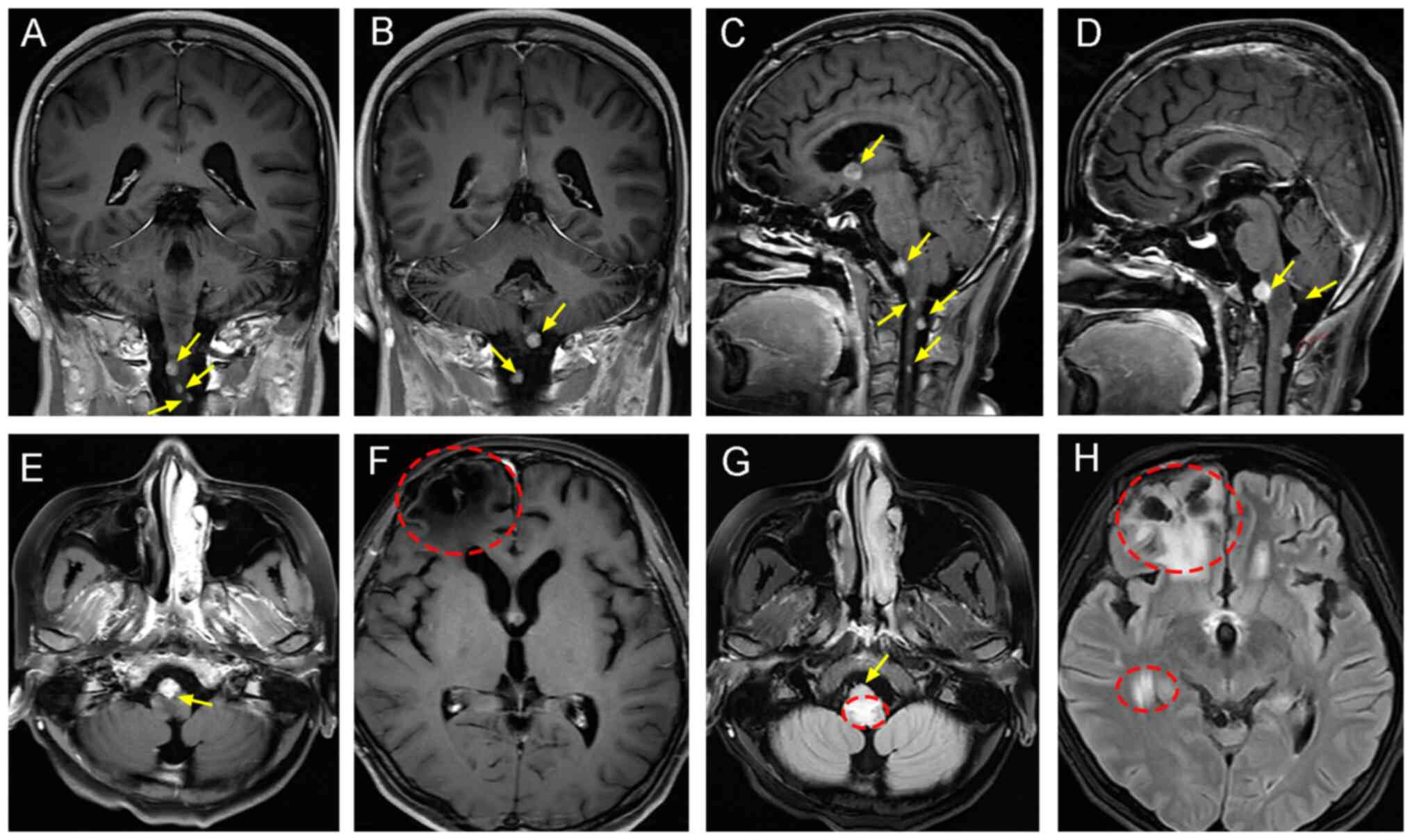
score of 8–9. The patient abandoned the treatment and opted for
conservative management limited to the maintenance of vital signs,
before succumbing to respiratory and cardiac arrest from multiple
site (brainstem) metastasis (Fig.
4). The survival time from diagnosis to mortality was 28
months, with a survival time of 2 months from ECM to mortality.
Discussion
GBM is the most common type of malignant brain
tumor, accounting for ~49% of primary malignant brain tumors in the
United States (1). The 5-year
overall survival rate is 6.8% (2)
and the prognosis is poor, with a median survival time of 12–16
months (3). One of the main
characteristics of GBM is its diffuse and highly invasive nature,
with postoperative recurrence being common. However, ECM is rare,
with an estimated incidence of 0.4–2.0%, and the most commonly
affected sites being the lungs, lymph nodes, liver and spine
(4,5). The rarity of ECM may be attributed to
the presence of the blood-brain barrier (BBB) and dura mater, and
the lack of a lymphatic system. The low incidence rate of ECM may
also be due to the short survival time of patients with GBM, who
will typically succumb to complications before ECM can occur
(12–15).
Although ECM is rare, cases of it continue to
emerge, with the proposed mechanisms including hematogenous spread
or direct seeding (16). Since the
first report in 1928 of glioma recurrence with pulmonary metastasis
(17), various types of glioma ECM
have been reported, with GBM being more common in comparison to
other primary intracranial tumors with ECM (18).
The mechanisms of ECM in GBM remain poorly
understood, but risk factors have been widely described, including
previous craniotomy or biopsy, ventriculoperitoneal shunt, younger
age, radiation therapy, prolonged survival time, genetic mutations,
tumor recurrence and the presence of gliosarcomatous components
(17). In total, 90% of reported
cases of ECM in GBM have undergone craniotomy. Hamilton et
al (19) previously suggested
that craniotomy can cause iatrogenic extracranial structural
pathways, including ventriculoperitoneal shunt procedures, which
can disrupt normal anatomical barriers, leading to tumor cell
dissemination through the bloodstream (20). Although the majority of ECM cases
are associated with surgery, there have also been reports of
patients who developed ECM prior to surgery (21). This occurrence is hypothesized to be
associated with various mechanisms, such as glioma angiogenesis
inhibition and escape during tumor chemoradiotherapy (22), where primary tumor growth is
suppressed but tumor cell invasion and proliferation increase near
the brain tissue. Piccirilli et al (23) previously reported 128 cases of GBM
with ECM, with a mean patient age of 40 years at the time of
diagnosis, patients without ECM had a mean age of 54 years at
diagnosis (24). Younger patients
are therefore hypothesized to be more likely to develop ECM
compared with older patients with chronic diseases, as they provide
more time for tumor cells to escape the brain and form distant
metastases (25,26). With advancements in treatment and
diagnostic technology, the survival time of patients with GBM has
increased, which also widens the time window for potential
metastasis. Prolonged survival increases the possibility of GBM
cells shedding into the lymphatic and circulatory systems (27,28).
Andersen et al (29)
reported that 7.8% of patients with primary gliomas that
metastasized to the meninges had sarcomatous components. It is
suggested that GBM with sarcomatous or mesenchymal features may
promote ECM (30). Additionally,
genomic studies (30–32) have reported associations with longer
survival in patients with GBM and mutations in TP53, RB1, ATRX,
PTEN, TERT and IDH1. The patient in the present case was
relatively young, underwent craniotomy and radiotherapy at initial
diagnosis, and had a longer survival time than average (12–16
months), consequently presenting risk factors for ECM. Furthermore,
the surgical specimen from the spinal canal resection clearly
demonstrated GBM dissemination.
ECM of GBM is relatively rare, with spinal cord
metastases demonstrating an incidence rate of 20–40% in post-mortem
examinations. This elevated incidence associates with the short
survival periods of patients (33–35).
The most frequent anatomical sites for spinal metastases involve
the lower thoracic, upper lumbar and lumbosacral junction regions
(36). The current case presented
with metastases at the L1-L2 spinal canal, consistent with these
documented locations.
The clinical manifestations of GBM are determined by
tumor location and proliferation rate. Spinal metastases typically
present with sensory symptoms, radicular pain, back pain,
paraparesis, quadriplegia, paraplegia and bowel/bladder dysfunction
with sexual impairment (37). The
most frequently reported symptom remains paraparesis, as previously
documented by Schwaninger et al (38), where it was predominantly observed
in younger patients. The present case developed these
characteristic spinal metastatic symptoms progressively in latter
disease stages, including persistent lumbar pain, recurrent
intestinal distension and eventual progression to complete
quadriplegia.
Patients with spinal metastases from GBM demonstrate
a median survival of ~1 year, typically succumbing within months of
symptom onset, reflecting the poor prognosis associated with this
condition. Regarding the treatment of GBM, it does not differ based
on histological subtype. The patient in the present case was
diagnosed with giant cell GBM (IDH wild-type and MGMT
methylated), where the treatment approach was consistent with that
of other histological subtypes. The standard treatment for GBM at
initial diagnosis includes surgery, temozolomide-based concurrent
radiotherapy and further adjuvant temozolomide therapy (6). Surgical resection allows for accurate
histopathological diagnosis, tumor gene profiling and a reduction
in tumor volume, which is beneficial for postoperative
radiotherapy. In addition, TTF provide low-intensity alternating
electric fields, which have been approved for use in combination
with temozolomide as an adjuvant treatment. TTF is primarily used
as an anti-mitotic therapy, with its use during temozolomide
maintenance being shown to extend survival time in patients with
supratentorial disease (7).
However, the high cost, treatment adherence issues and skin
toxicity are barriers to the clinical application of TTF. The
United States Food and Drug Administration has approved the use of
TTF as an option for eligible patients who are willing to undergo
this treatment. The patient in the present case started TTF therapy
~4 months after diagnosis, which may be one reason for the extended
survival time.
After standard concurrent chemoradiotherapy and
adjuvant chemotherapy, the majority of patients with GBM will
typically experience recurrence within 6 months (6). For recurrent or metastatic disease,
further surgical resection, re-irradiation, systemic treatments
(lomustine or bevacizumab), combination therapy or supportive care,
particularly for younger patients with good performance status, can
be considered (39,40). The treatment plan in the present
case, both at initial diagnosis and after recurrence, followed the
current treatment guidelines (41).
Regarding the use of bevacizumab for anti-angiogenesis in patients
with GBM, Lah et al (42)
suggests that this treatment is associated with early ECM in
patients with GBM (42), where
long-term use may increase tumor aggressiveness (43). To this effect, two large randomized
trials in 2014 confirmed that although bevacizumab prolonged
progression-free survival, it did not improve overall survival and
it increased the incidence of adverse events (hypertension and
thromboembolism) (44,45). The present patient underwent 13
cycles of bevacizumab treatment, but the condition worsened with
lumbar metastasis, and the possibility of bevacizumab-induced
hypoxia and tumor-associated macrophage involvement could not be
excluded. Due to the lack of notable therapeutic benefits from
bevacizumab (46), the European
Medicines Agency has rejected its use in patients with recurrent
GBM, and the present patient did not receive further bevacizumab
treatment.
Furthermore, the use of corticosteroids, such as
dexamethasone, may decrease the therapeutic efficacy of
chemotherapy and radiotherapy in GBM patients and potentially
shorten survival, thereby negatively impacting prognosis. This may
be due to the protective effect of dexamethasone against the
anti-proliferative action of radiotherapy and chemotherapy (which
causes genetic toxicity stress) (47). Corticosteroids can cause morbidity,
including steroid myopathy, immune dysfunction, adrenal
insufficiency and bowel perforation, and mortality through their
direct toxicity. Previous meta-analyses have shown that
corticosteroids can inhibit antitumor immune responses in glioma
and increase the risk of mortality in patients with GBM (48–51).
High blood glucose (52) and muscle
wasting (53) are risk factors for
poor survival outcomes, treatment discontinuation and decreased
progression-free survival time. The present patient received
dexamethasone treatment for COVID-19 pneumonia 23 months after the
initial surgery. However, no tumor recurrence was observed during
outpatient follow-ups. After 2 months of corticosteroid use, the
patient presented with bilateral lower limb edema and lumbar pain,
and was found to have distant lumbar metastasis. The possibility
that corticosteroids accelerated the tumor progression and
shortened the patient's survival time cannot be excluded.
ECM of GBM progresses rapidly, has a poor prognosis
and lacks a definitive treatment protocol. Despite using all
available treatment options, the present patient succumbed, with
only a 2-month survival time between the ECM diagnosis and
mortality. Compared with solid tumors, metastatic GBM presents with
notable treatment challenges in terms of biological factors, such
as the BBB, and the unique tumor and immune microenvironment
(54). Current research has focused
on immunotherapy and precision oncology, such as immune checkpoint
therapy (CD73) (55), chimeric
antigen receptor T-cell therapy (56) and TAT-Cx43266-283 (an Src-inhibiting
peptide with antitumor properties in preclinical GBM models)
(57). Nanomedicine offers
innovative diagnostic strategies for GBM, including the use of
nanoparticle-based contrast agents to enhance MRI resolution, and
nanosensors for detecting circulating tumor biomarkers with high
specificity and sensitivity. Magnetic nanoparticles or their
composites have proven effective in simultaneously inducing
ferroptosis and enabling MRI imaging, demonstrating remarkable
potential in the suppression of glioblastoma (GBM) (58,59).
In conclusion, although ECM in GBM is rare, its
prognosis is poor and the associated survival time is short;
therefore, surgeons should be vigilant regarding the possibility of
ECM. At present, surgical resection and concurrent
chemoradiotherapy remain the first-line treatments for GBM.
Therefore, achieving a gross total resection during surgery to
reduce the possibility of ECM should be prioritized. Several novel
therapies have shown promising results in cases of recurrence or
metastasis, but there remains a need for enhanced supportive care
and treatment to improve the patient's quality of life and survival
outcomes.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
PH, ML and ZL analyzed the data, and reviewed and
edited the manuscript. ML obtained medical images. ZL and MC
advised on patient treatment or analyzed patient data. MC and CC
contributed to the study methodology, supervision, validation,
reviewing and editing. PH, ML, ZL, MC and CC confirm the
authenticity of all the raw data. All authors have read and
approved the final version of the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
The husband of the patient provided written informed
consent for publication of the medical data and images.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
ECM
|
extracranial metastasis
|
|
GBM
|
glioblastoma
|
|
TTF
|
tumor treating fields
|
References
|
1
|
Schaff LR and Mellinghoff IK: Glioblastoma
and other primary brain malignancies in adults: A review. JAMA.
329:574–587. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ostrom QT, Cioffi G, Gittleman H, Patil N,
Waite K, Kruchko C and Barnholtz-Sloan JS: CBTRUS statistical
report: Primary brain and other central nervous system tumors
diagnosed in the United States in 2012–2016. Neuro Oncol. 21 (Suppl
5):v1–v100. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Linz U: Commentary on effects of
radiotherapy with concomitant and adjuvant temozolomide versus
radiotherapy alone on survival in glioblastoma in a randomised
phase III study: 5-year analysis of the EORTC-NCIC trial (Lancet
Oncol. 2009;10:459-466). Cancer. 116:1844–1846. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Pasquier B, Pasquier D, N'Golet A, Panh MH
and Couderc P: Extraneural metastases of astrocytomas and
glioblastomas: Clinicopathological study of two cases and review of
literature. Cancer. 45:112–125. 1980. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kalokhe G, Grimm SA, Chandler JP,
Helenowski I, Rademaker A and Raizer JJ: Metastatic glioblastoma:
Case presentations and a review of the literature. J Neurooncol.
107:21–27. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tan AC, Ashley DM, López GY, Malinzak M,
Friedman HS and Khasraw M: Management of glioblastoma: State of the
art and future directions. CA Cancer J Clin. 70:299–312. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Stupp R, Taillibert S, Kanner A, Read W,
Steinberg D, Lhermitte B, Toms S, Idbaih A, Ahluwalia MS, Fink K,
et al: Effect of tumor-treating fields plus maintenance
temozolomide vs maintenance temozolomide alone on survival in
patients with glioblastoma: A randomized clinical trial. JAMA.
318:2306–2316. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kurokawa R, Kurokawa M, Baba A, Ota Y,
Pinarbasi E, Camelo-Piragua S, Capizzano AA, Liao E, Srinivasan A
and Moritani T: Major changes in 2021 World Health Organization
classification of central nervous system tumors. Radiographics.
42:1474–1493. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Childs JD, Piva SR and Fritz JM:
Responsiveness of the numeric pain rating scale in patients with
low back pain. Spine (Phila Pa 1976). 30:1331–1334. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Rodriguez CS: Pain measurement in the
elderly: A review. Pain Manag Nurs. 2:38–46. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Li MMJ, Ocay DD, Larche CL, Vickers K,
Saran N, Ouellet JA, Gélinas C and Ferland CE: Validation of the
critical-care pain observation tool (CPOT) in pediatric patients
undergoing orthopedic surgery. Can J Pain. 7:21563322023.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Figueroa P, Lupton JR, Remington T, Olding
M, Jones RV, Sekhar LN and Sulica VI: Cutaneous metastasis from an
intracranial glioblastoma multiforme. J Am Acad Dermatol.
46:297–300. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Al-Ali F, Hendon AJ, Liepman MK,
Wisniewski JL, Krinock MJ and Beckman K: Oligodendroglioma
metastatic to bone marrow. AJNR Am J Neuroradiol. 26:2410–2414.
2005.PubMed/NCBI
|
|
14
|
Lun M, Lok E, Gautam S, Wu E and Wong ET:
The natural history of extracranial metastasis from glioblastoma
multiforme. J Neurooncol. 105:261–273. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kurdi M, Baeesa S, Okal F, Bamaga AK,
Faizo E, Fathaddin AA, Alkhotani A, Karami MM and Bahakeem B:
Extracranial metastasis of brain glioblastoma outside CNS:
Pathogenesis revisited. Cancer Rep (Hoboken). 6:e19052023.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Newton HB, Rosenblum MK and Walker RW:
Extraneural metastases of infratentorial glioblastoma multiforme to
the peritoneal cavity. Cancer. 69:2149–2153. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Davis L: SPONGIOBLASTOMA MULTIFORME OF THE
BRAIN. Ann Surg. 87:8–14. 1928.PubMed/NCBI
|
|
18
|
Liwnicz BH and Rubinstein LJ: The pathways
of extraneural spread in metastasizing gliomas: A report of three
cases and critical review of the literature. Hum Pathol.
10:453–467. 1979. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Hamilton JD, Rapp M, Schneiderhan T, Sabel
M, Hayman A, Scherer A, Kröpil P, Budach W, Gerber P, Kretschmar U,
et al: Glioblastoma multiforme metastasis outside the CNS: three
case reports and possible mechanisms of escape. J Clin Oncol.
32:e80–e84. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Terheggen HG and Müller W:
Extracerebrospinal metastases in glioblastoma. Case report and
review of the literature. Eur J Pediatr. 124:155–164. 1977.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Hoffman HJ and Duffner PK: Extraneural
metastases of central nervous system tumors. Cancer. 56 (7
Suppl):S1778–S1782. 1985. View Article : Google Scholar
|
|
22
|
Tuettenberg J, Grobholz R, Korn T, Wenz F,
Erber R and Vajkoczy P: Continuous low-dose chemotherapy plus
inhibition of cyclooxygenase-2 as an antiangiogenic therapy of
glioblastoma multiforme. J Cancer Res Clin Oncol. 131:31–40. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Piccirilli M, Brunetto GM, Rocchi G,
Giangaspero F and Salvati M: Extra central nervous system
metastases from cerebral glioblastoma multiforme in elderly
patients. Clinico-pathological remarks on our series of seven cases
and critical review of the literature. Tumori. 94:40–51. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Polley MY, Lamborn KR, Chang SM, Butowski
N, Clarke JL and Prados M: Conditional probability of survival in
patients with newly diagnosed glioblastoma. J Clin Oncol.
29:4175–4180. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wu W, Zhong D, Zhao Z, Wang W, Li J and
Zhang W: Postoperative extracranial metastasis from glioblastoma: A
case report and review of the literature. World J Surg Oncol.
15:2312017. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Blume C, von Lehe M, van Landeghem F,
Greschus S and Boström J: Extracranial glioblastoma with
synchronous metastases in the lung, pulmonary lymph nodes,
vertebrae, cervical muscles and epidural space in a young
patient-case report and review of literature. BMC Res Notes.
6:2902013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Rosen J, Blau T, Grau SJ, Barbe MT, Fink
GR and Galldiks N: Extracranial metastases of a cerebral
glioblastoma: A case report and review of the literature. Case Rep
Oncol. 11:591–600. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Anghileri E, Castiglione M, Nunziata R,
Boffano C, Nazzi V, Acerbi F, Finocchiaro G and Eoli M: Extraneural
metastases in glioblastoma patients: two cases with YKL-40-positive
glioblastomas and a meta-analysis of the literature. Neurosurg Rev.
39:37–45. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Andersen BM, Miranda C, Hatzoglou V,
DeAngelis LM and Miller AM: Leptomeningeal metastases in glioma:
The memorial sloan kettering cancer center experience. Neurology.
92:e2483–e2491. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Noch EK, Sait SF, Farooq S, Trippett TM
and Miller AM: A case series of extraneural metastatic glioblastoma
at Memorial Sloan Kettering cancer center. Neurooncol Pract.
8:325–336. 2021.PubMed/NCBI
|
|
31
|
Cantero D, de Lope ÁR, de la Presa RM,
Sepúlveda JM, Borrás JM, Castresana JS, D'Haene N, García JF,
Salmon I, Mollejo M, et al: Molecular study of long-term survivors
of glioblastoma by gene-targeted next-generation sequencing. J
Neuropathol Exp Neurol. 77:710–716. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Cantero D, Mollejo M, Sepúlveda JM,
D'Haene N, Gutiérrez-Guamán MJ, de Lope ÁR, Fiaño C, Castresana JS,
Lebrun L, Rey JA, et al: TP53, ATRX alterations, and low tumor
mutation load feature IDH-wildtype giant cell glioblastoma despite
exceptional ultra-mutated tumors. Neurooncol Adv.
2:vdz0592020.PubMed/NCBI
|
|
33
|
Karatas Y, Cengiz SL and Ustun ME: A case
of symptomatic synchronous cervical and cerebellar metastasis after
resection of thoracal metastasis from temporal glioblastoma
multiforme without any local recurrence. Asian J Neurosurg.
11:4522016. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Stark AM, Nabavi A, Mehdorn HM and Blömer
U: Glioblastoma multiforme-report of 267 cases treated at a single
institution. Surg Neurol. 63:162–169. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Hübner F, Braun V and Richter HP: Case
reports of symptomatic metastases in four patients with primary
intracranial gliomas. Acta Neurochir (Wien). 143:25–29. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Karaca M, Andrieu MN, Hicsonmez A, Guney Y
and Kurtman C: Cases of glioblastoma multiforme metastasizing to
spinal cord. Neurol India. 54:428–430. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Buhl R, Barth H, Hugo HH, Hutzelmann A and
Mehdorn HM: Spinal drop metastases in recurrent glioblastoma
multiforme. Acta Neurochir (Wien). 140:1001–1005. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Schwaninger M, Patt S, Henningsen P and
Schmidt D: Spinal canal metastases: A late complication of
glioblastoma. J Neurooncol. 12:93–98. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Ringel F, Pape H, Sabel M, Krex D, Bock
HC, Misch M, Weyerbrock A, Westermaier T, Senft C, Schucht P, et
al: Clinical benefit from resection of recurrent glioblastomas:
Results of a multicenter study including 503 patients with
recurrent glioblastomas undergoing surgical resection. Neuro Oncol.
18:96–104. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Cabrera AR, Kirkpatrick JP, Fiveash JB,
Shih HA, Koay EJ, Lutz S, Petit J, Chao ST, Brown PD, Vogelbaum M,
et al: Radiation therapy for glioblastoma: Executive summary of an
American Society for radiation oncology evidence-based clinical
practice guideline. Pract Radiat Oncol. 6:217–225. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Mohile NA, Messersmith H, Gatson NT,
Hottinger AF, Lassman A, Morton J, Ney D, Nghiemphu PL, Olar A,
Olson J, et al: Therapy for diffuse astrocytic and oligodendroglial
tumors in adults: ASCO-SNO guideline. J Clin Oncol. 40:403–426.
2022. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Lah TT, Novak M and Breznik B: Brain
malignancies: Glioblastoma and brain metastases. Semin Cancer Biol.
60:262–273. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Venur VA and Leone JP: Targeted therapies
for brain metastases from breast cancer. Int J Mol Sci.
17:15432016. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Chinot OL, Wick W, Mason W, Henriksson R,
Saran F, Nishikawa R, Carpentier AF, Hoang-Xuan K, Kavan P, Cernea
D, et al: Bevacizumab plus radiotherapy-temozolomide for newly
diagnosed glioblastoma. N Engl J Med. 370:709–722. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Gilbert MR, Dignam JJ, Armstrong TS, Wefel
JS, Blumenthal DT, Vogelbaum MA, Colman H, Chakravarti A, Pugh S,
Won M, et al: A randomized trial of bevacizumab for newly diagnosed
glioblastoma. N Engl J Med. 370:699–708. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Yu Z, Zhao G, Zhang Z, Li Y, Chen Y, Wang
N, Zhao Z and Xie G: Efficacy and safety of bevacizumab for the
treatment of glioblastoma. Exp Ther Med. 11:371–380. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Pitter KL, Tamagno I, Alikhanyan K,
Hosni-Ahmed A, Pattwell SS, Donnola S, Dai C, Ozawa T, Chang M,
Chan TA, et al: Corticosteroids compromise survival in
glioblastoma. Brain. 139:1458–1471. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Seidel C and Kortmann RD: Corticosteroids
compromise survival in glioblastoma patients after radio- and
chemotherapy. Strahlenther Onkol. 193:982–983. 2017.(In German).
View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Zhou L, Shen Y, Huang T, Sun Y, Alolga RN,
Zhang G and Ge Y: The prognostic effect of dexamethasone on
patients with glioblastoma: A systematic review and meta-analysis.
Front Pharmacol. 12:7277072021. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Swildens KX, Smitt PAE, van den Bent MJ,
French PJ and Geurts M: The effect of dexamethasone on the
microenvironment and efficacy of checkpoint inhibitors in
glioblastoma: A systematic review. Neurooncol Adv.
4:vdac0872022.PubMed/NCBI
|
|
51
|
Arora H, Mammi M, Patel NM, Zyfi D, Dasari
HR, Yunusa I, Simjian T, Smith TR and Mekary RA: Dexamethasone and
overall survival and progression free survival in patients with
newly diagnosed glioblastoma: A meta-analysis. J Neurooncol.
166:17–26. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Klement RJ and Champ CE: Corticosteroids
compromise survival in glioblastoma in part through their elevation
of blood glucose levels. Brain. 140:e162017.PubMed/NCBI
|
|
53
|
Troschel FM, Troschel BO, Kloss M, Jost J,
Pepper NB, Völk-Troschel AS, Wiewrodt RG, Stummer W, Wiewrodt D and
Eich HT: Sarcopenia is associated with chemoradiotherapy
discontinuation and reduced progression-free survival in
glioblastoma patients. Strahlenther Onkol. 200:774–784. 2024.
View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Bianconi A, Palmieri G, Aruta G,
Monticelli M, Zeppa P, Tartara F, Melcarne A, Garbossa D and Cofano
F: Updates in glioblastoma immunotherapy: An overview of the
current clinical and translational scenario. Biomedicines.
11:15202023. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Goswami S, Walle T, Cornish AE, Basu S,
Anandhan S, Fernandez I, Vence L, Blando J, Zhao H, Yadav SS, et
al: Immune profiling of human tumors identifies CD73 as a
combinatorial target in glioblastoma. Nat Med. 26:39–46. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Brown MP, Ebert LM and Gargett T: Clinical
chimeric antigen receptor-T cell therapy: A new and promising
treatment modality for glioblastoma. Clin Transl Immunology.
8:e10502019. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Álvarez-Vázquez A, San-Segundo L,
Cerveró-García P, Flores-Hernández R, Ollauri-Ibáñez C,
Segura-Collar B, Hubert CG, Morrison G, Pollard SM, Lathia JD, et
al: EGFR amplification and EGFRvIII predict and participate in
TAT-Cx43266-283 antitumor response in preclinical glioblastoma
models. Neuro Oncol. 26:1230–1246. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Dhar D, Ghosh S, Das S and Chatterjee J: A
review of recent advances in magnetic nanoparticle-based
theranostics of glioblastoma. Nanomedicine (Lond). 17:107–132.
2022. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Angom RS, Nakka NMR and Bhattacharya S:
Advances in glioblastoma therapy: An update on current approaches.
Brain Sci. 13:15362023. View Article : Google Scholar : PubMed/NCBI
|