Introduction
Microsatellite instability-high (MSI-H) tumors
account for 4–5% of all solid tumors, with the highest prevalence
observed in colorectal (up to 15%) and endometrial cancer (up to
30%) (1). MSI-H status results from
deficiency in the DNA mismatch repair system, occurring either
sporadically or through germline mutations associated with Lynch
syndrome. These tumors are characterized by a high tumor mutational
burden and abundant neoantigen production. In clinical practice,
the therapeutic effect of programmed death ligand 1 (PD-L1)
blockade using pembrolizumab against MSI-H tumors is hypothesized
to extend beyond the organ system (2). Although most MSI-H tumors occur
sporadically in several organs and are not associated with
hereditary disease, the possibility of Lynch syndrome can only be
entirely excluded if germline testing is performed.
TC is a rare and highly malignant tumor. Treatment
strategies include surgical resection when feasible, followed by
platinum-based chemotherapy and radiotherapy. Complete surgical
resection is essential for achieving favorable outcomes. The
prognosis of patient with incompletely resected or metastatic TC is
poor, and systemic therapy for unresectable, progressive or
recurrent TC is supported by limited clinical data (3–7).
Generally, TCs exhibit high PD-L1 expression but low
mutational burden (8–10). MSI-H status in TCs is exceedingly
rare, reported in <1% of case (11–13).
To the best of our knowledge, only one case report has described an
MSI-H thymic carcinoma treated with ICIs, which achieved a partial
response (12). The present report
describes a rare case of recurrent MSI-H TC that responded notably
well to ICIs and may provide useful data for the immunotherapy of
future cases of recurrent MSI-H TC.
Case report
A 78-year-old woman with an abnormal pulmonary
shadow was referred to the Department of Thoracic Surgery (Tokai
University Hachioji Hospital, Tokyo, Japan) for examination in
April 2020 with a medical history including hypertension and
complete atrioventricular block with an implanted pacemaker. The
patient had surgery for right breast cancer ~30 years prior and for
cerebellar meningioma ~20 years prior. No abnormalities were
observed during the initial physical examination.
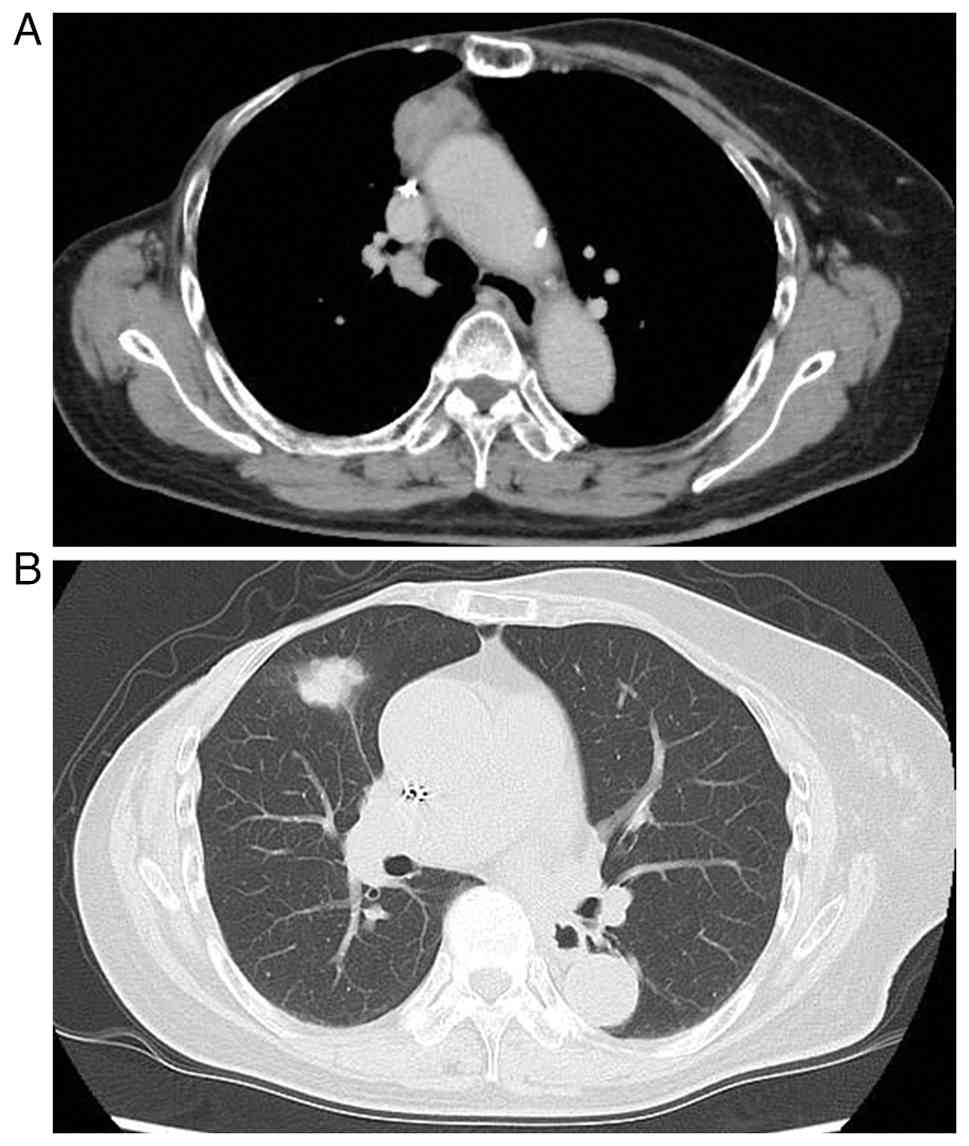
Contrast-enhanced chest computed tomography (CT)
revealed a pulmonary nodule (26 mm in size) in the right middle
lobe adjacent to the interlobar pleura without mediastinal lymph
node enlargement, and a solid tumor (30 mm in size) in the right
anterior mediastinum (Fig. 1).
Positron emission tomography (PET) revealed an accumulation of
fluorodeoxyglucose [standardized uptake value (SUV) max, 4.3 and
4.5] but no accumulation elsewhere (data not shown). Blood test
results were normal, including those of tumor markers
[carcinoembryonic antigen (CEA), squamous cell carcinoma (SCC)
associated antigen and cytokeratin 19 fragment]. The SUVmax value
of the mediastinal lesion was low for malignant lymphoma or TC,
which typically show SUVmax value exceeding 5.0–10.0 (14,15).
By contrast, the mediastinal lesion in this case demonstrated a
lower SUVmax of 4.5. Therefore, it was considered a thymoma. The
pulmonary lesion was diagnosed as either lung cancer [C-T2a(pl1)
N0M0] based on the TNM classification system (8th edition)
(16) or pulmonary metastasis from
breast cancer.
CT-guided biopsy was not performed prior to surgery,
as the lesions were considered resectable. This procedure often
yields limited tissue samples, which may compromise accurate
histopathological diagnosis, particularly in thymic epithelial
tumor. Moreover, it was avoided due to the potential risk of tumor
seeding along the puncture tract. In addition, the anatomical
location of lesions raised concern for air embolism associated with
transthoracic needle insertion. Therefore, upfront surgical
resection was selected: Middle lobectomy with systemic lymph node
dissection and radical thymectomy with partial pericardium were
performed via videoscopic surgery. Intraoperative pathology
revealed both tumors to be poorly differentiated carcinomas. The
sample was embedded in a cryoprotective compound and frozen at −10
to −15°C. Sections were cut at 5-µm thickness using a cryotome and
subsequently stained by the rapid hematoxylin and eosin (H&E)
technique for ~3 min at room temperature. The slides were
microscopically evaluated by two pathologists using a light
microscope (BX53; Olympus Corporation). However, determining the
primary tumor was difficult. Macroscopically, a whitish solid tumor
(25×20×30 mm in size) was observed in the resected anterior
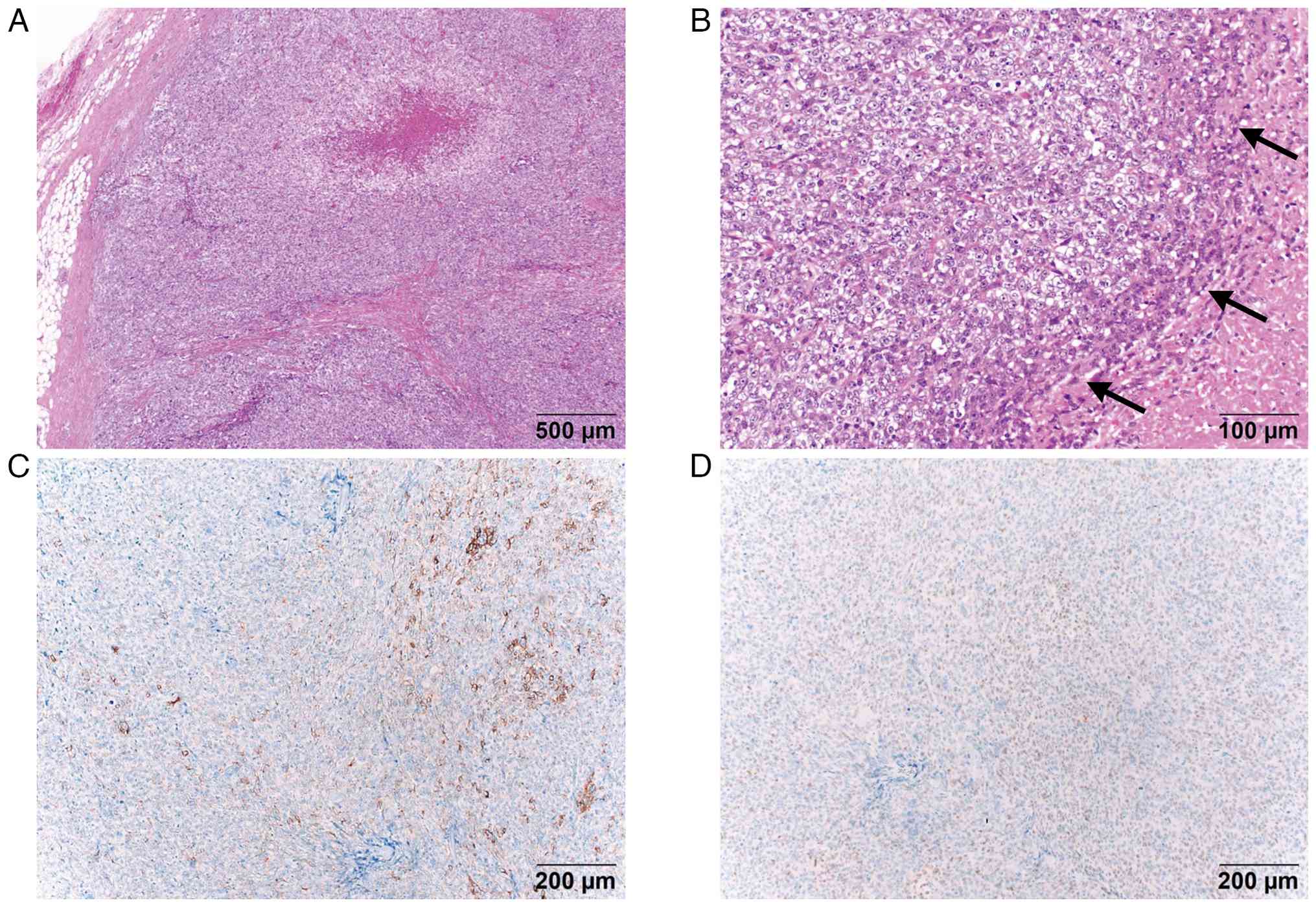
mediastinal resected specimen. Histologically (Fig. 2A and B), the tumor was surrounded by
a fibrous capsule, but focal fatty invasion and necrosis were
observed. The tumor was composed of epithelioid cells with marked
pleomorphism and frequent mitosis. Furthermore, the tumor contained
thymoma components equivalent to type B2-3 accompanied by
lymphocytic infiltration. These finding indicated poorly
differentiated and highly malignant thymic-origin tumor. All
specimens were fixed with 10% neutral buffered formalin for 24–48 h
at room temperature, embedded in paraffin and cut into 4-µm thick
sections. Immunohistochemistry was performed using the BenchMark
Autostainer (Roche Diagnostics) according to the manufacturer's
recommended protocol. Antigen retrieval was performed with
PROTEASE1 for 4 min or with ULTRA Cell Conditioning Solution (ULTRA
CC1) at 100°C for 64 min. The BenchMark Autostainer automatically
performed all subsequent processes, including deparaffinization in
xylene and rehydration in ethanol. Sections were then immersed in
0.01 mol/l citric acid buffered solution, followed by blocking
using the UV DAB inhibitor and protein blocking reagent included in
the UltraView Universal DAB Detection Kit (Roche Diagnostics),
which was applied at room temperature according to the
manufacturer's protocol. Endogenous peroxidase activity was
quenched automatically on the BenchMark Autostainer using the
hydrogen peroxide-based inhibitor included in the same detection
kit.
The following primary antibodies were applied at
36°C for 32–40 min: cytokeratin (cat. no. NCL-L; clone AE1/AE3,
Leica, 1:100), p63 (cat. no. NCL-L; clone 7-Jul, Leica, 1:20),
c-kit (cat. no. NCL-L-CD117-32; clone EP10, Leica, 1:20), CD5 (cat.
no. NCL-L-CD5-4C7; clone 4C7, Leica, 1:200), TTF-1 (cat. no. CMQ
343M-96-RUO; clone 8G7G3/1, Cell Marque, 1:100), CEA (cat. no.
413121; clone COL-1; Nichirei, 1:100), and MART-1 (cat. no. 413381;
clone M2-7C10, Nichirei, 1:10). Visualization was achieved using
the Ultra View Universal DAB Detection Kit (Roche Diagnostics).
Microscopic evaluation was performed with a BX53
optical light microscope (Olympus Corporation), and two
pathologists independently assessed the staining results.
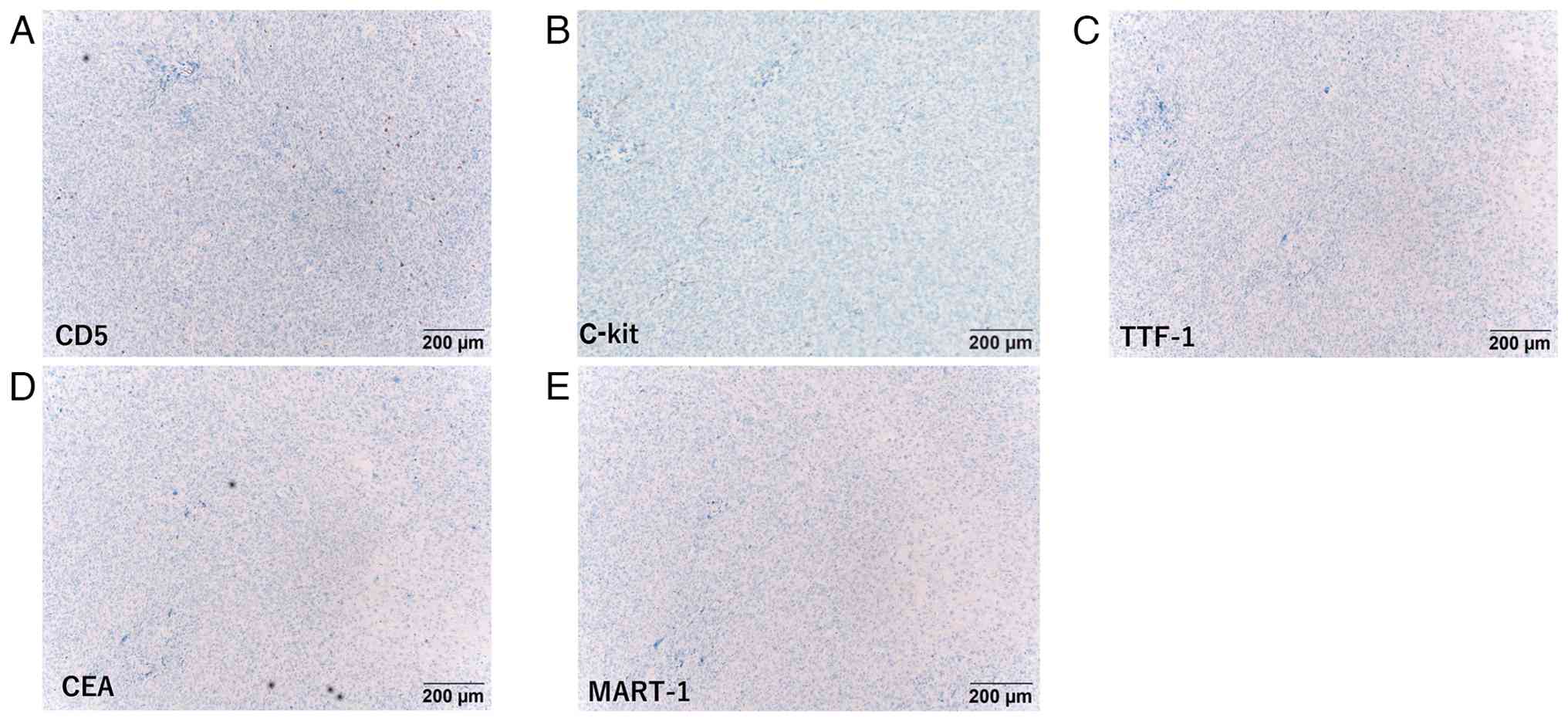
Immunostaining revealed partial positivity for keratin AE1/3 and
P-63 (Fig. 2C and D), but
negativity for C-kit and CD5 (Fig. 3A
and B), suggesting a poorly differentiated thymic SCC or
undifferentiated carcinoma, differing from typical thymic SCC.
Additionally, negativity for thyroid transcription factor 1, CEA
and melanoma antigen recognized by T cells (Fig. 3C-E) ruled out metastatic tumors
originating from the lung adenocarcinoma or amelanotic melanoma.
The pulmonary tumor measured 20×15 mm in size and histologically
resembled a mediastinal lesion with multiple venous infiltrations.
No metastasis to the mediastinal or hilar lymph nodes was observed;
however, there was a suspected high potential for hematogenous
metastasis. Based on the aforementioned findings, the tumor was
diagnosed as a poorly differentiated thymic SCC/undifferentiated
carcinoma with pulmonary metastasis and stage IVb disease (Masaoka
classification) (17).
Adjuvant therapy with carboplatin and paclitaxel was
administered intravenously on postoperative days 84 and 121. The
regimen consisted of carboplatin (300 mg/body kg) and paclitaxel
(290 mg/body kg). Although the standard interval between cycles is
3 weeks, the second cycle was delayed, resulting in a 37-day
interval. However, due to the advanced age of the patient, severe
bone marrow suppression and anorexia, chemotherapy was discontinued
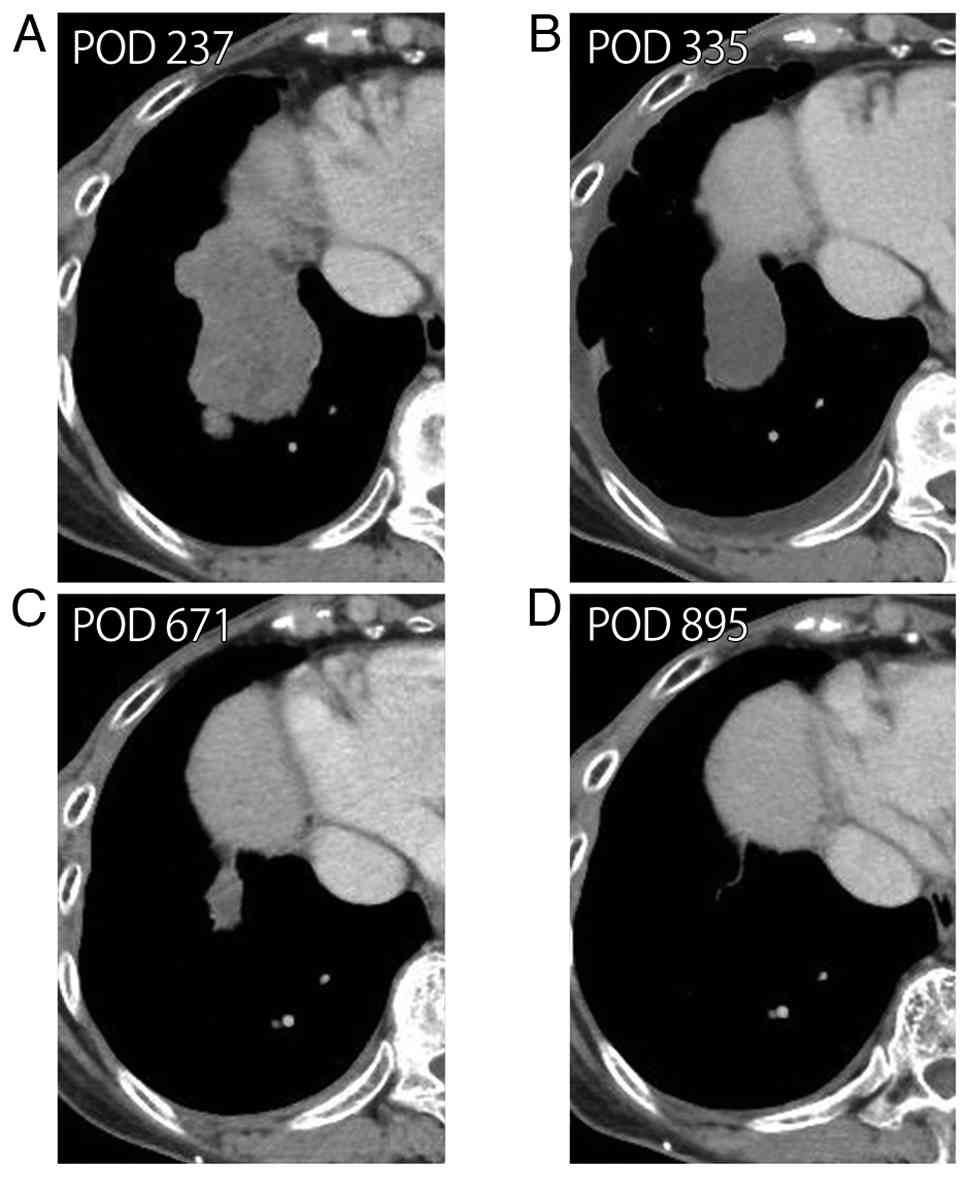
after the second cycle. A follow-up contrast CT scan 8 months after
surgery revealed local recurrence of TC in the anterior mediastinum
and multiple pulmonary metastases (Fig.
4A) with pleural dissemination and right hilar lymph node
metastases. However, the patient could not tolerate further
chemotherapy.
MSI testing was performed on the formalin-fixed,
paraffin-embedded tumor tissue using an MSI testing kit (FALCO
HOLDINGS Co., Ltd.), and the tissue was classified as MSI-H.
Additional biomarkers, including PD-L1 expression and tumor
mutation burden (TMB), were not assessed. In Japan, ICIs are not
approved for TC as a standalone indication, and PD-L1 testing is
not routinely performed in such a setting (3,18).
Furthermore, at the time of treatment initiation, tissue-agnostic
approval for TMB-high tumor was not yet available, and
comprehensive genomic profiling was not available.
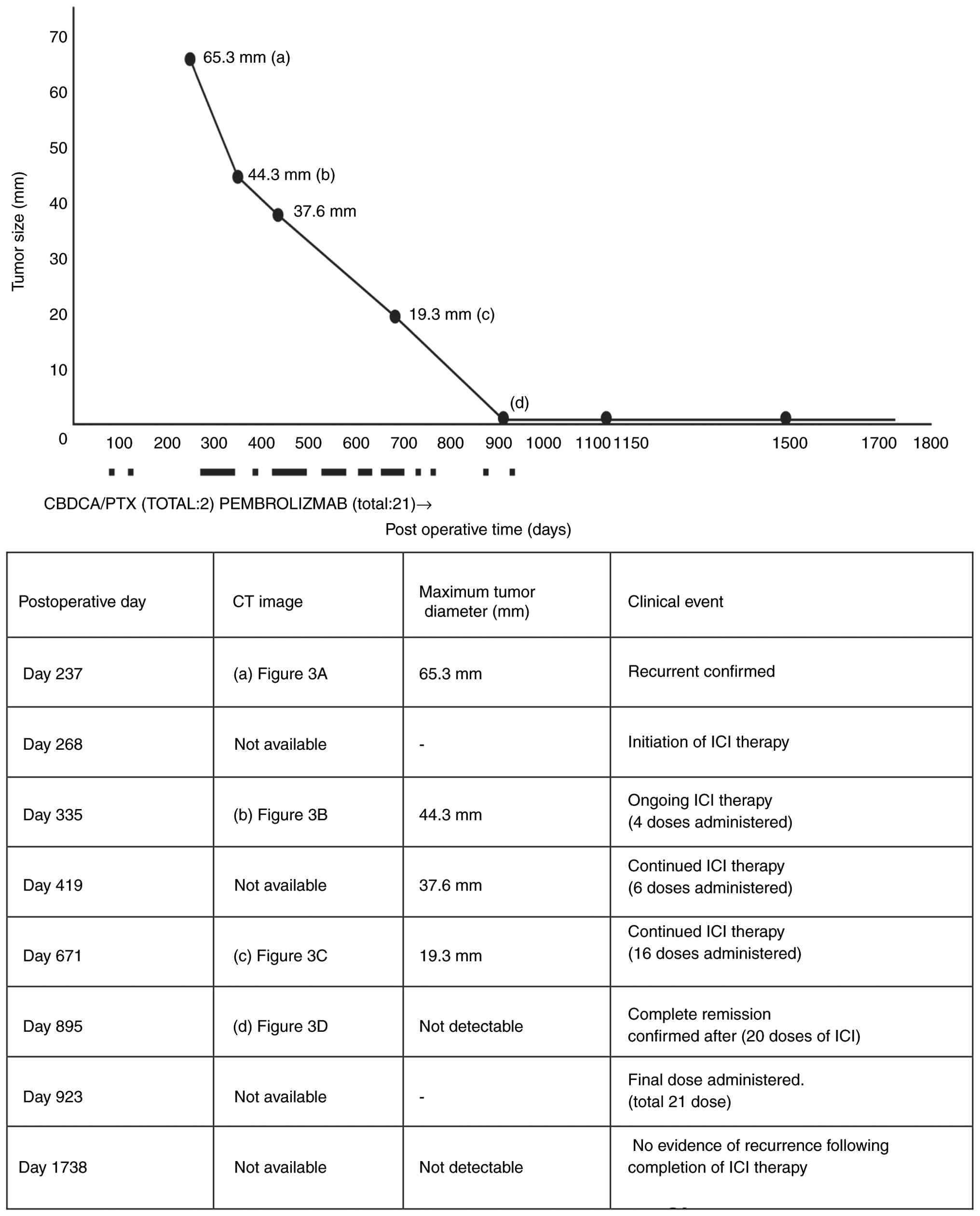
Pembrolizumab (200 mg/dose) was initiated 9 months
after surgery and administered intravenously every 3 weeks for
total of 21 cycles over 1 year and 9 months, without any
immune-related adverse events. A timeline of the tumor response and
pembrolizumab monotherapy is presented in Fig. 5. Subsequently, at 1.5 years after
the initiation of pembrolizumab treatment, chest CT revealed that
the recurrent lesions, including those in the anterior mediastinum,
multiple pulmonary metastases, pleural dissemination and right
hilar lymph node metastases, had almost completely disappeared
(Fig. 4B-D). A total of 4 years and
9 months after the initial surgery, the patient is alive without
recurrence.
Discussion
TC is an extremely rare tumor with an incidence of
0.07–0.38% per 100,000 individuals (4). Complete surgical resection is
essential for achieving good outcomes; however, TC is highly
malignant, and ~68% of patients develop progressive disease with
lymph node or distant metastases (5).
Systemic therapy for unresectable progressive or
recurrent TC has limited clinical data. Currently, the key drug is
a platinum agent and combination therapy (6). Lenvatinib, a multi-kinase inhibiter,
has also shown promising activity in this setting (7). Nevertheless, in clinical practice,
there are few effective treatment options after second-line
treatment, compared with that in non-small cell lung cancer. In the
present case, the identification of MSI-H status provided a
rationale for immune checkpoint inhibition, which led to a complete
response.
ICI therapy has expanded in the field of thoracic
surgery to include adjuvant therapy after lung cancer surgery and
for lung cancer recurrence, with PD-L1 expression and its
associated therapeutic effects gaining attention. In advanced TC
with a history of initial chemotherapy and no autoimmune disease,
the PD-L1 positivity rate is relatively high at 54–75%. The overall
response rate (ORR) of pembrolizumab has been reported to be ~20%,
with a median progression free survival of 4.2–6.1 months. An
association has also been reported between PD-L1 expression and
therapeutic effect (9,10). However, due to insufficient data,
ICI therapy for TC is not covered by insurance in Japan (3,18).
The incidence of unresectable or metastatic MSI-H
solid cancers varies according to cancer type, with endometrial
cancer being the most common (16.85%), followed by small intestinal
(8.63%), gastric (6.74%), duodenal (5.60%) and colon/rectal (3.78%)
cancer (8). In a phase II trial of
pembrolizumab (anti-programmed cell death protein 1 antibody)
therapy for MSI-H advanced solid cancers that were resistant or
intolerant to standard therapy, the ORR was ~37% and median overall
survival was 13.4 months, demonstrating a certain level of efficacy
regardless of solid cancer type (9). Therefore, MSI testing is expected to
serve as a companion test for predicting the efficacy of ICI
therapy against solid tumors. In Japan, it is currently approved
exclusively used in solid tumors, particularly solid cancer
(19).
The incidence of unresectable or metastatic MSI-H
solid cancers in thoracic surgery is extremely low (1.1% for
non-small cell lung cancer and 0.67% for TC) (20,21).
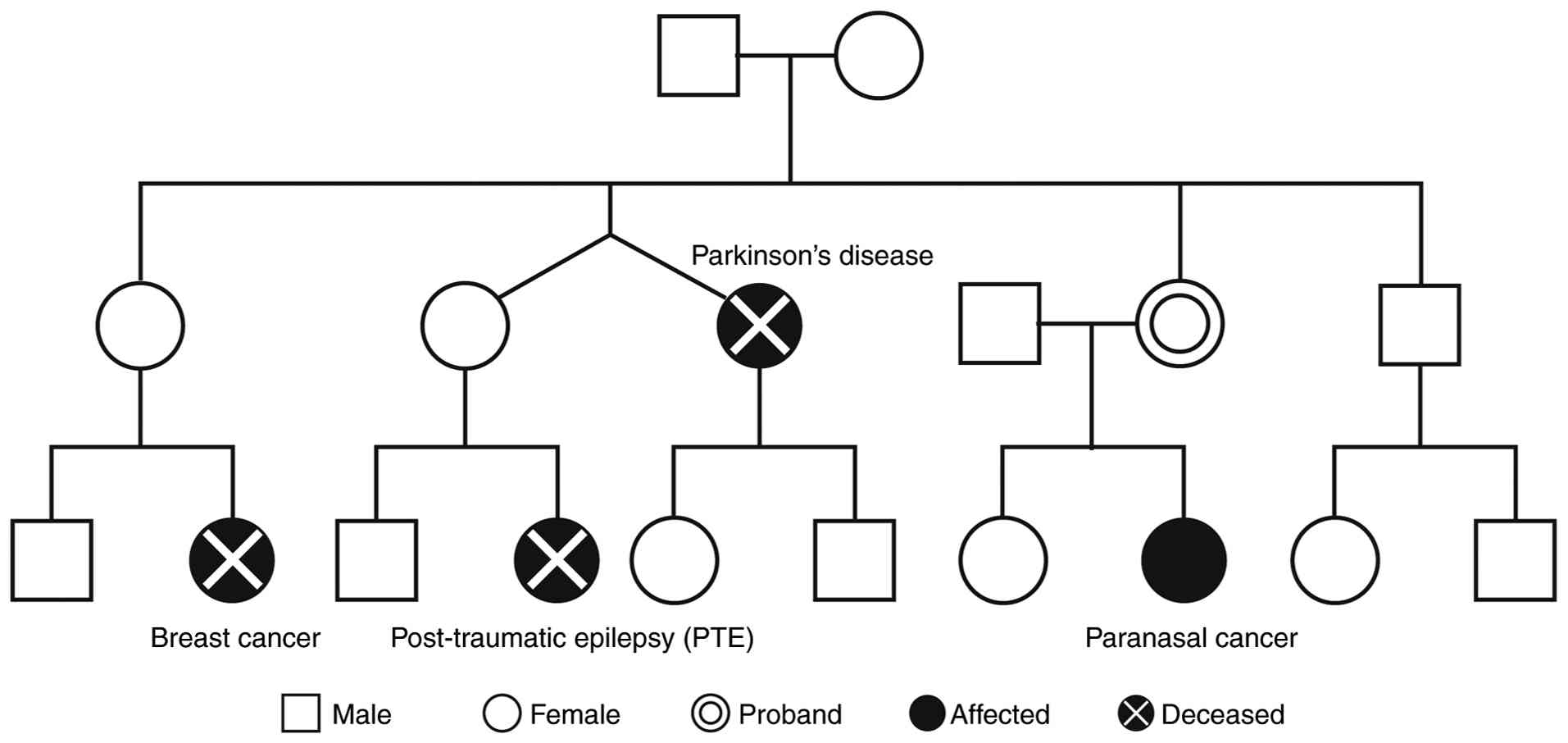
In the present case, MSI testing was performed due
to the lack of alternative treatment options, and tumor was
confirmed to be MSI-H. MSI-H TCs can be associated with Lynch
syndrome (12,13), and although the finding of MSI-H in
the present case suggested the possibility of Lynch syndrome, the
family history of the patient, summarized in Fig. 6, did not meet the revised Bethesda
or modified Amsterdam criteria (22,23).
Although comprehensive genomic profiling was not available,
germline testing for mismatch repair gene mutations was separately
recommended to confirm the diagnosis; however, the patient declined
this genetic testing. As a result, a definitive diagnosis of Lynch
syndrome could not be established in the present case.
Repetto et al (12) reported a case of MSI-H TC associated
with Lynch syndrome; however, the present case has several notable
distinctions in the clinical course, disease setting and treatment
response. Whilst both reported involved MSI-H status and
post-platinum chemotherapy settings, the patient in the present
case experienced postoperative recurrence and was treated
pembrolizumab monotherapy, resulting in a complete and durable
response, maintained over an extended period. By contrast, Repetto
et al reported a case involving unresectable progressive
disease, which was treated with avelumab plus axitinib combination
therapy, achieving a partial response that persisted for >15
months. Notably, this combination therapy was administered within
the context of an exploratory phase II trial and is not considered
a standard treatment. However, the most decisive difference lies in
the treatment outcome; the patient in the present case achieved
complete remission, whereas the Repetto et al reported only
partial response. These findings underscore the heterogeneity of
ICI responsiveness in MSH-H TC and highlight the importance of
individualized therapeutic strategies based on disease context and
molecular profile.
Furthermore, the patient in the present case had no
history of autoimmune disease that would have increased the risk of
immune-related adverse events from immunotherapy; this was a key
factor in the decision to administer ICI treatment. Pembrolizumab
was administered for 1 year and 9 months (a total of 21 times). The
treatment was highly effective, with the lesions almost
disappearing, and complete remission achieved.
Unlike that of PD-L1 expression, the incidence of
MSI-H in TC is extremely low. Recently, the first case report, to
the best of our knowledge, on thymoma presenting with MSI-H and
demonstrating the efficacy of ICIs was published (24); however, the present case differs in
several key aspects from this previously reported case: Firstly,
thymoma and TC are distinct entities with differences in malignancy
and therapeutic approaches. Whilst ICIs are unsuitable for thymoma
due to a high risk of autoimmune complications, they can be
administered for TC with careful management (9,25).
Secondly, the present case underscores the indication of
pembrolizumab for MSI-H cancers in Japanese regulatory guidelines.
Unlike prior reports that included thymoma as a potential candidate
(10,25), the present report proposes that
thymoma may be biologically distinct from other MSI-H cancers,
necessitating further research. Lastly, the treatment outcomes
differ, as the patient in the present case achieved a complete
response with a prolonged ICI regimen, in comparison with the
partial response and shorter regimen reported in the thymoma case.
These key differences are summarized in Table I.
 | Table I.Comparison of the features of a case
of microsatellite instability-high thymoma and the present case of
MSI-H thymic carcinoma case, both involving pembrolizumab
monotherapy. |
Table I.
Comparison of the features of a case
of microsatellite instability-high thymoma and the present case of
MSI-H thymic carcinoma case, both involving pembrolizumab
monotherapy.
| Feature | Kaneko et al,
2024 (24) | Present case |
|---|
| Diagnosis | MSI-H thymoma | MSI-H thymic
carcinoma |
| Tumor
classification | Low-grade thymic
epithelial tumor | High-grade thymic
epithelial tumor |
| Risk of irAEs | High | Low, but required
careful monitoring |
| ICI suitability | Generally unsuitable
due to risk of irAEs | Suitable with careful
management and monitoring in the absent of auto-immune disease |
| Predictive value
o | Limited: MSI-H status
alone did not | Favorable: MSI-H
status supported |
| MSI-H status | justify pembrolizumab
use | pembrolizumab
initiation |
| Reported ICI
outcomes | Partial response with
short pembrolizumab regimen | Complete response
with prolonged pembrolizumab regimen |
| Pembrolizumab
indication (Japan) | Not approved: Not
classified as MSI-H solid cancer | Approved: Classified
as MSI-H solid cancer |
In conclusion, the present case highlights the
potential utility of MSI-H status as a predictive biomarker for
pembrolizumab therapy in TC. This represents a rare but clinically
meaningful entity and underscores the importance of molecular
profiling and individualized immunotherapy strategies in rare
thoracic malignancies. However, broader molecular profiling and
further multicenter or prospective studies are warranted to
validate the clinical significance of MSH-H status and therapeutic
implications of pembrolizumab in this context.
Acknowledgements
The authors would like to thank Dr Takuma Tajiri
(Department of Pathology, Tokai University Hachioji Hospital;
Hachioji, Japan) for guidance on the histopathological
interpretation of this case.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
TN contributed substantially to the conception of
the study and processing of the figures. TN and NA performed
surgery. HW performed the literature review, wrote the manuscript,
and managed postoperative chemotherapy. SY contributed to to the
study design, the literature search for related studies, and wrote
the manuscript. RM and MI analyzed and interpreted data, advised on
patient treatment, confirm the authenticity of all the raw data,
and revised the manuscript. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate.
The present report was approved by the Ethics
Committee of Tokai University School of Medicine (approval no.
24J006).
Patient content for publication
Written informed consent was obtained from the
patient for the publication of the presents case report and the
accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Lorenzi M, Amonkar M, Zhang J, Mehta S and
Liaw KL: Epidemiology of microsatellite instability-high (MSI-H)
and deficient mismatch repair (dMMR) in solid tumors: A structured
literature review. J Oncol. 2020:18079292020. View Article : Google Scholar
|
|
2
|
Marabelle A, Le DT, Ascierto PA, Di
Giacomo AM, De Jesus-Acosta A, Delord JP, Geva R, Gottfried M,
Penel N, Hansen AR, et al: Efficacy of pembrolizumab in patients
with noncolorectal high microsatellite instability/mismatch
repair-deficient cancer: Results from the phase II KEYNOTE-158
study. J Clin Oncol. 38:1–10. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Okuma Y: Prospects for thymic carcinoma
treatment. Haigan. 64:821–827. 2024. View Article : Google Scholar
|
|
4
|
Koizumi T, Otsuki K, Tanaka Y, Noguchi T,
Fukushuima T, Kobayashi T, Takesumi O, Sekiguchi N and Hamanaka K:
National incidence and initial therapy for thymic carcinoma in
Japan: Based on analysis of hospital-based cancer registry data,
2009–2015. Jpn J Clin Oncol. 50:434–439. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bakhos CT, Salami AC, Kaiser LR, Petrov RV
and Abbas AE: Thymic neuroendocrine tumors and thymic carcinoma:
Demographics, treatment, and survival. Innovations (Phila).
15:468–474. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hirai F, Yamanaka T, Taguchi K, Daga H,
Ono A, Tanaka K, Kogure Y, Shimizu J, Kimura T, Fukuoka J, et al: A
multicenter phase II study of carboplatin and paclitaxel for
advanced thymic carcinoma: WJOG4207L. Ann Oncol. 26:363–368. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Sato J, Satouchi M, Itoh S, Okuma Y, Niho
S, Mizugaki H, Murakami H, Fujisaka Y, Kozuki T, Nakamura K, et al:
Lenvatinib in patients with advanced or metastatic thymic carcinoma
(REMORA): A multicentre, phase 2 trial. Lancer Oncol. 21:843–850.
2020. View Article : Google Scholar
|
|
8
|
Cho J, Kim HS, Ku BM, Choi YL, Cristescu
R, Han J, Sun JM, Lee SH, Ahn JS, Park K and Ahn MJ: Pembrolizumab
for patients with refractory or relapsed thymic epithelial Tumor:
An open-label phase II trial. J Clin Oncol. 37:2162–2170. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Giaccone G, Kim C, Thompson J, McGuire C,
Kallakury B, Chahine JJ, Maning M, Mogg R, Blumenschein WM, Tan MT,
et al: Pembrolizumab in patients with thymic carcinoma: A
single-arm, single-centre, phase 2 study. Lancet Oncol. 19:347–355.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Yokoyama S and Miyoshi T: Thymic tumors
and immune checkpoint inhibutors. J Thorac Dis. 10:S1509–S1515.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Akagi K, Oki E, Taniguchi H, Nakatani K,
Aoki D, Kuawata T and Yoahino T: Real-world data on microsatellite
instability status in various unresectable or metastatic solid
tumors. Cancer Sci. 112:1105–1113. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Repetto M, Conforti F, Pirola S, Calvello
M, Pala L, Bonanni B, Catania C, Curigliano G and De Pas T: Thymic
carcinoma with Lynch syndrome or microsatellite instability, a rare
entity responsive to immunotherapy. Eur J Cancer. 153:162–167.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Watanabe M, Tanakaya K, Furukawa S,
Shiotani T, Sato Y, Taniguchi F, Kanaya N, Aoki H, Sugano K, Ishida
H, et al: Two cases of thymic cancer in patients with Lynch
syndrome. Intern Med. 62:649–653. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Yanagihara T, Kawamura T, Maki N,
Kobayashi N, Kikuchi S, Goto Y, Ichimura H and Sato Y: Practical
methods to differentiate thymic malignancies. Surg Today.
54:899–906. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Igai H, Matsuura N, Tarumi S, Chang SS,
Misaki N, Go T, Ishikawa S and Yokomise H: Usefulness of
[18F]fluoro-2-deoxy-D-glucose positron emission
tomography for predicting the World Health Organization malignancy
grade of thymic epithelial tumors. Eur J Cardiothorac Surg.
40:143–145. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Brierley JD, Gospodarowicz MK and
Wittekind C: TNM classification of malignant tumours. 8th edition.
Wiley-Blackwell; Oxford: pp. 114–124. 2017
|
|
17
|
Masaoka A, Monden Y, Nakahara K and
Tanioka T: Follow-up study of thymomas with special reference to
their clinical stages. Cancer. 48:2485–2492. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Pharmaceuticals and Medical Devices
Agency, . KEYTRUDA® Intravenous Infusion 100 mg: Package
Insert. Version 25. https://www.pmda.go.jp/PmdaSearch/bookSearch/01/14987185809730Accessed
(In Japanese). September 20–2025
|
|
19
|
Pharmaceutical Evaluation Division,
Pharmaceutical Safety, Environmental Health and Bureau, Ministry of
Health and Labour Welfare, . Report on the Deliberation Results:
Keytruda (pembrolizumab). https://www.pmda.go.jp/files/000231921.pdfMarch
8–2025
|
|
20
|
Hellmann MD, Nathanson T, Rizvi H, Creelan
BC, Sanchez-Vega F, Ahuja A, Ni A, Novik JB, Mangarin LMB,
Abu-Akeel M, et al: Genomic features of response to combination
immunotherapy in patients with advanced non-small-cell lung cancer.
Cancer Cell. 33:843–852.e4. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Vanderwalde A, Spetzler D, Xiao N,
Gatalica Z and Marshall J: Microsatellite instability status
determined by next-generation sequencing and compared with PD-L1
and tumor mutational burden in 11,348 patients. Cancer Med.
7:746–756. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Umar A, Boland CR, Terdiman JP, Syngal S,
de la Chapelle A, Rüschoff J, Fishel R, Lindor NM, Burgart LJ,
Hamelin R, et al: Revised Bethesda Guidelines for hereditary
nonpolyposis colorectal cancer (Lynch syndrome) and microsatellite
instability. J Natl Cancer Inst. 96:261–268. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Vasen HF, Watson P, Mecklin JP and Lynch
HT: New clinical criteria for hereditary nonpolyposis colorectal
cancer (HNPCC, Lynch syndrome) proposed by the international
collaborative group on HNPCC. Gastroenterology. 116:1453–1456.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kaneko T, Sekine A, Komatsu S, Otoshi R,
Haga S, Tagami Y, Kaneko T and Ogura T: Successful pembrolizumab
treatment for microsatellite instability-high thymoma: A case
report. Respir Investig. 62:517–519. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
de Camargo Correia GC, Tawfiq R, Lou Y,
Zhao Y, Li S, Ernani V, Parikh K and Manochakian R: Immune
checkpoint inhibitors (ICI) in thymic epithelial tumors (TET): A
real world assessment of efficacy and toxicity. J Clin Oncol. 43
(Suppl 16):e201412025.
|