Introduction
Previous reports have documented morphological
changes resembling cirrhosis in the livers of patients with breast
cancer and liver metastases who are undergoing chemotherapy
(1–3). The primary features of these changes
include a lobular liver contour, reduced hepatic segment volume and
enlargement of the caudate lobe. In 1994, Young et al
(1) reclassified this condition as
‘pseudocirrhosis’ based on its clinical and imaging features.
Subsequently, as reports of pseudocirrhosis cases in breast cancer
and other cancers increased, it drew the attention of clinicians.
In addition to cases in patients with breast cancer,
pseudocirrhosis has also been reported in other tumors. For
example, colorectal cancer, pancreatic cancer, esophageal cancer,
lung adenocarcinoma, gastric cancer, neuroendocrine cancer, thyroid
cancer and melanoma (4–12). Research on pseudocirrhosis primarily
relies on case reports and small-sample observational studies; its
incidence and pathogenesis remain incompletely understood.
Currently, there are no definitive diagnostic criteria for
pseudocirrhosis, and most diagnoses are based on imaging studies.
There is no specific treatment for pseudocirrhosis. When
pseudocirrhosis occurs, chemotherapy drugs should be discontinued
immediately. If ascites develops, symptomatic management should be
initiated promptly, including diuretic therapy, albumin infusion
and paracentesis. The present report describes the case of a
patient with lung squamous cell carcinoma and diffuse liver
metastases who developed pseudocirrhosis following immunotherapy
combined with chemotherapy.
Case report
In June 2024, a 74-year-old man was admitted to
Huai'an Hospital Affiliated to Yangzhou University and The Fifth
People's Hospital of Huai'an (Jiangsu, China) with symptoms of
coughing, hemoptysis, decreased appetite and abdominal distension.
The patient had a history of chronic obstructive pulmonary disease
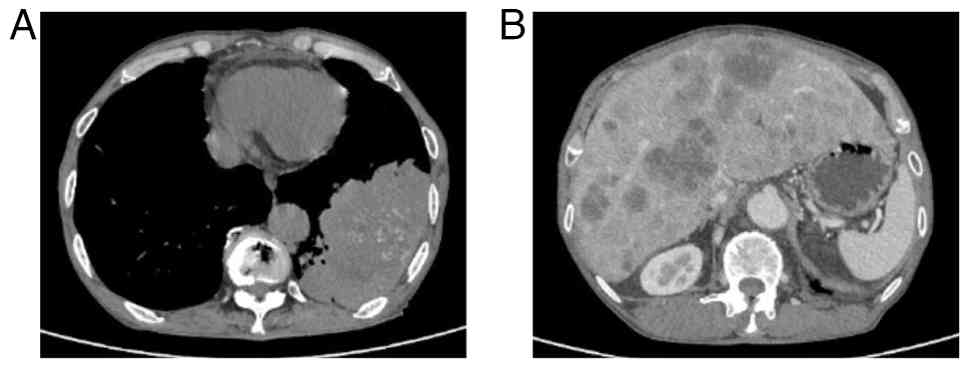
spanning over 20 years. Computed tomography (CT) identified a
12.3-cm soft-tissue mass in the left lower lobe of the lung, with
multiple metastatic lesions noted in the liver (Fig. 1). A biopsy of the lung lesion under
CT control was performed. Tissues were fixed in 10% neutral
formalin solution at room temperature for 24 h, then dehydrated and
embedded in paraffin. The tissues were sliced into 5-µm thick
sections. Immunohistochemical analysis was performed using the
EnVision two-step method. Both primary and secondary antibodies
were ready-to-use antibodies purchased from Henan Celnovte
Biotechnology Co., Ltd. The following antibodies were employed:
CK5/6 (clone C6H1/C1C8; catalog no. CCM-0983), p40 (clone C3B4;
catalog no. CPM-0133), p53 (clone C2H10; catalog no. CPM-0142) and
Ki-67 (clone C3G4; catalog no. CKM-0032). All staining was
performed using an automated immunohistochemical staining machine
(catalog no. CNT360-M2; Henan Celnovte Biotechnology Co., Ltd.),
according to the manufacturer's instructions. All section
observations and image acquisition were performed using a light
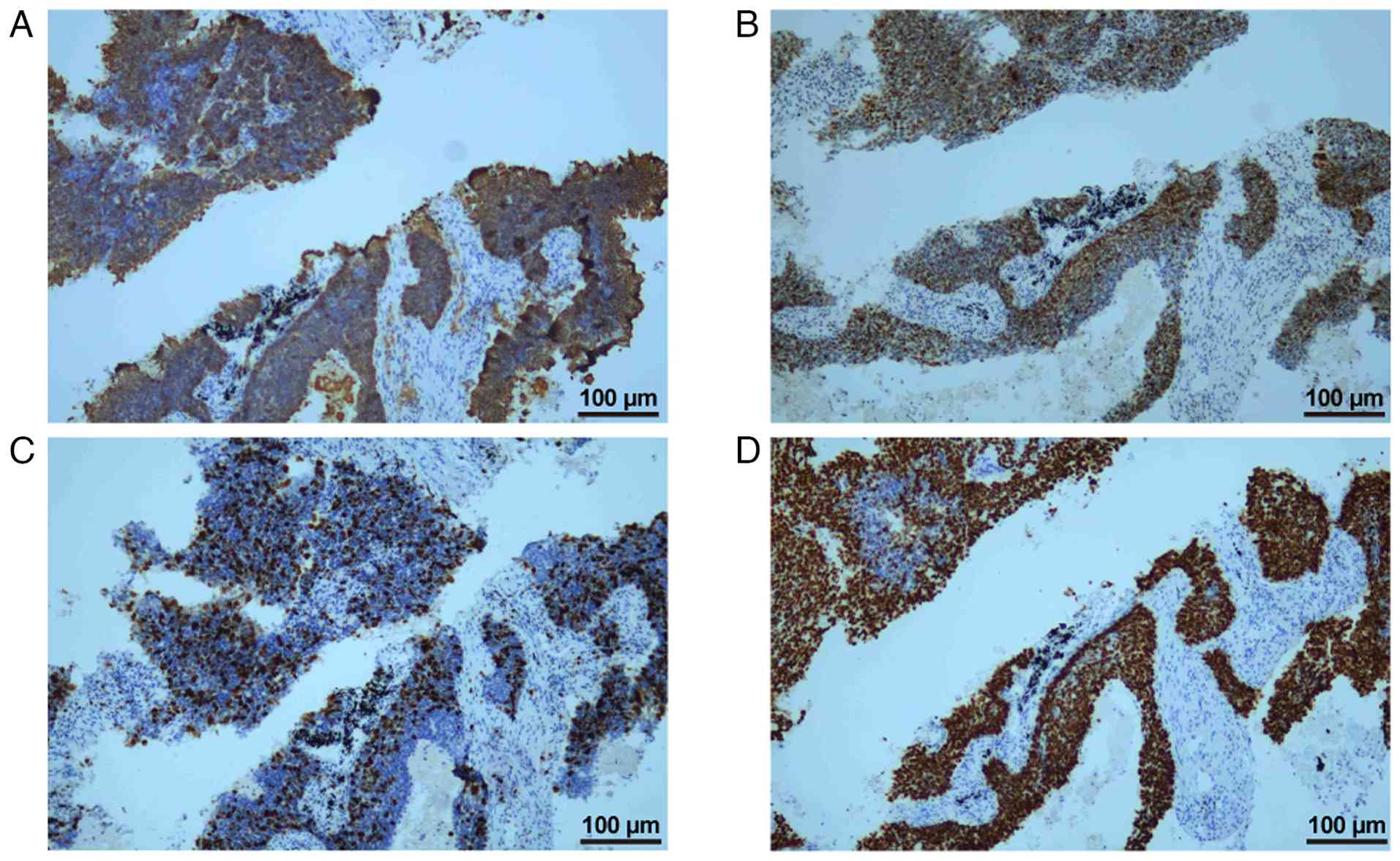
microscope (ECLIPSE Ci-S; Nikon Corporation). Immunohistochemical
analysis of the tissue sample revealed positive expression of
CK5/6, p53 and p40, and the Ki-67 index was 30% (Fig. 2). Based on clinical presentation,
imaging studies and pathological findings, the patient was
diagnosed with primary lung squamous cell carcinoma. The patient
refused a liver biopsy and programmed death ligand 1 testing. The
patient was diagnosed with squamous cell carcinoma of the left
lower lung lobe and liver metastasis, cT4N3M1c, clinical stage IVB,
according to the American Joint Committee on Cancer 8th edition
(13). The patient received
intravenous sintilimab (200 mg on day 1) and albumin-bound
paclitaxel (200 mg on day 1 and 100 mg on day 8) plus cisplatin (30
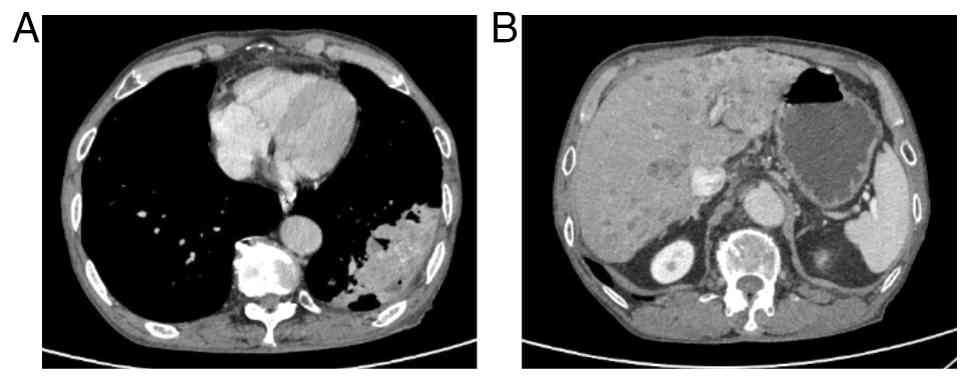
mg on days 1–3) of each 21-day cycle for 4 cycles. In October 2024,
the patient showed a significant reduction in measurable lesions
with regard to both the primary tumor and liver metastasis. The
mass in the lower lobe of the left lung decreased from 12.3 to 8.4
cm in diameter, while the largest liver metastasis shrank from 3.8
to 1.5 cm in diameter, with some liver metastases disappearing
(Fig. 3). Following the
aforementioned four cycles of sintilimab and albumin-bound
paclitaxel plus cisplatin, the patient continued maintenance
therapy with sintilimab (200 mg on day 1 of each 21-day cycle).
Tumor status was assessed every 6 to 8 weeks. The assessment
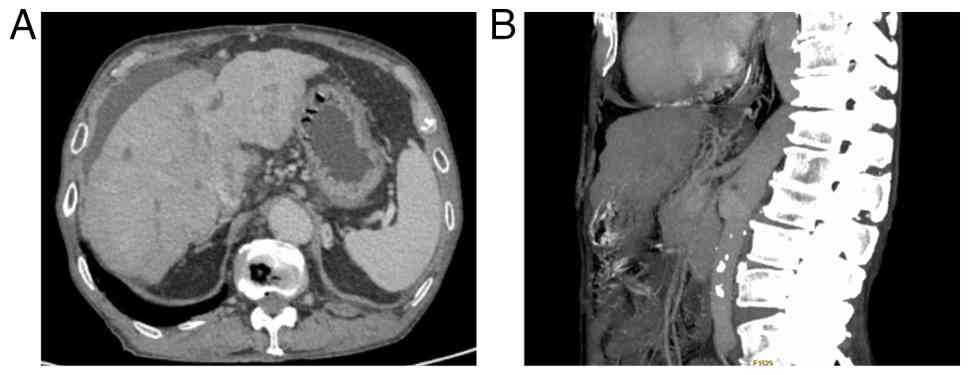
included CT scans of the chest, abdomen and pelvis. In June 2025,
CT demonstrated a nodular contour of the liver with capsular
retraction, mild ascites, and esophageal and gastric varices
(Fig. 4). The patient had no
history of alcohol consumption. Laboratory tests indicated negative
or normal results for all causes of liver disease, including
serological tests for hepatitis B and C, and serological tests for
autoimmune conditions. The patient refused to undergo a liver
biopsy. The patient's alanine aminotransferase level was 57 U/l
(normal range, 9–50 U/l), aspartate aminotransferase was 55 U/l
(normal range, 15–40 U/l), γ-glutamyl transferase was 185 U/l
(normal range, 15–40 U/l), total bilirubin was 27.9 µmol/l (normal
range, <26 µmol/l) and albumin was 29.4 g/l (normal range, 40–55
g/l). The patient underwent abdominal paracentesis, with
large-volume drainage of ascites, diuretic therapy and infusion of
human albumin (once daily, 10 g per dose) as part of active
treatment. Over the next 2 months, the Eastern Cooperative Oncology
Group (http://ecog-acrin.org/resources/ecog-performance-status/)
performance status gradually worsened. In August 2025, the patient
ultimately succumbed to hepatic failure.
Discussion
In 1924, an irregular lobulated liver contour was
first noted in the pathological changes of metastatic breast cancer
cases. Over the next decades, several reports emerged concerning
pseudocirrhosis of the liver in patients with breast cancer and
liver metastasis (1,14,15).
According to the literature, ~80% of cases of pseudocirrhosis occur
in patients with liver metastases from breast cancer (16). To the best of our knowledge, the
present study reports the first case of pseudocirrhosis developing
after treatment for hepatic metastases from squamous cell lung
carcinoma.
To date, there are no definitive diagnostic criteria
for pseudocirrhosis. The diagnosis of pseudocirrhosis is based on
characteristic imaging findings. The most common radiological
manifestation of pseudocirrhosis is the formation of diffuse
hepatic nodules, capsular retraction and enlargement of the caudate
lobe (17) Some patients can
develop features of portal hypertension, including portal-systemic
collateral circulation, splenomegaly and ascites (14). Reviewing the patient's medical
history and prior imaging studies can help identify pseudocirrhosis
caused by treated cancer metastases, while other chronic liver
diseases leading to cirrhosis must be ruled out. Portal
hypertension is the most frequent complication in patients with
pseudocirrhosis. The primary clinical manifestations include
ascites, splenomegaly with hypersplenism and esophagogastric
varices (18).
The pathogenesis of pseudocirrhosis remains poorly
understood. A retrospective analysis of patients with metastatic
breast cancer undergoing continuous treatment revealed that 55% of
those with liver metastases developed pseudocirrhosis, and all
patients with pseudocirrhosis had liver metastases (18). Despite undergoing chemotherapy,
patients without liver metastases typically do not develop
pseudocirrhosis. Several reports have suggested that
pseudocirrhosis may be associated with chemotherapy, as
chemotherapeutic agents can induce liver injury leading to nodular
regenerative hepatocyte hyperplasia. Studies have also suggested
that various chemotherapeutic drugs, such as paclitaxel,
capecitabine and doxorubicin, can induce vascular damage, including
sinusoidal spherical dilatation, microvascular injury, nodular
regenerative hepatocyte hyperplasia formation and long-term
fibrosis (2,3,16).
Alternatively, it has been proposed that pseudocirrhosis occurs as
potent cytotoxic anticancer drugs cause rapid shrinkage of liver
metastases, leading to compensatory fibrotic proliferation
(19). However, it has also been
indicated that pseudocirrhosis can occur in chemotherapy-naive
patients, and that it correlates positively with tumor size or
progression-related fibrosis (14).
Increased nodular regrowth, recurrent tumor cell infiltration and
accumulation of surrounding fibrosis cause distortion of hepatic
vessels and occlusion of some small hepatic veins or terminal
branches of the portal vein, leading to portal hypertension
(19). Overall, the
pathophysiological mechanisms underlying pseudocirrhosis are
diverse and sometimes overlap, and they remain incompletely
understood at present.
There is no specific treatment for pseudocirrhosis.
Whether it is associated with breast cancer or other tumors, when
pseudocirrhosis occurs, suspected causative medications should be
discontinued immediately. For ascites, symptomatic management
should be initiated promptly, including diuretics, albumin infusion
and paracentesis (9,11,20).
Transjugular intrahepatic portosystemic shunt (TIPS) is safe and
associated with few perioperative complications when used to treat
malignant symptomatic pseudocirrhosis, with clinical efficacy
comparable to TIPS for benign conditions (10).
The prognosis for pseudocirrhosis is generally poor.
In patients with breast cancer accompanied by pseudocirrhosis, the
median overall survival time from pseudocirrhosis onset to death
was recorded as 7.9 months (21). A
retrospective study by Engelmann et al (3), involving 48 patients with breast
cancer complicated by pseudocirrhosis, reported that the median
overall survival time following the emergence of abnormal liver
contours in this cohort was 8.5 months. The onset of
pseudocirrhosis in cancer types other than breast cancer ranges
from 3 to 17 months (4,8,9,11).
Treatment follows the same approach as that for cirrhosis,
primarily involving symptomatic management such as diuretics, human
albumin infusion, paracentesis and esophageal-gastric variceal
ligation.
Early identification of pseudocirrhosis is crucial.
Pseudocirrhosis may be a reversible condition. Two cases have been
reported where liver function recovered in patients with
pseudocirrhosis following active treatment. A patient with rectal
cancer and multiple liver metastases developed pseudocirrhosis
after regorafenib treatment. Following discontinuation of
regorafenib and aggressive supportive symptomatic management, the
patient's condition improved after 1 month (4). Another case of pancreatic cancer with
multiple liver metastases developed pseudocirrhosis following
chemotherapy. After discontinuing chemotherapy and administering
diuretics and human albumin infusion, both the imaging and clinical
manifestations of pseudocirrhosis were markedly resolved (5).
In conclusion, pseudocirrhosis most commonly occurs
in patients with metastatic breast cancer involving liver
metastases. Patients with other types of malignant tumors may also
develop the condition. Despite being termed ‘pseudocirrhosis’, its
clinical significance is comparable to that of ‘true’ cirrhosis.
Clinicians should remain vigilant for the possibility of
pseudocirrhosis in patients undergoing treatment for liver
metastases. Timely identification and treatment of these patients
can reduce the mortality associated with pseudocirrhosis.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
QL was responsible for investigation, acquisition of
data and writing the original draft. YLiu advised on patient
treatment, reviewed and edited the manuscript. DW and YLu obtained
medical images and analyzed patient data. JY performed the
histological examination of the tumor, and contributed to writing
the manuscript. DW and YLu confirm the authenticity of all the raw
data. All authors have read and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient's son for publication of the patient's clinical details and
any accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Young ST, Paulson EK, Washington K,
Gulliver DJ, Vredenburgh JJ and Baker ME: CT of the liver in
patients with metastatic breast carcinoma treated by chemotherapy:
Findings simulating cirrhosis. Am J Roentgenol. 163:1385–1388.
1994. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Jeong WK, Choi S and Kim J:
Pseudocirrhosis as a complication after chemotherapy for hepatic
metastasis from breast cancer. Clin Mol Hepatol. 19:190–194. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Engelman D, Moreau M, Lepida A, Zaouak Y,
Paesmans M and Awada A: Metastatic breast cancer and
pseudocirrhosis: An unknown clinical entity. ESMO Open.
5:e0006952020. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kumamoto K, Endo S, Isohata N, Nirei A,
Nemoto D, Utano K, Saito T and Togashi K: Pseudocirrhosis caused by
regorafenib in an advanced rectal cancer patient with multiple
liver metastases. Mol Clin Oncol. 6:63–66. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kang SP, Taddei T, McLennan B and Lac J:
Pseudocirrhosis in a pancreatic cancer patient with liver
metastases: A case report of complete resolution of pseudocirrhosis
with an early recognition and management. World J Gastroentero.
14:1622–1624. 2008. View Article : Google Scholar
|
|
6
|
Kobashigawa C, Nakamoto M, Hokama A,
Hirata T, Kinjo F and Fujita J: Pseudocirrhosis in metastatic
esophageal cancer. South Med J. 103:488–489. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Shijubou N, Sumi T, Keira Y, Shiraishi H,
Nagahisa Y, Matsuura K, Sekikawa M, Yamada Y, Nakata H and Chiba H:
Pseudocirrhosis due to liver metastasis from lung adenocarcinoma.
Thorac Cancer. 12:2407–2410. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Nakano S, Suzuki T, Takase Y, Ito M, Osaki
T, Yoshii A and Terauchi T: Pseudocirrhosis caused by lung
adenocarcinoma with diffuse liver metastasis: An autopsy case
report. Thorac Cancer. 12:2046–2049. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Shinoda T, Tanahashi T, Sakuratani T, Ota
M, Fujibayashi S, Kiriyama S, Matsumoto K, Yawata K, Sasaki Y,
Osada S and Yamada M: Pseudocirrhosis after chemotherapy for
gastric cancer with diffuse liver metastases: A case report. Mol
Clin Oncol. 16:112022. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Shreve LA, Leary CO, Clark TWI,
Stavropoulos SW and Soulen MC: Transjugular intrahepatic
portosystemic shunt for the management of symptomatic malignant
pseudocirrhosis. J Gastrointest Oncol. 13:279–287. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Harry BL, Smith ML, Burton JRJ, Dasari A,
Eckhardt SG and Diamond JR: Medullary thyroid cancer and
pseudocirrhosis: Case report and literature review. Curr Oncol.
19:e36–e41. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sadlik G, Anderson R, Lei X, Cen SY,
Duddalwar VA and Fong T: Pseudocirrhosis: A case series with
clinical and radiographic correlation and review of the literature.
Digest Dis Sci. 69:1004–1014. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Amin MB, Greene FL, Edge SB, Compton CC,
Gershenwald JE, Brookland RK, Meyer L, Gress DM, Byrd DR and
Winchester DP: The Eighth edition AJCC Cancer staging manual:
Continuing to build a bridge from a population-based to a more
‘personalized’ approach to cancer staging. CA Cancer J Clin.
67:93–99. 2017.PubMed/NCBI
|
|
14
|
Vuppalanchi R, Saxena R, Storniolo AMV and
Chalasani N: Pseudocirrhosis and liver failure in patients with
metastatic breast cancer after treatment with palbociclib.
Hepatology. 65:1762–1764. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Qayyum A, Lee GK, Yeh BM, Allen JN, Venook
AP and Coakley FV: Frequency of hepatic contour abnormalities and
signs of portal hypertension at CT in patients receiving
chemotherapy for breast cancer metastatic to the liver. Clin Imag.
31:6–10. 2007. View Article : Google Scholar
|
|
16
|
Villani R, Di Cosimo F, Sangineto M,
Romano AD and Serviddio G: Pseudocirrhosis and portal hypertension
in patients with metastatic cancers: A systematic review and
meta-analysis. Sci Rep. 12:198652022. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Jha P, Poder L, Wang ZJ, Westphalen AC,
Yeh BM and Coakley FV: Radiologic Mimics of Cirrhosis. Am J
Roentgenol. 194:993–999. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Oliai C, Douek ML, Rhoane C, Bhutada A, Ge
PS, Runyon BA, Wang X and Hurvitz SA: Clinical features of
pseudocirrhosis in metastatic breast cancer. Breast Cancer Res
Treat. 177:409–417. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Sonnenblick A, Appelbaum L and Peretz T:
Liver failure on the background of pseudocirrhosis in patients with
liver metastasis from breast cancer, who responded to treatment.
Onkologie. 34:199–201. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ma WL, Chang DY, Lin CH, Liu KL, Liang PC,
Lien HC, Hu CC, Huang LY, Yeh YC and Lu YS: Clinical outcomes of
metastatic breast cancer in patients having imaging liver
pseudocirrhosis with or without evident Varices. Oncologist.
27:1008–1015. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Huppert LA, Walker Z, Li M, Kim MO, Callan
J, Brandman D, Majure M, Melisko ME, Rugo HS, Behr S and Chien AJ:
Clinical characteristics and outcomes in patients with metastatic
breast cancer and pseudocirrhosis: A single center retrospective
cohort study. Breast Cancer Res Treat. 197:137–148. 2022.
View Article : Google Scholar : PubMed/NCBI
|