Introduction
Pancreatic head tumors are most commonly diagnosed
as primary pancreatic neoplasms, particularly pancreatic ductal
adenocarcinoma, which remains one of the leading causes of
cancer-related mortality worldwide (1). Despite advances in systemic therapy,
surgical resection by pancreaticoduodenectomy remains the only
potentially curative treatment for primary pancreatic head
malignancies and is therefore frequently performed when imaging
suggests a primary pancreatic head tumor (2–4).
Gastric cancer is also a prevalent malignancy
globally and is characterized by well-defined lymphatic drainage
pathways, including the infrapyloric lymph nodes (station no. 6),
which are anatomically adjacent to the pancreatic head (5,6).
Although gastric cancer typically presents with identifiable
mucosal lesions, poorly differentiated tumors may infiltrate and
spread into the submucosa and metastasize to regional lymph nodes
without forming an obvious mass (7,8).
Nevertheless, metastatic lymph nodes from
gastrointestinal malignancies, particularly gastric cancer, may
occasionally present as pancreatic head masses and pose a
significant diagnostic challenge (9–11).
Such cases are especially problematic when no primary lesion is
detected on preoperative endoscopic evaluation (7,8,12). We
report a case of occult gastric cancer in which metastatic
infrapyloric lymph node involvement closely mimicked a pancreatic
head tumor, highlighting a clinically relevant diagnostic pitfall
in the surgical evaluation of pancreatic head lesions and its
implications for preoperative assessment and intraoperative
decision-making.
Case report
A 76-year-old man presented to Niigata University
Medical and Dental Hospital (Niigata, Japan) with occasional back
pain and elevated serum carbohydrate antigen 19-9 (CA 19-9) levels
(462 U/ml). Preoperative serum carcinoembryonic antigen (CEA) level
was within normal range. Contrast-enhanced computed tomography at a
referring hospital revealed a mass in the pancreatic head, and the
patient was referred to our institution for further evaluation.
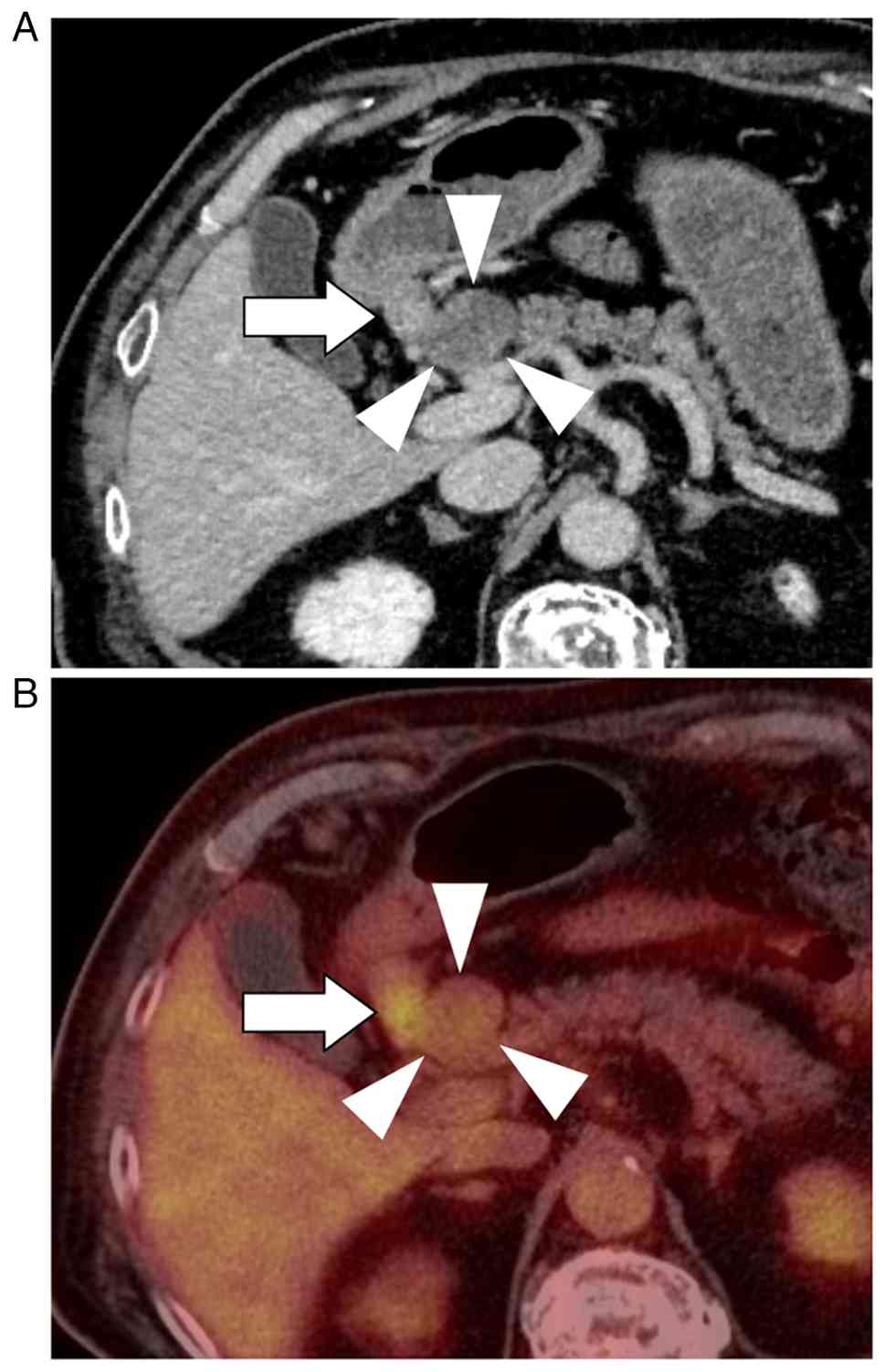
Subsequent imaging demonstrated a 30-mm protruding
mass in the pancreatic head, characterized by hypodensity in the
arterial phase and gradual enhancement in the portal and venous
phases, along with an enlarged lymph node in the infrapyloric
region (Fig. 1A). Positron emission
tomography-computed tomography demonstrated increased FDG uptake in
both the pancreatic head lesion (SUVmax, 2.74) and the infrapyloric
lymph node (station No. 6; SUVmax, 6.28), whereas no abnormal
uptake was observed in the gastric wall (Fig. 1B). Esophagogastroduodenoscopy was
performed with careful inspection of the entire stomach, including
the antrum and pyloric region. No endoscopically identifiable
lesion suggestive of primary gastric cancer was detected (Fig. S1). Endoscopic ultrasound
(EUS)-guided biopsy of the enlarged infrapyloric lymph node
demonstrated adenocarcinoma; however, the primary site of origin
could not be determined. EUS-guided sampling of the pancreatic head
lesion itself was not performed, as a safe and reliable puncture
route could not be secured due to intervening vascular
structures.
Preoperatively, the differential diagnoses included
primary pancreatic ductal adenocarcinoma, pancreatic neuroendocrine
neoplasm, malignant lymphoma, and bulky metastatic lymphadenopathy
from an occult gastrointestinal primary. Primary pancreatic ductal
adenocarcinoma was considered; however, the absence of pancreatic
ductal dilatation and the atypical protruding morphology of the
lesion made this diagnosis less likely. Pancreatic neuroendocrine
neoplasm was also considered, but was not strongly supported due to
the lack of typical hypervascular features on contrast-enhanced
imaging and normal serum neuroendocrine markers, including
neuron-specific enolase. Malignant lymphoma was included in the
differential diagnosis; however, the presence of adenocarcinoma on
biopsy of the infrapyloric lymph node and normal serum soluble
interleukin-2 receptor levels argued against this possibility.
Given the coexistence of infrapyloric lymphadenopathy and
adenocarcinoma on biopsy, bulky metastatic lymphadenopathy from an
occult gastrointestinal primary was also considered, although no
primary lesion was identified on preoperative endoscopic
evaluation.
Based on these findings, primary pancreatic cancer
including pancreatic ductal adenocarcinoma or neuroendocrine
carcinoma, which frequently includes adenocarcinoma component, with
lymph node metastasis was suspected, and pancreaticoduodenectomy
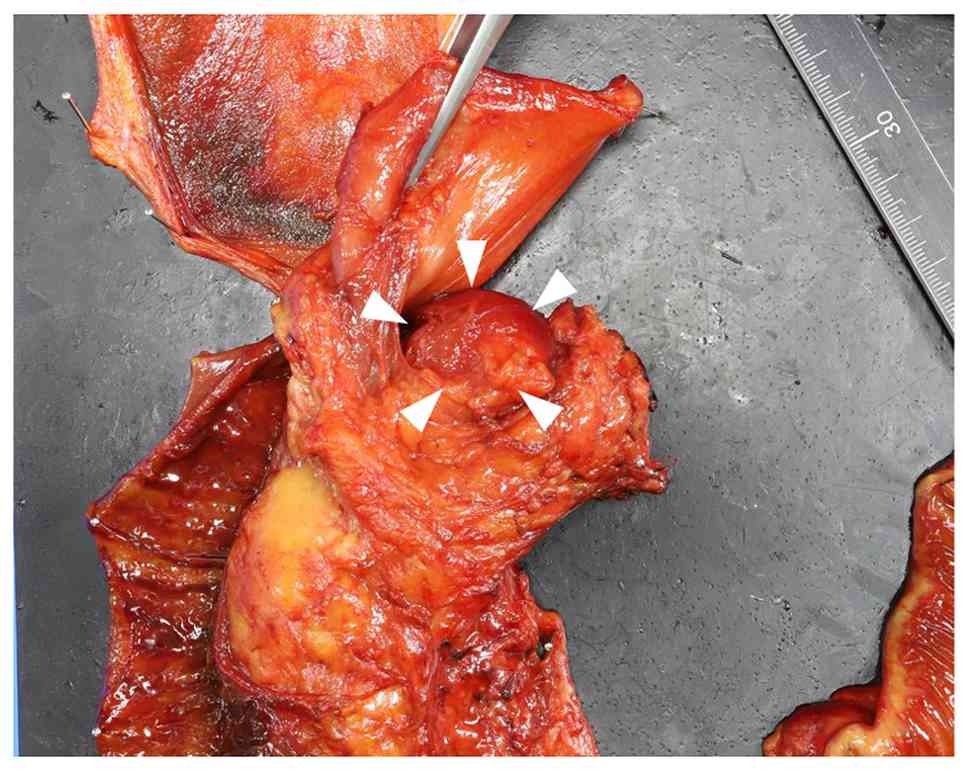
was planned. Intraoperatively, the pancreatic head lesion appeared
as a markedly protruding mass, raising suspicion of a bulky
metastatic lymph node. Consequently, the surgical procedure was
modified to include distal gastrectomy (Fig. 2).
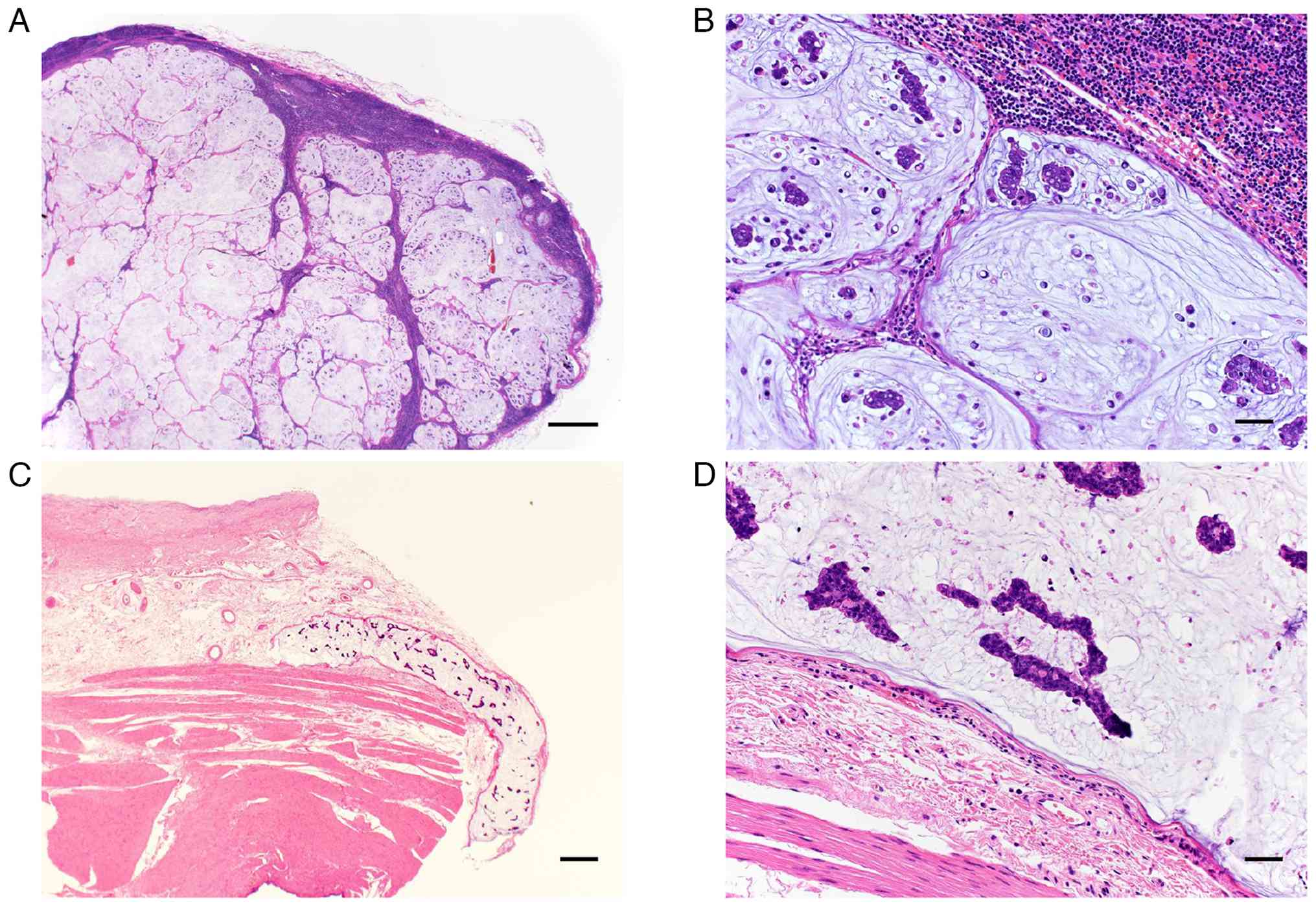
Histopathological examination revealed that the
pancreatic head lesion represented a metastatic lymph node composed
of poorly differentiated adenocarcinoma with signet ring cell
features (Fig. 3A and B).
Postoperative immunohistochemical analyses were performed on the
resected specimens, including the metastatic lymph node located at
the pancreatic head. The tumor cells were negative for
synaptophysin and chromogranin A, whereas they were positive for
cytokeratin 7, cytokeratin 20, CDX2, HNF4α, and mucin markers
(MUC2, MUC5AC, and MUC6) (data not shown), supporting a
gastrointestinal origin of the metastatic lesion.
No macroscopically identifiable primary gastric
tumor was detected in the resected stomach. However, microscopic
examination demonstrated lymphatic and vascular invasion composed
of poorly differentiated adenocarcinoma with signet ring cell
features in the submucosa of the gastric antrum along the lesser
curvature (Fig. 3C and D),
supporting the diagnosis of occult gastric cancer.
Metastatic lymph nodes were identified in the
infrapyloric region (station no. 6), the peripancreatic region
adjacent to the pancreatic head, and station no. 5. A total of 27
lymph nodes were retrieved, and metastatic involvement was
confirmed in these stations. All surgical margins were negative.
According to the UICC TNM classification (8th edition) (13), the final pathological stage was
pTxN2M0.
Postoperatively, the patient received adjuvant
chemotherapy with oral S-1 for one year. Follow-up consisted of
clinical evaluation every two months and contrast-enhanced computed
tomography every six months. Esophagogastroduodenoscopy performed
10 months after surgery revealed no remarkable findings. Serum
tumor marker levels, including CEA and CA19-9, remained within the
normal range during follow-up. The patient remains alive without
evidence of recurrence two years after surgery.
Discussion
Pancreatic head tumors are usually regarded as
primary pancreatic neoplasms and often prompt surgeons to proceed
directly to pancreaticoduodenectomy. However, bulky metastatic
lymph nodes from gastrointestinal malignancies may anatomically and
radiologically mimic pancreatic tumors, resulting in an important
oncologic diagnostic pitfall (9–11).
Metastatic involvement of the pancreas or peripancreatic region
from gastric cancer has been reported, although it remains uncommon
(11,14–18).
The present case illustrates how occult gastric cancer metastasis
can present as a pancreatic head tumor despite comprehensive
preoperative imaging and endoscopic evaluation (7,8,12,19).
From a practical standpoint, this case suggests that pancreatic
head masses presenting as protruding lesions extending outside the
pancreas and differing from the typical appearance of primary
pancreatic neoplasms should prompt consideration of metastatic
lymph node involvement, even when esophagogastroduodenoscopy
reveals no remarkable findings.
Bulky metastatic lymph nodes located in the
infrapyloric or peripancreatic region may anatomically overlap with
the pancreatic head, leading to imaging findings indistinguishable
from primary pancreatic tumors (11,15–19).
In particular, the infrapyloric lymph node (station No.6) is
situated adjacent to the pancreatic head and represents a major
lymphatic drainage pathway for distal gastric cancer (5,6).
Consequently, metastatic enlargement of these lymph nodes may
masquerade as a pancreatic head mass on computed tomography,
positron emission tomography-computed tomography, or EUS, even when
multimodal imaging is performed (10,11,20).
although adenocarcinoma was identified by preoperative biopsy of
the infrapyloric lymph node, the primary site could not be
determined, highlighting the limitation of tissue sampling in
distinguishing primary pancreatic cancer from metastatic disease
(17).
Occult gastric cancer is characterized by the
absence of an identifiable primary lesion on endoscopic examination
despite the presence of metastatic disease (7,8,19).
Poorly differentiated adenocarcinoma, including signet ring cell
carcinoma, may infiltrate the submucosa and lymphovascular
structures without forming an obvious mucosal lesion (7,8). In
the present case, microscopic vascular invasion with histological
features identical to those of the metastatic lymph nodes was
detected in the gastric submucosa, strongly suggesting a gastric
origin. This biological behavior explains why careful
esophagogastroduodenoscopy failed to detect a primary tumor and
underscores the limitation of endoscopic evaluation alone in
excluding gastric cancer. Furthermore, when postoperative
pathological examination reveals lymph node metastasis without
identification of a primary tumor, the possibility of a gastric
origin should be kept in mind, and close postoperative follow-up
with esophagogastroduodenoscopy may be appropriate.
From a surgical perspective, recognition of this
diagnostic pitfall has important implications for procedure
selection. When a protruding lesion is encountered in the
pancreatic head in association with suspicious infrapyloric
lymphadenopathy, metastatic lymph node involvement from occult
gastric cancer should be included in the differential diagnosis
(5,6). Previous studies have demonstrated that
pancreatic resection for isolated metastatic disease can be
performed safely in selected patients at high-volume centers
(17,21–23).
In the present case, intraoperative recognition of the protruding
nature of the lesion prompted modification of the surgical strategy
to include distal gastrectomy considering the possibility of the
lymph node metastasis from occult gastric cancer, enabling
oncologically appropriate en bloc resection.
This case underscores that, even when comprehensive
imaging and endoscopic evaluation suggest primary pancreatic
cancer, metastatic lymph nodes from occult gastric cancer may
represent an alternative diagnosis, particularly in the presence of
infrapyloric lymphadenopathy. Awareness of this diagnostic and
surgical pitfall is essential for appropriate surgical
decision-making when evaluating pancreatic head lesions accompanied
by perigastric lymphadenopathy.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
TA, YH, KT, JS, HIs, SA, YK, MN, HIc, YS and TW
participated in the conception and design of this report. TA and YH
drafted and revised the manuscript, and are responsible for the
paper. JS, HIs, SA and HIc provided advice on imaging findings,
interpreted the imaging data and contributed the writing of the
manuscript. KT, MN, YS and TW provided advice on histological
findings and contributed to the writing of the manuscript. KT, JS
and TW critically revised the paper. TA and YH confirm the
authenticity of all the raw data. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
The patient provided written informed consent for
the publication of the data.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Siegel RL, Giaquinto AN and Jemal A:
Cancer statics, 2024. CA Cancer J Clin. 74:12–49. 2024.PubMed/NCBI
|
|
2
|
Oba A, Del Chiaro M, Fujii T, Okano K,
Stoop TF, Wu YHA, Maekawa A, Yoshida Y, Hashimoto D, Sugawara T, et
al: ‘Conversion surgery’ for locally advanced pancreatic cancer: A
position paper by the study group at the joint meeting of the
International Association of Pancreatology (IAP) & Japan
Pancreas Society (JPS) 2022. Pancreatology. 23:712–720. 2023.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Perri G, Marchegiani G, Frigerio I,
Dervenis CG, Conlon KC, Bassi C and Salvia R: Management of
pancreatic cystic lesions. Dig Surg. 37:1–9. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Stoop TF, Javed AA, Oba A, Koerkamp BG,
Seufferlein T, Wilmink JW and Besselink MG: Pancreatic cancer.
Lancet. 405:1182–1202. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Rosa F, Costamagna G, Doglietto GB and
Alfieri S: Classification of nodal stations in gastric cancer.
Transl Gastroenterol Hepatol. 2:22017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tokunaga M, Ohyama S, Hiki N, Fukunaga T,
Yamada K, Sano T and Yamagucji T: Investigation of the lymphatic
stream of the stomach in gastric cancer with solitary lymph node
metastasis. World J Surg. 33:1235–1241. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lee SH, Lim KH, Song SY, Lee HY, Park SC,
Kang CD, Lee SJ, Choi DW, Park SB and Ryu YJ: Occult gastric cancer
with distant metastasis proven by random gastric biopsy. World J
Gastroenterol. 22:4270–4274. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kawakami N, Moriya T, Kato R, Nakamura K,
Saito H, Wakai Y, Saito K and Sakashita M: Pulmonary tumor
thrombotic microangiopathy in occult early gastric cancer that was
undetectable on upper endoscopy: A case report and review of
similar cases. BMC Gastroenterol. 21:4232021. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hammond NA, Miller FH, Day K and
Nikolaidis P: Imaging features of the less common pancreatic
masses. Abdom Imaging. 38:561–572. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
AI-Hawary MM, Kaza RK, Azar SF, Ruma JA
and Francis IR: Mimics of pancreatic ductal adenocarcinoma. Cancer
Imaging. 13:342–349. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Duan Q, Huang Y and Li H: Large metastatic
lymph nodes misdiagnosed as a pancreatic tumor: A case report. J
Surg Case Rep. 2025:rjaf5832025. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Rabenstein T, May A, Gossner L, Manner H,
Pech O, Günter E, Huijmans J, Vieth M, Stolte M and Ell C:
Invisible gastric carcinoma detected by random biopsy: Long-term
results after photodynamic therapy. Endoscopy. 40:899–904. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Brierley JD, Gospodarowicz MK and
Wittekind C: TNM Classification of Malignant Tumours. 8th edtion.
Wiley Blackwell; Chichester: pp. 93–95. 2017
|
|
14
|
Robbins EG, Franceschi D and Barkin JS:
Solitary metastatic tumors to the pancreas: A case report and
review of the literature. Am J Gastroenterol. 91:2414–2417.
1996.PubMed/NCBI
|
|
15
|
Adsay NV, Andea A, Basturk O, Kilinc N,
Nassar H and Cheng JD: Secondary tumors of the pancreas: An
analysis of a surgical and autopsy database and review of the
literature. Virchows Arch. 444:527–535. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Roalsø MT, Lucocq J, Pandanaboyama S and
Søreide K: Surgery for metastasis to the pancreas: Systematic
review of observational cohort studies. HPB (Oxford). 27:1290–1300.
2025. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Z'graggen K, Fernandez-del Castillo C,
Rattner DW and Warshaw AL: Metastases to the pancreas and their
surgical extirpation. Arch Surg. 133:413–417. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ma J, Kimura W, Takeshita A, Hirai I,
Moriya T and Mitzutani M: Neuroendocrine carcinoma of the stomach
with peripancreatic lymph node metastases successfully treated with
pancreaticoduodenectomy. Hepatogastroenterology. 54:1945–1950.
2007.PubMed/NCBI
|
|
19
|
Biswas M, Smith JC and Davies JS:
Bilateral adrenal enlargement and non-suppressible hypercortisolism
as a presenting feature of gastric cancer. Ann Clin Biochem.
41:494–497. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Tang Y, Sun X and Xu L: A slowly growing
solitary skip lymph nodule of occult gastric cancer: A case report.
Surg Case Rep. 6:1352020. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Reddy S and Wolfgang CL: The role of
surgery in the management of isolated metastases to the pancreas.
Lancet Oncol. 10:287–293. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Hiotis SP, Klimsta DS, Conlon KC and
Brennan MF: Results after pancreatic resection for metastatic
lesions. Ann Surg Oncol. 9:675–679. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Wente MN, Bergmann F, Fröhlich BE,
Schirmacher P, Bücheler MW and Freess H: Pancreatic metastasis from
gastric carcinoma: A case report. World J Surg Oncol. 2:432004.
View Article : Google Scholar : PubMed/NCBI
|