Introduction
Gastric cancer is one of the most prevalent
malignancies of the digestive system, ranking fifth in incidence
and fourth in mortality worldwide (1). At the advanced stage, gastric cancer
may metastasize to the liver, peritoneum and lungs, whereas bone
metastasis is relatively rare, occurring in ~11.3% of cases. Bone
metastasis is generally characterized by osteolytic bone
destruction and skeletal-related events (for example, pathological
fractures, spinal cord compression and hypercalcemia) (2). Related studies indicate that bone
metastasis in gastric cancer is associated with distinct
clinicopathological features (such as signet ring cell histology
and elevated alkaline phosphatase) and predicts a poor prognosis
(3).
Metastatic carcinoma of bone marrow is defined as a
group of diseases in which non-hematopoietic malignancies invade
the bone marrow through blood or lymphatic metastasis (4). As a subtype of bone metastasis, bone
marrow metastasis differs from typical osteolytic bone destruction
and predominantly manifests as hematological abnormalities. Bone
marrow metastasis is characterized by a low incidence, non-specific
clinical features and a low rate of early diagnosis (4). The present study reports a case with
bone marrow metastasis originating from gastric cancer and
describes the corresponding clinical characteristics and diagnostic
methods used based on a literature review, to provide potential
guidance for clinical diagnosis and treatment of similar cases.
Case report
A 50-year-old female patient with abdominal
distension and pain was admitted to Yichang Central People's
Hospital (Yichang, China) in September 2022. Subsequently, 8 days
later, the patient underwent 3D laparoscopic distal subtotal
gastrectomy, Y gastrojejunostomy and abdominal lymph node
dissection. The surgical specimen was fixed in 10% neutral buffered
formalin at room temperature for 24–48 h, followed by paraffin
embedding. Sections were cut at a thickness of 4 µm. Pathology
(Fig. 1A and B) revealed a poorly
differentiated gastric adenocarcinoma with a maximum diameter of
2.5 cm, which had invaded the subserosal layer of the stomach and
affected the nerves and vessels. No tumor was identified on the
bilateral resection margins. Metastasis was observed in the lymph
nodes of the perigastric adipose tissue (7/14). Immunohistochemical
staining revealed Cam5.2(+) (Fig.
1C) and HER-2(0) (Fig. 1D).
Based on the American Joint Committee on Cancer (AJCC) Cancer
Staging Manual, Eighth Edition (2017) (5), the pathological staging was pT3N3a,
with seven metastatic lymph nodes among the 14 retrieved, a yield
below the recommended minimum of 16, which may carry a risk of
stage migration. Preoperative assessment with contrast-enhanced CT
of the chest, abdomen and pelvis revealed no signs of distant
metastasis (M0). The patient was given six cycles of the XELOX
chemotherapy regimen [oxaliplatin 180 mg on day 1 (D1) and
capecitabine 1.5 g twice daily on D1-14, in a 21-day cycle] and
followed-up at 3-month intervals with gastroscopy, abdominal and
pelvic CT after chemotherapy was completed in April 2023, without
significant abnormalities.
In April 2024, the patient complained of fatigue,
poor appetite and lower back pain. The patient was admitted with
the discovery of an abdominal incisional hernia during physical
examination. Routine blood tests on admission revealed: White blood
cells count, 2.15×109/l (reference range,
3.5–9.5×109/l); red blood cells count,
2.37×1012/l (reference range, 3.8–5.1×109/l);
hemoglobin, 68 g/l (reference range, 115–150 g/l); and platelets
(PLT), 38×109/l (reference range,
125–350×109/l). Anemia-related indicators were: Serum
ferritin, 376.0 ng/ml (reference range, 13–232 ng/ml); folate,
>24 ng/ml (reference range, 5.21–20 ng/ml; and vitamin
B12, 235 pg/ml (reference range, 200–1,100 pg/ml). Tumor
markers were: Carcinoembryonic antigen (CEA) 5.5 ng/ml (reference
range, 0–6.5 ng/ml); and CA19-9, 133 U/ml (reference range, 0–39
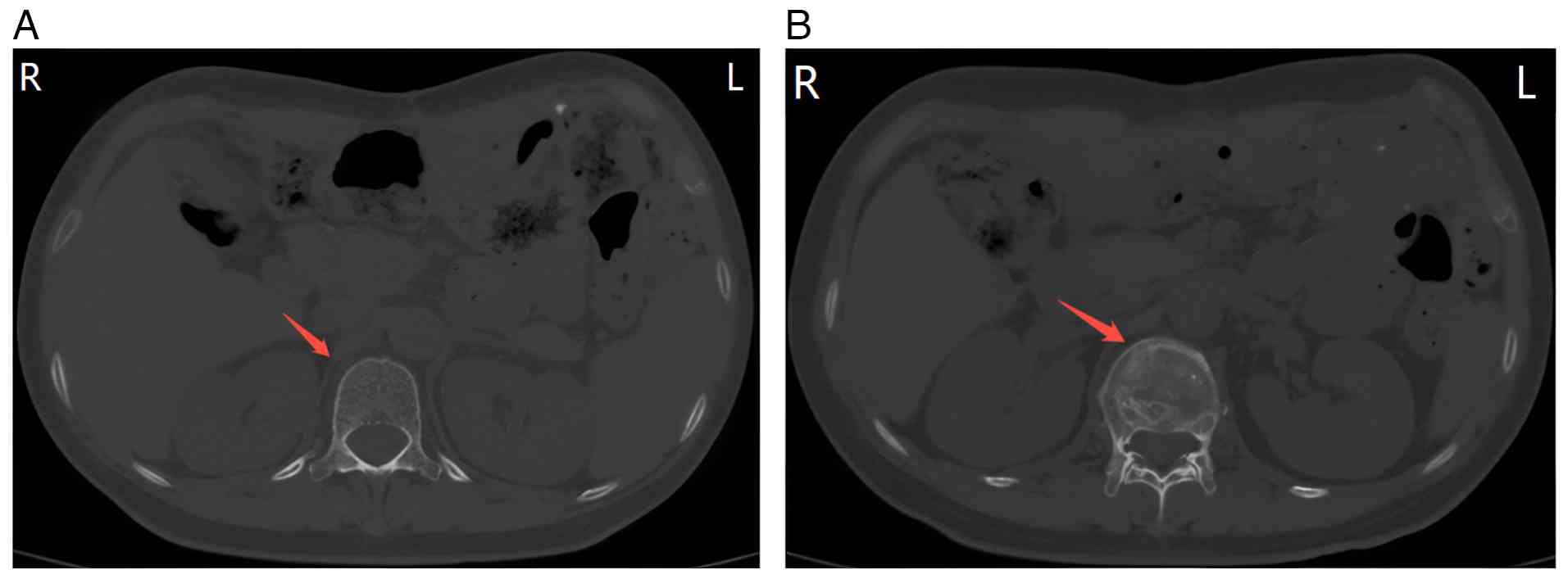
U/ml). Abdominal CT (Fig. 2) showed
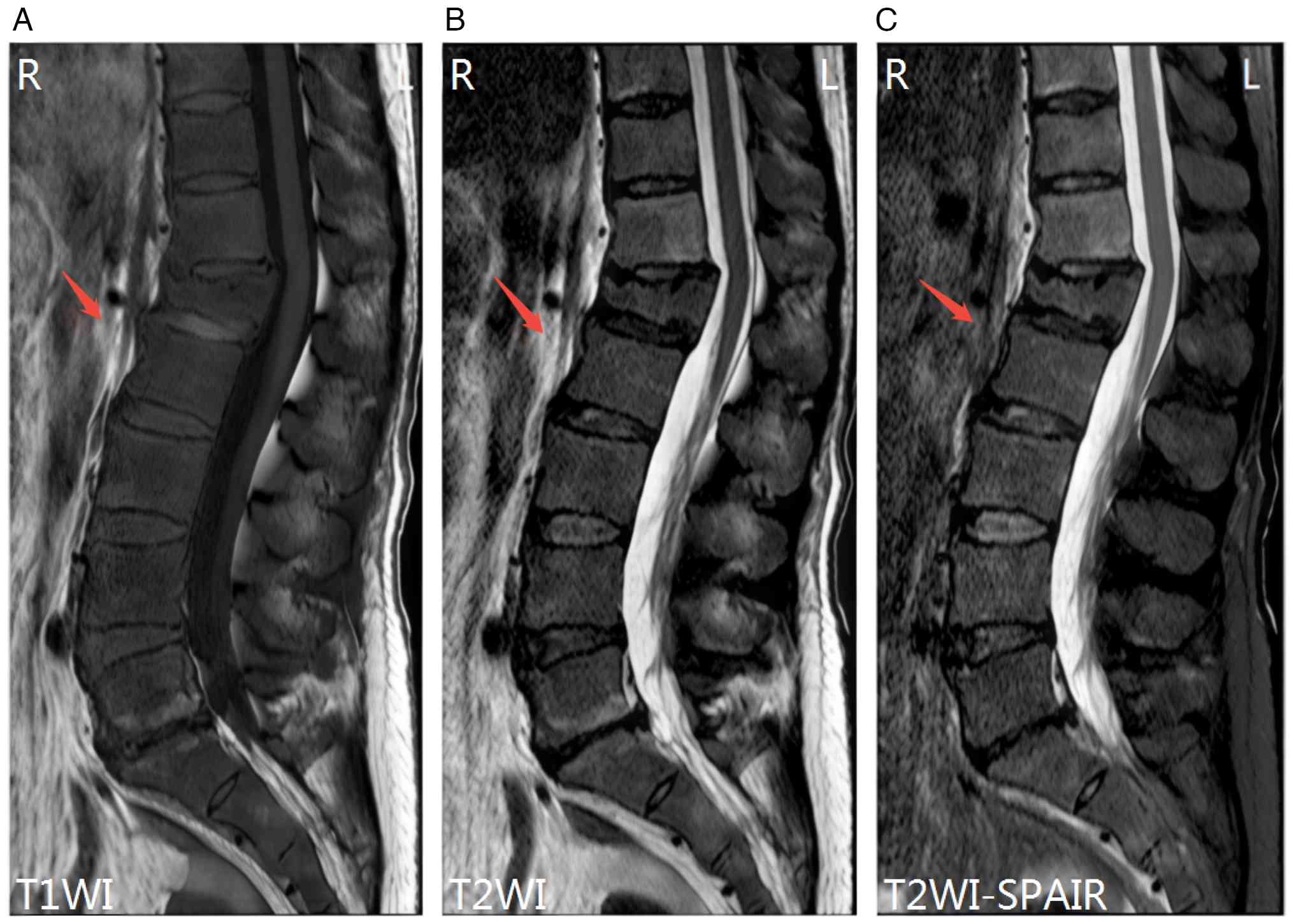
L1 vertebral compression fracture. Lumbar plain MRI (Fig. 3) showed diffuse reduction of T1 and
T2 signals in multiple thoracolumbar and sacral vertebrae.
Whole-body bone scan (Fig. 4) (3-h
acquisition after 7 mCi 99mTc-DTPA injection) showed
diffuse increased bone uptake of imaging agents (‘super-bone
scan’), suggestive of multiple bone metastases. The bone marrow
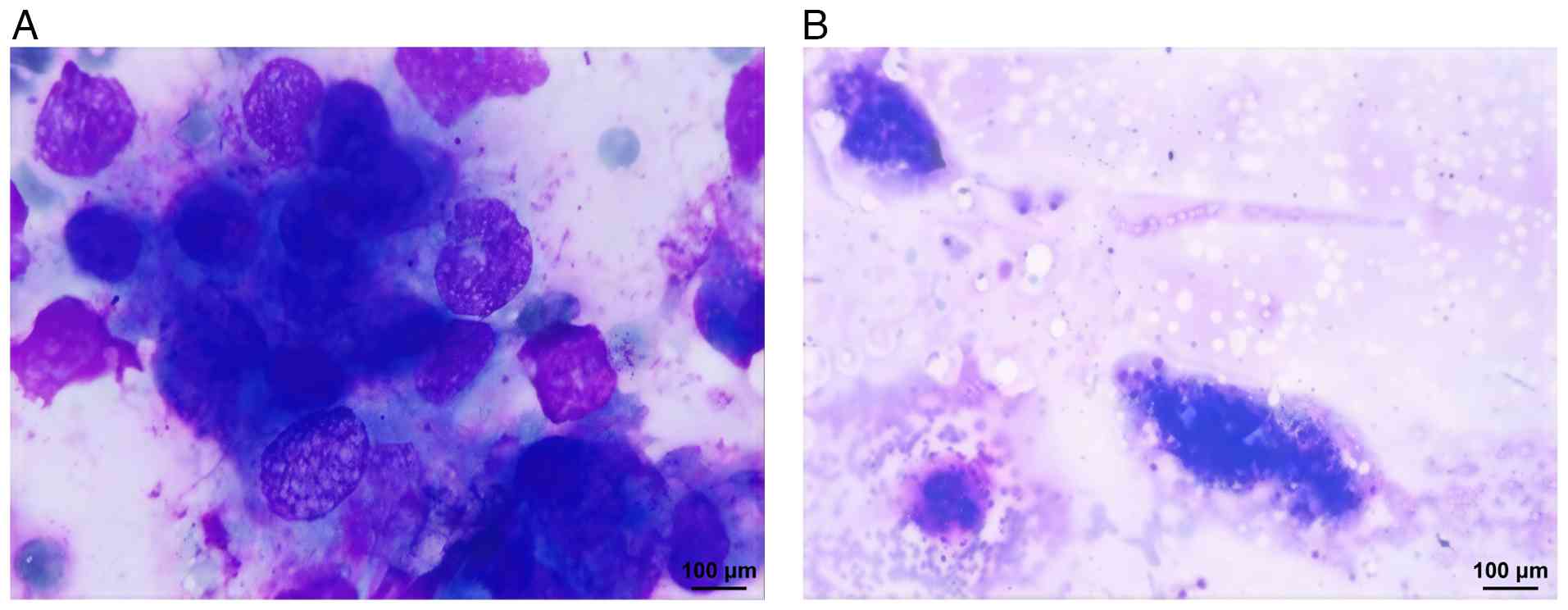
aspiration results (Fig. 5) showed
images of metastatic tumor cells, indicating tumor recurrence and
metastasis. Accordingly, the patient received five cycles of
combination regimen [albumin-bound paclitaxel 100 mg (D1,8) and
cedilimumab 200 mg (D1), in a 21-day cycle] and supplemented with
bone-modifying agent (denosumab 120 mg administered at 4-week
intervals). A partial response was achieved following five cycles
of therapy, which coincided with a steady recovery of PLT
(82×109/l) and a progressive decrease in CEA (1.4 ng/ml)
and CA19-9 (36.5 U/ml) levels.
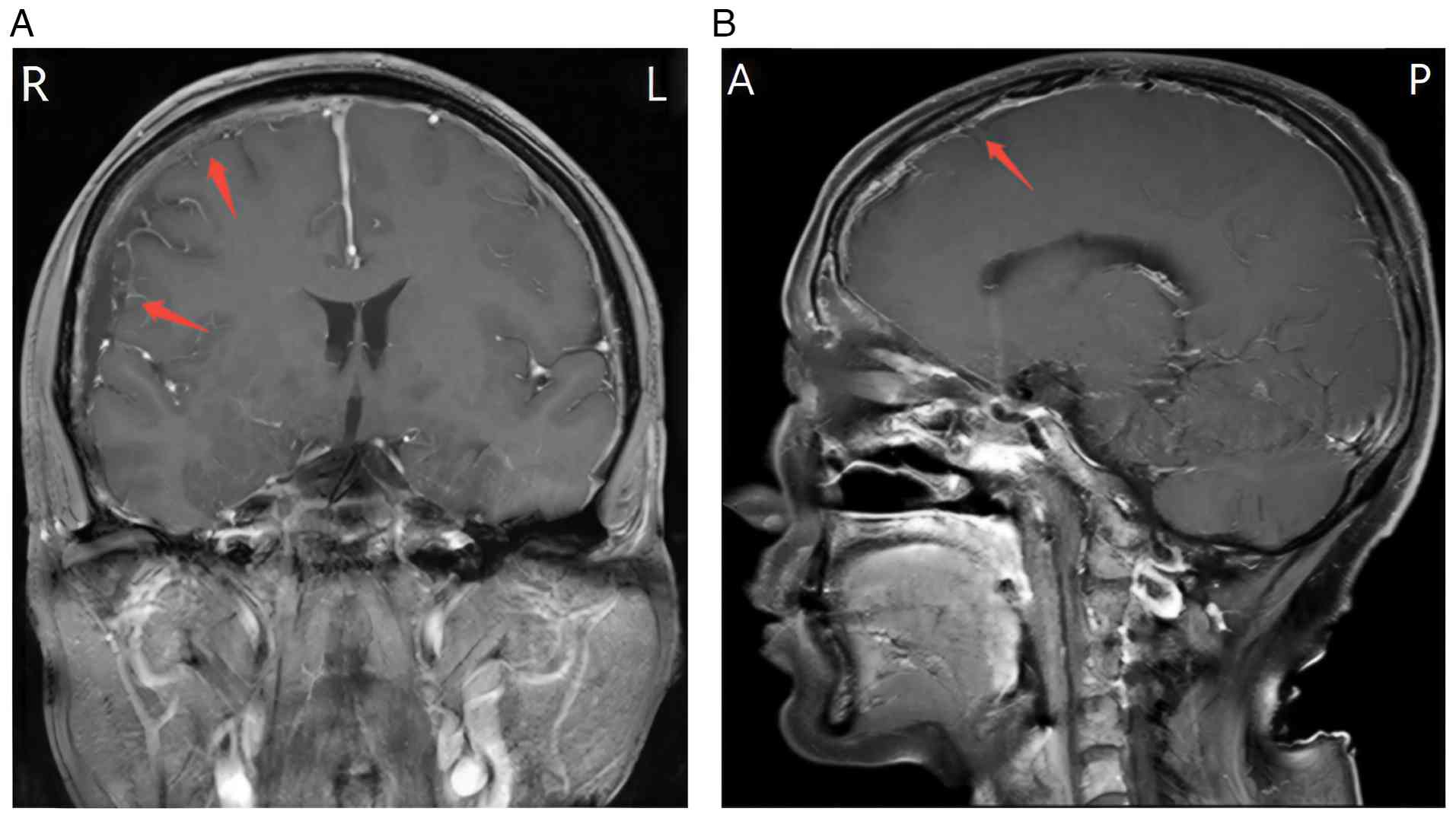
In August 2024, the patient was admitted to Yichang
Central People's Hospital (Yichang, China) with a deteriorating
left frontotemporal headache persisting for 2 weeks, accompanied by
nausea, vomiting, periorbital edema and visual disturbance.
Enhanced brain MRI (Fig. 6)
revealed extensive meningeal metastasis and slight effusion beneath
the meninges on the right forehead. In this regard, the patient was
receiving dehydration therapy to reduce intracranial pressure,
lumbar aspiration and intrathecal injection of chemotherapeutic
agent (pemetrexed 10 mg). As the family declined further treatment,
the patient was discharged in September 2024 and transferred to a
local hospital for further treatment. According to regular
follow-up, the overall survival time of the patient from the onset
of bone marrow metastasis to death was 6 months.
Discussion
Gastric cancer is a malignant tumor ranking fifth in
incidence (5.6%) and fourth in mortality (7.7%) worldwide. Most
patients are diagnosed at an advanced stage and the 5-year survival
rate is <10% (1). At the
advanced stage, metastasis may involve the liver, peritoneum and
lungs, while bone metastasis is relatively rare, occurring in
~11.3% of cases. Bone marrow metastasis is considered a subtype of
bone metastasis, showing a significantly lower incidence with no
systematic reports (6).
Metastatic carcinoma of bone marrow is defined as a
group of diseases in which non-hematopoietic malignancies invade
bone marrow through blood or lymphatic metastasis. It commonly
occurs in breast, prostate and lung cancers, whereas gastric cancer
accounts for a relatively low proportion of only 1.8% (7). With a poor understanding of its
pathogenesis at present, bone marrow metastasis is mostly believed
to be attributed to the detachment of cancer cells from the
original lesion that then enter the bloodstream. Cancer cells may
activate osteoclasts to absorb and destroy bones, providing a
favorable growth environment for the proliferation of cancer cells;
simultaneously, the growth and proliferation of cancer cells may be
boosted owing to the release of various growth factors stored in
the bone matrix into the bone marrow (4).
Bone marrow metastasis typically manifests with an
insidious onset. Clinically, patients may experience bone pain,
anemia and thrombocytopenia. An incidence of bone pain had been
reported in 65% of patients, predominantly affecting the spine and
frequently involving multiple sites. In the present case, bone pain
was the initial symptom. Patients may also develop non-infectious
fever, as well as elevation in alkaline phosphatase (ALP) and
lactate dehydrogenase (LDH) to varying degrees. Hung et al
(8) reported significant elevations
in ALP and LDH among patients with bone marrow metastasis: ALP was
elevated in 91% of cases, with 53% exceeding five times the upper
limit of the normal range, while LDH was elevated in 89%. These
findings suggested that ALP and LDH may be potential clinical
biomarkers. Meanwhile, immature cells in peripheral blood smears
are also common (9).
Bone marrow metastasis is mainly diagnosed based on
bone marrow aspiration/biopsy, MRI, whole-body bone scan and
PET/CT. Among these, bone marrow aspiration/biopsy is considered
the gold standard (10), but not
routinely performed for patients with cancer. Consequently, imaging
plays an important role in the screening and dynamic monitoring of
bone marrow metastasis.
In MRI, bone marrow metastasis may manifest as focal
or diffuse hypointensity in the vertebral body and posterior
components on T1- and T2-weighted imaging of the spine, with or
without cortical destruction (11).
In the present patient, diffuse reductions in T1 and T2 signals
were observed in the thoracolumbar and sacral vertebrae, exhibiting
typical imaging features. Nonetheless, diffuse hypointensity of T1
and T2 in spinal MRI is not a specific manifestation and may also
be observed in conditions such as multiple myeloma and
myelofibrosis (12,13). In addition, positive bone marrow
lesions on diffusion-weighted (DW)-MRI display focal or diffuse
lesions with limited diffusion. Rashidi et al (14) showed a sensitivity of 89.1% and
specificity of 100% for DW-MRI in the diagnosis of bone marrow
metastasis.
Single photon emission CT whole-body bone scan was
reported as a useful tool in the diagnosis of bone metastases, with
a sensitivity of 96.5% and specificity of 45.71% (15). Nevertheless, there is inadequate
data on its application in the diagnosis of bone marrow metastasis,
most of which were from case reports, manifested as locally active
metabolic foci, or diffuse skeletal metabolic increase throughout
the body, displayed as ‘super-bone scan’ (11). Similarly, the present case showed a
‘super-bone scan’ in whole-body bone imaging, suggesting the
possibility of multiple bone metastases. Based on the ‘seed-soil’
theory, the ‘super-bone scan’ is not only the result of a large
number of bone nutrient metastatic cancers infiltrating the bone
marrow or bone microenvironment, but also the outcome from the
interference of tumor-related endocrine factors (16).
PET/CT can be used to diagnose bone marrow
metastasis by identifying increased fluorodeoxyglucose uptake in
growing metastatic malignant tumor cells. Guinot et al
(17) found a sensitivity of 92.3%
and specificity of 99.4% for PET/CT in diagnosing bone marrow
metastasis. Moreover, combining DW-MRI with PET/CT significantly
improved diagnostic accuracy compared with DW-MRI alone (100 vs.
96.9%) (11). Basu et al
(18) proposed that a substantial
number of metabolically active tumor cells are typically present in
the bone marrow prior to the invasion of the bone matrix,
representing the initial stage of bone marrow metastasis. The
non-invasive nature of PET/CT has prompted investigations into its
potential to replace bone marrow aspiration as the diagnostic gold
standard (4). However, its clinical
application may be compromised by its high economic cost.
Several conditions should be considered when
evaluating a patient presenting with pancytopenia or bone
abnormalities on imaging. Aplastic/hypoplastic marrow failure,
characterized by pancytopenia, usually lacks bone pain or
radiographic signs of bone destruction. MRI commonly shows diffuse
hyperintensity or heterogeneous intensity on T1-weighted imaging,
and isointensity on T2-weighted imaging (19). Whole-body bone scans typically
appear unremarkable. Multiple myeloma similarly manifests bone pain
and osteolytic lesions (20);
nonetheless, it is frequently accompanied by renal impairment and
elevated levels of monoclonal protein in serum or urine, which are
crucial distinguishing features (21). Infection-related marrow suppression
(such as septicemia) may also present with pancytopenia (22). This condition is generally
characterized by fever and elevated inflammatory markers, but lacks
bone abnormalities on imaging. Furthermore, a comprehensive
immunohistochemical panel including epithelial/site-directed
markers [for example, cytokeratin (CK) AE1/AE3, CK7/CK20,
caudal-type homeobox 2, E-cadherin, mucin 1/2, HER2 and Ki-67] and
hematolymphoid markers (for example, myeloperoxidase, CD34 and
CD117) would have been valuable to confirm the epithelial origin
and exclude hematological malignancies in the present case
(23). As the current study was
retrospective with difficult access to additional bone marrow
aspiration samples, we were unable to conduct additional staining,
which represents a limitation of the present study. Future
prospective studies incorporating this panel are warranted to
definitively characterize bone marrow involvement and improve
diagnostic accuracy.
Bone marrow aspiration/biopsy remains the diagnostic
gold standard. Still, early detection is challenging when tumor
cells have not yet significantly proliferated within the marrow. In
a recent study, Dello Spedale Venti et al (24) revealed significant quantitative and
qualitative changes in bone marrow adiposity in biopsy samples.
These findings suggested that changes in bone marrow adiposity may
also be a potential biomarker for early bone marrow metastasis,
which requires validation through large studies in the future.
Bone marrow metastasis from gastric cancer is
commonly treated with symptomatic and comprehensive treatment.
Prognosis remains extremely poor, with a median overall survival of
6 months. In an analysis using a multivariate Cox proportional
hazards model, Sakin et al (25) identified chemotherapy as an
independent factor associated with improved prognosis. Nonetheless,
hemocytopenia resulting from bone marrow metastasis impedes
antitumor treatment significantly. Currently, it is recommended to
adopt systemic chemotherapy and/or targeted therapy based on the
genetic characteristics of tumors, combined with sufficient
supportive treatments (for example, blood transfusion, granulocyte
colony-stimulating factor, erythropoietin and thrombopoietin)
(26).
Following a partial response to systemic therapy,
the present patient subsequently developed meningeal metastases, a
severe complication with an intricate pathogenesis. The progression
of the disease may involve various mechanisms (27). Firstly, hematogenous dissemination
represents a primary pathway. The presence of bone marrow
metastasis in the present case may have provided a reservoir for
tumor cells to enter the circulation and invade the meninges.
Moreover, chemotherapy-induced resistance may select for clones
exhibiting enhanced migratory and invasive properties, thereby
predisposing them to central nervous system infiltration.
Additionally, alterations in the blood-brain barrier following
systemic therapy could facilitate tumor cell extravasation and
meningeal metastasis (28).
In conclusion, metastatic carcinoma of bone marrow
is a rare clinical disease with non-specific clinical
manifestations, low rates of early diagnosis and a poor prognosis.
The patient reported in the present study developed symptoms
related to bone marrow metastasis 1 year after completing
chemotherapy for gastric cancer. During this period, the patient
was examined without significant abnormalities in routine blood
tests and CT scans, but there was a diffuse reduction in the
thoracolumbar and sacral vertebrae signals in MRI. The diagnosis
was ultimately established through a subsequent whole-body bone
scan and bone marrow aspiration. Consequently, to improve the
prognosis of patients with bone marrow metastasis, it is important
to improve clinician awareness of bone marrow metastasis from solid
tumors, optimize diagnostic processes, increase early diagnosis
rates and develop standardized treatment plans.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
XW, WD and PD conceived and designed the study. XW
collected and assembled all clinical data, including imaging
studies and laboratory results, and analyzed and interpreted the
data. WD and PD critically reviewed and revised the manuscript for
important intellectual content. XW, WD and PD confirm the
authenticity of all the raw data. All authors contributed to the
article and read and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
The patient's next of kin provided written informed
consent for publication, authorizing the use of the patient's
imaging, pathological and clinical data for publication.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Peng H, Jiang L, Yuan J, Wu X, Chen N, Liu
D, Liang Y, Xie Y, Jia K, Li Y, et al: Single-cell characterization
of differentiation trajectories and drug resistance features in
gastric cancer with peritoneal metastasis. Clin Transl Med.
14:e700542024. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ren S, Wei Y, Liu W, Zhang Y, Wang Y, Yang
J, Liu B, Shi T and Wei J: Clinical characteristics, prognostic
factors and therapeutic strategies in gastric cancer patients with
bone metastasis: A retrospective analysis. Cancer Med.
14:e707812025. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kim YJ, Kim SH, Kim JW, Lee JO, Kim JH,
Bang SM, Lee JS and Lee KW: Gastric cancer with initial bone
metastasis: A distinct group of diseases with poor prognosis. Eur J
Cancer. 50:2810–2821. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zhang L, Chen F, Xu L, Li N, Zhuo Q, Guo
Y, Wang X, Wen M, Zhao Z and Li M: Comprehensive review of solid
tumor bone marrow metastasis. Crit Rev Oncol Hematol.
194:1042482024. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
In H, Solsky I, Palis B, Langdon-Embry M,
Ajani J and Sano T: Validation of the 8th edition of the AJCC TNM
staging system for gastric cancer using the national cancer
database. Ann Surg Oncol. 24:3683–3691. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sung H, Ferlay J, Siegel RL, Laversanne M,
Soerjomataram I, Jemal A and Bray F: Global cancer statistics 2020:
GLOBOCAN estimates of incidence and mortality worldwide for 36
cancers in 185 countries. CA Cancer J Clin. 71:209–249.
2021.PubMed/NCBI
|
|
7
|
Krishnan C, George TI and Arber DA: Bone
marrow metastases: A survey of nonhematologic metastases with
immunohistochemical study of metastatic carcinomas. Appl
Immunohistochem Mol Morphol. 15:1–7. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hung YS, Chou WC, Chen TD, Chen TC, Wang
PN, Chang H, Hsu HC, Shen WC, Cheng WH and Chen JS: Prognostic
factors in adult patients with solid cancers and bone marrow
metastases. Asian Pac J Cancer Prev. 15:61–67. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kumar S, Kumar K, Agrawal R and Choudhary
V: Bone marrow metastasis in non-hematological malignancies: Data
from a tertiary care hospital in North India. Cureus.
17:e827572025.PubMed/NCBI
|
|
10
|
Chandra S and Chandra H: Comparison of
bone marrow aspirate cytology, touch imprint cytology and trephine
biopsy for bone marrow evaluation. Hematol Rep. 3:e222011.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kanazawa K and Isozaki E: ‘Super bone
scan’ in a case of diffuse bone marrow metastasis of gastric
adenocarcinoma. Intern Med. 48:1719–1720. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Caranci F, Tedeschi E, Ugga L, D'Amico A,
Schipani S, Bartollino S, Russo C, Splendiani A, Briganti F, Zappia
M, et al: Magnetic resonance imaging correlates of benign and
malignant alterations of the spinal bone marrow. Acta Biomed.
89:18–33. 2018.PubMed/NCBI
|
|
13
|
Vande Berg BC, Kirchgesner T, Acid S,
Malghem J, Vekemans MC and Lecouvet FE: Diffuse vertebral marrow
changes at MRI: Multiple myeloma or normal? Skeletal Radiol.
51:89–99. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Rashidi A, Baratto L, Theruvath AJ, Greene
EB, Hawk KE, Lu R, Link MP, Spunt SL and Daldrup-Link HE:
Diagnostic accuracy of 2-[18F]FDG-PET and whole-body DW-MRI for the
detection of bone marrow metastases in children and young adults.
Eur Radiol. 32:4967–4979. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Mutuleanu MD, Paun DL, Lazar AM, Petroiu
C, Trifanescu OG, Anghel RM and Gherghe M: Quantitative vs.
qualitative SPECT-CT diagnostic accuracy in bone lesion
evaluation-A review of the literature. Diagnostics (Basel).
13:29712023. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Lin CY, Chen YW, Chang CC, Yang WC, Huang
CJ and Hou MF: Bone metastasis versus bone marrow metastasis?
Integration of diagnosis by 18F-fluorodeoxyglucose positron
emission/computed tomography in advanced malignancy with super bone
scan: Two case reports and literature review. Kaohsiung J Med Sci.
29:229–233. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Guinot A, Tabone-Eglinger S, Isnardi V,
Bahri H, Surdez D, Delattre O, Pierron G, Villemeur M, Lapouble E,
Brahmi M, et al: Staging of newly diagnosed Ewing sarcoma: Results
of bone marrow aspiration and biopsy versus 18FDG-PET/CT imaging
for bone marrow involvement. Eur J Cancer. 179:56–64. 2023.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Basu S, Torigian D and Alavi A: Evolving
concept of imaging bone marrow metastasis in the twenty-first
century: Critical role of FDG-PET. Eur J Nucl Med Mol Imaging.
35:465–471. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Yang X, Bai Y, Guo H, Shi M, Zhang W, Pei
Y, Song J, Drokow EK, Huang G, Liu X, Xu J and Kai Sun: Evaluating
and monitoring bone marrow hypoplasia in adults with aplastic
anemia via high-resolution iliac magnetic resonance imaging in the
current era. Medicine (Baltimore). 98:e182142019. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Wu F, Bernard S, Fayad LM, Ilaslan H,
Messiou C, Moulopoulos LA and Mulligan ME: Updates and ongoing
challenges in imaging of multiple myeloma: AJR expert panel
narrative review. AJR Am J Roentgenol. 217:775–785. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Malard F, Neri P, Bahlis NJ, Terpos E,
Moukalled N, Hungria VTM, Manier S and Mohty M: Multiple myeloma.
Nat Rev Dis Primers. 10:452025. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Tiewsoh I, Dey B, Chhangte M, Lyngdoh M
and Sathees V: Methotrexate-induced septicemia with severe
pancytopenia and diffuse cutaneous ulcerative lesions. Cureus.
13:e180692021.PubMed/NCBI
|
|
23
|
Landry M, Bienz MN, Sawan B, Temmar R,
Beauregard P, Chaunt F, Lavigne J and Knecht H: Bone marrow
immunohistochemistry and flow cytometry in the diagnosis of
malignant hematologic diseases with emphasis on lymphomas: A
comparative retrospective study. Appl Immunohistochem Mol Morphol.
28:508–512. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Dello Spedale Venti M, Palmisano B,
Donsante S, Farinacci G, Adotti F, Coletta I, Serafini M, Corsi A
and Riminucci M: Morphological and immunophenotypical changes of
human bone marrow adipocytes in marrow metastasis and
myelofibrosis. Front Endocrinol (Lausanne). 13:8823792022.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Sakin A, Sakalar T, Sahin S, Yasar N,
Demir C, Geredeli C and Cihan S: Factors affecting survival and
treatment efficacy in breast cancer patients with bone marrow
metastasis. Breast J. 26:815–818. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Wang D, Luo Y, Shen D, Yang L, Liu HY and
Che YQ: Clinical features and treatment of patients with lung
adenocarcinoma with bone marrow metastasis. Tumori. 105:388–393.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Yue Y, Ren Y, Lu C, Jiang N, Wang S, Fu J,
Kong M and Zhang G: The research progress on meningeal metastasis
in solid tumors. Discov Oncol. 16:2542025. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Karschnia P, Nelson TA and Dietrich J:
Mechanisms and treatment of cancer therapy-induced peripheral and
central neurotoxicity. Nat Rev Cancer. 25:887–909. 2025. View Article : Google Scholar : PubMed/NCBI
|















![Histological and immunohistochemical
analysis. The surgical specimen was fixed in 10% neutral buffered
formalin at room temperature for 24–48 h, followed by paraffin
embedding. Sections were cut at a thickness of 4 µm. Histological
image of poorly differentiated gastric adenocarcinoma
[hematoxylin-eosin stain; (A) ×40 magnification; (B) ×100
magnification]. Representative immunohistochemistry (×100
magnification) showing (C) Cam5.2 positivity and (D) HER-2
negativity.](/article_images/ol/31/5/ol-31-05-15528-g00.jpg)