Introduction
Hepatic small cell neuroendocrine carcinoma (HSCNEC)
is a poorly differentiated neuroendocrine tumor that is exceedingly
rare in clinical practice. Hepatic neuroendocrine tumors account
for ~0.3% of all neuroendocrine tumors (1). NEC is characterized by poorly
differentiated neuroendocrine tumor morphology and includes SCNEC
and large CNEC. These tumors are highly malignant and associated
with a poor prognosis. Furthermore, NECs generally carry a poorer
prognosis than neuroendocrine tumors (2), with a median survival of merely 11–12
months for metastatic disease (3).
Due to the high heterogeneity of NEC and the fact that most cases
are non-functional (i.e., they do not secrete hormones or bioactive
amines that cause a clinical syndrome), there is a lack of specific
biomarkers, making diagnosis challenging and treatment pathways
complex and varied (4). However,
with advancements in medical technology, transcatheter arterial
chemoembolization (TACE) combined with targeted immunotherapy has
emerged as an important treatment modality for advanced liver
cancers, including HSCNEC (5).
The current study presents a detailed analysis of
two recent cases of HSCNEC managed with comprehensive therapy. The
clinical characteristics and treatment decisions of these cases
were summarized to enhance the diagnostic and therapeutic
capabilities for such diseases, providing valuable insights for
clinical treatment decision-making.
Case report
Case 1
The patient was a 76-year-old male who was admitted
to Hebei General Hospital (Shijiazhuang, China) in July 2025 due to
intermittent pain in the right upper abdomen for the past 3 months.
Upon admission, the physical examination revealed significant
tenderness primarily in the right upper abdomen. The patient had a
history of hepatitis B for 50 years, hypertension for 20 years,
diabetes for 10 years and coronary artery disease for 5 years. A
complete blood count on admission showed a neutrophil percentage of
77.70% (normal range: 40–75%). Biochemical tests showed total
bilirubin at 92.7 µmol/l (normal: 5.1–17.1 µmol/l), direct
bilirubin at 53.3 µmol/l (normal: 0–5.1 µmol/l), indirect bilirubin
at 39.4 µmol/l (normal: 3.4–12.0 µmol/l), alanine aminotransferase
(ALT) at 141.1 U/l (normal: 7–40 U/l), aspartate aminotransferase
(AST) at 141.8 U/l (normal <40 U/l), gamma-glutamyl transferase
at 556.8 U/l (normal: 8–61 U/l) and alkaline phosphatase at 628.8
U/l (normal: 40–129 U/l). Tumor markers indicated carcinoembryonic
antigen (CEA) at 221.300 ng/ml (normal: <5 ng/ml), while other
laboratory results showed no significant abnormalities. All the
reported laboratory parameters were abnormal and elevated compared
to their respective normal ranges. This profile indicates
neutrophilia, significant conjugated hyperbilirubinemia, marked
elevation of cholestatic enzymes (ALP, GGT) and elevated
hepatocellular enzymes (ALT, AST), consistent with significant
hepatobiliary disease and possible obstruction. The CEA level was
also markedly elevated, suggestive of a malignant process.
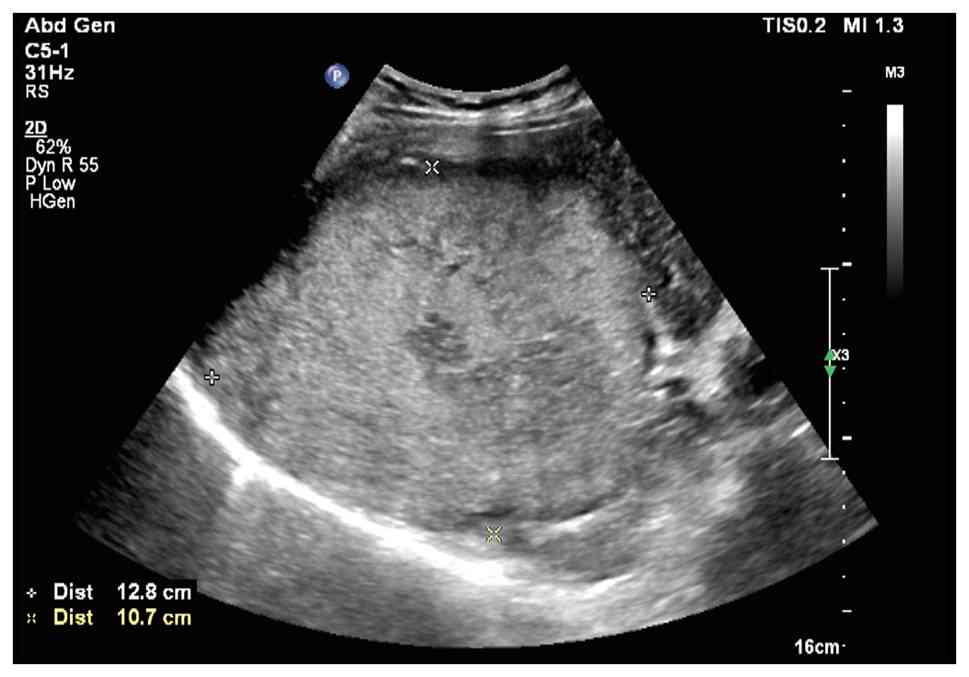
Ultrasound of the liver, gallbladder, pancreas,
spleen and kidneys revealed a large solid mass in the liver
(Fig. 1), a hypoechoic lesion
between the upper pole of the right kidney and the posterior
segment of the right lobe of the liver and a hypoechoic nodule in
the first hepatic portal area. The liver ultrasound findings were
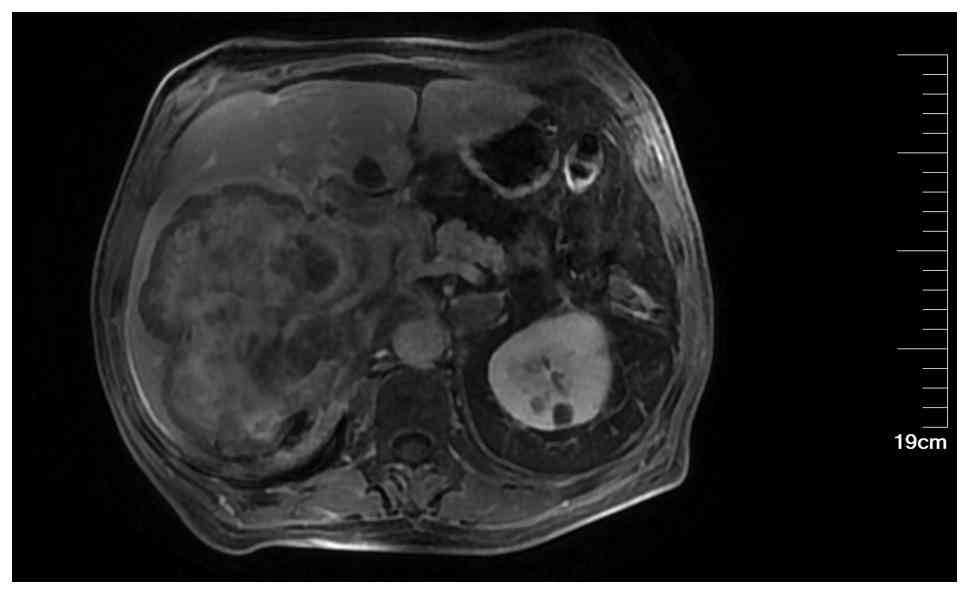
consistent with chronic liver disease. An enhanced MRI of the liver
suggested a high likelihood of hepatocellular carcinoma (HCC) in
the right lobe (Fig. 2), with
multiple metastatic tumors in the liver, bilateral adrenal glands
and pancreas. A chest CT scan with three-dimensional reconstruction
indicated a mass in the left hilum and left upper lobe of the lung,
raising concerns for a malignant lesion with obstructive
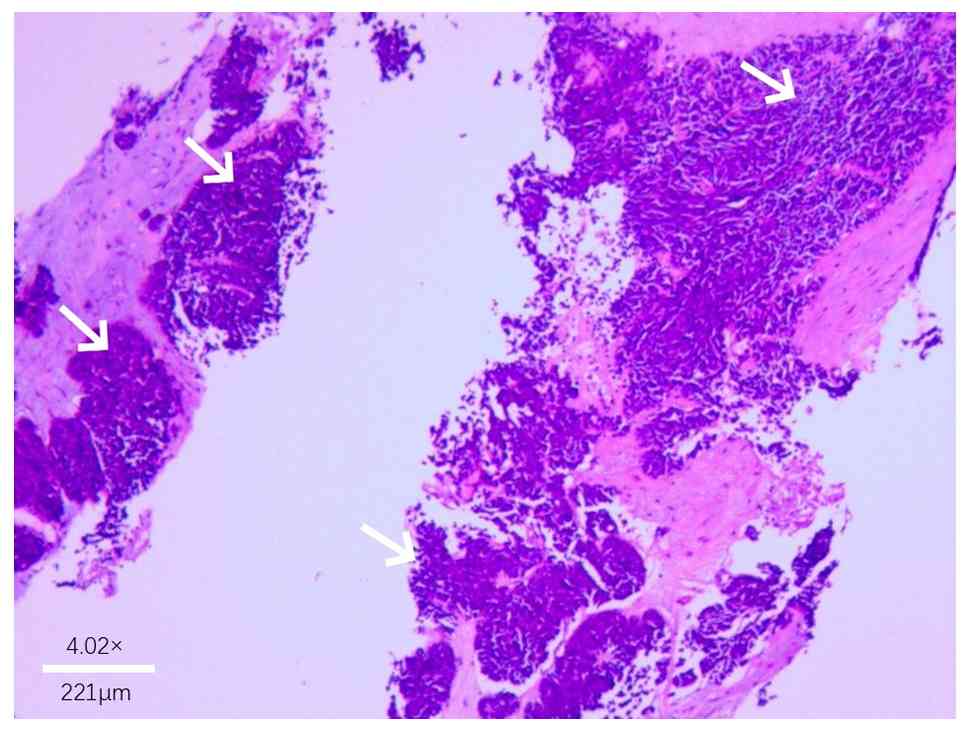
inflammation. The patient underwent ultrasound-guided biopsy of the
liver mass and lymph nodes in the left supraclavicular region.
Pathological examination (Fig. 3),
supported by immunohistochemical staining performed according to
the standard diagnostic protocols of the Department of Pathology at
Hebei General Hospital, confirmed the diagnosis of SCNEC.
Immunohistochemical staining (the full results are based on
pathology reports rather than retrievable images, as the pathology
reports cannot be published) included pan-cytokeratin (CKpan) (+),
vimentin (−), chromogranin A (CgA) (+), synaptophysin (Syn) (+),
cluster of differentiation 56 (CD56) (+), thyroid transcription
factor-1 (TTF-1) (+), arginase-1 (−), hepatocyte paraffin 1
(HepPar-1) (−) and P53 (+++), and Ki-67 showing an active region of
~70% positive.
Immunohistochemical staining was performed on
formalin-fixed, paraffin-embedded tissue sections using the
EnVision FLEX+ detection system (cat. no. K8002; Dako; Agilent
Technologies, Inc.) according to the manufacturer's instructions.
The following primary antibodies were used: Pan-cytokeratin (CKpan;
cat. no. ZM-0069), vimentin (cat. no. ZM-0260), CgA (cat. no.
ZA-0507), Syn (cat. no. ZA-0569), cluster of differentiation 56
(CD56; cat. no. ZM-0427), TTF-1 (cat. no. ZM-0270), arginase-1
(cat. no. ZA-0641), HepPar-1 (cat. no. ZM-0133), P53 (cat. no.
ZM-0408), Ki-67 (cat. no. ZM-0166), CD34 (cat. no. ZM-0046), CK19
(cat. no. ZM-0074), alpha-fetoprotein (AFP; cat. no. ZM-0008), CK7
(cat. no. ZM-0071), CK20 (cat. no. ZM-0072), Villin (cat. no.
ZM-0441), caudal type homeobox 2 (CDX2; cat. no. ZA-0520), MutL
homolog 1 (MLH1; cat. no. ZA-0544), MutS homolog 2 (MSH2; cat. no.
ZA-0542), MSH6 (cat. no. ZA-0546), postmeiotic segregation
increased 2 (PMS2; cat. no. ZA-0548), glutamine synthetase (cat.
no. ZA-0645), glypican-3 (cat. no. ZM-0446), heat shock protein 70
(HSP70; cat. no. ZA-0580; all ready-to-use; from OriGene
Technologies, Inc.), and programmed cell death ligand 1 (PD-L1;
cat. no. M3653; dilution 1:50; Dako; Agilent Technologies,
Inc.).
For all ready-to-use antibodies, staining was
performed following the manufacturer's instructions without
additional dilution. For PD-L1 (22C3), the antibody was diluted in
antibody diluent (Dako; Agilent Technologies, Inc.) and incubated
according to the manufacturer's recommended protocol. Secondary
antibody detection was performed using the EnVision FLEX+ detection
system (according to the manufacturer's instructions, which
includes horseradish peroxidase-conjugated secondary antibodies.
Diaminobenzidine was used as the chromogen and hematoxylin was used
for counterstaining.
After a multidisciplinary discussion, the decision
was made to proceed with TACE combined with targeted immunotherapy.
However, following TACE, the patient and his family declined any
further treatment. A follow-up phone call three months later
revealed that the patient had passed away.
Case 2
The patient is a 58-year-old male who was admitted
to Hebei General Hospital (Shijiazhuang, China) in June 2022 due to
discomfort and bloating in the upper abdomen for over 1 month,
along with a liver mass identified 1 week prior to admission at a
local hospital. In May 2022, the patient began experiencing
intermittent discomfort and bloating in the right upper abdomen
without any obvious triggers, which from then onwards affected the
patient's sleep and was accompanied by decreased appetite, fatigue
and occasional pain in the right shoulder and back. The patient
reported nausea but no vomiting.
On June 14, 2022, the patient visited a local
hospital where tumor markers were tested: AFP, 172.9 ng/ml (normal
<7.0 ng/ml); CEA, 9.16 ng/ml (normal <5.0 ng/ml) and CA199,
53.08 U/ml (normal <37 U/ml). Biochemical tests showed ALT at
75.0 U/l (normal range 7–40 U/l) and hepatitis B virus DNA
quantification at 5.35×105 IU/ml (indicating a high
viral load). An enhanced CT scan of the upper abdomen revealed a
low-density lesion in the right lobe of the liver measuring
7.98×6.65 cm, with possible liver cancer accompanied by
intrahepatic, hilar and gastric lesser curvature metastases, along
with potential peritoneal and retroperitoneal spread. The
pancreatic head and body showed heterogeneous density, suggesting
metastasis, and there were multiple small low-density lesions in
the liver, possibly cysts, along with a small amount of pleural
effusion on the right side and slight splenomegaly (data not
shown). The patient had a history of hepatitis B for >10 years
but had not been on regular entecavir treatment. Upon admission,
physical examination revealed tenderness in the right upper abdomen
and pain on percussion in the liver area. Laboratory tests showed
coagulation function with prothrombin time at 14.5 sec (slightly
prolonged; normal: 11.0–13.5 sec); fibrinogen level at 4.42 g/l
(elevated; normal: 2.0–4.0 g/l); and biochemical tests indicated
ALT at 55.5 U/l (elevated), AST at 81.3 U/l (elevated; normal
<40 U/l), gamma-glutamyl transferase at 154.0 U/l (elevated;
normal: 8–61 U/l), alkaline phosphatase at 107.4 U/l (normal range:
40–129 U/l), cholinesterase at 2,710 U/l (decreased; normal:
5,000-12,000 U/l) and hepatitis B surface antigen at 250.00 IU/ml
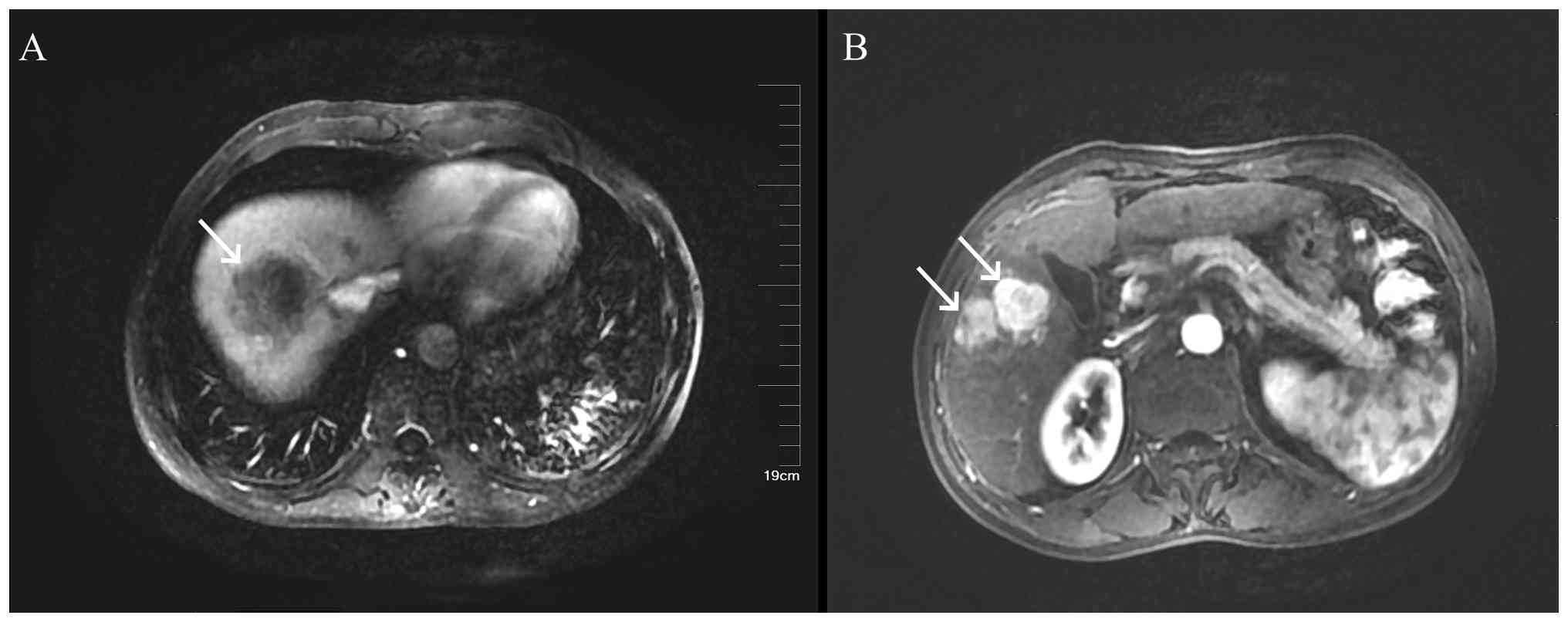
(positive). An MRI of the liver and spleen, both plain and
enhanced, showed a malignant lesion in segment (S)7-8 of the liver
(49×46×36 mm) and a high likelihood of multiple intrahepatic
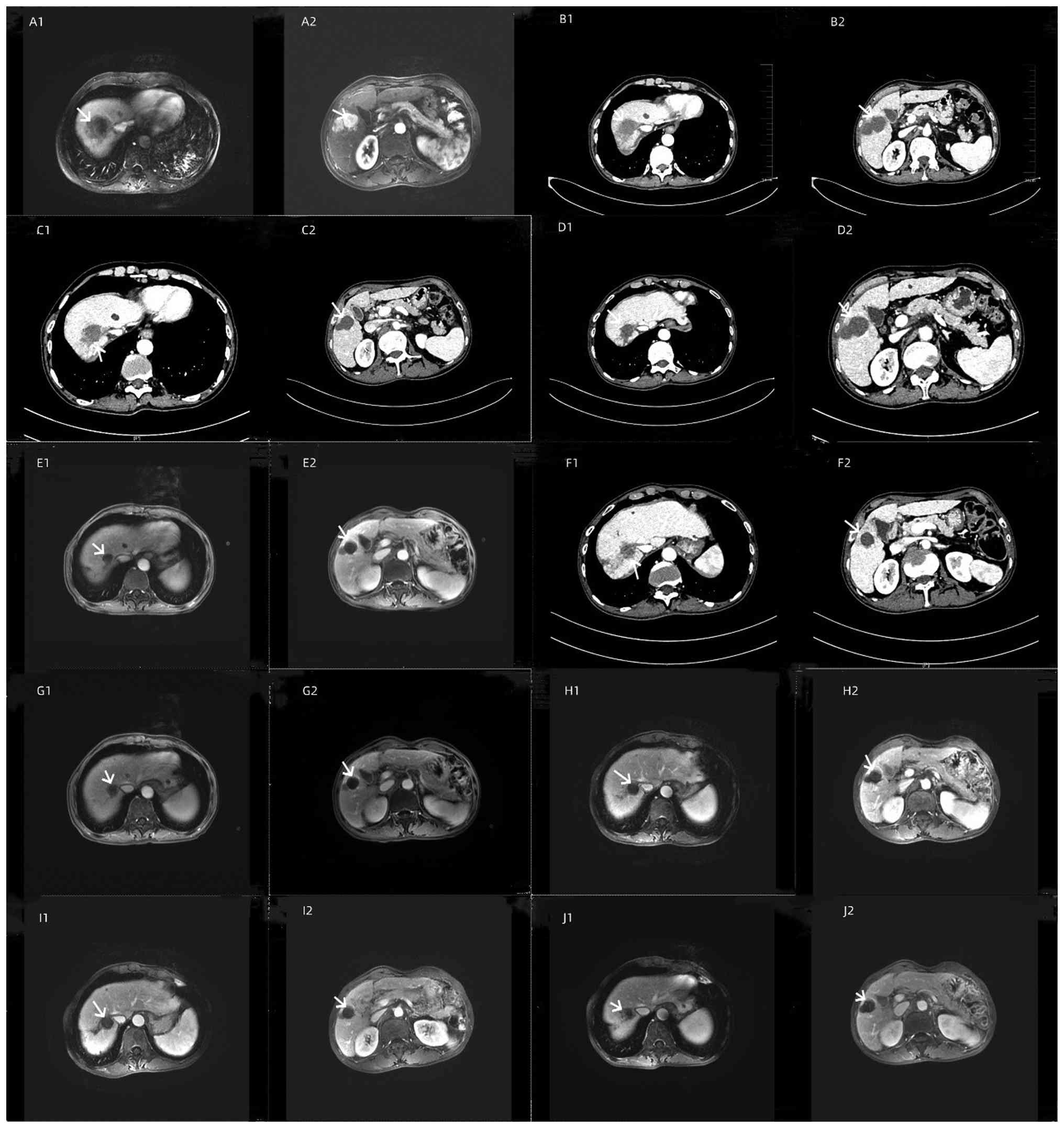
metastatic tumors (S5: 27 mm) (Fig.
4). An ultrasound of the liver, gallbladder, pancreas and
spleen indicated cirrhosis, multiple solid lesions in the liver,
multiple abnormal lymph nodes at the hepatic hilum, stage 3 liver
fibrosis and ascites. Endoscopy performed in late June 2022
revealed chronic non-atrophic gastritis (data not shown).
In late June 2022, a biopsy of the liver lesion in
segment S7-8 was performed, and pathology (Fig. 5) indicated a malignant tumor
consistent with poorly differentiated NEC, specifically SCNEC,
supported by immunohistochemical staining. Immunohistochemical
staining (the full results are based on pathology reports rather
than retrievable images, as the pathology reports cannot be
published) indicated the following: CKpan (weakly +), Syn (+), CgA
(+), CD56 (+), CD34 (−), CK19 (−), Arginase-1 (−), HepPar-1 (−),
AFP (−), Vimentin (weakly + in some cases), CK7 (−), CK20 (−),
Villin (−), TTF-1 (−), CDX2 (−), Ki-67 (~70%+ in active region),
MLH1 (+), MSH2 (+), MSH6 (+), PMS2 (+) and PD-L1 (22C3) (CPS 1)
(+). In July 2022, a biopsy of the liver mass in segment S5 was
performed, and pathology (Fig. 6)
was consistent with HCC. Immunohistochemical staining showed
glutamine synthetase (+), glypican-3 (focally +), HSP70 (focally
+), CD34 (showing diffuse capillary distribution), CK19 (−),
arginase-1 (+), HepPar-1 (+) and AFP (−), and Ki-67 (~15%+ in the
active area).
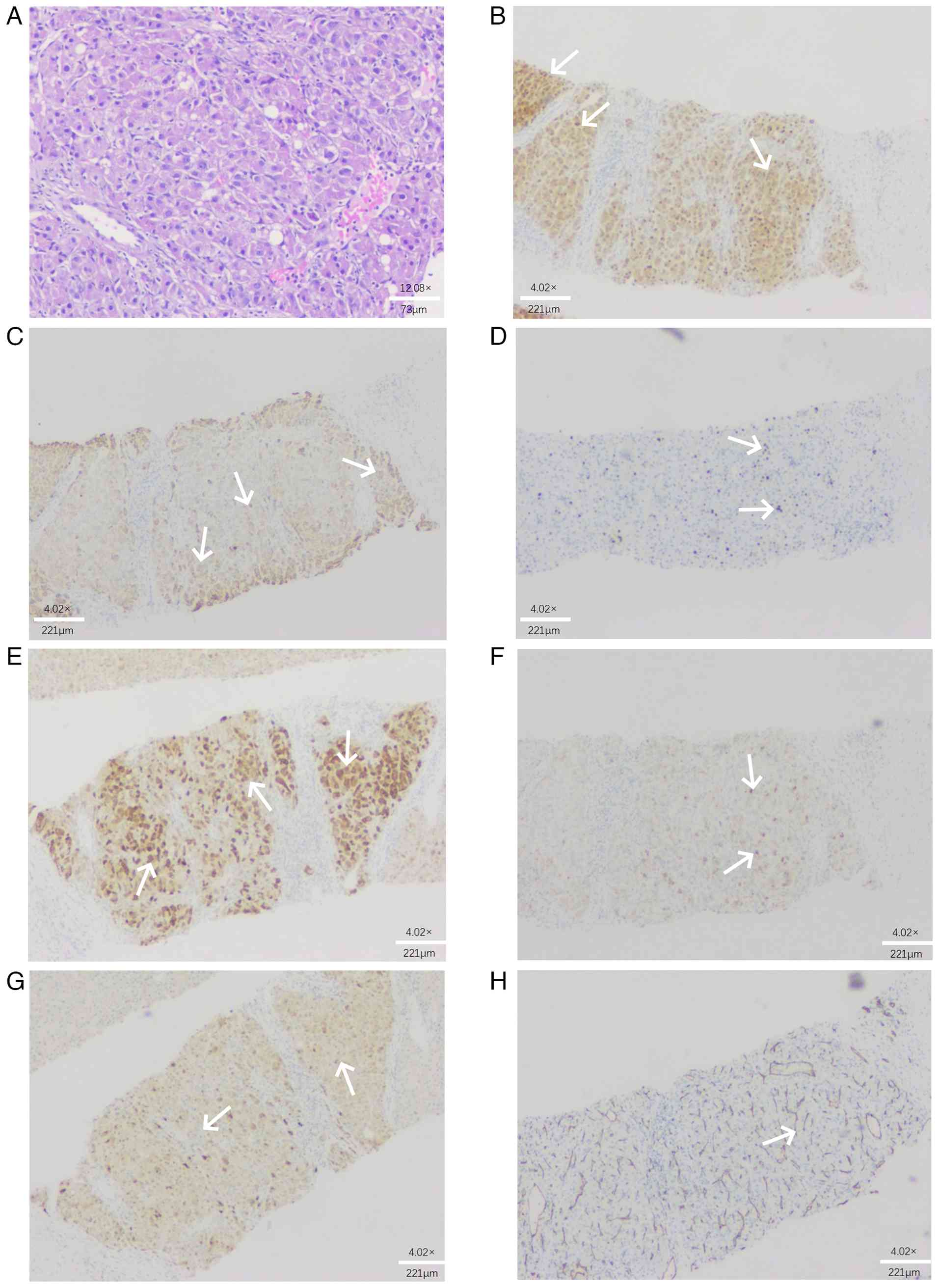
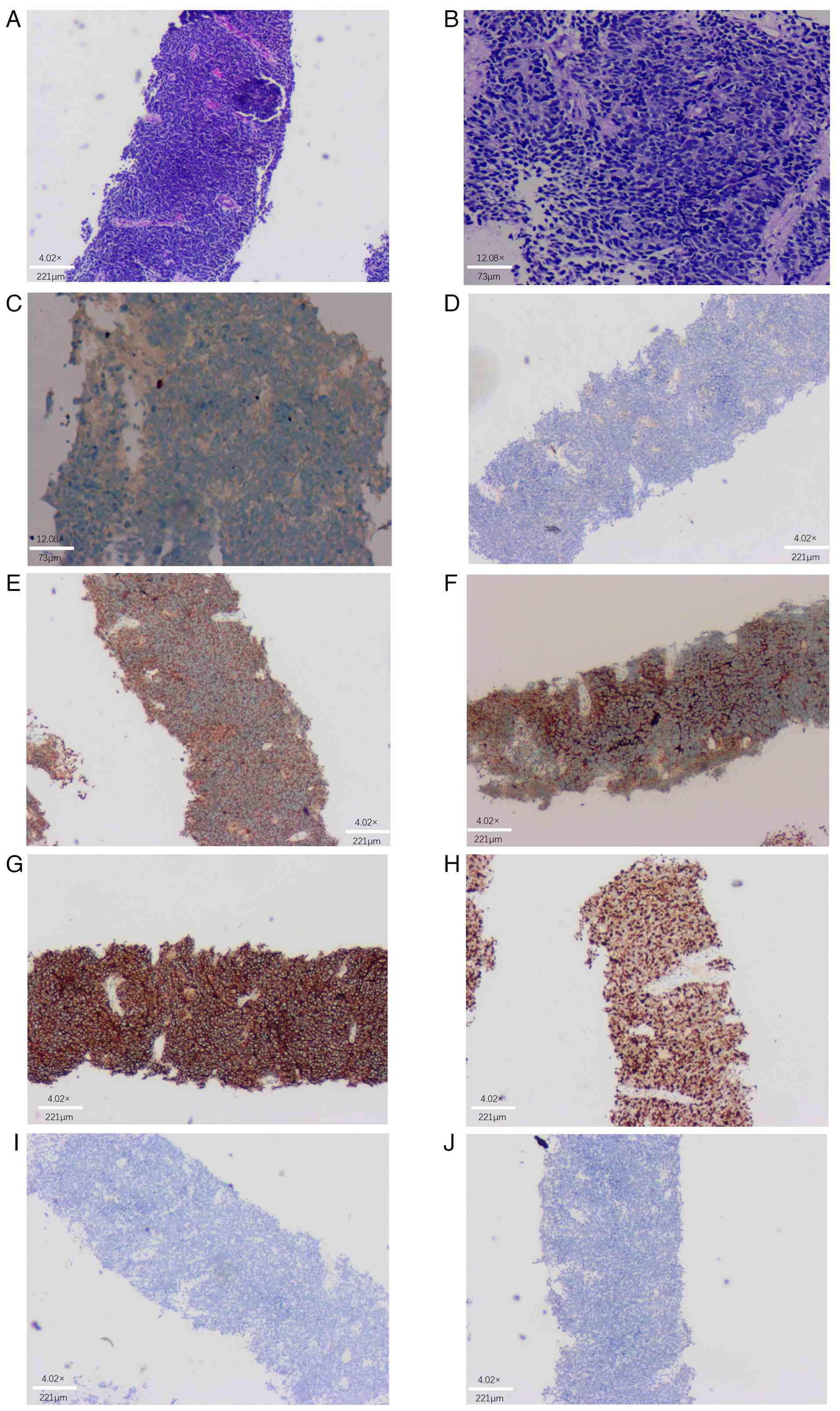 | Figure 5.Case 2: Pathology of segment 8
hepatocellular neuroendocrine carcinoma: Low magnification reveals
tumor cells arranged in a sheet-like pattern, while high
magnification shows tumor cells that are round, oval or short
spindle-shaped, with small, densely stained nuclei and a high
nuclear-to-cytoplasmic ratio. (A) H&E; magnification, ×40;
scale bar, 221 µm. (B) H&E; magnification, ×100; scale bar, 73
µm. Immunohistochemical results: (C) CKpan (weakly +);
magnification, ×100; scale bar, 73 µm; (D) CK7 (−); (E)
synaptophysin (+); (F) chromogranin A (+); (G) CD56 (+); (H) Ki-67
(~70%+ in active area); (I) CD34 (−); and (J) thyroid transcription
factor-1 (−) (magnification, ×40; scale bar, 221 µm). CK,
cytokeratin. |
 | Figure 6.Case 2: Pathology of S5 hepatocellular
carcinoma: High magnification reveals tumor cells that are
polygonal in shape, with round nuclei, prominent nucleoli and
cytoplasm exhibiting a finely granular appearance. (A) H&E
(magnification, ×100; scale bar, 73 µm). Immunohistochemical
results: (B) Arginase-1 (+), with arrows indicating cytoplasmic
positivity in tumor cells; (C) hepatocyte paraffin 1 (+), with
arrows indicating cytoplasmic granular positivity; (D) Ki-67 (~15%+
in active area), with arrows indicating nuclear positivity in
proliferating tumor cells; (E) glutamine synthetase (+), with
arrows indicating cytoplasmic positivity in a map-like distribution
pattern; (F) glypican-3 (focally +), with arrows indicating focal
cytoplasmic and membranous positivity; (G) heat shock protein 70
(focally +), with arrows indicating focal nuclear and cytoplasmic
positivity; and (H) CD34 (showing diffuse capillary distribution),
with arrows highlighting the characteristic sinusoidal endothelial
staining pattern (magnification, ×40; scale bar, 221 µm). |
After a multidisciplinary discussion, the patient
received liver protection, antiviral therapy and nutritional
support. Given the advanced stage of liver cancer, chemotherapy
with etoposide (1.7 g daily on days 1–3) plus cisplatin (60 mg
daily on days 1–2) was initiated in late June 2022, repeated every
21 days. Targeted therapy with sorafenib (0.4 g twice daily) began
in late July 2022. In mid-August 2022, TACE was performed in
conjunction with systemic targeted therapy using sorafenib (0.4 g
twice daily). The first combined immunotherapy with camrelizumab
(200 mg per dose, once every 3 weeks) was administered in late
October 2022. This was later switched to tislelizumab (200 mg per
dose, once every 3 weeks) in February 2023 due to the patient
developing a grade 2 immune-related rash attributed to
camrelizumab.
To date, the patient has undergone seven sessions of
TACE and eight sessions of combined targeted immunotherapy, and the
patient's condition is stable (Table
I). Following the initiation of combined therapy, the tumor
size gradually decreased and stabilized on serial imaging
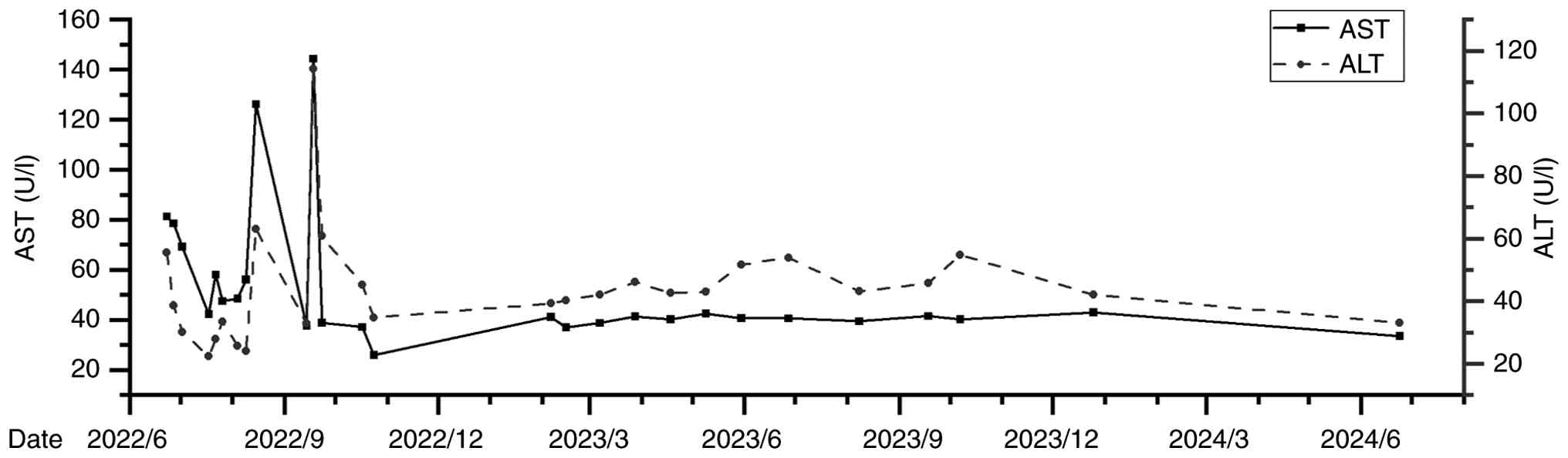
assessments performed between June 2022 and August 2024 (Fig. 7); liver function has remained stable
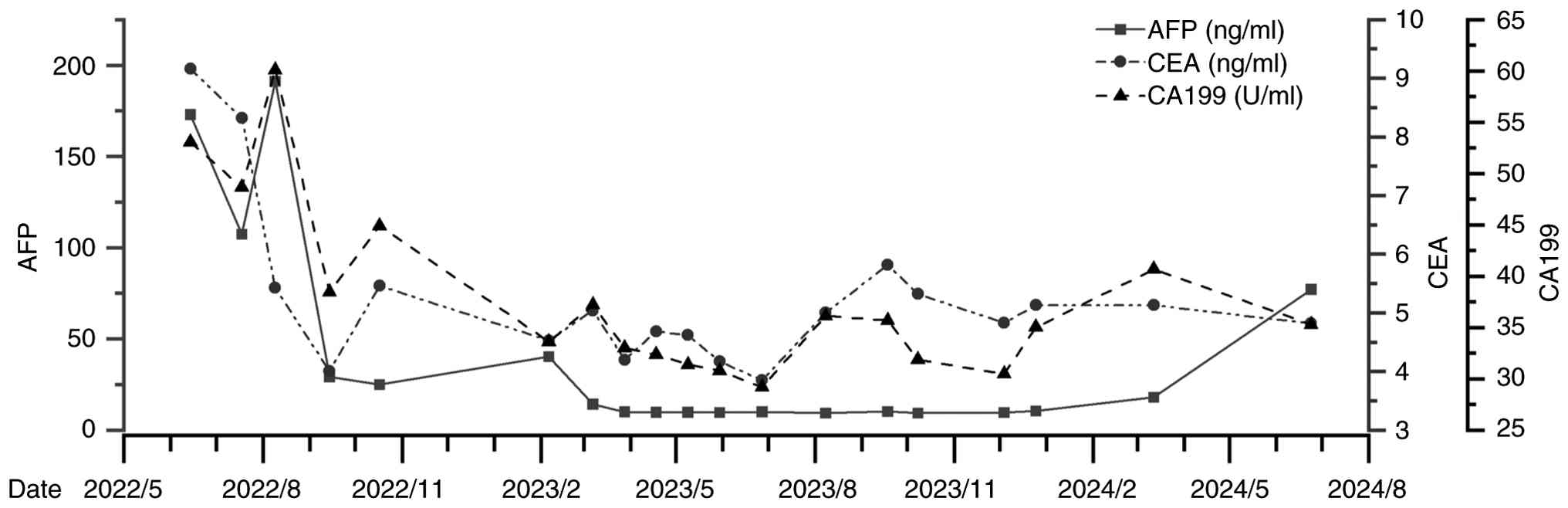
(Fig. 8), and tumor marker levels
have gradually decreased and stabilized (Fig. 9). As of August 2024, no significant
adverse reactions have been observed. Quality of life has
significantly improved and the patient is still undergoing regular
follow-up.
 | Table I.Treatment course for Case 2. |
Table I.
Treatment course for Case 2.
| Time-point | Event |
|---|
| June 2022 (first
hospitalization) | The pathological
diagnosis was small cell neuroendocrine carcinoma of the
liver. |
|
| Chemotherapy was
initiated in June 2022, with a regimen of etoposide (1.7 g daily on
days 1–3) plus cisplatin (60 mg daily on days 1–2), repeated every
21 days. |
| July 2022 (second
hospitalization) | A biopsy of the S5
liver mass in July 2022 yielded a pathology diagnosis (liver mass)
consistent with hepatocellular carcinoma based on staining.
immunohistochemical Treatment with sorafenib (0.4 g per dose, twice
daily) was initiated in July 2022. |
| August 2022 (third
hospitalization) | The first TACE
session was conducted in August 2022, alongside sorafenib therapy
(0.4 g twice daily). |
| September 2022
(fourth hospitalization) | The second TACE
session was conducted in September 2022, alongside sorafenib
therapy (0.4 g twice daily). |
| October 2022 (fifth
hospitalization) | The third cycle of
TACE was administered in October 2022, alongside continued
sorafenib (0.4 g twice daily). This was followed by the first dose
of camrelizumab (200 mg) in October 2022, marking the commencement
of combination immunotherapy. |
| February 2023 (sixth
hospitalization) | Following the fourth
TACE procedure in February 2023, a combined regimen of sorafenib
(0.4 g twice daily) and tislelizumab (200 mg) for immunotherapy was
initiated within the same hospitalization period, ~2-3 days after
the TACE procedure. |
| March-June 2023
(seventh to 12th hospitalization) | A combined regimen of
sorafenib (0.4 g twice daily) and tislelizumab (200 mg) was used
for immunotherapy. |
| August 2023 (13th
hospitalization) | Treatment consisted
of sorafenib (0.4 g twice daily). |
|
| Targeted therapy with
sorafenib (0.4 g twice daily) was maintained in September
2023. |
| October 2023 (14th
hospitalization) | TACE was carried out
in October 2023, concurrent with sorafenib therapy (0.4 g twice
daily). |
| December 2023 (15th
hospitalization) | A TACE session was
performed in December 2023, alongside ongoing sorafenib therapy
(0.4 g twice daily). |
| July 2024 (16th
hospitalization) | A TACE procedure was
performed in July 2024. |
| Ongoing (until August
2024) | Regular
follow-up. |
Discussion
HSCNEC is a rare and clinically challenging
malignancy. The first case reported by the present study involved a
76-year-old male patient who was admitted due to intermittent right
upper abdominal pain for three months. The patient had a 50-year
history of hepatitis B and multiple other chronic health issues,
leading to a complex clinical presentation. Intermittent right
upper abdominal pain was the initial symptom, and examinations
revealed a liver mass and a lesion in the left lung. Based on
history, clinical manifestations, examination results and pathology
findings, the patient was ultimately diagnosed with HSCNEC.
Considering the patient's age, medical history and the extent of
the disease, the treatment strategy focused on alleviating symptoms
and improving quality of life. However, after undergoing TACE
treatment, the patient and the patient's family declined further
targeted immunotherapy, and the patient passed away three months
later.
The second patient had a history of hepatitis B for
>10 years, with elevated AFP levels. A biopsy of the liver mass
was performed under ultrasound guidance, revealing SCNEC in segment
S8 and HCC in segment S5. Combined with specific pathological
immunohistochemical findings, the diagnosis was established as
HSCNEC accompanied by HCC. The patient received a comprehensive
treatment regimen of TACE combined with sorafenib and tislelizumab,
a programmed cell death 1 (PD-1) immune checkpoint inhibitor. Since
admission, the patient's tumor size had gradually decreased and
stabilized, and tumor marker levels showed a downward trend, with
no significant adverse reactions observed during treatment. The
patient is currently under regular follow-up.
Both patients underwent ultrasound-guided biopsy of
the liver masses and the pathological examination confirmed the
presence of SCNEC in the liver. The immunohistochemical profiles
(e.g., Synaptophysin+, Chromogranin A+, CD56+) supported
neuroendocrine differentiation.
In Case 1, the immunohistochemical profile included
chromogranin A (+), synaptophysin (+) and CD56 (+), all of which
are established and highly specific markers for neuroendocrine
differentiation. The positivity for these markers, along with the
characteristic small cell morphology and high Ki-67 index (~70%),
strongly supports the diagnosis of SCNEC. While analyses for
pro-gastrin-releasing peptide, neuron-specific enolase and
insulinoma-associated protein 1 were not routinely performed in
this case, their absence does not undermine the diagnostic
certainty, as the combination of chromogranin A, synaptophysin and
CD56 is widely regarded as sufficient for diagnosing SCNEC in
clinical and pathological practice (2). Furthermore, TTF-1 positivity (as
reported) is also frequently associated with a small cell
morphology and further supports the diagnosis (6).
In Case 2, the patient had a concurrent HCC
component in segment S5, which was confirmed by biopsy and
immunohistochemistry (arginase-1+, HepPar-1+). The small cell
neuroendocrine component (in segment S8) was AFP-negative on
immunohistochemistry, indicating that the elevated serum AFP was
attributable to the HCC component rather than the NEC. This dual
pathology-HSCNEC coexisting with HCC-is rare but documented in the
literature (7) and underscores the
importance of comprehensive sampling and immunohistochemical
profiling. The diagnosis of HSCNEC in this case was based on the
immunohistochemistry results of the S8 lesion, which showed strong
positivity for synaptophysin, chromogranin A and CD56, and a high
Ki-67 index (~70%), consistent with high-grade NEC. The imaging
changes in the pancreatic region were considered nonspecific and
possibly related to metastasis rather than a primary pancreatic
tumor. The patient also had a concurrent HCC in segment S5, further
supporting the liver as the primary site of pathology.
In both cases, the treatment strategy was tailored
to the dominant hepatic disease. The management of hepatitis B
virus (HBV) was a cornerstone of the present therapeutic strategy,
particularly for the second patient who received combined therapy.
As documented in the case report, this patient had a high viral
load at admission (5.35×105 IU/ml). Potent antiviral
therapy was initiated and maintained throughout the patient's
treatment course. This prophylactic measure was crucial to prevent
HBV reactivation-a known risk associated with immune checkpoint
inhibitors (8)- and to safeguard
liver function during repeated TACE sessions. The successful
prevention of reactivation and the maintenance of stable liver
function were fundamental enablers, allowing the patient to safely
complete multiple cycles of TACE combined with sorafenib and
camrelizumab.
While the direct role of HBV in the oncogenesis of
HSCNEC itself is not well-defined, its presence significantly
shaped the management plan in the present study. The contrasting
outcomes of the two cases powerfully highlight the critical
importance of the comprehensive treatment regimen. The first
patient, who received only TACE and declined further targeted
immunotherapy, succumbed to the disease rapidly. In stark contrast,
the second patient, under the protective cover of antiviral
therapy, successfully received the full combination of TACE,
targeted therapy and immunotherapy. It is this specific and safely
administered combination that was instrumental in achieving tumor
control, reduction in tumor markers and the remarkable improvement
in the patient's quality of life and overall survival.
HSCNEC is a rare intrahepatic neuroendocrine tumor.
Surgery is the primary potential treatment option, aimed at
directly removing tumor tissue and reducing the tumor burden.
However, patients must meet specific surgical criteria to be
eligible for this intervention. For localized NEC classified as
stage I to III according to the clinical staging of liver cancer in
China, the five-year overall survival rate after surgery is only 25
to 40% (9). However, not all
patients are suitable for surgical resection, particularly those
with unfavorable tumor locations, multiple tumors or distant
metastases. Research has shown that the intrinsic histopathological
features of the tumor (its composition, including differentiation
grade, histological subtype and the presence of mixed components),
lymph node involvement, distant metastasis and clinical staging are
significant factors influencing patient prognosis (7). The pathogenesis of HSCNEC differs from
that of traditional liver cancer and is often accompanied by
multiple metastases, leading to varied responses to existing
treatment modalities. Consequently, TACE alone often has limited
efficacy, necessitating treatment strategies that are tailored to
the patient's individual condition, tumor biology and overall
health status. Combining targeted therapies with immunotherapy can
provide a more precise treatment approach, enhancing the
effectiveness of tumor management. Clinical applications have
demonstrated certain efficacy and advantages in this context.
TACE is an interventional treatment technique that
is widely used in the management of liver tumors (10,11).
TACE involves the direct injection of chemotherapy drugs into the
hepatic artery supplying the tumor, utilizing local chemotherapy
and embolization to obstruct the tumor's blood supply, thereby
controlling tumor growth. The advantages of TACE include its
minimally invasive nature, good operability and relatively low
risk, which can contribute to extending patients' survival.
However, TACE is not without its limitations. Post-treatment, there
often remains a histological level of tumor tissue that is not
completely necrotic, increasing the risk of tumor recurrence.
Additionally, repeated TACE treatments can significantly impair
liver function, particularly in cases of large HCC or massive liver
tumors. The tumor microenvironment may also change following TACE,
potentially promoting immune evasion, where tumor cells can utilize
various mechanisms to reduce the immune system's ability to
recognize and attack them. TACE often struggles to ensure complete
necrosis of tumor tissue (10), and
for certain patients, tumor recurrence can occur after treatment
(12). To enhance the efficacy of
TACE and reduce the risk of distant metastasis, early combination
with targeted molecular therapies should be considered (12,13).
Currently, the combination of TACE with targeted molecular
therapies has shown superior efficacy compared to the use of
targeted therapies alone (14,15).
In recent years, there have been increasing explorations of
combining targeted therapies with immunotherapy.
Targeted therapy primarily focuses on specific
molecular markers unique to tumor cells, inhibiting their
proliferation and metastasis by blocking particular signaling
pathways or molecular targets. This approach effectively attacks
tumor cells while minimizing damage to normal cells (16). By contrast, immunotherapy works by
activating or enhancing the patient's own immune system to
recognize and eliminate tumor cells (17).
The application of TACE in combination with targeted
and immunotherapy can attack tumor cells on multiple levels: TACE
directly destroys tumor cells, while targeted therapies address the
specific molecular alterations in these cells, obstructing pathways
that promote tumor growth and spread. Furthermore, in certain
cases, the combination of targeted therapy and immunotherapy can
produce synergistic effects, enhancing the body's ability to
eliminate tumors. Given their distinct mechanisms, the combination
of TACE with targeted and immunotherapy can extend the survival of
patients with advanced liver cancer, demonstrating superior
efficacy compared to TACE alone (5,18,19).
This synergistic approach can lead to improved overall treatment
outcomes. When TACE is combined with targeted immunotherapy, the
advantages of both approaches are integrated, allowing for
complementary benefits. This combination enables local control of
the tumor, as well as a systemic immune response. The use of TACE
in conjunction with PD-1/PD-L1 inhibitors and targeted therapies
has shown significant advantages in progression-free survival,
overall survival and objective response rates in patients with
advanced liver cancer (5). In
clinical practice, the combination of TACE with targeted
immunotherapy offers patients a more personalized treatment
approach. By analyzing the molecular and biological characteristics
of the tumor, suitable targeted therapies can be selected,
alongside immune checkpoint inhibitors and other immunotherapeutic
agents, to enhance the comprehensiveness and depth of treatment.
This integrated treatment model helps to overcome the limitations
of single-modality therapies and improves therapeutic efficacy
(20).
The advantages of combining TACE with targeted
immunotherapy are also evident in treatment outcomes. This
comprehensive approach can significantly enhance treatment
effectiveness, prolonging both progression-free survival and
overall survival for patients. Additionally, combination therapy
can improve patients' quality of life, reduce adverse reactions
during treatment, lower recurrence rates and ultimately improve
patient prognosis (21). However,
the combination of TACE with targeted immunotherapy also faces
challenges. This approach may lead to more severe adverse effects
(22–24), which can vary from person to person.
In cases where adverse effects occur, treatment can be paused for
observation and symptomatic supportive care can be provided.
Furthermore, selecting the appropriate targeted immunotherapy
agents, determining the optimal treatment combinations, monitoring
treatment responses and managing potential adverse reactions all
require ongoing optimization and standardization through clinical
trials and practice. Finally, due to the heterogeneity of
hepatocellular NEC, its response to the combination of TACE and
targeted immunotherapy may differ from that of traditional HCC,
necessitating further research to explore these differences.
In conclusion, HSCNEC is a rare intrahepatic
neuroendocrine tumor and its etiology remains unclear. Preoperative
imaging diagnosis primarily relies on enhanced CT and MRI, while
definitive diagnosis requires biopsy of the tumor for pathological
assessment (11). Radical surgical
resection is the preferred treatment option (9), and for patients who are not candidates
for surgery, TACE combined with targeted immunotherapy can be
considered (5). This multimodal
approach can significantly enhance treatment efficacy, prolong
overall survival, improve quality of life, reduce treatment-related
adverse events, lower recurrence rates and ultimately improve
prognosis (5,21). Additionally, regular follow-up is
essential after comprehensive treatment (11).
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
Conceptualization was conducted by RF and XX. Formal
analysis and data interpretation were performed by RF, XX, HW, YZ,
XZ and HT. Data acquisition and clinical management were carried
out by HT, HW and YZ. Literature analysis was conducted by XX, HW
and YZ. Writing of the original draft was conducted by XX, RF and
HW. Reviewing and editing of the manuscript was performed by XX,
RF, HW, YZ, XZ and HT. Supervision was provided by RF, XZ, YZ and
HT. Project administration was conducted by HW, YZ and HT. All
authors read and approved the final version of the manuscript. RF,
XX and HW confirm the authenticity of all the raw data.
Ethics approval and consent to
participate
All the procedures were in accordance with the
ethical standards of the responsible committee on human
experimentation (institutional and national) and with the Helsinki
Declaration of 1975, as revised in 2008, and the study received
approval from the Ethics Committee of Hebei General Hospital
(approval no. 2024-LW-048). For this retrospective case analysis,
all patient data were anonymized prior to review and inclusion in
the study.
Patient consent for publication
Written informed consent for the publication of
anonymized clinical data and accompanying images was obtained from
Patient 2 and from the legal guardian of the deceased Patient
1.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Xu X, Lian Y, Li T and Liang H:
Hepatomegaly as the main manifestation in one case of primary
hepatic neuroendocrine carcinoma. J Chin Pract Diagn Ther.
37:851–853. 2023.(In Chinese).
|
|
2
|
Mao XX and Chen J: Interpretation on the
update of 2022 WHO classification of neuroendocrine tumors.
Zhonghua Bing Li Xue Za Zhi. 53:655–659. 2024.(In Chinese).
PubMed/NCBI
|
|
3
|
Dasari A, Shen C, Devabhaktuni A, Nighot R
and Sorbye H: Survival according to primary tumor location, stage,
and treatment patterns in locoregional gastroenteropancreatic
high-grade neuroendocrine carcinomas. Oncologist. 27:299–306. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yueze L, Chen D, Zeyu Z, Yi D and Taiping
Z: Interpretation of the European neuroendocrine tumor society
(ENETS) 2023 guidance paper for digestive neuroendocrine carcinoma.
Chin J Dig Surg. 22:953–957. 2023.(In Chinese).
|
|
5
|
Zhu HD, Li HL, Huang MS, Yang WZ, Yin GW,
Zhong BY, Sun JH, Jin ZC, Chen JJ, Ge NJ, et al: Transarterial
chemoembolization with PD-(L)1 inhibitors plus molecular targeted
therapies for hepatocellular carcinoma (CHANCE001). Signal
Transduct Target Ther. 8:582023. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Rindi G, Klimstra DS, Abedi-Ardekani B,
Asa SL, Bosman FT, Brambilla E, Busam KJ, de Krijger RR, Dietel M,
El-Naggar AK, et al: A common classification framework for
neuroendocrine neoplasms: An international agency for research on
cancer (IARC) and World Health Organization (WHO) expert consensus
proposal. Mod Pathol. 31:1770–1786. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Huang YC, Yang NN, Chen HC, Huang YL, Yan
WT, Yang RX, Li N, Zhang S, Yang PP and Feng ZZ:
Clinicopathological features and prognostic factors associated with
gastroenteropancreatic mixed neuroendocrine non-neuroendocrine
neoplasms in Chinese patients. World J Gastroenterol. 27:624–640.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Terrault NA, Lok ASF, McMahon BJ, Chang
KM, Hwang JP, Jonas MM, Brown RS Jr, Bzowej NH and Wong JB: Update
on prevention, diagnosis, and treatment of chronic hepatitis B:
AASLD 2018 hepatitis B guidance. Hepatology. 67:1560–1599. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sorbye H, Grande E, Pavel M, Tesselaar M,
Fazio N, Reed NS, Knigge U, Christ E, Ambrosini V, Couvelard A and
Tiensuu Janson E: European neuroendocrine tumor society (ENETS)
2023 guidance paper for digestive neuroendocrine carcinoma. J
Neuroendocrinol. 35:e132492023. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lencioni R, de Baere T, Soulen MC, Rilling
WS and Geschwind JFH: Lipiodol transarterial chemoembolization for
hepatocellular carcinoma: A systematic review of efficacy and
safety data. Hepatology. 64:106–116. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
National Health Commission of the People's
Republic of China and Department of Medical Administration, .
Guideline for diagnosis and treatment of primary liver cancer (2024
version). Chin J Hepatol. 32:581–630. 2024.
|
|
12
|
Wang Q, Xia D, Bai W, Wang E, Sun J, Huang
M, Mu W, Yin G, Li H, Zhao H, et al: Development of a prognostic
score for recommended TACE candidates with hepatocellular
carcinoma: A multicentre observational study. J Hepatol.
70:893–903. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Wang Z, Wang E, Bai W, Xia D, Ding R, Li
J, Wang Q, Liu L, Sun J, Mu W, et al: Exploratory analysis to
identify candidates benefitting from combination therapy of
transarterial chemoembolization and sorafenib for first-line
treatment of unresectable hepatocellular carcinoma: A multicenter
retrospective observational study. Liver Cancer. 9:308–325. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Peng Z, Fan W, Zhu B, Wang G, Sun J, Xiao
C, Huang F, Tang R, Cheng Y, Huang Z, et al: Lenvatinib combined
with transarterial chemoembolization as first-line treatment for
advanced hepatocellular carcinoma: A phase III, randomized clinical
trial (LAUNCH). J Clin Oncol. 41:117–127. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Xia D, Bai W, Wang E, Li J, Chen X, Wang
Z, Huang M, Huang M, Sun J, Yang W, et al: Lenvatinib with or
without concurrent drug-eluting beads transarterial
chemoembolization in patients with unresectable, advanced
hepatocellular carcinoma: A real-world, multicenter, retrospective
study. Liver Cancer. 11:368–382. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hanahan D and Weinberg RA: Hallmarks of
cancer: The next generation. Cell. 144:646–674. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Topalian SL, Drake CG and Pardoll DM:
Immune checkpoint blockade: A common denominator approach to cancer
therapy. Cancer Cell. 27:450–461. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Jin ZC, Zhong BY, Chen JJ, Zhu HD, Sun JH,
Yin GW, Ge NJ, Luo B, Ding WB, Li WH, et al: Real-world efficacy
and safety of TACE plus camrelizumab and apatinib in patients with
HCC (CHANCE2211): A propensity score matching study. Eur Radiol.
33:8669–8681. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Li S, Wu J, Wu J, Fu Y, Zeng Z, Li Y, Li
H, Liao W and Yan M: Prediction of early treatment response to the
combination therapy of TACE plus lenvatinib and anti-PD-1 antibody
immunotherapy for unresectable hepatocellular carcinoma:
Multicenter retrospective study. Front Immunol. 14:11097712023.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Finn RS, Qin S, Ikeda M, Galle PR, Ducreux
M, Kim TY, Kudo M, Breder V, Merle P, Kaseb AO, et al: Atezolizumab
plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J
Med. 382:1894–1905. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Zhang F, Dong Y, Chen F, Niu M, Liu Z and
Tan Y: Clinical Observation of Lenvatinib, PD-1 Inhibitor Combined
with Transcatheter Arterial Chemoembolization in the Treatment of
Unresectable Hepatocellular Carcinoma. China Pharmaceuticals.
33:102–105. 2024.(In Chinese).
|
|
22
|
Chinese Medical Doctor Association
Respiratory Physicians Branch and Chinese Medical Doctor
Association Multidisciplinary Oncology Diagnosis and Treatment
Committee, . Suggestions on prevention and management of immune
checkpoint inhibitor related toxicity. Natl Med J China. 1811–1832.
2022.(In Chinese).
|
|
23
|
Travis WD, Dacic S, Wistuba I, Sholl L,
Adusumilli P, Bubendorf L, Bunn P, Cascone T, Chaft J, Chen G, et
al: IASLC multidisciplinary recommendations for pathologic
assessment of lung cancer resection specimens after neoadjuvant
therapy. J Thorac Oncol. 15:709–740. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Li N, Feng S, Xue J, Wei XB, Shi J, Guo
WX, Lau WY, Wu MC, Cheng SQ and Meng Y: Hepatocellular carcinoma
with main portal vein tumor thrombus: A comparative study comparing
hepatectomy with or without neoadjuvant radiotherapy. HPB (Oxford).
18:549–556. 2016. View Article : Google Scholar : PubMed/NCBI
|