Introduction
Stage III non-small cell lung cancer (NSCLC), a
subgroup characterized by substantial heterogeneity, accounts for
20–25% of all NSCLC cases (1–4).
Patients are typically categorized as having resectable,
unresectable or partially resectable disease after neoadjuvant
treatment (5). A multidisciplinary
team (MDT) approach is recommended for treatment decision-making
(6). Neoadjuvant chemoimmunotherapy
has emerged as a promising strategy for patients with initially
unresectable, locally advanced NSCLC. Previous studies have
demonstrated that neoadjuvant chemoimmunotherapy improves the
pathological response rate in patients undergoing surgery for stage
III NSCLC (7–9). Furthermore, the CheckMate 816 and
NeoTORCH trials demonstrated that neoadjuvant chemoimmunotherapy
notably improved clinical outcomes in surgically treated patients
(10,11). However, 10–33% of patients did not
proceed to surgical intervention after neoadjuvant therapy
(7–9). For patients who do not undergo surgery
following neoadjuvant chemoimmunotherapy, the efficacy and safety
of consolidation immune checkpoint inhibitors (ICIs) after
concurrent chemoradiotherapy (cCRT) remain uncertain.
Immunotherapy and radiotherapy may exhibit
synergistic antitumor effects but can also increase toxicity
(12,13). The toxicities and adverse effects
associated with cCRT after chemoimmunotherapy remain a concern. The
PACIFIC regimen, which combines cCRT with durvalumab consolidation,
markedly improves prognosis and has become the standard treatment
strategy for patients with unresectable stage III NSCLC (14–16).
However, the PACIFIC-2 trial found that administering durvalumab
during cCRT did not confer significant survival benefits compared
with a placebo, and the CheckMate-73L trial reported that adding
nivolumab did not improve progression-free survival (PFS) (17,18).
These findings may be related to premature T-cell exhaustion and
cumulative toxicity (19,20). Nevertheless, the 5-year follow-up
results of the KEYNOTE-799 trial indicated that pembrolizumab
combined with cCRT provides durable antitumor activity in patients
with unresectable, locally advanced stage III NSCLC and maintains a
manageable safety profile (21). In
addition, real-world studies have also demonstrated similar
inconsistencies, suggesting that optimization strategies for
induction immunotherapy require further investigation (22,23).
Therefore, for patients who experience failure of neoadjuvant
chemoimmunotherapy, the efficacy and safety of radical cCRT
following combined immunochemotherapy remain controversial.
In the present study, a retrospective analysis was
conducted to evaluate the efficacy and safety of cCRT followed by
immunotherapy consolidation in patients with stage III NSCLC who
experienced failure of neoadjuvant chemoimmunotherapy.
Patients and methods
Patients and study design
The present retrospective study included patients
who received first-line immunotherapy at The Second Affiliated
Hospital of Nanchang University, Nanchang, China, between May 2018
and August 2024. The inclusion criteria were as follows: i) Age ≥18
years; ii) histologically confirmed stage III NSCLC; and iii)
receipt of cCRT. The exclusion criteria were as follows: i)
Presence of other active malignancy; ii) prior surgical resection
for lung cancer; iii) incomplete radiotherapy course; iv) loss to
follow-up during first-line immunotherapy; and v) receipt of
consolidation ICIs only. To contextualize the efficacy of the study
intervention, a retrospective comparator cohort of 30 patients was
identified. These patients had initially unresectable stage III
NSCLC and were treated strictly according to the standard PACIFIC
regimen at the same institution between March 2017 and December
2023. Key differences from the primary cohort were: i) Patients
received definitive cCRT without any prior induction immunotherapy;
and ii) consolidation immunotherapy utilized programmed
death-ligand 1 (PD-L1) inhibitors. The same inclusion/exclusion
criteria otherwise applied. According to the Response Evaluation
Criteria in Solid Tumors (RECIST) version 1.1 (24), neoadjuvant failure was defined as
disease progression after neoadjuvant treatment or, following MDT
discussion, the tumor failure to shrink sufficiently to allow
surgical resection. This study was approved by the Institutional
Review Board of the Second Affiliated Hospital of Nanchang
University.
Treatment strategy
All patients in this study received two to four
cycles of induction immunotherapy with PD-1 inhibitors in
combination with chemotherapy. All patients received the same
baseline dose of chemotherapy. For patients with non-squamous cell
carcinoma, pemetrexed combined with carboplatin is the common
treatment regimen. The dose of pemetrexed is 500 mg/m2,
and the carboplatin dosage is administered at an area under the
curve (AUC) of 5, once/3 weeks. For patients with squamous cell
carcinoma, the treatment regimen usually involves paclitaxel or
albumin-bound paclitaxel combined with carboplatin. The
administration regimen of paclitaxel was 175 mg/m2,
administered once every three weeks. Albumin-bound paclitaxel also
follows a 21-day cycle. During each cycle, three doses are
administered on the first day, the eighth day, and the fifteenth
day, with each dose being 100 mg/m2. The administration
scheme and dosage of carboplatin are the same as those for
non-squamous cell carcinoma patients. Patients who were unable to
undergo or declined surgery subsequently received cCRT.
Radiotherapy was administered using intensity-modulated radiation
therapy. Most patients received a total dose of 60 Gy in 30
fractions, whereas 3 patients underwent an escalated regimen of 70
Gy delivered as 40 Gy in 20 fractions plus 30 Gy in 10 fractions.
In the PACIFIC cohort, 2 patients used the same escalating dose
regimen, while the remaining patients received irradiation with a
total dose of 60 Gy. The concurrent chemotherapy regimen was as
follows: For non-squamous carcinoma, pemetrexed combined with a
platinum agent every 3 weeks; and for squamous carcinoma,
paclitaxel + platinum agent administered weekly. For patients with
non-epithelial carcinoma, the administration regimen was the same
as that of induction chemotherapy. Patients with squamous cell
carcinoma received weekly administration regimen of paclitaxel +
carboplatin. The paclitaxel dose was 50 mg/m2 and
carboplatin at an AUC of 2. All patients received consolidation
immunotherapy for up to 2 years or until the occurrence of
intolerable adverse events or disease progression.
Data collection
Baseline demographic and treatment data were
extracted from electronic medical records, including sex, age,
Eastern Cooperative Oncology Group (ECOG) performance status
(25), smoking history, cancer
stage, pathological subtype of NSCLC, PD-L1 expression level,
radiotherapy dose and volume, and the types and grades of
treatment-related toxicity. Tumor staging was performed according
to the eighth edition of the American Joint Committee on Cancer
(AJCC) TNM classification system (26). Adverse events were graded based on
the Common Terminology Criteria for Adverse Events version 5.0
(27), and treatment efficacy was
evaluated using RECIST version 1.1.
Statistical analysis
Kaplan-Meier curves were used to analyze survival
outcomes for the neoadjuvant immunotherapy and consolidation
immunotherapy groups. The primary endpoint was PFS, and the
secondary endpoints were treatment-related adverse events and
overall survival (OS). PFS was defined as the time from treatment
initiation to tumor progression or death from any cause, and OS was
defined as the time from treatment initiation to death from any
cause or the last follow-up. The log-rank test was used to compare
survival differences between groups. Missing data were treated as
separate categorical variables in the analysis. As this was a
single-arm, retrospective real-world study, no prospective
hypothesis-driven sample size calculation was performed.
In the univariate analysis, the Cox proportional
hazards regression model was used to identify factors significantly
associated with survival, including sex, age, ECOG performance
status, smoking history, cancer stage, pathological subtype of
NSCLC, PD-L1 expression level, and the types and grades of
treatment-related toxicities. All variables were analyzed as either
continuous or categorical, as appropriate. Variables with a P-value
<0.20 in the univariate analysis were included in the
multivariate regression model. Results are expressed as hazard
ratios (HRs) with corresponding 95% confidence intervals (CIs). All
statistical analyses were performed using R software version 4.4.0
(R Foundation for Statistical Computing), and two-sided P<0.05
was considered to indicate a statistically significant
difference.
Results
Patient characteristics
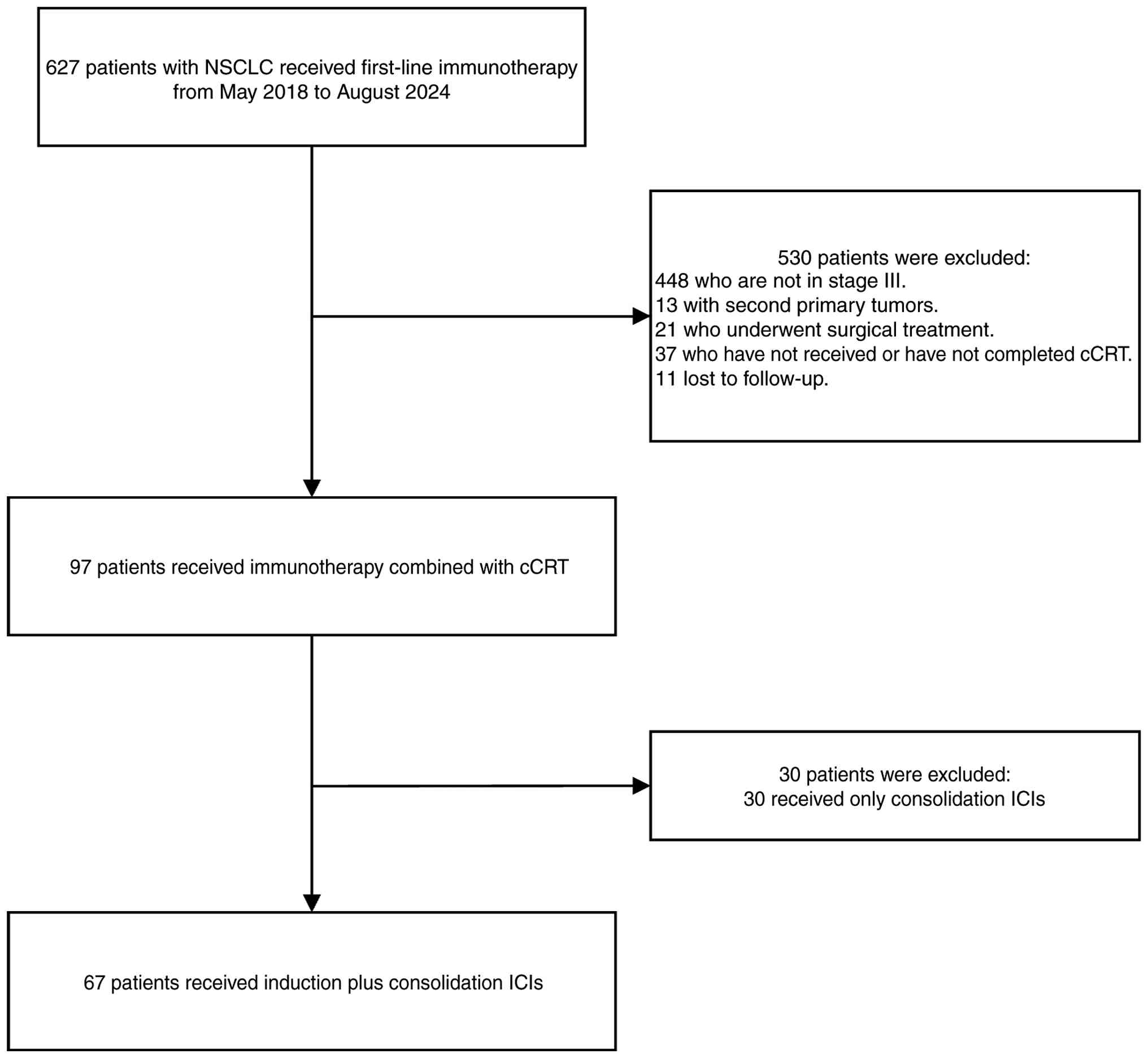
A total of 67 patients with unresectable stage III
NSCLC who experienced neoadjuvant immunotherapy failure were
included in the present study (Fig.
1). Baseline demographic and clinical characteristics are
summarized in Table I. The median
age was 65 years [interquartile range (IQR), 58–69 years]. There
were 3 women (4.48%) and 64 men (95.52%). Most had an ECOS PS of 1,
and more patients had a score of 2 than 0. Squamous cell carcinoma
accounted for 73.13% of cases, and non-squamous cell carcinoma for
26.87%. According to the eighth edition of the AJCC staging system,
11 patients (16.42%) had stage IIIA, 47 (70.15%) had stage IIIB and
nine (13.43%) had stage IIIC disease. PD-L1 expression ≥1% was
detected in 44.78% of patients. The treatment regimen primarily
consisted of platinum-based doublet chemotherapy combined with ICIs
as induction therapy, followed by concurrent or sequential
chemoradiotherapy and subsequent consolidation immunotherapy. In
the PACIFIC regimen cohort, the median age was 63 years (IQR, 57–70
years), with 24 males (80.00%) and 6 women (20.00%). The majority
of patients had an ECOG performance status of 0 or 1. In terms of
histology, squamous cell carcinoma accounted for 53.33% (16/30) and
non-squamous cell carcinoma for 46.67% (14/30) of cases. Disease
staging according to the AJCC staging 8th edition was as follows: 6
patients (20.00%) with stage IIIA, 19 patients (63.33%) with stage
IIIB and five patients (16.67%) with IIIC. PD-L1 expression was ≥1%
in 36.67% of patients. All patients received platinum-based doublet
chemotherapy concurrent with radiotherapy, followed by
consolidation immunotherapy with a PD-L1 inhibitor.
 | Table I.Baseline characteristics of patients
(n=97). |
Table I.
Baseline characteristics of patients
(n=97).
| Variable | Induction +
consolidation ICIs (n=67) | Consolidation ICIs
(n=30) |
|---|
| Median age
(Q1-Q3), years | 65.00
(58.00–69.00) | 63.00
(57.00–70.00) |
| Sex, n (%) |
|
|
|
Male | 64 (95.52) | 24 (80.00) |
|
Female | 3 (4.48) | 6 (20.00) |
| ECOG PS, n (%) |
|
|
| 0 | 4 (5.97) | 2 (6.67) |
| 1 | 56 (83.58) | 20 (66.67) |
| 2 | 7 (10.45) | 8 (26.67) |
| Smoking history, n
(%) |
|
|
| No | 9 (13.43) | 6 (20.00) |
|
Yes | 58 (86.57) | 24 (80.00) |
| T stage, n (%) |
|
|
| T1 | 6 (8.96) | 2 (6.67) |
| T2 | 19 (28.36) | 9 (30.00) |
| T3 | 24 (35.82) | 10 (33.33) |
| T4 | 18 (26.87) | 9 (30.00) |
| N stage, n (%) |
|
|
| N0 | 2 (2.99) | 0 (0.00) |
| N1 | 3 (4.48) | 2 (6.67) |
| N2 | 41 (61.19) | 20 (66.67) |
| N3 | 21 (31.34) | 8 (26.67) |
| Overall stage, n
(%) |
|
|
|
IIIA | 11 (16.42) | 6 (20.00) |
|
IIIB | 47 (70.15) | 19 (63.33%) |
|
IIIC | 9 (13.43) | 5 (16.67%) |
| Pathological type,
n (%) |
|
|
|
Non-squamous cell
carcinoma | 18 (26.87) | 14 (46.47) |
|
Squamous cell carcinoma | 49 (73.13) | 16 (53.33) |
| PD-L1 expression, n
(%) |
|
|
| NA | 17 (25.37) | 19 (63.33) |
|
<1 | 20 (29.85) | 0 (0.00) |
|
1-50 | 11 (16.42) | 8 (26.67) |
|
>50 | 19 (28.36) | 3 (10.00) |
| Median PTV dose
(range), Gy | 60 (60–70) | 60 (60–70) |
| Median PTV
(Q1-Q3) | 206.28
(114.28–327.07) | 49.09
(34.54–76.42) |
Survival outcomes
At a median follow-up of 19.4 months, 38 patients
(56.72%) had disease progression, and 20 patients (29.85%) had died
at the data cutoff (data not shown). The PACIFIC regimen remains
the standard treatment for patients with unresectable stage III
NSCLC. To evaluate the efficacy of consolidation immunotherapy
following cCRT after failure of neoadjuvant chemoimmunotherapy, PFS
was compared between patients in this study and previously treated
patients at The Second Affiliated Hospital of Nanchang University
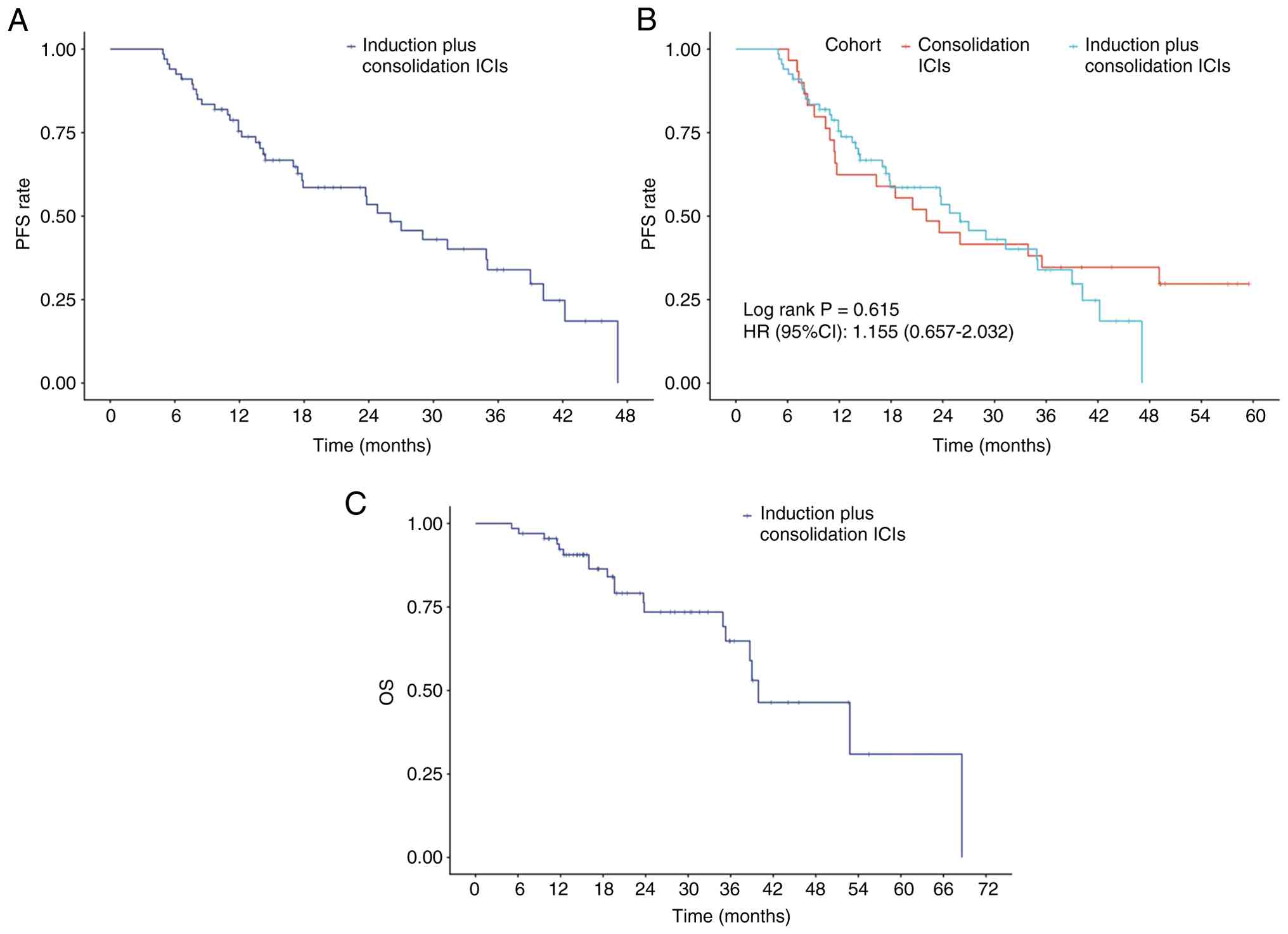
who received the PACIFIC regimen. The median PFS time was 26.0
months (95% CI, 17.8–39.0) in the induction plus consolidation ICI
group (Fig. 2A), compared with 22.1
months (95% CI, 11.7-not reached) in the consolidation ICI-only
group. No statistically significant difference was observed between
the two groups (HR, 1.155; 95% CI, 0.657–2.032; log-rank P=0.615;
Fig. 2B). The 1-, 2- and 3-year OS
rates were 92.5, 79.1 and 77.6%, respectively. The median OS time
was not reached (Fig. 2C).
Safety profiles
Treatment-related adverse events are summarized in
Table II. The overall incidence of
bone marrow suppression was 86.57%, including the reduction of
white blood cells, granulocytes, as well as the decrease in red
blood cells and platelets. Leukopenia occurred in 50 patients
(74.63%). Granulocytopenia was reported in 67.17% of patients,
thrombocytopenia in 40.3% and erythropenia in 68.66%.
Immune-related adverse events (irAEs) were observed in 23 patients
(34.33%), and radiation-related adverse events (rrAEs) in 43
patients (64.18%). IrAEs included Pruritus (itching),
Immune-related pneumonitis, Hepatic dysfunction, Hypothyroidism,
Cognitive impairment, Colitis and Fatigue. RrAE include Radiation
esophagitis, Radiation pneumonitis and Radiodermatitis. Grade ≥3
pneumonitis associated with immunotherapy and radiotherapy occurred
in 4 cases (5.97%) and three cases (4.48%), respectively. No
unexpected safety signals were detected.
| Table II.Treatment-related adverse events
(n=67). |
Table II.
Treatment-related adverse events
(n=67).
| Adverse event | Grade <3, n
(%) | Grade ≥3, n
(%) |
|---|
| Any | 64 (95.52) | 38 (56.72) |
| Leukopenia | 34 (50.75) | 16 (23.88) |
|
Granulocytopenia | 30 (44.78) | 15 (22.39) |
|
Thrombocytopenia | 20 (29.85) | 7 (10.45) |
| Erythropenia | 36 (53.73) | 10 (14.93) |
| Erythema | 4 (5.97) | 1 (1.49) |
| Pruritus
(itching) | 1 (1.49) | 0 (0.0) |
| Immune-related
pneumonitis | 5 (7.46) | 4 (5.97) |
| Hepatic
dysfunction | 1 (1.49) | 2 (2.99) |
| Hypothyroidism | 2 (2.99) | 2 (2.99) |
| Cognitive
impairment | 0 (0.0) | 2 (2.99) |
| Colitis | 0 (0.0) | 1 (1.49) |
| Fatigue | 1 (1.49) | 0 (0.0) |
| Radiation
esophagitis | 29 (43.28) | 5 (7.46) |
| Radiation
pneumonitis | 8 (11.94) | 3 (4.48) |
|
Radiodermatitis | 2 (2.99) | 0 (0.0) |
Prognostic factors
In the multivariate analysis, grade ≥3
granulocytopenia was identified as a significant prognostic factor,
with an HR of 3.78 (95% CI, 1.23–11.62; P=0.020). Grade ≥3
erythropenia was also significantly associated with poorer PFS,
with an HR of 5.70 (95% CI, 1.58–20.59; P=0.008), indicating a
strong relationship between severe hematological toxicity and
unfavorable PFS. Conversely, grade 1–2 thrombocytopenia was
significantly associated with improved PFS, with an HR of 0.20 (95%
CI, 0.06–0.67; P=0.009). Other factors analyzed were not
significant predictors of PFS in the multivariate model (Table III).
| Table III.Univariate and multivariate analyses
of prognostic factors for progression-free survival. |
Table III.
Univariate and multivariate analyses
of prognostic factors for progression-free survival.
| Variables | P-value | HR (95% CI) | P-value | HR (95% CI) |
|---|
| Age | 0.462 | 0.98
(0.94–1.03) |
|
|
| Sex |
|
|
|
|
|
Female |
| 1.00
(Reference) |
|
|
|
Male | 0.745 | 1.27
(0.30–5.36) |
|
|
| ECOG PS |
|
|
|
|
| 0 |
| 1.00
(Reference) |
|
|
| 1 | 0.755 | 1.26
(0.30–5.29) |
|
|
| 2 | 0.471 | 1.88
(0.34–10.50) |
|
|
| Smoking status |
|
|
|
|
|
Never |
| 1.00
(Reference) |
|
|
|
Smoker | 0.357 | 1.64
(0.57–4.71) |
|
|
| Stage at
diagnosis |
|
|
|
|
|
IIIA |
| 1.00
(Reference) |
|
|
|
IIIB | 0.239 | 1.88
(0.66–5.42) |
|
|
|
IIIC | 0.405 | 1.72
(0.48–6.12) |
|
|
| Histology |
|
|
|
|
|
NSCC |
| 1.00
(Reference) |
|
|
|
SCC | 0.506 | 1.28
(0.61–2.69) |
|
|
| PD-L1
expression |
|
|
|
|
|
Negative |
| 1.00
(Reference) |
|
|
|
1-49% | 0.494 | 1.35
(0.57–3.20) |
|
|
|
≥50% | 0.365 | 0.54
(0.15–2.03) |
|
|
|
N/A | 0.696 | 0.84
(0.35–2.02) |
|
|
| Leukopenia |
|
|
|
|
| No |
| 1.00
(Reference) |
|
|
| Grade
1–2 | 0.614 | 0.81
(0.36–1.83) |
|
|
| Grade
≥3 | 0.245 | 1.69
(0.70–4.11) |
|
|
|
Granulocytopenia |
|
|
|
|
| No |
| 1.00
(Reference) |
| 1.00
(Reference) |
| Grade
1–2 | 0.875 | 0.94
(0.43–2.07) | 0.629 | 1.23
(0.52–2.91) |
| Grade
≥3 | 0.103 | 1.99
(0.87–4.53) | 0.020a | 3.78
(1.23–11.62) |
|
Thrombocytopenia |
|
|
|
|
| No |
| 1.00
(Reference) |
| 1.00
(Reference) |
| Grade
1–2 | 0.172 | 0.58
(0.27–1.27) | 0.009a | 0.20
(0.06–0.67) |
| Grade
≥3 | 0.399 | 1.52
(0.57–4.02) | 0.332 | 0.51
(0.13–1.97) |
| Erythropenia |
|
|
|
|
| No |
| 1.00
(Reference) |
| 1.00
(Reference) |
| Grade
1–2 | 0.184 | 1.74
(0.77–3.93) | 0.460 | 1.39
(0.58–3.34) |
| Grade
≥3 | 0.058 | 2.69
(0.97–7.47) | 0.008a | 5.70
(1.58–20.59) |
| irAE |
|
|
|
|
| No |
| 1.00
(Reference) |
|
|
| Grade
1–2 | 0.377 | 0.67
(0.27–1.64) |
|
|
| Grade
≥3 | 0.460 | 0.71
(0.29–1.75) |
|
|
| rrAE |
|
|
|
|
| No |
| 1.00
(Reference) |
| 1.00
(Reference) |
| Grade
1–2 | 0.721 | 0.88
(0.43–1.79) | 0.495 | 0.76
(0.35–1.66) |
| Grade
≥3 | 0.169 | 0.52
(0.20–1.32) | 0.545 | 0.72
(0.25–2.06) |
Discussion
The present study evaluated the efficacy and safety
of consolidation immunotherapy following cCRT in patients with
unresectable stage III NSCLC who experienced treatment failure
after neoadjuvant chemoimmunotherapy. The median PFS time was 26.0
months. When compared with 30 patients treated according to the
PACIFIC regimen, no significant difference in PFS time was observed
(HR, 1.155; 95% CI, 0.657–2.032; P=0.615). Additionally, the
overall safety profile was manageable. To the best of our
knowledge, this study represents the first real-world analysis of
clinical outcomes and safety in patients with unresectable stage
III NSCLC who experienced failure of neoadjuvant
chemoimmunotherapy.
Patients who successfully undergo conversion therapy
can achieve significantly improved prognoses after surgery
(28–30). The present results indicated that
there was no significant difference in prognosis between patients
who experienced failure of conversion therapy and those who
received standard treatment. However, multiple studies have
reported differing findings regarding the optimal timing of
immunotherapy intervention. According to research by Yang et
al (22), induction combined
with consolidation therapy using ICIs significantly reduced the
risk of distant metastasis compared with consolidation
immunotherapy alone, with trends toward a greater benefit observed
in patients <65 years and those with N3 disease (22). Another study reported that, among
patients with unresectable stage III disease, neoadjuvant
chemoradiotherapy combined with immunotherapy achieved better
outcomes than consolidation immunotherapy with fewer treatment
cycles (23). The phase II clinical
trial KEYNOTE-799 further demonstrated the potential benefits of
early immunotherapy intervention (21). In Cohort A, which included both
patients with squamous and non-squamous disease, the median PFS
time was 29.0 months (95% CI, 16.6–48.5), while the median OS time
was 35.6 months (95% CI, 26.1–44.2). By contrast, Cohort B, which
included only patients with non-squamous disease, had a median PFS
time of 45.3 months (95% CI, 17.9-not reached) and a median OS time
of 56.7 months (95% CI, 41.1-not reached) (21). The discrepancy between the present
findings and those of the aforementioned studies may be attributed
to the distinct characteristics of the present study population.
Whereas the previous studies included all patients with stage III
NSCLC, the present study focused on patients who experienced
failure of neoadjuvant chemoimmunotherapy, a group likely to have a
higher tumor burden and more aggressive disease biology.
Furthermore, patients in the present study received two to four
cycles of combined chemoimmunotherapy before cCRT, whereas in the
KEYNOTE-799 trial (21), cCRT
combined with immunotherapy was initiated after a single cycle of
chemoimmunotherapy. This earlier initiation may have led to T cell
exhaustion, potentially influencing both treatment efficacy and
safety outcomes. Radiotherapy induces the expression of chronic
type I interferons and interferon-stimulated genes, upregulates
PD-L1 and indoleamine 2,3-dioxygenase, an essential enzyme involved
in tumor proliferation and immune suppression, on the tumor
surface, enhances the activity of immunosuppressive cells, and
ultimately leads to lymphocyte depletion and exhaustion of immune
effector cells (31). This process
may represent a key potential mechanism underlying the poor
clinical response observed in some patients during the subsequent
immune maintenance phase. Furthermore, the KEYNOTE-799 study
(21) demonstrated that enhanced
immune activation resulted in longer survival outcomes among
patients with non-squamous cell carcinoma. However, in the present
cohort, a higher proportion of patients had squamous cell carcinoma
(73.13%), which may partially explain the shorter median PFS time
compared with that reported in the KEYNOTE-799 trial (21). Several other studies support this
interpretation, indicating that histological subtype is an
important modulatory factor influencing the therapeutic efficacy of
treatment in stage III NSCLC (32,33).
A high proportion of the patients included in the
present study exhibited squamous cell carcinoma and were male. This
population distribution is closely associated with the
epidemiological characteristics of lung cancer in China and with
the specific inclusion criteria of the present study. First,
smoking is the principal risk factor for lung cancer in China, and
squamous cell carcinoma is strongly correlated with tobacco
exposure (34). Second, previous
research has reported a high prevalence of stage III squamous cell
carcinoma (35). While earlier
large-scale Chinese studies have documented a clear male
predominance in squamous cell carcinoma (36), emerging evidence reveals a
significant rise in female incidence and a shifting epidemiological
landscape (37). The present cohort
composition, with its predominance of male patients, mirrors the
historical distribution pattern of this disease in China. Given
that male patients continue to constitute a major proportion of the
squamous cell carcinoma population, the present results maintain
clinical relevance for this subgroup. Nevertheless, this population
imbalance may limit the generalizability of the study findings.
Future prospective, multicenter studies should aim to recruit a
more balanced patient population to validate and extend these
results.
Regarding treatment-related adverse events, although
the overall incidence was 95.52%, the incidence of
chemotherapy-related bone marrow suppression reached 86.57%. While
some studies have suggested that combining chemotherapy with
immunotherapy may increase the risk of bone marrow suppression
(38–40), additional clinical data are required
to confirm this association. The incidence of adverse events
related to immunotherapy and radiotherapy in the present study was
higher than that reported in the PACIFIC trial (41), but comparable to the findings of the
KEYNOTE-799 trial (21). This
difference may be attributed to the synergistic interaction between
radiotherapy and immunotherapy, which can result in additive tissue
damage. Nevertheless, the overall safety profile remained
manageable. Notably, univariate analysis revealed a positive trend
between irAEs and rrAEs and prolonged PFS time, although this did
not reach statistical significance. This finding provides further
support for a synergistic effect between radiotherapy and
immunotherapy.
Based on clinical data and relevant literature,
factors with a P-value <0.20 in the univariate analysis may also
influence prognosis (42).
Therefore, variables with a P-value <0.20 were included in the
multivariate regression model. The multivariate analysis
demonstrated a strong association between grade ≥3 granulocytopenia
and erythropenia and poorer PFS. Severe bone marrow suppression may
affect clinical outcomes by altering drug dosage, shortening
treatment duration and increasing susceptibility to infection.
Furthermore, a reduction in granulocytes can weaken innate
immunity, whereas anemia exacerbates hypoxia within the tumor
microenvironment and impairs the efficacy of antitumor therapy
(43,44). These findings suggest that severe
treatment-related toxicities may adversely affect therapeutic
effectiveness and highlight the need to develop alternative
treatment strategies for patients experiencing severe adverse
events to improve prognosis. Notably, grade 1–2 thrombocytopenia
was significantly associated with prolonged PFS in the present
study, possibly reflecting the role of platelets in modulating the
tumor microenvironment and promoting tumor cell survival and
proliferation (45).
The present study has several limitations. As a
single-center retrospective analysis, it is inherently subject to
bias. First, differences exist between the patient cohorts. The
study population consisted of patients with stage III disease who
did not undergo surgery after neoadjuvant chemoimmunotherapy,
whereas the PACIFIC cohort included patients with initially
unresectable stage III disease who received definitive cCRT
followed by consolidation immunotherapy. Second, temporal
variations in clinical practice may have introduced era bias. The
treatment periods of the two cohorts spanned several years, during
which advances occurred in radiotherapy techniques, supportive care
and the management of immune-related adverse events. Additionally,
the KEYNOTE-799 study (21)
demonstrated survival differences between squamous and non-squamous
cell carcinoma. Due to the limited sample size, subgroup analysis
to evaluate prognostic differences among histological subtypes was
not feasible in the present study. Future large-scale, prospective,
multicenter studies are warranted to validate these findings and to
better identify prognostic factors and therapeutic targets for this
high-risk population.
In conclusion, the present study evaluated the
prognosis and safety of patients with unresectable stage III NSCLC
who experienced failure of neoadjuvant chemoimmunotherapy. The
results indicate that their prognosis was comparable to that of
patients receiving standard treatment, with a manageable safety
profile. Therefore, neoadjuvant chemoimmunotherapy may represent a
promising therapeutic approach for newly diagnosed, unresectable
stage III NSCLC, offering efficacy and safety comparable to
standard treatment regardless of conversion therapy outcome.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
ZZ conceived and designed the study. LP, FZ, RL and
ZZ performed the data analysis. LP, FZ and RL drafted the
manuscript. LP, FZ, RL, JH, CL, ZC and ZZ reviewed the manuscript.
RL, LP, JH, CL and ZC interpreted data. ZZ supervised the entire
study. All authors have read and approved the final version of the
manuscript. RL and LP confirm the authenticity of all the raw
data.
Ethics approval and consent to
participate
The study protocol was reviewed and approved by the
Ethics Review Committee of the Second Affiliated Hospital of
Nanchang University [Nanchang, China; (2025). no. 111]. As this
research involved retrospective data analysis and all patient
information was anonymized, the committee waived the requirement
for written informed consent. The study was conducted in accordance
with the ethical principles of the Declaration of Helsinki.
Patient consent for publication
This article contains no personally identifiable
information, and all data are presented in aggregated form.
Therefore, individual patient consent for publication was not
required.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Feng R, Su Q, Huang X, Basnet T, Xu X and
Ye W: Cancer situation in China: What does the china cancer map
indicate from the first national death survey to the latest cancer
registration? Cancer Commun (Lond). 43:75–86. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Wei W, Zeng H, Zheng R, Zhang S, An L,
Chen R, Wang S, Sun K, Matsuda T, Bray F and He J: Cancer
registration in China and its role in cancer prevention and
control. Lancet Oncol. 21:e342–e349. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Zeng H, Ran X, An L, Zheng R, Zhang S, Ji
JS, Zhang Y, Chen W, Wei W and He J; HBCR Working Group, :
Disparities in stage at diagnosis for five common cancers in China:
A multicentre, hospital-based, observational study. Lancet Public
Health. 6:e877–e887. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Chen Z, Fillmore CM, Hammerman PS, Kim CF
and Wong KK: Non-small-cell lung cancers: A heterogeneous set of
diseases. Nat Rev Cancer. 14:535–546. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Remon J, Soria JC and Peters S; ESMO
Guidelines Committee. Electronic address, : simpleclinicalguidelines@esmo.org:
Early and locally advanced non-small-cell lung cancer: An update of
the ESMO clinical practice guidelines focusing on diagnosis,
staging, systemic and local therapy. Ann Oncol. 32:1637–1642. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Park K, Vansteenkiste J, Lee KH,
Pentheroudakis G, Zhou C, Prabhash K, Seto T, Voon PJ, Tan DSW,
Yang JCH, et al: Pan-asian adapted ESMO clinical practice
guidelines for the management of patients with locally-advanced
unresectable non-small-cell lung cancer: A KSMO-ESMO initiative
endorsed by CSCO, ISMPO, JSMO, MOS, SSO and TOS. Ann Oncol.
31:191–201. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ricciuti B, Fusco F, Cooper A, Garbo E,
Pecci F, Aldea M, Wang X, Mayoral Penalva M, Ginsberg M, Sholl LM,
et al: Neoadjuvant PD-1 and PD-L1 blockade with chemotherapy for
borderline resectable and unresectable stage III non-small cell
lung cancer. JAMA Oncol. 11:735–741. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sun C, Wang X, Xu Y, Shao G, Chen X, Liu
Y, Zhang P, Lin X, Ma X, Qiu S, et al: Efficiency and safety of
neoadjuvant PD-1 inhibitor (sintilimab) combined with chemotherapy
in potentially resectable stage IIIA/IIIB non-small cell lung
cancer: Neo-pre-IC, a single-arm phase 2 trial. EClinicalMedicine.
68:1024222024. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Yu X, Huang C, Du L, Wang C, Yang Y, Yu X,
Lin S, Yang C, Zhao H, Cai S, et al: Efficacy and safety of
perioperative sintilimab plus platinum-based chemotherapy for
potentially resectable stage IIIB non-small cell lung cancer
(periSCOPE): An open-label, single-arm, phase II trial.
EClinicalMedicine. 79:1029972024. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Forde PM, Spicer J, Lu S, Provencio M,
Mitsudomi T, Awad MM, Felip E, Broderick SR, Brahmer JR, Swanson
SJ, et al: Neoadjuvant nivolumab plus chemotherapy in resectable
lung cancer. N Engl J Med. 386:1973–1985. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lu S, Zhang W, Wu L, Wang W, Zhang P;
Neotorch Investigators, ; Fang W, Xing W, Chen Q, Yang L, et al:
Perioperative toripalimab plus chemotherapy for patients with
resectable non-small cell lung cancer: The neotorch randomized
clinical trial. JAMA. 331:201–211. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Dovedi SJ, Adlard AL, Lipowska-Bhalla G,
McKenna C, Jones S, Cheadle EJ, Stratford IJ, Poon E, Morrow M,
Stewart R, et al: Acquired resistance to fractionated radiotherapy
can be overcome by concurrent PD-L1 blockade. Cancer Res.
74:5458–5468. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Wei J, Montalvo-Ortiz W, Yu L, Krasco A,
Ebstein S, Cortez C, Lowy I, Murphy AJ, Sleeman MA and Skokos D:
Sequence of αPD-1 relative to local tumor irradiation determines
the induction of abscopal antitumor immune responses. Sci Immunol.
6:eabg01172021. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Antonia SJ, Villegas A, Daniel D, Vicente
D, Murakami S, Hui R, Yokoi T, Chiappori A, Lee KH, de Wit M, et
al: Durvalumab after chemoradiotherapy in stage III non-small-cell
lung cancer. N Engl J Med. 377:1919–1929. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Zhou Q, Chen M, Jiang O, Pan Y, Hu D, Lin
Q, Wu G, Cui J, Chang J, Cheng Y, et al: Sugemalimab versus placebo
after concurrent or sequential chemoradiotherapy in patients with
locally advanced, unresectable, stage III non-small-cell lung
cancer in China (GEMSTONE-301): Interim results of a randomised,
double-blind, multicentre, phase 3 trial. Lancet Oncol. 23:209–219.
2022. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Wu YL, Wang L, Sendur MAN, Kim YC, Zhu Z,
Cheng Y, Li P, Qin Y, Macpherson E, Dennis PA and Lu S: PACIFIC-5:
Phase III study of durvalumab after either concurrent or sequential
chemoradiotherapy (CRT) in patients with stage III NSCLC. Ann
Oncol. 30:ix113–ix114. 2019. View Article : Google Scholar
|
|
17
|
Bradley JD, Sugawara S, Lee KHH, Ostoros
G, Demirkazik A, Zemanova M, Sriuranpong V, Gelatti A, Menezes J,
Zurawski B, et al: LBA1 durvalumab in combination with
chemoradiotherapy for patients with unresectable stage III NSCLC:
Final results from PACIFIC-2. ESMO open. 9:1029862024. View Article : Google Scholar
|
|
18
|
Peters S, Tan DSW, Gerber DE, Urbanic J,
Ramalingam SS, Yu J, Xing L, Rittmeyer A, Ciuleanu TE, Menezes JE,
et al: 65O CheckMate 73L: Phase III study comparing nivolumab (N) +
concurrent chemoradiotherapy (CCRT) followed by N ± ipilimumab (I)
v CCRT followed by durvalumab (D) for previously untreated, locally
advanced stage (stg) III NSCLC. ESMO. 24:1008082024.
|
|
19
|
Kumar V, Bauer C and Stewart JH IV: Cancer
cell-specific cGAS/STING signaling pathway in the era of advancing
cancer cell biology. Eur J Cell Biol. 102:1513382023. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Boukhaled GM, Harding S and Brooks DG:
Opposing roles of type I interferons in cancer immunity. Annu Rev
Pathol. 16:167–198. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Reck M, Lee KH, Frost N, Breder V,
Kowalski DM, Levchenko E, Reguart N, Martinez-Marti A, Houghton B,
Paoli JB, et al: 1860: Pembrolizumab (pembro) plus concurrent
chemoradiation therapy (cCRT) in unresectable locally advanced
non-small cell lung cancer (NSCLC): final analysis of KEYNOTE-799.
J Thoracic Oncol. 20:S124–S125. 2025. View Article : Google Scholar
|
|
22
|
Yang Y, Wang J, Zhang T, Zhou Z, Wang Y,
Jiang Y, Liu W, Xiao Z, Deng L, Feng Q, et al: Efficacy and safety
of definitive chemoradiotherapy with or without induction immune
checkpoint inhibitors in patients with stage III non-small cell
lung cancer. Front Immunol. 14:12818882023. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Guan S, Wang Y, Liu Q, Yan M, Ren K, Wang
J, Bi N and Zhao L: Induction chemoimmunotherapy may achieve
non-inferior outcomes to consolidation immunotherapy in patients
with unresectable stage III NSCLC: A real-world multicenter
retrospective study. Front Immunol. 16:15911342025. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Oken MM, Creech RH, Tormey DC, Horton J,
Davis TE, McFadden ET and Carbone PP: Toxicity and response
criteria of the Eastern Cooperative Oncology Group. Am J Clin
Oncol. 5:649–655. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Amin MB, Edge SB, Greene FL, Byrd DR,
Brookland RK, Washington MK, Gershenwald JE, Compton CC, Hess KR,
et al: AJCC Cancer Staging Manual. 8th edition. Springer-Verlag;
New York, NY, USA: pp. 431–467. 2017
|
|
27
|
U.S. Department of Health and Human
Services: Common Terminology Criteria for Adverse Events (CTCAE)
Version 5. 2017.
|
|
28
|
Guan S, Sun J, Wang Y, Han S, Chen C, Yue
D, Huang Y, Ren K, Wang J, Wang J and Zhao L: Chemoradiotherapy
versus surgery after neoadjuvant chemoimmunotherapy in patients
with stage III NSCLC: A real-world multicenter retrospective study.
Cancer Immunol Immunother. 73:1202024. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Deng H, Liu J, Cai X, Chen J, Rocco G,
Petersen RH, Brunelli A, Ng CSH, D'Amico TA, Liang W and He J:
Radical minimally invasive surgery after immuno-chemotherapy in
initially-unresectable stage IIIB non-small cell lung cancer. Ann
Surg. 275:e600–e602. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Wang M, Wang X, Yang R, Geng M, Zhang S,
Yang Z, Huang Q, Wang S, Xu S, Jiang K and Liao Y: Conversion
surgery for initially unresectable stage III nonsmall cell lung
cancer after induction treatment of immunochemotherapy: A
multicenter study. Clin Lung Cancer. 26:e131–e140.e1. 2025.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Wang X, Wang Y, Zhang Y, Shi H, Liu K,
Wang F, Wang Y, Chen H, Shi Y and Wang R: Immune modulatory roles
of radioimmunotherapy: Biological principles and clinical
prospects. Front Immunol. 15:13571012024. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Toriyama K, Yomota M, Asai M, Hashimoto K,
Mirokuji K, Kawai S, Watanabe K, Narita K and Hosomi Y: Real-world
prognostic data on unresectable stage III non-small-cell lung
cancer treated with concurrent chemoradiation therapy by
histological type. Intern Med. 63:2757–2765. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Johnson ML, Cho BC, Luft A,
Alatorre-Alexander J, Geater SL, Laktionov K, Kim SW, Ursol G,
Hussein M, Lim FL, et al: Durvalumab with or without tremelimumab
in combination with chemotherapy as first-line therapy for
metastatic non-small-cell lung cancer: The phase III POSEIDON
study. J Clin Oncol. 41:1213–1227. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Leiter A, Veluswamy RR and Wisnivesky JP:
The global burden of lung cancer: Current status and future trends.
Nat Rev Clin Oncol. 20:624–639. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Yu J, Xing L, Cheng G, Chen L, Dong L, Fu
X, Guo Y, Han Z, Jiang D, Li J, Lin Y, et al: P21.10 real-world
treatment patterns in Chinese stage III NSCLC patients-a
prospective, non-interventional study (MOOREA trial). J Thoracic
Oncol. 16:S367–S368. 2021. View Article : Google Scholar
|
|
36
|
Chen W, Zheng R, Baade PD, Zhang S, Zeng
H, Bray F, Jemal A, Yu XQ and He J: Cancer statistics in China,
2015. CA Cancer J Clin. 66:115–132. 2016.PubMed/NCBI
|
|
37
|
Wang J, Cao H, He N, Liu X, Fu F, Deng C,
Li Y, Zhang Y and Chen H: Evolving trends in surgically managed
lung cancer: A 16-year hospital-based epidemiological analysis.
Lung Cancer. 208:1087542025. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Gandhi L, Rodríguez-Abreu D, Gadgeel S,
Esteban E, Felip E, De Angelis F, Domine M, Clingan P, Hochmair MJ,
Powell SF, et al: Pembrolizumab plus chemotherapy in metastatic
non-small-cell lung cancer. N Engl J Med. 378:2078–2092. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Hellmann MD, Paz-Ares L, Bernabe Caro R,
Zurawski B, Kim SW, Carcereny Costa E, Park K, Alexandru A,
Lupinacci L, de la Mora Jimenez E, et al: Nivolumab plus ipilimumab
in advanced non-small-cell lung cancer. N Engl J Med.
381:2020–2031. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Socinski MA, Jotte RM, Cappuzzo F, Orlandi
F, Stroyakovskiy D, Nogami N, Rodríguez-Abreu D, Moro-Sibilot D,
Thomas CA, Barlesi F, et al: Atezolizumab for first-line treatment
of metastatic nonsquamous NSCLC. N Engl J Med. 378:2288–2301. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Spigel DR, Faivre-Finn C, Gray JE, Vicente
D, Planchard D, Paz-Ares L, Vansteenkiste JF, Garassino MC, Hui R,
Quantin X, et al: Five-year survival outcomes from the PACIFIC
Trial: Durvalumab after chemoradiotherapy in stage III
non-small-cell lung cancer. J Clin Onco. 40:1301–1311. 2022.
View Article : Google Scholar
|
|
42
|
Heinze G and Dunkler D: Five myths about
variable selection. Transpl Int. 30:6–10. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Tang Z, Hu J, Li XC, Wang W, Zhang HY, Guo
YY, Shuai X, Chu Q, Xie C, Lin D and Zhong B: A subset of
neutrophils activates anti-tumor immunity and inhibits
non-small-cell lung cancer progression. Dev Cell. 60:379–395.e8.
2025. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Zhang Y, Guo F and Wang Y: Hypoxic tumor
microenvironment: Destroyer of natural killer cell function. Chin J
Cancer Res. 36:138–150. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Goubran HA, Stakiw J, Radosevic M and
Burnouf T: Platelet-cancer interactions. Semin Thromb Hemost.
40:296–305. 2014. View Article : Google Scholar : PubMed/NCBI
|