Introduction
Bladder cancer (BC) is the ninth most common cancer
worldwide (1). According to global
data from 2022, ~615,000 new cases were diagnosed, and >220,000
deaths occurred due to BC, with the incidence notably higher in men
than in women (2). Based on data
from Cancer Statistics 2025, BC ranks as the fourth most common
cancer in men and eighth in cancer-related deaths in the United
States (US) (3). The median age at
diagnosis is 69 years in men and 71 years in women (4,5).
Although several risk factors for BC have been identified,
cigarette smoking remains the most notable, particularly in Western
populations (6). Tobacco smoke
contains numerous carcinogens, including polycyclic aromatic
hydrocarbons and N-nitrosamines, which are implicated in bladder
carcinogenesis (7).
From a histopathological perspective, urothelial
carcinoma (UC) is the predominant subtype of BC, accounting for
~90% of cases in the US and Western Europe. By contrast,
non-urothelial bladder cancer (NUC) is more prevalent in regions
such as the Middle East, largely due to the endemic presence of
schistosomiasis, an established risk factor (8). In a retrospective analysis of 72,452
patients with UC and NUC in the US, it was found that
adenocarcinoma was diagnosed at younger ages, that non-squamous
NUCs were more common in males, and that squamous cell carcinoma
(SqCC) and small cell neuroendocrine carcinoma subtypes were
associated with poorer prognoses than UC. The same study reported
that >60% of NUC cases were diagnosed at advanced stages, while
nearly 80% of UC cases were identified at early stages (9).
UC may present as pure urothelial carcinoma (PUC) or
with variant histologies (VHs), including squamous, glandular,
micropapillary, trophoblastic, sarcomatoid, nested and
neuroendocrine components. Among these, squamous differentiation in
UC (SD) is the most common, found in ~20% of UC cases (10,11).
SD is characterized histologically by intercellular bridging and
keratinization (12). In one study,
the incidence of high-stage disease (T3-T4) in patients with SD was
72.3%, compared with 43.1% in patients with PUC (11). Furthermore, nodal involvement was
more frequent in patients with diffuse SD (46.2%) than in those
with PUC (27%). Certain studies have suggested that SD is
associated with a more aggressive clinical course and poorer
response to adjuvant chemotherapy (CT) and radiotherapy (RT)
compared with PUC (13–15). However, evidence on the prognostic
impact of SD remains controversial. For example, Wasco et al
(16) reported that although VHs,
including SD, were associated with higher T stages and more
frequent muscle invasion or extravesical extension, they did not
significantly affect disease-free survival (DFS). By contrast,
another study found that the presence of VHs in UC was associated
with worse survival outcomes, particularly with micropapillary,
plasmacytoid and small cell variants, while SD demonstrated similar
survival to PUC (17). Although SD
has been associated with advanced stage and poor prognosis in some
studies, its impact in pathological stage T2N0 (pT2N0) UC remains
unclear (18–26).
The present study aimed to evaluate the clinical
features, treatment response and survival outcomes of patients with
pT2N0 UC exhibiting squamous differentiation in comparison with
those with PUC. It is hypothesized that the study will contribute
to an improved understanding of the clinical course and treatment
strategies of pT2N0 UC with SD.
Materials and methods
Study population
The present study is a clinical, observational,
retrospective cohort study. Pathology reports of all cystectomy
procedures (n=632) performed at Uludag University Faculty of
Medicine (Bursa, Turkey) between December 2010 and December 2023
were reviewed retrospectively. Demographic and clinical data were
extracted from 115 patients with either SD or PUC and a
pathological stage of pT2N0 at cystectomy. The data were obtained
from the institutional hospital automation system. This study was
approved by the Uludag University Faculty of Medicine Clinical
Research Ethics Committee (Bursa, Turkey; approval no. 2025/4-26).
The inclusion criteria were as follows: i) Patients aged ≥18 years;
ii) histopathological diagnosis of UC with or without SD; iii)
pathological stage pT2N0 at the time of cystectomy; iv) no evidence
of distant metastasis and v) availability of complete clinical and
follow-up data. The exclusion criteria were as follows: i) <18
years of age; ii) histological differentiation other than SD; iii)
distant metastases at diagnosis; and iv) did not undergo curative
surgery.
Data collection
The data were obtained through retrospective review
of hospital electronic records and archived clinical files. The
following variables were recorded: i) Demographic, clinical and
pathological characteristics; ii) smoking history; iii)
comorbidities; iv) stage at diagnosis; v) the Bacillus
Calmette-Guerin treatment; vi) surgical procedures; vii) adjuvant
systemic treatments (CT and/or RT); viii) recurrence status; ix)
survival status; and x) last follow-up date.
Histopathological examination
Histopathological evaluation was performed on
formalin-fixed, paraffin-embedded tissue sections using routine
hematoxylin and eosin staining. Tissue samples were fixed in 10%
neutral buffered formalin at room temperature for 24–48 h.
Paraffin-embedded sections were cut at a thickness of 4 µm.
Hematoxylin and eosin staining was performed at room temperature,
with hematoxylin staining for 5 min followed by eosin staining for
2 min. All slides were reviewed by an experienced genitourinary
pathologist according to the 2022 World Health Organization
classification criteria (27) using
light microscopy. Histopathological re-evaluation was performed in
a subset of patients (n=69) after the application of the predefined
exclusion criteria. Based on the initial pathology reports, 15
patients with SD and 31 patients with PUC were excluded (Fig. 1). The remaining 69 patients
underwent review by a genitourinary pathologist. Among these, six
patients initially reported as PUC were reclassified as squamous
differentiation and subsequently included in the SD group. In
addition, one patient with a non-squamous VH (trophoblastic
differentiation) was excluded. Only patients with confirmed pT2N0
disease after pathological re-evaluation were included in the final
analysis. The study flow diagram illustrating the patient selection
process is presented in Fig. 1.
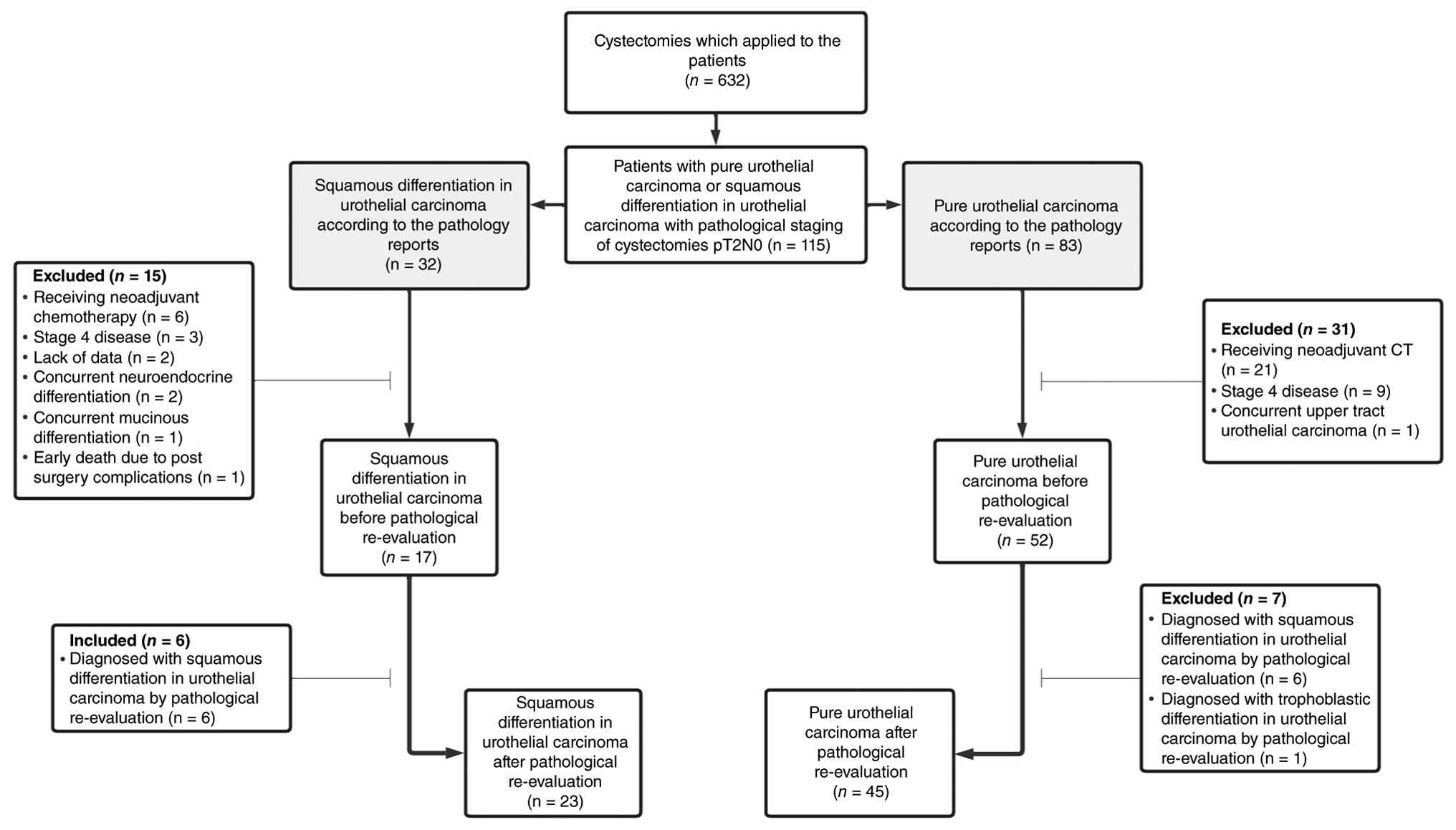 | Figure 1.Study flow diagram of patient
selection and histopathological re-evaluation. A total of 632
patients who underwent cystectomy were screened, of whom 115
patients with pT2N0 UC were identified based on initial pathology
reports. After applying predefined exclusion criteria (including
neoadjuvant CT, stage IV disease, missing data, concurrent VHs and
early postoperative mortality), 69 patients underwent
histopathological re-evaluation. Following re-evaluation, 23
patients were classified as having SD and 45 as PUC; one patient
with a non-squamous VH was excluded. pT2N0, pathological stage
T2N0; UC, urothelial carcinoma; VH, variant histology; SD, squamous
differentiation in urothelial carcinoma; PUC, pure urothelial
carcinoma. |
Statistical analysis
Statistical analyses were conducted using IBM SPSS
Statistics version 25.0 (IBM Corp.). Categorical variables were
summarized as frequencies and percentages, and continuous variables
were expressed as the mean ± standard deviation, median and range
(minimum-maximum). Kolmogorov-Smirnov and Shapiro-Wilk tests were
used to assess normality of distribution. Comparisons between two
independent groups were performed using the independent samples
t-test for normally distributed variables and the Mann-Whitney U
test for non-normally distributed variables. Survival analyses were
performed using the Kaplan-Meier method, and survival curves were
generated accordingly. DFS was defined as the time from curative
surgery to recurrence, last follow-up or death. Overall survival
(OS) was defined as the time from curative surgery to death or last
follow-up. Univariate Cox regression analysis was used to identify
factors associated with survival outcomes. P<0.05 was considered
to indicate a statistically significant difference.
Results
The median age of the patients was 66 years (range,
43–80 years), the majority were men and the median follow-up
duration was 5.27 years (range, 0.23–16.60 years). The most common
comorbidity was hypertension, which was present in 37 patients
(54.4%). Among the 68 patients included in the present study, the
SD group consisted of 23 patients. Comparative analysis revealed no
significant differences between the two groups in terms of
demographic and clinical characteristics, except for sex. Adjuvant
CT was administered to only four patients (two in each group).
Given the very limited number of cases, no meaningful comparison or
subgroup analysis could be performed. Baseline characteristics of
the study population are summarized in Table I.
 | Table I.Baseline clinicopathological
characteristics of the study population. |
Table I.
Baseline clinicopathological
characteristics of the study population.
| Characteristics
(n=68) | Squamous
differentiation (n=23) | Pure urothelial
carcinoma (n=45) | P-value |
|---|
| Age, median
(range) | 67 (48–77) | 65 (43–80) | 0.183 |
| Sex (%) |
|
| 0.028 |
|
Male | 18 (78.3) | 43 (95.6) |
|
|
Female | 5 (21.7) | 2 (4.4) |
|
| Comorbidity
(%) |
|
|
|
|
Hypertension | 11 (47.8) | 26 (57.8) | 0.439 |
|
Diabetes mellitus | 4 (17.4) | 7 (15.6) | 0.847 |
|
IHD | 3 (13.0) | 14 (31.1) | 0.106 |
|
Asthma/COPD | 3 (13.0) | 12 (26.7) | 0.203 |
| Smoking
statusa, n (%) |
|
| 0.191 |
|
Yes | 7 (30.4) | 19 (42.2) |
|
| No | 5 (21.7) | 3 (6.7) |
|
|
Missing | 11 (47.8) | 23 (51.1) |
|
| Smoking
(pack/year), mean ± SD | 39.0±6.7 | 39.8±3.7 | 0.918 |
| De novo pT2,
n (%) | 15 (65.2) | 34 (75.6) | 0.372 |
| BCG, n (%) | 2 (8.7) | 6 (13.3) | 0.577 |
| Type of surgery, n
(%) |
|
| 0.377 |
|
RCP | 18 (78.3) | 39 (86.7) |
|
| RC | 5 (21.7) | 6 (13.3) |
|
| Adjuvant
chemotherapy, n (%) | 2 (8.7) | 2 (4.4) | 0.484 |
| Follow-up duration,
years mean ± SD | 5.76±0.75 | 6.49±0.68 | 0.697 |
Recurrence occurred in seven patients (30.4%) in the
SD group and 10 patients (22.2%) in the PUC group. A total of 11
patients (47.8%) in the SD group and 21 patients (46.7%) in the PUC
group died. The median DFS was 5.61 years [95% confidence interval
(CI), 0.63–10.59] in the SD group and 9.17 years (95% CI,
1.64–16.70) in the PUC group (P=0.998). The median OS was 5.61
years (95% CI, 0.58–10.64) in the SD group and 10.15 years (95% CI,
3.49–16.82) in the PUC group (P=0.795). Kaplan-Meier survival
curves are presented in Figs. 2 and
3.
Univariate Cox regression analysis was performed to
identify potential prognostic factors associated with survival
outcomes. In the univariate Cox regression analysis, age at
diagnosis emerged as a potential prognostic factor of both DFS and
OS. The detailed results of the univariate Cox regression analysis
for DFS and OS are presented in Table
II.
| Table II.Univariate cox regression analysis of
factors associated with DFS and OS. |
Table II.
Univariate cox regression analysis of
factors associated with DFS and OS.
| A, DFS |
|---|
|
|---|
|
|
| 95% CI |
|
|---|
|
|
|
|
|
|---|
| Variable | HR | Lower | Upper | P-value |
|---|
| Agea | 1.089 | 1.029 | 1.152 | 0.003 |
| Sexb | 0.228 | 0.031 | 1.667 | 0.145 |
| Smoking
statusc | 2.325 | 0.517 | 10.448 | 0.271 |
| Smoking
(pack/year) | 1.000 | 0.966 | 1.035 | 0.994 |
| Pathological
subtyped | 0.999 | 0.486 | 2.057 | 0.998 |
| De novo
pT2e | 0.558 | 0.274 | 1.139 | 0.109 |
| BCGf | 0.631 | 0.192 | 2.069 | 0.447 |
| Adjuvant
CTg | 0.305 | 0.042 | 2.238 | 0.243 |
| B, OS |
|
|
|
| 95% CI |
|
|
|
|
|
|
|
Variable | HR | Lower | Upper | P-value |
|
| Agea | 1.099 | 1.036 | 1.167 | 0.002 |
| Sexb | 0.251 | 0.034 | 1.840 | 0.174 |
| Smoking
statusc | 1.970 | 0.429 | 9.038 | 0.383 |
| Smoking
(pack/year) | 0.998 | 0.961 | 1.037 | 0.920 |
| Pathological
subtyped | 0.908 | 0.436 | 1.891 | 0.796 |
| De novo
pT2e | 0.519 | 0.251 | 1.074 | 0.077 |
| BCGf | 0.702 | 0.213 | 2.311 | 0.560 |
| Adjuvant
CTg | 0.326 | 0.044 | 2.398 | 0.271 |
Discussion
In the present study, no significant differences in
survival were observed between patients with SD and those with PUC.
This finding was observed in a highly selected cohort of patients
who did not receive neoadjuvant therapy, had no distant metastasis
and had pT2N0 disease.
Transcriptomic profiling studies have demonstrated
that BC can be classified into molecular subtypes, including
luminal and basal-like tumors (28). Basal tumors are more frequently
associated with squamous features and tend to have a more
aggressive clinical course, whereas luminal tumors are linked to a
more favorable prognosis and distinct therapeutic targets (28,29).
It has also been reported that basal subtype tumors may have an
improved response to immune checkpoint inhibitors (ICIs), while
luminal tumors may benefit more from fibroblast growth factor
receptor 3- and human epidermal growth factor receptor 2-targeted
therapies (30). Moreover, SqCC has
been associated with responsiveness to epidermal growth factor
receptor-targeted agents (29).
Within this biological framework, the clinical
importance of squamous differentiation remains to be clarified. In
this context, it is important to distinguish SD from SqCC, which is
defined by complete squamous differentiation (30). SD is considered an intermediate
phenotype between SqCC and UC based on immunohistochemical
characteristics (31). While
treatment responses and prognostic implications have been
relatively well described for SqCC, data on the clinicopathological
features and survival outcomes of patients with SD remain limited,
particularly in early-stage disease.
The patient population in the present study
represents a highly specific and distinct cohort. All patients
included had a diagnosis of either SD or PUC, a pathological stage
of T2, no lymph node involvement or distant metastasis, had not
received neoadjuvant systemic therapy, and underwent cystectomy. To
the best of our knowledge, no prior study in the literature has
examined a cohort with such narrowly defined inclusion criteria.
The majority of studies in the literature involve broader patient
populations, including varying pathological stages and the presence
of nodal or distant metastases, which may explain discrepancies in
reported outcomes. For example, Minato et al (18) evaluated clinical characteristics and
survival outcomes in 101 patients with cT2-T4aN0M0 disease who
underwent radical cystectomy (PUC, n=81; SD, n=20). Unlike the
present study, the multivariate analysis identified the presence of
squamous differentiation as a factor negatively affecting OS.
However, the cohort included a higher proportion of advanced-stage
patients, with 60% of the SD group and 30.9% of the PUC group
diagnosed with pathological stage T3 or higher, and nodal
positivity reported in 45 and 21% of cases, respectively. Notably,
only eight patients in the SD group had stage ≤pT2 disease
(18). Izard et al (19) conducted another large study
including 178 patients with SqCC, 325 with SD and 2,884 with PUC.
Similar to the present study, a higher proportion of female
patients was noted in the SD group. However, in contrast to the
findings of the present study, their cohort included ~40% of
patients with T3 stage disease and 25% with lymph node positivity.
Furthermore, T3 stage disease was more common in the SD and SqCC
groups, while T1 disease was more prevalent in the PUC group. The
5-year OS rates were reported as 34% for SD and 28% for PUC. In
their multivariate analysis, factors that were independently
associated with OS included age ≥70 years, advanced T and N stages
and positive surgical margins. In the present univariate analysis,
age at diagnosis was associated with both DFS and OS. Other
variables could not be compared due to the homogeneity of the
present cohort, whereby all patients had pT2N0 disease with
negative surgical margins (19).
Several studies have reported findings consistent with the present
study, demonstrating no notable survival difference between SD and
PUC following cystectomy (20–24).
By contrast, certain studies have suggested a negative prognostic
impact of squamous differentiation, particularly in cohorts
including more advanced-stage disease (18,25).
These discrepancies may largely be explained by differences in
patient selection, particularly with respect to pathological stage
and nodal involvement.
Previous studies have suggested that patients with
progressive T2 disease following non-muscle-invasive bladder cancer
may have worse oncological outcomes compared with those with de
novo disease (32–34). By contrast, the present study did
not demonstrate a significant difference between these groups,
although this finding should be interpreted with caution due to the
limited sample size.
In a study evaluating cancer-specific survival (CSS)
and OS in 117,275 patients with BC using the Surveillance,
Epidemiology, and End Results database from 2004 to 2015, age ≥75
years at diagnosis was identified as an independent factor
associated with poorer CSS and OS outcomes (35). Similarly, the present study
demonstrated that age ≥65 years at the time of diagnosis was a
potential risk factor negatively impacting both DFS and OS.
In the study conducted by Laymon et al
(36) the clinicopathological
characteristics and survival outcomes of 223 patients with SD and
318 patients with SqCC were evaluated. The findings showed that
lymph node involvement and extravesical extension were more common
among patients with SD, and the 5-year recurrence-free survival was
significantly worse in the SD group compared with the SqCC group
(36). By contrast, in the present
study a comparative analysis between patients with SD and those
with PUC was conducted, allowing specific examination of the
prognostic implications of squamous differentiation within the
context of UC.
Smoking is a well-established risk factor for BC and
has been associated with more aggressive tumor biology and VHs,
including SD (37,38). In the present study, smoking status
was comparable between groups and was not associated with survival
outcomes, possibly due to the limited sample size.
Notably, a significant difference in sex
distribution was observed between the SD and PUC groups in the
present study. Although definitive evidence is lacking, previous
studies have suggested that VHs, including SD and SqCC, may be
relatively more frequent in women compared with PUC, potentially
due to differences in carcinogen exposure, hormonal factors and
delays in diagnosis (39,40). The findings of the present study
appear to be consistent with these observations. However, this
result should be interpreted with caution given the relatively
small sample size and the retrospective design of the study.
The present study had several limitations. The most
notable is its single-center, retrospective design and relatively
small sample size, particularly in the SD group, which may have
limited the statistical power to detect significant differences,
thereby increasing the risk of a type II error. Additionally, only
four patients received adjuvant CT, and none received ICIs,
limiting the ability to evaluate the impact of adjuvant treatment
on survival outcomes. The exclusion of patients who received
neoadjuvant CT further restricted the generalizability of the
findings. Another important limitation is the lack of quantitative
assessment of the extent of squamous differentiation. Although
histopathological re-evaluation was performed by a dedicated
genitourinary pathologist, the available specimens and pathology
reports did not include a standardized or reproducible
quantification of the squamous component. Therefore, the prognostic
impact of the percentage of squamous differentiation was not
reliably assessed. Future prospective studies with standardized
pathological reporting are needed to clarify this issue. Finally,
multivariate Cox regression analysis was not performed due to the
limited number of events. Therefore, only univariate analysis was
considered appropriate.
In conclusion, the present study demonstrated that
the presence of squamous differentiation does not impact DFS or OS
in patients with pT2N0 UC who underwent cystectomy without prior
neoadjuvant treatment or evidence of metastasis. Although existing
literature presents conflicting results, the findings align with
the majority of studies suggesting no prognostic difference between
SD and PUC in this patient population. However, these findings
should be interpreted with caution and may not be generalizable to
patients with more advanced pathological stages, nodal involvement
or those receiving neoadjuvant systemic therapy. Larger,
prospective, multi-center studies are warranted to establish more
definitive conclusions.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
AC, TE and IY conceptualized the study. AC, ABS, SK,
MED and EC performed the experiments. MED, AC, ABS and AD analyzed
the data. SS and BEO contributed to data interpretation and
critically revised the manuscript for important intellectual
content. MK and GS performed study validation, contributed to
retrospective clinical data collection and verification, and
critically revised the manuscript for important intellectual
content. SK, SS, AD, TE and IY obtained the resources. AC, SK, MED,
SS, BEO, MK and GS contributed to clinical data collection and
organization. AC and ABS wrote the original draft. AC, ABS and EC
reviewed and edited the manuscript. AD, MK and GS constructed the
figures. AC, ABS, TE and IY supervised the study. All authors have
read and approved the final version of the manuscript. AC and ABS
confirm the authenticity of all the raw data.
Ethics approval and consent to
participate
This study was approved by the Uludag University
Faculty of Medicine Clinical Research Ethics Committee (Bursa,
Turkey; approval no. 2025/4-26; date: February 19, 2025). Due to
the retrospective design of the study, the requirement for informed
consent was waived by the ethics committee.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bray F, Laversanne M, Sung H, Ferlay J,
Siegel RL, Soerjomataram I and Jemal A: Global cancer statistics
2022: GLOBOCAN estimates of incidence and mortality worldwide for
36 cancers in 185 countries. CA Cancer J Clin. 74:229–263.
2024.PubMed/NCBI
|
|
2
|
Safiri S, Kolahi AA and Naghavi M; Global
Burden of Disease Bladder Cancer Collaborators, : Global, regional
and national burden of bladder cancer and its attributable risk
factors in 204 countries and territories, 1990–2019: A systematic
analysis for the global burden of disease study 2019. BMJ Glob
Health. 6:e0041282021. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Siegel RL, Kratzer TB, Giaquinto AN, Sung
H and Jemal A: Cancer statistics, 2025. CA Cancer J Clin. 75:10–45.
2025.PubMed/NCBI
|
|
4
|
Lynch CF and Cohen MB: Urinary system.
Cancer. 75 (1 Suppl):S316–S329. 1995. View Article : Google Scholar
|
|
5
|
Scosyrev E, Noyes K, Feng C and Messing E:
Sex and racial differences in bladder cancer presentation and
mortality in the US. Cancer. 115:68–74. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Jubber I, Ong S, Bukavina L, Black PC,
Compérat E, Kamat AM, Kiemeney L, Lawrentschuk N, Lerner SP, Meeks
JJ, et al: Epidemiology of bladder cancer in 2023: A systematic
review of risk factors. Eur Urol. 84:176–190. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hecht SS: Cigarette smoking: Cancer risks,
carcinogens, and mechanisms. Langenbecks Arch Surg. 391:603–613.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Amin HAA, Kobaisi MH and Samir RM:
Schistosomiasis and bladder cancer in Egypt: Truths and Myths. Open
Access Maced J Med Sci. 7:4023–4029. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Martin JW, Jefferson FA, Huang M, Sung JM,
Chang J, Piranviseh K, Ziogas A, Anton-Culver H and Youssef RF: A
california cancer registry analysis of urothelial and
non-urothelial bladder cancer subtypes: Epidemiology, treatment,
and survival. Clin Genitourin Cancer. 18:e330–e336. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lopez-Beltran A and Cheng L: Histologic
variants of urothelial carcinoma: Differential diagnosis and
clinical implications. Hum Pathol. 37:1371–1388. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Liu Y, Bui MM and Xu B: Urothelial
carcinoma with squamous differentiation ıs associated with high
tumor stage and pelvic lymph-node metastasis. Cancer Control.
24:78–82. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Gellert LL, Warrick J and Al-Ahmadie HA:
Urothelial carcinoma with squamous differentiation-the
pathologists' perspective. Urol Oncol. 33:437–443. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Billis A, Schenka AA, Ramos CC, Carneiro
LT and Araújo V: Squamous and/or glandular differentiation in
urothelial carcinoma: Prevalence and significance in transurethral
resections of the bladder. Int Urol Nephrol. 33:631–633. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Logothetis CJ, Johnson DE, Chong C, Dexeus
FH, Sella A, Ogden S, Smith T, Swanson DA, Babaian RJ, Wishnow KI,
et al: Adjuvant cyclophosphamide, doxorubicin, and cisplatin
chemotherapy for bladder cancer: An update. J Clin Oncol.
6:1590–1596. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Martin JE, Jenkins BJ, Zuk RJ, Blandy JP
and Baithun SI: Clinical importance of squamous metaplasia in
invasive transitional cell carcinoma of the bladder. J Clin Pathol.
42:250–253. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Wasco MJ, Daignault S, Zhang Y, Kunju LP,
Kinnaman M, Braun T, Lee CT and Shah RB: Urothelial carcinoma with
divergent histologic differentiation (mixed histologic features)
predicts the presence of locally advanced bladder cancer when
detected at transurethral resection. Urology. 70:69–74. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Mori K, Abufaraj M, Mostafaei H, Quhal F,
Karakiewicz PI, Briganti A, Kimura S, Egawa S and Shariat SF: A
systematic review and meta-analysis of variant histology in
urothelial carcinoma of the bladder treated with radical
cystectomy. J Urol. 204:1129–1140. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Minato A, Noguchi H, Tomisaki I, Fukuda A,
Kubo T, Nakayama T and Fujimoto N: Clinical significance of
squamous differentiation in urothelial carcinoma of the bladder.
Cancer Control. 25:10732748188002692018. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Izard JP, Siemens DR, Mackillop WJ, Wei X,
Leveridge MJ, Berman DM, Peng Y and Booth CM: Outcomes of squamous
histology in bladder cancer: A population-based study. Urol Oncol.
33:425.e7–e13. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Monn MF, Kaimakliotis HZ, Pedrosa JA, Cary
KC, Bihrle R, Cheng L and Koch MO: Contemporary bladder cancer:
Variant histology may be a significant driver of disease. Urol
Oncol. 33:18.e15–e18.e20. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kim SP, Frank I, Cheville JC, Thompson RH,
Weight CJ, Thapa P and Boorjian SA: The impact of squamous and
glandular differentiation on survival after radical cystectomy for
urothelial carcinoma. J Urol. 188:405–409. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Mitra AP, Bartsch CC, Bartsch G Jr,
Miranda G, Skinner EC and Daneshmand S: Does presence of squamous
and glandular differentiation in urothelial carcinoma of the
bladder at cystectomy portend poor prognosis? An intensive
case-control analysis. Urol Oncol. 32:117–127. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Pereira JN, Reis JD, Braga I, Freitas R,
Moreira da Silva V, Magalhães S, Lobo F and Morais A: Variant
histologies of urothelial carcinoma: Does it change the survival
outcomes in patients managed with radical cystectomy? Arch Ital
Urol Androl. 94:138–143. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Xylinas E, Rink M, Robinson BD, Lotan Y,
Babjuk M, Brisuda A, Green DA, Kluth LA, Pycha A, Fradet Y, et al:
Impact of histological variants on oncological outcomes of patients
with urothelial carcinoma of the bladder treated with radical
cystectomy. Eur J Cancer. 49:1889–1897. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Antunes AA, Nesrallah LJ, Dall'Oglio MF,
Maluf CE, Camara C, Leite KR and Srougi M: The role of squamous
differentiation in patients with transitional cell carcinoma of the
bladder treated with radical cystectomy. Int Braz J Urol.
33:339–346. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Chen Q, Li L, Wang G, Hu J, Sun T and Fu
B: Do histological variants in urothelial carcinoma of the bladder
portend poor prognosis? A systematic review and meta-analysis.
Oncotarget. 8:48263–48271. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
WHO Classification of Tumours Editorial
Board, . Urinary and male genital tumours. WHO classification of
tumours. 5th edition. volume 8. International Agency for Research
on Cancer; Lyon: 2022, https://publications.iarc.fr/Book-And-Report-Series/Who-Classification-Of-Tumours/Urinary-And-Male-Genital-Tumours-2022April
24–2026
|
|
28
|
Cancer Genome Atlas Research Network, .
Comprehensive molecular characterization of urothelial bladder
carcinoma. Nature. 507:315–322. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Choi W, Porten S, Kim S, Willis D, Plimack
ER, Hoffman-Censits J, Roth B, Cheng T, Tran M, Lee IL, et al:
Identification of distinct basal and luminal subtypes of
muscle-invasive bladder cancer with different sensitivities to
frontline chemotherapy. Cancer Cell. 25:152–165. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Agrawal P, Rostom M, Alam R, Florissi I,
Biles M, Rodriguez K, Hahn NM, Johnson BA III, Matoso A, Smith A,
et al: Clinicopathologic and survival after cystectomy outcomes in
squamous cell carcinoma of the bladder. Clin Genitourin Cancer.
21:631–638.e1. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Gaisa NT, Braunschweig T, Reimer N,
Bornemann J, Eltze E, Siegert S, Toma M, Villa L, Hartmann A and
Knuechel R: Different immunohistochemical and ultrastructural
phenotypes of squamous differentiation in bladder cancer. Virchows
Arch. 458:301–312. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Moschini M, Sharma V, Dell'oglio P,
Cucchiara V, Gandaglia G, Cantiello F, Zattoni F, Pellucchi F,
Briganti A, Damiano R, et al: Comparing long-term outcomes of
primary and progressive carcinoma invading bladder muscle after
radical cystectomy. BJU Int. 117:604–610. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Kayama E, Kikuchi E, Fukumoto K, Shirotake
S, Miyazaki Y, Hakozaki K, Kaneko G, Yoshimine S, Tanaka N,
Takahiro M, et al: History of non-muscle-ınvasive bladder cancer
may have a worse prognostic ımpact in cT2-4aN0M0 bladder cancer
patients treated with radical cystectomy. Clin Genitourin Cancer.
16:e969–e976. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Vlaming M, Kiemeney LALM and van der
Heijden AG: Survival after radical cystectomy: Progressive versus
de novo muscle invasive bladder cancer. Cancer Treat Res Commun.
25:1002642020.PubMed/NCBI
|
|
35
|
Lin W, Pan X, Zhang C, Ye B and Song J:
Impact of age at diagnosis of bladder cancer on survival: A
surveillance, epidemiology, and end results-based study 2004–2015.
Cancer Control. 30:107327482311523222023. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Laymon M, Mosbah A, Hashem A, Mahmoud O,
Harraz AM, Elsawy AA and Abol-Enein H: Oncologic outcomes of
squamous cell carcinoma versus urothelial carcinoma with squamous
differentiation after radical cystectomy for bladder carcinoma.
Clin Genitourin Cancer. 20:148–154. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Alfred Witjes J, Max Bruins H, Carrión A,
Cathomas R, Compérat E, Efstathiou JA, Fietkau R, Gakis G, Lorch A,
Martini A, et al: European association of urology guidelines on
muscle-invasive and metastatic bladder cancer: Summary of the 2023
guidelines. Eur Urol. 85:17–31. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Freedman ND, Silverman DT, Hollenbeck AR,
Schatzkin A and Abnet CC: Association between smoking and risk of
bladder cancer among men and women. JAMA. 306:737–745. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Mungan NA, Kiemeney LA, van Dijck JA, van
der Poel HG and Witjes JA: Gender differences in stage distribution
of bladder cancer. Urology. 55:368–371. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Marks P, Soave A, Shariat SF, Fajkovic H,
Fisch M and Rink M: Female with bladder cancer: What and why is
there a difference? Transl Androl Urol. 5:668–682. 2016. View Article : Google Scholar : PubMed/NCBI
|
















