Introduction
It is generally accepted that schwannomas are
neurogenic tumours originating from Schwann cells (1). Schwannomas demonstrate a predilection
for the head, neck and extremities, and those originating in the
pelvis are rare, accounting for only 1–3% of all schwannomas
according to the relevant literature (2). In most cases, schwannomas are benign
lesions that typically do not require adjuvant therapy following
surgery and are associated with a low recurrence rate (3–5).
However, pelvic schwannomas are challenging to detect and difficult
to identify at an early stage due to the lack of specific clinical
manifestations and imaging features (6,7). A
definitive diagnosis requires histopathological confirmation,
characterized by the typical alternating hypercellular Antoni A
areas and hypocellular Antoni B areas composed of spindle cells,
along with strong and diffuse S-100 protein immunohistochemical
positivity (8). At present, reports
of pelvic schwannomas concomitant with colorectal cancer are
limited. In the two cases reported in the present study, colorectal
cancer was the primary diagnosis in both patients, and the lesions
were initially considered pelvic metastases preoperatively, with
schwannomas subsequently confirmed by postoperative pathological
examination. Misdiagnosis may lead to inaccurate tumour staging and
may result in missed opportunities for radical surgery. The present
report retrospectively analyses these cases, summarises the
findings, and proposes relevant strategies to improve future
clinical diagnosis.
Case report
Case 1
A 55-year-old female patient presented to the 900th
Hospital of PLA Joint Logistic Support Force (Fuzhou, China) with a
3-day history of constipation and a 1-day history of lower
abdominal pain and discomfort. Colonoscopy revealed a
circumferential mass located 17 cm from the anal verge, with
luminal obstruction preventing passage of the endoscope. Biopsy
pathology indicated high-grade atypical hyperplasia of the
adenomatous epithelium/intraepithelial neoplasia and carcinoma
(Fig. S1A) [all biopsy and
surgical specimens were fixed in 10% neutral buffered formalin at
room temperature for 24–48 h, routinely dehydrated and embedded in
paraffin. Serial sections (3-µm thick) were prepared, and
hematoxylin and eosin staining was performed at 28°C for 15 min.
Slides were examined using an OLYMPUS BX53 light microscope
(Olympus Corporation), with magnifications indicated in the
respective figure legends]. Whole-body 18F-fluorodeoxyglucose
(18F-FDG) positron emission tomography-computed
tomography (PET-CT) findings demonstrated: i) Localised thickening
at the rectosigmoid junction with slight hypermetabolism [maximum
standardised uptake value (SUVmax, 2.8), suggestive of
malignancy with possible extraserosal invasion; and ii) a
soft-tissue-density mass on the medial aspect of the right pelvic
wall, also with slight hypermetabolism (SUVmax, 2.8),
raising suspicion of metastasis (Fig.
1A). After multidisciplinary team (MDT) evaluation, the patient
was assigned a preliminary clinical stage of cT4NxM1 based on the
National Comprehensive Cancer Network (NCCN) Clinical Practice
Guidelines in Oncology for Colorectal Cancer (9,10), and
subsequently received six cycles of neoadjuvant therapy at 3-week
intervals. KRAS mutation testing had been performed prior to
treatment using the amplification refractory mutation system (ARMS)
fluorescence quantitative PCR method on a tumor biopsy specimen
obtained from the patient. However, the molecular pathology results
were not yet available at the time of treatment initiation. After a
thorough discussion of the potential benefits and risks with the
patient and her family, it was decided to proceed with neoadjuvant
therapy as scheduled. The initial regimen was FOLFOXIRI, comprising
irinotecan (200 mg intravenous infusion on day 1), oxaliplatin (120
mg intravenous infusion on day 1), calcium levofolinate (300 mg
intravenous infusion on day 1) and fluorouracil (3,000 mg
continuous intravenous infusion over 44 h). Given the subsequently
confirmed KRAS mutation, bevacizumab (300 mg intravenous infusion)
was added from the second cycle onward. Due to the occurrence of
Common Terminology Criteria for Adverse Events grade 2
myelosuppression (11), the regimen
was adjusted to FOLFOX (120 mg oxaliplatin intravenously on day
1,300 mg calcium levofolinate intravenously on day 1 and 500 mg
fluorouracil by intravenous bolus followed by a continuous infusion
of 3,000 mg over 44 h) for the remaining two cycles. Subsequent
pelvic CT indicated regression of both the intestinal lesion and
the right pelvic wall mass (Figs.
S1B-D and S2). The patient
then underwent radical resection of the sigmoid colon carcinoma
along with excision of the mass from the right pelvic wall.
Postoperative pathology confirmed moderately differentiated
adenocarcinoma of the sigmoid colon (Fig. 2A) with focal residual mucinous
adenocarcinoma involving the serosal membrane. Histological
examination of the right pelvic wall mass revealed alternating
Antoni A areas containing densely packed spindle cells and Antoni B
areas with sparsely distributed spindle cells (Fig. 2B and C), and immunohistochemical
staining revealed positivity for S-100 (Fig. 2D), establishing the diagnosis of a
schwannoma. Immunohistochemical staining was performed on surgical
specimens using the EliVision two-step method. Briefly, 3-µm thick
paraffin sections were dewaxed and rehydrated, followed by blocking
endogenous peroxidase activity with 3% hydrogen peroxide
(H2O2) at room temperature for 10 min.
Sections were incubated with a ready-to-use primary antibody
against S-100 protein [cat. no. B26011908; Hangzhou Bailing
(Biolynx) Biotechnology Co., Ltd.] at 28°C for 40 min, washed, and
subsequently incubated with a ready-to-use horseradish peroxidase
(HRP)-conjugated EnVision secondary antibody (cat. no. 2603020805B;
Fuzhou Maixin Biotechnology Development Co., Ltd.) at 28°C for 40
min. Immunoreactivity was visualized with 3,3′-diaminobenzidine
chromogen at 28°C for 15 min, followed by hematoxylin
counterstaining. Slides were observed under an OLYMPUS BX53 light
microscope.
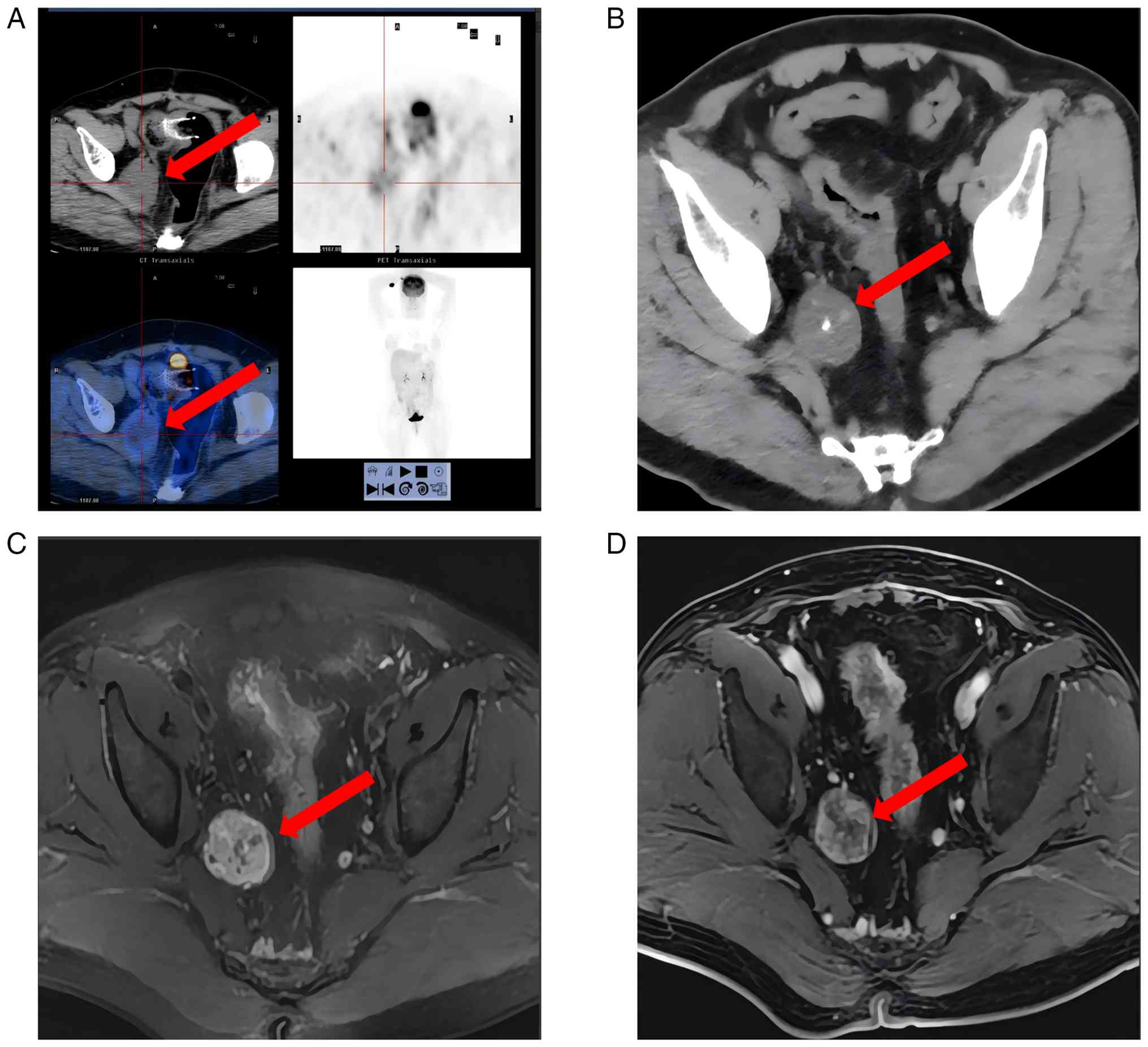 | Figure 1.PET-CT images of pelvic schwannoma in
case 1, and CT and MRI of pelvic schwannoma in case 2. (A) PET-CT
image (case 1): A round, low-density mass (CT value, 27 HU) (red
arrow) measuring 5.4×4.8 cm is evident on the right pelvic wall,
exhibiting clear margins, intact perimetrium, no apparent
haemorrhage, necrosis or calcification, homogeneous density, and no
significant enhancement on contrast-enhanced images. PET imaging
demonstrates slightly increased metabolism (SUVmax,
2.8). (B) Contrast-enhanced CT image (case 2): A rounded mass (red
arrow) with mixed density is observed on the right pelvic wall,
featuring internal calcifications and mild-to-moderate
heterogeneous enhancement after contrast administration. (C)
T2-weighted fat-suppressed MRI (case 2): A nodular mass (3.2×3.4
cm) (red arrow) is noted in the right pelvic obturator region,
appearing slightly hyperintense with heterogeneous signal
intensity. (D) Contrast-enhanced MRI (case 2): The mass (red arrow)
in the right pelvic obturator region displays heterogeneous
enhancement post-contrast, with scattered punctate low-signal areas
observed centrally. PET-CT, positron emission tomography-computed
tomography; MRI, magnetic resonance imaging; SUVmax,
maximum standardised uptake value. |
Following the operation, the patient underwent
postoperative adjuvant therapy at the 900th Hospital of PLA Joint
Logistic Support Force. Initially, two cycles of the CAPEOX regimen
were administered, comprising intravenous oxaliplatin (180 mg) on
day 1, and oral capecitabine at doses of 1,000 mg in the morning
and 1,500 mg in the evening on days 1–14, repeated every 3 weeks.
Subsequently, imaging follow-up suggested possible tumour
recurrence and metastasis. Therefore, the treatment was revised to
a 3-week cycle regimen consisting of oral capecitabine (1.5 g twice
daily, days 1–14), trifluridine-tipiracil (TAS102; 50 mg orally
twice daily, days 1–5) and bevacizumab (300 mg). All three agents
were administered on a 3-week cycle. To date, the patient has
completed five cycles of this revised regimen. Regular
postoperative follow-up has been conducted every 3 weeks, and at
the most recent evaluation, the patient remained in stable
condition.
ARMS fluorescence quantitative
PCR
Genomic DNA was isolated from 10-µm thick
formalin-fixed, paraffin-embedded (FFPE) tumor tissue sections
using the Nucleic Acid Extraction Kit (FFPE DNA; Amoy Diagnostics
Co., Ltd.) according to the manufacturer's instructions, and only
samples with a concentration >2 ng/µl and with an OD260/OD280
ratio between 1.8 and 2.0 as measured by a Nanodrop 2000
spectrophotometer (Thermo Fisher Scientific, Inc.) were used for
subsequent analysis. Detection of KRAS, NRAS, PIK3CA and BRAF
mutations was performed with the Human KRAS/NRAS/PIK3CA/BRAF Gene
Mutation Joint Detection Kit (fluorescence PCR; cat. no. 801.0173;
Amoy Diagnostics Co., Ltd.), which is based on the amplification
refractory mutation system ARMS fluorescent quantitative PCR. The
reaction mixture was prepared by combining 65.8 µl of extracted DNA
with 4.2 µl of the supplied KNPB Enzyme Mix, which contained a
thermostable DNA polymerase, specific forward and reverse primers,
fluorescent probes and internal control components; the sequences
of the forward and reverse primers are proprietary to the kit and
were not disclosed by the manufacturer. After brief vortexing and
centrifugation, 5 µl of the mixture was dispensed into each tube of
the 12-strip PCR array. Amplification and fluorescence detection
were carried out on an ABI 7500 Real-Time PCR System with the
following dye settings: Reporter dye, FAM and VIC; quencher dye,
TAMRA; passive reference, nONE. Thermal cycling conditions were as
follows: Initial denaturation at 95°C for 5 min (1 cycle); followed
by 15 cycles of denaturation at 95°C for 25 sec, annealing at 64°C
for 20 sec and extension at 72°C for 20 sec; then 31 cycles of
denaturation at 93°C for 25 sec, annealing at 60°C for 35 sec
(fluorescence signal acquisition during this step) and extension at
72°C for 20 sec. No agarose gel electrophoresis was performed, as
the assay directly monitors amplicon accumulation via real-time
fluorescence. Mutation status was assigned according to the
manufacturer's cut-off criteria: A FAM Cq value ≤26 in a
mutation-specific reaction tube, with a valid VIC (internal
control) signal, was considered positive for the corresponding
mutation; a FAM Cq value >26 or undetermined was considered
negative. The positive control was required to yield Cq values
<20 for both FAM and VIC, and the no-template control had to be
free of FAM amplification.
Case 2
A 73-year-old man was admitted to the 900th Hospital
of PLA Joint Logistic Support Force with an 8-year history of
intermittent haematochezia. Colonoscopy revealed an irregular mass
located 15–19 cm from the anal verge, occupying approximately
one-half of the intestinal lumen, with surface erosion and
necrosis; biopsy pathology suggested moderately differentiated
adenocarcinoma (Fig. S3A). Pelvic
CT findings indicated: i) Sigmoid colon cancer with metastasis to
the regional mesenteric lymph nodes; and ii) a mass with
calcification adjacent to the iliac vessels in the right pelvic
wall peritoneal region, suggestive of a tumour, with metastatic
disease not excluded (Fig. 1B).
Pelvic magnetic resonance imaging (MRI) demonstrated: i) Sigmoid
colon cancer with regional mesenteric lymph node metastasis; and
ii) a mass on the right pelvic wall, with metastasis considered
likely (Fig. 1C and D). MDT
discussion determined the clinical stage to be
T3N+M1 based on the NCCN Clinical
Practice Guidelines in Oncology for Colorectal Cancer (9,10). The
patient underwent six cycles of neoadjuvant therapy consisting of
the CAPEOX regimen combined with bevacizumab, administered every 3
weeks for a total of 18 weeks. The specific regimen included
oxaliplatin (200 mg intravenous infusion on day 1), oral
capecitabine at doses of 1,000 mg in the morning and 1,500 mg in
the evening on days 1–14 and bevacizumab (300–400 mg intravenous
infusion on day 1). After six cycles of neoadjuvant therapy,
follow-up evaluation showed that the colonic lesion had decreased
in size, whereas the right pelvic wall mass remained largely
unchanged (Figs. S4 and S5). Subsequently, the patient underwent a
radical resection of sigmoid colon cancer and an excision of the
right pelvic wall mass. Postoperative pathology confirmed the
initial diagnosis of moderately differentiated adenocarcinoma of
the sigmoid colon (Fig. S3B);
following neoadjuvant therapy, only scattered residual tumour nests
were identified after extensive sampling. Histopathological
examination of the right pelvic wall mass again revealed
alternating Antoni A and B areas, with immunohistochemical
positivity for S-100, confirming a schwannoma (Fig. S3C and D). No adjuvant therapy was
administered postoperatively. Monthly telephone follow-ups
indicated stable clinical status, and regular clinical evaluations
were performed at a local hospital.
Discussion
According to the latest 2022 GLOBOCAN estimates from
the International Agency for Research on Cancer, the global burden
of colorectal cancer has increased significantly over the past
decade, with absolute increases in new cases and deaths of 41.5 and
34.7%, respectively (12,13). Previous studies (14,15)
have indicated that >20% of patients with colorectal cancer
present with distant metastases to sites such as the liver, lung,
peritoneum and ovary at the initial diagnosis. Approximately
one-quarter of patients exhibit peritoneal metastases, and these
patients typically have a poor prognosis. Furthermore, colorectal
cancer represents a common primary origin for ovarian metastases
(16,17).
Schwannomas originate from well-differentiated
Schwann cells, and the vast majority of these tumours are benign
(1). Malignant schwannomas are rare
and are often associated with neurofibromatosis (18). Pelvic schwannomas are uncommon
clinically, and some researchers (3) have proposed that they originate from
the peripheral nerve sheath of the sacral nerve or the hypogastric
plexus. A solitary, intact and well-defined capsule is
characteristic of schwannomas; however, pelvic schwannomas often
demonstrate atypical presentations, including cystic degeneration,
haemorrhage and calcification (3,8). Due
to their slow growth and non-specific clinical symptoms, pelvic
schwannomas are challenging to detect at an early stage; they
typically become noticeable only when compression or invasion of
adjacent tissues and organs causes corresponding symptoms (2). Imaging studies indicate that pelvic
schwannomas frequently appear as well-defined, hypodense lesions on
CT scans (19). Compared with CT,
MRI offers superior visualisation of pelvic masses, demonstrating
higher sensitivity and specificity for detecting schwannomas
(20,21). Clinical studies (22,23)
have shown schwannomas to typically exhibit hypointensity on
T1-weighted imaging (T1WI), hyperintensity on T2WI, and
heterogeneous enhancement following contrast administration on
T1WI; these features are consistent with the MRI findings observed
in the cases of the present study. Notably, scholarly opinions
differ on the diagnostic certainty achievable by preoperative
imaging alone. Tong et al (24) suggested that confirmation of the
association between the pelvic mass and peripheral nerves or blood
vessels through imaging is critical for diagnosing schwannomas. By
contrast, Wu et al (7)
concluded that imaging of pelvic schwannomas lacks specificity,
making differentiation from other pelvic masses difficult. In
pathological assessments, apart from the specific
immunohistochemical marker S-100, positive staining for
neuron-specific enolase and microfilament proteins has also been
reported to support the diagnosis of schwannomas (25–27).
Microscopically, schwannomas are composed of densely packed
spindle-shaped cells (Antoni A areas) and loosely arranged tumour
cells (Antoni B areas) (8,28). Currently, surgical resection is the
optimal treatment for schwannomas (7). An intercontinental multicenter study
(29) recommended MDT discussions
before pelvic schwannoma resection to determine whether local or
radical resection is appropriate, considering both the patient's
postoperative prognosis and the anatomical relationships with
surrounding nerves and blood vessels. Damage to pelvic peripheral
nerves and vessels during surgery may lead to neurological
impairment (8,30). In the follow-up described for case
1, the patient presented with localized postoperative neurological
dysfunction, manifested as numbness, pain and cold sensory
paresthesia in the right lower extremity. Consequently,
preoperative MDT evaluation is particularly important in managing
pelvic schwannomas.
Common to both cases reported in the present study
was the preoperative misdiagnosis of a pelvic schwannoma as a
metastatic lesion originating from colorectal cancer. The reasons
are as follows: First, schwannomas typically occur in the head,
neck and limbs, with pelvic schwannomas being rare (31). Second, symptoms associated with
pelvic schwannomas lack specificity and vary according to the
lesion's size and location (27).
The absence of specific clinical manifestations in both cases
described within the present study further complicated the
preoperative diagnosis. Third, imaging findings in pelvic
schwannomas, which often exhibit rich blood supply and atypical
features such as cystic degeneration, liquefaction necrosis and
calcification, are easily mistaken for malignant pelvic tumours
without histopathological confirmation (3,32,33).
Malignant ovarian tumours commonly present as mixed cystic-solid,
solid or cystic masses on CT scans, and MRI may reveal cystic-solid
lesions or nodular structures similar to schwannomas, with high
signal intensity on diffusion-weighted imaging (DWI) and
heterogeneous enhancement following contrast administration
(34–36). Pelvic malignancies, including
leiomyosarcoma, seminoma, fallopian tube carcinoma and
extra-gastrointestinal stromal tumours, also share imaging
characteristics with schwannomas (37–42).
Advanced MRI techniques, including contrast-enhanced magnetic
resonance neurography (CE-MRN) and DWI, offer distinct advantages
over conventional MRI in identifying neurogenic tumours in the
pelvic region (43–45). However, CE-MRN exhibits lower
spatial resolution compared with conventional MRI, limiting its
ability to adequately evaluate tumour microstructure, function or
metabolism (43). In addition,
schwannomas frequently present with cystic degeneration and
necrosis, leading to pseudo-limited diffusion on DWI (46). Therefore, these techniques should be
combined with other imaging modalities for more accurate
assessment. Additionally, 18F-FDG is a non-specific
tracer that can exhibit increased uptake not only in malignant
tumours but also in some benign lesions, leading to false-positive
results (47–49). In case 1 of the present study,
preoperative 18F-FDG PET-CT also demonstrated mild
hypermetabolism. Boré et al (49) argued that false-positive
18F-FDG findings could influence preoperative diagnosis
and treatment decisions in patients with schwannomas. Currently,
pathological examination following complete surgical resection
remains the gold standard for diagnosing schwannomas.
Upon reviewing the imaging data of the two pelvic
mass cases presented within the current study, although no
characteristic imaging features were identified, both lesions were
located in anatomical regions along the pelvic wall or obturator
nerve plexus, suggesting the possibility of schwannomas. In
addition, when a pelvic mass demonstrates imaging features such as
the target sign and nerve entry-exit sign with well-defined
margins, schwannoma should also be included in the routine
differential diagnosis (43). A
previous report has described a case in which a peritoneal mass was
misdiagnosed as a metastatic malignant lesion. Similar to cases 1
and 2 in the present report, after MDT discussion, no preoperative
biopsy was performed, and the diagnosis of schwannoma was
ultimately confirmed by postoperative pathological examination
(50). This has prompted
consideration of how the MDT model could be further improved in
preoperative diagnostic decision-making. Preoperative biopsy is
necessary; however, preoperative biopsy of schwannomas is prone to
sampling error due to tumour cell degeneration and pleomorphism,
which may lead to misdiagnosis (51). Therefore, the involvement of
subspecialty radiologists (such as musculoskeletal or pelvic
radiologists) in multidisciplinary diagnosis and treatment
processes for pelvic masses is essential for providing specialised
imaging consultations. Additionally, greater emphasis should be
placed on comparing imaging morphology, lesion invasion extent and
preoperative biopsy histopathological characteristics during MDT
discussions to improve the accuracy of preoperative assessments
(52,53). Although pelvic schwannomas have
previously been misdiagnosed as malignant tumours (54,55),
most existing studies have not systematically summarised the key
points for differentiating pelvic schwannomas from pelvic
metastatic lesions of colorectal cancer. Furthermore, no
standardised clinical diagnosis and treatment protocol has been
established for patients with colorectal cancer complicated by
pelvic masses. Based on the diagnostic experience from the present
cases, we believe it is clinically valuable to establish a clear,
practical and systematic diagnostic pathway and optimise MDT
evaluations for patients with colorectal cancer presenting with
pelvic masses. Based on prior literature, the present study
analysed the distinguishing features between pelvic schwannomas and
colorectal cancer pelvic metastatic lesions in terms of growth
patterns, associations with neurovascular structures and imaging
characteristics (Table I) (4,19,22,43,56–61).
Pelvic schwannomas typically exhibit slow growth with clear
margins, originate from the nerve sheath (sacral or hypogastric
plexus), demonstrate the ‘entering and exiting nerve sign’ and lack
vascular invasion. Radiologically, schwannomas appear as
well-defined hypodense masses on non-contrast CT, demonstrate
T1-hypointensity and T2-hyperintensity on MRI (occasionally
exhibiting the ‘target sign’ or ‘fat-splitting sign’), and show
variable metabolic activity on PET-CT. By contrast, colorectal
cancer pelvic metastases grow rapidly and invasively with
indistinct boundaries, initially lack direct neural involvement
(with potential sacral plexus involvement at advanced stages), and
EMVI, vascular encirclement and lymph node metastasis. Imaging
typically reveals ill-defined soft-tissue masses with heterogeneous
density and uneven enhancement on CT, T1-hypointensity,
T2-isointensity and DWI hyperintensity on MRI, along with markedly
hypermetabolic activity on PET-CT (4,19,22,43,56–61).
In addition, we propose a standardised diagnostic and therapeutic
workflow for patients with colorectal cancer and pelvic masses of
unknown origin (Fig. 3), aiming to
provide guidance and reference for clinical decision-making in
similar cases. This workflow initiates with clinical screening of
patients with who present with pelvic masses of uncertain etiology.
High-resolution multiparametric pelvic MRI is employed to clarify
lesion origin, invasive extent, and anatomical relationships
between pelvic lesions and the rectosigmoid colon. Patients are
then stratified into two treatment pathways based on the spatial
continuity between lesions and the intestinal tract: Masses
adjacent to the bowel indicate local infiltration by primary
colorectal cancer, necessitating systematic examinations for
accurate tumour staging. For isolated pelvic lesions unrelated to
the colorectum, preliminary MDT consultation should occur first,
followed by image-guided needle biopsy after excluding
contraindications, combined with whole-body staging assessments and
differential diagnosis of common pelvic tumours. A subsequent
multidisciplinary consensus discussion is then held to formulate
personalized therapeutic regimens.
 | Table I.Differential diagnosis between pelvic
schwannomas and pelvic metastases originating from colorectal
cancer. |
Table I.
Differential diagnosis between pelvic
schwannomas and pelvic metastases originating from colorectal
cancer.
| Feature | Pelvic
schwannoma | Pelvic metastasis
from colorectal cancer | (Refs.) |
|---|
| Growth pattern | Slow, expansive
growth with clear margins and. encapsulation | Rapid, invasive
growth with. indistinct boundaries, infiltrating surrounding
tissues | (4,56) |
| Relationship with
nerves and blood vessels | Arises from the
nerve sheath (sacral/hypogastric plexus), showing the ‘entering and
exiting nerve sign’, and displaces vessels without invasion. | No direct neural
involvement initially; advanced stages may involve the sacral
plexus. EMVI is common, with vessels encircling the lesion and
lymph node metastasis. | (57–59) |
| Imaging
findings | CT: A well-defined
hypodense mass on non-contrast CT, with either homogeneous or
heterogeneous attenuation. MRI: Hypointense on T1WI and
hyperintense on T2WI, with hallmark features including the ‘target
sign’, ‘entering and exiting nerve sign’ and ‘fat-splitting sign’
observed in a subset of cases. PET-CT: Highly variable metabolic
activity, with a mean SUVmax of 5.4±2.7. | CT: A soft-tissue
mass with indistinct boundaries, heterogeneous density and uneven
enhancement. MRI: Hypointense on T1WI, isointense on T2WI and
hyperintense on DWI. PET-CT: Demonstrates significant
hypermetabolic activity. | (19,22,43,60,61) |
In conclusion, the current study presents two cases
of pelvic schwannomas initially misdiagnosed as colorectal cancer
metastases. This misdiagnosis underscores the importance of
preoperative differential diagnosis in evaluating pelvic masses.
Additionally, the diagnostic challenge is further complicated by
the non-specific clinical and imaging features of pelvic
schwannomas. Postoperative pathological examination remains
essential for a definitive diagnosis. The present case report and
associated retrospective analysis highlight the necessity for
clinicians to consider pelvic schwannomas when investigating the
origin of pelvic masses.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
SW made substantial contributions to the conception
and design of the study, acquisition, organization and analysis of
clinical data, as well as drafting the initial manuscript. JL
participated in the critical revision of the manuscript for
important intellectual content, provided academic guidance on the
study design and data interpretation, and gave final approval of
the version to be published. KZ and XL were involved in the
identification of study cases, acquisition and preliminary analysis
of clinical data, coordination of patient follow-up, and
participated in the discussion of individual patient treatment
plans. FX and JY made substantial contributions to the acquisition,
analysis and professional interpretation of imaging data and
pathological specimen images, provided key imaging and pathological
evidence for the diagnosis and treatment of cases, and participated
in the revision of the manuscript related to imaging and pathology.
All authors have made substantial intellectual contributions to the
study. All authors read and approved the final manuscript, and
agreed to be accountable for all aspects of the work to ensure that
any questions related to the accuracy or integrity of the work are
appropriately investigated and resolved. SW and JL confirm the
authenticity of all the raw data.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patients for the publication of their clinical data and
accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Lee SH, Lee SJ and Lee CS: A rare case of
pelvic concurrent schwannoma(neurilemmoma) and neurofibroma. Asian
J Surg. 45:1084–1085. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Bulot AL, Nyangoh Timoh K, Bretonnier M,
Lavoué V, Morandi X and Levêque J: Case report: Dyspareunia as a
symptom of a pelvic schwannoma. J Gynecol Obstet Hum Reprod.
51:1024022022. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Dau MHT, Tran MTT, Nguyen HQ, Vo KYT,
Nguyen TTT, Hoang TH, Hoang VT and Hoang DT: Pelvic schwannoma in
an adult male. Acta Radiol Open. 11:205846012211028222022.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kawahori T, Mukai S, Saito Y, Nishida T,
Fukuda T and Ohdan H: A rare case of giant pelvic retroperitoneal
schwannoma. Radiol Case Rep. 19:5738–5743. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Santos AJ, Duarte L, Santos SC and
Casimiro C: A 68-year-old woman presenting with recurrent abdominal
pain and a diagnosis of a presacral retroperitoneal benign
schwannoma that mimicked an ovarian tumor on pelvic magnetic
resonance imagining. Am J Case Rep. 23:e9359852022. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kalagi D, Bakir M, Alfarra M, Aborayya A
and Anwar I: Two unusual presentations of presacral schwannoma; a
case series. Int J Surg Case Rep. 61:165–168. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Wu X, Meng H, Fan Q, Qi Z and Pan W: Image
features and clinical analysis of retroperitoneal pelvic
schwannoma: A case report. BMC Neurol. 24:2302024. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Zhou S, Wan S, Li L, Dong W, Ma X, Chu H
and Zhong Y: Rare retroperitoneal giant sacral schwannoma: A case
report. Oncol Lett. 27:2612024. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Benson AB, Venook AP, Adam M, Chang G,
Chen YJ, Ciombor KK, Cohen SA, Cooper HS, Deming D, Garrido-Laguna
I, et al: Colon cancer, version 3.2024, NCCN clinical practice
guidelines in oncology. J Natl Compr Canc Netw. 22:e2400292024.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Amin MB, Edge SB, Greene FL, Byrd DR,
Brookland RK, Washington MK, Gershenwald JE, Compton CC, Hess KR,
Sullivan DC, et al: AJCC cancer staging manual. 8th ed. Springer
International Publishing; Cham: 2017
|
|
11
|
National Cancer Institute, . Common
Terminology Criteria for Adverse Events (CTCAE) Version5.0.
National Institutes of Health; Bethesda, MD: 2017
|
|
12
|
No authors listed. Global cancer burden
growing, amidst mounting need for services. Saudi Med J.
45:326–327. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Bray F, Laversanne M, Sung H, Ferlay J,
Siegel RL, Soerjomataram I and Jemal A: Global cancer statistics
2022: GLOBOCAN estimates of incidence and mortality worldwide for
36 cancers in 185 countries. CA Cancer J Clin. 74:229–263.
2024.PubMed/NCBI
|
|
14
|
He K, Wang Z, Luo M, Li B, Ding N, Li L,
He B, Wang H, Cao J, Huang C, et al: Metastasis organotropism in
colorectal cancer: Advancing toward innovative therapies. J Transl
Med. 21:6122023. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Vatandoust S, Price TJ and Karapetis CS:
Colorectal cancer: Metastases to a single organ. World J
Gastroenterol. 21:11767–11776. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Franko J, Shi Q, Meyers JP, Maughan TS,
Adams RA, Seymour MT, Saltz L, Punt CJA, Koopman M, Tournigand C,
et al: Prognosis of patients with peritoneal metastatic colorectal
cancer given systemic therapy: An analysis of individual patient
data from prospective randomised trials from the analysis and
research in cancers of the digestive system (ARCAD) database.
Lancet Oncol. 17:1709–1719. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Franko J, Shi Q, Goldman CD, Pockaj BA,
Nelson GD, Goldberg RM, Pitot HC, Grothey A, Alberts SR and Sargent
DJ: Treatment of colorectal peritoneal carcinomatosis with systemic
chemotherapy: A pooled analysis of north central cancer treatment
group phase III trials N9741 and N9841. J Clin Oncol. 30:263–267.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yao C, Zhou H, Dong Y, Alhaskawi A, Hasan
Abdullah Ezzi S, Wang Z, Lai J, Goutham Kota V, Hasan Abdulla Hasan
Abdulla M and Lu H: Malignant peripheral nerve sheath tumors:
Latest concepts in disease pathogenesis and clinical management.
Cancers (Basel). 15:10772023. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Nasu K, Arima K, Yoshimatsu J and Miyakawa
I: CT and MRI findings in a case of pelvic schwannoma. Gynecol
Obstet Invest. 46:142–144. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Elsherif SB, Agely A, Gopireddy DR,
Ganeshan D, Hew KE, Sharma S and Lall C: Mimics and pitfalls of
primary ovarian malignancy imaging. Tomography. 8:100–119. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Schraepen C, Donkersloot P, Duyvendak W,
Plazier M, Put E, Roosen G, Vanvolsem S, Wissels M and Bamps S:
What to know about schwannomatosis: A literature review. Br J
Neurosurg. 36:171–174. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Conde Vasco I, Martins Pereira G, Ferreira
J and Cunha TM: Schwannoma mimicking ovarian malignancy. Radiol
Case Rep. 17:4308–4313. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Crist J, Hodge JR, Frick M, Leung FP, Hsu
E, Gi MT and Venkatesh SK: Magnetic resonance imaging appearance of
schwannomas from head to toe: A pictorial review. J Clin Imaging
Sci. 7:382017. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Tong RSK, Collier N and Kaye AH: Chronic
sciatica secondary to retroperitoneal pelvic schwannoma. J Clin
Neurosci. 10:108–111. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Zaresharifi N, Karimzadhagh S, Ebrahimian
R, Reihanian Z, Abbaspour E, Karimian P and Taheri Talesh J:
Successful management of a giant retroperitoneal ancient schwannoma
mimicking malignant tumors: A case report and literature review.
Ann Med Surg (Lond). 85:6279–6284. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Chen W, Dang C, Zhu K and Li K:
Preoperative management of giant retroperitoneal schwannoma: A case
report and review of the literature. Oncol Lett. 11:4030–4034.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Machairiotis N, Zarogoulidis P, Stylianaki
A, Karatrasoglou E, Sotiropoulou G, Floreskou A, Chatzi E, Karamani
A, Liapi G, Papakonstantinou E, et al: Pelvic schwannoma in the
right parametrium. Int J Gen Med. 6:123–126. 2013.PubMed/NCBI
|
|
28
|
Leclerc A, Lebreton G, Huet A, Alves A and
Emery E: Management of giant presacral schwannoma. Clinical series
and literature review. Clin Neurol Neurosurg. 200:1064092021.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Transatlantic Australasian Retroperitoneal
Sarcoma Working Group, : Intercontinental collaborative experience
with abdominal, retroperitoneal and pelvic schwannomas. Br J Surg.
107:452–463. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Cho DH: Retroperitoneal schwannoma
misdiagnosed as an ovarian malignancy. BMJ Case Rep.
2018:bcr20182255022018. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Attia H, Agboola JO, Seong G, Thida A,
Chiu E and Agaronov M: Synchronous pelvic schwannoma with
metastatic prostate cancer: A rare case and pathology review.
Cureus. 16:e523562024.PubMed/NCBI
|
|
32
|
Hughes MJ, Thomas JM, Fisher C and
Moskovic EC: Imaging features of retroperitoneal and pelvic
schwannomas. Clin Radiol. 60:886–893. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Jindal T, Mukherjee S, Kamal MR, Sharma
RK, Ghosh N, Mandal SN, Das AK and Karmakar D: Cystic schwannoma of
the pelvis. Ann R Coll Surg Engl. 95:e1–e2. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Bourgioti C, Konidari M and Moulopoulos
LA: Manifestations of ovarian cancer in relation to other pelvic
diseases by MRI. Cancers (Basel). 15:21062023. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Chen Z, Liu Z, Yang J, Sun J and Wang P:
The clinicopathological characteristics, prognosis, and CT features
of ovary metastasis from colorectal carcinoma. Transl Cancer Res.
10:3248–3258. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Foti PV, Attinà G, Spadola S, Caltabiano
R, Farina R, Palmucci S, Zarbo G, Zarbo R, D'Arrigo M, Milone P and
Ettorre GC: MR imaging of ovarian masses: Classification and
differential diagnosis. Insights Imaging. 7:21–41. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Marko J and Wolfman DJ: Retroperitoneal
leiomyosarcoma from the radiologic pathology archives.
Radiographics. 38:1403–1420. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Marko J, Wolfman DJ, Aubin AL and
Sesterhenn IA: Testicular seminoma and its mimics: From the
radiologic pathology archives. Radiographics. 37:1085–1098. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Veloso Gomes F, Dias JL, Lucas R and Cunha
TM: Primary fallopian tube carcinoma: Review of MR imaging
findings. Insights Imaging. 6:431–439. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Dande A, Pajai S, Acharya N, Joshi KS,
Patel DJ and Gupta A: Gastrointestinal stromal tumors mimicking
ovarian mass: A case report. Cureus. 16:e583202024.PubMed/NCBI
|
|
41
|
Arellano-Gutiérrez G, Martínez-Aldrete LF,
Pérez-Fabián A and Maldonado-García EL: Primary
extra-gastrointestinal stromal tumor (EGIST) of the mesentery: Case
report and review of literature. Ann Med Surg (Lond). 60:480–483.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Watal P, Brahmbhatt SG, Thoriya PJ and
Bahri NU: Retroperitoneal extragastrointestinal stromal tumor:
Radiologic pathologic correlation. J Clin Imaging Sci. 4:342014.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Wu W, Ding Y, Su Y, Wang Y, Liu T, Zhang
Z, Liu D, Li C, Zheng C and Wang L: Novel MRI signs for
differentiating neurogenic and non-neurogenic peripheral nerve
tumors: Insights from contrast-enhanced magnetic resonance
neurography. Eur J Radiol. 183:1118942025. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Ristow I, Apostolova I, Kaul MG, Stark M,
Zapf A, Schmalhofer ML, Mautner VF, Farschtschi S, Adam G, Bannas
P, et al: Discrimination of benign, atypical, and malignant
peripheral nerve sheath tumours in neurofibromatosis type
1-intraindividual comparison of positron emission computed
tomography and diffusion-weighted magnetic resonance imaging.
EJNMMI Res. 14:1272024. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Yuh EL, Jain Palrecha S, Lagemann GM,
Kliot M, Weinstein PR, Barbaro NM and Chin CT: Diffusivity
measurements differentiate benign from malignant lesions in
patients with peripheral neuropathy or plexopathy. AJNR Am J
Neuroradiol. 36:202–209. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Said EN, Mohamed DHE, Abdellatif RS,
Nashed GA and Beshir MMR: Radiological pitfalls in DWI in
characterization of primary retroperitoneal masses. Med. J. Cairo
Univ. 91:245–257. 2023.
|
|
47
|
Long NM and Smith CS: Causes and imaging
features of false positives and false negatives on F-PET/CT in
oncologic imaging. Insights Imaging. 2:679–698. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Zhu Y, Wu J, Wang Y, Geng J and Zhang C:
Presacral benign schwannoma mimics malignancy on 18F-FDG and
68Ga-FAPI PET/CT. Clin Nucl Med. 47:277–278. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Boré P, Descourt R, Ollivier L, Le Roux PY
and Abgral R: False positive 18F-FDG positron emission tomography
findings in schwannoma-A caution for reporting physicians. Front
Med (Lausanne). 5:2752018. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Pan S, Wang P, Chen Z, Liu Y and Zhou Z:
Retroperitoneal schwannoma mimicking a metastatic lymph node of
renal clear cell carcinoma: A case report. Front Neurol.
15:14502172024. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Maidarti M, Wibawa YS, Garinasih PD,
Hellyanti T, Harzif AK and Nuryanto KH: Rare case of pelvic
schwannoma mimicking intra-ligamenter uterine fibroid: A case
report. Int J Surg Case Rep. 96:1073272022. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Jeon SK, Kim SH, Shin CI, Yoo J, Park KJ,
Ryoo SB, Park JW, Kim TY, Han SW, Lee DW, et al: Role of dedicated
subspecialized radiologists in multidisciplinary team discussions
on lower gastrointestinal tract cancers. Korean J Radiol.
23:732–741. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Beaman FD, Kransdorf MJ and Menke DM:
Schwannoma: Radiologic-pathologic correlation. Radiographics.
24:1477–1481. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Chou D, Zahid A and Cheng E: Lateral
pelvic wall schwannoma: A case report and literature review.
Cureus. 17:e995692025.PubMed/NCBI
|
|
55
|
Bai J, Kleyser-Sugrue K, Nerenstone SR and
Welch JP: Synchronous colonic adenocarcinoma and pelvic schwannoma.
Conn Med. 75:93–95. 2011.PubMed/NCBI
|
|
56
|
El Asmar A, Demetter P, Fares F, Sclafani
F, Hendlisz A, Donckier V, Vermeulen P and Liberale G: The
prognostic value of distinct histological growth patterns of
colorectal peritoneal metastases: A pilot study. Ann Surg Oncol.
30:3320–3328. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Mazzola CR, Power N, Bilsky MH, Robert R
and Guillonneau B: Pudendal schwannoma: A case report and
literature review. Can Urol Assoc J. 8:E199–E203. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Richart V, Castillo-Fortuño A and
Garcia-Diez AI: Advance imaging with magnetic resonance neurography
for the diagnosis of unusual extensive pelvic perineural spread in
colorectal cancer: A case report. J Med Case Rep. 19:1912025.
View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Chandramohan A, Mittal R, Dsouza R,
Yezzaji H, Eapen A, Simon B, John R, Singh A, Ram TS, Jesudason MR,
et al: Prognostic significance of MR identified EMVI, tumour
deposits, mesorectal nodes and pelvic side wall disease in locally
advanced rectal cancer. Colorectal Dis. 24:428–438. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Dewey BJ, Howe BM, Spinner RJ, Johnson GB,
Nathan MA, Wenger DE and Broski SM: FDG PET/CT and MRI features of
pathologically proven schwannomas. Clin Nucl Med. 46:289–296. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Cervantes A, Adam R, Roselló S, Arnold D,
Normanno N, Taïeb J, Seligmann J, De Baere T, Osterlund P, Yoshino
T, et al: Metastatic colorectal cancer: ESMO clinical practice
guideline for diagnosis, treatment and follow-up. Ann Oncol.
34:10–32. 2023. View Article : Google Scholar : PubMed/NCBI
|
















