Introduction
NSCLC accounts for ~85% of all lung cancer cases and
is the leading cause of cancer-related mortality worldwide, with an
estimated 2.2 million new cases and 1.8 million deaths annually
(1). Neoadjuvant therapy has become
an established method for the management of initially unresectable
stage IIIA and stage IV non-small cell lung carcinoma (NSCLC) at
the time of diagnosis (2,3). It is particularly beneficial for
achieving tumor downstaging in cases with single-station N2 lymph
node involvement or large tumors associated with arterial or venous
invasion. Accumulating evidence has indicated that, particularly
with the addition of immunotherapy to conventional chemotherapy
(CT) regimens, neoadjuvant treatment improves survival and
resectability while also enhancing pathologic response rates
(4,5).
To address this need, the International Association
for the Study of Lung Cancer (IASLC) has published comprehensive
multidisciplinary recommendations for the pathologic evaluation of
lung cancer resection specimens following neoadjuvant therapy
(5). These guidelines emphasize
meticulous identification and sampling of the tumor bed,
quantification of residual viable tumor (RVT) and uniform
definitions for major pathologic response (mPR), defined as ≤10%
RVT and pathologic complete response (pCR), defined as 0% RVT,
irrespective of treatment modality.
However, the addition of immunotherapy to
conventional CT has highlighted the need to incorporate new
regression patterns into tumor regression grading systems. Features
such as proliferative fibrosis, neovascularization, dense
lymphocytic infiltrates, foamy macrophages and stromal alterations
have led to the development of a quantitative scoring system
referred to as the immune-related pathologic response criteria
(irPRC) (6).
The density of tumor-infiltrating lymphocytes (TILs)
within the tumor microenvironment has emerged as an important
parameter following neoadjuvant therapy (7,8) Tumor
cells exhibit enhanced glycolytic activity, resulting in increased
lactate production and accumulation within the tumor
microenvironment, which has been shown to suppress T-cell function
and promote immunosuppression. In this context, tumor-derived
metabolic alterations, particularly lactate accumulation, have been
shown to suppress T-cell function and promote an immunosuppressive
microenvironment (9). The irPRC
system has been applied across multiple tumor types, including
NSCLC, melanoma, urothelial carcinoma and breast cancer, in
patients treated with PD-1/PD-L1 inhibitors (6,10–12).
Pivotal clinical trials have further highlighted the
importance of standardized pathologic assessment. The phase III
CheckMate 816 trial (trial no. NCT02998528) demonstrated that the
addition of nivolumab to platinum-doublet chemotherapy
significantly increases both mPR and pCR rates compared with
chemotherapy alone, while maintaining surgical safety and
feasibility (13). Similarly, the
Lung Cancer Mutation Consortium 3 (LCMC3) trial (trial no.
NCT02927301), which evaluated neoadjuvant atezolizumab monotherapy,
reported meaningful pathological responses, including 20% mPR and
7% pCR, supporting the biological activity of single-agent
immunotherapy in early-stage NSCLC (14). These results underscore the ability
of immunotherapy to induce deeper tumor regression compared with
traditional cytotoxic treatment.
The pathologist serves a central role in the
quantitative assessment of these responses. Distinguishing viable
tumor from therapy-induced stromal changes, defining the boundaries
of the tumor bed and assessing the extent of necrosis can present
challenges in routine practice. Therefore, the application of
standardized criteria is important (15). Tumor bed mapping and the
identification of immune-mediated regression features, such as
proliferative fibrosis, neovascularization, dense lymphocytic
infiltrate and foamy macrophages, are required for accurate
interpretation of post-treatment resection specimens (16).
Comparative studies have provided additional insight
into histologic patterns associated with different neoadjuvant
treatment modalities, with a number of studies having suggested
that, compared with CT alone, chemo-immunotherapy (CIT) may be
associated with more pronounced fibrotic remodeling, denser TIL
infiltration, lower viable tumor burden and a reduced frequency of
adverse prognostic features, such as spread through air spaces
(STAS) and pleural invasion (4,17–19).
Collectively, the existing literature demonstrates
that standardized evaluation integrating both IASLC and irPRC
principles is important in accurately quantifying therapeutic
effect, predicting clinical outcomes and enabling comparison across
neoadjuvant trials. Despite notable progress, real-world studies
comparing histologic response patterns between CT and CIT remain
limited, particularly regarding the association between fibrosis,
inflammation, necrosis, STAS and survival outcomes. Therefore, the
present study aimed to address this gap by systematically
evaluating pathologic response and regression features in NSCLC
resection specimens following neoadjuvant therapy using both IASLC
and irPRC frameworks. Proportional assessment of residual tumor,
fibrosis, inflammation, necrosis and the tumor bed may thus reveal
differences in treatment response between CT and CIT protocols.
Materials and methods
Patient selection
The present retrospective study included resected
lung cancer specimens from patients who underwent neoadjuvant CT or
CIT at the Department of Pathology, Etlik City Hospital, Ankara,
Türkiye, between November 2022 and July 2025. Clinical data were
obtained from medical records, including age, sex, smoking history,
treatment regimen, clinical stage, radiologic findings and
follow-up information.
Inclusion criteria were as follows: i)
histologically confirmed non-small cell lung cancer (NSCLC); ii)
receipt of neoadjuvant CT or CIT followed by surgical resection;
and iii) availability of adequate pathological material for
evaluation. Exclusion criteria included: i) incomplete clinical or
follow-up data; ii) insufficient tumor tissue for histopathological
assessment; and iii) prior history of other malignancies or
previous lung cancer treatment.
The present study was conducted in accordance with
the Declaration of Helsinki and was approved by the Ethics
Committee of Etlik City Hospital (approval no.
AEŞH-BADEK2-2025-285). The requirement for informed consent was
waived due to the retrospective nature of the study.
Pathologic examination
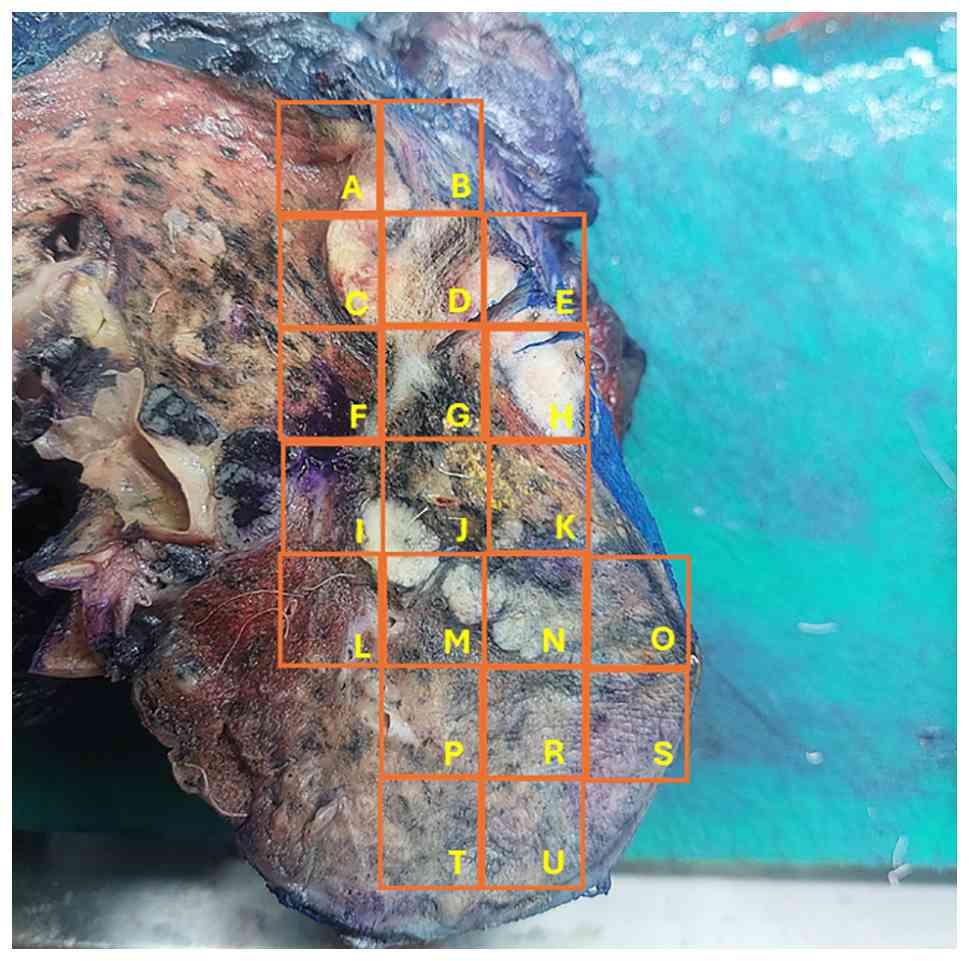
All resection specimens were grossly examined in
accordance with IASLC recommendations, with particular attention
paid to accurate identification and mapping of the tumor bed
(5). Fibrotic and necrotic areas
within the tumor bed were extensively sampled, and the entire tumor
bed was comprehensively submitted for histopathological evaluation
to ensure adequate representation of treatment-induced changes. As
shown in Fig. 1, each specimen was
systematically sectioned and subdivided into grid areas to enable
precise mapping and comprehensive assessment of the tumor bed
(Fig. 1). Representative sections
were obtained from the entire tumor bed, including areas of
fibrosis, necrosis, and any residual viable tumor. All nodal
stations were systematically evaluated to assess metastatic
involvement. Lymph nodes from each station were dissected and
entirely submitted for histological evaluation when feasible.
Surgical specimens were fixed in 10% neutral
buffered formalin (Sigma-Aldrich; Merck KGaA) at room temperature
for 24–48 h. Following fixation, tissues were routinely processed
using an automated tissue processor and embedded in paraffin.
Paraffin blocks were sectioned at a thickness of 4 µm using a
rotary microtome and mounted on glass slides Histopathological
assessment focused on quantifying the percentage of RVT and
assigning tumor regression grade according to established criteria
(5,6). The pattern and extent of fibrosis, the
presence and degree of coagulative necrosis and the distribution of
inflammatory infiltrates, including stromal and intratumoral TILs,
were documented. Briefly, sections were deparaffinized in xylene
and rehydrated through graded ethanol solutions. Hematoxylin
staining (Harris hematoxylin; Sigma-Aldrich; Merck KGaA) was
performed for 5–7 min at room temperature, followed by rinsing in
running tap water and differentiation. Slides were counterstained
with eosin Y solution (Sigma-Aldrich; Merck KGaA) for 1–2 min at
room temperature, dehydrated through graded alcohols, cleared in
xylene, and coverslipped using a mounting medium. All stained
slides were examined using a light microscope. Histopathological
evaluation was performed independently by experienced pathologists.
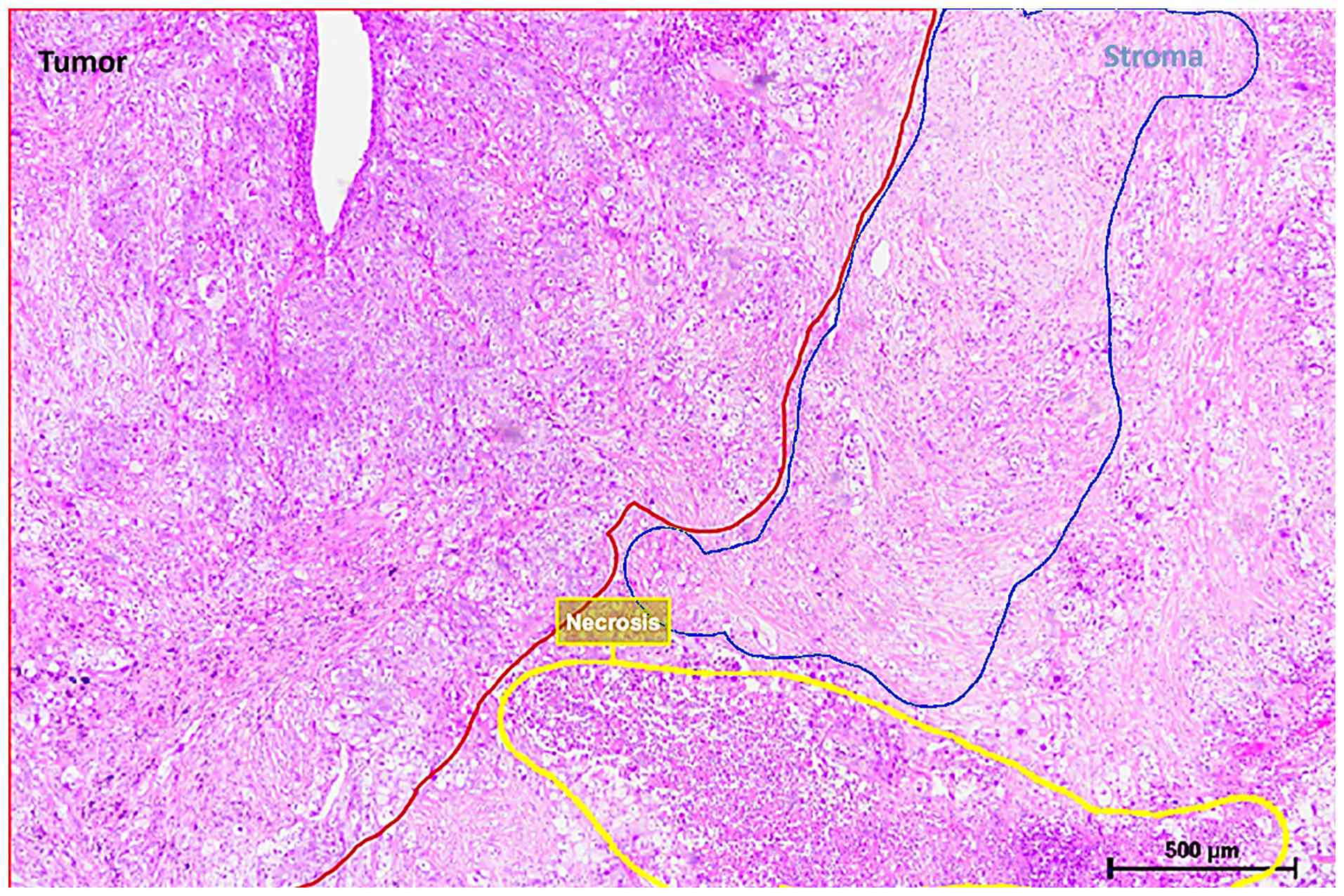
Whole-slide images were reviewed using QuPath (version 0.6.0)
(20). Tumor, necrotic and stromal
regions were manually delineated using annotation tools and area
measurements were extracted to calculate the relative proportions
of each tissue component (Fig. 2).
Additional regression-associated features such as foamy
macrophages, cholesterol clefts and hemosiderin deposition were
evaluated. Adverse morphologic parameters, including STAS and
pleural invasion, were recorded when present. Lymph nodes were also
examined for residual metastatic tumor. All histopathologic
evaluations were performed jointly by three pathologists. Cases
were reviewed in a consensus-based manner and any discrepancies in
the assessment of histologic parameters were resolved through joint
re-evaluation and agreement. Although formal interobserver
variability was not quantified, a standardized evaluation approach
based on IASLC recommendations was applied to ensure consistency
(5). Digital quantification using
QuPath was applied to obtain objective measurements of tumor,
stromal and necrotic components. Although manual annotation was
required for region selection, the use of a standardized digital
analysis platform helped reduce observer-dependent variability.
Criteria for pathologic response
Pathologic response was assessed in accordance with
established neoadjuvant therapy criteria (5,6) pCR
represented the complete absence of viable tumor cells in the
resected lung specimen and regional lymph nodes and mPR was defined
by an RVT fraction of ≤10%, indicative of notable treatment effect.
Specimens with >10% viable tumor were classified as non-mPR,
reflecting limited pathologic regression.
Statistical analysis
Statistical analyses and data visualization were
performed using the Python programming language (Version 3.13.7;
Python Software Foundation). The distribution characteristics of
continuous variables were assessed using the Shapiro-Wilk and
Kolmogorov-Smirnov test. For data that did not follow a normal
distribution and for variables with limited sample size,
descriptive statistics are reported as the median [interquartile
range (IQR): 25–75th percentile], while categorical variables are
presented as frequencies (n) and percentages (%). The nonparametric
Mann-Whitney U test was used to compare continuous variables
between two independent groups. For categorical variables, Fisher's
exact tests and χ2 tests were preferred due to the small
sample size and low expected cell frequencies. Spearman's rank
analysis was applied to examine correlation between variables.
P<0.05 was considered to indicate a statistically significant
difference for all analyses. Given that the dataset lacked exact
dates of mortality and recurrence, survival analysis was conducted
using a pseudo-overall survival (pseudo-OS) approach based on the
time from diagnosis to the last follow-up date.
Results
Patient characteristics and
clinicopathological data
A total of 30 patients diagnosed with resectable
NSCLC who received neoadjuvant therapy were included in the present
study. The median age was 65.0 years (IQR: 59.2–68.5) and the
majority of patients were male (93.3%). Patients were divided into
two cohorts according to the treatment regimen administered. The CT
cohort consisted of 22 patients (73.3%) who received platinum-based
CT, with 2 patients having also undergone radiotherapy. The CIT
cohort consisted of 8 patients (26.7%) who received immunotherapy
(PD-1/PD-L1 inhibitors) combined with CT.
No significant differences were observed between the
two treatment groups with regard to age, sex, smoking burden,
histologic subtype, clinical stage, baseline tumor size, PD-L1
expression level or mutational status (P>0.05). However, given
the limited sample size, group comparability should be interpreted
with caution (Table I).
 | Table I.Clinical and pathological
characteristics of patients according to treatment regimen. |
Table I.
Clinical and pathological
characteristics of patients according to treatment regimen.
| Variable | Overall (n=30) | CIT (n=8) | CT (n=22) | P-value |
|---|
| Age, median years
(IQR) | 65.0
(59.2–68.5) | 65.0
(55.5–71.5) | 65.0
(62.2–67.0) | 0.906 |
| Sex (%) |
|
|
| 0.064 |
|
Male | 28 (93.3) | 6 (75.0) | 22 (100.0) |
|
|
Female | 2 (6.7) | 2 (25.0) | 0 (0.0) |
|
| Smoking history,
median pack-years (IQR) | 47.5
(22.5–60.0) | 45.0
(11.2–65.0) | 47.5
(30.0–60.0) | 0.706 |
| Histology, n
(%) |
|
|
| 0.215 |
|
Adenocarcinoma | 15 (50.0) | 6 (75.0) | 9 (40.9) |
|
|
Squamous cell carcinoma | 15 (50.0) | 2 (25.0) | 13 (59.1) |
|
| Indication for
neoadjuvant therapy, n (%) |
|
|
| 0.369 |
| Nodal
involvement | 16 (53.3) | 6 (75.0) | 10 (45.5) |
|
| T4
disease/other | 14 (46.7) | 2 (25.0) | 12 (54.5) |
|
| Clinical stage, n
(%) |
|
|
| 0.789 |
|
IB-IIB | 4 (13.3) | 1 (12.5) | 3 (13.6) |
|
|
IIIA | 16 (53.3) | 5 (62.5) | 11 (50.0) |
|
|
IIIB-IVA | 10 (33.3) | 2 (25.0) | 8 (36.4) |
|
| Baseline tumor
size, median cm (IQR) | 5.7 (4.8–7.0) | 5.3 (4.9–5.8) | 5.9 (4.6–7.1) | 0.439 |
| PD-L1 expression, n
(%) |
|
|
| 0.340 |
|
Negative (<1%) | 18 (60.0) | 4 (50.0) | 14 (63.6) |
|
|
Positive (≥1%) | 12 (40.0) | 4 (50.0) | 8 (36.4) |
|
| Mutation status, n
(%) |
|
|
| 0.284 |
| Wild
type (negative) | 26 (86.7) | 6 (75.0) | 20 (90.9) |
|
|
Mutant | 4 (13.3) | 2 (25.0) | 2 (9.1) |
|
Tumor response and pathologic
regression
When the primary endpoints of pathologic response
were evaluated, a trend toward improved pathologic response was
observed in the CIT cohort. The proportion of viable tumor cells in
the resected specimens after treatment decreased to a median of
7.5% (IQR: 0.0–55.0) in the CIT group, whereas it remained at 55.0%
(IQR: 32.5–67.5) in the CT group (P=0.156; Table II). Furthermore, mPR (≤10% viable
tumor) was achieved in 62.5% (5/8) of patients in the CIT cohort,
compared with 22.7% (5/22) in the CT cohort. Statistical analysis
showed that this difference approached significance (P=0.078;
Table II). pCR (stage ypT0N0) was
observed in 37.5% (3/8) of patients in the CIT group and 13.6%
(3/22) of those in the CT group.
| Table II.Post-treatment pathological findings
and tumor microenvironment. |
Table II.
Post-treatment pathological findings
and tumor microenvironment.
| Morphologic
feature | Overall (n=30) | CIT (n=8) | CT (n=22) | P-value |
|---|
| Postoperative tumor
size, median cm (IQR) | 2.8 (0.8–4.3) | 1.6 (0.0–3.4) | 2.9 (1.6–4.5) | 0.268 |
| Viable tumor,
median % (IQR) | 50.0
(10.0–67.5) | 7.5 (0.0–55.0) | 55.0
(32.5–67.5) | 0.156 |
| Tumor fibrosis,
median % (IQR) | 20.0
(12.5–30.0) | 27.5
(20.0–42.5) | 20.0
(10.0–30.0) | 0.178 |
| Tumor inflammation,
median % (IQR) | 15.0
(6.2–33.8) | 32.5
(12.5–40.0) | 10.0
(6.2–27.5) | 0.274 |
| Median tumor
necrosis, % (IQR) | 10.0
(5.0–20.0) | 5.0 (4.5–21.2) | 10.0
(5.0–18.8) | 0.794 |
| Total stroma,
median % (IQR) | 40.0
(20.5–68.8) | 67.5
(39.2–91.2) | 32.5
(20.0–57.5) | 0.121 |
| TIL pattern
(lymphocytic), n (%) | 12 (40.0) | 5 (62.5) | 7 (31.8) | 0.210 |
| pCR, n (%) | 6 (20.0) | 3 (37.5) | 3 (13.6) | 0.300 |
| mPR, n (%) | 10 (33.3) | 5 (62.5) | 5 (22.7) | 0.078 |
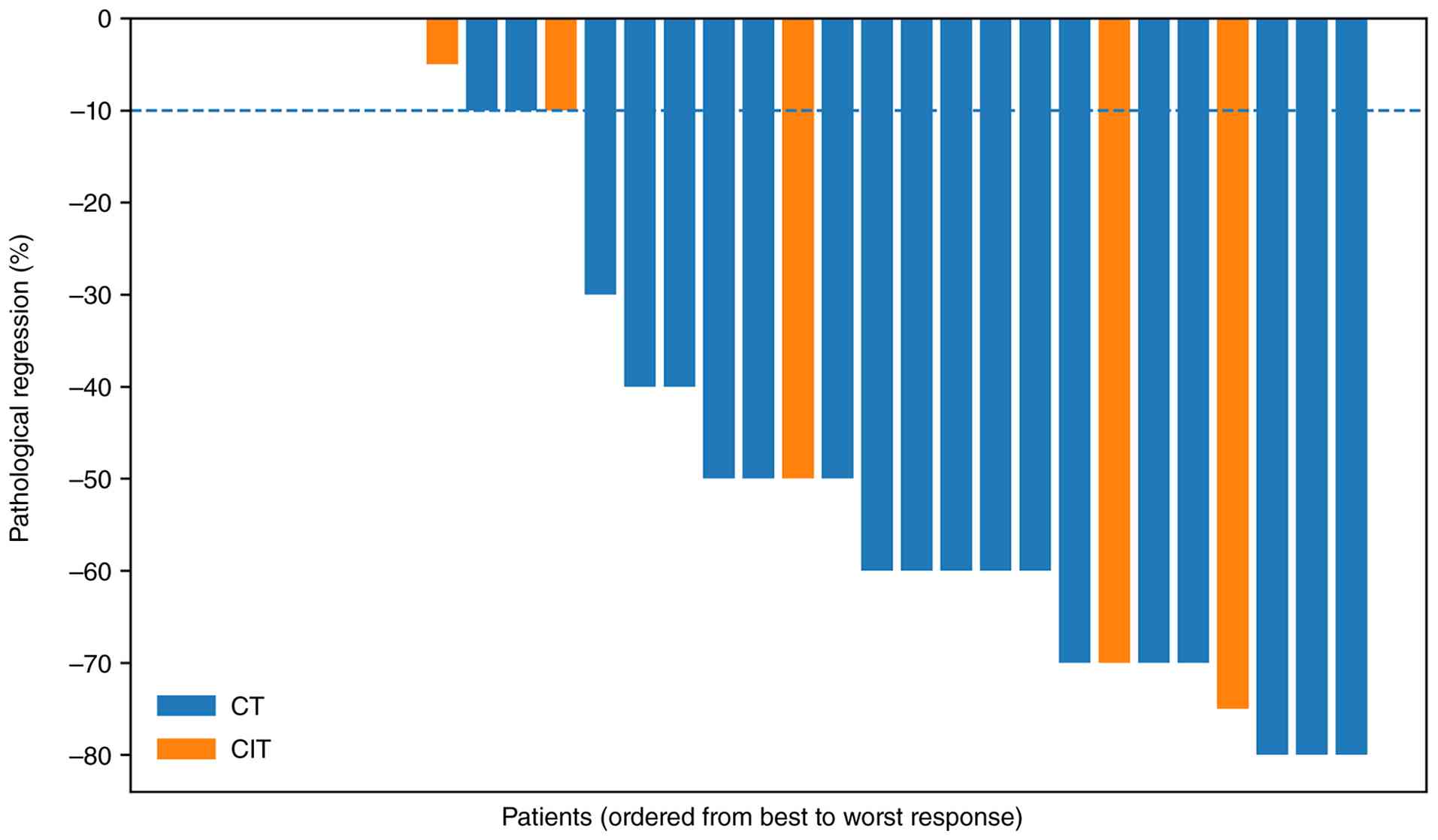
The depth of pathologic response in each patient is
visualized in the waterfall plot (Fig.
3). Notably, patients receiving chemo-immunotherapy tended to
cluster in the region associated with the greatest tumor
regression, including pCR and mPR.
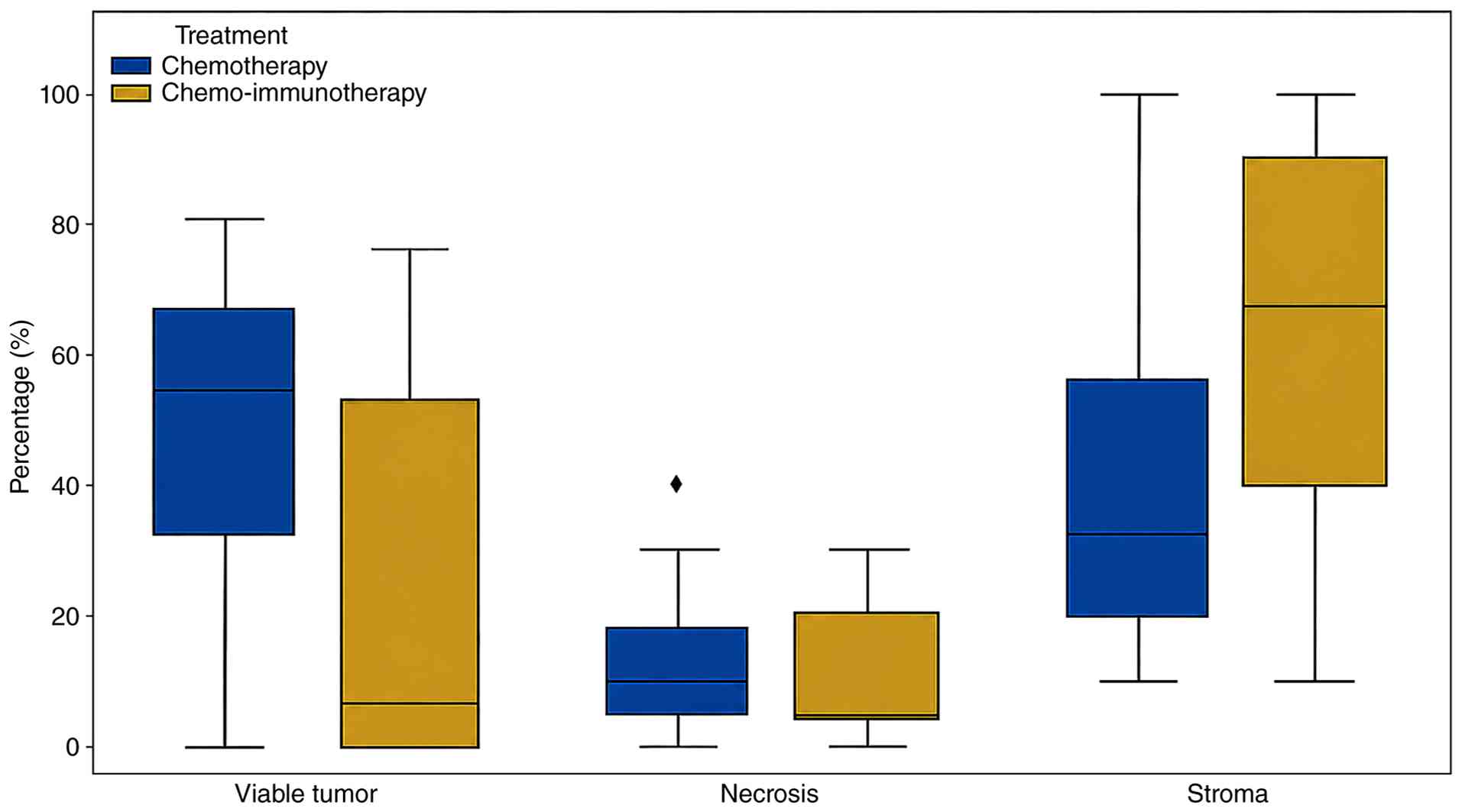
Tumor microenvironment and histologic
changes
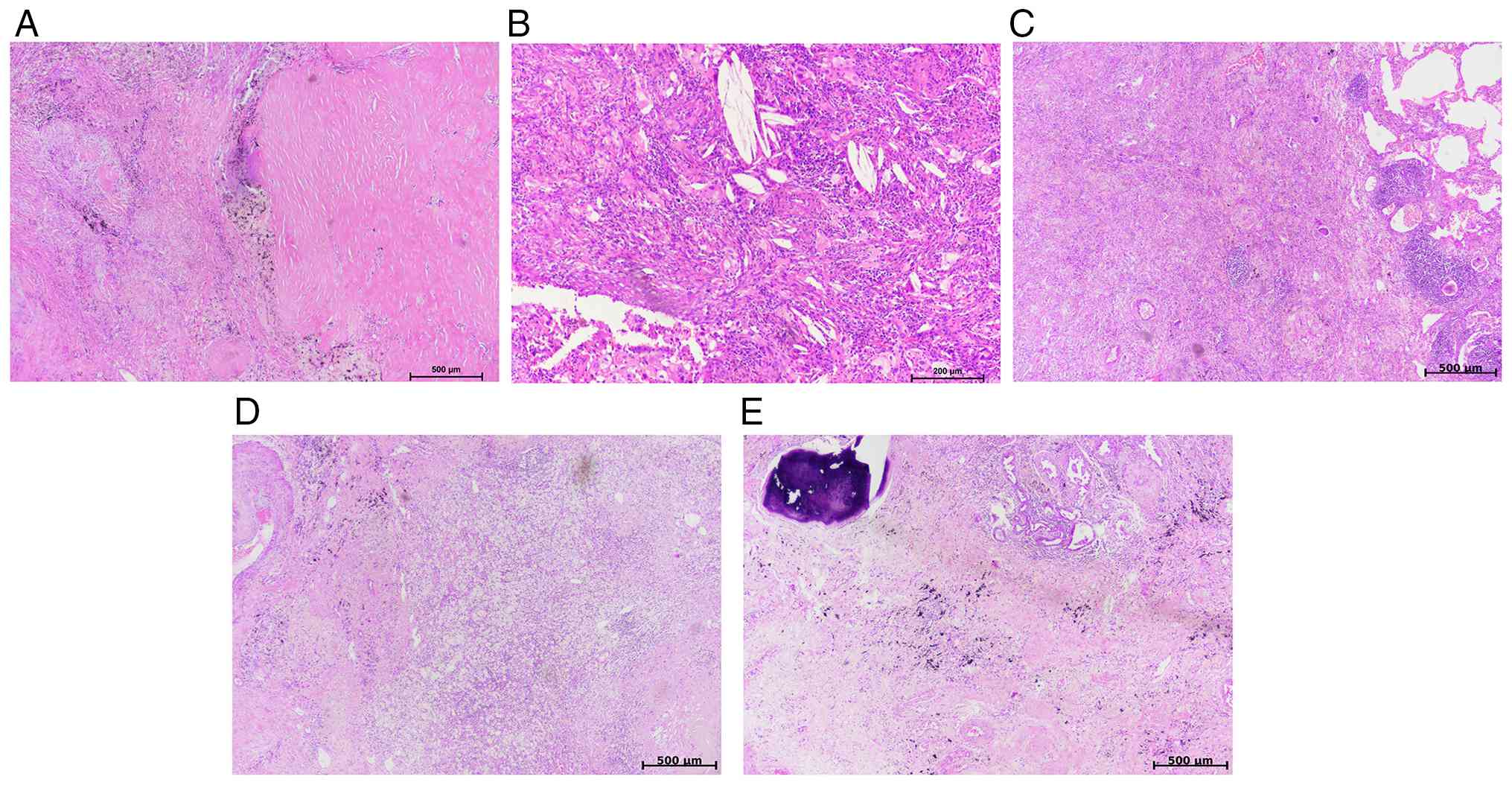
Histopathologic alterations occurring within the
tumor bed in treatment-responsive patients, including fibrosis,
inflammation, necrosis and stromal reactions, were analyzed
(Table II). The total stromal
component (fibrosis + inflammation) exhibited a median of 67.5% in
the CIT group and 32.5% in the CT group. This suggested that
immunotherapy not only promoted tumor regression but may have also
promoted immune-mediated stromal remodeling within the tumor bed
(Fig. 4A-E). Tumor-associated
inflammation was found to be higher in the CIT cohort (median
32.5%) compared with the CT cohort (10.0%). In addition, when TIL
patterns were evaluated, a lymphocytic-dominant pattern was
observed more frequently in the CIT group (62.5%) compared with the
CT group (31.8%; Table II).
Necrosis rates appeared to be similar between the two groups,
indicating that necrosis did not serve as a distinguishing
parameter of treatment response (P=0.794; Table II). These morphological changes are
illustrated in the boxplot (Fig.
5), in which the viable tumor box lies markedly closer to the
baseline in the CIT group, whereas the stromal component is shifted
upward.
PD-L1-associated parameters
Correlation analysis revealed no significant
associations between PD-L1 expression score and viable tumor
percentage (rs=−0.17), necrosis (rs=−0.15), or fibrosis (rs=−0.06;
P>0.05). A significant inverse correlation was observed between
viable tumor percentage and fibrosis (rs=−0.52; P<0.01; Table III). The association between PD-L1
expression and the pattern of TILs (histiocytic vs. lymphocytic)
was borderline significant (χ2=5.92; P=0.052; Table III). Lymphocytic immune response
was more pronounced in PD-L1-positive cases.
| Table III.Spearman correlation analysis between
PD-L1 expression and histopathologic variables. |
Table III.
Spearman correlation analysis between
PD-L1 expression and histopathologic variables.
| Variable | PD-L1 | Viable tumor | Necrosis | Fibrosis |
|---|
| PD-L1 score | 1.00 |
|
|
|
| Viable tumor
(%) | −0.17 | 1.00 |
|
|
| Necrosis (%) | −0.15 | −0.09 | 1.00 |
|
| Fibrosis (%) | −0.06 | −0.52a | 0.08 | 1.00 |
Treatment, clinical factors and
response association
Results indicated that mPR was 62.5% in patients who
received CIT, whereas it was 22.7% in the CT group (P=0.078;
Table IV). The rate of pCR was
found to be 37.5% in the CIT group and 13.6% in the CT group
(P=0.300; Table II). Tumor
shrinkage was found to be significantly greater in patients who
achieved a pathologic response (pCR and mPR) compared with
nonresponders (P<0.001 for both pCR and mPR; Table IV). No statistically significant
association was found between pathologic response (pCR or mPR) and
baseline clinical stage (P>0.05) or smoking burden
(P>0.05).
| Table IV.Associations between clinical and
treatment characteristics and mPR. |
Table IV.
Associations between clinical and
treatment characteristics and mPR.
| Variable | mPR present
(n=10) | mPR absent
(n=20) | P-value |
|---|
| Treatment regimen,
n (%) |
|
| 0.078 |
|
CIT | 5 (62.5) | 3 (37.5) |
|
| CT | 5 (22.7) | 17 (77.3) |
|
| Clinical stage, n
(%) |
|
| 0.449 |
|
I–II | 1 (10.0) | 3 (15.0) |
|
|
III–IV | 9 (90.0) | 17 (85.0) |
|
| Smoking history,
median pack-years (IQR) | 57.5 (36–84) | 43.5 (19–60) | 0.508 |
| Tumor size, median
% (IQR) | −100.0 (−100 to
−91) | −30.3 (−49 to
−13) | <0.001 |
Association between pathologic response (mPR and
pCR) and tumor tissue characteristics/Histopathologic features
of the tumor bed, including viable tumor, necrosis and fibrosis,
were compared between responders (mPR/pCR) and nonresponders using
the Mann-Whitney U test.
Both mPR and pCR responders exhibited significantly
lower viable tumor percentages compared with nonresponders
(P<0.001; Table V). Fibrosis, a
strong indicator of treatment response, was found to be
significantly higher in the mPR group (median: 40%) compared with
the nonresponders (median: 20%; P<0.001; Table V). Similarly, fibrosis was
significantly elevated in the pCR group (P=0.009; Table V), while tumor necrosis did not
differ significantly between mPR and non-mPR groups or pCR and
non-pCR groups (P=0.448 and P>0.99, respectively; Table V). STAS positivity was significantly
lower in patients with mPR, indicating an inverse association
(P<0.001). Despite pleural invasion being absent in patients
with pCR, this finding was not statistically significant and
therefore only reflected a trend (P>0.05; Table V).
| Table V.Comparison of tumor tissue
characteristics according to pathologic response status. |
Table V.
Comparison of tumor tissue
characteristics according to pathologic response status.
| Variable | mPR present | mPR absent | P-value | pCR present | pCR absent | P-value |
|---|
| Viable tumor,
median % (IQR) | 0.0 (0.0–5.0) | 60.0
(50.0–70.0) | <0.001 | 0.0 (0.0–0.0) | 60.0
(40.0–70.0) | <0.001 |
| Tumor fibrosis,
median % (IQR) | 40.0
(30.0–53.0) | 20.0
(10.0–28.0) | <0.001 | 37.5
(31.0–55.0) | 20.0
(10.0–30.0) | 0.009 |
| Tumor necrosis,
median % (IQR) | 10.0
(5.0–14.0) | 7.5 (5.0–23.0) | 0.448 | 7.5 (4.0–24.0) | 10.0
(5.0–20.0) | 0.990 |
| STAS positivity
(%) | 20.0 | 70.0 | 0.012 | 0.0 | 66.7 | <0.001 |
| Pleural invasion
(%) | 0.0 | 30.0 | 0.061 | 0.0 | 25.0 | 0.191 |
PD-L1 and immune response
Comparisons between PD-L1-negative and
PD-L1-positive groups revealed no significant differences in viable
tumor percentage (P=0.305), necrosis (P=0.606) or fibrosis
(P=0.761), and no significant association with achievement of mPR
(P=0.693; Table VI). However, a
lymphocytic TIL pattern was observed significantly more frequently
in PD-L1-positive patients compared with PD-L1-negative patients
(66.7% vs. 22.2%; P=0.040; Table
VI).
| Table VI.Comparison of histopathologic and
clinical characteristics according to PD-L1 status. |
Table VI.
Comparison of histopathologic and
clinical characteristics according to PD-L1 status.
| Variable | PD-L1 negative
(n=18) | PD-L1 positive
(n=12) | Test | P-value |
|---|
| Viable tumor,
median (%) | 55.0 | 40.0 | Mann-Whitney U | 0.305 |
| Tumor necrosis,
median (%) | 10.0 | 5.0 | Mann-Whitney U | 0.606 |
| Tumor fibrosis,
median (%) | 20.0 | 20.0 | Mann-Whitney U | 0.761 |
| mPR present, n
(%) | 5 (27.8) | 5 (41.7) | χ2 | 0.693 |
| TIL pattern
(lymphocytic), n (%) | 4 (22.2) | 8 (66.7) | χ2 | 0.040 |
Survival analysis
Given that the dataset lacked precise dates of
mortality and recurrence, survival analysis was performed using a
pseudo-OS approach, defined as the interval between diagnosis and
the most recent follow-up. Within this framework, mPR was found to
be associated with improved survival in the log-rank analysis
(P=0.036). Increasing clinical stage was associated with higher
mortality risk in the Cox regression model (HR=2.62; P=0.033).
Higher tumor inflammation levels were also associated with improved
survival (log-rank P=0.043), whereas tumor fibrosis and necrosis
were not significantly associated with survival outcomes
(P>0.05; data not shown).
Discussion
Neoadjuvant therapy is increasingly being used
across numerous solid tumor types with the aim of reducing tumor
burden and improving surgical resectability (6,10–12).
This approach has been well established in malignancies such as
breast, gastric and rectal cancer. The application of neoadjuvant
therapy in NSCLC has gained increasing attention (2,3,13). One
of the major challenges in NSCLC is that a marked proportion of
patients may not proceed to surgical resection following
neoadjuvant treatment because of disease progression or loss of
operability. Consequently, the development of more effective
neoadjuvant treatment strategies remains a necessity in this
setting.
In this context, immunotherapy has emerged as a
promising addition to conventional treatment approaches. As in
other tumor types, accurate evaluation of post-treatment specimens
is key, as characterization of the tumor bed provides important
prognostic information. Histopathologic assessment serves a central
role in this process. Therefore, understanding the
histomorphological effects of CIT, beyond conventional CT-induced
changes, is central to improving response assessment and guiding
clinical decision-making in NSCLC.
In the present study, detailed assessment of
pathologic response in resected NSCLC specimens following
neoadjuvant therapy suggested that CIT may be associated with a
more pronounced pattern of tumor regression compared with CT alone.
Although these findings did not reach statistical significance, the
lower proportion of RVT and the higher rates of mPR and pCR
observed in the CIT group suggested a potential biological
advantage of incorporating immunotherapy into neoadjuvant
treatment. These findings should be interpreted as
hypothesis-generating and are consistent with the explanatory
framework provided by the IASLC recommendations, which emphasize
standardized assessment of tumor bed composition and viable tumor
quantification (5).
The regression patterns observed in the present
cohort, including increased fibrosis and lymphocytic infiltration,
broadly align with the immune-mediated changes described in the
irPRC proposed by Cottrell et al (6). While these features are more
frequently observed in immunotherapy-treated tumors, they should be
interpreted within the context of treatment-related stromal
remodeling. Increased TIL density may reflect a metabolically
permissive tumor microenvironment, as tumor-derived factors (such
as lactate) have been shown to suppress T cell function (9).
CheckMate 816 reported higher rates of mPR and pCR
with the addition of immunotherapy to CT, supporting the potential
contribution of immune activation to tumor regression (13). Similarly, the LCMC3 trial
demonstrated that single-agent immunotherapy can induce measurable
pathologic responses in early-stage NSCLC (14). However, given the limited sample
size and lack of statistical significance in the present cohort,
these observations should be interpreted cautiously.
Assessment of pathologic response in NSCLC resection
specimens after neoadjuvant therapy presents notable challenges,
particularly in distinguishing viable tumor from therapy-induced
stromal changes and in accurately defining the boundaries of the
tumor bed. The pathologist serves a critical role in the accurate
assessment of treatment response following neoadjuvant therapy,
particularly through standardized evaluation and appropriate
interpretation of post-treatment histologic changes (15). Weissferdt et al further
demonstrated that appropriate sampling strategies, tumor bed
mapping and recognition of immune-mediated regression features are
central to accurate interpretation (16).
The differences observed between CIT and CT in the
present study, namely greater fibrosis, a more pronounced
inflammatory response, predominant lymphocytic TIL patterns and
reduced STAS positivity, are broadly consistent with findings
reported in the literature (17).
In a cohort study including 358 patients, Pataer
et al (21) demonstrated
that fibrosis is a reliable indicator of tumor response following
neoadjuvant therapy (consistent with the present findings), whereas
necrosis did not show a significant association with treatment
response and lacks specificity as a marker of therapy-induced tumor
regression. These patterns may reflect the combined effects of
direct tumor cell death and immune-mediated remodeling of the tumor
microenvironment. STAS has been recognized as an adverse prognostic
factor associated with increased recurrence risk and aggressive
tumor behavior in lung cancer (22). The reduced STAS positivity observed
in mPR cases in the present study may reflect more effective
elimination of invasive tumor components following neoadjuvant
therapy. Assessment of STAS in post-neoadjuvant specimens may be
challenging due to treatment-related architectural distortion and
potential artifacts, which should be considered when interpreting
its presence or absence.
Increased lymphocytic infiltration and stromal
activation may represent an active immune response induced by
immunotherapy. However, certain features should be interpreted with
caution. Although increased fibrosis is frequently observed in
responding tumors, it may partly reflect treatment-related tissue
replacement rather than an independent predictive biomarker.
Similarly, the assessment of STAS following neoadjuvant therapy may
be influenced by treatment-induced architectural distortion and
sampling variability. Therefore, these findings should be
considered within the context of treatment effects and interpreted
as descriptive rather than definitive indicators of tumor
biology.
In the present study, nodal regression could not be
adequately assessed, as there is currently no standardized method
for the evaluation of post-neoadjuvant lymph node changes. In
addition, lymph node assessment is challenging due to the frequent
absence of distinct fibrotic regression patterns, with nodes often
reverting to a near-normal appearance, and the presence of
anthracosis and histiocytic aggregates that may further obscure
treatment-related changes. Previous studies have shown that
pathologic responses of the primary tumor and lymph nodes may
frequently differ in NSCLC following neoadjuvant CIT (23,24).
Joint evaluation of both primary tumor and nodal responses is
important in accurate prognostic stratification and the lack of
comprehensive assessment of nodal regression represents one of the
limitations of the present study (25). The association between TIL
enrichment and pathologic response in the present cohort also
aligns with biomarker-focused studies such as that of Rojas et
al (26).
In the present study, pathologic evaluation was
performed jointly by three pathologists. In a study addressing the
subjectivity of mPR assessment in NSCLC after neoadjuvant therapy,
interobserver agreement among pathologists was found to be high; in
addition, the ≤10% viable tumor threshold was shown to be a
reliable criterion for predicting survival. Therefore, standardized
assessment is of marked importance in clinical research and patient
management (27).
It should be noted that certain associations
observed in the present study may be partly influenced by the
definitions of response criteria. For example, the lower viable
tumor percentage in mPR cases is inherent to the definition of mPR
rather than an independent biological finding. In addition, given
the relatively small sample size and the number of subgroup
analyses performed, a number of the observed associations should be
interpreted as exploratory. Future studies with larger cohorts and
validation analyses are thus required to further determine these
findings.
Due to the absence of precise data regarding
recurrence and mortality, survival outcomes in the present study
were assessed using a pseudo-OS metric, which does exhibit inherent
limitations. Within this exploratory framework, mPR appeared to be
associated with improved survival, consistent with previous studies
reporting an association between RVT and clinical outcomes
(7,16,21).
Similarly, increased tumor-associated inflammation exhibited a
trend toward improved survival. Meta-analytic data have suggested
that CIT may improve survival outcomes and increase pCR rates in
NSCLC (28). However, these
observations should be interpreted cautiously, as pseudo-OS may be
influenced by follow-up duration, censoring patterns and
treatment-associated factors, such as differences in neoadjuvant
regimens, variability in treatment response and the use of adjuvant
therapy. Therefore, these findings should be considered
hypothesis-generating rather than definitive evidence of prognostic
importance. Previous studies have suggested that the degree of
histologic tumor regression after neoadjuvant therapy in NSCLC may
serve as a potential biomarker for predicting patient survival
(7,21,29).
In routine practice, assessment of pathologic
response provides an early indication of treatment effectiveness
and may help guide clinical decision-making. In the context of
neoadjuvant or perioperative CIT, standardized pathologic
evaluation remains particularly important for both patient
management and research (30).
In the present study, a higher degree of tumor
inflammation and increased TIL density were observed following CIT.
However, a number of studies have reported that, although
immunotherapy is associated with greater lymphocytic infiltration
and more prominent immune response features within the tumor
microenvironment, the overall patterns of pathological regression,
including fibrosis, necrosis and residual viable tumor
distribution, largely overlap with those seen after CT (6,17,26,30).
The degree of pathologic response, particularly mPR and pCR, is a
strong predictor of survival in patients treated with both
immunotherapy and CT (31). These
findings further suggest an important role for the tumor
microenvironment in shaping treatment response.
Despite this, the applicability of a uniform ≤10%
viable tumor threshold across all histologic subtypes has been
questioned. Qu et al (32)
demonstrated that the optimal cut-off for RVT differs markedly
between adenocarcinoma and squamous cell carcinoma when these tumor
types are evaluated separately and that a higher threshold is
required for prognostic stratification in adenocarcinomas; however,
in the present study, adenocarcinoma and squamous cell carcinoma
were not analyzed separately and were instead evaluated
categorically under the umbrella of NSCLC. In this context,
although the ≤10% cut-off was applied in accordance with guidelines
(5), it is conceivable that
histology-specific cut-off values may be adopted in future studies.
This further supports the need for subtype-specific interpretation
of pathologic response in NSCLC.
Despite the promising efficacy of immunotherapy, a
notable proportion of patients with NSCLC develop either primary or
acquired resistance to treatment. As highlighted by Wang et
al (33), immunotherapy
resistance is a multifactorial process involving tumor-intrinsic
genetic alterations, dysregulation of immune checkpoint pathways
and the establishment of an immunosuppressive tumor
microenvironment. These mechanisms may impair effective T-cell
activation, reduce immune cell infiltration and ultimately limit
treatment response. In this context, the tumor microenvironment
emerges as a key determinant of therapeutic efficacy, aligning with
the present findings demonstrating associations between
inflammatory response and treatment-associated changes. Notably,
the development of resistance underscores the need for alternative
and combinatorial treatment strategies, including the integration
of targeted therapies, anti-angiogenic agents and novel
immunomodulatory approaches. This is particularly relevant to the
present findings, in which variations in inflammatory response and
TIL density may reflect underlying differences in tumor immune
competence and potential resistance mechanisms. These observations
may have implications for treatment stratification and response
assessment in the neoadjuvant setting, particularly in
distinguishing effective immune-mediated responses from residual
disease.
Emerging therapeutic strategies, including
macrophage-mediated nanomedicine delivery systems and nano-assisted
radiotherapy approaches, further highlight the active role of the
tumor microenvironment in modulating therapeutic response in lung
cancer (34,35).
An additional consideration is the potential
confounding effect of radiotherapy, as a subset of patients in the
CT cohort also received radiotherapy. Radiotherapy is known to
influence tumor morphology by increasing necrosis, promoting
fibrosis and altering stromal composition, which may complicate the
distinction between viable tumor and treatment-related changes and
thereby affect histopathological assessment (29,36).
However, only a limited number of patients (n=2) received combined
chemoradiotherapy in the present cohort. Upon evaluation of these
cases, both demonstrated minimal pathologic response, suggesting
that radiotherapy is unlikely to have contributed markedly to the
regression patterns observed in the present cohort. Although
radiotherapy may induce prominent histopathologic alterations such
as fibrosis and tissue remodeling, these changes do not necessarily
reflect a strong therapeutic response and may complicate the
distinction between viable tumor and treatment effect, as
previously reported in radiotherapy-treated NSCLC resection
specimens (36). This factor should
be considered when interpreting the results. Given that only a
small number of patients received radiotherapy, subgroup analysis
was not feasible (36).
Pathologic complete response is considered an
important parameter in the assessment of patient prognosis;
however, it is not always sufficient as a standalone indicator. As
highlighted by Huynh et al (37), long-term survival is influenced not
only by the extent of tumor eradication but also by tumor biology,
treatment modality and characteristics of the tumor
microenvironment such as TIL density, patterns of immune response,
and stromal composition including fibrosis and inflammatory cell
infiltration. Therefore, even in cases without pathologic complete
response, prognostic evaluation should not rely solely on the
presence of residual tumor but should also incorporate a
comprehensive assessment of the tumor microenvironment and immune
response. This perspective is consistent with the present findings,
in which variations in inflammatory response and TIL density were
associated with treatment-associated changes.
Recent advances in artificial intelligence
(AI)-assisted pathology have further emphasized the value of
objective response assessment. In the LCMC3 study, Dacic et
al (38) demonstrated that
AI-powered quantification of pathologic response in NSCLC treated
with neoadjuvant atezolizumab provides reproducible and scalable
evaluation of tumor regression. These findings support the
integration of digital pathology tools, such as QuPath, into
routine practice to enhance the accuracy and consistency of
post-treatment assessment.
Collectively, the present findings suggest that CIT
may be associated with a more pronounced pattern of pathologic
response compared with CT alone. These observations are consistent
with the growing body of evidence supporting the role of
neoadjuvant immunotherapy in resectable NSCLC and thus emphasize
the importance of standardized pathologic response assessment in
both clinical practice and research settings (4,13,14).
These findings also highlight the evolving role of the tumor
microenvironment as a key determinant of treatment response.
The present study is limited by its relatively small
sample size and single-center, retrospective design, which may
introduce selection bias and restrict generalizability. The limited
number of cases reflects the restricted availability of resected
specimens following neoadjuvant therapy in routine clinical
practice, as not all patients proceed to surgery after systemic
treatment. In addition, treatment heterogeneity across patients may
have influenced the observed patterns of pathologic response and
the absence of precise recurrence and mortality data limited the
ability to conduct conventional survival analyses. In addition, the
use of pseudo-OS may have introduced bias related to variability in
follow-up duration and censoring patterns and the limited number of
survival events further restricts the strength and interpretability
of survival-associated findings. Furthermore, the inclusion of a
small number of patients who received radiotherapy in addition to
CT may have influenced histopathologic features such as necrosis,
fibrosis and stromal remodeling. Although evaluation of these cases
demonstrated minimal pathologic response, the potential confounding
effect of radiotherapy cannot be entirely excluded and should be
interpreted with caution.
Additional limitations may have included the lack of
formal interobserver agreement analysis. Although all cases were
evaluated jointly by three pathologists using a consensus-based
approach, some variability in the assessment of histologic
parameters such as fibrosis, inflammation and viable tumor cannot
be entirely excluded. Furthermore, the absence of blinding to
treatment groups may have introduced potential bias. Lastly, given
that manual annotation was required for region selection, a degree
of observer-dependent variability remains unavoidable, despite
digital image analysis using QuPath having provided a more
objective and reproducible framework for quantifying tumor, stromal
and necrotic components.
In conclusion, neoadjuvant CIT may be associated
with deeper pathologic regression compared with CT alone,
characterized by increased fibrosis and enhanced immune activation,
including higher TIL density and reduced STAS positivity. In
addition, mPR may serve as a potential prognostic indicator.
Overall, integration of IASLC and irPRC criteria, together with
tumor microenvironment assessment, may improve the evaluation of
treatment response in resectable NSCLC.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
ÖKK conceived and designed the study, performed
histopathological evaluation and wrote the manuscript. YSÇ and NSB
performed histopathological evaluation and interpreted
clinicopathological data. MB performed statistical analysis and
assisted with retrieving and organizing patient data from the
hospital information system. All authors have read and approved the
manuscript. ÖKK and MB confirm the authenticity of all the raw
data.
Ethics approval and consent to
participate
The present study was conducted in accordance with
the Declaration of Helsinki and was approved by the Institutional
Ethics Committee of Etlik City Hospital (Ankara, Turkey; approval
no: AEŞH-BADEK2-2025-285). Due to the retrospective nature of the
present study, the requirement for informed consent was waived by
the ethics committee.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Thai AA, Solomon BJ, Sequist LV, Gainor JF
and Heist RS: Lung cancer. Lancet. 398:535–554. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Provencio M, Nadal E, Insa A,
García-Campelo MR, Casal-Rubio J, Dómine M, Majem M,
Rodríguez-Abreu D, Martínez-Martí A, De Castro Carpeño J, et al:
Neoadjuvant chemotherapy and nivolumab in resectable non-small-cell
lung cancer (NADIM): An open-label, multicentre, single-arm, phase
2 trial. Lancet Oncol. 21:1413–1422. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Wakelee H, Liberman M, Kato T, Tsuboi M,
Lee SH, Gao S, Chen KN, Dooms C, Majem M, Eigendorff E, et al:
Perioperative pembrolizumab for early-stage non-small-cell lung
cancer. N Engl J Med. 389:491–503. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sorin M, Prosty C, Ghaleb L, Nie K,
Katergi K, Shahzad MH, Dubé LR, Atallah A, Swaby A, Dankner M, et
al: Neoadjuvant chemoimmunotherapy for NSCLC: A systematic review
and meta-analysis. JAMA Oncol. 10:621–633. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Travis WD, Dacic S, Wistuba I, Sholl L,
Adusumilli P, Bubendorf L, Bunn P, Cascone T, Chaft J, Chen G, et
al: IASLC multidisciplinary recommendations for pathologic
assessment of lung cancer resection specimens after neoadjuvant
therapy. J Thorac Oncol. 15:709–740. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Cottrell TR, Thompson ED, Forde PM, Stein
JE, Duffield AS, Anagnostou V, Rekhtman N, Anders RA, Cuda JD,
Illei PB, et al: Pathologic features of response to neoadjuvant
anti-PD-1 in resected non-small-cell lung carcinoma: A proposal for
quantitative immune-related pathologic response criteria (irPRC).
Ann Oncol. 29:1853–1860. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hou Z, Zhao L, Zou L and Li B: The
prognostic value of tumor-infiltrating lymphocytes in non-small
cell lung cancer patients who received neoadjuvant chemotherapy
followed by surgery. Adv Clin Exp Med. 32:847–853. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yan Q, Li S, He L and Chen N: Prognostic
implications of tumor-infiltrating lymphocytes in non-small cell
lung cancer: A systematic review and meta-analysis. Front Immunol.
15:14763652024. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Fischer K, Hoffmann P, Voelkl S,
Meidenbauer N, Ammer J, Edinger M, Gottfried E, Schwarz S, Rothe G,
Hoves S, et al: Inhibitory effect of tumor cell-derived lactic acid
on human T cells. Blood. 109:3812–3819. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Tetzlaff MT, Messina JL, Stein JE, Xu X,
Amaria RN, Blank CU, van de Wiel BA, Ferguson PM, Rawson RV, Ross
MI, et al: Pathological assessment of resection specimens after
neoadjuvant therapy for metastatic melanoma. Ann Oncol.
29:1861–1868. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Rizzo A, Mollica V, Santoni M, Palmiotti G
and Massari F: Pathologic complete response in urothelial carcinoma
patients receiving neoadjuvant immune checkpoint inhibitors: A
meta-analysis. J Clin Med. 11:10382022. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Symmans WF, Peintinger F, Hatzis C, Rajan
R, Kuerer H, Valero V, Assad L, Poniecka A, Hennessy B, Green M, et
al: Measurement of residual breast cancer burden to predict
survival after neoadjuvant chemotherapy. J Clin Oncol.
25:4414–4422. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Forde PM, Spicer J, Lu S, Provencio M,
Mitsudomi T, Awad MM, Felip E, Broderick SR, Brahmer JR, Swanson
SJ, et al: Neoadjuvant nivolumab plus chemotherapy in resectable
lung cancer. N Engl J Med. 386:1973–1985. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Chaft JE, Oezkan F, Kris MG, Bunn PA,
Wistuba II, Kwiatkowski DJ, Owen DH, Tang Y, Johnson BE, et al:
Neoadjuvant atezolizumab for resectable non-small cell lung cancer:
An open-label, single-arm phase II trial. Nat Med. 28:2155–2161.
2022. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Dacic S: Neoadjuvant therapy and lung
cancer: Role of pathologists. Arch Pathol Lab Med. 149:e78–e81.
2025. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Weissferdt A, Leung CH, Lin H, Sepesi B,
William WN, Swisher SG, Cascone T, Lee JJ and Pataer A: Pathologic
processing of lung cancer resection specimens after neoadjuvant
therapy. Mod Pathol. 37:1003532024. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Alì G, Poma AM, Di Stefano I, Zirafa CC,
Lenzini A, Martinelli G, Romano G, Chella A, Baldini E, Melfi F and
Fontanini G: Different pathological response and histological
features following neoadjuvant chemotherapy or chemo-immunotherapy
in resected non-small cell lung cancer. Front Oncol.
13:11151562023. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Liu Z, Gao Z, Zhang M, Wang X, Gong J,
Jiang S and Zhang Z: Real-world effectiveness and prognostic
factors analysis of stages I–III non-small cell lung cancer
following neoadjuvant chemo-immunotherapy or neoadjuvant
chemotherapy. Ann Thorac Cardiovasc Surg. 28:111–120. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kalvapudi S, Vedire Y, Yendamuri S and
Barbi J: Neoadjuvant therapy in non-small cell lung cancer: Basis,
promise, and challenges. Front Oncol. 13:12861042023. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Bankhead P, Loughrey MB, Fernández JA,
Dombrowski Y, McArt DG, Dunne PD, McQuaid S, Gray RT, Murray LJ,
Coleman HG, et al: QuPath: Open source software for digital
pathology image analysis. Sci Rep. 7:168782017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Pataer A, Kalhor N, Correa AM, Raso MG,
Erasmus JJ, Kim ES, Behrens C, Lee JJ, Roth JA, Stewart DJ, et al:
Histopathologic response criteria predict survival of patients with
resected lung cancer after neoadjuvant chemotherapy. J Thorac
Oncol. 7:825–832. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kadota K, Nitadori JI, Sima CS, Ujiie H,
Rizk NP, Jones DR, Adusumilli PS and Travis WD: Tumor spread
through air spaces is an important pattern of invasion and impacts
the frequency and location of recurrences after limited resection
for small stage I lung adenocarcinomas. J Thorac Oncol. 10:806–814.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Ma R, Yang H, Ge Y, Ma T, Wang J, Li S,
Feng T, Feng S, Zhang C, Sun T, et al: Prognostic implications of
lymph node status in non-small-cell lung cancer patients before and
after neoadjuvant chemoimmunotherapy: A multicenter retrospective
study. Clin Lung Cancer. 26:370–383. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Chiappetta M, Tabacco D, Iaffaldano AG,
Evangelista J, Congedo MT, Sassorossi C, Meacci E, D'Argento E,
Bria E, Vita E, et al: Clinical stage III NSCLC patients treated
with neoadjuvant therapy and surgery: The prognostic role of nodal
characteristics. Life (Basel). 12:17532022.PubMed/NCBI
|
|
25
|
Huang S, Wu J, Li S, Li X, Zeng R, Tang Y,
Tang J, Ben X, Zhang D, Xie L, et al: Evaluation of combined
pathological responses in primary tumor and lymph nodes following
neoadjuvant chemoimmunotherapy in non-small cell lung cancer. Lung
Cancer. 186:1074012023. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Rojas F, Parra ER, Wistuba II, Haymaker C
and Solis Soto LM: Pathologic response and immune biomarker
assessment in non-small-cell lung carcinoma receiving neoadjuvant
immune checkpoint inhibitors. Cancers (Basel). 14:27752022.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Kim S, Lee J and Chung JH: Histological
assessment and interobserver agreement in major pathologic response
for non-small cell lung cancer with neoadjuvant therapy. Cancer Res
Treat. 57:401–411. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Banna GL, Hassan MA, Signori A, Giunta EF,
Maniam A, Anpalakhan S, Acharige S, Ghose A and Addeo A:
Neoadjuvant chemo-immunotherapy for early-stage non-small cell lung
cancer: A systematic review and meta-analysis. JAMA Netw Open.
7:e2468372024. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Junker K, Thomas M, Schulmann K, Klinke F,
Bosse U and Müller KM: Tumour regression in non-small-cell lung
cancer following neoadjuvant therapy. Histological assessment. J
Cancer Res Clin Oncol. 123:469–477. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Elsner F, Kümpers C, Ott G, Döring J,
Schildknecht K, Fisseler-Eckhoff A, von Laffert M, Baier L, Giulini
L, Kraus D, et al: Current practice of pathologic response
assessment following chemoimmunotherapy for non-small cell lung
cancer (NSCLC) in Germany: First real-world data from the
multicentre Re-GraDE study. Histopathology. 87:869–879. 2025.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Nie F, Wang Y, Shi W, Zhu L, Hao J and Tao
R: Prognosis prediction using significant pathological response
following neoadjuvant immunotherapy in resectable non-small-cell
lung tumors: A meta-analysis. Front Surg. 11:15005932024.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Qu Y, Emoto K, Eguchi T, Aly RG, Zheng H,
Chaft JE, Tan KS, Jones DR, Kris MG, Adusumilli PS and Travis WD:
Pathologic assessment after neoadjuvant chemotherapy for NSCLC:
Importance and implications of distinguishing adenocarcinoma from
squamous cell carcinoma. J Thorac Oncol. 14:482–493. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Wang H, Niu X, Jin Z, Zhang S, Fan R, Xiao
H and Hu SS: Immunotherapy resistance in non-small cell lung
cancer: From mechanisms to therapeutic opportunities. J Exp Clin
Cancer Res. 44:2502025. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Liu C, Chen Y, Xu X, Yin M, Zhang H and Su
W: Utilizing macrophages missile for sulfate-based nanomedicine
delivery in lung cancer therapy. Research (Wash D C).
7:04482024.PubMed/NCBI
|
|
35
|
Zhao L, Li M, Shen C and Luo Y, Hou X, Qi
Y, Huang Z, Li W, Gao L, Wu M and Luo Y: Nano-assisted radiotherapy
strategies: New opportunities for treatment of non-small cell lung
cancer. Research (Wash D C). 7:04292024.PubMed/NCBI
|
|
36
|
Roy SF, Louie AV, Liberman M, Wong P and
Bahig H: Pathologic response after modern radiotherapy for
non-small cell lung cancer. Transl Lung Cancer Res. 8 (Suppl
2):S124–S134. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Huynh C, Sorin M, Rayes R, Fiset PO, Walsh
LA and Spicer JD: Pathological complete response as a surrogate
endpoint after neoadjuvant therapy for lung cancer. Lancet Oncol.
22:1056–1058. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Dacic S, Travis WD, Giltnane JM, Kos F,
Abel J, Hilz S, Fujimoto J, Sholl L, Ritter J, Khalil F, et al:
Artificial intelligence-powered assessment of pathologic response
to neoadjuvant atezolizumab in patients with NSCLC: Results from
the LCMC3 study. J Thorac Oncol. 19:719–731. 2024. View Article : Google Scholar : PubMed/NCBI
|