Introduction
Cervical cancer is one of the most common cancers
among women globally, with an estimated 660,000 new cases and
350,000 deaths in 2022. Despite a decrease in incidence in
well-developed countries due to effective preventive screening
programs and vaccination, an estimated 13,360 new cases and 4,320
deaths from cervical cancer were reported in the U.S. in 2025
(1). Approximately 80–90% of
cervical cancers are squamous cell carcinomas (SCCs), and more than
90–95% of these tumors are related to high-risk human
papillomaviruses (HPVs), most commonly HPV16 and HPV18 (2,3). In
the majority of cases, high-risk HPV DNA integrates into the host
cell genome, resulting in persistent overexpression of the viral
oncoproteins E6 and E7, which subsequently inactivate tumor
suppressors p53 and RB1, respectively, and promote uncontrolled
cell growth, genomic instability, and tumor development (4).
The evolution of invasive SCCs from their precursor
lesions, namely, low-grade and high-grade squamous intraepithelial
lesions (LSIL and HSIL), occurs in a stepwise fashion, as
demonstrated in model systems (5).
While HPV-related inactivation of p53 and RB1 represents the
initial step of oncogenesis, somatic driver mutations accumulate as
the disease progresses from precancerous stages to invasive
carcinoma. Genome-wide analyses have revealed recurrent pathogenic
mutations in cervical carcinomas, including PIK3CA, EP300,
FBXW7, PTEN, HLA-A/B, ARID1A, NFE2L2, KRAS, ERBB2/3, and other
less common mutations (6,7). Among these genes, PIK3CA
mutations represent the most frequent genetic alteration in
cervical SCCs (6,7).
The PIK3CA gene encodes the p110α protein,
which is the catalytic subunit of the phosphoinositide 3-kinase
(PI3K) enzyme. PI3K is a lipid kinase generating lipid second
messengers, which subsequently activate AKT and mTOR signaling
cascades. This pathway is involved in numerous essential and
pathogenic cellular processes, including cell proliferation and
growth, survival, apoptosis, DNA damage repair, migration and
motility, angiogenesis, and cancer metastasis (8,9).
Mutations in PIK3CA lead to an overactive PI3K enzyme,
potentially contributing to cancer development, metastasis, and
therapeutic resistance. Notably, PIK3CA is one of the most
frequently mutated genes in cancer (9), with most mutations occurring in the
helical domain (exon 9) and the kinase domain (exon 20) (10). In cervical cancers, the reported
PIK3CA mutation rate varies widely, ranging from 8.15% to
60.0% (11–32), underscoring its potential role in
cervical cancer development and progression. While some studies
suggest that PIK3CA mutation confers favorable survival
outcomes, others have reported an association with poorer
prognosis. In a meta-analysis comprising 12 articles and 2,196
women with cervical cancer, the authors demonstrated that the
impact of PIK3CA mutations on survival outcomes remains
inconclusive (33). To minimize
confounding factors, we investigated the prevalence of
PIK3CA hotspot mutations in pathology-confirmed SCCs in a
single institution and correlated these mutations with
clinicopathological features.
Materials and methods
Case selection
In-house cases were identified from the pathology
archives of The Johns Hopkins Hospital between January 2000 and
August 2023 by searching for ‘squamous cell carcinoma’ and
‘cervix’. Patient demographics (including age and ethnicity),
clinical presentations and histories, procedures, gross specimen
descriptions, clinical courses, and follow-up information were
retrieved and reviewed from electronic medical records. Histologic
sections were independently re-reviewed by a board-certified
gynecologic pathologist (D.X.) to confirm the diagnosis. This study
was approved by the Institutional Review Board of The Johns Hopkins
Hospital (approval no. IRB00223822).
HPV in situ hybridization
In situ hybridization (ISH) was performed
using a high-risk HPV RNA probe solution (RNAscope, Advanced Cell
Diagnostics, Newark, CA; HPV types 16, 18, 26, 31, 33, 35, 39, 45,
51, 52, 53, 56, 58, 59, 66, 68, 73, 82) and type-specific probes
for HPV16 and HPV18 (RNAscope, Advanced Cell Diagnostics, Newark,
CA) (34). Additionally, ISHs for
wide-spectrum HPV DNA (cocktail of HPV 6, 11, 16, 18, 31, 33, 45,
51, 52, Dako, Carpinteria, CA), type-specific DNA probes for HPV16
and HPV18 (Dako, Carpinteria, CA), and high-risk HPV DNA (Ventana
INFORM HPV III family 16 probe, HPV genotypes: 16, 18, 31, 33, 35,
39, 45, 51, 52, 56, 58, 66, Ventana, Tucson, AZ) had been performed
on earlier cases at the time of diagnosis (35).
DNA extraction and polymerase chain
reaction (PCR) and Sanger sequencing to detect hotspot mutations of
the PIK3CA gene
DNA extraction was performed as described previously
(34). The following primers were
used to amplify PIK3CA exon 9, which includes hotspot mutations
E542K and E545K: PIK3CA-9F1: 5′-GGGAAAAATATGACAAAGAAAGC-3′;
PIK3CA-9F2: 5′-CAGAGTAACAGACTAGCTAG-3′; PIK3CA-9R1:
5′-GAGATCAGCCAAATTCAGTT-3′; PIK3CA-9R2:
5′-GAATCTCCATTTTAGCACTTAC-3′. The following primers were used to
amplify PIK3CA exon 20, which includes hotspot mutation H1047R:
PIK3CA-20F1: 5′-CTCTGGAATGCCAGAACTAC-3′; PIK3CA-20F2:
5′-ACATTCGAAAGACCCTAGCC-3′; PIK3CA-20R1:
5′-TGTGGAATCCAGAGTGAGCTT-3′; PIK3CA-20R2:
5′-CTTTTCAGTTCAATGCATGCTG-3′. First-round PCR amplification
(PIK3CA-9F1/PIK3CA-9R1; PIK3CA-20F1/PIK3CA-20R1) was performed
under the following conditions: an initial denaturation at 95°C for
2 min, followed by 30 cycles of 94°C for 30 sec, 51°C for 30 sec,
and 72°C for 45 sec, with a final elongation at 72°C for 7 min. PCR
products from the first round were diluted 10-fold and used as
templates for a second PCR amplification (nested PCR) using another
pair of primers (PIK3CA-9F2/PIK3CA-9R2; PIK3CA-20F2/PIK3CA-20R2).
The second round PCR was carried out under similar reaction
conditions except for an annealing temperature of 56°C. Sequencing
of the purified PCR products was performed using the ABI 3730
High-Throughput DNA Sequencer. Mutations and variations were
analyzed using Unipro UGENE software.
PD-L1 immunohistochemistry
Immunohistochemical staining for PD-L1 (mouse
monoclonal, 22C3; Dako/Agilent, Santa Clara, CA) was performed on
formalin-fixed, paraffin-embedded tissue sections as previously
described (36).
Semi-quantitative assessment of PD-L1
protein expression
PD-L1 protein expression was assessed using the
Combined Positive Score (CPS), which is calculated as the number of
PD-L1-positive cells (including tumor cells, lymphocytes, and
macrophages) relative to the total number of tumor cells (36).
Although the CPS can exceed 100, the maximum score
is defined as 100. PD-L1 expression was interpreted as follows: CPS
<1, no PD-L1 expression; CPS ≥1, PD-L1 expression. CPS was
independently assessed by three board-certified pathologists (J.M.,
C.S., and D.X.), and the average score with standard deviation was
calculated. PD-L1 protein expression was also evaluated using the
Tumor Proportion Score (TPS), which is calculated as the number of
PD-L1-positive tumor cells relative to the total number of tumor
cells (36).
Statistical analysis
Statistical methods were performed as described
previously (37). The χ2
test and Fisher's exact test were used to evaluate differences
between categorical variables. The Wilcoxon rank-sum test was used
to compare continuous variables. Prognostic factors predictive of
cause-specific survival (CSS) and overall survival (OS) were
analyzed using univariate and multivariate Cox proportional hazards
models. CSS and OS were calculated using the Kaplan-Meier method
and compared using the log-rank test. Statistical analyses were
performed with SAS version 9.4 (SAS Institute, Cary, NC, USA).
P<0.05 was considered to indicate a statistically significant
difference.
Results
PIK3CA hotspot mutations in cervical
squamous cell carcinomas
From 2000 to 2023, a total of 231 in-house cases of
invasive cervical SCC were identified, and PIK3CA hotspot
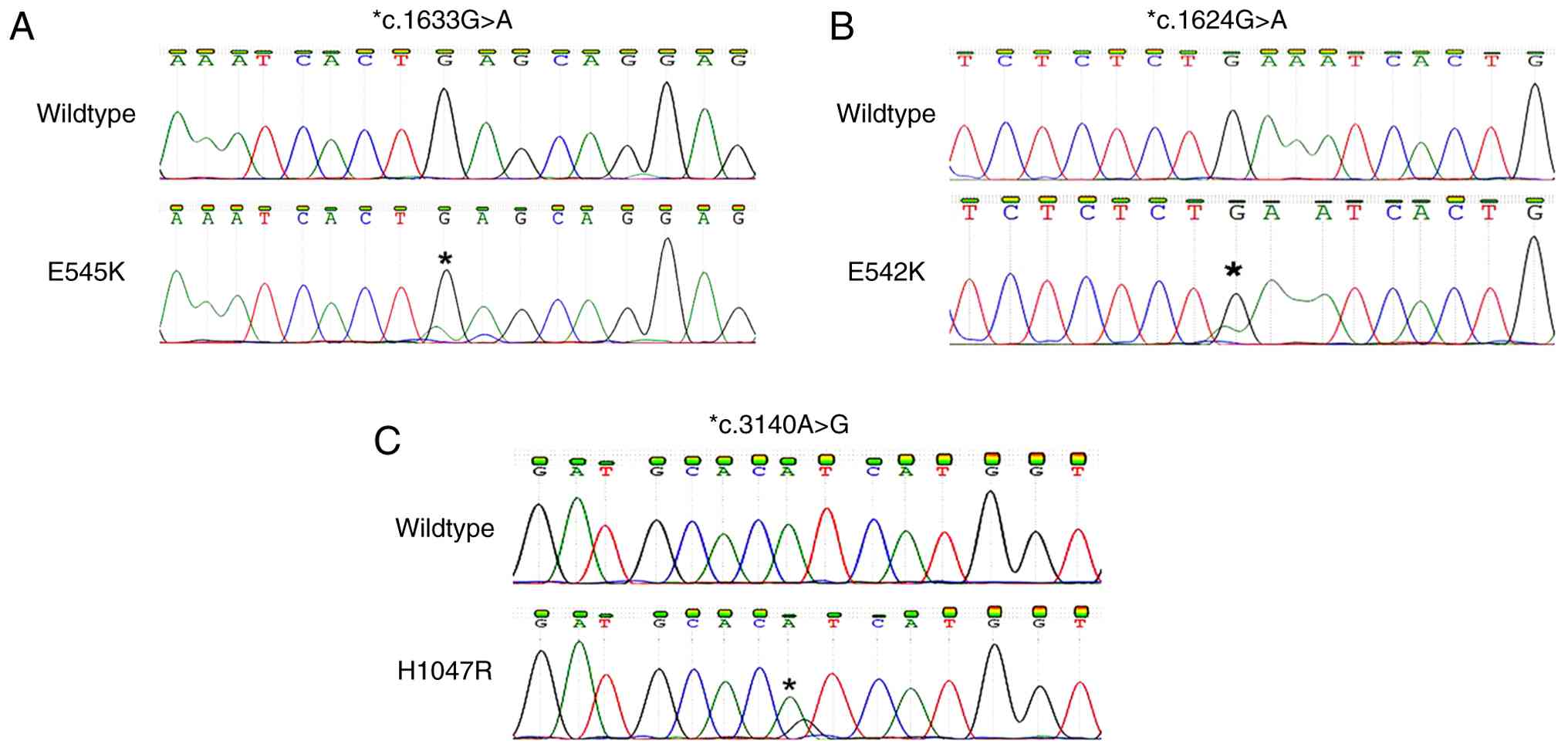
mutations were successfully analyzed in 207 cases. Sequencing of
purified PCR products detected PIK3CA exon 9 mutations in 26
(12.6%) of the 207 cases, including 21 cases with an E545K mutation
(Fig. 1A), 4 with an E542K mutation
(Fig. 1B), and 1 with a T544I
mutation. The H1047R hotspot mutation in exon 20 (Fig. 1C) was detected in only one case
(0.5%). In total, 27 cases (13.0%) harbored PIK3CA hotspot
mutations in this cohort. No case harbored two mutations.
Clinicopathological features of
PIK3CA-wildtype and PIK3CA-mutant tumors
Clinicopathological features are summarized in
Table I. In this cohort, patients
with cervical SCC ranged in age from 23 to 86 years (median, 48
years). A similar age range was observed among patients with
wild-type PIK3CA; in contrast, patients with mutant
PIK3CA tended to be older (median, 54 years, P=0.1976) and
ranged in age from 26 to 79 years. When stratified by age, the
mutation rate was significantly higher among patients aged ≥50
years compared with those <50 years [18/98 (18.4%) vs. 9/109
(8.3%); P=0.0310].
 | Table I.Clinicopathological
characteristics. |
Table I.
Clinicopathological
characteristics.
| Variable | Total |
PIK3CA-wildtype |
PIK3CA-mutant | P-value |
|---|
| N | 207 | 180 | 27 |
|
| Median age at
diagnosis, years (range) | 48 (23–86) | 48 (23–86) | 54 (26–79) | 0.1976 |
| Age, n |
|
|
| 0.0310 |
| <50
years | 109 | 100 | 9 |
|
| ≥50
years | 98 | 80 | 18 |
|
| Ethnicity, n |
|
|
| 0.9485 |
|
White | 106 | 92 | 14 |
|
|
Black | 74 | 64 | 10 |
|
|
Other | 27 | 24 | 3 |
|
| Clinical stage,
cases with available information, n | 179 | 155 | 24 |
|
| I | 74 | 69 | 5 |
|
| II | 33 | 28 | 5 |
|
|
III | 42 | 36 | 6 |
|
| IV | 30 | 22 | 8 | 0.0575 |
| I | 74 | 69 | 5 |
|
| II +
III + IV | 105 | 86 | 19 | 0.0284 |
| Procedure at
diagnosis, n |
|
|
| 0.4666 |
|
Biopsy | 101 | 85 | 16 |
|
|
Excision | 25 | 23 | 2 |
|
|
Hysterectomy | 81 | 72 | 9 |
|
| Chemo and/or
radiation, cases with available information, n | 188 | 164 | 24 | 0.0089 |
|
Yes | 139 | 116 | 23 |
|
| No | 49 | 48 | 1 |
|
| HPV infection,
cases with available information, n | 197 | 171 | 26 |
|
|
HPV16 | 90 | 76 | 14 |
|
|
HPV18 | 21 | 20 | 1 |
|
|
HPV-non16/18 | 64 | 56 | 8 |
|
| Not
detected | 22 | 19 | 3 | 0.6816 |
| Follow-up |
|
|
|
|
| N of
available follow-up | 198 | 173 | 25 |
|
| Median
follow-up time, months (range) | 30 (1–250) | 32 (1–250) | 24 (1–228) | 0.1972 |
Of the 207 patients, clinical staging information
was available in 179 cases, including 74 cases (41.3%) of stage I,
33 (18.4%) of stage II, 42 (23.5%) of stage III, and 30 (16.8%) of
stage IV disease. When stratified by stage, a trend toward a higher
frequency of PIK3CA mutations in patients with
advanced-stage disease was observed (P=0.0575), although the
difference did not reach statistical significance. The mutation
rate was 6.8% (5/74) among patients with stage I carcinoma,
increasing to 18.1% (19/105) among those with stage II or higher
disease (P=0.0284). Chemoradiation data were available for 188
patients, and nearly all PIK3CA-mutant patients (96%, 23/24)
underwent chemotherapy and/or radiation therapy (P=0.0089).
Regarding ethnicity and procedures performed at the
initial diagnosis, no statistically significant difference was
observed between PIK3CA-wildtype and PIK3CA-mutant
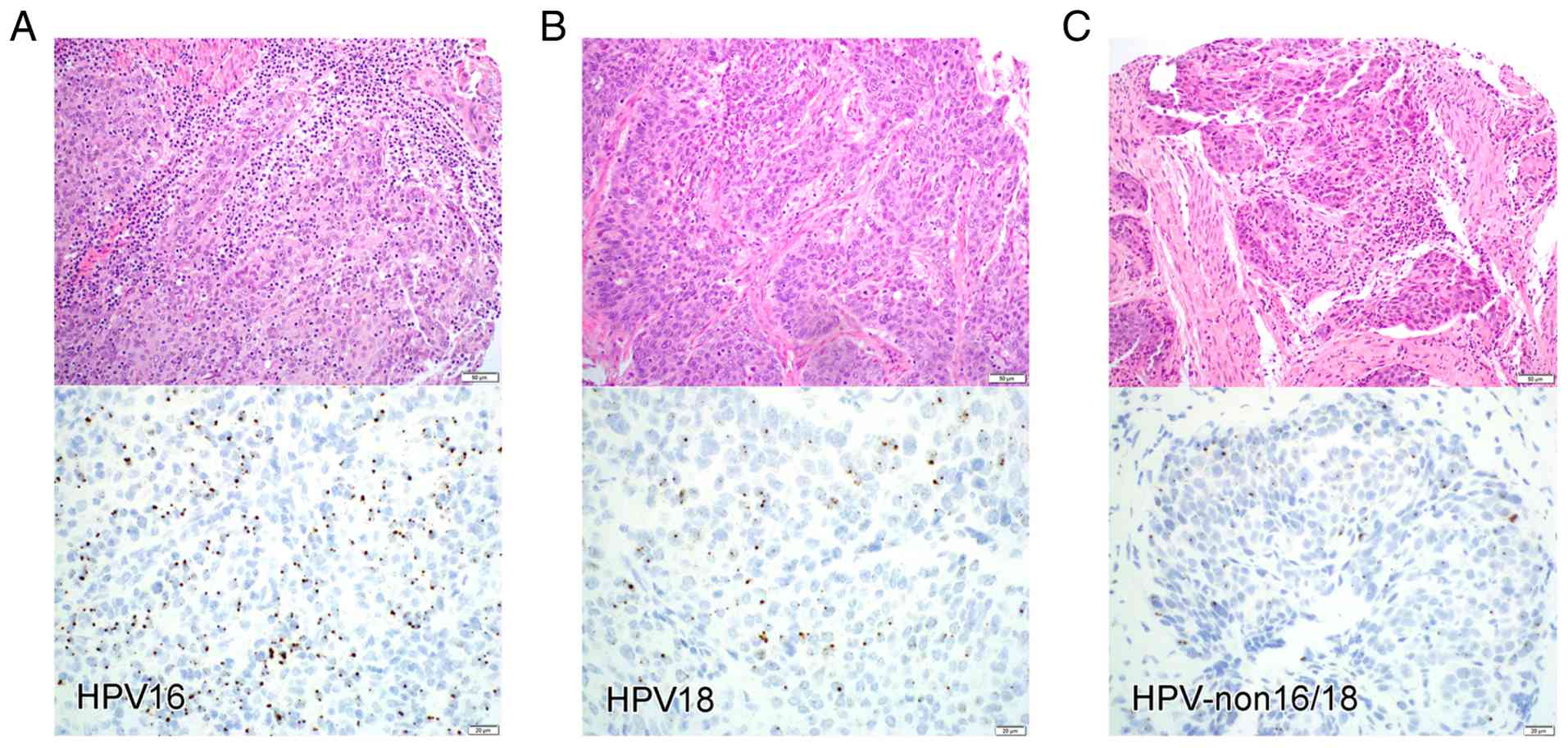
patients. Information on HPV infection was available in 197 cases,
of which 90 (45.7%, Fig. 2A) were
infected with HPV16, 21 (10.7%, Fig.
2B) with HPV18, and 64 (32.5%, Fig.
2C) with non-16/18 HPV subtypes. HPV signals were not detected
by ISH in 22 cases (11.1%). HPV status appeared to be unrelated to
PIK3CA mutation status (P=0.6816). Specifically, 14 mutant
cases were infected with HPV16, 1 with HPV18, and 8 with non-16/18
HPV subtypes.
PD-L1 expression in PIK3CA-wildtype
and PIK3CA-mutant cases
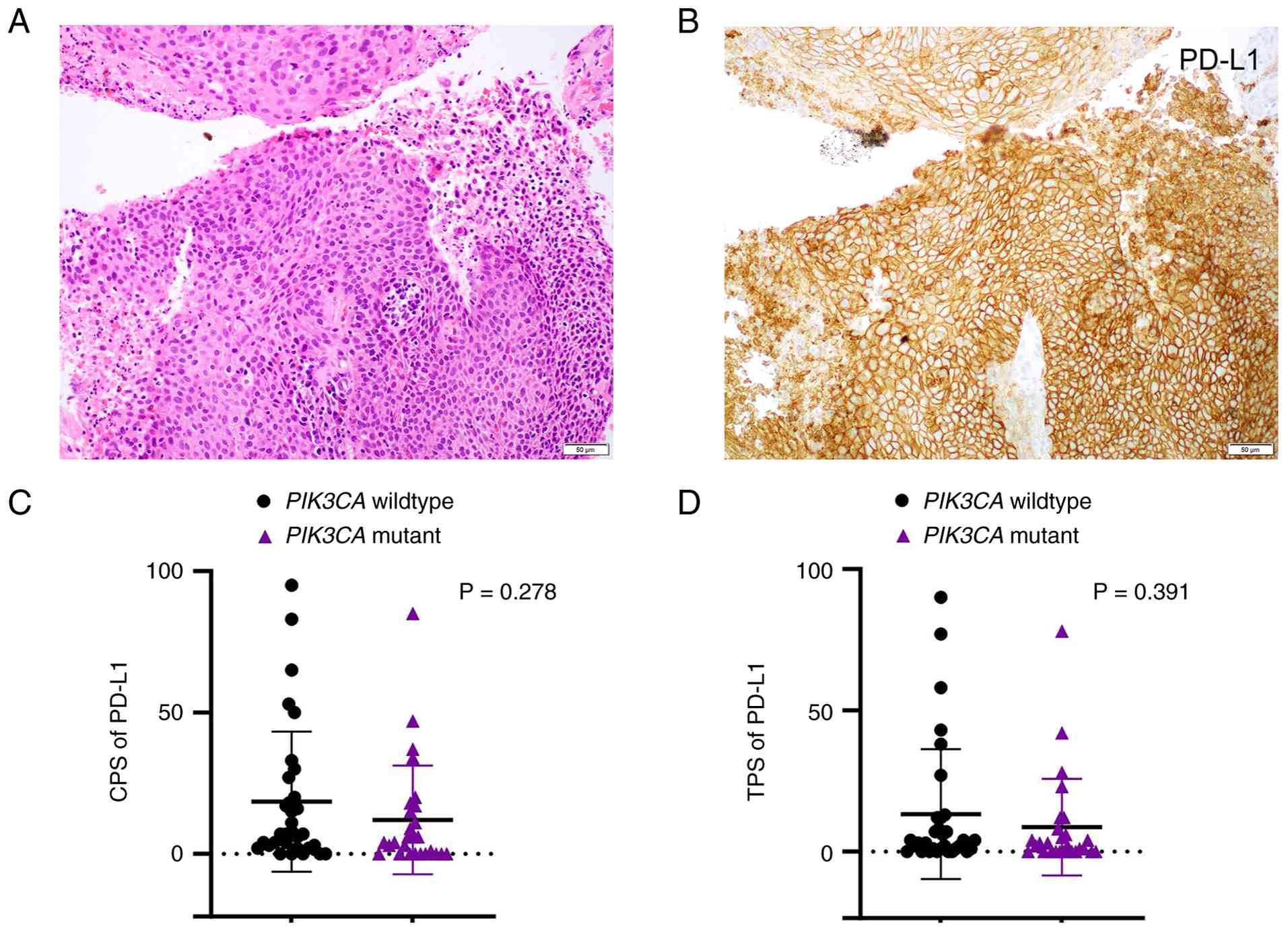
A total of 59 cases (32 PIK3CA-wildtype and 27
PIK3CA-mutant) were tested for PD-L1 expression and then evaluated
using both CPS and TPS. PD-L1 expression (CPS ≥1) was observed in
45 of 59 (76.3%) cervical SCCs (Fig. 3A
and B), while 14 tumors showed no PD-L1 expression. In the
PIK3CA-wildtype group, CPS values ranged from 0 to 95 (mean,
18.50), whereas in the PIK3CA-mutant group, scores ranged from 0 to
85 (mean, 12.07). No statistically significant difference was
observed between the two groups (P=0.2784; Fig. 3C). Similarly, TPS values did not
differ significantly between PIK3CA-wildtype and PIK3CA-mutant
cases (mean TPS: 13.31 vs. 8.67; P=0.3907; Fig. 3D).
Prognostic factors
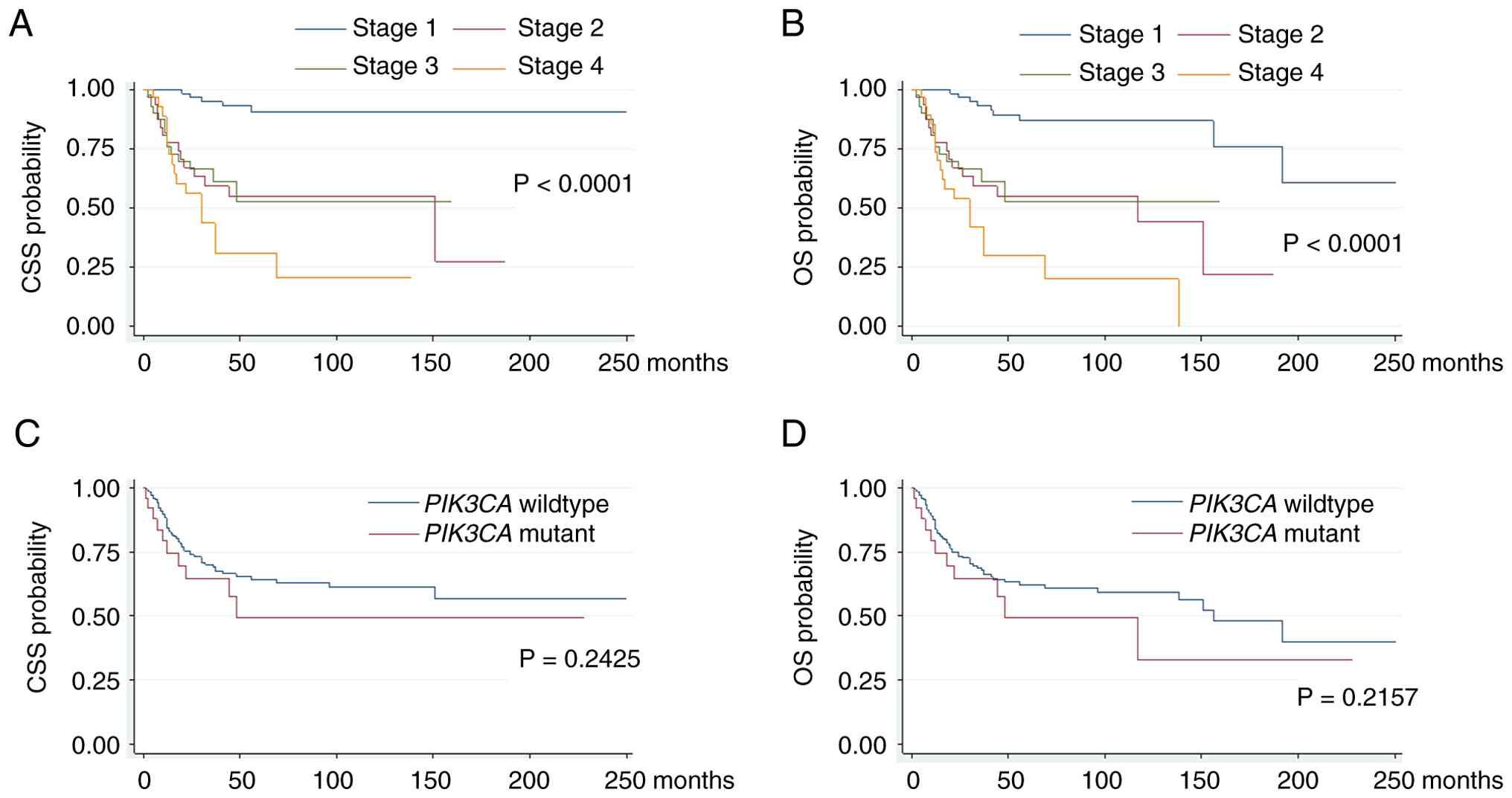
Among the clinicopathological variables analyzed in
this cervical SCC cohort, the only factor significantly associated
with CSS by both univariate and multivariate analyses was clinical
stage (Table II). Age, ethnicity,
and HPV subtype were not associated with clinical outcome or
prognosis. Although the presence of a PIK3CA mutation was
correlated with older age and higher disease stage, it was not an
independent prognostic factor for CSS. Similarly, both univariate
and multivariate analyses indicated that clinical stage, but not
age, HPV subtype, or PIK3CA mutation, was associated with OS
(Table III). While Black patients
showed poorer OS in the univariate analysis [hazard ratio (HR),
1.689; 95% confidence interval (CI), 1.047–2.724], ethnicity was no
longer an independent prognostic factor in the multivariate
analysis (HR, 1.242; 95% CI, 0.717–2.152). Consistently,
Kaplan-Meier plots (Fig. 4)
demonstrated significant differences in both CSS and OS according
to clinical stage. However, no statistically significant
differences were observed between PIK3CA mutation status and
either CSS or OS.
| Table II.Univariate and multivariate analysis
of hazard ratio of cause specific survival. |
Table II.
Univariate and multivariate analysis
of hazard ratio of cause specific survival.
|
| Univariate | Multivariate |
|---|
|
|
|
|
|---|
| Variable | Hazard ratio | P-value | Hazard ratio | P-value |
|---|
| Age at
diagnosis | 0.994 (0.976,
1.013) | 0.5272 | 0.985 (0.965,
1.005) | 0.1379 |
| Ethnicity |
|
|
|
|
|
White | Reference |
| Reference |
|
|
Black | 1.464 (0.876,
2.448) | 0.1459 | 1.069 (0.592,
1.931) | 0.8249 |
|
Other | 0.821 (0.352,
1.917) | 0.6488 | 0.381 (0.128,
1.134) | 0.0830 |
| Clinical stage |
|
|
|
|
| I | Reference |
| Reference |
|
| II | 8.171 (2.981,
22.393) | <0.0001 | 5.131 (1.445,
18.218) | 0.0114 |
|
III | 8.239 (3.010,
22.555) | <0.0001 | 5.519 (1.530,
19.914) | 0.0091 |
| IV | 14.130 (5.460,
36.567) | <0.0001 | 7.279 (2.181,
24.293) | 0.0012 |
| HPV infection |
|
|
|
|
|
HPV16 | Reference |
| Reference |
|
|
HPV18 | 0.301 (0.077,
1.170) | 0.0830 | 0.433 (0.094,
1.997) | 0.2828 |
|
HPV-non16/18 | 1.117 (0.667,
1.868) | 0.6742 | 1.132 (0.590,
2.169) | 0.7097 |
| PIK3CA |
|
|
|
|
|
Wildtype | Reference |
| Reference |
|
|
Mutant | 1.497 (0.761,
2.947) | 0.2425 | 1.309 (0.610,
2.808) | 0.4887 |
| Table III.Univariate and multivariate analysis
of hazard ratio of overall survival. |
Table III.
Univariate and multivariate analysis
of hazard ratio of overall survival.
|
| Univariate | Multivariate |
|---|
|
|
|
|
|---|
| Variable | Hazard ratio | P-value | Hazard ratio | P-value |
|---|
| Age at
diagnosis | 1.002 (0.986,
1.019) | 0.7877 | 0.996 (0.977,
1.015) | 0.6688 |
| Ethnicity |
|
|
|
|
|
White | Reference |
| Reference |
|
|
Black | 1.689 (1.047,
2.724) | 0.0316 | 1.242 (0.717,
2.152) | 0.4398 |
|
Others | 0.817 (0.348,
1.915) | 0.6413 | 0.394 (0.129,
1.200) | 0.1010 |
| Clinical stage |
|
|
|
|
| I | Reference |
| Reference |
|
| II | 5.791 (2.497,
13.427) | <0.0001 | 3.110 (1.213,
7.977) | 0.0182 |
|
III | 5.707 (2.399,
13.574) | <0.0001 | 3.102 (1.176,
8.180) | 0.0221 |
| IV | 11.100 (5.198,
23.705) | <0.0001 | 4.672 (1.974,
11.059) | 0.0005 |
| HPV infection |
|
|
|
|
|
HPV16 | Reference |
| Reference |
|
|
HPV18 | 0.282 (0.073,
1.095) | 0.0675 | 0.433 (0.100,
1.876) | 0.2631 |
|
HPV-non16/18 | 1.108 (0.676,
1.818) | 0.6836 | 1.057 (0.567,
1.969) | 0.8625 |
| PIK3CA |
|
|
|
|
|
Wildtype | Reference |
| Reference |
|
|
Mutant | 1.498 (0.790,
2.842) | 0.2157 | 1.229 (0.615,
2.456) | 0.5591 |
Discussion
In this study, we characterized the
clinicopathological features of cervical SCC with PIK3CA
mutations at a single institution, focusing primarily on the most
common PIK3CA mutations in the helical domain (exon 9, E542K
and E545K) and the kinase domain (exon 20, H1047R) (10,33).
We found that the prevalence of PIK3CA hotspot mutations in
this cohort was 13%, consistent with findings from several previous
studies (6,11,20,24).
However, our reported mutation rate is relatively lower than that
observed in most other studies. The reasons for these differences
remain unclear; however, Sanger sequencing of PIK3CA hotspot
mutations, unlike next-generation sequencing, may underestimate the
overall mutation rate, as these hotspot mutations account for
approximately 80% of all mutations in the gene (10,24,38,39).
Other possible contributing factors include age distribution,
ethnic heterogeneity, differences in tumor stage, and degradation
of genomic material in archival formalin-fixed, paraffin-embedded
(FFPE) tissues (11).
As an oncogene regulating the PI3K/AKT/mTOR pathway,
PIK3CA is one of the most frequently mutated genes in human
cancers. Consistent with previous investigations (11,16–18,24,38),
we found that 96.3% (26/27) of mutations were clustered in the
helical domain (exon 9), whereas only one case (3.7%) harbored
H1047R, a mutation in the kinase domain (exon 20). Our findings in
cervical cancer, as well as the findings in previous investigations
(7), are similar to results
reported in bladder cancer (40)
and HPV-associated head and neck cancers (41) but differ from observations in breast
(42), endometrial (43), and many other cancers, which
predominantly harbor PIK3CA mutations in the kinase domain.
This distinct mutation profile may reflect the difference in
etiology, cell-of-origin, and oncogenic mechanisms across different
cancers (44,45). The helical domain of the PIK3CA
protein (p110α) has been shown to function as a scaffold that
biochemically interacts with the inhibitory p85α protein. Somatic
mutations in this domain disrupt the inhibitory interface between
the p110α catalytic subunit and the p85α regulatory subunit,
releasing the enzyme from normal inhibitory control and resulting
in enzymatic overactivity. This overactivity mimics a
growth-factor-activated state and is highly dependent on the
Ras-binding domain. In contrast, mutations in the kinase domain
alter the protein's conformation, enhancing its affinity for
substrates on the cell membrane, which increases kinase activity.
This pathway functions independently of Ras. Regardless of the
mutation sites, these variants directly affect the PI3K enzyme,
leading to overactive AKT and subsequent mTOR activity, which
promotes tumor growth, proliferation, and resistance to certain
therapies. Given their different oncogenic potential and
context-dependent crosstalk, mutations in the helical domain and
kinase domain may respond differently to inhibitors (46–48), a
factor that should be considered when designing targeted therapies
for cervical SCC.
In this cohort, patients with mutant PIK3CA
tended to be older, and the mutation rate was significantly higher
among those aged ≥50 years compared with those <50 years (18.4%
vs. 8.3%, P=0.031). Because more than half of the patients were
younger than 50 years, this age distribution may partly explain the
relatively low PIK3CA mutation rate observed in this study.
A similar correlation between age and PIK3CA mutational
status has been consistently reported in several studies (11,24),
although the reason for this association remains unclear.
Interestingly, although less common than the H1047R kinase domain
mutation, helical domain hotspot mutations in breast cancer have
also been associated with older age at diagnosis (P=0.004)
(49). These observations in
cervical SCC and breast cancer may highlight an age-associated link
in the pathogenesis of PIK3CA helical domain hotspot
mutations.
Although most studies have reported no correlation
between PIK3CA mutations and tumor stage (16,20,24),
our results showed that patients with higher-stage disease tended
to harbor mutant PIK3CA (P=0.0575). When stratified by
stage, patients with stage II or higher tumors had a significantly
higher frequency of PIK3CA mutations than those with stage I
tumors (P=0.0284). Consistent with their higher stage, nearly all
PIK3CA-mutant patients (96%) in this cohort underwent
chemotherapy and/or radiation therapy (P=0.0089). Another study
also observed a similar trend between PIK3CA mutations and
pT2-T3 staging, although the difference did not reach statistical
significance (P=0.078) (23).
PIK3CA somatic mutations have been postulated to represent a
late event in cervical carcinogenesis, as these mutations are
rarely detected in cervical intraepithelial neoplasia (38).
Some studies have reported an association between
PIK3CA mutations and HPV16 infection (50). Consistent with previous studies
(7), HPV16 was the most common HPV
subtype among cervical SCCs in this cohort. However, our results
indicated that HPV status was not associated with PIK3CA
mutations. Although one study reported that American Indian and
Alaska Native populations have the highest rate of PIK3CA
mutations in cervical cancer (32),
statistical analyses have shown no significant differences in
PIK3CA mutation frequency by ethnicity, consistent with our
findings.
Compared with single-agent chemotherapy,
PD-1-blocking antibody-based immunotherapy significantly improves
survival among patients with recurrent cervical cancer following
first-line platinum-containing treatment (51). One study reported that PIK3CA
mutations lead to increased mRNA and protein expression of PD-L1 in
cervical cancer (52). To
investigate the relationship between PD-L1 expression and
PIK3CA mutation, we analyzed 59 cases of cervical SCC (32
PIK3CA wild-type and 27 PIK3CA-mutant). Consistent
with previous studies (51), PD-L1
expression (CPS ≥1) was observed in 76.3% of cervical SCCs.
However, immunohistochemical analysis did not reveal a
statistically significant association between PD-L1 expression and
PIK3CA mutation. These findings suggest that in vivo
PD-L1 expression may be regulated by complex mechanisms involving
diverse genetic and epigenetic alterations. Notably, although PD-L1
expression was observed in more than 75% of samples in our series,
the lack of correlation with PIK3CA mutational status may
reflect the limited sample size (n=59), resulting in an
underpowered subset analysis. Future studies involving all cases,
with evaluation of PD-L1 expression and assessment of its
relationship with clinical outcomes, are warranted.
In our study, PIK3CA mutations were not
associated with the prognosis of cervical SCCs. The only factor
significantly correlated with the CSS and OS in this cohort was
clinical stage. PIK3CA plays a well-established role in
carcinogenesis; although its prognostic significance in cervical
SCC has been extensively investigated, the results remain
controversial. Some studies, including the largest to date (771
cases), have reported that the presence of PIK3CA mutations
is associated with significantly better clinical outcomes (11–15),
whereas others have identified PIK3CA mutations as a poor
prognostic factor linked to unfavorable survival (16–20).
In contrast, several investigations, including the present study,
have demonstrated no association between PIK3CA mutations
and survival outcomes (21–25). Multiple factors, including tumor
stage, patient demographics, mutation subtype, and treatment
modalities, may contribute to these discrepancies. Interestingly,
in a phase II study evaluating the long-term efficacy and survival
outcomes of sintilimab (a monoclonal antibody targeting PD-1) in
combination with anlotinib (a multikinase inhibitor with broad
inhibitory effects on tumor angiogenesis and growth) in patients
with PD-L1-positive recurrent or metastatic cervical cancer,
PIK3CA mutation was identified as an independent favorable
prognostic factor for OS (15).
Similarly, another phase II study demonstrated that patients with
PIK3CA mutations treated with camrelizumab (a PD-1
inhibitor) in combination with apatinib (a vascular endothelial
growth factor receptor-2 inhibitor) experienced significantly
improved progression-free survival and OS (12,14).
These clinical trial-based studies suggest that activation of the
PI3K/AKT/mTOR pathway through PIK3CA mutation may represent
a promising indicator for response to immunotherapy.
However, our study has certain limitations. First,
as mentioned above, targeted Sanger sequencing of PIK3CA
hotspot mutations may underestimate the overall mutation rate. This
Sanger sequencing-based analysis is limited by its sensitivity in
detecting mutant allele frequencies of approximately 80 to 85%,
which may miss a subset of low-level mosaic mutations below 15 to
20% (53,54). Ideally, next-generation sequencing
should be used to investigate the mutational profile in these
tumors. The application of advanced molecular techniques not only
allows for a thorough investigation of all possible pathogenic
mutations across the entire PIK3CA gene but also helps identify a
mutational landscape that may involve other key genes in the
PI3K/AKT/mTOR pathway or crosstalk with other carcinogenic pathways
(21,26). Second, although a single-institution
study with a sizable case number and centralized pathology review
helps minimize heterogeneity in patient population and tumor
characteristics, our findings may still be influenced by local
variations in patient demographics and treatment approaches,
thereby reducing generalizability. Regional and demographic
differences may affect mutation frequencies and clinical outcomes.
Notably, 41.3% of patients in this cohort had stage I disease, and
most were cured after treatment at our tertiary care center. The
high proportion of stage I patients and the relatively low
frequency of PIK3CA mutations in this group may have
confounded the analysis of survival outcomes. Third, in addition to
somatic mutations, PIK3CA gene expression and copy number
variation may also affect the downstream pathway. These alterations
were not investigated in our cases. Although the relationship
between PIK3CA gene expression and mutation has been
reported, the findings remain inconclusive (55,56).
Given its clinicopathological focus, the functional validation of
PIK3CA gene expression and mutations was not performed in this
study. Future studies incorporating these analyses may provide a
more comprehensive understanding of the role of the PI3K/AKT/mTOR
pathway in cervical cancer development, progression, and treatment.
Finally, as with other retrospective studies, selection bias may be
present in our cohort due to reliance on existing clinical data. In
particular, therapeutic strategy may have varied over time,
contributing to treatment heterogeneity.
In summary, despite certain limitations, our study
highlights and expands upon the clinicopathological characteristics
of cervical SCCs with PIK3CA hotspot mutations within a
single-institution cohort. We further demonstrate that
PIK3CA helical domain mutations are more frequently observed
in tumors from older patients and are associated with higher tumor
stage. Nearly all patients harboring PIK3CA mutations
underwent chemoradiation therapy; however, the mutation was not an
independent prognostic factor in this cohort. Additionally, PD-L1
expression appears to be unrelated to PIK3CA mutational
status. Future studies should focus on evaluating the efficacy of
PI3K inhibitors alone or in combination with immunotherapy and
other targeted treatments in selected patients, based on molecular
alterations that may predict therapeutic benefit.
Acknowledgments
The authors would like to thank Ms. Melanie Vukovich
(Department of Pathology, The Johns Hopkins Medical Institutions)
for their assistance with manuscript editing and preparation.
Funding
Thus study was supported by the National Institutes of Health
(NIH, Bethesda, MD) T-32 Postdoctoral Research Training Grant
[grant no. 5T32CA193145 (J.M.)]; the Eggleston Award in the
Department of Pathology at The Johns Hopkins Hospital (H.K.); the
NIH and the National Cancer Institute (Bethesda, MD) for the
Cervical Cancer Specialized Programs of Research Excellence (SPORE)
program [grant no. P50CA098252 (T.-C. Wu)]; and the Pilot Project
Award by the Cervical Cancer SPORE program at The Johns Hopkins
Hospital (D.X.)
Availability of data and materials
The PIK3CA gene mutational profile data
generated in the present study may be found in the NCBI ClinVar
database under accession numbers SCV007346396, SCV007346397,
SCV007346398 and SCV007346399 or at the following URLs: https://www.ncbi.nlm.nih.gov/clinvar/variation/13655/?term=SCV007346396;
https://www.ncbi.nlm.nih.gov/clinvar/variation/31944/?term=SCV007346397;
https://www.ncbi.nlm.nih.gov/clinvar/variation/4690213/?term=SCV007346398;
https://www.ncbi.nlm.nih.gov/clinvar/variation/13652/?term=SCV007346399.
The other data generated in the present study may be requested from
the corresponding author.
Authors' contributions
JM, HK, CS, TCW and DX conceived and designed the
study, and participated in acquisition of data. JM, HK, CS, AAW,
LSFW, YCT, CFH, TCW and DX participated in ancillary analysis
(Sanger sequencing and immunohistochemistry) and interpretation of
data. DX wrote the draft of the manuscript. JM, HK, CS, LSFW, TCW
and DX reviewed and revised the manuscript. TCW and DX supervised
the study. JM and DX confirm the authenticity of all the raw data.
All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Institutional Review
Board at The Johns Hopkins University/Hospital (approval no.
IRB00223822). Patient consent was waived by JHU IRB policy since
this is minimal-risk research using/involving secondary material
for which consent is not required.
Patient consent for publication
Not applicable.
Competing interests
Not applicable.
References
|
1
|
Siegel RL, Kratzer TB, Giaquinto AN, Sung
H and Jemal A: Cancer statistics, 2025. CA Cancer J Clin. 75:10–45.
2025.PubMed/NCBI
|
|
2
|
de Sanjose S, Quint WG, Alemany L, Geraets
DT, Klaustermeier JE, Lloveras B, Tous S, Felix A, Bravo LE, Shin
HR, et al: Human papillomavirus genotype attribution in invasive
cervical cancer: A retrospective cross-sectional worldwide study.
Lancet Oncol. 11:1048–1056. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
WHO Classification of Tumours Editorial
Board, . WHO Classification of Tumours: Female Genital Tumours. 5th
edition. Volume 4. International Agency for Research on Cancer
Publications; Lyon, France: pp. 347–349. 2020
|
|
4
|
Yeo-Teh NSL, Ito Y and Jha S: High-risk
human papillomaviral oncogenes E6 and E7 target key cellular
pathways to achieve oncogenesis. Int J Mol Sci. 19:17062018.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Henkle TR, Lam B, Kung YJ, Lin J, Tseng
SH, Ferrall L, Xing D, Hung CF and Wu TC: Development of a novel
mouse model of spontaneous high-risk HPVE6/E7-expressing carcinoma
in the cervicovaginal tract. Cancer Res. 81:4560–4569. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ojesina AI, Lichtenstein L, Freeman SS,
Pedamallu CS, Imaz-Rosshandler I, Pugh TJ, Cherniack AD, Ambrogio
L, Cibulskis K, Bertelsen B, et al: Landscape of genomic
alterations in cervical carcinomas. Nature. 506:371–375. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Cancer Genome Atlas Research Network;
Albert Einstein College of Medicine; Analytical Biological
Services; Barretos Cancer Hospital; Baylor College of Medicine;
Beckman Research Institute of City of Hope; Buck Institute for
Research on Aging; Canada's Michael Smith Genome Sciences Centre;
Harvard Medical School, . Helen F, et al: Integrated genomic and
molecular characterization of cervical cancer. Nature. 543:378–384.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Wang Y, Rozen V, Zhao Y and Wang Z:
Oncogenic activation of PI K3 CA in cancers: Emerging targeted
therapies in precision oncology. Genes Dis. 12:1014302025.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Arafeh R and Samuels Y: PIK3CA in cancer:
The past 30 years. Semin Cancer Biol. 59:36–49. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Samuels Y, Wang Z, Bardelli A, Silliman N,
Ptak J, Szabo S, Yan H, Gazdar A, Powell SM, Riggins GJ, et al:
High frequency of mutations of the PIK3CA gene in human cancers.
Science. 304:5542004. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Xiang L, Jiang W, Li J, Shen X, Yang W,
Yang G, Wu X and Yang H: PIK3CA mutation analysis in Chinese
patients with surgically resected cervical cancer. Sci Rep.
5:140352015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Huang X, He M, Peng H, Tong C, Liu Z,
Zhang X, Shao Y, Zhu D, Zhang J and Yin JC: Genomic profiling of
advanced cervical cancer to predict response to programmed death-1
inhibitor combination therapy: A secondary analysis of the CLAP
trial. J Immunother Cancer. 9:e0022232021. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hou MM, Liu X, Wheler J, Naing A, Hong D,
Coleman RL, Tsimberidou A, Janku F, Zinner R, Lu K, et al: Targeted
PI3K/AKT/mTOR therapy for metastatic carcinomas of the cervix: A
phase I clinical experience. Oncotarget. 5:11168–11179. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lan C, Lu H, Zhou L, Liao K, Liu J, Xie Z,
Liang H, Zou G, Yang T, Xu Q and Huang X: Long-term survival
outcomes and immune checkpoint inhibitor retreatment in patients
with advanced cervical cancer treated with camrelizumab plus
apatinib in the phase II CLAP study. Cancer Commun (Lond).
44:654–669. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Liu J, Lan C, Liu T, Liu Q, Chang L, Zang
L, Zhu F, Zhu M, Zhang H, Kang Y, et al: Long-term efficacy and
updated survival outcomes of sintilimab plus anlotinib in patients
with PD-L1-positive recurrent or metastatic cervical cancer. BMC
Med. 23:3692025. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Chung TKH, Cheung TH, Yim SF, Yu MY, Chiu
RWK, Lo KWK, Lee IPC, Won RRY, Lau KKM, Wang VW, et al: Liquid
biopsy of PIK3CA mutations in cervical cancer in Hong Kong Chinese
women. Gynecol Oncol. 146:334–339. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wright AA, Howitt BE, Myers AP, Dahlberg
SE, Palescandolo E, Van Hummelen P, MacConaill LE, Shoni M, Wagle
N, Jones RT, et al: Oncogenic mutations in cervical cancer: Genomic
differences between adenocarcinomas and squamous cell carcinomas of
the cervix. Cancer. 119:3776–3783. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
McIntyre JB, Wu JS, Craighead PS, Phan T,
Kobel M, Lees-Miller SP, Ghatage P, Magliocco AA and Doll CM:
PIK3CA mutational status and overall survival in patients with
cervical cancer treated with radical chemoradiotherapy. Gynecol
Oncol. 128:409–414. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Martell K, McIntyre JB, Kornaga EN, Chan
AMY, Phan T, Kobel M, Enwere EK, Dean ML, Ghatage P, Lees-Miller SP
and Doll CM: PIK3CA mutation and CNV status and
post-chemoradiotherapy survival in patients with cervical cancer.
Gynecol Oncol. 158:776–784. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Lachkar B, Minaguchi T, Akiyama A, Liu S,
Zhang S, Xu C, Shikama A, Tasaka N, Sakurai M, Nakao S, et al:
Prognostic significance of PIK3CA mutation in stage IIB to IVA
cervical cancers treated by concurrent chemoradiotherapy with
weekly cisplatin. Medicine (Baltimore). 97:e113922018. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Yoshimoto Y, Sasaki Y, Murata K, Noda SE,
Miyasaka Y, Hamamoto J, Furuya M, Hirato J, Suzuki Y, Ohno T, et
al: Mutation profiling of uterine cervical cancer patients treated
with definitive radiotherapy. Gynecol Oncol. 159:546–553. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Spaans VM, Trietsch MD, Peters AA, Osse M,
Ter Haar N, Fleuren GJ and Jordanova ES: Precise classification of
cervical carcinomas combined with somatic mutation profiling
contributes to predicting disease outcome. PLoS One.
10:e01336702015. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Martell K, McIntyre JB, Abedin T, Kornaga
EN, Chan AMY, Enwere E, Köbel M, Dean ML, Phan T, Ghatage P, et al:
Prevalence and prognostic significance of PIK3CA mutation and CNV
status and phosphorylated AKT expression in patients with cervical
cancer treated with primary surgery. Int J Gynecol Pathol.
43:158–170. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Cui B, Zheng B, Zhang X, Stendahl U,
Andersson S and Wallin KL: Mutation of PIK3CA: Possible risk factor
for cervical carcinogenesis in older women. Int J Oncol.
34:409–416. 2009.PubMed/NCBI
|
|
25
|
Voutsadakis IA: PI3KCA mutations in
uterine cervix carcinoma. J Clin Med. 10:2202021. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Rose MM, Dhamodharan S, Revathidevi S,
Chakkarappan SR, Jagadeesan MG, Subbiah S, Nakaoka H, Inoue I,
Murugan AK and Munirajan AK: High incidence of PI3K pathway gene
mutations in South Indian cervical cancers. Cancer Genet.
264-265:100–108. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Lou H, Villagran G, Boland JF, Im KM, Polo
S, Zhou W, Odey U, Juárez-Torres E, Medina-Martínez I,
Roman-Basaure E, et al: Genome analysis of latin american cervical
cancer: Frequent activation of the PIK3CA pathway. Clin Cancer Res.
21:5360–5370. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Friedman CF, Ravichandran V, Miller K,
Vanderbilt C, Zhou Q, Iasonos A, Vivek M, Mishra P, Leitao MM Jr,
Broach V, et al: Assessing the genomic landscape of cervical
cancers: Clinical opportunities and therapeutic targets. Clin
Cancer Res. 29:4660–4668. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Bao C, An N, Xie H, Xu L, Zhou B, Luo J,
Huang W and Huang J: Identifying potential neoantigens for cervical
cancer immunotherapy using comprehensive genomic variation
profiling of cervical intraepithelial neoplasia and cervical
cancer. Front Oncol. 11:6723862021. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Kim YN, Lee K, Park E, Park J, Lee YJ, Nam
EJ, Kim SW, Kim S, Kim YT and Lee JY: Comprehensive genomic and
immunohistochemical profiles and outcomes of immunotherapy in
patients with recurrent or advanced cervical cancer. Front Oncol.
13:11569732023. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Qiu L, Feng H, Yu H, Li M, You Y, Zhu S,
Yang W, Jiang H and Wu X: Characterization of the genomic landscape
in cervical cancer by next generation sequencing. Genes (Basel).
13:2872022. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Femi OF: Genetic alterations and PIK3CA
gene mutations and amplifications analysis in cervical cancer by
racial groups in the United States. Int J Health Sci (Qassim).
12:28–32. 2018.PubMed/NCBI
|
|
33
|
Pergialiotis V, Nikolaou C, Haidopoulos D,
Frountzas M, Thomakos N, Bellos I, Papapanagiotou A and Rodolakis
A: PIK3CA mutations and their impact on survival outcomes of
patients with cervical cancer: A systematic review. Acta Cytol.
64:547–555. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Xing D, Zheng G, Schoolmeester JK, Li Z,
Pallavajjala A, Haley L, Conner MG, Vang R, Hung CF, Wu TC and
Ronnett BM: Next-generation sequencing reveals recurrent somatic
mutations in small cell neuroendocrine carcinoma of the uterine
cervix. Am J Surg Pathol. 42:750–760. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Xing D, Schoolmeester JK, Ren Z, Isacson C
and Ronnett BM: Lower female genital tract tumors with adenoid
cystic differentiation: P16 expression and high-risk HPV detection.
Am J Surg Pathol. 40:529–536. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Xing D, Liu Y, Park HJ, Baek I, Tran H,
Cheang G, Novo J, Dillon J, Matoso A, Farmer E, et al: Recurrent
genetic alterations and biomarker expression in primary and
metastatic squamous cell carcinomas of the vulva. Hum Pathol.
92:67–80. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Xing D and Lu J: Distinctive
clinicopathological features and disease-specific survival of
adenoid cystic carcinoma and adenoid basal carcinoma in the lower
female genital tract. Oncol Rep. 41:1769–1778. 2019.PubMed/NCBI
|
|
38
|
Verlaat W, Snijders PJ, van Moorsel MI,
Bleeker M, Rozendaal L, Sie D, Ylstra B, Meijer CJ, Steenbergen RD
and Heideman DA: Somatic mutation in PIK3CA is a late event in
cervical carcinogenesis. J Pathol Clin Res. 1:207–211. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Ligresti G, Militello L, Steelman LS,
Cavallaro A, Basile F, Nicoletti F, Stivala F, McCubrey JA and
Libra M: PIK3CA mutations in human solid tumors: role in
sensitivity to various therapeutic approaches. Cell Cycle.
8:1352–1358. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Cancer Genome Atlas Research Network, .
Comprehensive molecular characterization of urothelial bladder
carcinoma. Nature. 507:315–322. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Cancer Genome Atlas Network, .
Comprehensive genomic characterization of head and neck squamous
cell carcinomas. Nature. 517:576–582. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Cancer Genome Atlas Network, .
Comprehensive molecular portraits of human breast tumours. Nature.
490:61–70. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Bredin HK, Krakstad C and Hoivik EA:
PIK3CA mutations and their impact on survival outcomes of patients
with endometrial cancer: A systematic review and meta-analysis.
PLoS One. 18:e02832032023. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Chaudhari A, Krumlinde D, Lundqvist A,
Akyurek LM, Bandaru S, Skalen K, Ståhlman M, Borén J, Wettergren Y,
Ejeskär K and Sopasakis VR: p110alpha hot spot mutations E545K and
H1047R exert metabolic reprogramming independently of p110alpha
kinase activity. Mol Cell Biol. 35:3258–3273. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Guo S, Loibl S, von Minckwitz G,
Darb-Esfahani S, Lederer B and Denkert C: PIK3CA H1047R mutation
associated with a lower pathological complete response rate in
triple-negative breast cancer patients treated with
anthracycline-taxane-based neoadjuvant chemotherapy. Cancer Res
Treat. 52:689–696. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Janku F, Wheler JJ, Naing A, Falchook GS,
Hong DS, Stepanek VM, Fu S, Piha-Paul SA, Lee JJ, Luthra R, et al:
PIK3CA mutation H1047R is associated with response to PI3K/AKT/mTOR
signaling pathway inhibitors in early-phase clinical trials. Cancer
Res. 73:276–284. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Jiang W, Wu Y, He T, Zhu H, Ke G, Xiang L
and Yang H: Targeting of β-catenin reverses radioresistance of
cervical cancer with the PIK3CA-E545K mutation. Mol Cancer Ther.
19:337–347. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Madsen RR, Le Marois A, Mruk ON, Voliotis
M, Yin S, Sufi J, Qin X, Zhao SJ, Gorczynska J, Morelli D, et al:
Oncogenic PIK3CA corrupts growth factor signaling specificity. Mol
Syst Biol. 21:126–157. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Kalinsky K, Jacks LM, Heguy A, Patil S,
Drobnjak M, Bhanot UK, Hedvat CV, Traina TA, Solit D, Gerald W and
Moynahan ME: PIK3CA mutation associates with improved outcome in
breast cancer. Clin Cancer Res. 15:5049–5059. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Spaans VM, Mahendra IN, Purwoto G,
Trietsch MD, Osse M, Haar NT, Peters AAW, Fleuren GJ and Jordanova
ES: The landscape of somatic mutations in Indonesian cervical
cancer is predominated by the PI3K pathway. Gynecol Oncol.
148:189–196. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Tewari KS, Monk BJ, Vergote I, Miller A,
de Melo AC, Kim HS, Kim YM, Lisyanskaya A, Samouëlian V, Lorusso D,
et al: Survival with cemiplimab in recurrent cervical cancer. N
Engl J Med. 386:544–555. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Jiang W, Ouyang X, Li C, Long Y, Chen W,
Ji Z, Shen X, Xiang L and Yang H: Targeting PI3Kα increases the
efficacy of anti-PD-1 antibody in cervical cancer. Immunology.
170:419–438. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Rohlin A, Wernersson J, Engwall Y, Wiklund
L, Bjork J and Nordling M: Parallel sequencing used in detection of
mosaic mutations: Comparison with four diagnostic DNA screening
techniques. Hum Mutat. 30:1012–1020. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Williams GA II, Wu AA, Eugene HC, Tsai YC,
Wong M, Nonogaki H, Hung CF, Wu TC, Vang R and Xing D:
Clinicopathologic features and viral status of low-risk HPV6 and
HPV11-associated squamous cell carcinoma of the uterine cervix and
vulva. Am J Surg Pathol. 49:458–470. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Palimaru I, Brugmann A, Wium-Andersen MK,
Nexo E and Sorensen BS: Expression of PIK3CA, PTEN mRNA and PIK3CA
mutations in primary breast cancer: Association with lymph node
metastases. Springerplus. 2:4642013. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Kolodziej P, Nicos M, Krawczyk PA, Bogucki
J, Karczmarczyk A, Zalewski D, Kubrak T, Kołodziej E, Makuch-Kocka
A, Madej-Czerwonka B, et al: The correlation of mutations and
expressions of genes within the PI3K/Akt/mtor pathway in breast
cancer-a preliminary study. Int J Mol Sci. 22:20612021. View Article : Google Scholar : PubMed/NCBI
|